Back to Journals » Clinical Interventions in Aging » Volume 18
A Physiotherapy-Led Transition to Home Intervention for Older Adults Following Emergency Department Discharge: A Pilot Feasibility Randomised Controlled Trial (ED PLUS)
Authors Conneely M, Leahy S, O'Connor M ![]() , Corey G, Gabr A, Saleh A, Okpaje B, O' Shaughnessy Í, Synnott A, McCarthy A, Holmes A, Robinson K, Ryan L, Griffin A
, Corey G, Gabr A, Saleh A, Okpaje B, O' Shaughnessy Í, Synnott A, McCarthy A, Holmes A, Robinson K, Ryan L, Griffin A ![]() , Barry L
, Barry L ![]() , Trépel D
, Trépel D ![]() , Ryan D
, Ryan D ![]() , Galvin R
, Galvin R ![]()
Received 17 April 2023
Accepted for publication 11 July 2023
Published 24 October 2023 Volume 2023:18 Pages 1769—1788
DOI https://doi.org/10.2147/CIA.S413961
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Nandu Goswami
Mairéad Conneely,1 Siobhán Leahy,2 Margaret O’Connor,3 Gillian Corey,3 Ahmed Gabr,3 Anastasia Saleh,3 Blessing Okpaje,3 Íde O’ Shaughnessy,1,3 Aoife Synnott,3 Aoife McCarthy,3 Alison Holmes,1 Katie Robinson,1 Lorna Ryan,1 Anne Griffin,1 Louise Barry,4 Dominic Trépel,5 Damian Ryan,6 Rose Galvin1 On behalf of Ageing Research Centre Public and Patient Involvement (PPI) Panel of older adults
1School of Allied Health, Faculty of Education and Health Sciences, Ageing Research Centre, Health Research Institute, University of Limerick, Limerick, Ireland; 2Department of Sport, Exercise & Nutrition, School of Science & Computing, Atlantic Technological University, Galway, Ireland; 3Department of Ageing and Therapeutics, University Hospital Limerick, Limerick, Ireland; 4School of Nursing and Midwifery, Faculty of Education and Health Sciences, University of Limerick, Limerick, Ireland; 5Trinity Institute of Neurosciences, School of Medicine, Trinity College Dublin, Dublin, Ireland; 6Limerick EM Education Research Training (ALERT), Emergency Department, University Hospital Limerick, Limerick, Ireland
Correspondence: Mairéad Conneely, Email [email protected]
Background: Older adults frequently attend the emergency department (ED) and experience high rates of subsequent adverse outcomes including functional decline, ED re-presentation and unplanned hospital admission. The development of effective interventions to prevent such outcomes is a key priority for research and service provision. Our aim was to evaluate the feasibility of a physiotherapy-led integrated care intervention for older adults discharged from the ED (ED PLUS).
Patients and Methods: Older adults presenting to the ED of a university teaching hospital with undifferentiated medical complaints and discharged within 72 hours were computer randomised in a ratio of 1:1:1 to deliver usual care, Comprehensive Geriatric Assessment (CGA) in the ED, or ED PLUS. ED PLUS is an evidence-based and stakeholder-informed intervention to bridge the care transition between the ED and community by initiating a CGA in the ED and implementing a six-week, multi-component, self-management programme in the patient’s home. Feasibility and acceptability were assessed quantitatively and qualitatively. All clinical and process outcomes were assessed by a research nurse blinded to group allocation. Data analyses were primarily descriptive.
Results: Twenty-nine participants were recruited indicating a 67% recruitment rate. At 6 months, there was 100% retention in the usual care group, 88% in the CGA group and 90% in the ED PLUS group. ED PLUS participants expressed positive feedback, and there was a trend towards improved function and quality of life and less ED revisits and unscheduled hospitalisations in the ED PLUS group.
Conclusion: ED PLUS bridges the transition of care between the index visit to the ED and the community and is feasible using systematic recruitment strategies. Despite recruitment challenges in the context of COVID-19, the intervention was successfully delivered and well received by participants. There was a lower incidence of functional decline and improved quality of life in the ED PLUS group.
Trial Registration: The trial was registered in Clinical Trials Protocols and Results System as of 21st July 2021, with registration number NCT04983602.
Plain Language Summary: Older people need support when they are discharged from the Emergency Department (ED) to their home as a visit to the ED is linked to negative outcomes. This study reports on a trial to reduce negative outcomes in older people discharged from the ED by an assessment in the ED and treatment in the home. Twenty-nine patients attending the ED of University Hospital Limerick were randomly assigned to three groups as follows: One group got the normal care and treatment; Group two received a comprehensive assessment by a dedicated geriatric doctor in the ED and were referred to other health professionals as needed; a third group, called ED PLUS, also received a comprehensive assessment by a dedicated geriatric doctor in the ED and an additional six-week treatment program led by a physiotherapist. The physiotherapist visited the older adult in their own home within twenty-four hours of discharge to start treatment based on what the older adult needed to do to live safely in their own home and again at week four and week six. The same geriatric doctor who saw the older adult in the ED telephoned the older adult in week two to check medications and discussed the case with the physiotherapist. A dietitian and occupational therapist telephoned the older adults to check nutritional intake and if any aids were needed in the home. All older adults in the ED PLUS group had improved quality of their life, improved mobility and did not need to go back to the hospital or ED at six weeks and six months unlike the two other groups. The COVID-19 pandemic affected recruitment, but all ED PLUS patients were extremely satisfied.
Keywords: emergencies, recruitment, integrated care, care transitions, public and patient involvement
Introduction
As life expectancy increases, the percentage of older adults (aged 65 and over) is rising in many countries. One such nation experiencing this is Ireland, where there are currently 742,300 older adults in the population and that number is expected to increase to 1.56 million by 2051.1 As a result, increasing numbers of older adults are accessing acute care, with a rise in the incidence of multimorbidity2–6 and lower thresholds for accessing acute care.7 Older adults account for up to 25% of all Emergency Department (ED) attendances internationally.8,9 As a consequence of polypharmacy, the number of people living with chronic conditions and population ageing, ED presentations by older adults are increasing markedly and projected to continue doing so.10,11 ED use is currently outpacing population growth.12 EDs play an increasingly important role in the care of general populations, particularly older adults.13 The ED acts as an important point of entry for older people into acute care services that are available 24 hours a day for medical and social needs and acts as a bridge between the community and the hospital.14,15 Older adults have been described as “frequent users” of emergency services,16 accounting for up to 25% of all ED attendees.17 There are a number of reasons why older adults seek care in the ED including the management of an acute illness or emergency, perceived health status, a more definite resolution of their primary complaint,18 previous ED visits, previous hospitalisations, number of chronic conditions,19 a lack of access to primary care20 and geographical location.21,22
Once in the ED, older adults are more likely to experience longer lengths of stay and have more complex presentations, with higher rates of adverse outcomes following discharge from the ED than younger people.23–25 Adverse outcomes include functional decline, poorer quality of life, unscheduled return visits to the ED, hospitalisation and mortality.26,27 The ED plays an important role in the healthcare of older adults and in regulating hospital admissions.28
Given the high rates of adverse outcomes experienced by older adults following ED attendance,17,27,29–32 as well as the international focus on moving to longitudinal, coordinated models of healthcare delivery,33 we conducted an umbrella review of the effectiveness of ED-based or ED-initiated interventions to prevent adverse outcomes in this population post ED discharge.34 Our umbrella review identified low-quality evidence to support ED interventions in reducing functional decline, improving patient experience and improving quality of life. The quality of evidence of the effectiveness of ED interventions to reduce mortality and ED revisits varied from very low to moderate. Notably, while health and social care professionals (HSCPs) (eg, physiotherapists, occupational therapists) are key health disciplines in supporting functional rehabilitation, we did not identify any systematic review or randomised controlled trial (RCT) that explored the impact of HSCP-led interventions to reduce the incidence of functional decline and improve quality of life in this cohort. Research is growing that these disciplines can play a role in the ED in improving patient experience, reducing length of ED stay and preventing hospital admissions in other age groups.35,36 In recognition of these improvements in other age groups, a RCT tested the effect of adding a dedicated team of HSCP to the ED and concluded that early assessment and intervention for low urgency older adults can facilitate shorter stays in the ED, reduced risk of hospital admissions, improved satisfaction with their care as well as reporting better function at follow-up.37 The authors of this trial recommended further research for integration of care following discharge from the ED.
Underpinned by the Medical Research Council (MRC) framework for the development and evaluation of complex interventions,38 we developed a novel intervention, ED PLUS, in response to the findings from our umbrella review, with the support of a Public and Patient Involvement (PPI) panel of older adults, to address healthcare needs of older adult ED attendees.39 ED PLUS, a physiotherapist led, multidisciplinary intervention, bridges the transition of care between the index visit to the ED and the community.39 The intervention is initiated in the ED with a Comprehensive Geriatric Assessment (CGA) and a six-week follow-up self-management programme in the person’s own home following discharge from the ED to reduce the incidence of functional decline. The data generated from this pilot feasibility RCT will inform the conduct and delivery of a definitive RCT.
Aims and Objectives
The overall aim was to examine the feasibility and acceptability of implementing a 6-week transitional intervention delivered both face to face and via telephone support for older adults discharged from the ED.
Primary aims were
- To assess the feasibility of undertaking a definitive RCT of the ED PLUS intervention by a physiotherapist in this population, evaluating the process of recruitment, screening, randomisation, and collection of baseline and outcome data.
- To establish whether the intervention was acceptable to older adults discharged from the ED.
- To explore any trial design aspects that may require refinement prior to proceeding to a full RCT.
Secondary aims were
- To examine the effect of ED PLUS on functional decline at 6 weeks and 6 months.
- To explore the effect of the ED PLUS on quality of life at 6 weeks and 6 months.
- To examine the effects of ED PLUS on process outcomes (ED revisits, unplanned admission, hospital length of stay) at 6 weeks and 6 months.
- To examine the unit costs associated with implementing ED PLUS.
Materials and Methods
Study Design Overview
The methods for this feasibility RCT are published in detail elsewhere.39 This is a parallel group pilot RCT with a 1:1:1 allocation ratio. The trial is registered at Clinical trials.gov (NCT04983602). Ethics approval was obtained from the HSE Mid-Western Area Research Ethics Committee (Ref: 088/2020). As recommended for the conduct of pilot RCTs, we also obtained qualitative data to supplement the quantitative data.40 The reporting of this study follows the Consolidated Standards of Reporting Trials (CONSORT) extension for randomised pilot and feasibility trial guidelines41 and the CONSORT extension for reporting of patient-reported outcomes,42(Supplementary Information 1).
Trial Setting
The pilot RCT was conducted in the ED and Acute Medical Assessment Unit (AMU) of a university teaching hospital in the Mid-West region of Ireland. University Hospital Limerick (UHL) serves both rural and urban areas of Limerick, Clare and North Tipperary, catering for general medical, surgical, and emergency treatment of patients in its catchment area of 470,000 people. UHL provides 24 hours and 7 days a week ED to this population.
The inclusion criteria for participants were adults aged ≥65 years with undifferentiated medical complaints presenting to an ED Monday to Thursday (8am-5pm). Participants had to:
- Be medically stable as deemed by the treating physician (vital signs are within normal limits, patients do not require a surgical assessment).43
- Have a score of ≥2 on the Identification of Seniors at Risk (ISAR) screening tool.44,45 The ISAR is a validated five-item screening tool for use in the ED to detect older adults at risk of adverse outcomes including functional decline, revisits to the ED, unplanned hospitalisation and mortality within 6 months of the ED presentation.
- Be community dwelling.
- Have a short-term ED attendance or AMU admission with a predicted length of stay of ≤72 hours from ED presentation.
- Have a confirmed negative COVID-19 test on presentation to the ED.
Recruitment and Baseline Assessment
Recruitment commenced on 13th September 2021 and ended on November 5th 2021, which included an extension of one week owing to a target sample of 30 patients not being reached on 29th October 2021. Eligible older adults were invited to participate in the trial by a dedicated research nurse (GC) during their ED or AMAU visit. They were given an opportunity to read the patient information leaflet and ask any questions they had before providing written informed consent if agreeable. After consenting to take part, a baseline assessment was carried out on each participant by the dedicated research nurse (GC).
Demographic information including the participants’ gender, age, marital status and living arrangement were collected by GC. The health assessment comprised the following measurements: functional status measured through the Barthel Index for activities of daily living (ADLs),46 health-related quality of life through the EuroQoL survey 5-dimension and 5-levels form (EQ-5D-5L),47 frailty via the Rockwood’s Clinical Frailty Scale,48 co-existing diseases via the Charlson Comorbidity Index,49 screening tool for delirium and cognitive impairment via 4AT,50 nutritional status through the Mini Nutritional Assessment short form (MNA-SF),51 whether the person had experienced any falls in the 3 months prior to the ED visit and whether the person had been hospitalised in the 6 months prior to the ED visit (via ISAR). This assessment took 45 to 60 minutes.
Randomisation
Eligible participants were randomised using a computer generated 1:1:1 allocation through an online, central randomisation service, Sealed Envelope website (www.sealedenvelope.com). This technique is frequently used in clinical trials to minimise selection bias and to allocate an equal number of participants to each treatment arm by sequencing participant assignments by blocks of three.52 This method is especially useful for small sample sizes.53 Allocation was concealed from participants, and researchers until informed consent was obtained and baseline evaluations performed. The research nurse (GC) assigned participants to interventions once allocation was revealed via the online randomisation service.
Blinding
Due to the nature of the intervention, trial participants and treating clinicians were not blinded to group allocation. The outcome assessor, a second research nurse (LB), was blinded to group allocation.
Interventions
The interventions used in this study are described elsewhere in detail.39 Briefly, there were three arms to this pilot feasibility trial: usual care, intervention arm 1 (CGA) and intervention arm 2 (ED PLUS).
Usual Care
Participants in the usual care group received routine care provided by the Emergency Medicine doctors and nursing staff for the duration of their stay in the ED and AMU. They were assessed by one or more members of the dedicated interdisciplinary HSCP team (senior occupational therapist, one senior physiotherapist, and one senior medical social worker); however, there was no dedicated team to systematically deliver CGA (incorporating geriatric medical expertise) to frail older adults in the ED or AMAU. The assessment included, but was not limited to, an interdisciplinary assessment of functional and mobility status, cognition, and psychosocial needs. Supplementary Table 1 outlines the assessment that each of the participants in the usual care group received in the ED and AMU at baseline.
Intervention Arm 1 Comprehensive Geriatric Assessment (CGA)
The SOLAR team (consisting of a consultant in geriatric medicine/geriatric specialist registrar (SpR), specialist geriatric nurse, senior physiotherapist, senior occupational therapist, and senior medical social worker) in the ED and AMU adopted an interdisciplinary model of assessment of all participants in the intervention groups and performed CGA. The intervention arm 1 comprised a detailed interdisciplinary assessment and intervention by one or more members of the dedicated SOLAR team in UHL (AG, AS, BO, ÍO’S, AS, AMcC). CGA included, but was not limited to, a medical assessment, medication review, nursing assessment, falls assessment, assessment of mobility and stairs, transfers, personal care, activities of daily living (ADLs), social support, baseline cognition and continence.23 Members of the SOLAR team were guided by their clinical expertise and codes of professional practice. Similarly, interventions prescribed by the SOLAR team were based on subjective and objective assessment of patients and included medication alterations, lifestyle advice, prescription of mobility aids and enabling equipment, provision of home exercise programmes and onward community referral as appropriate. Supplementary Table 2 outlines the assessment that each of the participants in the CGA group received in the ED at baseline.
Intervention Arm 2 ED PLUS
The ED PLUS programme consisted of CGA in the ED plus a six-week multicomponent, multidisciplinary, patient centred self-management support and exercise programme.39 The ED PLUS team consisted of a geriatrician, SpR in geriatrics (AG, AS, BO), staff grade dietitian (LR), and senior occupational therapist (ÍO’S) and led by a clinical specialist physiotherapist (MC). It was designed and structured to maximise the patient’s self-efficacy and support independence in functional activities and provide a continuum of care from the ED to the patient’s home.39 ED PLUS aimed to address issues with mobility, strength, balance, nutrition, medication adherence, fatigue and enable self-management.39
The six-week programme involved a telephone call from the dedicated research nurse (GC) to the clinical specialist physiotherapist (MC), and the physiotherapist met the participant in the ED or AMU to arrange a physiotherapist home visit. The home visit took place within 24 hours post ED discharge. HSCP includes professions such as social work, physiotherapy, occupational therapy and dietetics. In Ireland, HSCPs are the second largest clinical grouping of the healthcare workforce, yet they are often neglected in policy debates and health workforce planning. There is a growing evidence base to inform HSCP-led models of care for older adults seeking unscheduled care. While older adults seek emergency care for a variety of reasons, some ED attendances may be better suited to alternative out-of-hospital pathways. To this end, there is an opportunity to provide timely specialist assessment and intervention by dedicated HSCP teams in the ED to some older adults to reduce the risk of long ED waiting times and avoidable hospital admissions. A previous randomised controlled trial37 showed that early assessment and intervention by a dedicated ED-based HSCP team reduced ED length of stay and the risk of hospital admissions among older adults, as well as improving patient satisfaction. However, no differences at follow-up were observed in terms of ED re-presentation or hospital admission. The ED PLUS pilot RCT built on these previous findings and addressed key gaps in the literature by exploring the feasibility of a new integrated HSCP-led model of care to enhance the transition of care out of the ED for older adults. The lead and anchor authors are both physiotherapists with extensive clinical and research experience in the assessment and treatment of older adults.
The initial visit involved an assessment in the participants’ home (1.5–2 hours duration), discussion with the participant regarding the assessment and the formulation of a treatment plan alongside the setting of participant goals over the six-week period. The programme involved three home visits by a physiotherapist over a period of six weeks with telephone support in between the visits by the physiotherapist. The other members of the team contacted the patient as outlined in Figure 1. The physiotherapist implemented a personalised treatment plan based on the assessment of the participant, in line with patient-identified goals, liaising with the geriatric specialist registrar (SpR) (AG, BO, AS), senior occupational therapist (ÍO’S) and staff grade dietitian (LR) with key regard to medication adherence, exercise prescription, physical activity and strength. As outlined in Supplementary Table 3, the geriatric SpR discussed medication adherence and addressed concerns regarding same via telephone. The dietitian (LR) engaged in a one-to-one dietetic session to optimise dietary intake, ensuring adequate energy, protein and micronutrient status. The occupational therapist (ÍO’S) discussed self-management of morbidity, fatigue and energy conservation to ensure ongoing engagement in physical activity programmes and leisure pursuits. The physiotherapist acted as the key caseworker/care coordinator and supported the patient during the six-week programme to address any issues related to their health with liaison with the participants GP, Public Health Nurse, and Consultant as required. All healthcare professionals adhered to guidelines for COVID-19 throughout the duration of the intervention. At the time of recruitment, the Delta variant of COVID-19 was spreading, with continuing increases in hospitalisation and intensive care admissions in Ireland. The highest number of cases recorded in Ireland since January 2021 was recorded on the 18th of October 2021, at week 5 of recruitment.
 |
Figure 1 Frequency of ED PLUS sessions. |
Supplementary Table 3 outlines the ED PLUS intervention with specifics on the intervention delivered and Figure 1 illustrates the frequency of the sessions. Supplementary Information 2 provides further details of the ED PLUS Intervention characteristics.
Patient and Public Involvement
The ED PLUS programme was developed in conjunction with a local Public and Patient Involvement (PPI) panel of older adults in the Mid-West/UHL catchment area; this panel was set up to support researchers in ageing research.54 The lead author (MC) conducted telephone conversations with representatives from the panel (N=5) to initiate interest in such a trial, discuss solutions to recruitment challenges of older adults in the ED, develop the consent form, assist in the selection of patient centred outcomes and the preparation of a patient information leaflet for the trial. The PPI group also assisted in the design of a patient exercise program leaflet explaining the role of a physiotherapist in improving function, the benefits of exercise for older adults and a community program contact template for older adults in the mid-west region. A plain lay summary of the trial findings for this paper was written by the PPI panel of older adults following a presentation and discussion of the methodology and results of the trial by the lead author to the PPI panel.
Data Collection and Outcomes
There was one outcome assessor blinded to group allocation (LB).
Recruitment, Retention and Adherence
Data from screening, recruitment and follow-up logs were used to generate realistic estimates of eligibility, recruitment, consent and follow-up rates. Feasibility was described in terms of recruitment rates, adherence, retention and acceptability of ED PLUS. Recruitment rate was described as the percentage of eligible study population who consented to participate in ED PLUS. Adherence was recorded as the number of home visits made by the physiotherapist in the ED PLUS team plus the number of interactions with the geriatrician, dietician, physiotherapist and occupational therapist. Retention was defined as the percentage of enrolled participants completing the post-intervention assessment at 6 weeks.
Participant and Provider/Staff Experience
We assessed the acceptability of the intervention through qualitative interviews, to supplement the quantitative data.40 The qualitative evaluation assessed the acceptability of the trial methods, evaluated the acceptability of the ED PLUS, identified modifications to ED PLUS and described participants’ experiences of ED PLUS. One-to-one semi-structured telephone interviews with nine trial participants in intervention arm 2 and all medical and HSCP involved in the intervention arm 2 were undertaken on completion of the programme by a person independent of the trial (AH). Participants were contacted to undertake a telephone interview following completion of the ED PLUS intervention. All interviews were digitally recorded and transcribed verbatim. All participants were offered an opportunity to view their own transcript.
Clinical Outcome Measures
We assessed the following clinical and process outcomes at 6 weeks and 6 months post ED visit via telephone contact by a research nurse (LB) who was blinded to group allocation:
- Functional status using the Barthel Index.55
- Quality of life using the EuroQoL-5D EQ-5D-5L.
- ED revisit assessed via hospital data systems.
- Unplanned hospitalisation and nursing home admission assessed via hospital data systems and patient recall medical records.
- Mortality.
- Healthcare utilisation was captured by telephone contact.
Progression to a Full Trial
A number of progression criteria were pre-defined with the Trial Steering Committee (TSC) as per our protocol:
- A minimum of 80% recruitment of eligible patients
- A minimum of 80% completion rate of key outcome measures (including follow-up)
Economic Evaluation
A pilot health economic analysis was conducted in conjunction with the feasibility trial. The health economic evaluation will evaluate the direct costs of ED PLUS to understand the economic effectiveness of a future definite trial. Details of the costings are in Supplementary Information 3.
Statistical Data Analysis
As this was a feasibility study with a relatively small sample size, formal hypothesis testing was not appropriate; rather, the purpose of any analyses was to generate estimates to inform the planning of the definitive future trial, as detailed in the protocol.39 The analysis was completed in two stages. Stage 1 summarised the feasibility outcomes. Stage 2 summarised the clinical outcomes data at 6 weeks and 6 months. As it is inappropriate to use feasibility trial data to formally test for between-group treatment effects, the analyses are of a descriptive nature,40,41 Data analyses were primarily descriptive. All analyses were documented in a Statistical Analysis Plan as per a published protocol. Feasibility outcomes were estimated using descriptive statistics (%) and included recruitment rates, follow-up rates in both arms of the trial, missing data, and intervention adherence. Demographic and clinical characteristics at baseline were summarized in the three intervention arms. Clinical outcomes were summarized descriptively for participants with outcome data with the allocated intervention performed via STATA statistical software (STATA Corp, College Station, TX; version 16).
Qualitative Analysis
Interview data were transcribed in full and analysed (AH) H using a reflexive approach to thematic analysis56 which acknowledges the centrality of researcher subjectivity. Analysis was facilitated using NVIVO 12 software. Both participants and HSCPs were invited to review and discuss preliminary analysis of the interview data and contribute to the process of identifying themes. The entire findings of the qualitative study will be reported elsewhere, but the key findings pertaining to acceptability are reported here.
Results
Feasibility Outcomes
Recruitment
A total of 108 participants were screened for eligibility, and 43 participants were deemed eligible for the intervention. Of these, 29 participants were randomised into the three groups (Figure 2). Despite extending the recruitment window by one week, we failed to recruit the anticipated sample size of 30 participants. This indicates a 67% recruitment of eligible patients, not satisfying criteria 1 for progression to a full trial. Only one patient declined to enter the trial and 13 additional eligible older adults were excluded as per Figure 2. One patient was deemed potentially eligible for inclusion but was not vaccinated against COVID-19, and thus the TSC deemed it inappropriate to potentially expose the patient to multiple healthcare professionals and excluded the patient from the trial. Given that this was not an explicit exclusion criterion, we are reporting it as a deviation from our protocol.
 |
Figure 2 CONSORT extension for pilot and feasibility trials flow chart. |
Randomisation, Retention and Adherence
Randomisation procedures were implemented successfully, resulting in the allocation of 10 participants to the usual care group, nine participants to the CGA only group and 10 participants to the ED PLUS group. Staff reported that the randomisation procedure was easy to administer. The overall retention rate at 6 weeks was 100% in the usual care group, 88.8% in the CGA only group and 100% in the ED PLUS group. At 6 months, there was 100% retention in the usual care group, 88% and 90% in the CGA only and ED PLUS groups, respectively. There were no withdrawals from the study, except one mortality within 6 weeks for the CGA only group and one mortality within 6 months for the ED PLUS group. At six-week follow up, data on process outcomes (ED revisits, unscheduled hospital admissions, and nursing home admissions) were available for all participants; data on function and quality of life was available on 28 participants (n = 1 lost to follow-up due to mortality). At 6 months, analyses of patient-reported outcomes included 27 patients (excluding 2 participants who had died within six months).
Staff Experiences Regarding ED PLUS Feasibility
Staff agreed that ED PLUS was feasible to deliver, however they noted several caveats. Firstly, several staff voiced concerns about the intensive workload for the ED PLUS clinical specialist physiotherapist and queried whether this workload would be sustainable if the intervention was scaled up in the future. Secondly, the availability of the SpR in geriatrics to complete CGA with older adult participants in the ED in a timely manner was an issue. Delays in the SpR’s availability impacted not only the patient and the ED PLUS staff but also created challenges for ED staff when older adults were ready to leave the ED but were awaiting CGA. Thirdly, staff noted that recruitment of older adults to the trial was affected by the volatility of patient presentation. In some cases, participants deteriorated, or their status changed while in the ED or AMU meaning that they shifted from being eligible to participate to becoming ineligible to participate over a short time period (ie, patients were admitted to the hospital from the ED). Finally, the feasibility of one key caseworker (physiotherapist) completing home visits with older adults over a large geographical area was questioned by some staff. Staff voiced concerns about travel time, the safety of the physiotherapist acting alone, resources and the resultant need for the physiotherapist to communicate with multiple general practitioners (GPs), public health nurses (PHN) and primary care teams. Due to the ongoing COVID-19 pandemic during the study period, recruitment was affected as potential participants tested positive and thus became ineligible for inclusion (as visualised in Figure 2). Staff testing positive for COVID-19 were unable to attend work at the ED or AMU and this impacted the ability of the SpR in geriatrics to complete CGA in the ED or AMU. In the final three weeks of the recruitment period, delays in COVID-19 testing also affected recruitment.
Staff Experiences of ED PLUS
Staff were very receptive to CGA being completed. They reported that it was effective and beneficial for older adults and viewed home visits as key to the success of ED PLUS. Staff valued communication back from the home visit by the clinical specialist physiotherapist (MC), as a key caseworker, in terms of informing their decision-making and supporting effective team working. Staff indicated that virtual elements of ED PLUS would not have been effective without the home visit element of the intervention. Additionally, they identified that it was important for ED PLUS staff to be integrated into the ED and AMU with a physical presence in the ED. ED staff emphasised that ED PLUS must be perceived by staff to be contributing or adding benefit for patients and not just adding to the ED workload.
Programme Acceptability and Engagement
Nine of the ten participants (90%) allocated to the ED PLUS intervention completed the intervention and thus we met the criteria for engagement with the programme (satisfying progression criterion two). One participant completed the CGA component of the ED PLUS intervention but became ill during the CGA process and was subsequently admitted for an inpatient stay. The remaining nine participants completed all the home visits and all the telephone calls with members of the ED PLUS team (Figure 1), indicating 100% adherence with the ED PLUS intervention. One participant refused a referral to Bone Health services at 6 months post intervention, while all others accepted appointments offered to other healthcare services.
All strongly endorsed the acceptability of ED PLUS. Older adults valued the ease of access to ED PLUS given that it was delivered primarily in their homes. Older adults positively evaluated the experience of having a single point of contact/case manager and indicated that the case manager in this reach/outreach model was effective. Older adults identified that risks in terms of COVID-19 infection were well managed during the ED PLUS intervention.
Demographic and Clinical Characteristics at Baseline
Table 1 outlines the demographics and clinical characteristics of the 29 participants at baseline. A total of twenty females (68.9%) and nine males were recruited with a mean age of 81.31 years (SD=6.52). Most participants (75.86%) presented to the ED via self-referral with 51.72% of all participants (n=15) brought in by ambulance (BIBA). The groups were similar at baseline with respect to clinical characteristics, with 75% of all 29 patients experiencing at least one fall in the previous three months. The presenting complaint for twenty patients (68.67%) was a fall (Table 1). Of note, the majority of the patients, n=23 (79.3%) were rated mild to moderately frail on the Clinical Frailty Scale.48
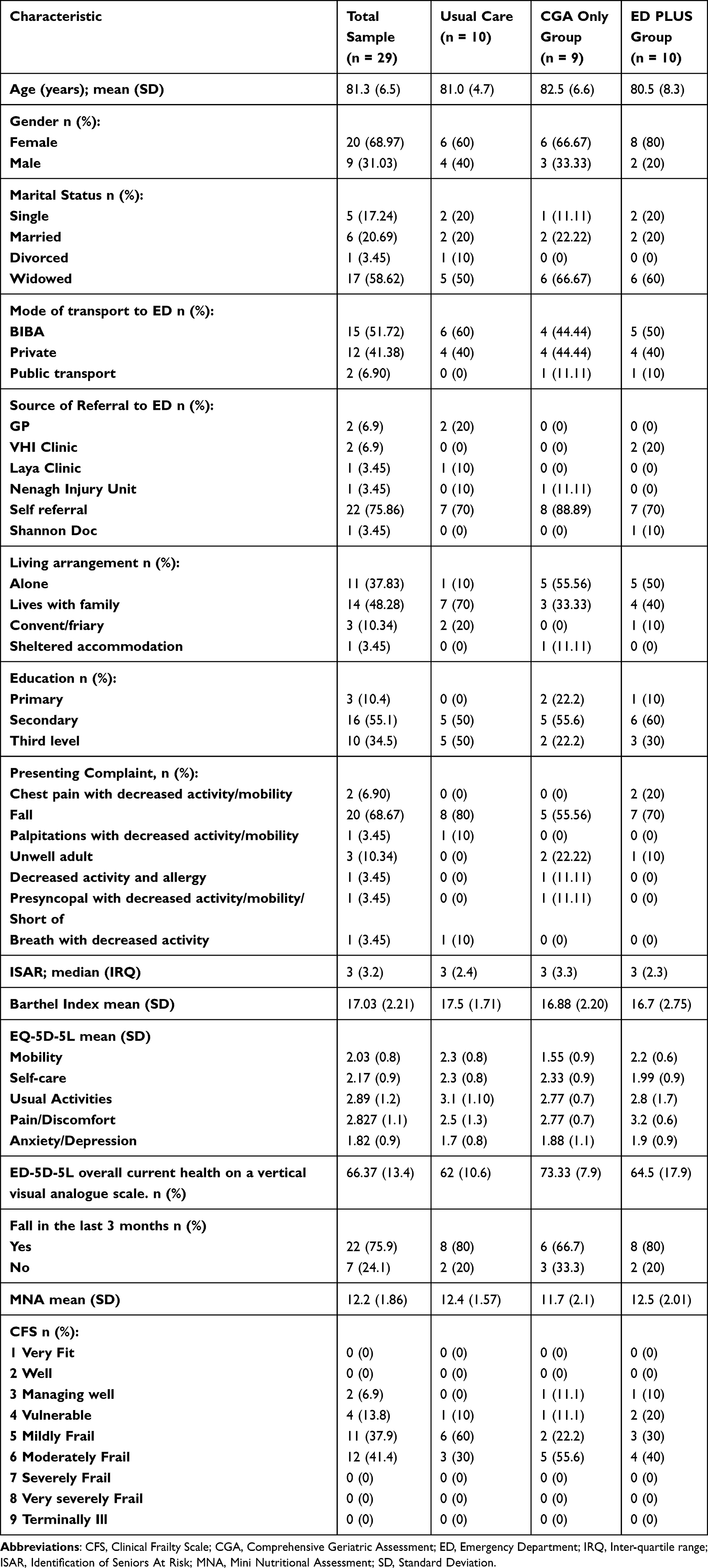 |
Table 1 Baseline Demographic and Clinical Characteristics |
Secondary Outcomes: Outcome Measures
Tables 2 and 3 provide details on the secondary outcomes for this pilot feasibility trial. The outcomes show a trend towards improved function, as measured by Barthel Index, in the ED PLUS group in comparison to the control and CGA only group at both 6 weeks and 6 months (Tables 2 and 3). A similar trend is evident for the ED-5D-5L domains (Mobility, Self-Care, Usual Activities, Pain/Discomfort and Anxiety Depression) and overall perceived health status. Patterns of healthcare utilisation, in terms of ED revisits and hospital admissions, were lower in the ED PLUS group in comparison to the CGA only group and the usual care groups, as represented in Tables 2 and 3.
 |
Table 2 Six-Week Clinical Outcome Measures |
 |
Table 3 Six-Month Clinical Outcome Measures |
Discussion
This pilot feasibility RCT examined the feasibility and acceptability of a physiotherapist led, multidisciplinary intervention, which bridged the transition of care between the index visit to the ED or AMU and the community by initiating a CGA intervention in the ED and implementing a six-week follow-up self-management programme in the participant’s own home. Twenty-nine participants were recruited, representing 67% of eligible participants. A total of 90% of participants completed the ED-PLUS intervention. All ED PLUS participants expressed positive feedback about the intervention. There was a trend towards improved function and quality of life, and less ED revisits and unscheduled hospitalisations in the ED PLUS group versus the usual care and the CGA only groups.
Recruiting older adults to interventions can be a complex and challenging process due to barriers related to exclusion criteria (eg, specific comorbidities), lack of perceived benefits and distrust of research staff.57–60 Recruitment was challenged in this study by the number of positive COVID-19 cases that rendered participants ineligible and affected staff resources to carry out the CGA in the CGA-only group and the ED PLUS group. In future RCTs, older adults who test positive for COVID-19 can be included as potentially eligible for participation in ED PLUS as knowledge about the virus grows and vaccination roll out continues. International research demonstrates that older adults who contracted COVID-19 and were hospitalised exhibit decreased quality of life and a decline in function.61–64 These older adults may benefit from an ED PLUS intervention to improve their health status, similar to the heterogenous group of older adults recruited for this study. Prospective cohort studies indicate that a CGA-based strategy could enhance the management of older persons with COVID-19 by first identifying domains that have more impairment, but also by enabling the establishment of personalised care plans in various settings.65–67 Given that full safety precautions were undertaken during the entire study process from the ED to the participants’ homes, including a telephone call to assess participants’ symptoms before home visits and with the use of Personal Protective Equipment (PPE) for all interactions with patients, including older adults with a positive COVID-19 status would seem practical going forward. The effects on the pandemic aside, only one older adult declined to participate, reflecting the positive trust of the participants in the recruiting staff68 and the program itself. The strategies that were employed to enhance recruitment included the engagement with a PPI panel of older adults who assisted in preparing the patient information leaflet and the consent form. A dedicated research nurse with extensive knowledge of the ED context embedded study methods in the patient care pathway for the duration of the length of stay in the ED. Given the dynamic nature and overcrowding in many EDs internationally,69,70 the role of a dedicated research nurse with an interest in the care of older adults in the ED is essential.71 Availability of geriatric medical staff to support CGA assessment is challenging without dedicated resourcing and is essential given the complexity and multi-morbidity of frail older adults.72 Owing to the effects of COVID-19 and the precautionary measures of isolation, staff were unable to attend for work and carry out the CGA for the CGA only and the ED PLUS groups, thus patients were unable to be recruited.
The literature on the willingness of older adults to participate in clinical research yields contradictory findings,73,74 with some older adults declining due to a lack of transport to a research or clinical site as well as seeing no perceived benefit to participation.68,75 The ED PLUS intervention was delivered as a hybrid model of care including home visits and telephone calls to participants, thus supporting older adults in their own environment. To optimise recruitment and retention rates, home-based interventions have been suggested, with flexibility on timing and dates.76 In aligning our intervention alongside the WHO policy on integrated care,77 the Geriatric ED Guidelines,78 research priorities in the area of European Geriatric Medicine79 as well as with the Irish Health Service Executive (HSE) National Strategy for Older Adults, our intervention facilitated a naturalistic observation and treatment in the person’s own home environment, empowering the older adult to feel in control.80 Home visits offer the opportunity to identify unmet medical, social and environmental needs.81 Acceptability of the ED-PLUS intervention was supported by the high adherence rate, in line with international research.80,82 The retention rate at six weeks was 88.8% in the CGA group, 100% in the usual care and ED PLUS groups; a rate higher than a systematic review of eight RCTs in frail older adults that reported a retention rate of 85% or greater.83 The high retention rate stresses the importance of linking research on the health of older adults into their community, connecting them with other relevant local organisations, and establishing a good relationship with participants and their families.68,71 Optimising care transitions is a recommendation of the Geriatric ED Guidelines; while these guidelines provide a “template” for creating a “geriatric-friendly” ED, they do not offer suggestions on particular interventions for older adults seeking care in the ED.78 Instead, recommendations centre on staffing, administration, physical environment, and leadership, with a call to provide innovative local measures to support older adults to age in place and an exploration of a community-based model of care with tailored interventions.3
Patient-centred care is one strategy to enhance healthcare systems by improving patient satisfaction and health outcomes with lowering healthcare costs.84 Having a key caseworker, a clinical specialist physiotherapist, allowed for a case management approach to the care transition of the older adult with the integration of the multidisciplinary team.85 Older adults report a preference for a single professional responsible for their overall care, taking into consideration their unique presentation and preferences for their management.86,87 A case management approach was incorporated into study design, leading to positive participant experiences and high adherence in ED PLUS. Older adults cite a lack of written information about their admission and lack of home management planning,88,89 and programs should keep centred on the needs and wants of older adults incorporating their social and functional requirements.88,90 Furthermore, the existing evidence base supports the appointment of one clearly defined healthcare professional who co-ordinates care, with a focus on patient preferences, shared decision-making and a focus on functional outcomes.91,92 HSCP, such as physiotherapists, offer the potential to improve patient and population health and well-being by driving service improvements, research, management and leadership.93,94 This pilot RCT indicates that both patients and other staff (SpR Geriatrics, Occupational Therapist, Dietician) valued the role of a key caseworker acting in a team leadership role and this is an avenue for further research. Staff felt ED PLUS was effective and beneficial for older adults and viewed home visits as key to the success of ED PLUS.
The fundamental challenge in evaluating a complex intervention is the number of components that work both independently and interdependently.38,95,96 This pilot RCT provides important learning points that can inform future RCTs in older adults that present to the ED and are being discharged home. We did not reach our recruitment goal due to the number of positive COVID-19 cases that rendered participants ineligible and affected staff resources to carry out the CGA in the CGA-only group and the ED PLUS group. The operational metrics of the ED in Ireland altered during COVID-19 with service reorganisation to allow for capacity to manage those infected with COVID-19.97,98
Considering the small sample size of the study and therefore lack of statistical power to detect effectiveness, no definite conclusions can be drawn from the results which should be interpreted with caution. However, potential signs of improvements can be identified which can be relevant for future research, especially the trends towards improving function, improving quality of life, patient experience and a decrease in unscheduled ED visits and hospital admissions amongst those participants in the ED PLUS group. The evidence generated from the pilot study will go to inform the design and conduct of a full economic evaluation to assess the cost-effectiveness of the developed programme. For the cost-utility analysis, Quality Adjusted Life-Years (QALYs) will be estimated using data collected via the EQ-5D-5L survey instrument at baseline and over the follow-up period.99
Limitations of this RCT include the relatively short duration of the RCT, absence of a long-term follow-up and lack of statistical power meant that it was not possible to investigate whether the clinical measures are likely to be sufficiently responsive for use in a future definitive RCT. Previous research has demonstrated that there is uncertainty regarding the ability of the Barthel index to be sensitive to change.100 We acknowledge that we mainly recruited mild to moderately frail women so the results may not be generalisable to men and more frail populations, however this could be considered reflective of population demography. In addition, recruitment was affected by the COVID-19 pandemic and may not necessarily reflect normal circumstances. Pilot feasibility RCTs are context dependent, and it is not possible to infer that the results yielded here would be reproduced in other EDs and regions.101–103
The strengths of this pilot feasibility RCT provide valuable information to inform the design of any subsequent definitive study including, for example, approaches to consent, ability to collect data at six weeks and six months, willingness to recruit and randomisation, and adherence. The ED PLUS pilot RCT was methodologically rigorous and followed international guidelines for the development and evaluation of complex interventions,38 with a peer-reviewed protocol published in advance of the trial. A PPI panel of older adults was involved from inception to dissemination further strengthening this study.
Both staff and patients reported satisfaction with the model of delivery of care and the role of the physiotherapist acting as a key caseworker, supporting the care transition from the ED to the home. Our model of health service delivery aligns to national and international policies on healthy and successful ageing and integration of care, particularly in relation to supporting older adults to live in their own homes and communities.3 International Geriatric Medicine guidelines call for creative local strategies to assist with the growing challenging issue of increased ED presentations by older adults, and we have designed a novel integrated care intervention to bridge the ED to community interface.79,104
Conclusion
ED PLUS has provided valuable process, management and scientific data including preliminary evidence that the intervention had beneficial effects on clinical outcomes and healthcare utilization. A pilot feasibility trial, ED PLUS, bridges the transition of care between the index visit to the ED and the community, for an older adult visiting the ED, and is feasible using systematic recruitment strategies. Despite recruitment challenges in the context of COVID 19, the intervention was successfully delivered and well received by participants. There was a lower incidence of functional decline and improved quality of life in the ED PLUS group. This preliminary evidence requires confirmation in a future definite, adequately powered RCT that incorporates long-term follow-up of important clinical and process outcomes.
Data Sharing Statement
The datasets generated during and/or analysed during the current study are openly available at https://osf.io/3hmda.
Ethical Approval
This study was conducted in accordance with the Declaration of Helsinki. This study was conducted with approval from the HSE Mid-Western Area Research Ethics Committee (Ref: 088/2020). No identifiable participant information (such as patients’ images, faces, or names) was disclosed in the study.
Acknowledgment
The authors report that an abstract of this pilot feasibility trial was presented at the WONCA Conference in the University of Limerick in June 2022, the 18th EuGMS Congress in London in September 2022 and the Irish Gerontological Society Annual Meeting in November 2022. The abstracts were subsequently published in Rural and Remote Health, European Emergency Journal and Age and Ageing.
Funding
MC was supported by the Health Research Board (HRB) of Ireland (Health Research Board, Grattan House 67–72 Lower Mount Street, Dublin 2, D02 H638) through the HRB Collaborative Doctoral Awards under Grant CDA-2018-005 (“Right Care” Programme). The funder has no role in the study design, collection, management, analysis, interpretation of the data or writing of the protocol.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Clark D. Population of Ireland by age group in 2019. Statista; 2022. Available from: https://www.statista.com/statistics/710767/irish-population-by-age/.
2. Kingston A, Robinson L, Booth H, Knapp M, Jagger C, Project M. Projections of multi-morbidity in the older population in England to 2035: estimates from the Population Ageing and Care Simulation (PACSim) model. Age Ageing. 2018;47(3):374–380. doi:10.1093/ageing/afx201
3. Prince MJ, Wu F, Guo Y, et al. The burden of disease in older people and implications for health policy and practice. Lancet. 2015;385(9967):549–562. doi:10.1016/s0140-6736(14)61347-7
4. Caughey GE, Ramsay EN, Vitry AI, et al. Comorbid chronic diseases, discordant impact on mortality in older people: a 14-year longitudinal population study. J Epidemiol Community Health. 2010;64(12):1036–1042. doi:10.1136/jech.2009.088260
5. Kirchberger I, Meisinger C, Heier M, et al. Patterns of multimorbidity in the aged population. Results from the KORA-Age study. PLoS One. 2012;7(1):e30556. doi:10.1371/journal.pone.0030556
6. Chatterji S, Byles J, Cutler D, Seeman T, Verdes E. Health, functioning, and disability in older adults—present status and future implications. Lancet. 2015;385(9967):563–575. doi:10.1016/S0140-6736(14)61462-8
7. Smith P, McKeon A, Blunt I, Edwards N. NHS Hospitals Under Pressure: Trends in Acute Activity Up to 2022. London: Nuffield Trust; 2022.
8. Hoon LS, Mackey S, Hong-Gu H. Elderly patients’ experiences of care received in the emergency department: a systematic review. JBI Evid Synth. 2012;10(23):1363–1409.
9. Beaton K, Grimmer K. Tools that assess functional decline: systematic literature review update. Clin Interv Aging. 2013;8:485. doi:10.2147/CIA.S42528
10. Burkett E, Martin-Khan MG, Scott J, Samanta M, Gray LC. Trends and predicted trends in presentations of older people to Australian emergency departments: effects of demand growth, population aging and climate change. Aust Health Rev. 2016;41(3):246–253. doi:10.1071/AH15165
11. van Tiel S, Rood PP, Bertoli-Avella AM, et al. Systematic review of frequent users of emergency departments in non-US hospitals: state of the art. Eur J Emerg Med. 2015;22(5):306–315. doi:10.1097/MEJ.0000000000000242
12. Pines JM, Mullins PM, Cooper JK, Feng LB, Roth KE. National trends in emergency department use, care patterns, and quality of care of older adults in the United States. J Am Geriatr Soc. 2013;61(1):12–17. doi:10.1111/jgs.12072
13. Goodridge D, Stempien J. Understanding why older adults choose to seek non-urgent care in the emergency department: the patient’s perspective. Can J Emerg Med. 2019;21(2):243–248. doi:10.1017/cem.2018.378
14. Franchi C, Cartabia M, Santalucia P, et al. Emergency department visits in older people: pattern of use, contributing factors, geographical differences and outcomes. Aging Clin Exp Res. 2017;29:319–326. doi:10.1007/s40520-016-0550-5
15. Huang -H-H, Chang JC-Y, Tseng -C-C, et al. Comprehensive geriatric assessment in the emergency department for the prediction of readmission among older patients: a 3-month follow-up study. Arch Gerontol Geriatr. 2021;92:104255. doi:10.1016/j.archger.2020.104255
16. Legramante JM, Morciano L, Lucaroni F, et al. Frequent use of emergency departments by the elderly population when continuing care is not well established. PLoS One. 2016;11(12):e0165939. doi:10.1371/journal.pone.0165939
17. Samaras NMD, Chevalley TMD, Samaras DMD, Gold GMD. Older patients in the emergency department: a review. Ann Emerg Med. 2010;56(3):261–269. doi:10.1016/j.annemergmed.2010.04.015
18. Kaskie B, Obrizan M, Jones MP, et al. Older adults who persistently present to the emergency department with severe, non-severe, and indeterminate episode patterns. BMC Geriatr. 2011;11:1–10. doi:10.1186/1471-2318-11-65
19. McCusker J, Karp I, Cardin S, Durand P, Morin J. Determinants of emergency department visits by older adults: a systematic review. Acad Emerg Med. 2003;10(12):1362–1370. doi:10.1197/S1069-6563(03)00539-6
20. Cheung PT, Wiler JL, Lowe RA, Ginde AA. National study of barriers to timely primary care and emergency department utilization among Medicaid beneficiaries. Ann Emerg Med. 2012;60(1):4–10. e2. doi:10.1016/j.annemergmed.2012.01.035
21. Griffin E, McCarthy JP, Thomas F, Kingham S. New Zealand Healthline call data used to measure the effect of travel time on the use of the emergency department. Soc Sci Med. 2017;179:91–96. doi:10.1016/j.socscimed.2017.02.035
22. Lutz BJ, Hall AG, Vanhille SB, et al. A framework illustrating care-seeking among older adults in a hospital emergency department. Gerontologist. 2018;58(5):942–952. doi:10.1093/geront/gnx102
23. Ellis G, Marshall T, Ritchie C. Comprehensive geriatric assessment in the emergency department. Clin Interv Aging. 2014;9:2033. doi:10.2147/CIA.S29662
24. Carpenter CR, Shelton E, Fowler S, et al. Risk factors and screening instruments to predict adverse outcomes for undifferentiated older emergency department patients: a systematic review and meta‐analysis. Acad Emerg Med. 2015;22(1):1–21. doi:10.1111/acem.12569
25. Hastings SN, Heflin MT. A systematic review of interventions to improve outcomes for elders discharged from the emergency department. Acad Emerg Med. 2005;12(10):978–986. doi:10.1197/j.aem.2005.05.032
26. Lowthian J, Straney LD, Brand CA, et al. Unplanned early return to the emergency department by older patients: the Safe Elderly Emergency Department Discharge (SEED) project. Age Ageing. 2016;45(2):255–261. doi:10.1093/ageing/afv198
27. Nagurney JM, Fleischman W, Han L, Leo-Summers L, Allore HG, Gill TM. Emergency department visits without hospitalization are associated with functional decline in older persons. Ann Emerg Med. 2017;69(4):426–433. doi:10.1016/j.annemergmed.2016.09.018
28. De Brauwer I, Cornette P, D’Hoore W, et al. Factors to improve quality for older patients in the emergency department: a qualitative study of patient trajectory. BMC Health Serv Res. 2021;21(1):965. doi:10.1186/s12913-021-06960-w
29. Aminzadeh F, Dalziel WB. Older adults in the emergency department: a systematic review of patterns of use, adverse outcomes, and effectiveness of interventions. Ann Emerg Med. 2002;39(3):238–247. doi:10.1067/mem.2002.121523
30. Albert M, McCaig LF, Ashman JJ. Emergency Department Visits by Persons Aged 65 and Over: United States, 2009–2010. US Department of Health and Human Services, Centers for Disease Control; 2013.
31. Giroux M, Émond M, Nadeau A, et al. Functional and cognitive decline in older delirious adults after an emergency department visit. Age Ageing. 2021;50(1):135–140. doi:10.1093/ageing/afaa128
32. Salvi F, Morichi V, Grilli A, et al. Screening for frailty in elderly emergency department patients by using the Identification of Seniors At Risk (ISAR). J Nutr Health Aging. 2012;16(4):313–318. doi:10.1007/s12603-011-0155-9
33. de Carvalho IA, Epping-Jordan J, Pot AM, et al. Organizing integrated health-care services to meet older people’s needs. Bull World Health Organ. 2017;95(11):756. doi:10.2471/BLT.16.187617
34. Conneely M, Leahy S, Dore L, et al. The effectiveness of interventions to reduce adverse outcomes among older adults following emergency department discharge: umbrella review. BMC Geriatr. 2022;22(1):1–23. doi:10.1186/s12877-022-03007-5
35. Cassarino M, Robinson K, Quinn R, et al. Impact of early assessment and intervention by teams involving health and social care professionals in the emergency department: a systematic review. PLoS One. 2019;14(7):e0220709–e0220709. doi:10.1371/journal.pone.0220709
36. Wylie K, Crilly J, Toloo G, et al. Review article: emergency department models of care in the context of care quality and cost: a systematic review. Emerg Med Aust. 2015;27(2):95–101. doi:10.1111/1742-6723.12367
37. Cassarino M, Robinson K, Trépel D, et al. Impact of assessment and intervention by a health and social care professional team in the emergency department on the quality, safety, and clinical effectiveness of care for older adults: a randomised controlled trial. PLoS Med. 2021;18(7):e1003711. doi:10.1371/journal.pmed.1003711
38. Skivington K, Matthews L, Simpson SA, et al. A new framework for developing and evaluating complex interventions: update of medical research council guidance. BMJ. 2021;2021:374.
39. Conneely M, Leahy A, O’Connor M, et al. A physiotherapy-led transition to home intervention for older adults following emergency department discharge: protocol for a pilot feasibility randomised controlled trial. Pilot Feasibility Stud. 2022;8(1):3. doi:10.1186/s40814-021-00954-5
40. Thabane L, Ma J, Chu R, et al. A tutorial on pilot studies: the what, why and how. BMC Med Res Methodol. 2010;10(1):1. doi:10.1186/1471-2288-10-1
41. Eldridge SM, Chan CL, Campbell MJ, et al. CONSORT 2010 statement: extension to randomised pilot and feasibility trials. BMJ. 2016;355:i5239. doi:10.1136/bmj.i5239
42. Calvert M, Blazeby J, Altman DG, et al. Reporting of patient-reported outcomes in randomized trials: the CONSORT PRO extension. JAMA. 2013;309(8):814–822. doi:10.1001/jama.2013.879
43. Parenti N, Reggiani MLB, Iannone P, Percudani D, Dowding D. A systematic review on the validity and reliability of an emergency department triage scale, the Manchester Triage system. Int J Nurs Stud. 2014;51(7):1062–1069. doi:10.1016/j.ijnurstu.2014.01.013
44. McCusker J, Bellavance F, Cardin S, Trépanier S, Verdon J, Ardman O. Detection of older people at increased risk of adverse health outcomes after an emergency visit: the ISAR screening tool. J Am Geriatr Soc. 1999;47(10):1229–1237. doi:10.1111/j.1532-5415.1999.tb05204.x
45. Yao JL, Fang J, Lou QQ, Anderson RM. A systematic review of the identification of seniors at risk (ISAR) tool for the prediction of adverse outcome in elderly patients seen in the emergency department. Int J Clin Exp Med. 2015;8(4):4778–4786.
46. Mahoney FI, Barthel DW. Functional evaluation: the Barthel index. Md State Med J. 1965;14(2):61–65.
47. Herdman M, Gudex C, Lloyd A, et al. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual Life Res. 2011;20:1727–1736. doi:10.1007/s11136-011-9903-x
48. Rockwood K, Song X, MacKnight C, et al. A global clinical measure of fitness and frailty in elderly people. Cmaj. 2005;173(5):489–495. doi:10.1503/cmaj.050051
49. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383. doi:10.1016/0021-9681(87)90171-8
50. Bellelli G, Morandi A, Davis DH, et al. Validation of the 4AT, a new instrument for rapid delirium screening: a study in 234 hospitalised older people. Age Ageing. 2014;43(4):496–502. doi:10.1093/ageing/afu021
51. Kaiser MJ, Bauer JM, Ramsch C, et al. Validation of the Mini Nutritional Assessment Short-Form (MNA®-SF): a practical tool for identification of nutritional status. JNHA. 2009;13:782–788.
52. Taves DR. Minimization: a new method of assigning patients to treatment and control groups. Clin Pharmacol Ther. 1974;15(5):443–453. doi:10.1002/cpt1974155443
53. Efird J. Blocked randomization with randomly selected block sizes. Int J Environ Res Public Health. 2011;8(1):15–20. doi:10.3390/ijerph8010015
54. Conneely M, Boland P, O’Neill A, et al. A protocol for the establishment and evaluation of an older adult stakeholder panel for health services research [version 2; peer review: 2 approved]. HRB Open Res. 2020;3:1. doi:10.12688/hrbopenres.12979.1
55. Fried TR, Bradley EH, Williams CS, Tinetti ME. Functional disability and health care expenditures for older persons. Arch Intern Med. 2001;161(21):2602–2607. doi:10.1001/archinte.161.21.2602
56. Braun V, Clarke V. Thematic analysis; 2012.
57. Areán PA, Alvidrez J, Nery R, Estes C, Linkins K. Recruitment and retention of older minorities in mental health services research. Gerontologist. 2003;43(1):36–44. doi:10.1093/geront/43.1.36
58. Ory MG, Lipman PD, Karlen PL, et al. Recruitment of older participants in frailty/injury prevention studies. Prev Sci. 2002;3(1):1–22. doi:10.1023/A:1014610325059
59. Katula JA, Kritchevsky SB, Guralnik JM, et al. Lifestyle Interventions and Independence for Elders pilot study: recruitment and baseline characteristics. J Am Geriatr Soc. 2007;55(5):674–683. doi:10.1111/j.1532-5415.2007.01136.x
60. Rodrigues IB, Wang E, Keller H, et al. The MoveStrong program for promoting balance and functional strength training and adequate protein intake in pre-frail older adults: a pilot randomized controlled trial. PLoS One. 2021;16(9):e0257742. doi:10.1371/journal.pone.0257742
61. Walle-Hansen MM, Ranhoff AH, Mellingsæter M, Wang-Hansen MS, Myrstad M. Health-related quality of life, functional decline, and long-term mortality in older patients following hospitalisation due to COVID-19. BMC Geriatr. 2021;21(1):199. doi:10.1186/s12877-021-02140-x
62. Grund S, Caljouw MAA, Haaksma ML, et al. Pan-European study on functional and medical recovery and geriatric rehabilitation services of post-COVID-19 patients: protocol of the EU-COGER study. J Nutr Health Aging. 2021;25(5):668–674. doi:10.1007/s12603-021-1607-5
63. Poco PCE, Aliberti MJR, Dias MB, et al. Divergent: age, frailty, and atypical presentations of COVID-19 in hospitalized patients. J Gerontol. 2021;76(3):e46–e51. doi:10.1093/gerona/glaa280
64. Mendes A, Serratrice C, Herrmann FR, et al. Predictors of in-hospital mortality in older patients with COVID-19: the COVIDAge study. J Am Med Dir Assoc. 2020;21(11):1546–1554. e3. doi:10.1016/j.jamda.2020.09.014
65. Inzitari M, Arnal C, Ribera A, et al. Comprehensive Geriatric hospital at home: adaptation to referral and case-mix changes during the COVID-19 pandemic. J Am Med Dir Assoc. 2023;24(1):3–9. e1. doi:10.1016/j.jamda.2022.11.003
66. Pilotto A, Custodero C, Palmer K, et al. A multidimensional approach to older patients during COVID-19 pandemic: a position paper of the special interest group on comprehensive geriatric assessment of the European Geriatric Medicine Society (EuGMS). European Geriatric Medicine. 2023 2023. doi:10.1007/s41999-022-00740-3.
67. Sathyamurthy P, Madhavan S, Pandurangan V. Prevalence, pattern and functional outcome of post COVID-19 syndrome in older adults. Cureus. 2021;13(8):1.
68. Provencher V, Mortenson WB, Tanguay-Garneau L, Bélanger K, Dagenais M. Challenges and strategies pertaining to recruitment and retention of frail elderly in research studies: a systematic review. Arch Gerontol Geriatr. 2014;59(1):18–24. doi:10.1016/j.archger.2014.03.006
69. Yarmohammadian MH, Rezaei F, Haghshenas A, Tavakoli N. Overcrowding in emergency departments: a review of strategies to decrease future challenges. J Res Med Sci. 2017;22. doi:10.4103/1735-1995.200277
70. Di Somma S, Paladino L, Vaughan L, Lalle I, Magrini L, Magnanti M. Overcrowding in emergency department: an international issue. Intern Emerg Med. 2015;10(2):171–175. doi:10.1007/s11739-014-1154-8
71. Forsat ND, Palmowski A, Palmowski Y, Boers M, Buttgereit F. Recruitment and retention of older people in clinical research: a systematic literature review. J Am Geriatr Soc. 2020;68(12):2955–2963. doi:10.1111/jgs.16875
72. Harding S. Comprehensive geriatric assessment in the emergency department. Age Ageing. 2020;49(6):936–938. doi:10.1093/ageing/afaa059
73. Petty D, Zermansky A, Raynor D, et al. “No thank you”: why elderly patients declined to participate in a research study. Pharm World Sci. 2001;23(1):22–27. doi:10.1023/A:1011276924820
74. Tolmie EP, Mungall MM, Louden G, Lindsay GM, Gaw A. Understanding why older people participate in clinical trials: the experience of the Scottish PROSPER participants. Age Ageing. 2004;33(4):374–378. doi:10.1093/ageing/afh109
75. Vitale C, Fini M, Spoletini I, Lainscak M, Seferovic P, Rosano GM. Under-representation of elderly and women in clinical trials. Int J Cardiol. 2017;232:216–221. doi:10.1016/j.ijcard.2017.01.018
76. Strotmeyer ES, Arnold AM, Boudreau RM, et al. Long‐term retention of older adults in the cardiovascular health study: implications for studies of the oldest old. J Am Geriatr Soc. 2010;58(4):696–701. doi:10.1111/j.1532-5415.2010.02770.x
77. World Health Organization. Integrated care for older people: guidelines on community-level interventions to manage declines in intrinsic capacity; 2017.
78. Force GE, American College of Emergency Physicians, American Geriatrics Society, Emergency Nurses Association. Geriatric emergency department guidelines. Ann Emerg Med. 2014;63(5):e7–25. doi:10.1016/j.annemergmed.2014.02.008
79. Mooijaart SP, Nickel CH, Conroy SP, et al. A European research agenda for geriatric emergency medicine: a modified Delphi study. Eur Geriatr Med. 2021;12(2):413–422. doi:10.1007/s41999-020-00426-8
80. Nivestam A, Petersson P, Westergren A, Haak M. Older person’s experiences of benefits gained from the support and advice given during preventive home visits. Scand J Caring Sci. 2021;35(4):1096–1103. doi:10.1111/scs.12923
81. Elkan R, Egger M, Kendrick D, et al. Effectiveness of home based support for older people: systematic review and meta-analysisCommentary: when, where, and why do preventive home visits work? BMJ. 2001;323(7315):719. doi:10.1136/bmj.323.7315.719
82. Lippens T, Mackenzie CS. Treatment satisfaction, perceived treatment effectiveness, and dropout among older users of mental health services. J Clin Psychol. 2011;67(12):1197–1209.
83. de Labra C, Guimaraes-Pinheiro C, Maseda A, Lorenzo T, Millán-Calenti JC. Effects of physical exercise interventions in frail older adults: a systematic review of randomized controlled trials. BMC Geriatr. 2015;15(1):1–16. doi:10.1186/s12877-015-0155-4
84. Scholl I, Zill JM, Härter M, Dirmaier J. An integrative model of patient-centeredness–a systematic review and concept analysis. PLoS One. 2014;9(9):e107828. doi:10.1371/journal.pone.0107828
85. Hickman LD, Phillips JL, Newton PJ, Halcomb EJ, Al Abed N, Davidson PM. Multidisciplinary team interventions to optimise health outcomes for older people in acute care settings: a systematic review. Arch Gerontol Geriatr. 2015;61(3):322–329. doi:10.1016/j.archger.2015.06.021
86. Bayliss EA, Edwards AE, Steiner JF, Main DS. Processes of care desired by elderly patients with multimorbidities. Fam Pract. 2008;25(4):287–293. doi:10.1093/fampra/cmn040
87. Rennke S, Nguyen OK, Shoeb MH, Magan Y, Wachter RM, Ranji SR. Hospital-initiated transitional care interventions as a patient safety strategy: a systematic review. Ann Intern Med. 2013;158(5_Part_2):433–440. doi:10.7326/0003-4819-158-5-201303051-00011
88. Harvey G, Dollard J, Marshall A, Mittinty MM. Achieving integrated care for older people: shuffling the deckchairs or making the system watertight for the future? Int J Health Policy Manag. 2018;7(4):290. doi:10.15171/ijhpm.2017.144
89. Hall AG, Schumacher JR, Brumback B, et al. Health-related quality of life among older patients following an emergency department visit and emergency department-to-home coaching intervention: a randomized controlled trial. Int J Care Coord. 2017;20(4):162–170. doi:10.1177/2053434517733263
90. Hwang U, Hastings SN, Ramos K. Improving emergency department discharge care with telephone follow-up. Does it connect? J Am Geriatr Soc. 2018;66(3):436. doi:10.1111/jgs.15218
91. Salisbury C, Man M-S, Bower P, et al. Management of multimorbidity using a patient-centred care model: a pragmatic cluster-randomised trial of the 3D approach. Lancet. 2018;392(10141):41–50. doi:10.1016/S0140-6736(18)31308-4
92. Leithaus M, Beaulen A, de Vries E, et al. Integrated care components in transitional care models from hospital to home for frail older adults: a systematic review. Int J Integr Care. 2022;22(2):28. doi:10.5334/ijic.6447
93. Weeks LE, Macdonald M, Martin-Misener R, et al. The impact of transitional care programs on health services utilization in community-dwelling older adults: a systematic review. JBI Evid Synth. 2018;16(2):345–384.
94. Dorning H, Bardsley M. Focus On: Allied Health Professionals Can We Measure Quality of Care. London: The Health Foundation & The Nuffield Trust; 2014.
95. Campbell M, Fitzpatrick R, Haines A, et al. Framework for design and evaluation of complex interventions to improve health. BMJ. 2000;321(7262):694–696. doi:10.1136/bmj.321.7262.694
96. Shiell A, Hawe P, Gold L. Complex interventions or complex systems? Implications for health economic evaluation. BMJ. 2008;336(7656):1281–1283. doi:10.1136/bmj.39569.510521.AD
97. Stanley C, Kelly M, Elzaki M, Butler A, Condon F, Lenehan B. Lessons from lockdown: virtual clinics and service reorganisation in fracture management during COVID 19 experience of an Irish Regional Trauma Unit. Surgeon. 2021;19(6):e325–e330. doi:10.1016/j.surge.2021.02.006
98. Cummins NM, Garavan C, Barry LA, et al. The impact of COVID-19 on an Irish Emergency Department (ED): a cross-sectional study exploring the factors influencing ED utilisation prior to and during the pandemic from the patient perspective. BMC Emerg Med. 2022;22(1):1–11. doi:10.1186/s12873-022-00720-7
99. Hobbins A, Barry L, Kelleher D, et al. Utility values for health states in Ireland: a value set for the EQ-5D-5L. PharmacoEconomics. 2018;36:1345–1353. doi:10.1007/s40273-018-0690-x
100. Lee SY, Kim DY, Sohn MK, et al. Determining the cut-off score for the modified Barthel Index and the modified Rankin Scale for assessment of functional independence and residual disability after stroke. PLoS One. 2020;15(1):e0226324. doi:10.1371/journal.pone.0226324
101. Thabane L, Lancaster G. A guide to the reporting of protocols of pilot and feasibility trials. Pilot Feasibility Stud. 2019;5(1):37. doi:10.1186/s40814-019-0423-8
102. Powell L, Freedland KE, Kauffman P. Behavioral Clinical Trials for Chronic Diseases. Springer; 2020.
103. Freedland KE. Pilot trials in health-related behavioral intervention research: problems, solutions, and recommendations. Health Psychol. 2020;39(10):851. doi:10.1037/hea0000946
104. Mooijaart SP, Lucke JA, Brabrand M, Conroy S, Nickel CH. Geriatric emergency medicine: time for a new approach on a European level. LWW. 2019;2019:75–76.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.