Back to Journals » Cancer Management and Research » Volume 18

A Prognostic Nomogram Combining Radiologic Emphysema and Clinical Parameters in Small Cell Lung Cancer
Authors Kim YS, Lee EC, Lee HY ![]()
Received 24 September 2025
Accepted for publication 18 January 2026
Published 28 January 2026 Volume 2026:18 565811
DOI https://doi.org/10.2147/CMAR.S565811
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Harikrishna Nakshatri
Young Saing Kim,1 Eung Chang Lee,2 Hee Young Lee3
1Division of Oncology, Department of Internal Medicine, Gil Medical Center, Gachon University College of Medicine, Incheon, Republic of Korea; 2Department of General Surgery, Seongnam Citizens Medical Center, Seongnam, Republic of Korea; 3Department of Radiology, Gil Medical Center, Gachon University College of Medicine, Incheon, Republic of Korea
Correspondence: Hee Young Lee, Department of Radiology, Gil Medical Center, Gachon University College of Medicine, 21, Namdong-daero 774 beon-gil, Namdong-gu, Incheon, 21565, Republic of Korea, Tel +82 10-9933-1605, Fax +82 32-460-3065, Email [email protected]
Purpose: Small cell lung cancer (SCLC) is an aggressive malignancy with poor survival. Existing prognostic models provide limited patient-level risk stratification and often overlook accessible clinical and imaging data. There remains a need for refined tools to support individualized prognostication in SCLC.
Patients and Methods: We retrospectively analyzed 149 SCLC patients diagnosed between 2010 and 2014, representing a pre-immunotherapy era cohort. Demographics, CT scans, and treatment details were reviewed. Emphysema burden was quantified using an AI-based automated tool that segmented the lungs and calculated the percentage of low-attenuation areas (< − 950 Hounsfield Units). Multivariate Cox regression identified predictors for overall survival (OS), informing nomogram construction. Performance was measured by Harrell’s C-index and calibration plots. Validation included bootstrap resampling and a 3:1 data split. Decision curve analysis (DCA) evaluated clinical utility.
Results: Age, emphysema, and treatment modality were independently associated with OS. The nomogram demonstrated excellent discrimination (C-index = 0.807; 95% confidence interval [CI], 0.771– 0.843) and good calibration for 1- and 3-year survival. Internal validity was high, with a bootstrap-adjusted C-index of 0.805 (95% CI, 0.779– 0.845), and performance remained robust in the validation subset (C-index = 0.740; 95% CI, 0.668– 0.812). Stratification by nomogram-derived risk quartiles significantly differentiated survival (log-rank p < 0.001). DCA demonstrated superior net clinical benefit compared to treat-all or treat-none strategies across clinically relevant thresholds.
Conclusion: This validated nomogram, based on three readily available variables, provides accurate survival predictions for patients with SCLC. It may assist clinicians in refining treatment strategies and enhancing shared decision-making. External validation is warranted.
Keywords: cox proportional hazards models, calibration, decision support techniques, risk assessment, survival analysis
Introduction
Small cell lung cancer (SCLC) represents a distinct subtype of lung cancer characterized by rapid cellular proliferation, early metastasis, and high initial responsiveness to chemotherapy and radiation therapy.1–4 Despite this sensitivity, disease progression is frequent and overall prognosis remains poor.3–7 SCLC, which comprises approximately 15% of all lung cancers worldwide, is closely associated with cigarette smoking.1,2,7
Although disease stage and performance status are well-established prognostic factors,8,9 emerging evidence suggests that additional comorbidities, particularly chronic obstructive pulmonary disease (COPD) and computed tomography (CT)-detected emphysema, have important implications for survival outcomes.10–12 Emphysema, marked by alveolar wall destruction and airspace enlargement, exacerbates pulmonary impairment and may hinder treatment tolerance.12,13
Radiologic detection of emphysema by CT is a non-invasive and reliable method for evaluating pulmonary parenchymal integrity.14,15 While extensively studied in non-small cell lung cancer (NSCLC),16,17 few models have addressed its impact in SCLC. Additionally, the aging population presents further prognostic variability due to comorbid burden and altered treatment tolerance.18,19
Nomograms have become widely utilized for risk stratification and individualized prognostic prediction in oncology.20–22 These visual tools translate complex regression models into clinically accessible formats and offer a probabilistic approach to outcome forecasting.20–22 In this study, we aim to construct a validated nomogram incorporating CT-defined emphysema, age, and treatment modality to predict overall survival (OS) in SCLC patients. We hypothesize that inclusion of radiologic parameters will significantly improve predictive accuracy and support clinical decision-making.
Materials and Methods
Study Design and Population
The present retrospective cohort study was carried out at Gachon University Gil Medical Center, a tertiary care institution located in South Korea. A total of 149 patients who were newly diagnosed with SCLC between January 2010 and December 2014 were identified using institutional pathology and imaging databases. Inclusion criteria were: (1) histologically confirmed SCLC, (2) availability of baseline chest CT imaging performed within 30 days of diagnosis, (3) complete clinical and demographic data, and (4) documented follow-up for survival status. Patients were excluded if they had a history of other malignancies or were lost to follow-up within the first month after diagnosis.
Data Collection and Variables
Electronic medical records were reviewed to extract clinical, demographic, and treatment-related information. Variables included age at diagnosis, sex, body mass index (BMI), smoking status (current, former, never), Eastern Cooperative Oncology Group (ECOG) performance status, presence of COPD, Charlson Comorbidity Index (CCI), lactate dehydrogenase (LDH) level, and cancer stage (limited vs extensive). BMI was categorized into four groups according to World Health Organization (WHO) criteria for Asian populations: underweight (<18.5 kg/m2), normal (18.5–22.9 kg/m2), overweight (23.0–24.9 kg/m2), and obese (≥25 kg/m2). Treatment strategies were categorized as chemotherapy alone, concurrent chemoradiotherapy, and supportive care, the latter of which comprised best supportive care (n = 31) and chest radiotherapy alone (n = 2). The first-line chemotherapy regimens were also recorded.
Radiologic Evaluation of Emphysema
Chest CT examinations were performed using Siemens multidetector helical scanners (SOMATOM Definition or SOMATOM Definition Flash, Siemens Healthcare, Forchheim, Germany). Images were obtained with patients in the supine position during full inspiration. The acquisition protocol included a collimation width of 1 mm, tube voltages of 120–140 kV, tube currents ranging from 75 to 350 mA, a rotation time of 0.75–1.0 s, and reconstructed slice thicknesses of 1–2 mm. Lung parenchyma was automatically segmented from chest CT images using a Python-based deep learning tool (Lungmask, v0.2.10), trained on publicly available annotated CT datasets. Emphysema burden was quantified by calculating the percentage of lung voxels with attenuation below −950 Hounsfield Units (HU) using standard thresholding techniques in Python (NumPy and SimpleITK).23,24 Emphysema was defined as a low attenuation area ≥ 6%, with high-density regions (≥ −300 HU) excluded to reduce the impact of imaging noise.25
Statistical Analysis
All statistical analyses were performed using R software (version 4.4.3). Continuous variable was presented as median with interquartile range, depending on its distribution. Categorical variables were summarized as frequencies and percentages. Baseline characteristics were compared between patients with and without emphysema using the Chi-square test or Fisher’s exact test for categorical variables, and the Student’s t-test or Mann–Whitney U-test for continuous variables.
Survival Analysis and Model Development
Univariate Cox proportional hazards regression was initially performed to examine the association between each covariate and OS. Variables with a p-value < 0.10 in the univariate analysis were considered candidates for multivariate analysis. A multivariate Cox proportional hazards model was then constructed using stepwise variable selection based on minimization of the Akaike Information Criterion (AIC) to identify independent prognostic factors. Hazard ratios (HRs) with corresponding 95% confidence intervals (CIs) were reported.
A nomogram was constructed using the final multivariate Cox model to estimate individualized probabilities of 1- and 3-year OS. The nomogram was developed using the “rms” package in R. Model performance was assessed using Harrell’s concordance index (C-index) to evaluate discrimination. The calibration of the nomogram was evaluated by comparing predicted survival probabilities with observed outcomes using calibration plots.20
Internal Validation
To evaluate the internal validity of the model, both bootstrap resampling and data-splitting techniques were employed. Bootstrap validation with 200 iterations was conducted to obtain bias-corrected estimates of model performance. For data partitioning, the entire dataset was randomly split into a training set (75%) and a validation set (25%). The model developed from the training cohort was then applied to the validation cohort to assess generalizability. Discriminative performance was quantified using the C-index and compared between training and validation sets.
Decision Curve Analysis
The clinical utility of the nomogram was evaluated using decision curve analysis (DCA), implemented through the stdca() function of the “ggscidca” package in R. DCA quantifies the net benefit of a predictive model by balancing the trade-off between true-positive results (benefit) and false-positive decisions (harm) across a range of threshold probabilities. This methodology allows comparison of the model against default strategies of treating all patients or treating none, providing insight into whether the model offers clinical value in guiding treatment decisions. To assess the statistical robustness of the model’s net benefit, 95% CI was calculated using 200 bootstrap resamples.
Results
Patient Characteristics
A total of 149 patients with histologically confirmed SCLC were included in the final analysis. The median age was 69.7 (62.7–75.1) years, and the majority were male (85.2%). Among the patients, 101 (67.8%) had CT-defined emphysema, while 48 (32.2%) did not. Table 1 summarizes the baseline characteristics of the entire cohort and stratified by training and validation sets. In the overall cohort, 67.1% were current smokers and 52.3% had COPD. The distribution of ECOG performance status was 73.2% for 0–1 and 26.8% for ≥2. Most patients (67.8%) presented with extensive-stage disease. According to the CCI, 31.5% scored 0, 30.9% scored 1, and 37.6% scored ≥2. LDH levels were elevated (≥486 U/L) in 55.7% of patients. Regarding BMI distribution, 16.1% were underweight, 43.0% had normal BMI, 20.8% were overweight, and 20.1% were obese. No statistically significant differences were observed between the training and validation sets in terms of key baseline variables including sex, age, COPD, emphysema, ECOG performance status, or cancer stage”.
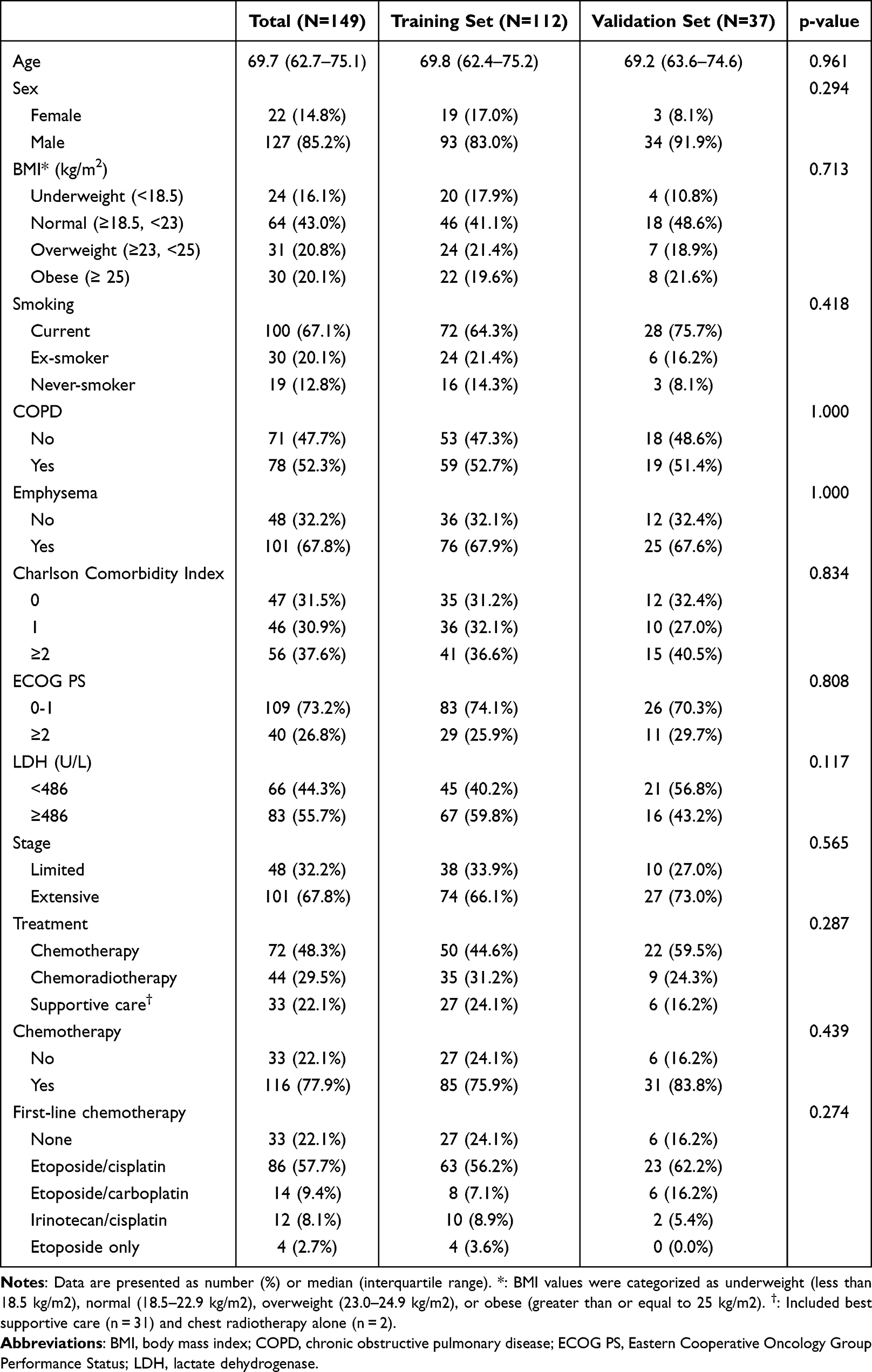 |
Table 1 Characteristics of the Study Population |
Among the study population, 72 patients (48.3%) received chemotherapy alone, 44 patients (29.5%) underwent concurrent chemoradiotherapy, and 33 patients (22.1%) received supportive care, which included best supportive care (n = 31) and chest radiotherapy alone (n = 2). Chemotherapy was administered to 116 patients (77.9%) in total. Among those treated with chemotherapy, the most common first-line regimen was etoposide plus cisplatin (n = 86), followed by etoposide plus carboplatin (n = 14), irinotecan plus cisplatin (n = 12), and etoposide monotherapy (n = 4).
Survival Analyses
The overall median survival for the entire cohort was 11.1 (95% CI, 8.7–14.2) months. In univariate Cox regression analysis, age, BMI, ECOG performance status, LDH, stage, treatment modality, and emphysema were significantly associated with OS. Full results are presented in Table 2. Kaplan–Meier analysis further demonstrated that patients with emphysema had significantly shorter overall survival compared with those without emphysema (p = 0.011), as illustrated in Figure 1.
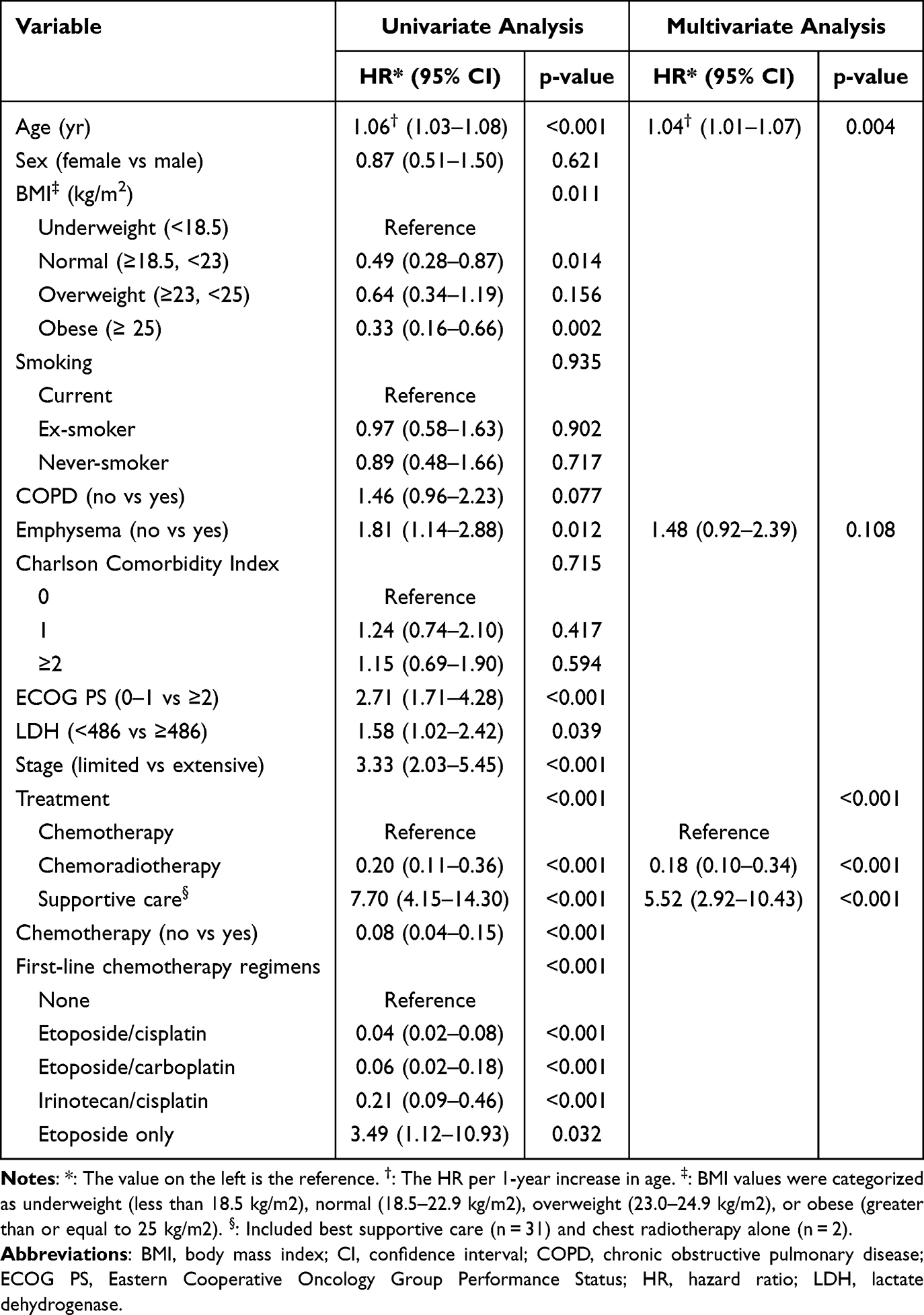 |
Table 2 Univariate and Multivariate Cox Proportional Hazards Analyses of Overall Survival |
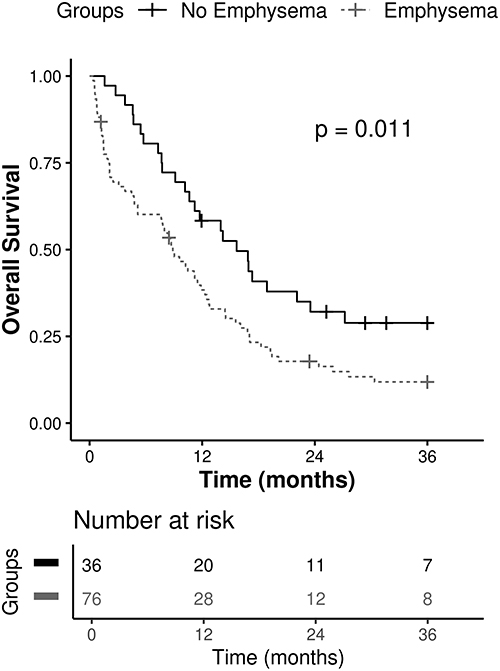 |
Figure 1 Kaplan-Meier overall survival curves according to presence of CT-defined emphysema. The solid line represents patients without emphysema, and the dotted line represents patients with emphysema. The number of patients at risk is shown below each curve. |
Multivariate Cox analysis identified older age (HR, 1.04; 95% CI, 1.01–1.07; p = 0.004), presence of emphysema (HR, 1.48; 95% CI, 0.92–2.39; p = 0.108), and treatment modality (chemoradiotherapy: HR, 0.18; 95% CI, 0.10–0.34; supportive care: HR, 5.52; 95% CI, 2.92–10.43; all p < 0.001) as independent predictors of OS. Variables such as BMI, ECOG performance status, LDH, and stage were not independently associated with survival.
Nomogram Construction and Performance
A nomogram incorporating age, emphysema status, and treatment modality was constructed to predict 1- and 3-year OS. The graphical tool allows for rapid individualized estimation of survival probabilities. Figure 2 depicts the final nomogram. Each predictor is assigned a weighted point value proportional to its hazard contribution, and the sum of points corresponds to a specific OS probability at different time intervals.
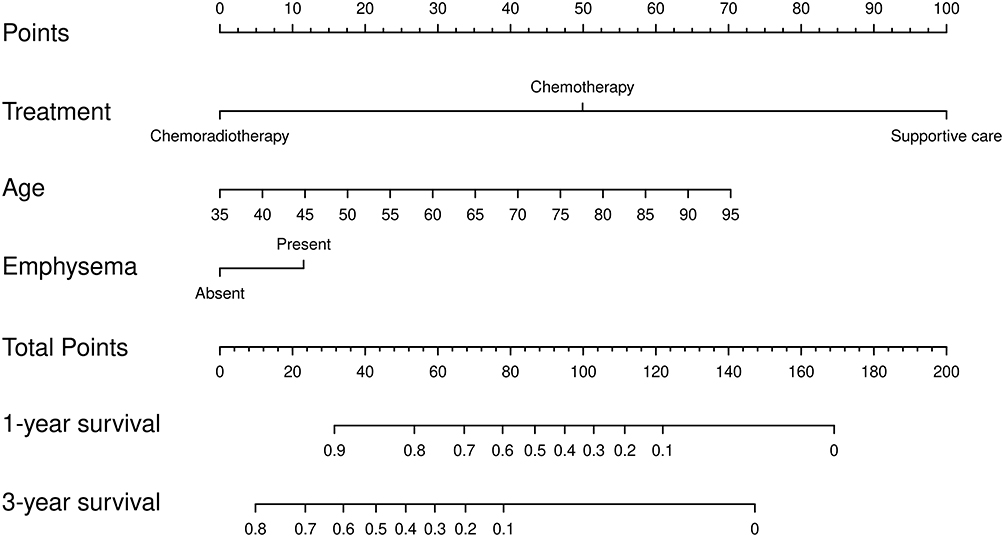 |
Figure 2 Nomogram to predict 1- and 3-year overall survival in patients with small cell lung cancer. For each variable, a vertical line is drawn to the “Points” axis to determine its score. The sum of all points corresponds to the estimated survival probability. |
The performance of the nomogram was assessed using Harrell’s C-index, which yielded a value of 0.807 (95% CI, 0.771–0.843), indicating excellent discriminatory power. Internal validation using 200 bootstrap resamples demonstrated minimal optimism, with a bias-corrected C-index of 0.805 (95% CI, 0.779–0.845). Calibration plots (Figure 3A and B) demonstrated strong agreement between predicted and observed survival probabilities at 1- and 3-year intervals, confirming the model’s reliability.
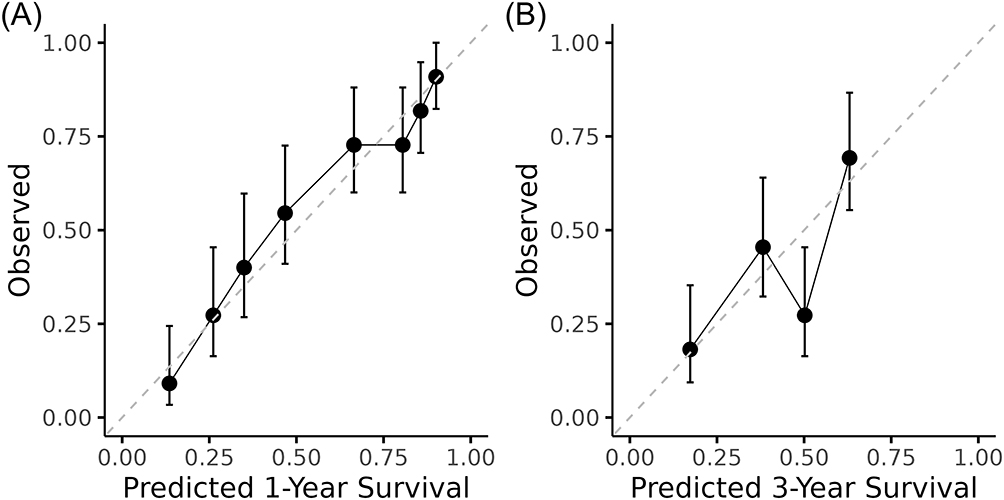 |
Figure 3 Calibration plots for the nomogram at (A) 1-year and (B) 3-year intervals. The dashed diagonal line indicates the ideal reference, and the solid line represents the predicted survival probabilities compared with the observed outcomes. Predicted and observed probabilities showed strong concordance. |
To further assess the model’s generalizability, we performed internal validation using a 3:1 data-splitting strategy. The model was trained on 75% of the cohort (n = 112) and tested on the remaining 25% (n = 37). When applied to the validation subset, the nomogram achieved a Harrell’s C-index of 0.740 (95% CI, 0.668–0.812), confirming robust predictive performance in independent internal samples. These results support the consistency and clinical applicability of the model beyond the derivation set.
The linear predictor derived from the nomogram was used to stratify patients into quartiles (Q1 to Q4) based on total risk score. Kaplan-Meier curves (Figure 4) demonstrated significant separation between the survival curves of each risk group (log-rank p < 0.001), indicating the nomogram’s utility in distinguishing between low-, intermediate-, and high-risk patients.
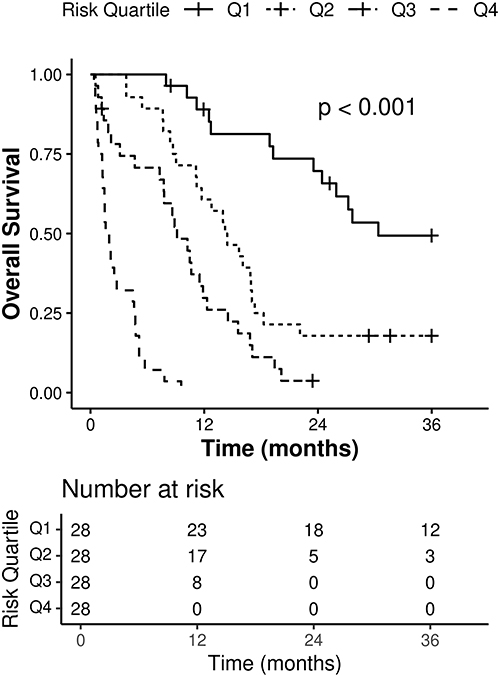 |
Figure 4 Kaplan-Meier curves stratified by risk quartile (Q1-Q4), based on the nomogram-derived linear predictor. Q1 is shown as a solid line, Q2 as a dotted line, Q3 as a dash-dotted line, and Q4 as a dashed line. The number of patients at risk is shown below each curve. Survival significantly differed across groups (P < 0.001). |
Decision Curve Analysis
Figure 5 presents the DCA of the nomogram for predicting 3-year OS in patients with SCLC. The nomogram consistently yielded greater net clinical benefit than the default strategies of treating all or none across a wide range of threshold survival probabilities, with particularly pronounced benefit between 0.1 and 0.4. Importantly, the nomogram maintained superiority over the default strategies in most other threshold ranges as well, reinforcing its applicability across varied clinical decision thresholds. Given the uniformly poor prognosis of SCLC, these findings highlight the model’s potential to guide treatment decisions even among patients with modest predicted survival. The shaded area represents the 95% CI of the net benefit, derived from 200 bootstrap iterations, underscoring the statistical robustness and reliability of the model’s performance.
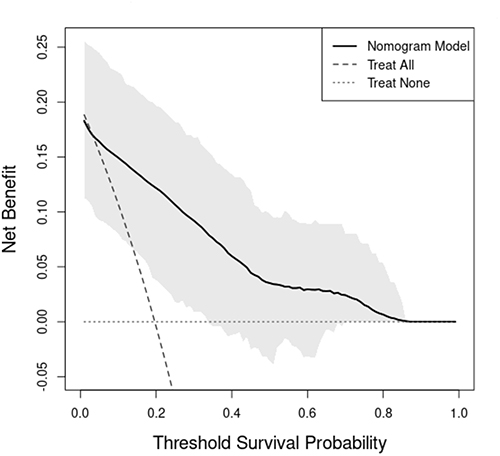 |
Figure 5 Decision curve analysis (DCA) for the 3-year survival prediction nomogram in small cell lung cancer. The x-axis indicates the threshold survival probability at which treatment would be considered; the y-axis represents the net clinical benefit. The solid black line represents the net benefit of the nomogram model, whereas the gray dashed and dotted lines reflect the “treat-all” and “treat-none” strategies, respectively. The shaded area reflects the 95% confidence interval for the net benefit of the nomogram, derived from 200 bootstrap iterations. |
Summary of Key Findings
The results demonstrate that older age, presence of emphysema, and absence of active cancer-directed therapy are strong independent predictors of poor survival in SCLC patients. The constructed nomogram provides an accurate, reproducible, and clinically useful tool for estimating individualized survival probabilities, with excellent calibration, discrimination, and decision utility. These findings support the integration of radiologic and clinical data into prognostic models to enhance patient-specific risk stratification and inform shared decision-making in SCLC care.
Discussion
In this study, we developed and internally validated a comprehensive nomogram model integrating three key clinical parameters—CT-detected emphysema, patient age, and treatment modality—to predict 1- and 3-year OS in individuals with SCLC. This model represents a pragmatic approach to risk stratification in a population characterized by poor prognosis and substantial heterogeneity in outcomes. Our findings underscore the importance of individualized prognostication that extends beyond tumor stage alone and instead incorporates physiologic and therapeutic factors.
The incorporation of emphysema as a radiologic biomarker into the prognostic model is particularly noteworthy. While emphysema is a well-known comorbidity in smokers and patients with COPD, its direct impact on survival in SCLC has not been well established. Our study demonstrated that CT-defined emphysema independently predicted worse survival, even after adjusting for COPD, performance status, and other clinical variables. This may reflect the compounded effects of impaired pulmonary reserve, increased systemic inflammation, and decreased tolerance to aggressive cancer treatment in patients with underlying emphysematous changes.12,26–29 While emphysema has been extensively studied as a prognostic factor in NSCLC,16,17 its clinical significance in SCLC remains largely unclear due to the paucity of available evidence. The present study offers preliminary support that CT-defined emphysema may have prognostic relevance in SCLC, although further validation in independent cohorts is warranted.
Age also emerged as an independent prognostic factor, in line with prior literature.19,30,31 Older patients frequently exhibit reduced physiological reserve, higher comorbidity burden, and more limited access or tolerance to aggressive oncologic treatments.32 In our cohort, even after adjusting for treatment type and performance status, advanced age consistently emerged as an independent predictor of poorer overall survival. This reinforces the need for geriatric-sensitive prognostic tools in thoracic oncology.
Treatment modality was the most powerful determinant of survival in our multivariate model. Patients who received supportive care only had significantly worse outcomes, while those treated with chemoradiotherapy exhibited the most favorable survival. This is consistent with existing clinical guidelines that advocate for combined modality therapy in patients with limited-stage disease and good performance status.33,34 Notably, chemotherapy alone also conferred a survival benefit compared to supportive care, further highlighting the central role of systemic treatment in SCLC management.
In this study, ECOG performance status showed significance in univariable analysis but did not remain an independent prognostic factor in the multivariable model. This appears to reflect its strong correlation with treatment modality and its physiologic overlap with age and CT-defined emphysema, whereby much of its explanatory effect was absorbed by other variables.
The strength of our model lies in its simplicity, interpretability, and accessibility. By limiting inputs to three routinely available clinical and radiologic parameters, we were able to construct a nomogram that does not require specialized molecular testing or extensive laboratory work-up, thereby maximizing its potential for use across diverse practice settings, including resource-limited environments. Moreover, the graphical layout of the nomogram enables rapid bedside estimation of survival probability, facilitating meaningful discussions between clinicians and patients about prognosis and treatment options.
Model performance was rigorously evaluated using multiple complementary methods. The high Harrell’s C-index (0.807) indicates strong discriminatory ability, while calibration plots confirmed the close alignment between predicted and observed outcomes across time intervals. Internal validation using bootstrap resampling showed minimal optimism, reinforcing the model’s robustness. Further, our use of data-splitting validation (3:1 ratio) provided an additional layer of methodological rigor, with the model achieving a C-index of 0.740 in the validation cohort. These results suggest that the model maintains its predictive capacity even in new, unseen data, which is a critical requirement for clinical implementation.
The DCA analysis revealed that the nomogram yielded greater net clinical benefit than either the treat-all or treat-none approach, particularly across the threshold survival probability range of 10% to 40%, with sustained net benefit observed through to the 80–90% range. This finding is clinically meaningful in the context of SCLC, a disease with uniformly poor prognosis, where even modest survival probabilities may influence treatment decisions. The model’s ability to yield benefit across a broad threshold range suggests its potential to guide clinicians in avoiding overtreatment while still selecting and targeting patients most likely to benefit from intervention. Moreover, the inclusion of 95% CI derived from bootstrap iterations reinforces the consistency and statistical robustness of the net benefit estimates. These results support the use of the nomogram as a practical tool to optimize individualized treatment strategies in high-risk oncology populations. In addition, risk stratification based on the nomogram’s linear predictor further confirmed its clinical utility, as patients in higher-risk quartiles exhibited significantly poorer survival outcomes.
The implications of our findings are multifaceted. Clinically, the nomogram can be integrated into multidisciplinary tumor board discussions to refine treatment recommendations. It may be especially valuable in borderline cases where the risks and benefits of intensive therapy are uncertain. The model may also serve as a patient communication aid, helping to set realistic expectations and support shared decision-making. From a research perspective, the model could be used to stratify patients in clinical trials or to inform risk-adapted treatment protocols.
Despite these strengths, several limitations remain to be considered. First, this study utilized data collected prior to the widespread adoption of immunotherapy for extensive-stage SCLC. While this temporal limitation may affect generalizability in high-income countries where immune checkpoint inhibitors have become part of the standard of care, access to immunotherapy remains substantially limited in many low- and middle-income countries.
Second, as a retrospective study conducted at a single institution, the generalizability of our findings may be limited. Although internal validation was robust, external validation in independent cohorts is necessary before the model can be universally adopted.
Conclusions
We developed and internally validated prognostic nomogram for SCLC that incorporates emphysema, age, and treatment modality. The model showed reasonable discrimination, acceptable calibration, and potential clinical value as indicated by decision curve analysis and risk stratification. As the predictors are routinely available in clinical practice, the tool may support individualized survival estimation and treatment planning. Nevertheless, these findings should be interpreted with caution, and prospective studies with external validation are needed to confirm the robustness and generalizability of the model.
Abbreviations
AIC, Akaike Information Criterion; BMI, body mass index; CCI, Charlson Comorbidity Index; CI, confidence interval; C-index, concordance index; COPD, chronic obstructive pulmonary disease; CT, computed tomography; DCA, decision curve analysis; ECOG, Eastern Cooperative Oncology Group; HR, Hazard ratio; HU, Hounsfield Units; NSCLC, non-small cell lung cancer; OS, overall survival; SCLC, small cell lung cancer; WHO, World Health Organization.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are derived from institutional clinical records and imaging archives. Due to patient privacy concerns and restrictions imposed by the Institutional Review Board, these data are not publicly available. De-identified data may be made available from the corresponding author upon reasonable request and with appropriate institutional approvals.
Ethical Approval and Informed Consent
This retrospective study was approved by the Institutional Review Board of GUGMC (approval number: GBIRB2017-387). The requirement for individual informed consent was waived owing to the retrospective nature of the study. All patient data were fully anonymized prior to analysis, and confidentiality was strictly maintained in accordance with institutional policies and ethical standards. The study was conducted in accordance with the Declaration of Helsinki and its subsequent amendments.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare that they have no conflicts of interest related to this work.
References
1. Wang Q, Gümüş ZH, Colarossi C, et al. SCLC: epidemiology, risk factors, genetic susceptibility, molecular pathology, screening, and early detection. J Thorac Oncol. 2023;18(1):31–12. doi:10.1016/j.jtho.2022.10.002
2. Siegel RL, Miller KD, Wagle NS, Jemal A. Cancer statistics, 2023. Ca a Cancer J Clin. 2023;73(1).
3. Saltos A, Shafique M, Chiappori A. Update on the biology, management, and treatment of small cell lung cancer (SCLC). Front Oncol. 2020;10:1074. doi:10.3389/fonc.2020.01074
4. Megyesfalvi Z, Gay CM, Popper H, et al. Clinical insights into small cell lung cancer: tumor heterogeneity, diagnosis, therapy, and future directions. Ca a Cancer J Clin. 2023;73(6):620–652. doi:10.3322/caac.21785
5. Byers LA, Rudin CM. Small cell lung cancer: where do we go from here? Cancer. 2015;121(5):664–672. doi:10.1002/cncr.29098
6. Rudin CM, Brambilla E, Faivre-Finn C, Sage J. Small-cell lung cancer. Nat Rev Dis Prim. 2021;7(1):3. doi:10.1038/s41572-020-00235-0
7. Kalemkerian GP, Loo BW, Akerley W, et al. NCCN guidelines insights: small cell lung cancer, version 2.2018. J National Compr Cancer Network. 2018;16(10):1171–1182. doi:10.6004/jnccn.2018.0079
8. Foster NR, Mandrekar SJ, Schild SE, et al. Prognostic factors differ by tumor stage for small cell lung cancer: a pooled analysis of North central cancer treatment group trials. Cancer. 2009;115(12):2721–2731. doi:10.1002/cncr.24314
9. Ma X, Zhang Z, Chen X, et al. Prognostic factor analysis of patients with small cell lung cancer: real‐world data from 988 patients. Thoracic Cancer. 2021;12(12):1841–1850. doi:10.1111/1759-7714.13846
10. Lee HY, Kim EY, Kim YS, Ahn HK, Kim YK. Prognostic significance of CT-determined emphysema in patients with small cell lung cancer. J Thoracic Dis. 2018;10(2):874. doi:10.21037/jtd.2018.01.97
11. Kang HS, Shin AY, Yeo CD, et al. A lower level of forced expiratory volume in one second predicts the poor prognosis of small cell lung cancer. J Thoracic Dis. 2018;10(4):2179. doi:10.21037/jtd.2018.03.121
12. Gao Y, Guan W, Liu Q, et al. Impact of COPD and emphysema on survival of patients with lung cancer: a meta‐analysis of observational studies. Respirology. 2016;21(2):269–279. doi:10.1111/resp.12661
13. Qi C, Sun S-W, Xiong X-Z. From COPD to lung cancer: mechanisms linking, diagnosis, treatment, and prognosis. Int J Chronic Obstr. 2022;Volume 17:2603–2621. doi:10.2147/COPD.S380732
14. Lynch DA, Austin JH, Hogg JC, et al. CT-definable subtypes of chronic obstructive pulmonary disease: a statement of the Fleischner society. Radiology. 2015;277(1):192–205. doi:10.1148/radiol.2015141579
15. Konietzke P, Wielpütz MO, Wagner WL, et al. Quantitative CT detects progression in COPD patients with severe emphysema in a 3-month interval. Eur Radiol. 2020;30(5):2502–2512. doi:10.1007/s00330-019-06577-y
16. Bishawi M, Moore W, Bilfinger T. Severity of emphysema predicts location of lung cancer and 5-y survival of patients with stage I non–small cell lung cancer. J Surg Res. 2013;184(1):1–5. doi:10.1016/j.jss.2013.05.081
17. Kinsey CM, San José Estépar R, Wei Y, Washko GR, Christiani DC. Regional emphysema of a non–small cell tumor is associated with larger tumors and decreased survival rates. Ann Am Thoracic Soc. 2015;12(8):1197–1205. doi:10.1513/AnnalsATS.201411-539OC
18. Schild SE, Zhao L, Wampfler JA, et al. Small-cell lung cancer in very elderly (≥ 80 years) patients. Clin Lung Cancer. 2019;20(4):313–321. doi:10.1016/j.cllc.2019.05.007
19. Stinchcombe TE, Fan W, Schild SE, et al. A pooled analysis of individual patient data from national clinical trials network clinical trials of concurrent chemoradiotherapy for limited‐stage small cell lung cancer in elderly patients versus younger patients. Cancer. 2019;125(3):382–390. doi:10.1002/cncr.31813
20. Iasonos A, Schrag D, Raj GV, Panageas KS. How to build and interpret a nomogram for cancer prognosis. J Clin Oncol. 2008;26(8):1364–1370. doi:10.1200/JCO.2007.12.9791
21. Balachandran VP, Gonen M, Smith JJ, DeMatteo RP. Nomograms in oncology: more than meets the eye. Lancet Oncol. 2015;16(4):e173–e180. doi:10.1016/S1470-2045(14)71116-7
22. Zhang Z, Kattan MW. Drawing nomograms with R: applications to categorical outcome and survival data. Ann Translat Med. 2017;5(10):211. doi:10.21037/atm.2017.04.01
23. Labaki WW, Martinez CH, Martinez FJ, et al. The role of chest computed tomography in the evaluation and management of the patient with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2017;196(11):1372–1379. doi:10.1164/rccm.201703-0451PP
24. Lynch DA, Moore CM, Wilson C, et al. CT-based visual classification of emphysema: association with mortality in the COPDGene study. Radiology. 2018;288(3):859–866. doi:10.1148/radiol.2018172294
25. Occhipinti M, Paoletti M, Bartholmai BJ, et al. Spirometric assessment of emphysema presence and severity as measured by quantitative CT and CT-based radiomics in COPD. Respir Res. 2019;20(1):101. doi:10.1186/s12931-019-1049-3
26. Murakami J, Ueda K, Sano F, Hayashi M, Nishimoto A, Hamano K. Pulmonary emphysema and tumor microenvironment in primary lung cancer. J Surg Res. 2016;200(2):690–697. doi:10.1016/j.jss.2015.09.004
27. Michael M, Babic B, Khokha R, et al. Expression and prognostic significance of metalloproteinases and their tissue inhibitors in patients with small-cell lung cancer. J Clin Oncol. 1999;17(6):1802. doi:10.1200/JCO.1999.17.6.1802
28. Eom JS, Song WJ, Yoo H, et al. Chronic obstructive pulmonary disease severity is associated with severe pneumonia. Ann Thoracic Med. 2015;10(2):105–111. doi:10.4103/1817-1737.151441
29. Spruit MA, Watkins ML, Edwards LD, et al. Determinants of poor 6-min walking distance in patients with COPD: the ECLIPSE cohort. Respir Med. 2010;104(6):849–857. doi:10.1016/j.rmed.2009.12.007
30. Xie D, Marks R, Zhang M, et al. Nomograms predict overall survival for patients with small-cell lung cancer incorporating pretreatment peripheral blood markers. J Thorac Oncol. 2015;10(8):1213–1220. doi:10.1097/JTO.0000000000000585
31. Wang S, Yang L, Ci B, et al. Development and validation of a nomogram prognostic model for SCLC patients. J Thorac Oncol. 2018;13(9):1338–1348. doi:10.1016/j.jtho.2018.05.037
32. Yang Y, Sun S, Wang Y, Xiong F, Xiao Y, Huang J. Development and validation of nomogram for predicting survival of elderly patients with stage I small-cell lung cancer. Bosnian J Basic Med Sci. 2021;21(5):632. doi:10.17305/bjbms.2020.5420
33. Ganti AKP, Loo BW, Bassetti M, et al. Small cell lung cancer, version 2.2022, NCCN clinical practice guidelines in oncology. J National Compr Cancer Network. 2021;19(12):1441–1464. doi:10.6004/jnccn.2021.0058
34. Dingemans A-M, Früh M, Ardizzoni A, et al. Small-cell lung cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow-up☆. Ann Oncol. 2021;32(7):839–853. doi:10.1016/j.annonc.2021.03.207
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.