Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
A Protocol for the Development and Assessment of a Non-Pharmacological Intervention Designed to Improve Cognitive Skills of Adults with Intellectual Disabilities: A Mixed Method Design
Authors Alopoudi A ![]() , Makri M, Alişoğlu B, Doğan A, Imbesi A, Karakoyun M, Lacapelle A, Navarro Roux MA, Pissa A, Tsolaki M
, Makri M, Alişoğlu B, Doğan A, Imbesi A, Karakoyun M, Lacapelle A, Navarro Roux MA, Pissa A, Tsolaki M ![]()
Received 25 May 2023
Accepted for publication 12 September 2023
Published 1 November 2023 Volume 2023:16 Pages 3215—3226
DOI https://doi.org/10.2147/JMDH.S422859
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Aristi Alopoudi,1,2 Marina Makri,1– 3 Batuhan Alişoğlu,4 Abdullah Doğan,5 Antonino Imbesi,6 Mehmetcan Karakoyun,5 Alexis Lacapelle,7 Marco Aurelio Navarro Roux,4 Alexia Pissa,8 Magda Tsolaki1– 3
1Greek Association of Alzheimer Disease and Related Disorders, Thessaloniki, Greece; 2Department of Neurology, School of Medicine, Faculty of Health Sciences, Aristotle University of Thessaloniki, Thessaloniki, Greece; 3Laboratory of Neurodegenerative Diseases Center for Interdisciplinary Research and Innovation (CIRI - Auth), Balkan Center, Aristotle University of Thessaloniki, Thessaloniki, Greece; 4Association of Inclusive Society (AIS), Vienna, Austria; 5Eurasia Innovative Society Association, Bursa, Turkey; 6EURO-NET, Potenza, Italy; 7Interactive 4D, Nice, France; 8Synthesis Center for Research and Education Limited, Lefkosia, Cyprus
Correspondence: Aristi Alopoudi, Tel +30 2310 810411, Fax +30 2310 925802, Email [email protected]; [email protected]
Aim: This paper describes the steps of a protocol for developing and assessing a non-pharmacological intervention, specifically a Serious Game, with the goal of improving eight cognitive skills in adults with Intellectual Disabilities. Serious games that focus on one deficit and/or are restricted to one disorder have been developed to improve the cognitive skills of people with Intellectual Disabilities. There is a lack of a single tool that targets various cognitive skills as well as a broader spectrum of disorders.
Purpose: The presentation of the protocol which describes the steps of developing a new Serious Game that will be evaluated in a randomised control trial intervention.
Participants and Methods: The protocol is divided into three stages: identification of cognitive deficits and development of the Serious Game, randomised control trial intervention- follow up assessment, and evaluation of the Serious Game by trainers and caregivers. The participants of the intervention are adults with Intellectual Disabilities.
Results: The protocol’s results are expected to cover the development of a new Serious Game for specific cognitive functions of a mixed group of adults with Intellectual Disabilities, evaluating the structure and content of the game through neuropsychological assessments for participants and specific questionnaires for trainers and caregivers, evaluating the improvement of specific cognitive abilities in participants in the intervention; and measuring the possible improvement of the quality of life and social interaction of people with Intellectual Disabilities.
Conclusion: This is the first study to develop a protocol and implement and assess this new Serious Game. This Serious Game is expected to assist people with Intellectual Disabilities in cognitive and social aspects.
Plain Language Summary: What is the main purpose of this study protocol? The main purpose of this publication is to present the mixed-method study protocol created by the Game4CoSkills project. Following this protocol, a new mobile Serious Game, the Game4CoSkills, was developed with the goal of improving eight cognitive skills in adults with Intellectual Disabilities. The game will be used as an interventional tool by participants, and its effectiveness will be evaluated. They also interact with health professionals and play the game, as they test the new mobile Serious Game for the first time. Following the six-month trial period, both the intervention and control groups will undergo neuropsychological testing to determine the game’s effectiveness. Following the follow-up assessment, the trainers and caregivers will provide feedback on the game through two structured questionnaires. Adults with ID may benefit from their participation.
Keywords: mobile game, cognitive skills, mild cognitive impairment, autism spectrum disorder, down syndrome, adults
Introduction
Intellectual disability (ID) is a term used to describe a person who has limitations in cognitive functioning and skills such as communication, taking care of themselves, and social skills. These limitations will cause a person to learn and develop more slowly than the average person.1–4 Adults with ID may require more time to learn to speak, walk and care for their personal needs such as dressing or eating. They are likely to have trouble understanding and remembering throughout their lives.1–4 ID is characterised by deficits in intellectual and adaptive functioning, and its prevalence has been estimated to range between 1% and 3% of the population, with some regional variations.5,6
People with mild ID struggle to learn and understand complicated language and academic concepts.1,2,4,7 They can perform academically at the level of the fourth or fifth grade.2,7 They struggle with language, arithmetic, and writing in addition to language.1,2,7 They can acquire fundamental reading, writing, and math abilities with the proper assistance. Most people can fill out a fundamental job application and compose simple letters. They have trouble understanding behavioural norms appropriate for their age and social environment, communicating, and interacting with others.1,2 They can form deep family and personal relationships with ongoing support. They are constrained by social judgment and decision-making.1 People with moderate ID exhibit substantial impairments in their ability to read, write, do math, and perform other tasks that call for understanding fundamental concepts.2,7
People with intermediate ID may acquire some basic abilities, such as the capacity to read sight words, copy information, and match numbers to quantities of goods.2,7 They can achieve academic skills on the level of the first grade. Adults with severe ID have severely restricted language and communication skills. Their spoken language is significantly limited, and they may only be able to communicate using single words or phrases.1,2 Utilizing augmentative communication techniques may help them communicate more effectively. To express fundamental requirements, they frequently employ gestures. They have considerable difficulties with ideas related to numbers, quantity, time, money management, and problem-solving.1,2,7 They tend to engage and form relationships primarily with their immediate families and caregivers.8 Adults with ID, can be diagnosed with Dementia, MCI, mild/moderate or severe ID, ASD or Down Syndrome. People with MCI have more cognitive dysfunctions than predicted for their age, more depressive symptoms, worse quality of life, and avoidant coping methods, such as withdrawal from social interactions.9,10 MCI has a diverse clinical spectrum and has proven difficult to define, recognise, and monitor in clinical practice. MCI may not always develop to dementia and can remain stable or revert to normal cognition if reversible reasons such as disrupted sleep, depression and anxiety symptoms, medications, vitamin deficiencies, and so on, are present. MCI is an acquired disorder and the difference between mild or moderate ID is that people with MCI are adults with acquired cognitive deficits, while mental retardation is not an acquired disorder but the individual was born with it. The cognitive function in MCI is mainly higher than in mild or moderate ID.
Assistive technology (AT) aids functioning, by allowing for independent actions and decision-making while also promoting well-being. AT facilitates social integration for people with cognitive dysfunctions and helps manage their frequent comorbidities.11 As the population ages, the demand for AT for older people with ID rises. Aging and environmental factors can cause cognitive decline in this group, and people with ID often lack access to healthcare services and AT. Additionally, AT supports rehabilitation and home-based practice helps not only to maintain cognitive functions and mental health, but also reduce rehabilitation costs.11,12 Internet use can empower individuals with ID to make life decisions, promoting app use and online interaction for entertainment, education, and socialization.13
Serious games (SG) are educational AT linked to improving cognitive skills, such as attention, problem-solving, socializing and enhancing daily skills, mental health and behaviour of older people with ID.14–16 SG proved beneficial, practical, enjoyable, and user-friendly interventions for people with ID, improving cognition and motor skills.16–21 Moreover, playing SG enhances attention, spatial cognition, perception, and physical abilities, all crucial for daily life.22,23 However, few cognitive skills have been studied. While SG’s cognitive impact on people with ID is abundant for children, but scarce for adults. For example, most studies have explored using SG to improve attention in students with ID and few have investigated SG’s impact on decision-making, problem-solving, working memory, academic skills and daily activities of adults with ID.23,24 Literature shows that a SG positively affects learning, social interaction, communication, and cognitive skills in ID or ASD.25,26 SG also aids ID people with daily tasks, such as shopping and reading.3,27 No studies have examined the effects of SG on main cognitive functions, such as visual recognition, calculation, logic, attention, dexterity, multitasking, memory, and accuracy in adults with ID. A new study is needed using mobile SG (more accessible) to assess the cognitive functions of people with different ID diagnoses (mid/moderate ID, MCI, ASD, and DS).24,25
The aim of this study is to present a mixed-method study protocol. The protocol is designed to develop the mobile Serious Game “Game4CoSkills” for adults with ID. The game is intended for use in clinical practice as an intervention tool for the development of cognitive skills in a wide variety of diagnoses. The main hypothesis of implementing this intervention (six-month trial of the game) is that the intervention group, which participates in the interventions twice a week for six months, will perform better on global cognition tasks, such as those that test colour recognition, memory, calculation, attention, critical thinking, multitasking, dexterity, and attention to details, compared to the control group, which will receive the intervention later. Another goal of implementing this intervention is to have a positive impact on participants’ quality of life and social interaction.
In summary, this study has the following primary objectives: 1) to develop a new mobile SG for specific cognitive functions for a mixed group of people with ID; 2) to evaluate the structure and content of a new mobile SG using neuropsychological assessment for participants and specific questionnaires for trainers and caregivers. The secondary objectives are: 3) to evaluate the improvement of specific cognitive abilities in participants in the intervention; 4) to measure the possible improvement of the quality of life and social interaction of people with ID.
Materials and Methods
A literature review was conducted to assess the needs of adults with ID in order to develop this protocol. The presented protocol describes a mixed-method study consisting of three stages. The study is being conducted in six European countries (France, Austria, Greece, Italy, Cyprus, and Turkey). The mixed-method study employs both qualitative and quantitative research methods to create and evaluate the effectiveness of the developed game. Mini games are used as an intervention tool in the protocol to gain a better understanding of the cognitive dysfunctions in eight different skills. After several trials, it will be determined whether cognitive skills can be improved using this SG which will be tested in a specific intervention. This is based on the fact that literature shows that interventions utilizing SG turn to be more effective than the traditional approaches that have been used in previous works. Additionally, this protocol adheres to a specific methodology for the collaboration of trainers of adults with ID. First, the team group is focuses on conducting a literature review about the cognitive needs of adults with ID. Then, the team group structures questionnaires for the health professionals, giving necessary information for the cognitive deficits of adults with ID. Following the selection of the questionnaires and the analysis of the data, the technicians create eight mini games based on eight cognitive skills and the new mobile SG is developed. Stage 2 involves participants playing the game for six months after it has been developed. The interventional tool is included in the new SG, and they practice for their cognitive functions. A follow-up assessment is performed, and participants in the intervention group are evaluated using neuropsychological tools to determine the impact of the game on their cognitive skills. The intervention will be delivered later to the control group. Trainers and carers of adults with ID provide feedback for the game via questionnaires in stage 3. Figure 1 describes the flow of the participants and Figure 2 describes the stages.
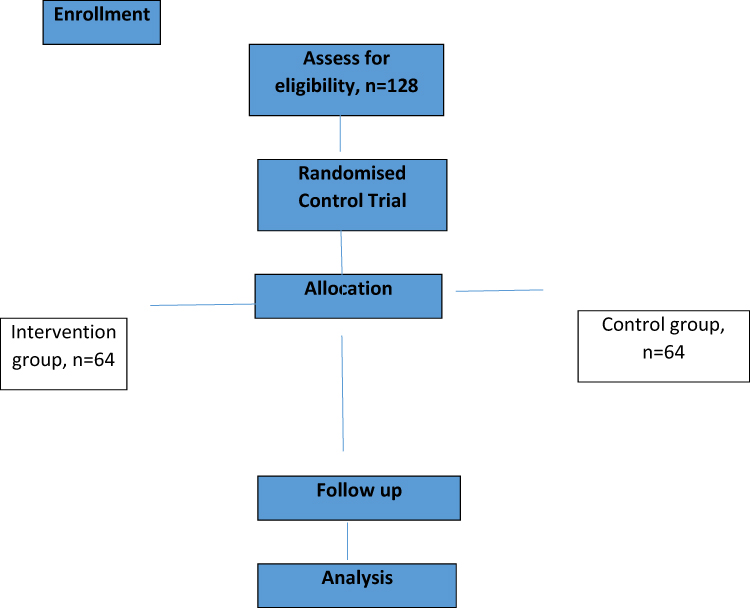 |
Figure 1 Flowchart of participants. |
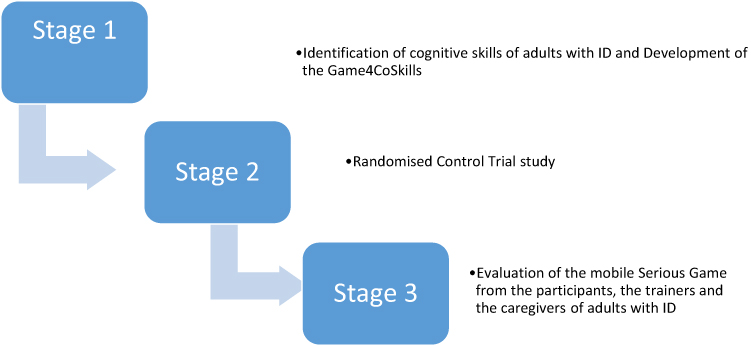 |
Figure 2 Stages of the mobile Serious Game mixed-method study. |
Furthermore, this innovative protocol is successfully submitted and granted by the Erasmus+KA2 - Cooperation for Innovation and the Exchange of Good Practices - KA220 - Strategic Partnerships for Adult Education (project number: 2021-1-FR01-KA220-ADU-000026181). The “Mobile Game for cognitive skills development and concept teaching for adults with ID” (Game4CoSkills) project is coordinated by the Interactive-4D Organisation (France) and is supported by the partners of the collaborative Organisations (Austrian Association of Inclusive Society (Austria), SYNTHESIS (Cyprus), Eurasia Innovative Society Association (Turkey), Alzheimer Hellas (Greece), and EURO-NET (Italy). All partners activate in the field of cognitive disorders, and AT and come from European countries with similar interests in the research field and innovations.
Stage 1: Identification of Cognitive Deficits in Adults with ID and Development of the Game4CoSkills
An extensive systematic review of the literature is performed regarding the cognitive skills of adults with ID. Each participant’s abilities should be evaluated using the literature. A questionnaire is included in the current approach. This stage of the study focuses on gathering demographic information and assessing participants’ cognitive abilities. Each country’s health professionals (doctors, nurses, special education teachers, speech-therapists, psychologists and other.) complete an “Assessment questionnaire” with two parts. The questionnaires are distributed online using an active link for one month via Google Forms, thus, online data collection and statistical analysis follow. All data will be saved for 10 years, for validation reasons and future analysis if it is needed. This information used to create the profile of all participants (health professionals and adults with ID). The questionnaire contains demographic data and statements that are answered by selecting the appropriate answer, such as: No, I do not know, He/she has often difficulties, He/she has sometimes difficulties, Yes. The statements will be the following:
- He/she recognises colours
- A colourful picture is visible to him/her.
- He/she usually remembers where he/she put personal items (keys, phone, documents, etc.).
- He /she has difficulty in recalling names of people or places.
- He /she can calculate a shopping bill quickly and accurately.
- He /she can solve math problems in his/ her mind.
- He /she can put things in order correctly.
- He /she can retain details on a topic.
- He /she can easily interpret maps.
- He /she can use critical thinking.
- He /she can do a puzzle.
- He /she stays focused on tasks despite distractions.
- He /she can do a to-do list.
- He /she can prioritize his/her daily tasks.
- He /she can recognise the differences between two pictures in their details.
- He /she can remember details of a story he/she has just heard.
- He /she can play mobile games.
- He /she can use a smartphone.
In the preparation phase of the material, a graphic designer collaborates with the technicians to create the eight mini games which consist of the new SG. In addition, the trainers have to prepare pre-game materials (colourful activities based on the new SG, such as puzzles, and sequencing cards) to assist adults with ID in understanding which cognitive skills they will practise. Each game corresponds to a specific cognitive skill, such as colour recognition, memory, calculation, accuracy, logic, dexterity, multitasking, and attention to details. The questionnaire is adapted to other countries and national contexts. Following the development of the game, a one-day training programme is created for the interaction of adults with ID with the new mobile SG. During this programme, the presentation of the game and the trials of the adults with ID, are the main factors for the stage 2. The tasks of the mobile SG and the small games are:
- Colour recognition games (a. choose the correct item with the same colour, b. recognise the colour which not match, c. recognise the item, created by colored dots)
- Memory games (a. memorise a sequence of numbers, b. remember details of a picture, c. reading and memorisation of the elements)
- Calculation games (a. simple calculations, b. count the bill, c. sequences of numbers)
- Accuracy (a. anagrammatism, b. find the missing letters, c. choose the right letter to create a word)
- Logic games (a. sequencing cards, b. completing the sentences with the correct given word, c. finding the correct sentence)
- Dexterity (a. find the correct combination- word with pictures, word to synonyms, b. choose similar pictures with a timer, c. create the puzzle)
- Multitasking (a. fill the gaps, choosing the correct word, b. put the things in correct order, c. match the products from the list with their pictures)
- Attention to details (a. find the differences between two pictures, b. memorise the picture and the details, c. find the hidden items in the picture).
Stage 2: Randomised Control Trial Study
People with ID are approached to participate in the study by a health professional of the associations of the six countries that participate in the Game4CoSkills project. The health professionals participate in the RCT study as trainers of adults with ID. Adults with ID play the mobile SG twice a week, for an hour, in small groups of four to six participants, for six months. This systematic trial of the game, constitutes an intervention for the adults with ID.
Trainers explain to the adults that the game they played in the one-day programme, is the tool they have to interact with. Then, trainers give to the adults with ID the new mobile SG and explain them the activities. The guidance of the trainers is required since adults with ID have difficulties with these activities. They feel comfortable participating while the procedure is not demanding, but it presents to the adults as an alternative manner to interact and have fun. All activities are colorful and in a great size, avoiding visual difficulties to take place.
As an adaptation period, participants have fifteen minutes to explore the game. When one activity is completed, then the individual continues with the next one. The trainers, as observers, take down notes about the reaction of the adults, the time needed to complete one task (to understand the potential difficulties) and which activity is completed correctly and in which the adults fail. The trainers have an observation form, including lists of achieving, fail, times and comments (about the reaction, what the adult says). All data are transferred and collected in an electronic file on each organization’s computer to ensure the validity and immutability of the data. The records are confidential to people not involved in the study. Data collection and analysis show the first trials of the participants and how they are or not improved through the stage. The validity of the data from stage 2 can be questioned because the performance of adults may be affected by the presence of the trainers and by the unknown tasks of the activities. For this reason, adults have three times before the first trial (one per day for three days, a week before the trial) to be familiar with the trainer and the activities. The adaptation period aims to reduce any potential interruption or discomfort. This is the rationale behind not analysing the first three day’s data. The qualitative type of study in this stage gives a clear result to the trainers about participants’ level during their performance with the cognitive activities.
Participants continue to play the game twice a week for a six-month period, This RCT examines their performance and any potential improvement of their cognitive skills. After the systematic six-month trials of the SG, the follow up assessment examines the effectiveness of the game. After a week the trials conclude, a follow-up assessment is conducted. Participants are tested using the same neuropsychological tools from stage 1 to compare their initial results to the results of the RCT assessment.
Participants
The sample include (n=128) adults with ID and 60 health professionals (10 from each country, who will perform as trainers) at all stages. All participants are selected from the collaborative participating organisations. Because of their interaction with people with ID, collecting participants with ID, MCI, high functioning ASD, and DS is a simple part of the study. Trainers are informed about the study and are able to decide whether or not to participate. Training adults with ID is a well-prepared procedure and adults feel comfortable and common.
Inclusion criteria are: all of them need to (1) be adults (18 years of age or older), (2) have a diagnosis of MCI according to Petersen criteria28 or have a diagnosis of high-functioning ASD (verbal ASD) or DS with cognitive deficits (according to DSM-5)29 or have a diagnosis of mild or moderate ID according to WAIS-IV,30 (3) can walk independently, and (4) visit the project’s participating organisations with their caregivers. The diagnosis will be supported by neuropsychological assessment including a comprehensive battery of psychometric tests such as (1) Mini Mental State Examination (MMSE)31 for the assessment of general cognitive function; (2) Functional Cognitive Assessment Scale (FUCAS)32 for general functional performance, (3) American Association on Intellectual and Developmental Disabilities (AAIDD) for the assessment of ID33 and (4) Diagnostic and Statistical Manual of Mental Disorders 5th edition (DSM-5) for the assessment of high functioning ASD and DS.29 Exclusion criteria are 1) affected disorders such as severe depression or anxiety and behavioural problems such as aggressiveness and irritability that could affect the effectiveness of the intervention, (2) other neurological disorders such as epilepsy, stroke, or hydrocephalus; (3) sensory deficits, such as visual and hearing problems, (4) existence of any terminal illness, and anticholinergic drugs, (5) mental illness, (6) pharmacological treatment with cholinesterase inhibitors, antipsychotic, and anticholinergic drugs and (7) participation in other interventions. The reason behind the exclusion of mental illnesses such as anxiety and depression is that the existence of such emotional diseases lower the effectiveness of cognitive training. Inclusion criteria for trainers are: (1) must be health professionals, (2) who interact with adults with ID, MCI, ASD and DS, (3) have an extensive experience with assistive technology. As exclusion criteria for trainers are (1) no experience in assistive technology and (2) no experience in adults with ID. All participants have been given a participant information sheet and have been required to complete informed consent before collecting any measurements.
Randomisation
Using matching and randomisation, cases are divided into groups (64 adults in the intervention group and 64 adults in the control group). Randomisation can eliminate bias in participant grouping, and matching methods can diminish baseline disparities between intervention and control groups.34 For the purposes of stratified randomisation, groups of two recruited cases are matched as nearly as feasible in terms of age, gender, education and cognitive ability. The web-based RRApp randomisation technique is applied in the investigation. An information technology technician uses an algorithm to perform randomisation prior to including individuals. The key outcome measures and the study hypothesis is not disclosed to the participants, and all of the health professionals who examine the participants in the neuropsychological assessment are unaware of the participants’ group assignments. Clinical psychologists that specialise in working with adults with ID first determine the eligibility of each participant before allocating them to one of the two groups.
Intervention Group
All participants are screened for eligibility by psychologists who work with people with ID and then are assigned to one of the two groups. After the first screening with the neuropsychological assessment, a professional (health professional with experience with people with cognitive dysfunction) who has received the standardised formal training in the game starts implementing the SG. The RCT study lasts for six months. Each trial lasts approximately 60 min, and participants play the game twice a week in small groups of 4 to 6 people. Thus, they have the time to repeat activities and get familiar with. This repetition offers them exposure to the target cognitive skill beyond the two hours of weekly trials. The effectiveness of this duration for non-pharmacological interventions has been well demonstrated through research findings and the experience of implementing non pharmacological interventions in the GAADRD day care centers during the last ten years.35,36 The game is designed for people with different levels of cognitive skills. The groups use the same material. In the RCT study (1) trainers explain to the adults what the activities require and give them the time to understand the structure and the rules of the activities through practice, while (2) adults interact with the activities in a one-day training programme in stage 1.
Control Group
This cohort will receive the intervention and serves as the study’s non-intervention control group.37 Control group will participate in RCT a month after the intervention group finishes the trials. The possibility of being assigned to one intervention is briefly clarified to the potential participants. Each time point’s assessment measures will be completely completed by each participant of the control group. Hence, before and after the trials of the game, participants in both groups will receive neuropsychological assessments.
This stage, focuses on the evaluation of the SG from the adults with ID, the trainers and the caregivers of the adults with ID. Following the completion of the RCT study for the intervention group and the control group, adults with ID complete an oral questionnaire for game evaluation. The trainers, also, complete a structured questionnaire to answer if the game as an interventional tool is effective and has potential to improve the specific eight cognitive skills of the adults with ID. A third questionnaire is designed for the caregivers’ opinion about the new game, the participation of the adults with ID to the RCT and which is the impact of this interaction. It is important to be declared the opinion of the caregivers as they interact with the adults with ID, and they may notice changes in their social interaction and cognitive skills. All data are selected and analysed using statistical analysis for the results of the study.
Stage 3: Evaluation of the SG from the participants, the trainers and the caregivers of adults with ID
Ethical Considerations
All participants who will participate in the intervention need to read and sign the informed consent form which explains the purpose of the study, withdrawal from participation at any time is possible, contact details of the researcher, and permission for the staff to use their basic demographic information such as age, gender, and education, as well as their total scores of neuropsychological tests only for research reasons. This study was approved by the Scientific and Ethics Committee of GAADRD (Scientific Committee Approved Meeting Number: 74/28-1-2022) and follows the principles outlined in the Helsinki Declaration. Participants will be invited to take part in this study, and those who consent will meet with a trained facilitator who will support their engagement throughout the study prior to the beginning of the intervention.
All data arising from this study will be confidential, and the research team will be the only one who will have access to the data. Completed neuropsychological assessments and other evaluations will be marked with case numbers and held in secure filing systems. Codified numerical data from the assessments will be stored on secured systems and in SPSS files. Records will be identified by case number only, and thus participants’ names will not be stored in these electronic systems. A master list linking case numbers with participants’ names and contact details will be held in a password-protected computer file. Articles, publications in journals, presentations and other publications arising from this study will contain aggregated data so individual cases may not be identified. The produced data of this study will be included in a subsequent results publication, in line with the research ethics approval. All the data will be kept anonymous. Adults will have the possibility to ask the health professionals questions about the research before giving their consent. Study participants will be informed about their participation, and they will participate voluntarily.
Data Availability
The data sets generated during and/or analysed during the current study will be available from the corresponding author upon reasonable request.
Analysis
Power
For the sample size calculation obtained a power analysis calculator, G*power 3.1, to determine parameters, a medium effect size (d = 0.50), and an alpha of 0.05. A total sample of 128 participants with two equal-sized groups of n = 64 (intervention group and control group) is required to achieve a power of 0.80.
Data Statistical Analysis
Demographic characteristics such as age, gender and profession from the stage 1 will be analysed at baseline using a Univariate analysis (ANOVA) to find the mean of the age, gender and profession and the percentage of the participation of each category. This kind of analysis will provide information about the given answers to the questionnaires, the social status of participants, the educational level of the trainers, and specify their diagnosis. Hence, the analysis will underline the target groups which will be participating, the difficulties in daily life that participants have to face and will guide the trainers for the first game trial which will follow. The statistical analysis of the results through the stages 2 and 3 will be performed with the IBM SPSS 23.34 The scores of trials, the failure and the achievements of stage 2 will be analysed to show if there was any improvement in the first trials. The analysis will include both the individual performance of each participant in all cognitive skill activities and in groups ASD, MCI, mild and moderate ID, and DS. At stage 3 the scores of each participant will be analysed. The scores of the first game trial until the last game trial will be compared. The scores between all participants will be analysed, as the scores of each participant individually. T-tests will be used during the procedure of the comparison of the scores and will show if there is any difference.
Results
The expected outcomes of this mixed-method study are that this game for cognitive deficits in adults with ID; mild and moderate ID, MCI, ASD and DS is created and shows to have a positive impact on the improvement of eight cognitive skills after a six-month period of playing the game. Additionally, is expected that through this approach, the participants will improve their quality of life. All these cognitive skills are required for daily living and their independence in daily-life activities.
Discussion
As Assistive Technology influences our lives and interventions can benefit from this kind of technology, many SGs have been developed through the years focused on people with ID. Some SG aim to develop the educational skills of adults with ID,38 the ability to read,39 to evaluate the reaction time of adults with MCI.35 It is proved that a gesture-based SG is more effective in the rehabilitation of MCI patients.36 Unfortunately, the majority of SG tends to focus on ID and MCI and the results of these SGs show that people with ID improve their quality of life and self-esteem by feeling a part of the community,15 improving the shopping skills, calculation,26,27 problem solving, working memory and academic skills.26,27 Many cognitive skills such as visual recognition of colour, dexterity, accuracy, logic and multitasking have not been investigated, analysed, or even been a part of previous SG which have been developed. The Virtual Supermarket Cognitive Training Application activates the cognitive skills of shopping, selecting items from a market, and using a list,40 the Bridge game enhances the cognitive skills of adults with MCI and ID,15 as well as the AD-gaming,16 but as it is shown their target group is also restricted, while these games could be used and could also refer to people with SD and ASD. For DS adults the SGs which have been developed, focused on their physical education skills,41 hence, cognitive skills are not included in this game. It is important to refer that a study underlines that adults with ID were improved only in motor skills and not in cognitive functions by playing SGs and this needs further investigation referring to the systematic play of a game, the time needed and the type of the game (which skills turn to enhance during the interaction).42 It is worth referring that SG for DS mostly refers to children and not to adults and this factor generates a gap based on adults with DS and their intervention, opportunities to enhance their cognitive skills and thus, to improve their quality of life.43 Additionally, studies about SG for adults with ASD mainly focused on social interaction and emotions,44 planning and decision making and mental health.23,44,45 For example, decision-making is one important cognitive skill but it is not the main cognitive ability and the enhancement of decision-making requires the improvement of logic-critical thinking, accuracy and other abilities. The literature shows that there is no SG for the improvement of many cognitive skills of this target group.46 These target groups face many difficulties in all aspects of their life and their cognitive skills can be improved, while people get taught how to learn. Even though there are many studies about SG and ASD, approximately all of them refer to the pediatric population and not to adults.46 Adults need to learn how to learn during the specific procedure which will be generated especially for their needs, with alternative methods of educational practices and through an interactive, well-prepared and entertaining way. As well as many studies and SGs have been developed, people need well-structured SGs to the point of the interaction with other people and increasing at the same time their performance of many cognitive skills, not only for memory, problem solving or decision making but for all aspects of functional cognition.47–49 An interactive procedure will enhance the ability of an adult with SD to socialize and contact with an adult with ASD or ID and MCI. The innovation of this study and game is that will be included all these target groups since previous works focused only on one or two target groups. This game will refer to the cognitive skills of adults with ID, MCI, DS, AD and ASD, and no previous game has this potential to be played and be designed for all these target groups and specifically focused on various cognitive functions. Finally, this study focuses on various objectives not only on the development of a new SG which is a mobile SG out of charge but also on the improvement of the daily life activities of adults with ID and this achievement may get managed through this study protocol. The main strength of the study lies in the fact that the cognitive skills of adults with ID have not been investigated in previous studies. Playing the game is presented to the participants as a systematic interventional tool usage, through which they try to improve their cognitive skills. It is not yet proved that the new mobile SG improve their skills, but it gives them the motivation to interact and through this approach they have benefits in many aspects.50
Limitations
The study is conducted in the organisations of the six countries, and in some countries other materials/pictures will be used for specific words of the tasks. Additionally, this study will not examine the long-term impact of the intervention. The effectiveness of the game is not certain that will last for a long time. Thus, repetition of follow-up assessments will be necessary. Also, in some countries, the trainers will use different tests for the neuropsychological assessment which will limit the validity of the results. The authors encourage future trainers to evaluate the intervention including more follow-ups. Finally, the generalization of the study’s results should be interpreted in light of these limitations.
Conclusion
This protocol presents a mixed-methodology approach for the development of a new mobile SG with the goal of improving cognitive skills in adults with ID. All the steps which are followed in the protocol, and the participated groups are chosen to fill the literature gap. Using a mobile SG to improve eight cognitive skills of adults with ID has not been received enough attention yet. This protocol’s development and implementation are tailored to the needs of people with ID as well as the perspectives of health professionals. If the efficacy of this protocol is confirmed, group-based interventions for people with ID could become a routinely available intervention that could improve participants’ well-being by reducing cognitive difficulties and increasing social interaction. The protocol of this study will also empower a future assessment of other interventions which will use new SG as an interventional tool. It is expected the development of a new mobile SG, as an interventional tool for adults with ID, to enhance their daily living skills, cognitive skills and quality of life.
Abbreviations
ID,Intellectual Disabilities; MCI, Mild Cognitive Impairment; ASD, Autism Spectrum Disorder; DS, Down Syndrome; SG, Serious Game; AT, Assistive Technology.
Acknowledgments
This research will be carried out and funded by the Game4Coskills Erasmus+ project under Grant 2021-1-FR01-KA220-ADU-000026181. The authors would like to express their gratitude to thank the participating organisations, the participants (adults with ID), the caregivers and the trainers (health professionals) for their willingness and participation during the duration of the project.
Disclosure
The authors report no conflicts of interest in this work.
References
1. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM). Washington, DC: American Psychiatric Association; 1994:866.
2. World Health Organisation. Disorders of Intellectual Development. World Health Organisation; 2020.
3. Schalock RL, Luckasson RA, Shogren KA, et al. The renaming of mental retardation: understanding the change to the term intellectual disability. Intellect Dev Disabil. 2007;45(2):116–124. doi:10.1352/1934-9556(2007)45[116:TROMRU]2.0.CO;2
4. Schalock RL, Luckasson R. A systematic approach to subgroup classification in intellectual disability. Intellect Dev Disabil. 2015;53(5):358–366. doi:10.1352/1934-9556-53.5.358
5. Patel DR, Apple R, Kanungo S, et al. Intellectual disability: definitions, evaluation and principles of treatment. Pediatr Med. 2018;1:11. doi:10.21037/pm.2018.12.02
6. Patel DR, Greydanus DE, Merrick J, et al. Introduction to intellectual and developmental disabilities. In: Rubin IL, Merrick J, Greydanus DE, et al. editors. Health Care for People with Intellectual and Developmental Disabilities Across the Lifespan. Cham: Springer; 2016:5–12.
7. Shapiro BK, O’Neill ME. Developmental delay and intellectual disability. In: Kliegman RM, St Geme JW, Blum NJ, editors. Nelson Textbook of Pediatrics,
8. Patel DR, Cabral MD, Ho A, et al. A clinical primer on intellectual disability. Transl Pediatr. 2020;9(S1):23–35. doi:10.21037/tp.2020.02.02
9. Owuor J, Larkan F, Maclachlan M. Leaving no-one behind: using assistive technology to enhance community living for people with intellectual disability. Disabil Rehabil Assist Technol. 2017;12(5):426–428. doi:10.1080/17483107.2017.1312572
10. Hatton C, Emerson E. Introduction: health disparities, health inequity, and people with intellectual disabilities. In: International Review of Research in Developmental Disabilities. Vol. 48. Academic Press; 2015:1–9.
11. Boot FH, Louw JS, Kuo HJ, Chen R. Editorial: intellectual disability and assistive technology. Front Public Health. 2019;7:171. doi:10.3389/fpubh.2019.00171
12. Delgado P, Ávila V, Fajardo I, et al. Training young adults with intellectual disability to read critically on the internet. J Appl Res Intellect Disabil. 2019;32(3):666–677. doi:10.1111/jar.12562
13. Choi E, Shin SH, Ryu JK, et al. Commercial video games and cognitive functions: video game genres and modulating factors of cognitive enhancement. Behav Brain Funct. 2020;16(1):2. doi:10.1186/s12993-020-0165-z
14. Zygouris S, Ntovas K, Giakoumis D, et al. A preliminary study on the feasibility of using a virtual reality cognitive training application for remote detection of mild cognitive impairment. J Alzheimers Dis. 2017;56(2):619–627. doi:10.3233/JAD-160518
15. Makri M, Tsolaki M Innovative Serious Games for People with Dementia developed through intergenerational interventions. The “Bridge” project: a European Innovative Approach. In
16. Makri M, Tsolaki M, Zygouris S. Development of the training platform “AD-GAMING” for the improvement of quality of life of people with dementia through “serious games”. J Fam Med. 2020;7:1207.
17. Lin YF, Liu MF, Ho MH, et al. A pilot study of interactive-video games in people with mild cognitive impairment. Int J Environ Res Public Health. 2022;19(6):3536. doi:10.3390/ijerph19063536
18. Shalash WM, AlTamimi S, Abdu E, et al. No Limit: a down syndrome children educational game. In
19. Bediou B, Adams DM, Mayer RE, et al. Meta-analysis of action video game impact on perceptual, attentional, and cognitive skills. Psychol Bull. 2018;144(1):77–110. doi:10.1037/bul0000130
20. Suárez-Iglesias D, Martínez-de-Quel Ó, Marín Moldes JR, et al. Effects of videogaming on the physical, mental health, and cognitive function of people with intellectual disability: a systematic review of randomized controlled trials. Games Health J. 2021;10(5):295–313. doi:10.1089/g4h.2020.0138
21. Torra MM, Canals SJ, Colomina FMT. Behavioral and cognitive interventions with digital devices in subjects with intellectual disability: a systematic review. Front Psychiatry. 2021;12:647.
22. Standen P, Rees F, Brown D. Effect of playing computer games on decision making in people with intellectual disabilities. J Assist Technol. 2009;3:4–12.
23. Tsikinas S, Xinogalos S. Towards a serious games design framework for people with intellectual disability or autism spectrum disorder. Educ Inf Technol. 2020;25(4):3405–3423. doi:10.1007/s10639-020-10124-4
24. Pashapoor L, Kashani-Vahid L, Hakimirad E Effectiveness of cognitive computer games on attention Span of students with intellectual disability,
25. Stančin K, Hoić-božić N, Skočić Mihić S. Using digital game-based learning for students with intellectual disabilities. a systematic literature review. Informa Educ. 2020;19:323–341. doi:10.15388/infedu.2020.15
26. Shabalina O, Guriev V, Kosyakov S, et al. Adaptable mobile software for supporting daily activities of people with intellectual disabilities. In: Kravets A, Groumpos P, Shcherbakov M, Kultsova M, editors. Creativity in Intelligent Technologies and Data Science. CIT&DS 2019. Communications in Computer and Information Science. Cham: Springer; 2019:1084.
27. Gjermestad A, Luteberget L, Midjo T, et al. Everyday life of persons with intellectual disability living in residential settings: a systematic review of qualitative studies. Disabil Soc. 2017;32(2):213–232. doi:10.1080/09687599.2017.1284649
28. Petersen RC, Morris JC. Mild cognitive impairment as a clinical entity and treatment target. Arch Neurol. 2004;62(7):1160–1163. doi:10.1001/archneur.62.7.1160
29. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders.
30. Erdodi LA, Abeare CA, Lichtenstein JD, et al. Wechsler Adult Intelligence Scale-Fourth Edition (WAIS-IV) processing speed scores as measures of noncredible responding: the third generation of embedded performance validity indicators. Psychol Assess. 2017;29(2):148–157. doi:10.1037/pas0000319
31. Folstein MF, Folstein SE, McHugh PR. ”Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12(3):189–198. doi:10.1016/0022-3956(75)90026-6
32. Kounti F, Tsolaki M, Kiosseoglou G. Functional cognitive assessment scale (FUCAS): a new scale to assess executive cognitive function in daily life activities in patients with dementia and mild cognitive impairment. Hum Psychopharmacol. 2006;21(5):305–311. doi:10.1002/hup.772
33. Harris AD, McGregor JC, Perencevich EN, et al. The use and interpretation of quasi-experimental studies in medical informatics. J Am Med Inform Assoc. 2006;13(1):16–23. doi:10.1197/jamia.M1749
34. IBM Corp. IBM SPSS Statistics for Windows, Version 23.0.2015. Armonk, NY: IBM Corp; 2013.
35. Chen YT, Hou CJ, Derek N, et al. Evaluation of the reaction time and accuracy rate in normal subjects, MCI, and dementia using serious games. Appl Sci. 2021;11(2):628. doi:10.3390/app11020628
36. Lau SYJ, Agius H. A framework and immersive serious game for mild cognitive impairment. Multimed Tools Appl. 2021;80(20):31183–31237. doi:10.1007/s11042-021-11042-4
37. Bernard HR. Research Methods in Anthropology: Qualitative and Quantitative Approaches.
38. Torrent J, Del Blanco A, Moreno-Ger P. Designing Serious Games for Adults Students with Cognitive Disabilities. In: Huang T, Zeng Z, Li C, Leung CS, editors. Neural Information Processing. ICONIP 2012. Lecture Notes in Computer Science. Berlin, Heidelberg: Springer; 2012.
39. Politis Y, Robb N, Yakkundi A, et al. People with disabilities leading the design of serious games and virtual worlds. Int J Serious Games. 2017;4(2):63–73. doi:10.17083/ijsg.v4i2.160
40. Zygouris S, Giakoumis D, Votis K, et al. Can a virtual reality cognitive training application fulfill a dual role? Using the virtual supermarket cognitive training application as a screening tool for mild cognitive impairment. J Alzheimers Dis. 2015;44:1333–1347.
41. Farías-Valenzuela C, Cofré-Bolados C, Ferrari G, et al. Effects of motor-games-based concurrent training program on body composition indicators of chilean adults with down syndrome. Sustainability. 2021;13(10):5737. doi:10.3390/su13105737
42. Perrot A, Maillot P, Le Foulon A, et al. Effect of exergaming on physical fitness, functional mobility, and cognitive functioning in adults with down syndrome. Am J Intellect Dev Disabil. 2021;126(1):34–44. doi:10.1352/1944-7558-126.1.34
43. Ritterfeld U, Weber R. Video games for entertainment and education. In: Playing Video Games. Lawrence Erlbaum Associates Publishers; 2006:399–413.
44. Grossard C, Grynspan O, Serret S, Jouen A-L, Bailly K, Cohen D. Serious games to teach social interactions and emotions to individuals with autism spectrum disorders (ASD). Comput Educ. 2017;113:195–211. doi:10.1016/j.compedu.2017.05.002
45. Lau HM, Smit JH, Fleming TM, et al. Serious games for mental health: are they accessible, feasible, and effective? A systematic review and meta-analysis. Front Psychiatry. 2017;7:209. doi:10.3389/fpsyt.2016.00209
46. Vallefuoco E, Bravaccio C, Gison G, et al. Personalized training via serious game to improve daily living skills in pediatric patients with autism spectrum disorder. IEEE J Biomed Health Inform. 2022;26(7):3312–3322. doi:10.1109/JBHI.2022.3155367
47. Lonner WG, Berry JW. Field Notes in Cross-Cultural Research. Newbury Park.CA: Sage Publications; 1986.
48. Sokolov AA, Collignon A, Bieler-Aeschlimann M. Serious video games and virtual reality for prevention and neurorehabilitation of cognitive decline because of aging and neurodegeneration. Curr Opin Neurol. 2020;33(2):239–248. doi:10.1097/WCO.0000000000000791
49. Erlingsson C, Brysiewicz P. (2017) A hands-on guide to doing content analysis. Afr J Emerg Med. 2017;7(3):93–99. doi:10.1016/j.afjem.2017.08.001
50. Bengtsson M. How to plan and perform a qualitative study using content analysis. NursingPlus Open. 2016;2:8–14. doi:10.1016/j.npls.2016.01.001
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.