")
Back to Journals » Cancer Management and Research » Volume 11
A prospective study on urine alkalization with an oral regimen consisting of sodium bicarbonate and acetazolamide in patients receiving high-dose methotrexate
Authors Reed DR, Pierce EJ, Sen JM , Keng MK
Received 13 May 2019
Accepted for publication 9 August 2019
Published 30 August 2019 Volume 2019:11 Pages 8065—8072
DOI https://doi.org/10.2147/CMAR.S190084
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Bilikere Dwarakanath
Daniel R Reed,1 Eric J Pierce,2 Jeremy M Sen,3 Michael K Keng1
1Division of Hematology/Oncology, Department of Medicine, University of Virginia, Charlottesville, VA, USA; 2Department of Medicine, University of Virginia, Charlottesville, VA, USA; 3Department of Pharmacy Services, University of Virginia, Charlottesville, VA, USA
Correspondence: Michael K Keng
University of Virginia, Department of Medicine, Division of Hematology/Oncology, 1300 Jefferson Park Avenue, West Complex, Room 6009, Charlottesville, VA 22908, USA
Tel +1 434 924 4257
Fax +1 434 244 7534
Email [email protected]
Purpose: Intravenous (IV) sodium bicarbonate is typically used in alkalization regimens for the safe use of the chemotherapeutic agent high-dose methotrexate (HDMTX). Urine parameters including urine output and pH are important in order to minimize the risk of kidney injury, which increases adverse effects and hospital length of stay following HDMTX. IV sodium bicarbonate has been on shortage, and there are limited literature describing the safety of alternative regimens.
Patients and methods: A single institution, prospective analysis of non-Hodgkin’s lymphoma and acute lymphoblastic leukemia patients receiving HDMTX for central nervous system (CNS) prophylaxis or disease. Patients received an oral (PO) regimen of sodium bicarbonate and acetazolamide to achieve a urine pH >7. This cohort was compared to a subsequent IV sodium bicarbonate control cohort. Multiple co-primary safety outcomes assessed the incidences of acute kidney injury and delayed methotrexate clearance as well as change in liver function tests. Secondary outcomes included time to urine pH, time to urine output, and length of stay.
Results: A total of 126 encounters were studied for the primary safety outcome. There was no difference between AKI incidence in patients receiving the PO alkalization regimen compared to patients receiving IV sodium bicarbonate (14.5% vs 9.3%, respectively, P=0.41). There was no difference in methotrexate clearance between the PO and IV groups (26.5% vs 37.2%, respectively, P=0.21). The use of PO alkalization regimen is estimated to have saved 2002 vials of IV sodium bicarbonate and was approximately US$226 less expensive per encounter.
Conclusion: This analysis supports the use of PO regimens to achieve urine alkalization necessary for safe administration of HDMTX during periods of IV sodium bicarbonate shortage. Further studies may determine optimal dosing strategies that decrease length of stay and ensure noninferiority of efficacy outcomes with PO regimens for urine alkalization with HDMTX.
Keywords: non-Hodgkin’s lymphoma, acute lymphoblastic leukemia, oral alkalization, alkalization, high-dose methotrexate, chemotherapy administration
Introduction
High-dose methotrexate (HDMTX) is a chemotherapeutic agent used in the treatment and prevention of central nervous system (CNS) disease for lymphoma, leukemia, and other malignancies like sarcoma. Methotrexate (MTX) is a competitive inhibitor of the enzyme dihydrofolate reductase that interrupts DNA biosynthesis. Because of poor penetration of the blood–brain barrier, HDMTX is administered to adequately penetrate cerebrospinal fluid (CSF) and parenchyma. HDMTX is typically given at doses 1–12 grams per square meter of body-surface area (g/m2).1
Following intravenous MTX administration, 90–95% is excreted unchanged by the kidneys.2 Therefore, acute kidney injury (AKI) after administration of HDMTX, is a medical emergency since prolonged MTX exposure leads to severe cytopenias, mucositis, febrile neutropenia, and liver toxicity. Previous studies have shown the rate of AKI to be 2–12%.3 MTX is poorly soluble at pH less than 7, and an acidic environment within the renal tubules may result in increased risk of MTX precipitation and AKI.2,4 Urine alkalization and hyperhydration with adjustment based upon serial monitoring of urine pH and output are cornerstones in the prevention of nephrotoxicity following HDMTX. In addition, avoidance of medications that interact with MTX clearance or plasma protein-binding, monitoring of serum creatinine (SCr) and MTX concentrations, and utilizing pharmacokinetic-guided leucovorin rescue per treatment protocols are necessary for safe administration.3 Implementation of supportive measures and monitoring, the incidence of life-threatening toxicity has decreased from approximately 10% to less than 1%.5
Hospitalization is warranted prior to and following administration of HDMTX due to the intensity of monitoring required. At the University of Virginia Medical Center, intravenous (IV) sodium bicarbonate has historically been utilized to achieve a goal urine pH of at least 7 and hyperhydration with a goal urine output of at least 125 mL/hr (over a 4-hr period) is required before and after administration of HDMTX.
In May 2017, IV sodium bicarbonate was on national shortage, which led our institution’s Pharmacy and Therapeutics Committee to implement restrictions based upon indication.6 At the time of the shortage, there were limited published data on the use of PO regimens to achieve urine alkalization in patients receiving HDMTX. Rouch et al detailed the safety and feasibility of utilizing PO sodium bicarbonate tablets and sodium citrate/citric acid suspension but did not define a standard dose.7 Shamash et al utilized an acetazolamide monotherapy regimen; however, there were concerns at our institution that prolonged carbonic anhydrase inhibition may lead to metabolic acidosis, the eventual inability to concentrate bicarbonate ions in the urine, and potentially, AKI. Therefore, an approach combining PO sodium bicarbonate and acetazolamide was conceived to prevent development of metabolic acidosis and to ensure consistent achievement of goal urine alkalization.8 This study aims to determine the safety and tolerability of this PO regimen for urine alkalization in patients receiving HDMTX.
Methods
A single institution, prospective cohort study was designed to evaluate patients admitted to a tertiary academic center receiving either IV or PO alkalization for administration of HDMTX during the period of May 2017 to March 2018. According to the Declaration of Helsinki, this study was approved by the Institutional Review Board for Health Sciences Research at the University of Virginia Health System. This study was deemed as quality improvement research. The University of Virginia Health System Institutional Review Board approved this study to be filed as Exempt Determination, which does not require written consent. Two cohorts were a part of this study: patient encounters initiated on PO alkalization observed from May 2017 to October 2017 and a control group of encounters who received IV alkalization from November 2017 to March 2018. All medications were obtained from a commercial wholesaler. The initial IV sodium bicarbonate and PO sodium bicarbonate plus acetazolamide regimens for urine alkalization are detailed in Table 1. In addition, encounters in both the PO and IV alkalization cohorts could receive up to 50 mEq of IV sodium bicarbonate admixed with the MTX infusion bag, which is standard practice for 2-hr infusion protocols at our institution. After starting alkalization, regimens could be modified as necessary to achieve urine pH or output goals—including starting IV sodium bicarbonate continuous infusion in the patients originated on the PO regimen—based upon the clinical judgment of the treating physician. No patient received oral alkalization prior to admission as this is not a standard practice at the University of Virginia.
 |
Table 1 Urine alkalization regimens used at the University of Virginia Medical Center |
Inclusion criteria consisted of patients ≥18 years of age scheduled to receive HDMTX for hematologic malignancies. HDMTX was administered as 2.8–3.5 g/m2 over 2 hrs for the treatment or prophylaxis of CNS disease for non-Hodgkin’s lymphoma, including primary CNS lymphoma. Patients with acute lymphoblastic leukemia were treated on HDMTX regimens administered over 24 hrs based upon either Hyper-CVAD (1 g/m2) or Children’s Oncology Group study AALL0232 (5 g/m2).9,10 Patients who received HDMTX doses greater than 5 g/m2 were excluded from this analysis.
Data including patient demographics, treatment regimens, lab values, and safety parameters were collected through review of the electronic medical record. Co-primary outcomes assessing safety included incidence of AKI, incidence of decreased MTX clearance, and change in the liver function tests aspartate aminotransferase (AST), alanine aminotransferase (ALT), and total bilirubin; these were assessed from the time of HDMTX infusion until hospital discharge. AKI was defined according to criteria defined by the Kidney Disease Improving Global Outcomes (KIDGO) practice guidelines.11 Creatinine clearance was also calculated by the Cockcroft–Gault formula utilizing actual body weight.12 A case of delayed MTX clearance was defined by failure to meet any protocol-specific goal for MTX plasma concentrations (Table S1). The secondary outcomes included length of hospital stay and time from hospital admission to initiation of MTX infusion, to meeting urine pH goal of 7, and to meeting urine output goal of greater than or equal to 125 mL/hr. All laboratory procedures were performed with commercial instruments in the core inpatient laboratory or FDA approved point-of-care medical devices on the oncology unit. Total quantity of IV and PO sodium bicarbonate and PO acetazolamide were also collected. Finally, a cost analysis was completed to determine if there were any financial consequences to using the PO alkalization regimen. For each medication, the lower end of the Average Wholesale Price range as published by Medi-Span was used to estimate costs associated with each regimen (Table S3).13
The statistical analysis made unadjusted comparisons of PO and IV alkalization using Student’s t-test for continuous variables and chi-square analysis for categorical variables. Statistical significance was defined at a two-sided alpha at 0.05. Descriptive statistics were done for continuous variables. All analyses used SPSS Statistics, version 22.0.0.0.
Results
Overall, 56 patients and 162 encounters were analyzed for inclusion. On average, patients had around three encounters for the treatment regimen. Twelve encounters were excluded due to receipt of HDMTX greater than 5 g/m2, and 24 encounters were excluded for receiving a planned, initial urine alkalization regimen that combined both PO sodium bicarbonate tablets and IV sodium bicarbonate as continuous infusion. Twenty patients were identified to meet inclusion criteria in the IV alkalization group and 28 patients met inclusion criteria in the oral alkalization group. One hundred twenty-six patient encounters were included in the study: 83 patient encounters in the PO alkalization and 43 patient encounters in the IV sodium bicarbonate cohorts. The PO alkalization encounters were older although not statistically significant than the IV cohort with a median age of 55 years (range 21–77) and 52 years (range 21–74), respectively (P=0.90). Patient cases from encounters utilizing the PO alkalization regimen had similar median weight compared to the IV alkalization group. Baseline characteristics of the two cohorts are described in Tables 2 and 3.
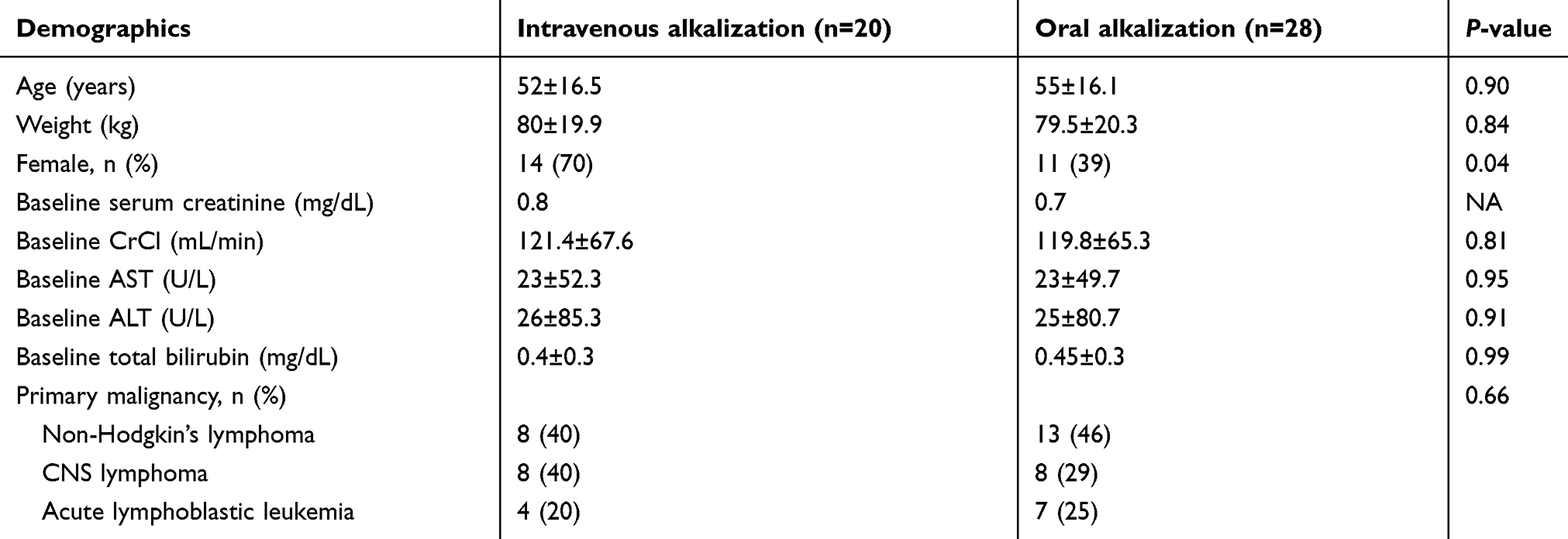 |
Table 2 Baseline demographics for high-dose methotrexate encounters |
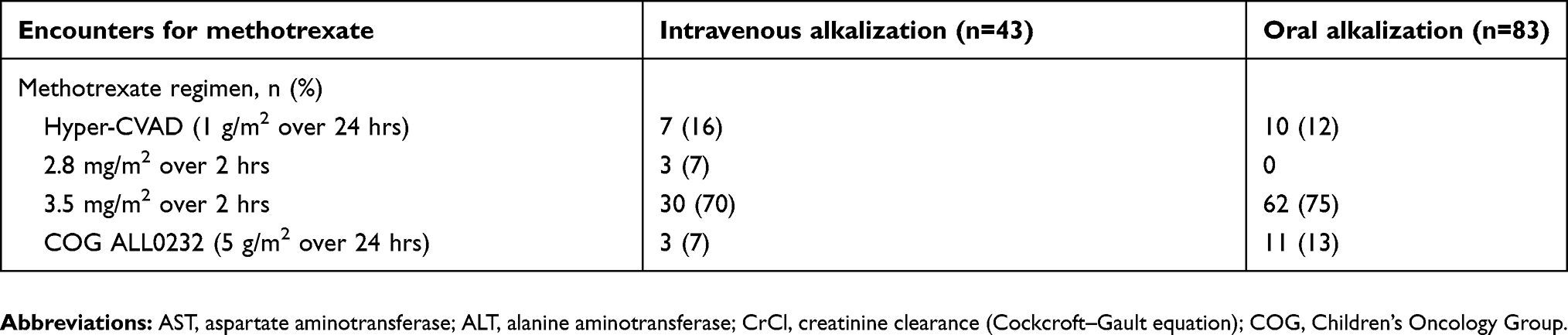 |
Table 3 Patient encounters analyzed |
In the safety analysis, there was a non-statistically significant trend toward higher AKI incidence with the PO regimen (14.5% vs 9.3%, P=0.41). However, there was no difference in the incidence of delayed methotrexate (26.5% for PO vs 37.2% for IV, P=0.21) or absolute change in AST, ALT, or total bilirubin (Table 4).
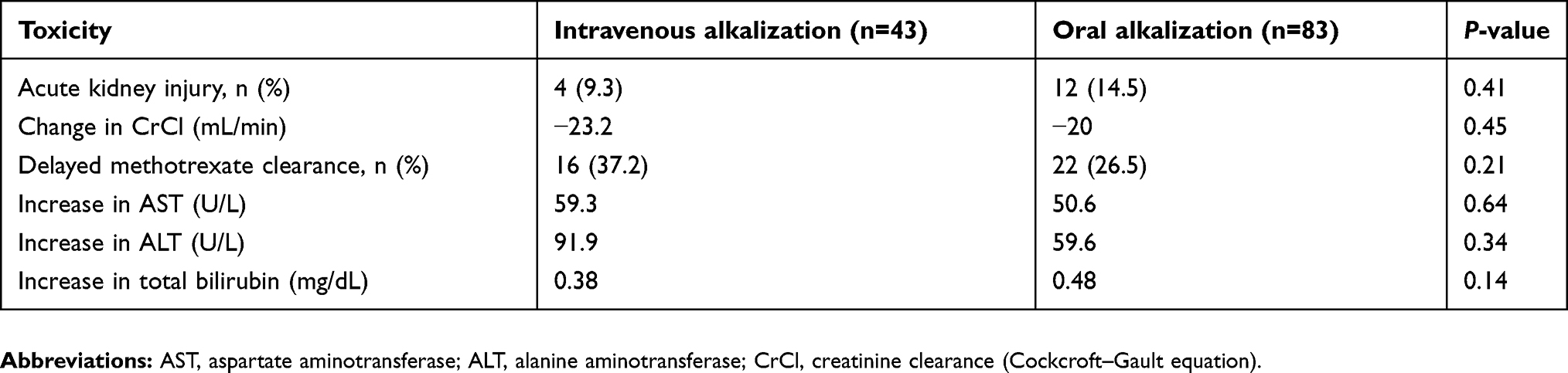 |
Table 4 Safety outcomes of the intravenous and oral regimens used for urine alkalization in patients receiving high-dose methotrexate |
In order to consistently calculate time to HDMTX (as the first chemotherapy received), time to urine output >125 mL/hr, time to urine pH >7, and hospital length of stay, a subset of patient encounters (n=66) were analyzed. These encounters were scheduled admissions with the plan to initiate HDMTX—as a single agent or as the first in a multi-agent chemotherapy regimen—immediately upon achievement of urine output and pH parameters. Unplanned HDMTX encounters for new or progressive disease or those with plans to start HDMTX later in the admission following other chemotherapy were excluded from these time-sensitive assessments. Results of these analyses are summarized in Table 5. Time to MTX was not statistically significant between alkalization regimens (7.9 hrs for PO vs 8.0 hrs for IV, P=0.6). Time to urinary output goal of 125 mL/hr was markedly reduced, but without statistical significance, with PO alkalization (5.9 hrs vs 9.2 hrs, P=0.1). Length of stay was also not statistically different; however, it was longer in encounters utilizing PO alkalization (3.8 days vs 3.1 days, P=0.3).
 |
Table 5 Secondary outcomes of the intravenous and oral regimens used for urine alkalization in patients receiving high-dose methotrexate |
The IV regimen for urine alkalization was associated with an average of 25.8 vials of 50-mEq IV sodium bicarbonate per HDMTX encounter, while the PO regimen utilized 90.7 sodium bicarbonate tablets, 13.8 acetazolamide tablets, and 1.6 vials of IV sodium bicarbonate per case. For the 83 patients administered the PO regimen, it is estimated 2002 vials of IV sodium bicarbonate were saved during the shortage. Furthermore, the PO regimen was approximately US$226 less expensive per HDMTX encounter ($57.87 vs $283.44). The estimated cost savings for all 83 patients in the PO cohort were $18,722. These data are described in Tables S2 and S3.
Discussion
National drug shortages are a common occurrence with a multitude of causes, which include manufacturing difficulties related to sterile injectables, shortage of raw ingredients, delays due to the production of multiple different therapeutic agents on the same supply line, inability of competing manufacturers to quickly increase output in response to production delay or discontinuation by another manufacturer, and lack of excess inventory throughout a complex distribution network.14 Given the several recent occurrences of IV sodium bicarbonate shortages, strategies to allow for the safe administration of HDMTX is imperative for the treatment of patients with hematologic malignancies. There have been limited attempts at modifying IV sodium bicarbonate regimens with PO substitutes or other alternatives outlined in Table 6. This study demonstrates that a PO alkalization regimen with PO sodium bicarbonate and PO acetazolamide is feasible and reduces the cost of treatment medications, albeit with increased pill burden. PO alkalization regimens in literature were limited at the time of the national shortage. Roy et al recently published another institution’s protocol for PO alkalization in the time of the national shortage.15 Their HDMTX “shortage” protocol included PO sodium bicarbonate at 3250 mg every 2 hrs in addition to PO or IV acetazolamide 250–500 mg every 6 hrs as needed. There were no statistically significant differences in MTX clearance, hospital length of stay, AKI, or hepatotoxicity. However, there was increased time of urine pH <7 and significant increase in length of stay. Shamash et al used monotherapy acetazolamide to keep patients’ urine alkalized and found no increase in AKI or difficulties with MTX clearance.8 The study demonstrated that if acetazolamide is used as single agent greater than 48 hrs, adverse effects occur. When used alone, prolonged carbonic anhydrase inhibition with acetazolamide results in depletion of the bicarbonate-carbon dioxide buffer in blood and could eventually lead to loss of urine alkalization followed by worsening MTX crystallization in the kidney tubules. Roy et al investigated an PO alkalization regimen similar to ours with sodium bicarbonate and PO acetazolamide; however, they used higher doses and more frequent PO sodium bicarbonate and reserved acetazolamide for use as needed when urine pH was <7.5.15
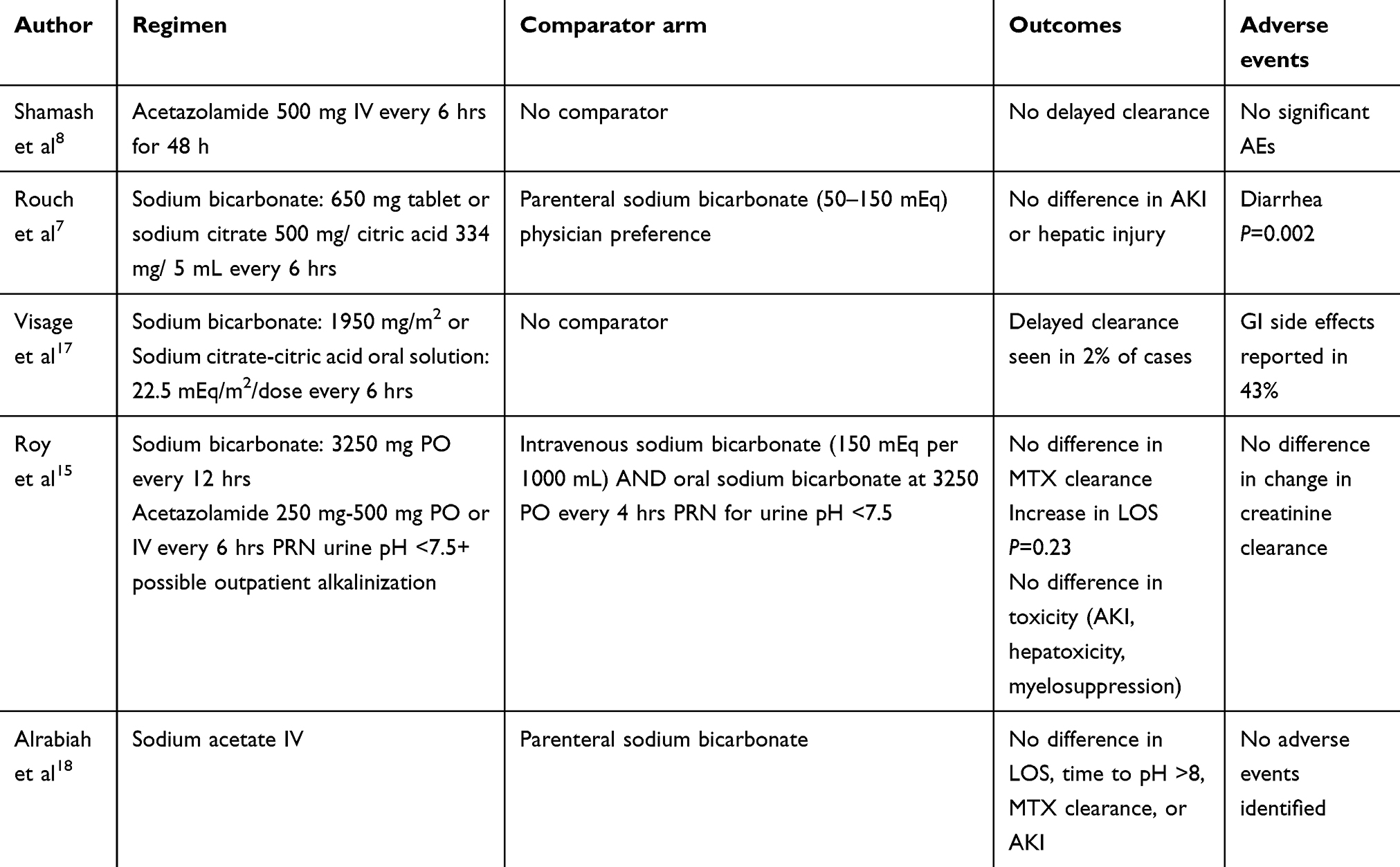 |
Table 6 Overview of previously published alternative regimens to intravenous sodium bicarbonate for urine alkalization |
We demonstrated in our study no significant difference in MTX clearance rate, which is similar to previous studies using PO sodium bicarbonate.7 There are several limitations to this study. HDMTX at doses exceeding 5 g/m2 were excluded because there were too few treatment courses at this dose that utilized the PO regimen for urine alkalization. The analysis was done in a prospective design; however, it was not a randomized controlled trial and was not analyzed with case match controls. We did not establish and incidence of mucositis or other potential toxicities due to inconsistent reporting in the EMR. However, there were no re-admissions for mucositis toxicity from HDMTX administration. In addition, cytopenias were difficult to assess in the setting of patients getting multi-agent chemotherapy for most regimens with ALL and CNS lymphoma. Cytopenias that occur were likely due to the combination effect of chemotherapy, rather than HDMTX. There was no documented evidence of MTX-induced rash or pneumonitis. No patients received glucarpidase or dialysis for the treatment of delayed methotrexate clearance and AKI.
Our studied intervention of PO sodium bicarbonate and acetazolamide was a well-tolerated. Compared to previously published PO treatment regimens, this study had a smaller sodium bicarbonate pill burden. The protocol was designed to accommodate patient sleep schedule and reduce wake times for pill administration. Finally, this is the first study of a PO regimen for urine alkalization to include a cost analysis, which demonstrated the PO regimen to be associated with potential significant savings if implemented in a large patient population.
Conclusion
Despite IV bicarbonate shortages, HDMTX can be administered safely with the implementation of several PO alkalization regimens for urinary alkalization. Our analysis is the largest prospective look at a PO alkalization method. While it has been attempted to decrease time to MTX administration, time to urine parameters, and ultimately length of stay, PO regimens do not appear to impact these objectives unless the oral alkalization regimen has been started prior to admission.16 Further prospective trials should be undertaken to establish the safety and efficacy of alternative PO alkalization regimens.
Disclosure
Preliminary data for this manuscript have been published online in the abstract only format (https://ascopubs.org/doi/abs/10.1200/JCO.2018.36.15_suppl.e18804). Dr Michael Keng is a member for the Advisory Board for Agios, outside the submitted work.The authors report no other conflicts of interest in this work.
References
1. Jolivet J, Cowan KH, Curt GA, Clendeninn NJ, Chabner BA. The pharmacology and clinical use of methotrexate. N Engl J Med. 1983;309(18):1094–1104. doi:10.1056/NEJM198311033091805
2. Bleyer WA. The clinical pharmacology of methotrexate: new applications of an old drug. Cancer. 1978;41(1):36–51. doi:10.1002/1097-0142(197801)41:1<36::aid-cncr2820410108>3.0.co;2-i
3. Widemann BC, Adamson PC. Understanding and managing methotrexate nephrotoxicity. Oncologist. 2006;11(6):694–703. doi:10.1634/theoncologist.11-6-694
4. Drost SA, Wentzell JR, Giguere P, et al. Outcomes associated with reducing the urine alkalinization threshold in patients receiving high-dose methotrexate. Pharmacotherapy. 2017;37(6):684–691. doi:10.1002/phar.1935
5. Howard SC, McCormick J, Pui CH, Buddington RK, Harvey RD. Preventing and managing toxicities of high-dose methotrexate. Oncologist. 2016;21(12):1471–1482. doi:10.1634/theoncologist.2015-0164
6. Thompson CA. Sodium bicarbonate shortage found to affect hospitals’ daily operations. Am J Heal Pharm. 2017;74(16):1208–1210. doi:10.2146/news170051
7. Rouch JA, Burton B, Dabb A, et al. Comparison of enteral and parenteral methods of urine alkalinization in patients receiving high-dose methotrexate. J Oncol Pharm Pract. 2017;23(1):3–9. doi:10.1177/1078155215610914
8. Shamash J, Earl H, Souhami R. Acetazolamide for alkalinisation of urine in patients receiving high-dose methotrexate. Cancer Chemother Pharmacol. 1991;28(2):150–151.
9. Thomas DA, O’Brien S, Faderl S, et al. Chemoimmunotherapy with a modified hyper-CVAD and rituximab regimen improves outcome in de novo Philadelphia chromosome-negative precursor B-lineage acute lymphoblastic leukemia. J Clin Oncol. 2010;28(24):3880–3889. doi:10.1200/JCO.2009.26.9456
10. Borowitz MJ, Wood BL, Devidas M, et al. Prognostic significance of minimal residual disease in high risk B-ALL: a report from Children’s Oncology Group study AALL0232. Blood. 2015;126(8):964–971. doi:10.1182/blood-2015-03-633685
11. Khwaja A. KDIGO clinical practice guidelines for acute kidney injury. Nephron Clin Pract. 2012;120(4):c179–84. doi:10.1159/000339789
12. Cockcroft DW, Gault MH. Prediction of creatinine clearance from serum creatinine. Nephron. 1976;16(1):31–41. doi:10.1159/000180580
13. Lexicomp Online. Hudson, Ohio: Wolters Kluwer Clinical Drug Information, Inc; Published 2019. Available from: http://online.lexi.com.
14. Fox ER, Sweet BV, Jensen V. Drug shortages: a complex health care crisis. Mayo Clin Proc. 2014;89(3):361–373. doi:10.1016/j.mayocp.2013.11.014
15. Roy AM, Lei M, Lou U. Safety and efficacy of a urine alkalinization protocol developed for high-dose methotrexate patients during intravenous bicarbonate shortage. J Oncol Pharm Pract. 2019;1078155218821406. doi:10.1177/1078155218821406
16. Kintzel PE, Campbell AD, Yost KJ, et al. Reduced time for urinary alkalinization before high-dose methotrexate with preadmission oral bicarbonate. J Oncol Pharm Pract. 2012;18(2):239–244. doi:10.1177/1078155211426913
17. Visage R, Kaiser N, Williams M, Kim A. Oral methods of urinary alkalinization for high-dose methotrexate administration: alternatives to intravenous sodium bicarbonate during a critical drug shortage. J Pediatr Hematol Oncol. 2018. doi:10.1097/MPH.0000000000001348
18. Alrabiah Z, Luter D, Proctor A, Bates JS. Substitution of sodium acetate for sodium bicarbonate for urine alkalinization in high-dose methotrexate therapy. Am J Health Syst Pharm. 2015;72(22):1932–1934. doi:10.2146/ajhp150407
Supplementary materials
 |
Table S1 Delayed methotrexate clearance definitions for each regimen. Cases failing to achieve a protocol-specific plasma concentration goal at any single time point were defined as having delayed clearance |
 |
Table S2 Medication utilization analysis for the intravenous and oral regimens used for urine alkalization in patients receiving high-dose methotrexate |
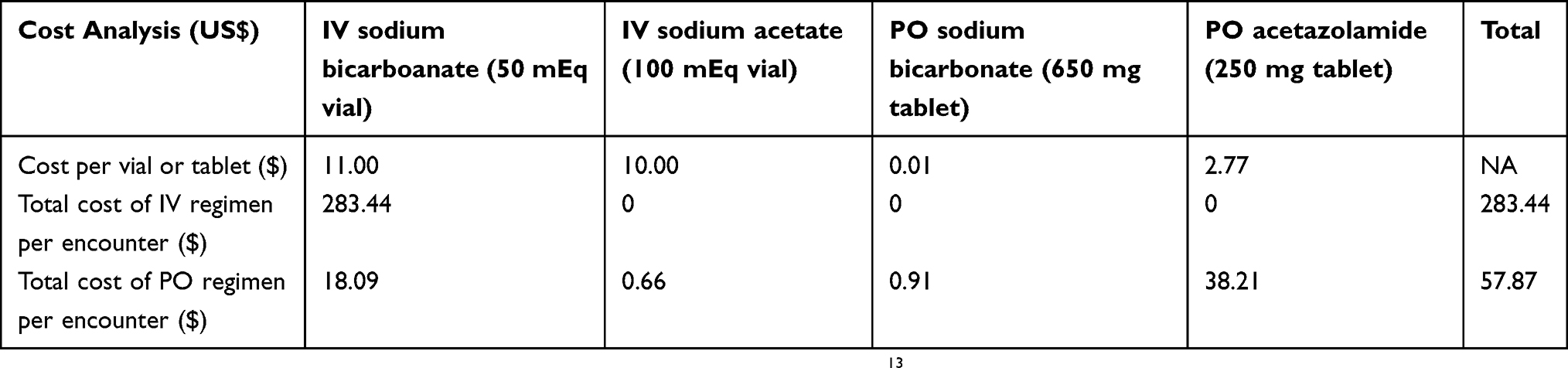 |
Table S3 Cost analysis for the intravenous and oral regimens used for urine alkalization in patients receiving high-dose methotrexate |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.