Back to Journals » Cancer Management and Research » Volume 13
A Prognostic Scoring System for Predicting Overall Survival of Patients with the TNM 8th Edition Stage I and II Hepatocellular Carcinoma After Surgery: A Population-Based Study
Authors Bai Y, Lian Y, Wu J ![]() , Chen S, Lai J, Zheng Y
, Chen S, Lai J, Zheng Y ![]() , Tian Y, Yan M
, Tian Y, Yan M ![]() , Wang Y
, Wang Y ![]()
Received 4 November 2020
Accepted for publication 20 January 2021
Published 2 March 2021 Volume 2021:13 Pages 2131—2142
DOI https://doi.org/10.2147/CMAR.S289826
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Antonella D'Anneo
Yannan Bai,1,* Yuan’e Lian,2,* Jiayi Wu,1 Shi Chen,1 Jianlin Lai,1 Yu Zheng,1 Yifeng Tian,1 Maolin Yan,1 Yaodong Wang1
1Hepatobiliary Surgery Department, Shengli Clinical Medical College of Fujian Medical University, Fujian Provincial Hospital, Fuzhou, 350001, China; 2Pathology Department, Fujian Medical University Union Hospital, Fuzhou, 350001, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yaodong Wang; Maolin Yan
Fujian Provincial Hospital, Shengli Clinical Medical College of Fujian Medical University, Fuzhou, 350001, People’s Republic of China
Tel +86-591-88217130
Fax +86-591-88217140
Email [email protected]; [email protected]
Purpose: Postoperative prognosis prediction models for patients with stage Ⅰ and Ⅱ hepatocellular carcinoma (HCC) according to the 8th edition of the Tumor-Node-Metastasis staging system after surgery are rare. This study aimed to build a prognostic score to predict survival outcomes and stratify these patients into different prognostic strata.
Patients and Methods: We developed a web-based nomogram that incorporated four selected risk factors based on the multivariate Cox regression, using a training set (n=3567) from the Surveillance, Epidemiology, and End Results (SEER) database. It was validated with an independent internal set from the SEER database (n=1783) and an external validation set of 516 Chinese patients. The predictive performance and discrimination ability of our model were further evaluated and compared with those of the conventional HCC staging systems.
Results: Our nomogram consistently outperformed the conventional staging systems in the training, internal validation set, and external validation set. We quantified the nomogram model into a numerical SNIG (an abbreviation of the incorporated variables – size, number, MVI, and grade) score by summing the points assigned to each incorporated variable, leading to the optimal cut-off values of 6 and 10, which could stratify patients into 3 categories (SNIG score < 6, 6– 10, ≥ 10). This yielded significantly different median overall survivals (interquartile ranges) of 42.0 (20.0– 72.0) and 37.0 (17.0– 67.0); 28.0 (12.0– 60.0) and 42.0 (21.75– 82.0); 40.0 (18.0– 70.0) and 29.0 (11.5– 61.0) months for the 3 categories in the entire SEER and external validation sets, respectively.
Conclusion: We developed a web-based SNIG model to graphically and numerically predict the overall survival of stage Ⅰ and Ⅱ HCC. This scoring system may shed light on risk stratification for these patients in clinical practice and clinical trials.
Keywords: hepatocellular carcinoma, overall survival, SNIG model, SEER
Introduction
Hepatocellular carcinoma (HCC) is the sixth most frequent malignancy and fourth leading cause of cancer deaths globally. Over 50% of new cases and deaths occur in China.1 Liver resection (LR) remains the first-line treatment for patients with HCC; however, the long-term prognosis after LR remains discouraging due to the high postoperative recurrence rate.2 Identifying prognostic factors would help to improve long-term prognosis after surgical treatment of HCC.
The commonly used staging systems include the Barcelona Clinic Liver Cancer, Cancer of the Liver Italian Program, Liver Cancer Study Group of Japan (LCSGJ), Japan Integrated Staging, Chinese University Prognostic Index, and Tumor-Node Metastasis (TNM), each with different prognostic models and therapeutic algorithms.3–6 TNM staging for HCC is endorsed by the American Joint Committee on Cancer (AJCC)/International Union against Cancer. It focuses on the pathologic tumor characteristics in patients who are eligible for surgery and serves as a bridge between a “population-based” and more “personalized” approach to cancer staging.7 However, the applicability of this “surgical” staging system is often challenged due to its poor prognostic ability in early-stage and advanced HCC.5,8,9 A critical evaluation by Kamarajah et al10 revealed that the updated 8th edition of the AJCC TNM staging system failed to improve the stratification of HCC prognosis when compared to the 7th edition, suggesting the need of substratification for early HCC.
A nomogram is a reliable statistical predictive model for estimating and predicting individual cancer-related outcomes for clinical use. Based on various combinations of serological markers, liver function and cirrhosis assessments, clinicopathological parameters, integrative and comprehensive genomic signatures, or biomarkers, an increasing number of nomogram models for prognosis prediction in patients with different stages of HCC receiving different treatments have been established.10–24 The prognostic power of these models is markedly superior to that of the traditional HCC staging systems. However, the predicted models were based on data that included patients who were not eligible for LR.11,13,25 No system has consistently been considered the best model of postoperative survival. Therefore, there is a need to develop effective models that incorporate well-established clinicopathological variables with a definite power to predict prognosis, particularly among patients with early HCC.
This study aimed to build and validate a prognostic nomogram model for overall survival (OS) of patients with early and resectable HCC (including stage I or II according to the 8th edition AJCC-TNM staging system) from the Surveillance, Epidemiology and End Results (SEER) dataset who underwent curative-intent LR. The model was validated with an internal set from the SEER dataset and an external set of 516 Chinese patients. In addition, we compared the discrimination and performance between the current nomogram model and the conventional staging systems in estimating individualized prognoses.
Patients and Methods
Study Population and Selection Criteria
Information on surgical patients with early and resectable HCC stage I (A and B) or II (according to the 8th edition AJCC-TNM staging system) registered in the SEER dataset between 1998 and 2015 was screened from the SEER 18 registry database using SEER*Stat 8.3.5 software (National Institutes of Health, Bethesda, MD, USA). The flow chart of the data extraction procedure is shown in Figure S1. HCC cases were screened using “The International Classification of Diseases for Oncology (ICD-O-3) Hist/behav, malignant,” “Summary stage 2000 (1998+),” “Derived AJCC Stage Group 6th (2004+),” “Derived AJCC Stage Group, 7th ed (2010–2015),” “EOD 10 - size (1988–2003),” “CS tumor size (2004+),” “EOD 10 - extent (1988–2003),” “CS extension (2004–2015),” “Lymph-vascular Invasion (2004+ varying by schema),” “RX Summ-Surg Prim Site (1998+),” and “Grading and differentiation codes in ICD-O-3” in this study. “Vital status recode” and “SEER cause-specific death classification” were used to set endpoints for OS, defined as the interval from HCC diagnosis to overall death using “survival months code”. Histology codes were used to identify patients with HCC (8170–8175). Patients were included if they were older than 18 years, underwent LR, and had pathologically confirmed T1a, T1b, or T2N0M0 primary HCC. We excluded patients who were treated with local tumor destruction or liver transplantation. Patients with missing data on surgery and tumor-related factors (ie, size, extent of disease, and histological grade), survival time <3 months or unknown, HCC in situ, and a death certificate or autopsy only were excluded to ensure the reliability of the staging data. Cases that were staged using the 3rd, 6th, or 7th edition of the AJCC staging system were restaged using the 8th edition of the AJCC staging system.10,26 All cases were randomly assigned into a training set with N×q samples and an internal validation set with N×(1–q) samples (where q=2/3).
To further evaluate the general prognostic ability of the model, an external validation set was made up of 516 patients who had early-stage HCC and underwent LR at Fujian Provincial Hospital (FPH) between January 2012 and December 2015. The study protocol was approved by the ethics committee of the Fujian Provincial Hospital, and the study was conducted in accordance with the tenets of the Declaration of Helsinki and its later amendments. Written informed consent was obtained from all patients prior to inclusion in the study.
Statistical Analysis
The primary endpoint was OS. Quantitative variables are presented as medians and interquartile ranges (IQRs); they were compared using the Student’s t-test or non-parametric Mann–Whitney U-test, as appropriate. Categorical variables are presented as frequencies with percentages and compared using the chi-square test or Fisher’s exact test, as appropriate. Variables that were significant in the univariate analysis were included in the multivariate Cox regression analyses in the training set (n=3567) to determine independent risk factors. The nomogram was built for OS prediction using the variables identified in the Cox regression analysis. The calibration, discrimination, and performance of the nomogram were assessed using calibration curves, Harrell’s C-index, Akaike information criterion (AIC), likelihood ratio chi-square test, and the area under time-dependent receiving operator characteristic curves (1-, 3-, and 5-year AUROCs), respectively. Decision curve analysis (DCA) was used to assess the clinical utility of the models based on a continuum of potential thresholds for the risk of death (horizontal axis) and net benefit of using the model for patient stratification according to risk (vertical axis), considering that no patient died.27–29 The model was validated via bootstrapping with 1000 samples. The model was compared with conventional staging systems, including the LCSGJ-TNM and the 7th and 8th editions of the AJCC-TNM staging system in the training, internal, and external validation sets.5,26,30
To quantify the constructed model, a new numerical variable was generated by calculating the sum of points assigned to each incorporated variable, as described previously.17,31 Then, the optimal cut-off values of the nomogram score were set using X-tile (Yale University, New Haven, CT, USA). The stratified 1-, 3-, and 5-year OS rates and the median OS were estimated, and the survival curves were plotted using the Kaplan–Meier method. Correlations with the relative hazard ratios (HRs) of OS and model nonlinearity were tested using six-knot restricted cubic splines. A web-based tool was further generated to enhance the illustration and clinical applicability. P < 0.05 was set as the level of statistical significance. All statistical analyses were performed using R version 3.6.1 with “survival,” “rms,” “nomogramEx,” “DynNom,” “Hmisc,” “rmda,” “timeROC,” and “splines” packages.
Results
Study Cohorts
A total of 5350 patients with stage I and II HCC from the SEER database were included in this study. The patients were randomly allocated into the training (n = 3567) and internal validation (n = 1783) sets to construct and validate the nomogram. The external validation set was composed of 516 patients with HCC enrolled at FPH. The median follow-up times were 33 (IQR, 15–64), 35 (15–69), and 38 (25–56) months in the training, internal, and external validation sets, respectively. The respective 1-, 3-, and 5-year OS rates were 79.9%, 47.0%, and 28.0% in the training set; 79.5%, 50.0%, and 31.0% in the internal validation set; and 86.1% and 55%, and 22% in the external validation set, respectively. The demographics and clinicopathological characteristics of the three cohorts are summarized in Table 1.
 |
Table 1 Baseline Demographics and Clinical Characteristics of the Training, Internal Validation, and External Validation Cohort |
Independent Risk Factors in the Training Set
Results of the univariable analysis are shown in Table 2. In the multivariate Cox analysis, tumor size, number, microvascular invasion (MVI), and grade of histologic differentiation (all P < 0.001) were independent risk factors and were used in developing the model.
 |
Table 2 Univariable Analysis and Cox Proportional Hazards Regression Analysis |
Development of the Prognostic Model
Tumor size (≤2, 2–5, 5–10 vs >10 cm) was encoded as a categorical factor. A nomogram (named the SNIG model, an abbreviation of the incorporated variables – size, number, MVI, and grade) was developed to predict the individualized 1-, 3-, and 5-year OS of patients with HCC using the independent risk factors identified above (Figure 1A).
 |
Figure 1 The dynamic nomogram (A) and web-tool (B) of the SNIG model for individual survival prediction in the training set. The nomogram is used by summing the points identified on the point scale for each variable. The total points projected on the bottom scales indicate the probability of 1-, 3-, and 5-year OS. The web-tool of the SNIG model is available at https://baiyannan.shinyapps.io/SNIG/. To use this tool, choose the assigned SNIG scores of a patient with HCC and the time point of the estimated survival time on the left panel. Examples present the estimated Kaplan–Meier curve and the predicted survival probability at 33 months after surgery on the right bottom panel (the black, light blue, or red curve represents example of survival probability from strata 1, 2, and 3, respectively). Abbreviations: HCC, hepatocellular carcinoma; OS, overall survival; MVI, microvascular invasion; SNIG, abbreviation of the incorporated variables – size, number, MVI, and grade. |
Calibration and Validation of the Prognostic Model
The calibration plots showed adequate concordance between the model predictions and actual observations for the 1-, 3-, and 5-year OS in the training set (Figure 2A); these results were similar for the internal and external validation sets (Figure 2B and C). The ROC curves showed that the SNIG model had an acceptable accuracy in predicting 1-, 3-, and 5-year OS in all the three study sets (Figure 2D–F and Table 3). The performance of the SNIG model and other staging systems (the 7th and 8th AJCC-TNM system and the LCSGJ-TNM system) were compared (Table 3). The SNIG model yielded greater AUROC values (1-, 3- and 5-year OS), C-indices, and likelihood ratio test results, implying a favorable performance in all the three study sets. On the other hand, the SNIG model yielded a smaller AIC than the other staging systems, which implied a better goodness-of-fit (Table 3). DCA was used to compare the models. In the training set, the SNIG model had a marginally better net benefit between thresholds of 0.20 and 0.40 when compared to the other staging systems (Figure 3A); similar results were found in the internal and external validation sets (Figure 3B and C).
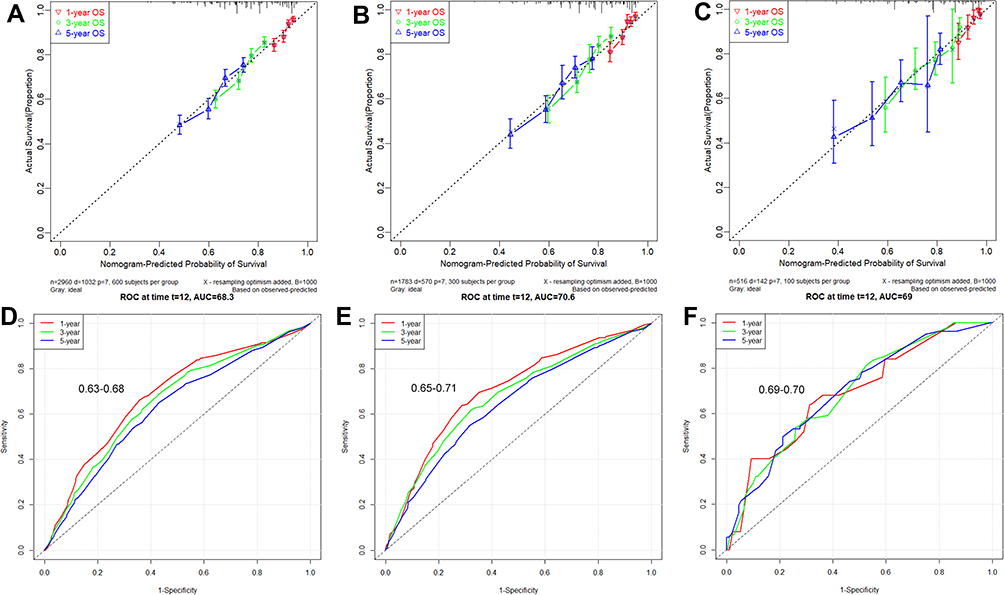 |
Figure 2 The calibration and performance of SNIG model in the 3 datasets. Calibration curves for predicting patient OS at each time point in the (A) training set, (B) internal validation set, and (C) external validation set, respectively. Model-predicted OS is plotted on the x-axis, and actual OS is plotted on the y-axis. A plot along the 45-degree line (dotted blue line) would indicate a perfect calibration model in which the predicted probabilities are identical to the actual outcomes. ROC curves for OS probability in the (D) training set, (E) internal validation set, and (F) external validation set, respectively. Abbreviations: SNIG, abbreviation of the incorporated variables – size, number, MVI, and grade; OS, overall survival; ROC, receiver operating characteristic curve. |
 |
Figure 3 DCA curves of the SNIG model at each time point in the (A) training set, (B) internal validation set, and (C) external validation set, respectively. The net benefits (y-axis) as calculated and it showed that nomogram model results in marginally outperforming between thresholds of 0.20 and 0.40 for prediction of OS. Abbreviations: DCA, decision curve analysis; OS, overall survival. |
 |
Table 3 Comparison of Time-Dependent AUROC, C-Index, Likelihood Ratio, and AIC Between the Current Model and the Other Prognostic Systems |
Cut-Off Value for Risk Stratification
To quantify the constructed model, a new numerical variable (SNIG score) was generated by summing the assigned points of each independent variable (Table S1). Evaluation of nonlinearity of the SNIG score indicated linear profiles in the training, internal, and external validation sets (P = 0.099, 0.23, and 0.75, respectively) (Figure 4). Next, based on the OS calculated using X-tile (Figure S2), the optimal cut-off values of the SNIG score were 6.1 and 10.0, rounded off to 6 and 10, respectively, for clinical use. Accordingly, the patients were classified into 3 categories: level 1, SNIG score <6; level 2, 6–10; level 3, ≥10.
In the entire SEER set, the median OS of the 3 categories from level 1 to level 3 was 42.0 (20.0–72.0), 37.0 (17.0–67.0), and 28.0 (12.0–60.0) months, respectively. With level 1 as the reference, the HRs for levels 2 and 3 were 1.23 (95% confidence interval [CI], 1.05–1.45; P = 0.01) and 2.38 (95% CI, 2.04–3.77; P < 0.001), respectively. In the training set, the median OS of the 3 categories was 42.0 (20.0–72.35), 36.0 (17.0–64.0), and 28.0 (12.0–58.0) months, respectively. With level 1 as the reference, the HRs for levels 2 and 3 were 1.40 (95% CI, 1.08–1.81; P = 0.01) and 2.63 (95% CI, 2.06–3.36; P < 0.001), respectively. In the internal validation set, the median OS of the 3 categories from level 1 to level 3 was 42.0 (IQR, 21.75–82.0), 40.0 (IQR, 18.0–70.0), and 29.0 (IQR, 11.5–61.0) months, respectively. With level 1 as the reference, the HRs for levels 2 and 3 were 1.39 (95% CI, 1.05–1.85; P = 0.02) and 2.58 (95% CI, 1.98–3.38; P < 0.001), respectively. In the external validation set, the median OS of the 3 categories was 56.0 (35.0–68.0), 40.0 (26.0–56.0), and 33.0 (23.0–51.5) months, respectively. With level 1 as the reference, the HRs for levels 2 and 3 were 2.45 (95% CI, 1.17–15.13; P = 0.02) and 4.85 (95% CI, 2.34–10.07; P < 0.001), respectively. The survival outcomes of the 3 categories in all the three cohorts were significantly different, showing an adequate discrimination power of risk stratification (log-rank P < 0.001) (Figures 4 and S3~4, Table S2). For the clinical application of these findings, a web-based model was created using the given numerical points of the SNIG score (https://baiyannan.shinyapps.io/SNIG/, Figure 1B).
Discussion
The main purpose of this study was to propose a new prognostic nomogram for individualized probabilities of a net survival benefit after LR in patients with early-stage HCC. Based on SEER-derived data and our series of patients with HCC who had undergone curative-intent LR, we constructed a web-based predictive nomogram that could reliably predict the numerical 1-, 3-, and 5-year OS and was tailored for individual patients. The nomogram was refined by testing all variables, including tumor size, number of nodules, MVI, and grade of histologic differentiation. This new prognostic model is simple and easy to use and incorporated four well-established clinicopathological variables that constitute the essentials of preoperative clinical evaluation and postoperative pathologic outcomes. This new prognostic model has a strong prognostic ability in different populations (the American population and one hospitalized Chinese population). The 1-, 3-, and 5-year median AUROC values of the SNIG model were 0.66 (range, 0.63–0.68), 0.68 (range, 0.65–0.71), and 0.69 (range, 0.69–0.70), and the C-indices were 0.63, 0.65, and 0.66 in the training, internal validation set, and external validation set, respectively. These results imply that although they were not perfect, they all outperformed the conventional staging systems. Similarly, the SNIG model had a better performance and discrimination ability (Table 3 and Figure 3). In this study, the SNIG score was generated as a new variable by summing the assigned points for each incorporated variable (Table S1), and it was proven to have a linearity profile when tested by restricted cubic splines (nonlinearity test p value˃0.05 in the three cohorts) (Figure 5). It could further be accurately stratified into 3 distinct risk cohorts (strata of <6, 6–10, and ≥10, respectively). The Kaplan–Meier survival curve of these numerical stratified cohorts showed an adequate discrimination power for predicting OS (Figures 4 and S2~3). This prediction model provides individualized prognoses and risk stratification for patients with HCC; therefore, the monitoring of surgical patients will be made easy.
 |
Figure 4 Kaplan–Meier curve of OS in the training set stratified by the 7th AJCC TNM staging (A), 8th AJCC TNM staging (B), LCSGJ TNM staging (C), and nomogram model (D). Abbreviations: OS, overall survival; AJCC, The American Joint Committee on Cancer; LCSGJ TNM, Liver Cancer Study Group of Japan. |
 |
Figure 5 Restricted cubic spline of total score of the current nomogram in the training set (A), the internal validation set (B), and external validation set (C). |
Curative LR is the treatment of choice for early and resectable HCC. Yet, the decision of “medically fit for a major operation” varies a lot, and it seems difficult to make a consensus among the staging systems.2 As a “surgical” staging system, the AJCC-TNM staging system outlines algorithms on the early surgical assessment by National Comprehensive Cancer Network (NCCN), based on the technical ability to resect the tumor, adequacy of the performance status, and liver function.32 The AJCC-TNM staging system typically stratifies the HCC population in stages by tumor morphological criteria (tumor size, number, and MVI). Of note, the major improvement in the 8th edition of the AJCC-TNM system from the 7th edition is that it can substratify the early stages of HCC; however, its prognosis prediction power remains controversial. For example, significant survival differences exist among patients with stage IA tumors with or without MVI,33 stage IB with a cut-off tumor size of 5 cm,34 or stage II with single or multiple nodular lesions.35 Accordingly, several proposed nomograms have been established with an aim to stratify outcomes in a particular patient cohort, with predicted C-indices of 0.75 with or without surgery,17 0.74 for whole staged HCC,11 0.66 for most early-stage HCC lesions,13 or 0.80 for recurrent HCC.15 Nomogram tools can quantify and weigh risk variables, providing a numerical point in individualized survival prediction. Rather discriminating factors in these nomograms, like pathological variables (morphological criteria of HCC), factors regarding pretreatment performance, and liver function, that seemingly have a smaller role play a major role in many staging systems.3–6 To this end, we believe that a nomogram for estimating individualized prognosis after LR may be more advantageous than the conventional staging systems and would help clinicians and patients predict survival more accurately.
The prognosis prediction power of our SNIG model was comparable to that of the prognostic nomogram by Shim et al for patients with HCC after LR;13 however, our cohorts included patients with earlier stages of HCC and no patients with stage IIIA disease. Of note, two key pathological variables in the SNIG model should be highlighted. First, we included MVI, which is a major risk factor for tumor recurrence and mortality in HCC. However, the MVI status can only be assessed by postoperative pathology; when assessed preoperatively, the tumor stage is often underestimated.36 Conventional staging systems do not consider important pathologic variables in prognostic prediction.37,38 Second, grade of histologic differentiation is a direct surrogate of disease aggressiveness and is another major risk factor of survival probability.5,36 Unfortunately, none of the major HCC staging systems incorporate this pathological variable. In the Metroticket study, the survival probabilities increased negatively and linearly with increasing tumor size and number, while the linearity effect reached a plateau (nonlinearity) after the morphological criteria reached a certain threshold.25 Therefore, we included these two variables in the nomogram to add value to the weights of the major independent factors and improve the prediction power of the model. The linearity of the SNIG score system was consistently observed in all the three cohorts (Figure 5).
Our study has several limitations. First, bias was inevitable due to the retrospective nature of the study. Second, the SEER database lacked data on liver function, hepatitis virus infection profile, severity of cirrhosis, relevant tumor biomarkers (eg, α-fetoprotein), and the specified number of tumor nodules, which could have compromised the predictive power of the model to some extent.39 Additionally, the SEER database lacked data on tumor recurrence, which is important for recurrence-free survival and is a more accurate representation of the biological characteristics of HCC than OS, which is mainly influenced by liver function and post-recurrence treatment. Although this model has potential benefits of long-term survival for patients with HCC who receive adjuvant or post-recurrence treatments, these data (such as transarterial chemoembolization, ablative therapy, targeting drug therapy, and so on) are equally unavailable in the SEER database. Furthermore, hepatitis B virus is the main causative factor for HCC in China, whereas 60–70% of HCC cases in the western countries can be attributed to hepatitis C virus and alcoholic hepatitis. Our SNIG model was constructed and internally validated using data of a western population, while the external validation was performed using data from an eastern population with a high prevalence of hepatitis B virus. This model should be used with caution, considering the differences in etiological background and impact on severe cirrhosis and high liver disease–related mortality. Despite these limitations, our SNIG model was built using a large population from the SEER database, presenting a distinctive opportunity to predict the OS of patients with HCC after curative-intent surgery.
In summary, we developed a web-based SNIG model for predicting OS in patients staged using the TNM 8th edition, especially in those with TNM stage I and Ⅱ HCC after curative-intent surgery. This nomogram may help clinicians and patients to predict survival more accurately. The results of the internal and external validations demonstrate the high performance and discrimination power of the model.
Acknowledgments
This work was supported in part by Fujian Provincial Natural Science Foundation (Grant number:2017J01177), and high-level hospital foster grants from Fujian Provincial Hospital (Grant number: 2019HSJJ03), Fujian province, China.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424. doi:10.3322/caac.21492
2. Forner A, Reig M, Bruix J. Hepatocellular carcinoma. Lancet. 2018;391(10127):1301–1314. doi:10.1016/S0140-6736(18)30010-2
3. Llovet JM, Bru C, Bruix J. Prognosis of hepatocellular carcinoma: the BCLC staging classification. Semin Liver Dis. 1999;19(03):329–338. doi:10.1055/s-2007-1007122
4. Kudo M, Chung H, Osaki Y. Prognostic staging system for hepatocellular carcinoma (CLIP score): its value and limitations, and a proposal for a new staging system, the Japan Integrated Staging Score (JIS score). J Gastroenterol. 2003;38(3):207–215. doi:10.1007/s005350300038
5. Minagawa M, Ikai I, Matsuyama Y, Yamaoka Y, Makuuchi M. Staging of hepatocellular carcinoma: assessment of the Japanese TNM and AJCC/UICC TNM systems in a cohort of 13,772 patients in Japan. Ann Surg. 2007;245(6):909–922. doi:10.1097/01.sla.0000254368.65878.da
6. Farinati F, Vitale A, Spolverato G, et al. Development and validation of a new prognostic system for patients with hepatocellular carcinoma. PLoS Med. 2016;13(4):e1002006. doi:10.1371/journal.pmed.1002006
7. Amin MB, Greene FL, Edge SB, et al. The eighth edition AJCC cancer staging manual: continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging. CA Cancer J Clin. 2017;67(2):93–99. doi:10.3322/caac.21388
8. Chun YH, Kim SU, Park JY, et al. Prognostic value of the 7th edition of the AJCC staging system as a clinical staging system in patients with hepatocellular carcinoma. Eur J Cancer. 2011;47(17):2568–2575. doi:10.1016/j.ejca.2011.07.002
9. Huang J, Zhang Y, Peng Z, et al. A modified TNM-7 staging system to better predict the survival in patients with hepatocellular carcinoma after hepatectomy. J Cancer Res Clin Oncol. 2013;139(10):1709–1719. doi:10.1007/s00432-013-1497-y
10. Kamarajah SK, Frankel TL, Sonnenday C, Cho CS, Nathan H. Critical evaluation of the American Joint Commission on Cancer (AJCC) 8th edition staging system for patients with Hepatocellular Carcinoma (HCC): a Surveillance, Epidemiology, End Results (SEER) analysis. J Surg Oncol. 2018;117(4):644–650. doi:10.1002/jso.24908
11. Cho CS, Gonen M, Shia J, et al. A novel prognostic nomogram is more accurate than conventional staging systems for predicting survival after resection of hepatocellular carcinoma. J Am Coll Surg. 2008;206(2):281–291. doi:10.1016/j.jamcollsurg.2007.07.031
12. Xu L, Peng ZW, Chen MS, et al. Prognostic nomogram for patients with unresectable hepatocellular carcinoma after transcatheter arterial chemoembolization. J Hepatol. 2015;63(1):122–130. doi:10.1016/j.jhep.2015.02.034
13. Shim JH, Jun MJ, Han S, et al. Prognostic nomograms for prediction of recurrence and survival after curative liver resection for hepatocellular carcinoma. Ann Surg. 2015;261(5):939–946. doi:10.1097/SLA.0000000000000747
14. Yang P, Qiu J, Li J, et al. Nomograms for pre- and postoperative prediction of long-term survival for patients who underwent hepatectomy for multiple hepatocellular carcinomas. Ann Surg. 2016;263(4):778–786. doi:10.1097/SLA.0000000000001339
15. He W, Peng B, Tang Y, et al. Nomogram to predict survival of patients with recurrence of hepatocellular carcinoma after surgery. Clin Gastroenterol Hepatol. 2018;16(5):756–764 e710. doi:10.1016/j.cgh.2017.12.002
16. Zhang XP, Gao YZ, Chen ZH, et al. An eastern hepatobiliary surgery hospital/portal vein tumor thrombus scoring system as an aid to decision making on hepatectomy for hepatocellular carcinoma patients with portal vein tumor thrombus: a multicenter study. Hepatology. 2018. doi:10.1002/hep.30490
17. Xiao Z, Yan Y, Zhou Q, et al. Development and external validation of prognostic nomograms in hepatocellular carcinoma patients: a population based study. Cancer Manag Res. 2019;11:2691–2708. doi:10.2147/CMAR.S191287
18. Marasco G, Colecchia A, Colli A, et al. Role of liver and spleen stiffness in predicting the recurrence of hepatocellular carcinoma after resection. J Hepatol. 2019;70(3):440–448. doi:10.1016/j.jhep.2018.10.022
19. Liu GM, Zeng HD, Zhang CY, Xu JW. Identification of a six-gene signature predicting overall survival for hepatocellular carcinoma. Cancer Cell Int. 2019;19(1):138. doi:10.1186/s12935-019-0858-2
20. Qiu J, Peng B, Tang Y, et al. CpG methylation signature predicts recurrence in early-stage hepatocellular carcinoma: results from a multicenter study. J Clin Oncol. 2017;35(7):734–742. doi:10.1200/JCO.2016.68.2153
21. Dong W, Yu H, Zhu YY, et al. A novel pathological scoring system for hepatic cirrhosis with hepatocellular carcinoma. Cancer Manag Res. 2020;12:5537–5547. doi:10.2147/CMAR.S223417
22. Zhou TH, Su JZ, Qin R, Chen X, Ju GD, Miao S. Prognostic and predictive value of a 15 Transcription Factors (TFs) panel for hepatocellular carcinoma. Cancer Manag Res. 2020;12:12349–12361. doi:10.2147/CMAR.S279194
23. Berardi G, Morise Z, Sposito C, et al. Development of a nomogram to predict outcome after liver resection for hepatocellular carcinoma in Child-Pugh B cirrhosis. J Hepatol. 2020;72(1):75–84. doi:10.1016/j.jhep.2019.08.032
24. Wang YY, Xiang BD, Ma L, et al. Development and validation of a nomogram to preoperatively estimate post-hepatectomy liver dysfunction risk and long-term survival in patients with hepatocellular carcinoma. Ann Surg. 2020;Publish Ahead of Print. doi:10.1097/SLA.0000000000004407
25. Mazzaferro V, Llovet JM, Miceli R, et al. Predicting survival after liver transplantation in patients with hepatocellular carcinoma beyond the Milan criteria: a retrospective, exploratory analysis. Lancet Oncol. 2009;10(1):35–43. doi:10.1016/S1470-2045(08)70284-5
26. Compton CC, Byrd DR, Garcia-Aguilar J, Kurtzman SH, Olawaiye A, Washington MK. Liver. In: Compton CC, Byrd DR, Garcia-Aguilar J, Kurtzman SH, Olawaiye A, Washington MK, editors. AJCC Cancer Staging Atlas: A Companion to the Seventh Editions of the AJCC Cancer Staging Manual and Handbook. New York: Springer New York; 2012:241–249.
27. Vickers AJ, Elkin EB. Decision curve analysis: a novel method for evaluating prediction models. Med Decis Making. 2006;26(6):565–574. doi:10.1177/0272989X06295361
28. Zhang Z, Rousson V, Lee WC, et al. Decision curve analysis: a technical note. Ann Transl Med. 2018;6(15):308. doi:10.21037/atm.2018.07.02
29. Liu T, Lin SW, Lin S, et al. Exploration of high-risk factors for pulmonary embolism in patients undergoing postoperative anti-thrombotic therapy among gynecologic oncology surgery: a retrospective study. Ann Transl Med. 2019;7(7):143. doi:10.21037/atm.2019.03.07
30. Chun YS, Pawlik TM, Vauthey JN. 8th edition of the AJCC cancer staging manual: pancreas and hepatobiliary cancers. Ann Surg Oncol. 2018;25(4):845–847. doi:10.1245/s10434-017-6025-x
31. Li HB, Zhao FQ, Zhou J. Prognostic nomogram for disease-specific survival in patients with non-metastatic ampullary carcinoma after surgery. Ann Surg Oncol. 2019;26(4):1079–1085. doi:10.1245/s10434-018-07115-8
32. Burkhart RA, Pawlik TM. Staging and prognostic models for hepatocellular carcinoma and intrahepatic cholangiocarcinoma. Cancer Control. 2017;24(3):1073274817729235. doi:10.1177/1073274817729235
33. Roayaie S, Obeidat K, Sposito C, et al. Resection of hepatocellular cancer. Hepatology. 2013;57(4):1426–1435. doi:10.1002/hep.25832
34. Hwang S, Lee YJ, Kim KH, et al. The impact of tumor size on long-term survival outcomes after resection of solitary hepatocellular carcinoma: single-institution experience with 2558 patients. J Gastrointest Surg. 2015;19(7):1281–1290. doi:10.1007/s11605-015-2849-5
35. Nathan H, Hyder O, Mayo SC, et al. Surgical therapy for early hepatocellular carcinoma in the modern era: a 10-year SEER-medicare analysis. Ann Surg. 2013;258(6):1022–1027. doi:10.1097/SLA.0b013e31827da749
36. Guerrini GP, Pinelli D, Di Benedetto F, et al. Predictive value of nodule size and differentiation in HCC recurrence after liver transplantation. Surg Oncol. 2016;25(4):419–428. doi:10.1016/j.suronc.2015.09.003
37. Pote N, Cauchy F, Albuquerque M, et al. Performance of PIVKA-II for early hepatocellular carcinoma diagnosis and prediction of microvascular invasion. J Hepatol. 2015;62(4):848–854. doi:10.1016/j.jhep.2014.11.005
38. Wang YY, Zhong JH, Xu HF, et al. A modified staging of early and intermediate hepatocellular carcinoma based on single tumour >7 cm and multiple tumours beyond up-to-seven criteria. Aliment Pharmacol Ther. 2019;49(2):202–210. doi:10.1111/apt.15074
39. Gray SH, White JA, Li P, et al. A SEER database analysis of the survival advantage of transarterial chemoembolization for hepatocellular carcinoma: an underutilized therapy. J Vasc Interv Radiol. 2017;28(2):231–237 e232. doi:10.1016/j.jvir.2016.09.022
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.