Back to Journals » Journal of Inflammation Research » Volume 19
A Predictive Model for Moderate or Severe Neonatal Acute Respiratory Distress Syndrome in Extremely Preterm Infants with Premature Rupture of Membranes: Development and Internal Validation
Authors Hu Y ![]() , Li Q, Wen X, Wan C, Lang Y, Chen S, Yan L
, Li Q, Wen X, Wan C, Lang Y, Chen S, Yan L
Received 25 August 2025
Accepted for publication 21 January 2026
Published 1 March 2026 Volume 2026:19 562324
DOI https://doi.org/10.2147/JIR.S562324
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Yuhan Xing
Yuan Hu,* Qin Li,* Xiaolin Wen, Changyong Wan, Yu Lang, Sheng Chen, Ling Yan
Department of Pediatrics, The First Affiliated Hospital of Army Medical University, Chongqing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ling Yan; Sheng Chen, Department of Pediatrics, The First Affiliated Hospital of Army Medical University, Chongqing, People’s Republic of China, Email [email protected]; [email protected]
Purpose: Preterm premature rupture of membranes (PROM) is a major cause of extremely preterm birth. Intrauterine infection and inflammation markedly increase the risk of neonatal acute respiratory distress syndrome (NARDS), particularly moderate or severe cases associated with poor outcomes. This study developed and validated a prediction model for moderate or severe NARDS in this population using inflammatory biomarkers.
Patients and Methods: This single center retrospective cohort study included 243 extremely preterm infants with PROM from 2015 to 2024. The primary outcome was moderate or severe NARDS occurring within 72 hours after delivery, diagnosed according to Montreux criteria. Patients were grouped by NARDS severity. Predictive variables were screened using LASSO regression and incorporated into a multivariable logistic model to build a nomogram. Model performance was assessed through receiver operating characteristic curves (ROC), calibration plots and decision curve analysis (DCA).
Results: The primary outcome incidence was 20.2% (49/243). Multivariable analysis identified elevated C-reactive protein (CRP) (OR=1.04, 95% CI:1.01– 1.07), decreased platelet count (OR=0.99, 95% CI:0.988– 0.998), decreased albumin (OR=0.87, 95% CI:0.80– 0.95), and decreased arterial pH (OR=0.01, 95% CI:0.001– 0.041) as independent predictors. The nomogram integrating these four parameters demonstrated excellent discrimination with an area under the curve (AUC) of 0.824. Internal validation demonstrated good robustness (C-index=0.795). To enhance clinical translation, we developed an interactive web calculator for real time risk assessment to guide pediatricians’ clinical decision making. DCA established a 30% risk threshold to inform early interventions.
Conclusion: The validated model containing CRP, platelets, albumin and pH effectively identifies high risk PROM infants. The web based interface enables practical bedside application for early detection of critical cases. Patients with predicted probabilities reaching 30% should be considered for preventive lung protection measures. Additional multicenter studies are needed to verify wider applicability and enhance clinical implementation protocols.
Keywords: acute respiratory distress syndrome, extremely preterm infants, premature rupture of membranes, nomogram, biological markers
Introduction
Preterm birth is a leading cause of neonatal morbidity and long-term complications worldwide. Preterm premature rupture of membranes (PROM), particularly occurring before 32 weeks of gestation, is a critical obstetric complication that significantly contributes to preterm delivery and substantially increases the risk of adverse neonatal outcomes.1,2 Neonatal acute respiratory distress syndrome (NARDS) is a severe inflammatory lung injury characterized by increased pulmonary vascular permeability, alveolar-capillary barrier dysfunction, and reduced lung compliance, ultimately resulting in refractory hypoxemia.3,4 The incidence of NARDS is markedly higher in extremely preterm infants (gestational age <32 weeks) due to lung immaturity.3 International multicenter research data from 2022 revealed the substantial burden of NARDS in this population, with an incidence reaching 34%, markedly higher than the overall incidence in newborns (1%–5%).5 Notably, over 94% of NARDS cases occur within the first 72 hours after birth.6 This narrow time window presents significant challenges for early intervention while simultaneously underscoring the urgent need to develop early warning tools.
The causal relationship between PROM and NARDS is well established. Beyond directly precipitating preterm birth, PROM may induce a systemic inflammatory response via intrauterine infections (eg, chorioamnionitis), thereby exacerbating neonatal lung injury and increasing NARDS risk.7,8 Additionally, the oligohydramnios resulting from PROM can further compromise fetal lung development, leading to pulmonary hypoplasia and worsening postnatal respiratory distress.9 Consequently, extremely preterm infants with PROM constitute a distinct clinical subgroup who simultaneously endure the dual challenges of extreme organ immaturity and the persistent inflammatory insult associated with PROM. This unique pathophysiological context may result in fundamental differences in the mechanisms underlying NARDS compared to non-PROM infants.8 This population consequently faces more rapid disease progression and poorer clinical prognosis.
Early diagnosis of NARDS in extremely preterm infants remains challenging due to overlapping clinical manifestations with other respiratory conditions, such as neonatal respiratory distress syndrome (NRDS). Compounded by the extremely limited physiological reserve of these infants, the disease condition often deteriorates rapidly within a short period. However, traditional diagnostic approaches, which predominantly rely on clinical presentation, imaging studies, and blood gas analysis, frequently lead to substantial diagnostic delays and often miss the optimal window for intervention. From a pathophysiological perspective, the systemic inflammatory response serves as the central driving factor in NARDS. Research has demonstrated that specific inflammatory mediators including interleukins (IL-6, IL-8), tumor necrosis factor-α (TNF-α), interferon-γ (IFN-γ),10 as well as surfactant proteins (SP-B, SP-D),11 exhibit significant correlations with NARDS severity. Nevertheless, the detection of these specific biomarkers is typically complex and costly, thereby substantially restricting their application in routine clinical practice, particularly for early risk assessment. Within this context, routinely available laboratory parameters demonstrate substantial potential value in the prediction and assessment of NARDS. Among inflammatory indicators, leukocyte count, neutrophil percentage, C-reactive protein (CRP), and serum albumin levels have been confirmed to significantly correlate with disease severity, with hypoalbuminemia specifically identified as an independent risk factor for NARDS.8 Regarding blood gas parameters, the oxygenation index (OI), base excess, and arterial pH value not only reflect disease severity but also effectively predict clinical outcomes.12 Coagulation parameters such as platelet count (PLT) not only participate in the coagulation process but also reflect the magnitude of microvascular injury and systemic inflammatory status.13,14 Furthermore, other conventional indicators, including red blood cell distribution width (RDW) and serum calcium levels, can also reflect pathophysiological processes associated with NARDS from different perspectives.4,14 The integrated application of these indicators can generate synergistic effects through multidimensional evaluation, theoretically capable of significantly enhancing the accuracy of NARDS prediction.
While previous studies have established several predictive models for NARDS and demonstrated their predictive performance,4,13–15 these existing models confront a crucial clinical translation bottleneck when applied to extremely preterm infants with PROM. The current knowledge gap does not lie in unawareness of these indicators’ existence, but rather in how to systematically identify and validate the core combination of predictive factors that most accurately predict the progression to moderate or severe NARDS in this specific population. Therefore, the core innovative focus of our study is not the discovery of novel biomarkers, but rather commitment to addressing a central translational medicine challenge.This study aims to develop a specialized predictive tool for this high-risk subgroup by transforming readily available clinical indicators. Specifically, we employ modern variable selection techniques and plan to create an online web application to facilitate point of care risk assessment. This approach seeks to enable early intervention and ultimately improve clinical outcomes for this vulnerable population.
Material and Methods
Study Participants
This retrospective cohort study was conducted at the First Affiliated Hospital of Army Medical University (Chongqing, China). We screened the medical records of all extremely preterm infants admitted to our neonatal intensive care unit (NICU) between January 2015 and December 2024. The study cohort specifically comprised infants who met the diagnostic criteria for PROM. The institutional ethics committee approved this study (approval number: BKY2025174) and granted a waiver of informed consent due to the retrospective nature of the research.
The inclusion criteria were: (1) preterm infants with gestational age <32 weeks; (2) presence of PROM; (3) hospital admission within 1 hour after birth. Exclusion criteria included: (1) major chromosomal abnormalities (n=2); (2) death or withdrawal of life sustaining treatment within 24 hours after birth (n=28); (3) congenital malformations or developmental disorders affecting respiratory function (eg, complex congenital heart disease, congenital diaphragmatic hernia) (n=7); (4) incomplete clinical data (n=8). A total of 243 patients were included in the final analysis (see the participant flow diagram in the Results section).
The proposed prediction model was designed to incorporate up to 4 key predictive variables. The sample size was estimated a priori using the widely adopted “10 events per variable” (EPV) rule for developing stable logistic regression models. Based on this rule, a minimum of 4 variables × 10 EPV = 40 positive events (ie, cases of moderate or severe NARDS) is required. Assuming a conservative event rate of 20% based on our institutional experience, the minimum total sample size was calculated as 40 / 0.20 = 200 cases. Our final cohort comprised 243 patients, with 49 observed positive events, which not only satisfies but exceeds the minimum requirement.
Definitions and Strategy for Case Grouping
Diagnosis and severity classification of NARDS were based on the 2017 Montreux criteria.16 Two senior NICU physicians independently reviewed all medical records for NARDS diagnosis. In cases of disagreement, a third senior physician made the final determination.
To align with the primary clinical objective of identifying infants at highest risk for clinical deterioration, we implemented a binary grouping strategy: (1) the moderate/severe NARDS group: this group encompassed infants diagnosed with both moderate and severe NARDS according to the Montreux criteria (OI ≥8). This grouping is clinically justified because both moderate and severe NARDS typically necessitate advanced respiratory support and are associated with higher mortality. This approach specifically targets the identification of cases that represent the most significant therapeutic challenge and consume the most clinical resources. (2) the mild/no NARDS group: this group combined infants with mild NARDS (OI 4-<8) and those without NARDS, given that their management strategies are often similar and require fewer resources.
Data Collection
To ensure reproducibility and data quality, a standardized and auditable data collection process was implemented. Data were extracted electronically from our hospital’s clinical databases. The collection was performed by two dedicated research members of our team. To mitigate error, the verification procedure entailed two steps: an initial electronic extraction and a subsequent manual review of a randomly selected 10% of the records by a second researcher. Inconsistencies were resolved by consensus with a third senior clinician. The following data were collected for all neonates: (1) basic information: gestational age, sex, birth weight; (2) prenatal factors: gestational hypertension, gestational diabetes mellitus, intrahepatic cholestasis of pregnancy, placental disorders (including placental abruption and placenta previa), meconium-stained amniotic fluid (MASF), chorioamnionitis, mode of delivery, duration of PROM; (3) postnatal factors: 1-minute Apgar score, 5-minute Apgar score, presence of birth asphyxia; (4) laboratory data: given the highest incidence of NARDS within the first 3 days after birth, laboratory data from the first 3 days of hospitalization were analyzed, including: blood gas analysis: pH, pCO2, pO2, lactate; complete blood count: WBC, absolute neutrophil count (ANC), hemoglobin (HGB), RDW, PLT, mean platelet volume (MPV), platelet distribution width (PDW); other biochemical markers: albumin, CRP, procalcitonin (PCT), lactate dehydrogenase (LDH); complications: presence of NRDS, early-onset sepsis (EOS), pulmonary hypertension (PPHN), pulmonary hemorrhage, grade III–IV intraventricular hemorrhage (IVH).
Statistical Analysis
Our statistical analysis proceeded according to a predetermined stepwise plan to ensure robustness and minimize overfitting. All statistical analyses were conducted using R software (version 4.2.2), with two-tailed tests and p<0.05 considered statistically significant.
Descriptive Statistics: We presented continuous variables that followed a normal distribution as the mean ± standard deviation  and used independent samples t-tests to compare them. For continuous variables that were not normally distributed, we used the median (interquartile range) [M (P25, P75)] and analyzed them with Mann–Whitney U-tests. Categorical variables were expressed as counts (percentages) [n (%)] and we used either χ2-tests or Fisher’s exact tests to compare them, opting for the latter when expected cell counts dipped below 5.
and used independent samples t-tests to compare them. For continuous variables that were not normally distributed, we used the median (interquartile range) [M (P25, P75)] and analyzed them with Mann–Whitney U-tests. Categorical variables were expressed as counts (percentages) [n (%)] and we used either χ2-tests or Fisher’s exact tests to compare them, opting for the latter when expected cell counts dipped below 5.
- Variable Selection: to address multicollinearity and identify the most parsimonious set of predictors from the high-dimensional candidate variables, we employed the least absolute shrinkage and selection operator (LASSO) regression with 10-fold cross-validation to select the optimal predictors.
- Model Building: the variables selected by LASSO were entered into a multivariable logistic regression model to generate the final prediction nomogram.
- Model Validation: the model’s performance was rigorously evaluated through: (1) receiver operating characteristic (ROC) curve analysis with area under the curve (AUC) calculation to evaluate discriminative ability; (2) calibration curves to assess agreement between predicted probabilities and observed values; (3) bootstrap resampling (1000 replicates) for internal validation, calculating the corrected C-index to evaluate model stability; and (4) decision curve analysis (DCA) to assess clinical net benefit across various risk thresholds, providing reference for making clinical decision.
- Clinical Translation: the final model was translated into an interactive web nomogram, enabling clinicians to obtain individualized risk predictions instantly at the bedside.
- Ethical Considerations: all data were fully anonymized prior to analysis by removing all personal identifiers and assigning unique study codes, ensuring participant confidentiality.
Results
Comparison of Baseline Characteristics and Laboratory Parameters
This retrospective study included 243 extremely preterm infants with PROM, stratified into a moderate/severe NARDS group (n=49) and a mild/no NARDS (n=194) group based on NARDS severity (Figure 1). Baseline analysis revealed no significant differences in sex distribution or cesarean delivery rate (p>0.05). However, the moderate/severe NARDS group exhibited significantly lower gestational age (203 vs 213 days) and birth weight (1219±390 g vs 1409±320 g, p<0.01), along with reduced Apgar scores. Perinatal complications analysis showed comparable rates of gestational hypertension, gestational diabetes mellitus, intrahepatic cholestasis, placental abnormalities, MASF, and PROM duration (p>0.05). Notably, the moderate/severe NARDS group had higher incidences of chorioamnionitis (42.9% vs 25.8%, p=0.019) and neonatal asphyxia (16.3% vs 5.2%, p=0.013). Laboratory findings demonstrated significantly lower pH, hemoglobin, platelet count, and serum calcium (p<0.05), alongside elevated lactate, RDW, CRP, PCT, and LDH levels in moderate/severe NARDS cases. (Table 1).
 |
Table 1 Comparison of Baseline Characteristics and Laboratory Parameters Between the Two Groups |
 |
Figure 1 Participant flow diagram for the study cohort. |
Comparison of Comorbidities Between Groups
As shown in Table 2, the moderate/severe NARDS group demonstrated significantly higher rates of comorbidities compared to those mild/no NARDS. The moderate/severe NARDS group exhibited markedly increased incidences of NRDS (93.9% vs 56.7%), EOS (32.7% vs 8.2%), PPHN (46.9% vs 0.5%), pulmonary hemorrhage (36.7% vs 3.1%), and severe IVH (Grade III–IV; 42.9% vs 9.8%). These findings highlight that NARDS in preterm infants is strongly associated with a substantially elevated risk of complications that are life threatening.
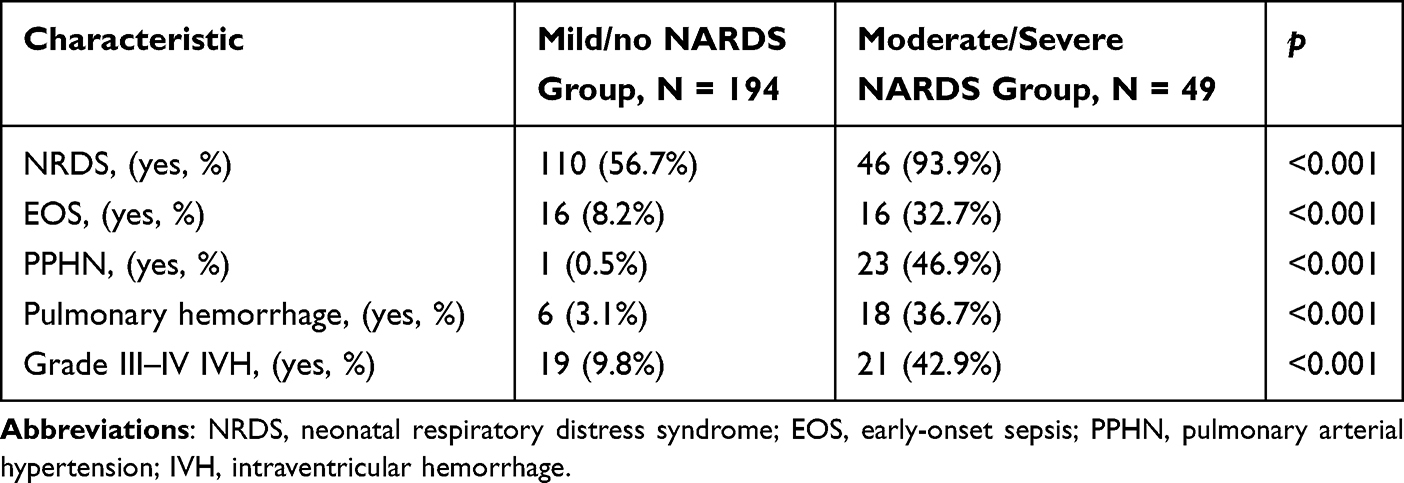 |
Table 2 Comparative Analysis of Comorbidities Between the Two Groups |
Elevated CRP and Reduced Platelet, Albumin, and pH as Independent Predictors of Moderate or Severe NARDS
All variables from Table 1 were subjected to LASSO regression analysis, with the optimal λ value determined through 10-fold cross-validation (minimum error ± 1 standard deviation). As illustrated in Figure 2, the coefficient trajectory and error curves identified four candidate predictors. Subsequent multivariate logistic regression analysis confirmed that elevated CRP (OR=1.04, 95% CI: 0.80–0.095, p=0.002), decreased platelet count (OR=0.99, 95% CI: 0.99–1.00, p=0.016), reduced albumin (OR=0.87, 95% CI: 0.80–0.95, p=0.002), and lower pH (OR=0.01, 95% CI: 0.00–0.041, p=0.013) were independent predictive factors for moderate or severe NARDS (Table 3). The final predictive model was formulated as: ln(P/1-P) = 34.739–4.323 × pH - 0.007 × PLT (×109/L) - 0.135 × Albumin (g/L) + 0.036 × CRP (mg/dL).
 |
Table 3 Results of Multivariate Logistic Regression |
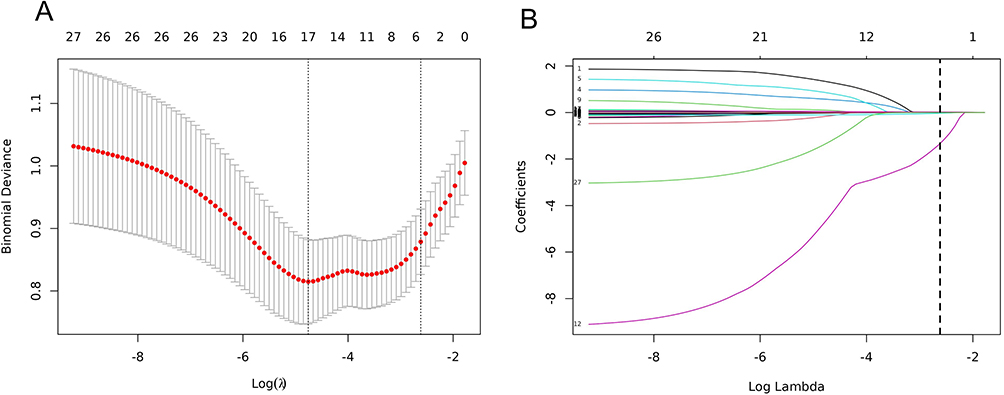 |
Figure 2 LASSO binary logistic regression model for the selection of clinical indicators. (A) Tuning parameter (lambda) selection in the LASSO model via 10-fold cross-validation. The dotted vertical line is drawn at the optimal lambda value (lambda.min) that gives the most regularized model within one standard error of the minimum binomial deviance. (B) LASSO coefficient profiles of the 22 candidate predictors. The vertical line indicates the lambda.min value where the four non-zero coefficients (pH, platelets, albumin, CRP) were selected. |
Development of a Nomogram Model for Predicting Moderate or Severe NARDS in Extremely Preterm Infants with PROM
Multivariate logistic regression analysis revealed associations between CRP, PLT, albumin, and pH with moderate or severe NARDS. A predictive model incorporating these four factors was developed, and the results of the regression analysis were visualized using a nomogram (Figure 3). As an example case in which the nomogram was applied, a premature infant with PROM had the following laboratory parameters: pH 7.2, platelet count 140×109/L, albumin 25 g/L, and CRP 30 mg/L. The predictive variables produced the following number of points in the nomogram model: pH: 32 points; platelet count: 39 points; albumin: 50 points; CRP: 20 points. Therefore, this patient had a total score of 141 points. Corresponding to the total score at the bottom of the chart, the probability of moderate or severe NARDS was approximately 55%.
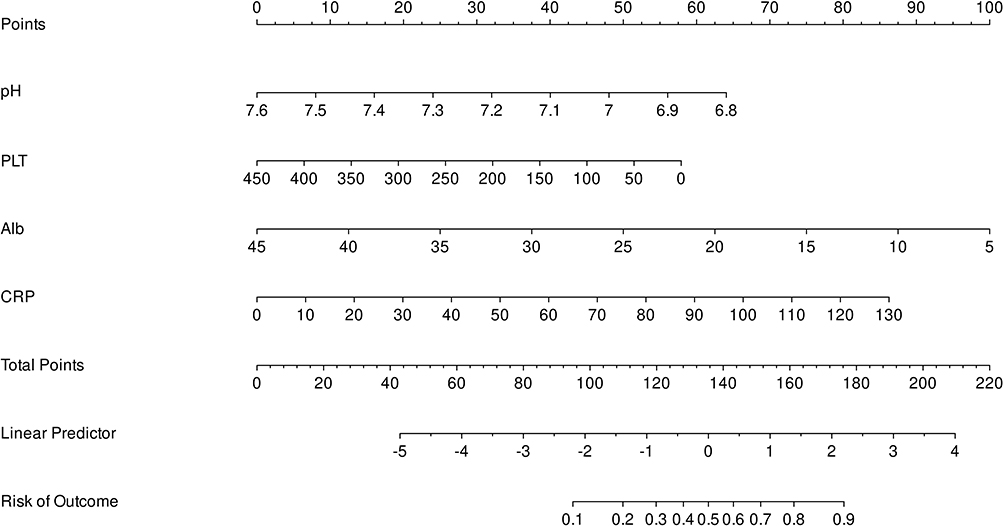 |
Figure 3 Predictive nomogram for moderate/severe NARDS in extremely premature infants with PROM. The nomogram enables clinicians to assign points for each of the four predictor variables. The total points correspond to the predicted probability of moderate-to-severe NARDS on the bottom scale. Abbreviations: PROM, premature rupture of membranes; PLT, platelet; Alb, albumin; CRP, C-reactive protein. |
Validation of the Nomogram Model
The predictive performance of individual indicators and the integrated model was evaluated through ROC curve analysis. As shown in Figure 4, the AUC values for pH, PLT, Albumin, and CRP were 0.695, 0.700, 0.712, and 0.726 respectively, while the combined predictive model demonstrated superior discriminative ability in the development cohort (AUC=0.824, 95% CI: 0.756–0.892), where the confidence interval excluding 0.5 with a narrow range indicated statistical significance. Further internal validation using bootstrap resampling (1000 replicates) yielded a C-index of 0.795, with excellent concordance between the original and corrected calibration curves (Figure 5A), confirming model robustness. The DCA indicated that the model provides a positive net benefit across a broad range of threshold probabilities (0.1–0.8), with a stable maximum clinical benefit observed between 0.20 and 0.40. Based on DCA, we identified a threshold probability of 30% as a pragmatic cutoff for clinical decision-making. (Figure 5B).
 |
Figure 4 Comparison of ROC curves for each predictor and prediction model. (A) each predictor; (B) prediction model. Abbreviations: PLT, platelet; Alb, albumin; CRP, C-reactive protein. |
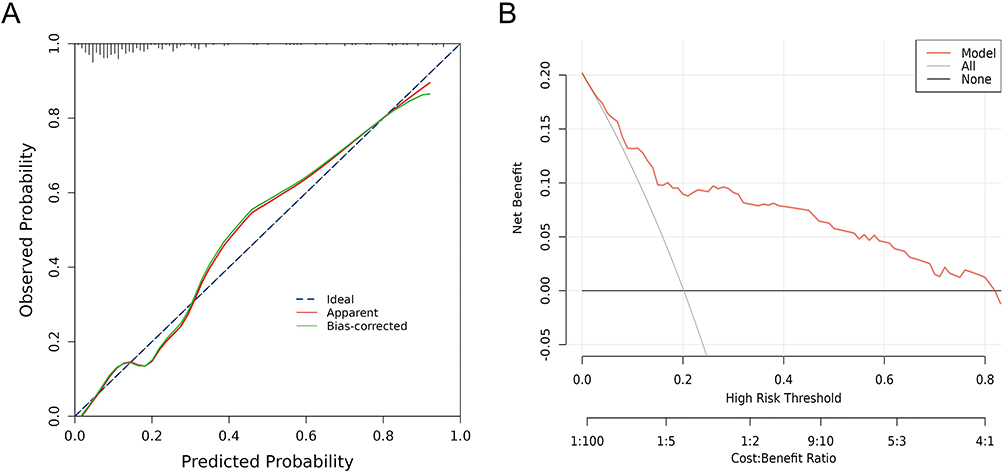 |
Figure 5 Validation and evaluation of prediction model. (A) The calibration curve for the nomogram model, the dotted line represents the performance of the model. The diagonal line represents the ideal prediction. (B) The DCA curve for the nomogram model, a standardized net risk is showed on the y-axis, while risk thresholds and cost-effectiveness ratios are showed on the x-axis. |
Sensitivity Analysis and Independence from EOS
To explicitly verify that the model’s predictive efficacy is independent of EOS, which shares overlapping inflammatory features with NARDS, we performed two additional analyses. First, we conducted a sensitivity analysis by reconstructing the logistic regression model in an EOS-negative subgroup (excluding all neonates with confirmed or clinical diagnosis of EOS, n=211). As shown in Table 4, the four core predictors (pH, PLT, albumin, CRP) remained statistically significant with stable OR. Second, we constructed an adjusted model using the entire cohort but including EOS status as a covariate. In this adjusted model (Table 5), the four original core predictors retained their high statistical significance (eg, the adjusted OR for CRP was 1.04, 95% CI: 1.01–1.06).
 |
Table 4 Results of Multivariate Logistic Regression Analysis in the Subgroup of Neonates without EOS |
 |
Table 5 Results of Multivariate Logistic Regression Analysis for Predicting Moderate or Severe NARDS Adjusted for EOS Status |
Implementation of the Web Calculator
To facilitate clinical application of our prediction model, we developed an interactive web calculator (Supplementary Figure 1). This online tool allows clinicians to input the four key variables identified in our model: pH, platelet count, albumin, and CRP. The web application automatically computes the total risk score and displays the corresponding probability of moderate or severe NARDS.
Discussion
ARDS represents a severe pulmonary disorder characterized by extensive damage to alveolar epithelial and vascular endothelial cells, leading to non-cardiogenic pulmonary edema, ventilation/perfusion mismatch, decreased lung compliance, and profound hypoxemia.17 In neonates, particularly extremely preterm infants, these pathological changes may be more pronounced due to immature lung architecture and underdeveloped defense mechanisms. Extremely preterm infants with PROM face elevated NARDS risk, likely attributable to intrauterine infection, inflammatory exposure, and developmentally immature immune systems.18,19 In this study, we developed and validated a novel nomogram for predicting moderate or severe NARDS risk in extremely preterm infants with PROM. To our knowledge, this represents the first specifically designed and validated predictive model for ARDS in this high-risk population. Through LASSO regression and multivariate logistic analysis, we identified four independent predictors: elevated CRP, decreased platelets, reduced albumin, and lower arterial pH.
CRP emerged as a key inflammatory predictor in our model. CRP is an acute phase protein; its level can surge up to 1000-fold during infection or inflammation.20 Although previous studies have not explicitly included CRP as an independent predictor in nomogram models for NARDS, its association with NARDS pathophysiology is evident. Mohammadi et al3 demonstrated that NARDS can be triggered by both direct and indirect inflammatory exposures, all of which are typically accompanied by significant inflammatory responses. Research by You et al8 highlighted EOS as a major risk factor for NARDS, with CRP serving as a key biomarker for diagnosing and monitoring sepsis. Mechanistically, CRP activates the complement system and enhances the release of inflammatory cytokines such as IL-1β, IL-6, and TNF-α, which further exacerbate pulmonary inflammation.3,20 Therefore, in extremely preterm infants with PROM, intrauterine infection and inflammatory exposure may lead to marked CRP elevation, which not only reflects the inflammatory status but also actively participates in the pathogenesis of NARDS.
Platelet count was another significant predictor in our model. Platelets play a pivotal role in maintaining vascular integrity and participating in inflammatory responses. Our findings align with previous research: Yu et al13 incorporated platelet count in their NARDS nomogram for neonates with pneumonia, while Shen et al14 similarly included it in their NARDS prediction model for meconium aspiration syndrome neonates. Wang et al’s systematic review demonstrated significant associations between low platelet counts and poorer outcomes in adult ARDS patients.21 The pathophysiological significance of thrombocytopenia in our cohort is multifactorial: on one hand, platelets interact with neutrophils, forming platelet-neutrophil aggregates that promote inflammatory factor release and microthrombi formation, thereby exacerbating pulmonary microcirculatory dysfunction,22–24 on the other hand, bioactive substances released by platelets can directly increase the permeability of alveolar epithelial and endothelial cells.22 They may also affect coagulation balance and pathogen clearance, further increasing pulmonary microcirculatory dysfunction and the risk of infection.24 For PROM extremely preterm infants, thrombocytopenia may simultaneously reflect the severity of infectious and non-infectious inflammatory responses, as well as the abnormal activation of the coagulation system, all of which are important mechanisms in the pathogenesis of NARDS.
Our research demonstrates that low albumin levels are an independent predictor of severe NARDS in extremely premature infants with PROM. Albumin is a vital protein in maintaining plasma oncotic pressure and acting as an antioxidant defence. The work of You et al has clearly shown that low serum albumin levels are an independent risk factor for NARDS resulting from EOS.8 A further study highlighted a significant correlation between low albumin levels and the incidence of NARDS in neonates with pneumonia. This study also demonstrated a dose-response relationship; for each 1 g/L increase in albumin concentration, the risk of NARDS was reduced by 17% (OR = 0.83, 95% CI 0.75–0.91, p < 0.001).25 Several potential mechanisms could explain this correlation: in NARDS, reduced albumin levels cause a decline in plasma oncotic pressure, facilitating fluid leakage into the pulmonary interstitium and alveoli. This leads to proteinaceous pulmonary oedema, impairing gas exchange and worsening respiratory distress. Furthermore, albumin leaking into the alveoli competes with pulmonary surfactant at the air-liquid interface, reducing its ability to lower surface tension. This results in alveolar collapse and reduced pulmonary compliance. Moreover, albumin functions as a crucial free radical scavenger; its deficiency renders the lungs more vulnerable to oxidative stress-related damage, thereby exacerbating inflammation-mediated lung injury. Finally, diminished albumin levels may impair its ability to bind and neutralise inflammatory mediators, leading to increased pathological effects of pro-inflammatory cytokines (such as TNF-α, IL-6), thereby further contributing to the development of NARDS.25–27 These findings indicate that monitoring and improving albumin levels in extremely premature infants could be of significant clinical value in preventing NARDS.
Our research establishes that a reduced arterial blood pH is another independent predictor. Blood pH is a crucial indicator of the body’s acid-base balance, and abnormal levels typically signify significant physiological imbalances. Newborns, particularly those born extremely preterm, have underdeveloped respiratory and circulatory systems, making them less tolerant of hypoxia and acidosis. When these newborns experience acute respiratory distress, their lungs’ ability to exchange gases is compromised, leading to carbon dioxide retention and subsequent respiratory acidosis. Concurrently, severe oxygen deprivation and inadequate tissue perfusion can increase anaerobic metabolism, resulting in lactic acid production and metabolic acidosis. Prior research indicates that acidosis is a significant indicator of poor prognosis in adult ARDS patients.28 Although fewer studies have focused on neonates, evidence suggests that acidosis is linked to a higher risk of IVH (OR=2.27) and, in conjunction with sepsis, increases the risk of mortality.29 Furthermore, severe metabolic acidosis in premature infants is associated with the development of bronchopulmonary dysplasia.30 Therefore, a reduced pH may also serve as an early indicator of underlying respiratory dysfunction. Acidosis can exacerbate inflammatory responses by activating acid-sensing ion channel 1a (ASIC1a), potentially contributing to alveolar-capillary barrier dysfunction.31 Additionally, carbonic anhydrase IX (CA IX) may worsen ARDS lung injury by affecting pulmonary bacterial clearance and vascular permeability during metabolic acidosis.32 In extremely premature infants, a reduced pH can be attributed to several factors, including placental insufficiency, inadequate tissue perfusion, and immature acid-base buffering systems, all of which collectively elevate the risk of NARDS.
Our study presents several unique strengths compared to other predictive models for NARDS. Primarily, we concentrated on a particularly vulnerable group: extremely preterm infants with PROM. Prior research has often involved general neonatal populations or specific conditions like meconium aspiration syndrome. Furthermore, we chose predictors that are standard laboratory measurements, readily available and inexpensive, thereby enhancing the model’s utility. Thirdly, our predictors encompass various dimensions, including inflammatory response (CRP), coagulation function (platelets), nutritional status (albumin), and acid-base balance (pH), providing a more comprehensive reflection of the complex pathophysiology of NARDS.
We noted that the predictive factors included in this model, such as CRP and platelets, are also classic markers of EOS. This is not an accident, since intrauterine infection and resulting EOS are the most common triggers of NARDS in extremely preterm infants with PROM.7,8 Therefore, the changes in these markers collectively depict a continuous pathophysiological process from infection and systemic inflammation to end-organ lung injury. A critical challenge in using inflammatory markers for NARDS prediction is distinguishing it from EOS. Our sensitivity analysis and adjusted models confirmed that the association between these markers and NARDS is independent of EOS status.
Furthermore, the model’s specificity for predicting lung injury, rather than just infection, is enhanced by the integration of parameters beyond general inflammation. Specifically, we observed a significant difference in PCT levels between the moderate/severe and mild/no NARDS groups in our baseline data. This finding suggests a combinatorial approach in clinical practice: significantly elevated PCT levels should raise high suspicion for EOS; however, in cases where PCT levels are equivocal or comparable, our model effectively stratifies the specific risk of severe lung injury. In this context, the model serves as a valuable risk stratification tool, prompting clinicians to initiate more aggressive respiratory support and lung-protective strategies in high-risk neonates.
To facilitate the clinical translation of our findings, we developed an interactive web nomogram, enabling clinicians to obtain individualized risk predictions instantly at the bedside. Based on DCA, we identified a threshold probability of 30% as a pragmatic cutoff for clinical decision-making. Infants with a predicted risk ≥30% should be considered for early preventive lung protective ventilation strategies, intensified monitoring, and preparedness for advanced respiratory support. This threshold transforms the statistical model into a practical decision-support tool for NICU clinicians.
This research has several notable constraints. To begin with, as a retrospective analysis conducted at a single institution, the restricted sample pool and relatively small case volume could lead to selection bias, potentially compromising how broadly these results can be applied. Second, constrained by the retrospective design, we were limited to using routine laboratory results as study variables and were unable to incorporate important clinical data, such as ventilator settings and imaging characteristics, which could diminish the model’s comprehensiveness. Third, while we developed a multi-parameter predictive model, we lacked an external validation cohort to assess its applicability across different healthcare institutions. Future studiesshould focus on prospective, multi-center studies with larger sample sizes to refine the predictive framework.
Conclusion
In summary, we developed and validated a practical prediction model for moderate/severe NARDS in extremely preterm infants with PROM. The model’s strength lies in its use of four readily available laboratory markers (CRP, platelets, albumin, pH) that capture the core pathophysiology from systemic inflammation to end-organ failure. Its clinical application is facilitated by an interactive web calculator, which allows for instant bedside risk assessment. For clinical implementation, we propose using a 30% probability threshold derived from DCA. Clinically, this model serves as a decision-support tool, prompting clinicians to initiate early, targeted interventions—such as lung-protective ventilation and intensified monitoring—for infants identified as high-risk. This tool addresses a critical gap by enabling early, evidence-based risk stratification, which is crucial for initiating timely support and potentially improving outcomes in this vulnerable population.
Data Sharing Statement
Due to privacy and ethical considerations, the dataset used in this study cannot be made publicly available. However, the study protocol and detailed statistical analysis methods can be provided upon reasonable request. Interested researchers may contact the corresponding author for access to these materials, subject to approval and compliance with relevant data protection regulations.
Ethics Approval and Informed Consent
This research adhered to the ethical guidelines established by the First Affiliated Hospital of Army Medical University (Ethics Approval No. BKY2025174), as well as national regulatory standards and the principles outlined in the 1964 Helsinki Declaration and its subsequent revisions. Participant anonymity and data confidentiality were strictly maintained throughout the investigation. Due to the retrospective design of this study, obtaining informed consent from participants was not required by the institutional review board.
Acknowledgments
We thank the support, cooperation, and trust of patients and their families.
Author Contributions
Yuan Hu: conceptualization, formal analysis, methodology, software, visualization, writing – original draft; Qin Li: data curation, investigation, project administration, writing – original draft; Xiaolin Wen: investigation, methodology, validation, writing – review and editing; Changyong Wan: data curation, investigation, writing – review and editing; Yu Lang: data curation, investigation, writing – review and editing; Sheng Chen: conceptualization, methodology, writing – review and editing; Ling Yan: conceptualization, project administration, writing – review and editing. All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by grants from the Chongqing Municipal Health Commission Medical Research Project (Project number: 2023WSJK039) and Chongqing Maternal and Neonatal Critical Care Program (Project number: 41561Z322).
Disclosure
No financial or non-financial benefits have been received or will be received from any party related directly or indirectly to the subject of this article. The authors have no conflicts of interest to declare.
References
1. Seravalli V, Colucci C, Di Cencio C, Morucchio A, Barsanti F, Di Tommaso M. Latency to delivery and incidence of adverse obstetric and perinatal outcomes in preterm premature rupture of membranes before 32 weeks. Arch Gynecol Obstet. 2025;311(6):1569–13. doi:10.1007/s00404-025-07970-3
2. American College of Obstetricians and Gynecologists. Prediction and prevention of spontaneous preterm birth: ACOG practice bulletin, number 234. Obstet Gynecol. 2021;138(2):e65–e90. doi:10.1097/AOG.0000000000004479.
3. Mohammadi A, De Luca D, Gauda EB. Characteristics, triggers, treatments, and experimental models of neonatal acute respiratory distress syndrome. Am J Physiol Lung Cell Mol Physiol. 2025;328(4):L512–L525. doi:10.1152/ajplung.00312.2024
4. Shen L, Cai N, Wan S, Chen S. Development and validation of a predictive model for early diagnosis of neonatal acute respiratory distress syndrome based on the Montreux definition. Front Pediatr. 2023;11(2):1276915. doi:10.3389/fped.2023.1276915
5. De Luca D, Tingay DG, van Kaam AH, et al. Epidemiology of neonatal acute respiratory distress syndrome: prospective, multicenter, international cohort study. Pediatr Crit Care Med. 2022;23(7):524–534. doi:10.1097/PCC.0000000000002961
6. Chen L, Li J, Shi Y. Clinical characteristics and outcomes in neonates with perinatal acute respiratory distress syndrome in China: a national, multicentre, cross-sectional study. EClinicalMedicine. 2023;55:101739. doi:10.1016/j.eclinm.2022.101739
7. Whitney JE, Lee IH, Lee JW, Kong SW. Evolution of multiple omics approaches to define pathophysiology of pediatric acute respiratory distress syndrome. ELife. 2022;11:e77405. doi:10.7554/eLife.77405
8. You T, Zhou YR, Liu XC, Li LQ. Risk factors and clinical characteristics of neonatal acute respiratory distress syndrome caused by early onset sepsis. Front Pediatr. 2022;10:847827. doi:10.3389/fped.2022.847827
9. Doktor F, Antounians L, Figueira RL, Khalaj K, Duci M, Zani A. Amniotic fluid stem cell extracellular vesicles as a novel fetal therapy for pulmonary hypoplasia: a review on mechanisms and translational potential. Stem Cells Transl Med. 2025;14(1):szae095. doi:10.1093/stcltm/szae095
10. Wu Y-Q, Ding Y-J. Overexpressed microRNA-615-3p promotes progression of neonatal acute respiratory distress syndrome by inhibiting differentiation of mesenchymal stem cells to alveolar type II epithelial cells. Eur Rev Med Pharmacol Sci. 2018;22(14):4625–4633. doi:10.26355/eurrev_201807_15521
11. Spadaro S, Park M, Turrini C, et al. Biomarkers for acute respiratory distress syndrome and prospects for personalised medicine. J Inflamm. 2019;16(1):1. doi:10.1186/s12950-018-0202-y
12. Wu H, Hong X, Qu Y, et al. The value of oxygen index and base excess in predicting the outcome of neonatal acute respiratory distress syndrome. J Pediatr. 2021;97(4):409–413. doi:10.1016/j.jped.2020.07.005
13. Yu A, Hou H, Ran L, Sun X, Xin W, Feng T. A nomogram for predicting neonatal acute respiratory distress syndrome in patients with neonatal pneumonia after 34 weeks of gestation. Front Pediatr. 2025;12(9):1451466. doi:10.3389/fped.2024.1451466
14. Shen L, Wan S, Sun X, Zheng R, Chen S. Establishment and evaluation of nomogram for predicting acute respiratory distress syndrome in meconium-stained amniotic fluid neonates. Pediatr Pulmonol. 2025;60(1):e27345. doi:10.1002/ppul.27345
15. Liu H, Li J, Guo J, Shi Y, Wang L. A prediction nomogram for neonatal acute respiratory distress syndrome in late-preterm infants and full-term infants: a retrospective study. EClinicalMedicine. 2022;50:101523. doi:10.1016/j.eclinm.2022.101523
16. De Luca D, van Kaam AH, Tingay DG, et al. The Montreux definition of neonatal ARDS: biological and clinical background behind the description of a new entity. Lancet Respir Med. 2017;5(8):657–666. doi:10.1016/S2213-2600(17)30214-X
17. Thompson BT, Chambers RC, Liu KD. Acute respiratory distress syndrome. N Engl J Med. 2017;377(6):562–572. doi:10.1056/NEJMra1608077
18. Kacerovsky M, Vrbacky F, Matulova J, et al. Late preterm prelabor rupture of membrane (>33 weeks): the risk of intraamniotic inflammation and fetal inflammation is influenced by the cervical microbial ecosystem and cervical inflammation. Am J Obstet Gynecol. 2025;6(16):S0002. doi:10.1016/j.ajog.2025.06.017
19. Lg DAB, Pastuschek J, Heimann Y, et al. Vaginal and neonatal microbiota in pregnant women with preterm premature rupture of membranes and consecutive early onset neonatal sepsis. BMC Med. 2023;21(1):92. doi:10.1186/s12916-023-02805-x
20. Sproston NR, Ashworth JJ. Role of C-Reactive protein at sites of inflammation and infection. Front Immunol. 2018;9(13):754. doi:10.3389/fimmu.2018.00754
21. Wang T, Liu Z, Wang Z, et al. Thrombocytopenia is associated with acute respiratory distress syndrome mortality: an international study. PLoS One. 2014;9(4):e94124. doi:10.1371/journal.pone.0094124
22. Middleton EA, Weyrich AS, Zimmerman GA. Platelets in pulmonary immune responses and inflammatory lung diseases. Physiol Rev. 2016;96(4):1211–1259. doi:10.1152/physrev.00038.2015
23. Li X, Tang Z, Kuang L, Wu Y, Huang X. Platelet membrane-coated nanoparticles inhibit platelet activation and neutrophil extracellular traps formation in acute lung injury. J Transl Med. 2025;23(1):841. doi:10.1186/s12967-025-06649-2
24. Dewitte A, Lepreux S, Villeneuve J, et al. Blood platelets and sepsis pathophysiology: a new therapeutic prospect in critically [corrected] ill patients? Ann Intensive Care. 2017;7(1):115. doi:10.1186/s13613-017-0337-7
25. Yu A, Hou H, Shi D, et al. Association between albumin levels and neonatal acute respiratory distress syndrome in newborn pneumoniae. J Inflamm Res. 2024;17:10015–10026. doi:10.2147/JIR.S492404
26. Taverna M, Marie AL, Mira JP, Guidet B. Specific antioxidant properties of human serum albumin. Ann Intensive Care. 2013;3(1):4. doi:10.1186/2110-5820-3-4
27. Bourdon E, Blache D. The importance of proteins in defense against oxidation. Antioxid Redox Signal. 2001;3(2):293–311. doi:10.1089/152308601300185241
28. Han J, Wang L, Jin L, Liu M. Association between bicarbonate levels and mortality among acute respiratory distress syndrome patients: an analysis based on Medical Information Mart for Intensive Care database. PLoS One. 2025;20(6):e0325498. doi:10.1371/journal.pone.0325498
29. Akuamoah-Boateng G, Moon TD, Amorim G, Bandini R, Ballot D. Intraventricular hemorrhage among very low birth weight infants in a South African cohort: a retrospective study of trends & short-term outcomes. BMC Pediatr. 2025;25(1):138. doi:10.1186/s12887-025-05426-w
30. Shin TW, Lee EJ, Choi HW, Yoo YM. Metabolic acidosis as a risk factor for bronchopulmonary dysplasia in preterm infants born between 23 + 0 and 31 + 6 weeks of gestation: a retrospective case-control study. Front Pediatr. 2025;13:1595348. doi:10.3389/fped.2025.1595348
31. Tan YY, Zhang DW, Yang C, et al. ASIC1a regulates airway epithelial cell pyroptosis in acute lung injury by NLRP3-Caspase1-GSDMD pathway. Int Immunopharmacol. 2024;143(Pt 3):113623. doi:10.1016/j.intimp.2024.113623
32. Stevens RP, Holston J, Maatouk K, et al. Carbonic anhydrase IX promotes acute lung injury and mortality in females during metabolic acidosis and pneumonia. Am J Physiol Lung Cell Mol Physiol. 2025;329(2):L266–L281. doi:10.1152/ajplung.00331.2024
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Development and Validation of a Nomogram Model for Predicting Chorioamnionitis in Patients with Term Premature Rupture of Membranes
Gao H, Gong L, Li Y, Huang W, Zhao J, Ren Z, Huang X, Lu J
International Journal of Women's Health 2026, 18:570474
Published Date: 6 March 2026