Back to Journals » Journal of Multidisciplinary Healthcare » Volume 15
A Qualitative Study of Older Adults’ Experiences of Embedding Physical Activity Within Their Home Care Services in Ireland
Authors Burton E ![]() , Horgan NF, Cummins V, Warters A
, Horgan NF, Cummins V, Warters A ![]() , Swan L, O'Sullivan M
, Swan L, O'Sullivan M ![]() , Skelton DA, Townley B, Doyle F
, Skelton DA, Townley B, Doyle F ![]() , Jabakhanji SB, Sorensen J
, Jabakhanji SB, Sorensen J ![]() , Rooney D, Murphy L, Galvin R
, Rooney D, Murphy L, Galvin R ![]()
Received 29 November 2021
Accepted for publication 7 March 2022
Published 19 May 2022 Volume 2022:15 Pages 1163—1173
DOI https://doi.org/10.2147/JMDH.S351714
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Elissa Burton,1,2 N Frances Horgan,3 Vanda Cummins,3,4 Austin Warters,5 Lauren Swan,6,7 Maria O’Sullivan,7 Dawn A Skelton,8,9 Bex Townley,9 Frank Doyle,10 Samira B Jabakhanji,11 Jan Sorensen,11 Debbie Rooney,6 Lisa Murphy,6 Rose Galvin12
1Curtin School of Allied Health, Curtin University, Perth, Western Australia, Australia; 2enAble Institute, Curtin University, Perth, Western Australia, Australia; 3School of Physiotherapy, RCSI University of Medicine and Health Sciences, Dublin, Ireland; 4Primary Care Physiotherapy Services CHO9, Health Service Executive (HSE), Dublin, Ireland; 5Older Person Services CHO9, Health Service Executive (HSE), Dublin, Ireland; 6North Dublin Home Care (NDHC), Dublin, Ireland; 7Department of Clinical Medicine, Trinity College Dublin (TCD), Dublin, Ireland; 8School of Health and Life Sciences, Glasgow Caledonian University, Glasgow, Scotland; 9Later Life Training Ltd, Killin, Scotland; 10Department of Health Psychology, RCSI University of Medicine and Health Sciences, Dublin, Ireland; 11Healthcare Outcomes Research Centre (HORC), RCSI University of Medicine and Health Sciences, Dublin, Ireland; 12School of Allied Health, Ageing Research Centre, Health Research Institute, University of Limerick (UL), Limerick, Ireland
Correspondence: Elissa Burton, Curtin School of Allied Health, Curtin University, GPO Box U1987, Bentley, Western Australia, 6845, Australia, Tel +61 8 9266 4926, Fax +61 8 9266 3699, Email [email protected]
Purpose: Physical activity has been shown to improve older adults’ functional capacity, independence, and quality of life. In a feasibility study, we embedded a movement approach within older adults existing home care services through “Care to Move” (CTM). The aim of this qualitative study is to explore older adults’ experiences of CTM within their home care support services and to identify the strengths and barriers of engaging in CTM from the perspective of the older recipient.
Materials and Methods: We conducted semi-structured telephone interviews with 13 older adults and one informal carer. Topics covered included participants’ overall experiences of CTM, changes to their overall activity and participation, aspects of CTM that they found valuable and issues that were challenging. Interview transcripts were coded and analyzed thematically to capture barriers and facilitators to the approach delivery.
Results: Four themes were developed: i) “I have good days and bad days”, ii) “safety and security is the name of the game”, iii) “we’re a team as it stands’, iv) “it’s [COVID-19] depressing for everybody at the moment”. Older adults identified benefits of CTM engagement including improvements in physical and psychological wellbeing. However, subjective frailty and self-reported multimorbidity influenced overall engagement. Participants expressed concerns around the logistics of delivering CTM and competing care staff interests. The broader role of care staff in supporting CTM was highlighted, as well as the emotional support that staff provided to older adults. Care staff continuity was identified as a barrier to ongoing engagement. The impact of COVID-19 on older adults physical and mental health negatively impacted the delivery of the approach.
Conclusion: Our findings suggest that embedding CTM within home care services is feasible and that older adults enjoyed engaging in CTM. Addressing care staff continuity and adopting individual approaches to CTM delivery may enhance the implementation of services.
Keywords: movement, older people, community care, motivation, barriers, home support
Introduction
The proportion of older adults (aged 65 years and over) is increasing in many countries, as life expectancy continues to rise. Ireland is one such country experiencing this, with a population of 696,000 older adults,1 which is predicted to double to 1.56 million by 2051.2 Many older adults live long and productive lives. However, it is also well known that a proportion will have multiple health conditions and in the latter years, experience reductions in physical function and decreases in strength, balance and endurance, often due to disuse, which can impact their ability to live independently.3
In Ireland in 2020, it was estimated that 53,700 older adults received a home support service to assist them to keep living in their homes.4 The average age for those receiving home support services was over 80 years.5 The Irish Longitudinal Study on Aging (TILDA) also found that 30% of those aged 85 years and over in their study were receiving home support services.6 Although home care support services such as personal care, meal preparation, medication prompts assist older adults to maintain their independence, ultimately over the longer term, these regular services do not help older adults to maintain their physical function.
A study by Kelly et al5 in Ireland found the prevalence of frailty amongst those receiving home support services to be 41.5%, and the frailer a person was, the more services they received.6 Frailty is accepted as a dynamic process but transitioning to a frailer status is more usual than transitioning out of frailty. Furthermore, the development of frailty often results in subsequent decline that manifests itself as increasing incidence of adverse outcomes including falls, functional decline, and hospital admission.7 To reduce the likelihood of transitioning into frailty, physical activity interventions and/or prehabilitation,8 nutritional interventions, geriatric evaluations and care tailored to the individual and/or cognitive training may be effective.9
Physical activity and/or exercise interventions specifically including older adults receiving home care support services are limited,10,11 particularly considering the millions of older people globally receiving services in their homes. Of the 18 studies included in the home care systematic review, many described multi-factorial interventions that included resistance training or repetitive functional tasks to improve activities of daily living (ADLs), such as stair walking, transferring and lifting shopping bags, or incorporating exercises into daily tasks, like bending the knees to pick up laundry or lifting up onto toes at the bench, while waiting for the kettle to boil.10 These findings also align with earlier research that found older adults receiving home care (support) services do not like to participate in structured exercise programs,12 even though the evidence demonstrates the many benefits they would gain from participating in such programs.13,14 Due to these findings, in more recent years researchers have been investigating ways of incorporating activity into functional or daily tasks and changing the language around “exercise”, to encourage older recipients of home support services to “move more” and prevent physical decline.
One of these approaches to being more active is Care to Move (CTM). CTM is designed to encourage the older adult to “move more” with activities associated with self-care and to incorporate mobility within their day using “movement prompts”, rather than being set a structured program and advised, for example, to complete 10 exercises, three times a day, every day.15 Another benefit of CTM is that it is aimed at being a whole workforce approach, where the language and messaging around delivering CTM remains the same regardless of who is speaking with the person receiving the support services.15 Due to the strengths of CTM it may be a beneficial approach to utilize with older adults receiving home support services, however to date no formal research evaluation has been undertaken.
The HSE in collaboration with key stakeholders made contact with the research team in 2015–2016 as there were already a number of aging studies nearing completion. In 2017, we applied for and successfully received a Health Research Board (HRB) Applied Partnership Award (APA) to undertake a feasibility study. The funding was awarded in 2018 and commenced 2019. This qualitative study is part of the larger feasibility study undertaken to determine whether CTM is feasible and acceptable to be implemented with older adults living in the community who were receiving home (care) support. More information about the feasibility study can be found in the published protocol.15
The aim of this current study was to explore the experiences of older adults undertaking the CTM approach within their home support services and to identify the strengths and barriers of adopting CTM from the perspective of the older recipient.
Materials and Methods
The Consolidated Criteria for Reporting Qualitative Research (COREQ) guidelines were followed to standardize the conduct and reporting of the study.16
Study Design
We employed a qualitative descriptive approach to facilitate the exploration of the views and experiences of CTM from the perspective of the individuals who participated (and in one case, their family member).
Potential Participants
Older adults (≥65 years), in receipt of home care support, who had a Clinical Frailty Score17 of 6 or less, had fallen at least once in the last year, and were independently mobile (with or without a walking aid), were recruited from a not-for-profit home care organization located in Dublin (Ireland). Care managers, supervisory staff and home care workers reviewed and screened a list of all service users eligible for CTM based on the inclusion criteria. Eligible service users were provided with a study invitation letter and participant information sheet and received a follow-up call within a week to establish if they would like to participate. A face-to-face meeting was subsequently arranged with the research physiotherapist (VC) to discuss the project.
Ethical Considerations
Ethics approval was obtained from the Royal College of Surgeons in Ireland Research Ethics Committee [Ref REC −2018:1489] and complies with the Declaration of Helsinki. All potential participants were provided with a detailed participant information leaflet that explained the purpose of the study, potential risks and benefits, issues relating to confidentiality in handling the data collected, anonymity in interviews and confidentiality in reporting (eg publication of anonymized responses) and disseminating the aggregate findings of the study. The information leaflet also detailed that study participation was entirely voluntary and that participants could withdraw at any time without any impact on their care. Explicit informed consent was obtained from all participants prior to commencement in the research.
Data Collection and Interviews
Participants received CTM for six months. Quantitative assessments were completed during home visits at baseline, after eight weeks and at six months by a research physiotherapist (VC). Semi-structured interviews were conducted in-person or via telephone between January – March 2021 with all participants left in the study. All interviews were audio-recorded for later transcription and notes were also recorded.18 The Supplementary Information (document) contains the interview guide which was developed to reflect the overall study aim, background literature and based on guidelines for conducting semi-structured interviews.19 Topics covered in the interviews included participants’ overall experiences of CTM, changes to their overall activity and engagement because of participation in CTM, aspects of the approach that they liked or found valuable and finally issues that they found challenging.
All interviews were conducted by one researcher (VC), a senior, female, physiotherapist who prior to this research study had no established relationship with any of the participants. The average length of interviews was 11 minutes (range from 7 to 17 minutes). Interviews were undertaken until no new information arose, each participant was interviewed once.
Care to Move (CTM)
Underpinned by behavior change principles and a series of pre-set “movement prompts”, CTM provides a clear framework for a whole workforce approach to supporting older people to move more frequently and efficiently. Increasing movement minutes with CTM approaches leads to increased feelings of confidence (balance) and having better movement to cope with the strength requirements of life. CTM is not a structured exercise program, as movement prompts are deployed by the workforce as part of everyday activities which means movements can be repeated across hours and days rather than in single (usually weekly) bouts expected in structured exercise programs. CTM has identified 12 essential movements from everyday life (eg, active sitting, hip walking, standing, shoulder movement) that form the “tool-box” of movements deployed alongside skilled, targeted conversations during usual interactions undertaken by care support staff. The consistent application of movement prompts and conversational skills aims to increase physical literacy and (by focusing on movement already being achieved), empowers older people to make different decisions about their sitting behaviors. The home care staff completed two-day CTM education comprising; “how to have meaningful conversations about movement”, interaction skills, understanding the essential movements and prompts and as added value, where applicable, this increased knowledge and conversation skills, which further supported the motivation for older people to engage with home exercise programs prescribed by therapy services.
Data Analysis
All interviews were transcribed verbatim by an independent data transcription company. Member checking was not completed following verbatim transcription. Data were collectively analyzed using a reflexive approach to thematic analysis.20–22 This inductive approach is data-driven without trying to fit data into an existing coding frame, or the researcher’s preconceived notions or presumptions.20
Phase one involved two experienced qualitative researchers (EB & RG) independently reading and re-reading the transcripts in their entirety. Phase two involved independent development of initial codes through an open coding approach, in Microsoft word, followed by organizing all the potentially relevant codes to generate themes in Phase 3. This third phase was supported by virtual discussions between RG and EB and conferring electronically with the researcher who collected the data (VC). Phase four was accomplished through the process of reviewing the coded data and then reviewing potential themes against the original dataset. Phase five involved scrutinizing potential themes against original data; then names were given to each theme. Phase six included the final analysis of the data, development of the conceptual map, full review with the research team and writing-up of the narrative report. Names were changed in the original transcripts to ensure anonymity of participants and carers.
Trustworthiness
As mentioned earlier, this study is part of a larger feasibility study, which will be published elsewhere. Multiple forms of data collection were undertaken over a number of assessment timepoints and although they were not specifically included in this current study, it did mean data and researcher triangulation occurred.23 For example, the researcher who interviewed the participants also collected the outcome data for the feasibility study. Data were initially analyzed independently by two experienced researchers, which improved trustworthiness.24 The two researchers who analyzed the current participant interview data, also discussed and debriefed the initial findings with the researcher who collected the outcome data, to further confirm the credibility of the results.23 Dependability was obtained by working through the six phase process outlined by Braun and Clarke20 as described in the data analysis section above.
Results
Thirteen participants were interviewed, plus one family member, demographic details for the one family member are not available. Table 1 describes the demographic details of these 13 participants.
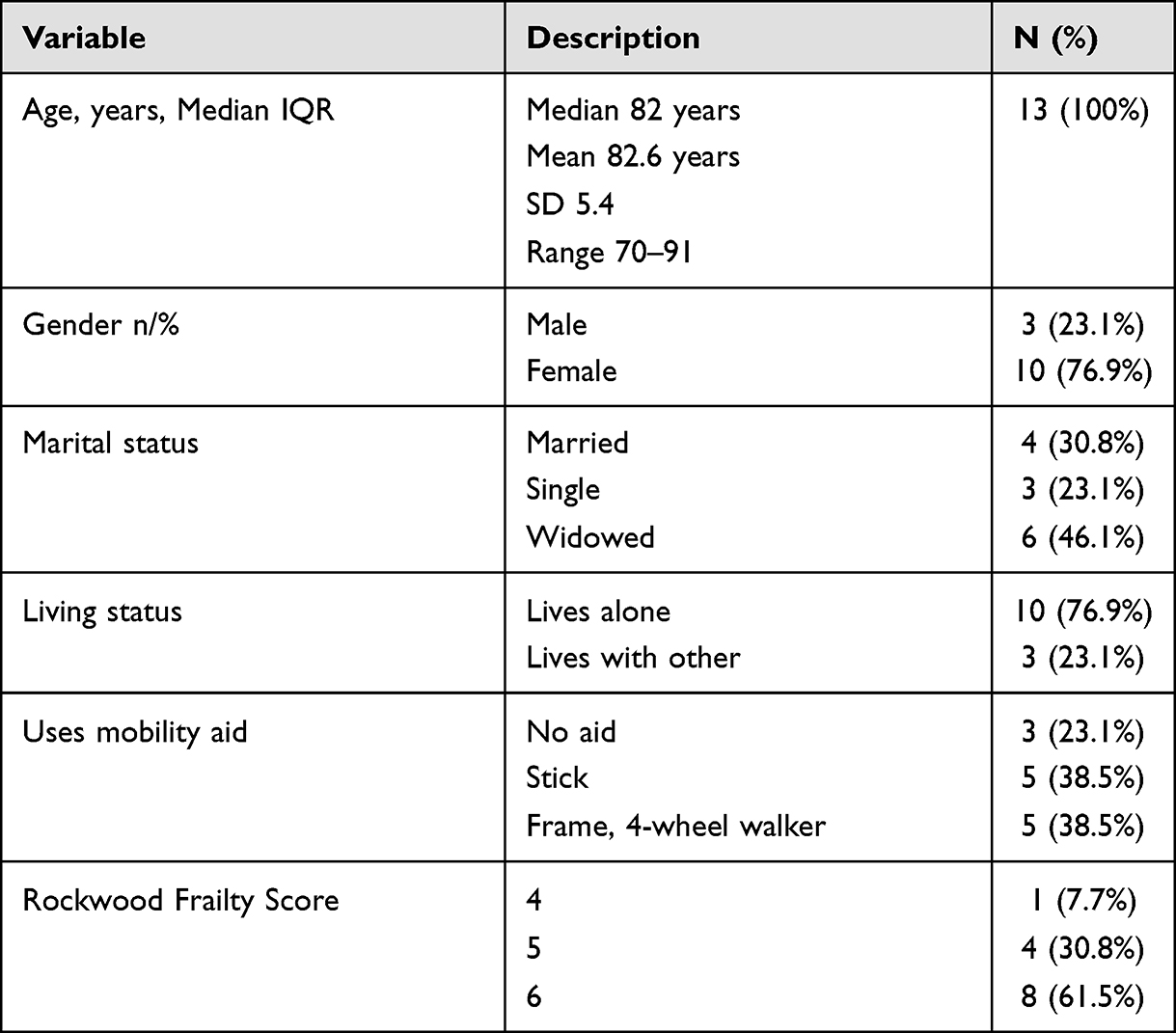 |
Table 1 Demographic and Clinical Characteristics of Interview Participants |
Four themes arose from the data, these included 1) “I have good days and bad days”, 2) “safety and security is the name of the game”, 3) “we are a team as it stands”, and 4) “it is depressing for everybody at the moment”. Some of the themes overlapped at times, however each theme contained specific subthemes, which identified the benefits and barriers to engaging in CTM. Figure 1 illustrates the four themes and subthemes.
 |
Figure 1 Concept map of the interview data. Note: CTM is Care to Move, ↑ indicates an increase, ↓ indicates a decrease. |
Theme 1 – “I Have Good Days and Bad Days”
Participants identified both physical and psychological benefits following engagement in CTM, including an increase in strength and confidence. While some participants noted that CTM was challenging at the outset, participants reported feeling the difference in terms of less pain, better movement, and an ability to do more activities.
It was great. I was able to move around much better and it was all painful in the beginning but the more I did them, the exercises and the movement, it was much better. CTM 037
That’s what I do at the sink you know, and then I go on my toes, I can reach now the top shelf which I couldn’t before. So I do exercises even sitting down I press down on my toes, lift my heels and I found that good. That I can reach the top shelf now. CTM 038
However, participants acknowledged that the co-existence of frailty, multimorbidity and illness influenced the degree in which they engaged with the “prompts”. Several participants highlighted the impact of an exacerbation of pre-existing conditions on balance and mobility. Fatigue was also noted by some participants as a limiting factor in terms of participation in CTM.
The fingers and hands I have very little use of my fingers I can’t feel things. But we did exercises for that, now, I think they were the ones I couldn’t do not so much I couldn’t do but I wouldn’t do because I know I would be in pain. I’ve been for pain management with my shoulder and there’s nothing they can do with it at this stage. CTM 028
I can look after myself although I am unsteady. Unsteady really is the word. But also, I’m not very robust, fragile, and unsteady I would say. But I do movement, I do movement, I mean I’m actually starting to do a little gardening. But my balance isn’t that good I’ve got to be very careful. I have to keep my alarm on me and keep my phone within distance, but I’ve only fallen once in the two years that I’ve been home. CTM 011
Motivation to do the movements was also highlighted by participants, both self-motivation and carer encouragement to engage. In some cases, this manifested itself as implicit and explicit goal setting by the participant. A small minority of participants expressed a lack of interest in engaging in the CTM approach as they perceived that they were too old, did not like to walk or did not want to “exercise” due to pain.
I didn’t need motivation. And I mean I do my own movement anyway. It’s nice to know that the carers are, are anxious to get you to move and are prepared to motivate you. CTM 011
But I did find, and the help I got like with the home help and that is brilliant as well. And she encourages me to do the exercises, which is good, … we don’t do very much, it wouldn’t be an hour or anything, but it would be just enough to keep you mobile … … I would set a goal to be able to go up the stairs without holding onto the banisters. That would be my goal but whether that happens now or not. CTM 038
Theme 2 “Safety and Security is the Name of the Game”
This theme focuses on the logistics of adopting the CTM approach. Safety and security were paramount and compounded by the COVID-19 pandemic which, hampered consistent delivery of the CTM approach. Issues included carer access, time with the carer, transport (especially during COVID-19) and physical space to move. In cases where movement outdoors was encouraged, the variability in the weather hampered engagement. “If the weather is crap, that rules out the walk” CTM 004.
This COVID virus has really put a halt to a lot of things for me because I can’t, ….my original plans were maybe the carer who is in, in the morning would bring me for a little walk up, a small walk up the road. That can’t be done now. because I, the carer has to be sure that we are not going to meet somebody, not going to have to say, oh no don’t stop here because maybe we would pick up the bug from them. CTM 027
I think that with COVID we were all locked in things were different, the carers were rushing to get out not to stay with you. Whereas I think you have to have the carers here a little longer for each time, if you could make a plan that you came at a certain time and stay and do what exercises you could do you know. CTM 040
Yes. Well, firstly if I may say that with regard to the … time is of the essence, not enough time to do the thing properly, safely. CTM 010
but twenty minutes is too short for them to do anything really. Because especially if it’s raining and they have to take off their clothes and their hat and put them on the rads to dry. CTM 010
Several participants highlighted the importance of a tailored approach to delivery, acknowledging that “people should be treated more individually” CTM 038 when participating in CTM. Some participants liked doing CTM by themselves, while others preferred to only do it with the carer. Issues around carer priorities when visiting the client and scope of practice of the carer were identified as barriers to CTM delivery.
It’s nice to know that the carers are, are anxious to get you to move and are prepared to motivate you. But as against that the amount of help they give in a physical sense is limited. I understand that that’s because the, the carers are not allowed to, to physically help you. I don’t know to what extent they can actually touch you or pick you up if you fall but I understand they are not allowed to do that. CTM 011
The importance of listening to the client was highlighted by some participants.
It is very, very important that they listen carefully to the needs of the person that they’re dealing with because not one size fits all. CTM 009
Theme 3 “We are a Team as It Stands”
A persistent thread across all participant interviews was the central role of carers. Participants identified a range of roles that the carers fulfilled in terms of emotional support, encouragement, reminders and meaningful discussion with the clients in relation to CTM.
Yeah, Karen does, everyday she comes “did you do your movement?” and I say “I did” and then maybe, there for a while at Christmas I didn’t do them at all and she’s here “you’ll have to get moving again” you know. So I started them there only what was it, last week only again. It’s much better to be doing them than sitting around you know. CTM 037
He keeps all the entries going, writing a book. He watches doing my exercises and walks and move. That’s what I like about him CTM 003
Some participants reported that CTM strengthened the bond between the carer and client. In other cases, participants identified an increase in independence away from relying on the carer when engaging with CTM.
But it does give one a bit of confidence to think that well, this can be done and somebody knows I can do it and so, I can try, you know, and if I don’t achieve what I’m trying to do, well okay, I’ll talk that through with the carer the next day. CTM 009
But then we, my carer and myself, you know … we are that kind of people that say, right, we do this, it’s not “you do this and you do that”, it’s we will do this and we’ll try it and we’ll see how we get on. That’s, you know, how we work in our ordinary caring day. CTM 009
However, carer continuity and a lack of sufficient numbers of carers trained, as well as locum carers, were noted by several participants as a barrier to delivery. Furthermore, buy-in from carers in the long term was identified as a potential barrier to future CTM delivery.
Well I had one most of the time but there were times when I had different ones when that girl was off because they are, you know, they take holidays, they are off for different reasons. So you have a different person and I found the stand in, locum, whatever, you know you call these people, is that they didn’t have a clue to be honest with you. CTM 009
But one thing I thought in the beginning was that we hadn’t enough of the carers trained to do the job you know it was supposed to work, and if you got a different carer in they didn’t know how to do it with you. CTM 040
No, my fear really is that you know when you train the carer and the carer is there with you and you are showing them they know exactly what to do. But I’m not sure whether the long-term interest would remain and that they could continue to do it on a regular basis. It would depend very much on the carer and their buy-in and also the time constraints on their visits. CTM 034
Participants also identified that some carers may need further training to build confidence in terms of adopting the approach.
Some of them I think are only getting their feet, they really are only getting their feet in … I think the ones that are only starting, one girl there was only starting a month or something and she said you have to tell me what you want me to do because she said I’m as nervous as hell. I said don’t be nervous … CTM 010
But I do think that the carer people should get more instruction about it. To give them more confidence to sort of deal with the situation. I would say it’s confidence that has to come from the carer and that confidence maybe has to come from the instructor to give them the confidence to give it to the person they’re dealing with. CTM 009
Theme 4 “It is Depressing for Everybody at the Moment”
The impact of COVID-19 featured in several of the interviews, with regards to the impact not only on CTM, but the wider implications in terms of social isolation for older adults, “10 months is a long time” CTM 027. Participants expressed a fear of the virus, particularly with regards to meeting other people. Loneliness, isolation and its impact on mental health of participants was noted by some participants.
Maybe extra phone calls might, you know, but maybe extra phone calls how are they doing or to talk to maybe some people don’t have anybody to talk to. That end of it, the mental end of it you know. I’m sure there’s people really been affected, sometimes I’m down and then I’m fine again. But I’m not down, only a day maybe and if the weather is good, I find it lifts my spirits you know. Where I appreciate the sun now more. (laughing) the fine weather, a lovely day I appreciate it more. CTM 038
Apart from being company in the house for me they do cook bits and they sort of sit and talk to me. Now there’s a virus at the moment which has really affected the whole world. But it affected me particularly … CTM 027
Some participants reported an increased dependence on their family support network and the wider community during the period of COVID-19 lockdown.
I have a family member that will come and take me. And they have been very, very good, very cognizant of the fact that I, you know, I’m not a hundred percent with the legs and they will help me, very gingerly along the way, support me and tell me how to get into the car and be very careful and you know, getting out of it as well. CTM 009
And I’ve very good neighbours, and during the pandemic the postman and all wanted to get me stuff. I had a friend of mine getting me stuff and all the neighbours knocking at the door. CTM 010
More specific to CTM, carer routine was impacted, and carers spent less time with clients. There was some sympathy towards carers in terms of the volume of work that needed to be completed in the limited time available.
In the last few years, I had them, you see, I had them for a long time they’d always have time to talk and tell you how things were getting on and they wouldn’t have much time for that anymore. And it’s just that they are all stressed out working so hard. CTM 040
Discussion
This study explored the experiences of older adults undertaking the CTM approach within their home care support services and identified the strengths and barriers of engaging in CTM based on the experiences of the older recipient. Overall, the older adults who participated described many benefits, including both physical and psychosocial. This is similar to previous research, which identified motivators and barriers to older people receiving home care support services in Australia, which were both a short-term restorative service and longer-term ongoing services.25 Burton et al25 found that well-being, health, fitness and being social with family or friends were the main reasons they liked to be physically active. The older adults who participated in CTM described improvements in their strength, balance and movement, and an increase in confidence and feeling motivated, illustrating physical activity and movement of any type can have similar positive outcomes for frail, older people.
Barriers to participating in CTM included subjective frailty, self-reported multi-morbidities, fatigue, illness, pain, a lack of interest or not liking to exercise and feeling too old. Environmental barriers were lack of space within the home, the weather and experiencing transport difficulties. Again, the findings in the Australian study reflected those found for this CTM study, where older Australian home care clients were not physically active due to ongoing injury or illness, pain, feeling too old, lack of transport, the weather and not being interested in exercise.25 Other studies have also found poor health to be a barrier to being active.11,26 The weather being a barrier reflected the country where the research was undertaken, with this current study taking place in Ireland, where rain was the perceived barrier, as was the case for another study with home care clients in the United Kingdom,26 whereas the Australian study25 reported hot weather in the summer (ie over 30°C for prolonged periods of time) as their barrier to participation.
Feeling too old or “old age” is often reported as a reason for not being physically active by older adults, not only for those receiving home care support services but for older people living in the community generally.10,27–30 However, it is not only a phenomenon perceived by older adults but also those who care for them in delivering home care support services.31 There is a distinct opportunity for home care support organizations to provide regular training for staff on approaches such as CTM, so that they can include strategies they can confidently implement to encourage and motivate their clients to move more or to become more active to maintain their health and independence, regardless of their age.
Care staff play an important role in the lives of older adults receiving home care support services.32 This study reflected this, with participants reporting strengthened relationships, which at times led to improved independence. However, maintaining care staff within an organization is a challenging prospect for many home care support organizations, not only those in Ireland.33,34 Due to these staff shortages, locum’s were often called in, who were not trained in CTM and a break in supporting the movement and activity of the client occurred. This also saw a change in the relationship where the care staff and person receiving care needed to begin again in building trust and rapport. If CTM is to be successfully translated into home care support organizations it is recommended all staff across the whole organization, including those providing care, need to be trained in the approach to avoid these changes in momentum. Also required are ongoing support systems and supervision processes and reporting, to ensure consistency and ongoing learning across the workforce.
CTM was chosen as the intervention for this feasibility study due to previous research illustrating many older adults receiving home care support services do not wish to exercise at this stage of their life.12 CTM focuses on prompting movements and the term exercise is not used within the approach.35 This difference, compared to usual exercise or physical activity programs utilized with this population was anticipated to increase the number of home care support clients willing to participate. Interestingly though, throughout the interviews the participants referred to CTM as exercise, or doing exercises, and therefore additional or a change to staff training may be required for better understanding of delivering the CTM approach. Also noted, was that some older clients wanted to only engage in CTM when the carer was with them, encouraging older home care clients to engage outside of these times would increase their movement and potentially lead to living independently for longer. It is recommended that future research be undertaken to better understand these two areas of interest and to encourage more movement and activity in this population.
The feasibility study commenced prior to the COVID-19 pandemic. However nine months into recruitment the pandemic began and Ireland went into lockdown in March 2020, curtailing child care, schooling and other aspects that affected carer staffing.36 This affected the CTM study and care staff made changes such as spending limited or no time in their clients’ home where possible, phone conversations became “visits” and when staff did go into homes interaction was time limited to keep both the clients and care staff safe. This was reflected in the results, where Theme 4 described an increase in social isolation and loneliness, decrease in mental health and an increase in stress for staff and their workloads due to the pandemic. Dependence on family and the community including neighbors and people such as the post-person, were also noted. Many of the findings reported were also found in Ontario and Nova Scotia, Canada where a qualitative study of home care clients and their caregivers was undertaken during COVID-19. They also found an increased need for family/friend support and that staff were working under difficult conditions and often cancelled appointments or had different staff members attend, particularly at short notice due to the pandemic and staff or clients becoming infected.37 Some physical activity programs became available on-line during this time, such as Homestrong (https://www.homestrong.net/) and Safe Exercise at Home (www.safeexerciseathome.org.au)38 and a movement approach called Make Movement Your Mission was introduced and became available three times a day through a Facebook page (https://www.facebook.com/groups/MakeMovementYourMission/). Many older adults throughout the United Kingdom logged onto the Make Movement Your Mission sessions, particularly throughout the lockdown periods and many allied health professionals encouraged their patients to participate also. These continue but as restrictions begin to lift, the importance of incidental activity in the maintenance of physical, social and mental health must be prioritized.
Due to the pandemic, there were limitations in the study, these included challenges in recruitment, maintaining participants throughout the project (interviews included only a third of the participants who commenced the feasibility study), along with completing the interviews in a timely manner. Not all interviews were completed face-to-face and completing interviews over the phone was more challenging for some. However, despite being conducted during a pandemic, a strength of the study was that it is possible to deliver the CTM approach and that older adults receiving home support services experienced benefits physically and psychosocially.
Conclusion
Our findings suggest that it is feasible to embed CTM within home care support services and that many older adults receiving care enjoyed engaging in CTM. Maintaining a whole of organization approach, potentially restructuring some services, addressing home support staff continuity, and adopting individual approaches to CTM delivery may enhance the implementation of services.
Acknowledgments
This work was funded by an APA-2017-013 Health Research Board of Ireland Applied Partnership Award. The authors would like to thank the interview participants from North Dublin Home Care and staff who delivered and participated in CTM.
Disclosure
Bex Townley and Dawn A. Skelton are Directors of Later Life Training Ltd, a not-for-profit company delivering training in exercise delivery with older people, including the Care To Move Approach. Debbie Rooney is CEO of North Dublin Home Care and Lisa Murphy is the Service and Quality Manager at North Dublin Home Care. Dr Elissa Burton reports grants from NHMRC Investigator Grant, outside the submitted work. Ms Lauren Swan reports grants from North Dublin Home Care, outside the submitted work. Dr Frank Doyle reports grants from Health Research Board, during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. Clark D Population of Ireland by age group in 2019. Statista; 2021. Available from: https://www.statista.com/statistics/710767/irish-population-by-age/.
2. Sheehan A, O’Sullivan R. Institute of Public Health - an overview of key statistics in Ireland and Northern Ireland. 2020.
3. Metti A, Best J, Shaaban C, Ganguli M, Rosano C. Longitudinal changes in physical function and physical activity in older adults. Age Ageing. 2018;47(4):558–564. doi:10.1093/ageing/afy025
4. Health Services Executive - Ireland. National service plan 2020; 2020. Available from: https://www.hse.ie/eng/services/publications/national-service-plan-2020.pdf.
5. Kelly S, O’Brien I, Smuts K, O’Sullivan M, Warters A. Prevalence of frailty among community dwelling older adults in receipt of low level home support: a cross-sectional analysis of the North Dublin Cohort. BMC Geriatr. 2017;17(121). doi:10.1186/s12877-017-0508-2
6. Murphy C, Whelan B, Normand C. Formal home-care utilisation by older adults in Ireland: evidence from the Irish Longitudinal Study on Ageing (TILDA). Health Soc Care Community. 2015;23(4):408–418. doi:10.1111/hsc.12157
7. Clegg A, Young J, Iliffe S, Rikkert M, Rockwood K. Frailty in elderly people. Lancet. 2013;381(9868):752–762. doi:10.1016/S0140-6736(12
8. Puts M, Toubasi S, Andrew M, et al. Interventions to prevent or reduce the level of frailty in community-dwelling older adults: a scoping review of the literature and international policies. Age Ageing. 2017;46(3):383–392. doi:10.1093/ageing/afw247
9. Marcucci M, Damanti S, Germini F, et al. Interventions to prevent, delay or reverse frailty in older people: a journey towards clinical guidelines. BMC Med. 2019;17(193). doi:10.1186/s12916-019-1434-2
10. Burton E, Farrier K, Galvin R, et al. Physical activity programs for older people in the community receiving home care services: systematic review and meta-analysis. Clin Interv Aging. 2019;14:1045–1064. doi:10.2147/CIA.S205019
11. Mjøsund H, Moe C, Burton E, Uhrenfeldt L. Integration of physical activity in reablement for community dwelling older adults: a systematic scoping review. J Multidiscip Healthc. 2020;13:1291–1315. doi:10.2147/JMDH.S270247
12. Burton E, Lewin G, Boldy D. Physical activity preferences of older home care clients. Int J Older People Nurs. 2015;10(3):170–178. doi:10.1111/opn.12065
13. Langhammer B, Bergland A, Rydwik E. The importance of physical activity exercise among older people. Biomed Res Int. 2018;2018:7856823. doi:10.1155/2018/7856823
14. Taylor A, Cable N, Faulkner G, Hillsdon M, Narici M, Van Der Bij AK. Physical activity and older adults: a review of health benefits and the effectiveness of interventions. J Sports Sci. 2003;22(8):703–725. doi:10.1080/02640410410001712421
15. Horgan N, Cummins V, Doyle F, et al. Enhancing existing formal home care to improve and maintain functional status in older adults: protocol for a feasibility study on the implementation of the Care to Move (CTM) programme in an Irish healthcare setting. JFSF. 2020;5(1):10–16. doi:10.22540/JFSF-05-010
16. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
17. Rockwood K, Song X, MacKnight C, et al. A global clinical measure of fitness and frailty in elderly people. Can Med Assoc J. 2005;173(5):489–495. doi:10.1503/cmaj.050051
18. Drabble L, Trocki K, Salcedo B, Walker P, Korcha R. Conducting qualitative interviews by telephone: lessons learned from a study of alcohol use among sexual minority and heterosexual women. Qual Soc. 2016;15(1):118–133. doi:10.1177/1473325015585613
19. McIntosh M, Morse J. Situating and constructing diversity in semi-structured interviews. Glob Qual Nurs Res. 2015;2:1–12. doi:10.1177/2333393615597674
20. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
21. Braun V, Clarke V, Hayfield N, Terry G. Thematic Analysis. In: Liamputtong P, editor. Handbook of Research Methods in Health Social Science. Springer; 2019:843–860.
22. Clarke V, Braun V. Using thematic analysis in counselling and psychotherapy research: a critical reflection. Couns Psychother Res. 2018;18(2):107–110. doi:10.1002/capr.12165
23. Nowell LS, Norris JM, White DE, Moules NJ. Thematic analysis: striving to meet the trustworthiness criteria. Int J Qual Methods. 2017;16:1–13. doi:10.1177/1609406917733847
24. Lincoln Y, Guba E. Naturalistic Enquiry. Sage Publications; 1985.
25. Burton E, Lewin G, Boldy D. Barriers and motivators to being physically active for older home care clients. Phys Occup Ther Geriatr. 2013;31(1):21–36. doi:10.3109/02703181.2012.751474
26. Whitehead P, Drummond A, Parry R, Walker M. Content and acceptability of an occupational therapy intervention in homecare re-ablement services (OTHERS). Br J Occup Ther. 2018;81(9):535–542. doi:10.1177/0308022618766844
27. Åhlund K, Öberg B, Ekerstad N, Bäck M. A balance between meaningfulness and risk of harm – frail elderly patients’ perceptions of physical activity and exercise – an interview study. BMC Geriatr. 2020;20(490). doi:10.1186/s12877-020-01868-2
28. Bopp M, Wilcox S, Oberrecht L, Kammermann S, McElmurray C. Correlates of strength training in older rural African American and Caucasian women. Women Health. 2004;40(1):1–20. doi:10.1300/J013v40n01_01
29. Burton E, Farrier K, Lewin G, et al. Motivators and barriers for older people participating in resistance training: a systematic review. J Aging Phys Act. 2017;25(2):311–324. doi:10.1123/japa.2015-0289
30. Meyer C, Dow B, Hill K, Tinney J, Hill S. The right way at the right time: insights on the uptake of falls prevention strategies from people with Dementia and their caregivers. Public Health Front. 2016;4:1–10. doi:10.3389/fpubh.2016.00001
31. Burton E, Boyle E, O’Connell H, Lewin G, Petrich M, Hill K. Community care staff attitudes towards delivering a falls prevention exercise intervention to community care clients. Health Soc Care Community. 2020;29(2):416–424. doi:10.1111/hsc.13101
32. Silverglow A, Johansson L, Lidén E, Wijk H. Perceptions of providing safe care for frail older people at home: a qualitative study based on focus group interviews with home care staff. Scand J Caring Sci. 2021;35:1–11. doi:10.1111/scs.13027
33. Eurofound. Long-term care workforce: employment and working conditions. 2020.
34. Talent for Care, United Kingdom Homecare Association (UKHCA). Retaining homecare workers in the independent and voluntary sector; 2020. Available from: https://www.homecareassociation.org.uk/asset/42EF14C4-4A8B-416D-927385AEEFF1042D/.
35. Later Life Training UK. About Care to Move (CTM) course. Later life training; 2021. Available from: https://www.laterlifetraining.co.uk/courses/care-move-ctm-course/.
36. Murray S. Timeline: the key dates in Ireland’s initial response to the global Covid-19 pandemic. thejournal.ie. Available from: https://www.thejournal.ie/timeline-ireland-coronavirus-5120358-Jun2020/.
37. Weeks L, Nesto S, Hiebert B, et al. Health service experiences and preferences of frail home care clients and their family and friend caregivers during the COVID-19 pandemic. BMC Res Notes. 2021;14(271). doi:10.1186/s13104-021-05686-6
38. Said C, Batchelor F, Duque G. Physical activity and exercise for older people during and after the coronavirus disease 2019 pandemic: a path to recovery. JAMDA. 2020;21:977–979. doi:10.1016/j.jamda.2020.06.001
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.