Back to Journals » Blood and Lymphatic Cancer: Targets and Therapy » Volume 12
A Promising Future for Precision Epigenetic Therapy for Follicular and Diffuse Large B-Cell Lymphoma?
Authors Chung C ![]()
Received 4 April 2022
Accepted for publication 28 July 2022
Published 4 August 2022 Volume 2022:12 Pages 99—106
DOI https://doi.org/10.2147/BLCTT.S282247
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Wilson Gonsalves
Clement Chung
Department of Pharmacy, Houston Methodist West Hospital, Houston, TX, USA
Correspondence: Clement Chung, Houston Methodist West Hospital, 18500 Katy Freeway, Houston, TX, 77094, USA, Tel +1-832-522-1051, Email [email protected]
Abstract: Epigenetic mechanisms such as DNA hypermethylation or histone deacetylation normally silence gene expression that regulates numerous cellular activities. Germinal center–derived lymphomas such as follicular lymphoma (FL) and diffuse large B cell lymphoma (DLBCL) are characterized by frequent mutations of histone-modifying genes. EZH2 is essential to the formation of germinal center in the secondary lymphoid tissue (eg, lymph nodes and spleen) and is one of the most frequently mutated histone-modifying genes in human lymphomas. EZH2 encodes a histone methyltransferase, mediates transcriptional repression and acts as an oncogene that promotes the development and progression of a variety of human malignancies, including FL and DLBCL. Thus, recurrent mutations in the EZH2 and other non-histone epigenetic regulators represent important targets for therapeutic interventions. Recently, an orally active inhibitor of EZH2, tazemetostat, has received regulatory approval for patients with mutated EZH2 relapsed or refractory FL after ≥ 2 prior systemic therapies. It is also approved for those with relapsed or refractory FL who have no satisfactory alternative treatment options, regardless of their mutational status of EZH2. Currently, tazemetostat and its combination therapies for patients with relapsed or refractory germinal center-derived lymphomas, as well as frontline therapies for previously untreated patients, are in various phases of clinical investigations. Despite the promise of epigenetic therapies, potential pitfalls such as target selectivity, risk of oncogenic activation, risk of secondary malignancies associated with epigenetic therapies must be carefully monitored. Future applications of epigenetic approach that incorporate clinical and genomic features are needed to determine how individualized treatments can be used for these hematologic malignancies.
Keywords: DLBCL, diffuse large B cell lymphoma, epigenetics, EZH2, follicular lymphoma, tazemetostat
Introduction
Lymphomas are a diverse group of hematologic malignancies that arise from T cells, B cells, or the natural killer cell lineage. The 2017 World Health Organization (WHO) classification for lymphoid neoplasms comprises more than 80 entities of mature lymphoid neoplasms (B-cell, T-cell, and Hodgkin lymphomas) which are defined according to their morphology, immunophenotype, genetic lesions, molecular profiles, clinical features, and cellular derivation.1 This classification also recognizes both incipient and indolent lymphoid neoplasms with a low potential of progression.1
Follicular lymphoma (FL) is the most common subtype of indolent non-Hodgkin lymphoma (NHL) arising from the germinal center in secondary lymphoid tissue (eg, lymph nodes, spleen). It is characterized by a distinct histology in which malignant mature B cells form follicle-like structures with non-malignant immune cells infiltrating within the follicular and interfollicular regions.2 FL cells share identical immunoglobulin (Ig) gene rearrangements, indicating that the transforming founder mutations occur after VDJ recombination, a process that allows the expression of IgM in pre-B cells.3 FL is graded by the proportion of centroblasts in the lymphoid follicle. The grades of FL were thought to reflect the multi-step of tumor progression.4 Grade 3B is often BCL-2 negative and is histologically similar to DLBCL.4,5 In general, the clinical course of grade 3B FL is more similar to that of diffuse large B cell lymphoma (DLBCL) than that of grade 1 or 2 FL. Although it is clinically important to differentiate grades 1 or 2 vs grade 3 FL, grading of FL does not provide a clear prognostic impact.2 Grade 3B often coexists with DLBCL at initial diagnosis, whereas grades 1, 2 and 3A FL are relatively indolent and transform to DLBCL at later stage, suggesting a different pathway of molecular transformation and progression in these distinct types of FL.5,6
About 85% of the FL cases show t(14;18) (q32;q21), which leads to an overexpression of BCL-2, which inhibits apoptosis of affected B cells.3,7 However, expression of BCL-2 alone is insufficient for FL development. Epigenetic dysregulations and host factors may also be involved.8 Histologic transformation to aggressive lymphoma occurs in up to 40% of the patients, frequently leading to death within a few years of transformation.9 Patients with localized stage I or II disease may be offered radiation, surveillance, or upfront chemoimmunotherapy (ie, rituximab or another anti-CD20 agent with systemic cytotoxic chemotherapy)10 Treatment is recommended when patients meet the following GELF criteria: a maximum diameter of any site of disease >7 cm, >3 nodal sites >3 cm in diameter, systemic B symptoms, a spleen size >16 cm, pleural effusions, local compressive symptoms, circulating lymphoma cells, or cytopenias as a result of the lymphoma.11 Despite a median overall survival (OS) of >10 years, approximately 20% of the patients with FL relapse within 2 years of therapy.12 Patients with early relapsing FL following induction therapy within 24 months (POD24) have worse clinical outcomes vs those who do not experience disease relapse in 2 years.13 These patients (POD24) may be considered for allogeneic hematopoietic stem cell transplantation (HSCT), which however is associated with non-relapse mortality of 40%.14 Recently, up-front chimeric antigen receptor T cell (CAR-T) therapy, instead of HSCT in POD24 patients represents an emerging treatment option based on the favorable clinical outcome of the former.15 In addition, following each relapse, FL patients experience decrease in duration of each subsequent remission, with eventual exhaustion of therapeutic options, indicating an unmet therapeutic need.16 Another therapeutic challenge is that CD20 is variably expressed on FL.17 CD20 level is predictive for response to rituximab in a diverse group of B-cell lymphomas.18 In fact, low CD20 expression has been associated with inferior outcome, regardless of whether patients were treated with or without rituximab.19
In contrast, DLBCL is the most common subtype of NHL in the United States. It falls under the group of high-grade B-cell lymphomas which may include certain molecular features of clinical importance, such as genomic alterations in MYC, BCL-2, and/or BCL-6 oncogenes.20 Alterations of epigenetic regulating genes are the most prominent in high-grade B-cell lymphomas with “double-hit” mutations (mutations in MYC with either BCL-2 or BCL-6).13 Based on the cell-of-origin classification of DLBCL derived from transcriptome analysis and gene-expression profiling, DLBCL can be further categorized into the activated B-cell–like (ABC) and germinal-center B-cell–like (GCB) subgroups.21,22 Frontline therapy for high-grade B-cell lymphomas comprises chemoimmunotherapy which often leads to remission and cure. However, 20–30% of the patients with DLBCL relapse or become refractory to frontline therapy, necessitating salvage therapy followed by autologous HSCT.23 Even among patients who undergo autologous HSCT, 40–50% tend to relapse.23 Although CAR-T therapy has been approved by the United States Food and Drug Administration (FDA) in this setting, this treatment is not widely available to all eligible patients, and many patients may not be considered fit to undergo this treatment.24,25 Thus, alternative treatment options, in addition to polatuzumab vedotin or loncastuximab tesirine (both are approved by FDA as third-line therapies), are needed for patients with relapsed or refractory DLBCL.
In addition to genomic alterations aforementioned, aberrant epigenetic alterations constitute another mechanism of pathogenesis for FL and DLBCL. Mutations in epigenetic modifiers in germinal center result in dysregulations of B cell differentiation and contribute to pathogenesis.8 Nevertheless, no epigenetic therapy for B-cell lymphomas has received regulatory approval prior to 2020.
This minireview examines the current level of understanding of epigenetic therapies for FL and DLBCL, with focus on a novel epigenetic therapy, tazemetostat (formerly EPZ-6438 or E7438) for relapsed or refractory FL. Optimal therapeutic approaches are briefly evaluated.
Epigenetic Dysregulations
Mutations of genes encoding chromatin modifiers are prevalent in FL and DLBCL. Chromatin is composed of DNA and proteins known as histones. Epigenetic modifications of histones (by methylation or acetylation) and DNA (by methylation) limit or promote the accessibility of DNA to transcription factors and DNA repair enzymes, thereby regulating gene expression and maintaining genomic stability during embryogenesis and differentiation.26,27 Furthermore, specific DNA methylation patterns are determined in early stages of B cell activation and lymphomagenesis, underlying its important role in cancer development.28 Of note, histone H3 lysine 4 (H3K4) trimethylation and histone 3 lysine 27 (H3K27) trimethylation lead to promoter hypermethylation and inactivation of transcription.26 Other mutations include genes that encode lysine-specific histone methyltransferase KMT2D (mutated in 89% of FL cases), histone and non-histone acetyltransferases such as cyclic adenosine 3.5-monophosphate response element binding proteins (CREBBP, mutated in 30% of FL cases) and E1A-associated protein p300 (EP300, mutated in 11% of FL cases). Both of which function as transcriptional coactivators in multiple signaling pathways.29 Mutations in KMT2D lead to increased genomic DNA damage and instability, increased mutation load, transcriptional instability, and infiltration of immune cells to the tumor microenvironment, making the tumor cells amenable to immunotherapy.30 Notably, KMT2D is one of the most frequently altered genes in double-hit DLBCL.31
EZH2 as an Epigenetic Repressor
Enhancer of zeste homolog 2 (EZH2) is a histone-associated methyltransferase. It is the catalytic subunit of an epigenetic regulator, polycomb repressive complex 2 (PRC2) that catalyzes trimethylation of H3K27 (H3K27me3). This H3K27me3 mark is transcriptionally repressive in silencing developmentally regulated genes. H3K27me3 promoters are bivalent by possessing both the repressive H3K27me3 mark and the activating H3K4 trimethylation (H3K4me3) mark. These promoters can be rapidly activated through the loss of H3K27me3 or repressed through the loss of H3K4me3.29 Biologically, EZH2 repress the expression of genes that are transcribed in naïve B cells (pre-B cells), either through addition of H3K27me3 to H3K4me3-marked promoters to create bivalency or through the addition of H3K27me3 to promoters that are not marked with H3K4me3.29
In pre-B cells, EZH2 is expressed to allow optimal V(D)J recombination in the adult bone marrow. It also represses genes involved in cell cycle arrest and terminal differentiation. During the migration of B cells to the secondary lymphoid tissue, EZH2 is downregulated until germinal center is formed. However, it is subsequently expressed again during somatic hypermutation and isotype switching to allow silencing of the anti-proliferative genes (eg, genes that encode cyclin-dependent kinase inhibitor 1A [CDKN1A1], cyclin-dependent kinase inhibitor 2A [CDKN2A]) and the pro-differentiation genes (eg, interferon regulatory factor 4 [IRF4], PR domain zinc finger protein 1[PRDM1]). As B cells begin to differentiate, EZH2 activity becomes increasingly opposed by a chromatin regulator, switch/sucrose non-fermentable (SWI/SNF) complex, which facilitates gene expression and terminal differentiation. EZH2 is repressed when mature B cells exit the germinal center.32,33
In summary, B cells with aberrant activity of EZH2, caused by the gain-of-function activating mutations of EZH2, result in epigenetic silencing, B cell proliferation, and clonal development of malignant cells.34,35 EZH2 gene mutations have been associated with the development of germinal center-derived lymphomas, including FL and DLBCL.36,37 They drive cancer development by repressing target genes involved in proliferation checkpoints (eg, CDKN1A) and B cell terminal differentiation (eg, IRF4 and PRDM1)34,35 and account for 27% of the patients with FL and 30% of the patients with germinal center-derived DLBCL36,38,39 Lastly, EZH2 participates in immune escape of tumor cells by suppressing antigen presentation and preventing homing of immune effector cells to the tumor microenvironment.30
CREBBP and KMT2D as Transcriptional Activators
CREBBP and KMT2D gene mutations are loss-of-function genetic aberrations that disrupt the B cell development in germinal center and promote the development of germinal center-derived lymphomas.39,40 Although the molecular pathogenesis of FL remains incompletely understood, current research postulates that BCL-2 gene rearrangements, CREBBP gene mutations and gain-of-function EZH2 gene mutations are “founder” events in oncogenesis, whereas KMT2D gene mutations occur late due to disease progression or drug resistance.39,40
Interestingly, both histone-modifying genes and genomic DNA have been associated with DLBCL oncogenesis. Among them, KMT2D is the most commonly (25% of cases) mutated gene in DLBCL.41 CREBBP and EP300 are usually mutually exclusive and are genetically altered in approximately 17% of DLBCL cases.34 Furthermore, high levels of DNA methylation heterogeneity in DLBCL at the time of diagnosis could predict relapse subsequent to certain systemic chemoimmunotherapy.42
Therapies Targeting Epigenetic Dysregulations
Historically, many epigenetic therapies (epidrugs) have been used in hematological malignancies. Abnormal epigenetic changes such as methylation of transcription promoter genes are universal in patients with myeloid malignancies, making the abnormal global methylation pattern amenable to DNA methyltransferase inhibitors such as azacitidine and decitabine.43,44 Moreover, mutations in genes such as IDH1 and IDH2 result in epigenetic abnormalities which also contribute to the development of myeloid malignancies and offer opportunities for targeted therapies with IDH1 (eg, ivosidenib) and IDH2 (eg, enasidenib) inhibitors.45
Histone deacetylases (HDAC) and histone acetyltransferases control acetylation of histone and non-histone proteins, thereby regulating gene transcription, protein function, and protein stability. Use of HDAC inhibitors causes hyperacetylation of histone and non-histone proteins, leading to the transcriptional activation of tumor suppressor genes, as well as genes involved in cell cycle control, cell division, and apoptosis, resulting in antitumor activity.46 Currently, various HDAC inhibitors that target histone acetylation are in active development. It is noteworthy that current clinically available HDAC inhibitors are not specific for histone deacetylases, but rather, they inhibit non-histone deacetylases. Two early phase II studies46,47 with epigenetic therapies for patients with NHL found that HDAC inhibitors such as abexinostat and vorinostat were clinically effective for patients with FL with acceptable toxicities, spurring the development of other epidrugs such as the EZH2 inhibitors.
Tazemetostat Approval for FL
Tazemetostat is a first-in-class oral inhibitor of wild type and mutant EZH2 for the treatment of NHL. FL with either wild-type EZH2 or mutant EZH2 are dependent on EZH2 due to its critical role in germinal center formation. EZH2 mutations occur in 20% of the FL cases. They are prognostic for longer failure-free survival and OS in high-risk FL.48
In an open-label, multicenter, dose escalation phase I trial (NCT01897571),32 eligible patients with relapsed or refractory B-cell NHL (n=21) or an advanced solid tumor (n=43) received tazemetostat orally from 100 mg twice daily to 1600 mg twice daily in 28-day cycles. The primary point was to establish the maximum tolerable dose (which was the recommended phase II dose of tazemetostat). Grade 4 thrombocytopenia was identified as the dose-limiting toxicity at the highest dose of 1600 mg twice daily. The recommended phase II dose was determined to be 800 mg twice daily. Durable objective responses were observed in eight (38%) of patients with B-cell NHL. Most common treatment-related adverse effects were asthenia (33%), anorexia (6%), muscle spasms (14%), nausea and/or vomiting (9%) and anemia (14%). They were usually of grade 1 or 2 in severity.32
Based on the favorable antitumor activity and tolerable adverse effects associated with tazemetostat, a phase II trial enrolled two cohorts of patients with relapsed or refractory FL after at least two prior systemic therapies.49 In the cohort of patients (n=45) with mutated EZH2 FL, objective response rate (ORR, primary end point) was 69%, with 13% complete response (CR) and 56% partial response (PR). Median duration of response was 10.9 months (range: 7.2 to not estimable) and median progression-free survival (PFS) was 13.8 months (range: 10.7–22 months). In the cohort of patients with wild-type EZH2 FL (n=54), ORR was 35%, with 4% CR and 31% PR. Median duration of response was 13 months (range: 5.6 to not estimable) and median PFS was 11.1 months (range: 3.7–14.6 months). Responses were delayed with a median time to first response of 3.7 months in both groups.
Among all 99 patients, treatment-related ≥grade 3 adverse events were usually hematologic which included thrombocytopenia (3%), neutropenia (3%) and anemia (2%). Four (4%) patients experienced a serious (grade 4) treatment-related adverse event (sepsis, health deterioration, and anemia). Nine (9%) patients had dose reductions and 27 patients (27%) had dose interruptions due to treatment-emergent adverse events. Lastly, it must be noted that although the study reported tumor response based the EZH2 mutational status, it was not designed to compare the clinical outcomes based on the EZH2 mutation status. Additionally, treatment-related adverse events were not categorized by the EZH2 mutational status.
On ground of its durable response and well-tolerated adverse effects in the phase II trial, tazemetostat received FDA approved indications for patients with mutated EZH2 relapsed or refractory FL after ≥2 prior systemic therapies in 2020. It is also approved for those with relapsed or refractory FL who have no satisfactory alternative treatment options, regardless of their mutational status of EZH2. Testing for EZH2 mutational status (Y646, A682, or A692) for patients with relapsed or refractory FL after two prior therapies is recommended based on the United States National Comprehensive Cancer Network (NCCN) guidelines.7 Testing should be performed by an approved sequencing assay on the paraffin-embedded specimen.
Emerging Epigenetic Therapies for DLBCL
Certain genetic lesions demonstrate a preferential distribution among the two major subtypes of DLBCL (ABC subtype vs GCB-type).50 Oncogenic mutations in EZH2 are observed in 22% of GCB DLBCL but are absent in the ABC phenotype.36 Moreover, although some gene lesions (eg, MYD88, BCL-2, CREBBP) are common in DLBCL, they are rare in clinical cases,51 confirming the findings that MYD88 mutations are commonly found in the ABC subtype but are rare in the GCB subtype or primary mediastinal large B-cell lymphomas.41,42 Since the ABC subtype has a worse prognostic outcome compared to the GCB subtype, these prognostic differences in survival outcomes may represent opportunities in precision medicine. To date, precision medicine aims to capitalize on these differences in molecular abnormalities is still lacking.
Tazemetostat has recently demonstrated promising clinical activity in about 20% of heavily pretreated, refractory patients with DLBCL, regardless of their EZH2 mutational status.46 A number of clinical trials [NCT02889523, NCT02220842] are investigating the role of tazemetostat with systemic chemotherapy or anti-CD20 agent. Table 1 provides a number of ongoing clinical trials of tazemetostat in FL and DLBCL in frontline and relapsed/refractory settings.
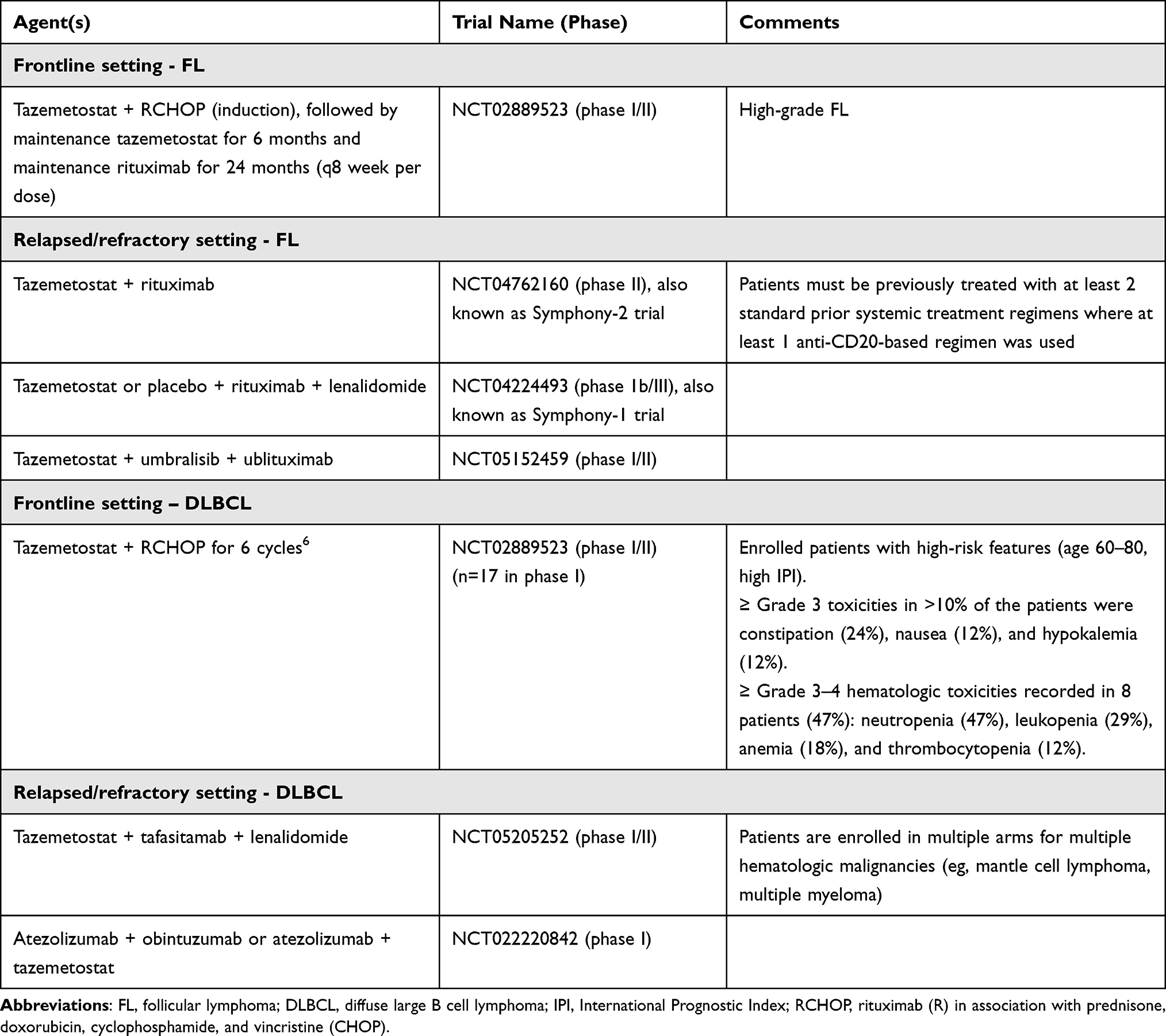 |
Table 1 Ongoing Clinical Trials of Tazemetostat in Follicular Lymphoma and Diffuse Large B Cell Lymphoma in Frontline and Relapsed/Refractory Settings |
Relevance to Clinical Practice
Aberrant epigenetic silencing occurs at a very early stage in neoplastic development, allowing precision medicine to target these epimutations. Some of these epigenetic regulators (eg, EZH2) prevent cellular differentiation in stem cells and/or cancer progenitor cells and their subsequent dysregulation represent excellent drug targets, lending to a “chemotherapy-free” option to patients with relapsed or refractory FL with or without mutated EZH2. Agents such as lenalidomide in combination with rituximab (R2 regimen), phosphatidylinositol 3-kinase (PI3K) inhibitors (copanlisib, duvelisib, umbralisib) and tazemetostat have received regulatory approvals for multiple relapsed FL. Current NCCN guideline suggests that tazemetostat is a third-line or subsequent-line option for relapsed or refractory FL.4 Other therapeutic agents for relapsed or refractory FL after two lines of therapy may include copanlisib, duvelisib, umbralisib (voluntarily withdrawn from the market in 2022) and CAR-T.7 It must be pointed out that umbralisib is recommended for the elderly and infirm in this treatment setting and may only be used under the expanded access program after its withdrawal.7
In the real world, therapeutic decisions are usually based on considerations of patient’s prior treatments, treatment-related toxicities, route of administration, patient preference, prescriber experience, and insurance eligibility. For example, tazemetostat may be preferred by some patients because of its oral route of administration, while others may prefer an intravenous regimen (eg, copanlisib, rituximab) that incorporates treatment-free days.52 Alternatively, tazemetostat may be offered to patients with EZH2 mutation in first relapse or to patients without EZH2 mutation in subsequent relapse.52
EZH2 inhibitors may be synergistic with other epigenetic modifying agents (such as HDAC inhibitors and DNA methyltransferase inhibitors), systemic chemotherapy, immunomodulatory agents, and even investigational agents (eg, acalabrutinib, daratumumab, pomalidomide, ublituximab) used in clinical trials for FL or DLBCL. Trials with some combinatorial therapies (NCT04224493, NCT05205252, NCT04762160 [Symphony-2 trial], NCT05152459) are under way.
However, a few problems remain with the epigenetic therapies: first, there is a lack of specificity of epidrugs. Second, epigenetic therapies may confer potential deleterious effects to the regular epigenetic processes of normal cells, resulting in off-target toxicities, ectopic gene activation and potential activation of the oncogenic pathways in normal cells,53,54 although many patients receiving these therapies unfortunately are not expected to live long enough to witness the manifestations of these secondary carcinogenic side effects. Current clinical data49,55 states that tazemetostat increases the risk of secondary malignancies, including myeloid malignancies and T cell lymphoma.
With an average wholesale acquisition cost of $17,746 based on a 30-day package56 and an estimated median treatment duration of 14 months (PFS) in mutated EZH2 FL patients, the total cost of treatment for tazemetostat is approximately $250,000, raising the stake of financial toxicity and access issue significantly, especially in elderly or indigent patients with economic limitations. To date, no cost analysis of tazemetostat or its cost comparison with other therapies has been published.
Conclusions
Major advances have been made in targeting the epigenetic signaling pathways in patients with advanced FL. They represent new opportunities to improve patient clinical outcome in the relapsed or refractory setting, while ongoing studies for early disease setting also show promise. Epigenetic therapies represent an option to augment antitumor effects, overcome drug resistance, and activation of host immune response. However, their potential pitfalls must be carefully monitored. Further studies are warranted to identify the combination therapies to maximize treatment benefits. Future applications of epigenetic approach that incorporate clinical and genomic features are needed to determine how individualized treatments can be used for FL and DLBCL.
Disclosure
The author reports no conflicts of interest in this work.
References
1. de Leval L, Jaffe ES. Lymphoma classification. Cancer J. 2020;26(3):176–185.
2. Kridel R, Sehn LH, Gascoyne RD. Pathogenesis of follicular lymphoma. J Clin Invest. 2012;122(10):3424–3431.
3. Green MR, Gentles AJ, Nair RV, et al. Hierarchy in somatic mutations arising during genomic evolution and progression of follicular lymphoma. Blood. 2013;121(9):1604–1611.
4. Mann RB, Berard CW. Criteria for the cytologic subclassification of follicular lymphomas: a proposed alternative method. Hematol Oncol. 1983;1(2):187–192.
5. Koch K, Richter J, Hanel C, et al. Follicular lymphoma grade 3B and diffuse large B-cell lymphoma present a histopathological and molecular continuum lacking features of progression/transformation. Haematologica. 2022. doi:10.3324/haematol.2021.279351
6. Sarkozy C, Morschhauser F, Dubois S, et al. A LYSA phase Ib study of tazemetostat (EPZ-6438) plus R-CHOP in patients with newly diagnosed diffuse large B-cell lymphoma (DLBCL) with poor prognosis features. Clin Cancer Res. 2020;26(13):3145–3153.
7. NCCN clinical practice guideline in B-cell lymphoma; 2022. Available from: https://www.nccn.org/professionals/physician_gls/pdf/b-cell.pdf.
8. Hanel W, Epperla N. Evolving therapeutic landscape in follicular lymphoma: a look at emerging and investigational therapies. J Hematol Oncol. 2021;14(1):104.
9. Kridel R, Sehn LH, Gascoyne RD. Can histologic transformation of follicular lymphoma be predicted and prevented? Blood. 2017;130(3):258–266.
10. Rummel MJ, Niederle N, Maschmeyer G, et al. Bendamustine plus rituximab versus CHOP plus rituximab as first-line treatment for patients with indolent and mantle-cell lymphomas: an open-label, multicentre, randomised, Phase 3 non-inferiority trial. Lancet. 2013;381(9873):1203–1210.
11. Brice P, Bastion Y, Lepage E, et al. Comparison in low-tumor-burden follicular lymphomas between an initial no-treatment policy, prednimustine, or interferon alfa: a randomized study from the Groupe d’Etude des Lymphomes Folliculaires. Groupe d’Etude des Lymphomes de l’Adulte. J Clin Oncol. 1997;15(3):1110–1117.
12. Nooka AK, Nabhan C, Zhou X, et al. Examination of the follicular lymphoma international prognostic index (FLIPI) in the National LymphoCare study (NLCS): a prospective US patient cohort treated in community practices. Ann Oncol. 2013;24(2):441–448.
13. Freedman A, Jacobsen E. Follicular lymphoma: 2020 update on diagnosis and management. Am J Hematol. 2020;95(3):316–327.
14. Avivi I, Montoto S, Canals C, et al. Matched unrelated donor stem cell transplant in 131 patients with follicular lymphoma: an analysis from the Lymphoma Working Party of the European Group for Blood and Marrow Transplantation. Br J Haematol. 2009;147(5):719–728.
15. Jacobson CA, Chavez JC, Sehgal AR, et al. Interim analysis of ZUMA-5: a phase II study of axicabtagene ciloleucel (axi-cel) in patients (pts) with relapsed/refractory indolent non-Hodgkin lymphoma (R/R iNHL). J Clin Oncol. 2020;38(suppl15):8008.
16. Kambhampati S, Fakhri B, Ai WZ, et al. Carfilzomib in combination with bendamustine and rituximab in patients With relapsed or refractory non-Hodgkin lymphoma: a phase I trial. Clin Lymphoma Myeloma Leuk. 2021;21(3):139–146.
17. Olejniczak SH, Stewart CC, Donohue K, et al. A quantitative exploration of surface antigen expression in common B-cell malignancies using flow cytometry. Immunol Invest. 2006;35(1):93–114.
18. Horvat M, Kloboves Prevodnik V. Predictive significance of the cut-off value of CD20 expression in patients with B-cell lymphoma. Oncol Rep. 2010;24(4):1101–1107.
19. Johnson NA, Boyle M, Bashashati A, et al. Diffuse large B-cell lymphoma: reduced CD20 expression is associated with an inferior survival. Blood. 2009;113(16):3773–3780.
20. Schmitz R, Wright GW, Huang DW, et al. Genetics and pathogenesis of diffuse large B-cell lymphoma. N Engl J Med. 2018;378(15):1396–1407.
21. Alizadeh AA, Eisen MB, Davis RE, et al. Distinct types of diffuse large B-cell lymphoma identified by gene expression profiling. Nature. 2000;403(6769):503–511.
22. Shaffer AL, Young RM, Staudt LM. Pathogenesis of human B cell lymphomas. Annu Rev Immunol. 2012;30:565–610.
23. Mounier N, Canals C, Gisselbrecht C, et al. High-dose therapy and autologous stem cell transplantation in first relapse for diffuse large B cell lymphoma in the rituximab era: an analysis based on data from the European Blood and Marrow Transplantation Registry. Biol Blood Marrow Transplant. 2012;18(5):788–793.
24. Schuster SJ, Svoboda J, Chong EA, et al. Chimeric antigen receptor T cells in refractory B-cell lymphomas. N Engl J Med. 2017;377(26):2545–2554.
25. Neelapu SS, Locke FL, Bartlett NL, et al. Axicabtagene ciloleucel CAR T-cell therapy in Refractory large B-cell lymphoma. N Engl J Med. 2017;377(26):2531–2544.
26. Lunning MA, Green MR. Mutation of chromatin modifiers; an emerging hallmark of germinal center B-cell lymphomas. Blood Cancer J. 2015;5(10):e361.
27. Meissner A. Epigenetic modifications in pluripotent and differentiated cells. Nat Biotechnol. 2010;28(10):1079–1088.
28. Lai AY, Mav D, Shah R, et al. DNA methylation profiling in human B cells reveals immune regulatory elements and epigenetic plasticity at Alu elements during B-cell activation. Genome Res. 2013;23(12):2030–2041.
29. Green MR. Chromatin modifying gene mutations in follicular lymphoma. Blood. 2018;131(6):595–604.
30. Wang X, Brea LT, Yu J. Immune modulatory functions of EZH2 in the tumor microenvironment: implications in cancer immunotherapy. Am J Clin Exp Urol. 2019;7(2):85–91.
31. Cucco F, Barrans S, Sha C, et al. Distinct genetic changes reveal evolutionary history and heterogeneous molecular grade of DLBCL with MYC/BCL2 double-hit. Leukemia. 2020;34(5):1329–1341.
32. Italiano A, Soria JC, Toulmonde M, et al. Tazemetostat, an EZH2 inhibitor, in relapsed or refractory B-cell non-Hodgkin lymphoma and advanced solid tumours: a first-in-human, open-label, Phase 1 study. Lancet Oncol. 2018;19(5):649–659.
33. Ribeiro ML, Reyes-Garau D, Armengol M, et al. Recent advances in the targeting of epigenetic regulators in B-cell non-Hodgkin lymphoma. Front Genet. 2019;10:986.
34. Béguelin W, Popovic R, Teater M, et al. EZH2 is required for germinal center formation and somatic EZH2 mutations promote lymphoid transformation. Cancer Cell. 2013;23:677–692.
35. Béguelin W, Teater M, Gearhart MD, et al. EZH2 and BCL6 cooperate to assemble CBX8-BCOR complex to repress bivalent promoters, mediate germinal center formation and lymphomagenesis. Cancer Cell. 2016;30:197–213.
36. Morin RD, Johnson NA, Severson TM, et al. Somatic mutations altering EZH2 (Tyr641) in follicular and diffuse large B-cell lymphomas of germinal-center origin. Nat Genet. 2010;42(2):181–185.
37. Bödör C, O’Riain C, Wrench D, et al. EZH2 Y641 mutations in follicular lymphoma. Leukemia. 2011;25(4):726–729.
38. Pasqualucci L, Trifonov V, Fabbri G, et al. Analysis of the coding genome of diffuse large B-cell lymphoma. Nat Genet. 2011;43:830–837.
39. Basso K, Dalla-Favera R. Germinal centres and B cell lymphomagenesis. Nat Rev Immunol. 2015;15(3):172–184.
40. Zhang J, Dominguez-Sola D, Hussein S, et al. Disruption of KMT2D perturbs germinal center B cell development and promotes lymphomagenesis. Nat Med. 2015;21(10):1190–1198.
41. Reddy A, Zhang J, Davis NS, et al. Genetic and functional drivers of diffuse large B cell lymphoma. Cell. 2017;171(2):481–494.e15.
42. Pan H, Jiang Y, Boi M, et al. Epigenomic evolution in diffuse large B-cell lymphomas. Nat Commun. 2015;6:6921.
43. Soriano AO, Yang H, Faderl S, et al. Safety and clinical activity of the combination of 5-azacytidine, valproic acid, and all-trans retinoic acid in acute myeloid leukemia and myelodysplastic syndrome. Blood. 2007;110(7):2302–2308.
44. Welch JS, Petti AA, Miller CA, et al. TP53 and decitabine in acute myeloid leukemia and myelodysplastic syndromes. N Engl J Med. 2016;375(21):2023–2036.
45. Chung C. Targeting the myeloid lineages and the immune microenvironment in myelodysplastic syndromes: novel and evolving therapeutic strategies. Ann Pharmacother. 2022;56(4):475–487.
46. Ribrag V, Kim WS, Bouabdallah R, et al. Safety and efficacy of abexinostat, a pan-histone deacetylase inhibitor, in non-Hodgkin lymphoma and chronic lymphocytic leukemia: results of a phase II study. Haematologica. 2017;102(5):903–909.
47. Kirschbaum M, Frankel P, Popplewell L, et al. Phase II study of vorinostat for treatment of relapsed or refractory indolent non-Hodgkin’s lymphoma and mantle cell lymphoma. J Clin Oncol. 2011;29(9):1198–1203.
48. Pastore A, Jurinovic V, Kridel R, et al. Integration of gene mutations in risk prognostication for patients receiving first-line immunochemotherapy for follicular lymphoma: a retrospective analysis of a prospective clinical trial and validation in a population-based registry. Lancet Oncol. 2015;16(9):1111–1122.
49. Morschhauser F, Tilly H, Chaidos A, et al. Tazemetostat for patients with relapsed or refractory follicular lymphoma: an open-label, single-arm, multicentre, Phase 2 trial. Lancet Oncol. 2020;21(11):1433–1442.
50. Bakhshi TJ, Georgel PT. Genetic and epigenetic determinants of diffuse large B-cell lymphoma. Blood Cancer J. 2020;10(12):123.
51. Lohr JG, Stojanov P, Lawrence MS, et al. Discovery and prioritization of somatic mutations in diffuse large B-cell lymphoma (DLBCL) by whole-exome sequencing. Proc Natl Acad Sci U S A. 2012;109(10):3879–3884.
52. Freedman AS, Friedberg JW. Treatment of relapsed or refractory follicular lymphoma. Waltham (MA): UpToDate; 2022.
53. Lu Y, Chan YT, Tan HY, et al. Epigenetic regulation in human cancer: the potential role of epi-drug in cancer therapy. Mol Cancer. 2020;19(1):79.
54. Cheng Y, He C, Wang M, et al. Targeting epigenetic regulators for cancer therapy: mechanisms and advances in clinical trials. Signal Transduct Target Ther. 2019;4:62.
55. Epizyme. Tazverik (Tazemetostat) Prescribing Information. Cambridge, MA: Epizyme; 2020.
56. Thompson Micromedex. Tazverik (Tazemetostat). Red Book Online [Internet Database]. Greenwood Village, CO: Thompson Micromedex; 2020.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
EZH2: From Oncogenic Driver to Therapeutic Target for Overcoming Drug Resistance in Hepatocellular Carcinoma
Tang W, Cao J, Wang N, Tang L, Cao J
Journal of Hepatocellular Carcinoma 2025, 12:3091-3104
Published Date: 31 December 2025