Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
A Pharmacist-Led VTE Management Program in Orthopedic Surgery Associated with Reduced Venous Thromboembolism and Increased Pharmacological Prophylaxis: A Retrospective Study
Authors Wang Y, Liu S ![]() , Tang X, Huang G, Xi X, Zhu J, Du Q, Dong J
, Tang X, Huang G, Xi X, Zhu J, Du Q, Dong J
Received 24 July 2025
Accepted for publication 7 October 2025
Published 30 October 2025 Volume 2025:18 Pages 7049—7059
DOI https://doi.org/10.2147/JMDH.S555848
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Charles V Pollack
Yalan Wang,1,2 Songqing Liu,1 Xuejiao Tang,3 Guili Huang,1 Xin Xi,1 Jun Zhu,1 Qian Du,1,* Jie Dong1,*
1Pharmacy Department, The Third Affiliated Hospital of Chongqing Medical University, Chongqing, People’s Republic of China; 2College of Pharmacy, Chongqing Medical University, Chongqing, People’s Republic of China; 3Medical Administration Department, The Third Affiliated Hospital of Chongqing Medical University, Chongqing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jie Dong, Pharmacy Department, The Third Affiliated Hospital of Chongqing Medical University, Shuanghu Branch Road 1, Chongqing, People’s Republic of China, Email [email protected] Qian Du, Pharmacy Department, The Third Affiliated Hospital of Chongqing Medical University, Shuanghu Branch Road 1, Chongqing, People’s Republic of China, Email [email protected]
Purpose: This study aimed to develop and assess the impact of a pharmacist-led, technology-supported venous thromboembolism (VTE) management program on improving VTE prophylaxis and incidence in patients undergoing orthopaedic surgery.
Patients and Methods: This was a retrospective, observational study with a pre-post design conducted in the trauma and joint ward of the Orthopaedic Department of a tertiary hospital in Chongqing, China. Surgical patients were included from the period before (December 2022 to May 2023) and after (June to November 2023) the implementation of pharmacist-led VTE management program (PL-VTEMP), in which pharmacists conducted standardized VTE risk verification and proactive medication monitoring. Primary endpoints included VTE incidence and prophylactic pharmacotherapy rate. Multivariable logistic regression was used to adjust for potential confounders, along with an E-value analysis to assess robustness to unmeasured confounding.
Results: In total, 651 participants were included (322 in the pre-program group and 329 in the post-program group). Following the implementation of pharmacist-led VTE management program, the incidence of VTE decreased significantly (7.8% vs 2.7%, p = 0.004) and the proportion of patients receiving pharmacological prophylaxis increased significantly among high-risk patients in the post-program group (51.6% vs 33.9%, p < 0.01). The pharmacist-led VTE management program was identified as a protective factor for VTE prevention in multivariate regression model (OR 0.223, 95% confidence interval [CI] 0.093– 0.535). Despite the average duration of drug prophylaxis not significantly increased to match guideline recommendations (7.18 days vs 6.80 days, p > 0.05), the proportion of patients receiving oral sequential anticoagulants had risen (29.4% vs 2.3%, p < 0.001). No significant differences were observed in the incidence of bleeding.
Conclusion: This study demonstrated the benefits of pharmacist-led VTE management program as thromboprophylaxis in patients undergoing orthopaedic surgery. Clinical pharmacists have the potential to be core members of the VTE management team.
Keywords: pharmacist services, VTE, trauma orthopaedic, multidisciplinary management
Introduction
Venous thromboembolism (VTE), including pulmonary embolism (PE) and deep vein thrombosis (DVT), is a common complication in orthopedic patients and represents one of the potential causes of perioperative phase.1 Epidemiological studies in Asia have demonstrated that 41% of patients who did not receive thromboprophylaxis following knee or hip replacement surgery or hip fracture surgery developed VTE.2 Among hospitalized patients who developed VTE after joint replacement surgery, the mortality rate reaches up to 7.1% (1203/16,838).3 However, implementing standard preventive measures and treatment strategies can reduce the incidence of postoperative VTE to 6–12%.4,5
Pharmacists have been recommended to serve as facilitators or leaders in the Enhanced Recovery After Surgery (ERAS) programs, which included structured VTE management.6 This recognition was due to their critical role in medication therapy management (MTM), as well as the strong collaborative relationships they have developed through consistent communication and coordination with surgical stakeholders, including physicians, anesthesiologists, nurses, and administrative personnel. These measures, including medication review, patient education, medication consultation and post-discharge medication follow-up,7–12 have significantly enhanced VTE risk assessment rates, prophylaxis rates, and medication appropriateness in orthopedic.13–15 Furthermore, integrating health information technology with proactive pharmacist involvement has been shown to improve clinical outcomes by optimizing antimicrobial use and preventing drug-induced liver injury.16–19 Therefore, integrating electronic information monitoring platform and pharmacist-led services into VTE management shows promise.
Current published research on pharmacological services for VTE in orthopedics focuses on patients undergoing joint replacement surgery, as this procedure was strongly associated with a high risk of VTE.13,20 However, other non-major orthopedic procedures—such as fracture fixation, arthroscopy, and external fixation—also pose a risk of VTE, particularly when accompanied by additional risk factors (including advanced age, obesity, prolonged immobilization, malignancy, hormonal therapy and previous thrombosis history).21,22 Unfortunately, existing studies on pharmacological services in orthopedics have largely overlooked these patients. The Caprini Risk Assessment Model (RAM) comprehensively incorporates these multifactorial determinants, demonstrating high efficacy in identifying patients at high risk of VTE,23,24 offering a systematic and evidence-based approach to risk stratification in orthopedic pharmaceutical care.
Accordingly, we conducted an information technology-driven initiative that utilized automatic screening to identify and deliver pharmaceutical care to patients at risk of VTE, with a preliminary assessment of its outcomes.
Methods
Study Design and Setting
This retrospective, single-center, pre-post study was conducted in the trauma and joint ward of the Department of Orthopedics at a university-affiliated hospital. The ward consisted of two treatment groups: one admitting patients with trauma and the other admitting those with trauma with joint diseases. Each group was staffed by a dedicated team of orthopedic surgeons and adhered to standardized surgical protocols. PL-VTEMP spanned from June to November 2023, and the pre-program period was from December 2022. During the post-program period, PL-VTEMP was implemented on the ward. During the study period, all physicians and nurses in the department benefited from pharmaceutical care. All patients receiving pharmacist care were provided normal clinical treatment.
Participants
The study participants were comprised two groups according to the time of admission: a pre-program group, defined as all consecutive surgical patients admitted in the six months before the PL-VTEPM, and a post-program group, comprising those admitted in the first six months after implementation. The inclusion criteria were as follows: (1) patients aged 18 years or older; (2) surgical patients with a Caprini score indicating moderate-to-high VTE risk during hospitalization, where at least one assessment met the threshold. The exclusion criteria were as follows: (1) patients who required long-term antiplatelet or anticoagulant therapy and did not discontinue prior to admission; (2) patients with an admission diagnosis of venous thrombosis; and (3) Doppler ultrasonography of lower limbs within 24 hours of admission confirmed positive. The patient enrollment process is illustrated in Figure 1.
 |
Figure 1 Participants Enrollment Flowchart. Abbreviation: VTE, venous thromboembolism. |
Pharmacist-Led VTE Management Program
Information Technology Tools for Management Applications
Clinical pharmacists utilized two intelligent electronic systems for patients’ management. The PIP PASS Pharm Care (1.1.202303.03, Medicom Software, Sichuan, China) was employed to screen eligible patients, conduct pharmaceutical ward rounds, and provide pharmaceutical care and patient education, thereby enhancing workflow efficiency. The VTE Intelligent Decision Support System (VTE-IDSS) (V3.0–20220932, Dr. Breath. Com, Beijing, China) automatically assessed VTE and bleeding risks for hospitalized patients at regular intervals, with all assessment outcomes and preventive measures systematically recorded. Both systems underwent final commissioning in May 2022 and completed 6 months of operational stabilization before study initiation. The VTE-IDSS permitted manual adjustments to risk evaluations and prevention strategies, ensuring alignment with clinical requirements. Data from PIP PASS Pharm Care, VTE-IDSS, and the Hospital Information System (HIS) were cross-referenced during analysis.
Clinical Pharmacist Services
The ward was staffed with one senior clinical pharmacist and two clinical pharmacy interns. This team worked from Monday to Friday, dedicating 4 to 6 hours daily to serve the 40-bed ward. Clinical pharmacist operations were administered under the PL-VTEMP framework (Supplementary Figure 1) with oversight from administration department and implemented six protocol-defined components through the operational workflow (Figure 2): (1) validation of VTE-IDSS-generated risk assessments, (2) anticoagulant therapy optimization, (3) real-time adverse drug reaction monitoring with patient education, (4) clinician anticoagulation training, (5) multidisciplinary critical care coordination, and (6) quality improvement cycle implementation.
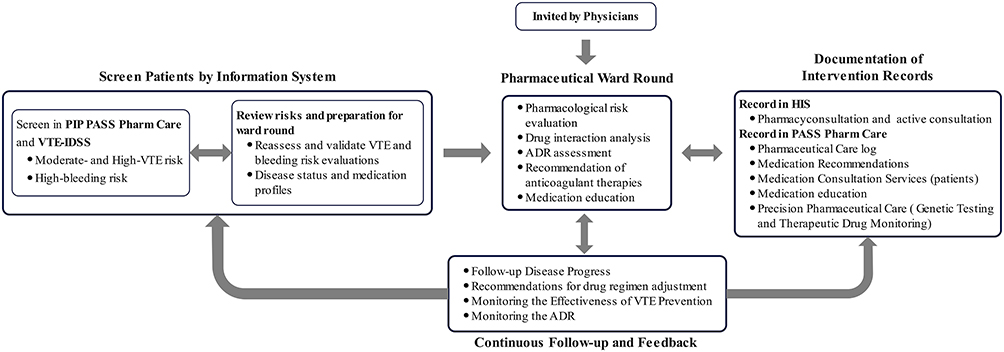 |
Figure 2 Workflow of pharmacists in PL-VTEMP. Abbreviations: PL-VTEMP, pharmacist-led VTE management program; PL-VTEMP, pharmacist-led VTE management program; ADR, Adverse Drug Reaction. |
The clinical pharmacists’ follow-up covered the entire hospitalization period. Using an electronic system, patients at moderate-to-high VTE risk—including those on anticoagulants or with special conditions such as renal or hepatic impairment—were proactively identified. After a comprehensive medical record review, individualized recommendations were provided. Each medication-related consultation or education session lasted approximately 15–20 minutes.
Definition and Data Collection
Data extracted from the HIS comprised demographic information (sex, age, diagnosis, surgery site, and length of hospitalization), VTE diagnosis, bleeding events and anticoagulant utilization records. The VTE-IDSS provided automated extraction of thromboembolic and hemorrhagic risk profiles. Data on clinical pharmacists’ workload were extracted from the PIP PASS pharmacy system and Hospital Information System (HIS), as detailed in Supplementary Table 2. DVT was confirmed by positive Doppler ultrasound in patients exhibiting lower extremity swelling or pain concurrent with elevated D-dimer levels. Thrombi distal to the popliteal vein were categorized as distal DVT. PE diagnosis relied on evaluation of clinical manifestations, laboratory findings, and Computed Tomography pulmonary angiography (CTPA). Bleeding events following anticoagulant therapy were assessed using HIS-documented clinical symptoms, fecal occult blood tests, urinalysis, hemoglobin measurements, and endoscopic reports. Major and non-major bleeding classifications adhered to the International Society on Thrombosis and Haemostasias (ISTH) guidelines. The prescription of oral anticoagulants at the time of discharge was defined as sequential oral therapy. Prophylactic pharmacotherapy was defined as anticoagulant drugs (low-molecular-weight heparins, unfractionated heparin, or fondaparinux) initiated within 24 hours post-VTE risk identification and maintained ≥3 consecutive days.
Study Outcomes
Primary outcome: The incidence of VTE and prophylactic pharmacotherapy rate.
Secondary outcomes: therapeutic duration, anticoagulants selection, sequential oral anticoagulants and ISTH-defined bleeding event.
Statistical Analysis
Statistical analyses were performed using SPSS Statistics 29.0 (IBM Corp). Continuous variables underwent analysis via parametric (Student’s t-test) or nonparametric (Mann–Whitney U) methods contingent upon distribution normality. Categorical variables were assessed using χ² or Fisher’s exact tests based on expected cell frequencies. Univariate logistic regression screened covariates for VTE prediction, with variables demonstrating α < 0.05 subsequently incorporated into multivariable logistic regression modeling. E-value analysis was employed to evaluate the potential impact of unmeasured confounding factors. Statistical significance was defined as two-tailed α = 0.05 throughout all inferential analyses.
Results
Demographic Characteristics
During the study period, a total of 867 consecutive patients were admitted to the trauma and joint ward, and 718 of them underwent surgery. Six hundred and fifty-one patients met the inclusion criteria, with 322 in the pre-program period and 329 in the post-program period. As summarized in Table 1, the pre-program group comprised 177 males and 145 females, with an average age of 56.48 years; The post-program group comprised 179 males and 150 females, with an average age of 56.99 years, with no significant difference between the two groups (p = 0.692). Additionally, there were no significant differences in the comorbidities counts. There were no significant differences in the surgical sites between the two groups (all p > 0.05).
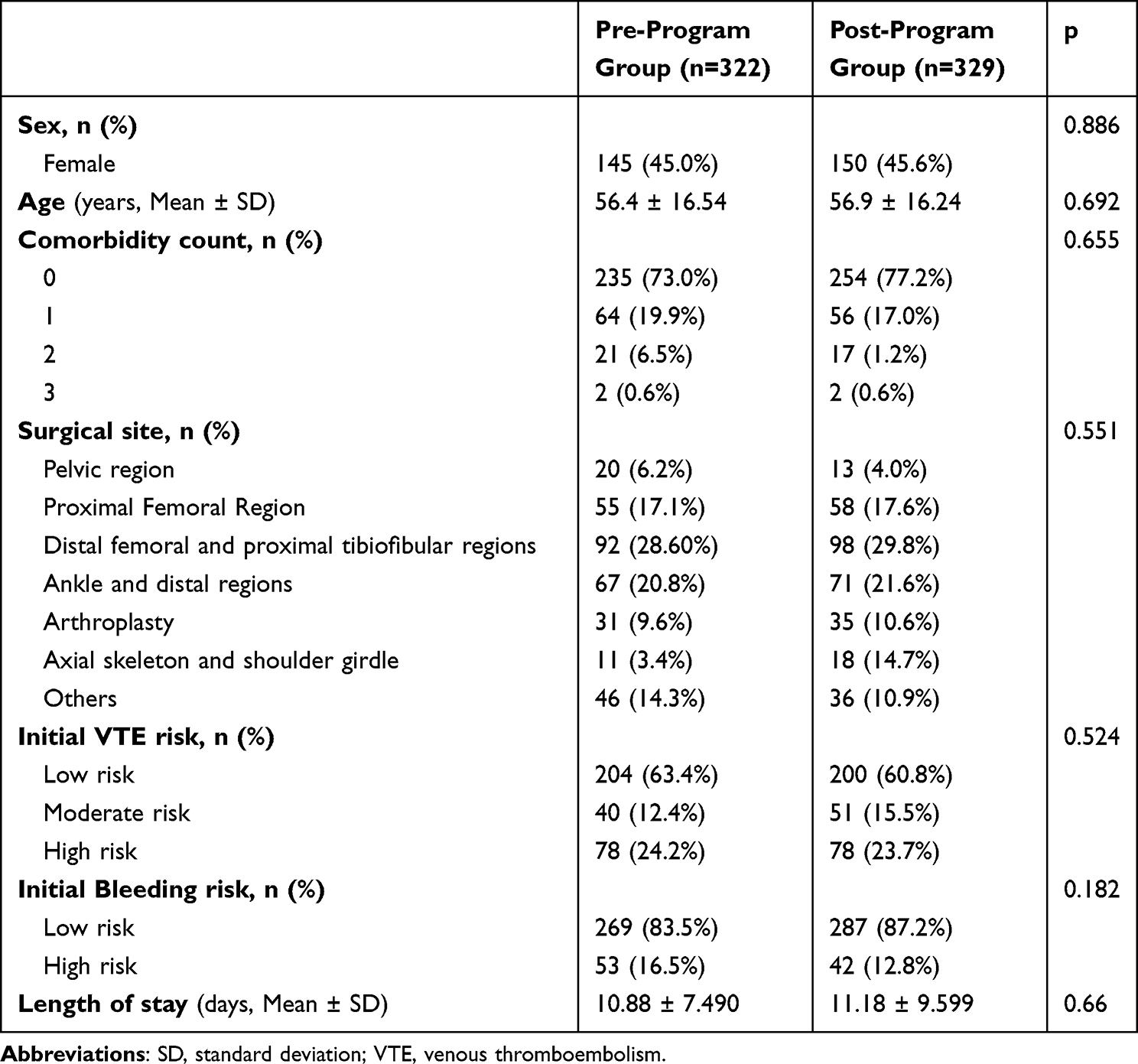 |
Table 1 Demographic Characteristics of the Subjects |
Logistic Regression Analysis
Univariate logistic regression identified four variables significantly associated with incidence of VTE (all p < 0.05): implementation of LP-VTEMP, age, initial VTE risk and length of stay. Multivariable logistic analysis identified protective effects of LP-VTEMP (OR 0.223, 95% confidence interval [CI] 0.093–0.535), indicating that the implementation of LPVTEMP was associated with an approximately 78% reduction in the odds of VTE occurrence. The protective effect was robust to potential unmeasured confounding, as supported by an E-value of 8.32 for a point estimate and 3.00 for the confidence interval limit. Advancing age (OR 1.054 per year, 95% CI 1.020–1.081) and prolonged length of stay (OR 1.125 per day, 95% CI 1.080–1.172) were independently associated with elevated VTE risk. No significant associations were observed with sex, comorbidity count, surgical site or baseline bleeding. The data of the logistic analysis were summarized in Table 2.
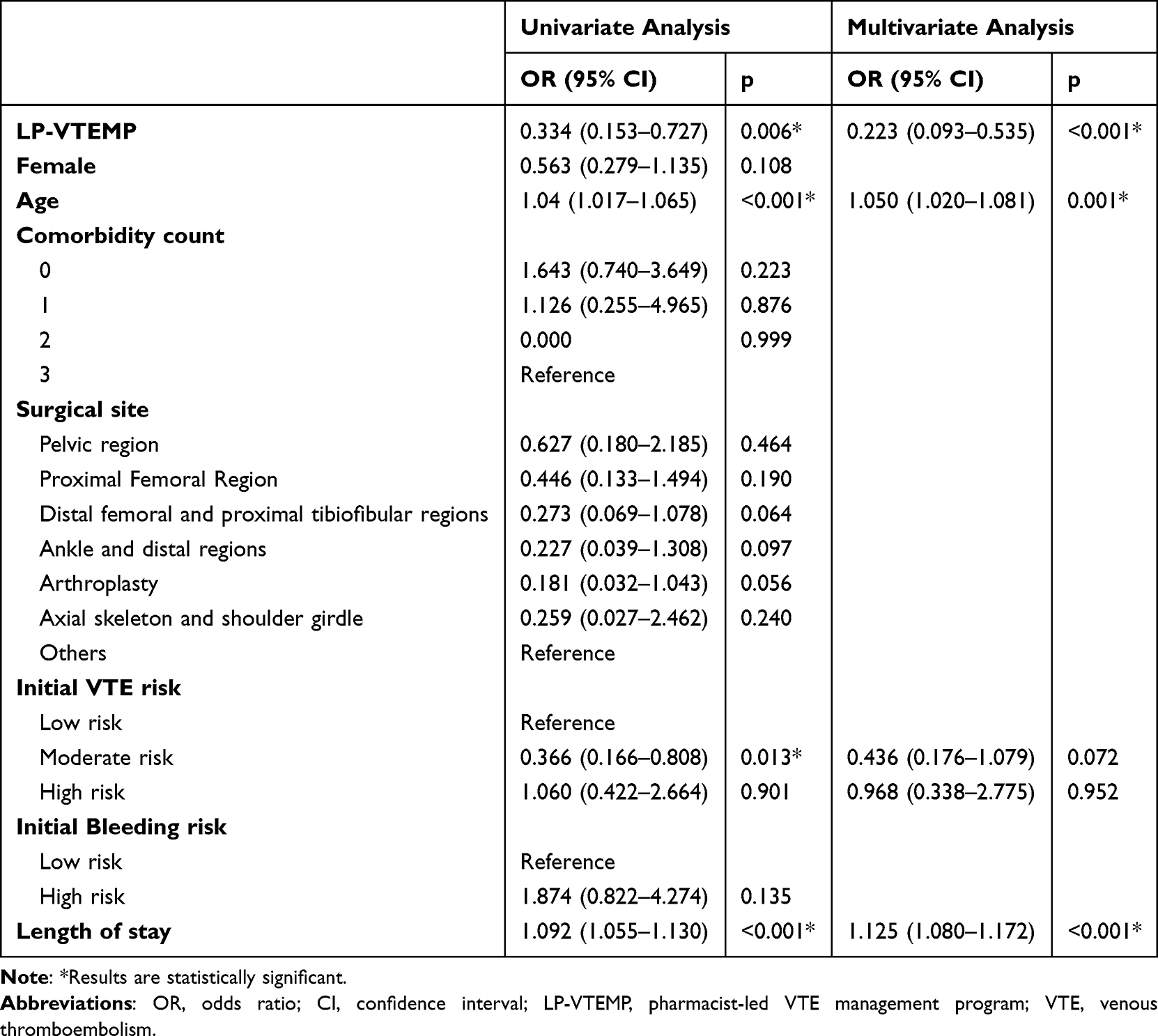 |
Table 2 Univariate Analysis and Multivariate Analysis of VTE-Related Risk Factors |
The Incidence of VTE and Prophylactic Pharmacotherapy Rate
A total of 25 patients manifested venous thrombosis on ultrasound during the hospital stay or before discharge in the pre-program period. In the post-program group, nine patients were indicated to have VTE, all of whom had distal DVT. The incidence of VTE was significantly lower in the post-program group than in the pre-program group (7.8% vs 2.7%, p = 0.004). The data are presented in Table 3.
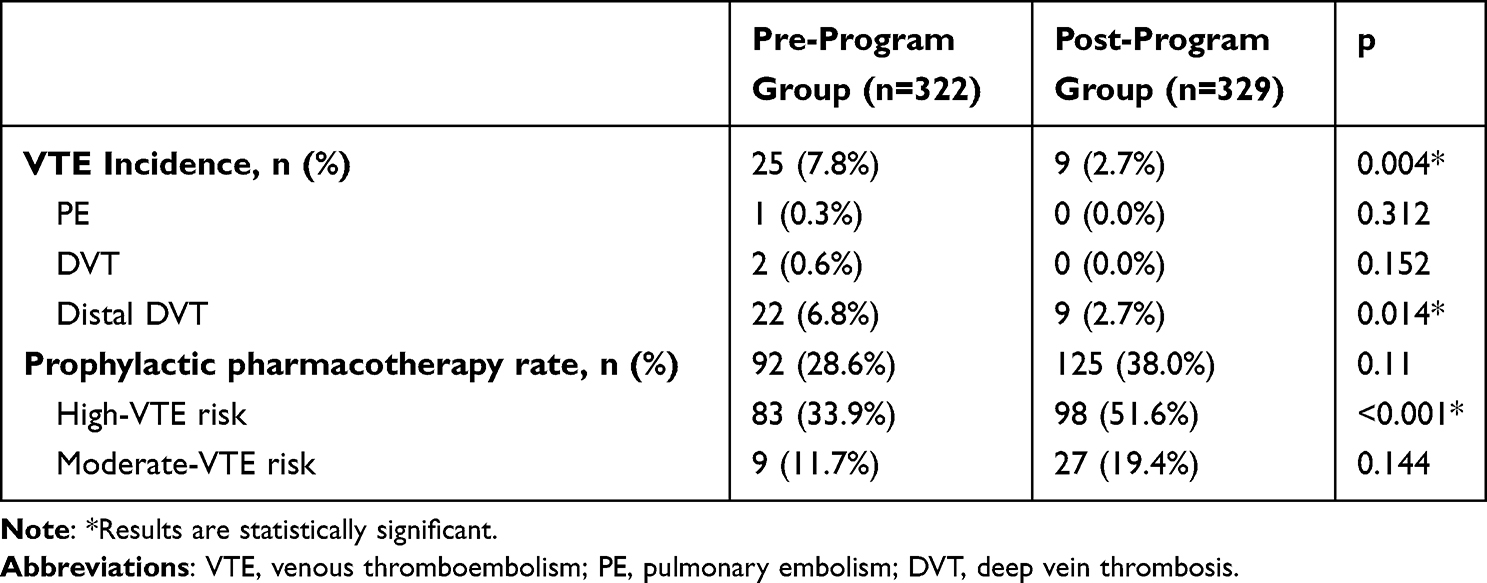 |
Table 3 VTE Incidence and Prophylactic Pharmacotherapy Rate |
Comparative analysis demonstrated a pharmacological prophylaxis rate of 38.0% during PL-VTEMP implementation compared to 28.6% at pre-program group, with not statistically significant between-group difference (p = 0.11). In high-VTE risk patients, the prophylactic pharmacotherapy rate in the post-program group was 51.6%, which was significantly higher than that in the pre-program group (33.9%; p < 0.01) (Table 3).
Implementation Efficiency of Pharmacological VTE Prophylaxis
The average duration of pharmacological prophylaxis for VTE was less than 10 days: 6.80 days and 7.18 days in the two groups, respectively (p > 0.05). Compared to the pre-program group, the proportion of patients in the post-program group who continued oral anticoagulants for post-discharge prophylaxis was significantly higher (2.3% vs 29.4%, p < 0.001) (Table 4).
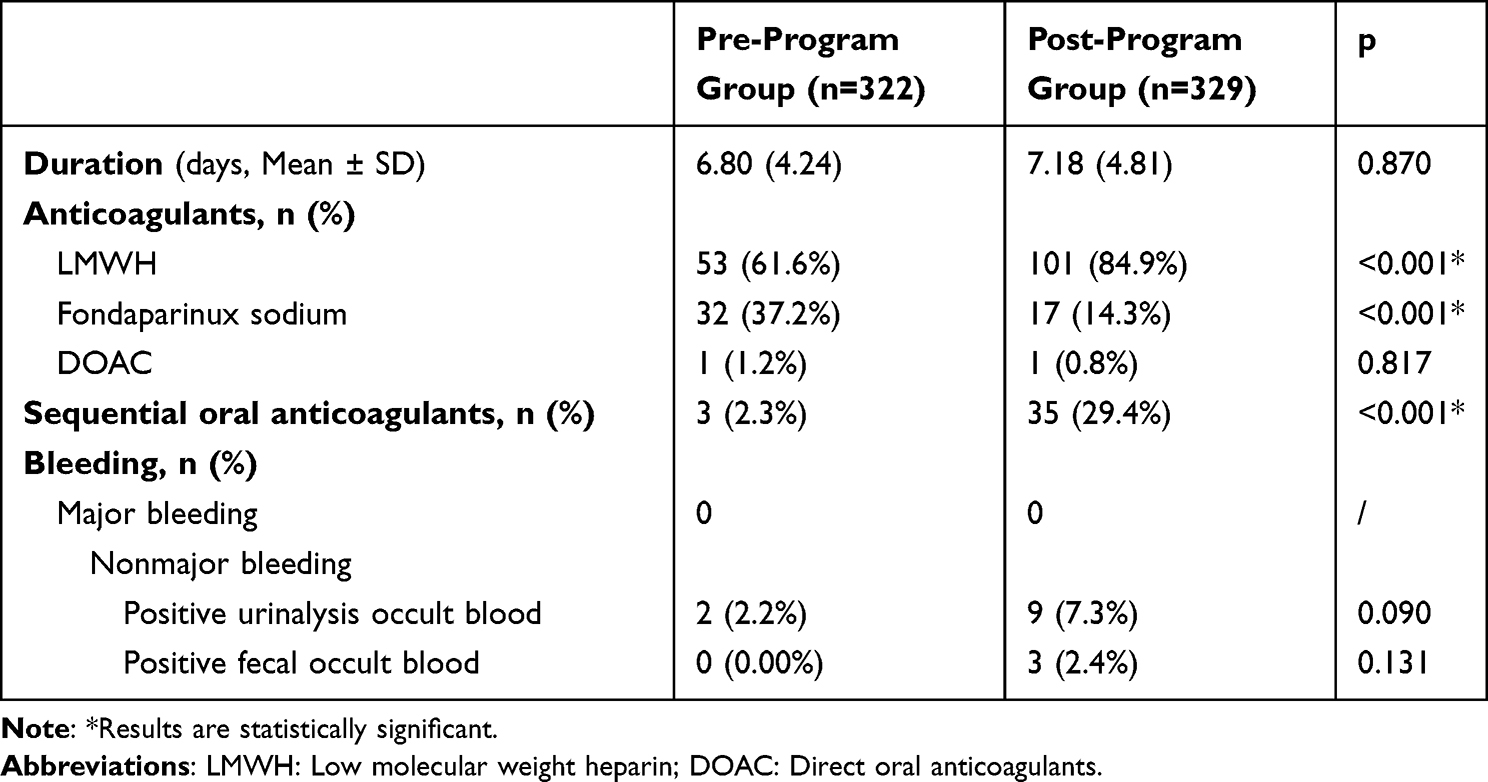 |
Table 4 Utilization of Prophylactic Anticoagulants |
Neither group showed any occurrence of gastrointestinal or intracranial hemorrhage. After the clinical pharmacist provided PL-VTEMP, urinalysis from nine patients indicated positive occult blood, three patients presented with positive fecal occult blood, and two patients in the pre-program group exhibited positive urinalysis for occult blood, with no patients showing positive fecal occult blood. There were no significant differences in bleeding between the two groups.
Discussion
Primary Outcomes of the Pharmacist-Led VTE Management Program
The PL-VTEMP, guided by Caprini risk stratification, established a novel pharmacotherapeutic pathway for multidisciplinary VTE management in orthopedic trauma. This program demonstrated lower VTE incidence (7.8% vs 2.7%, p = 0.004), and the prophylactic pharmacotherapy rate of high-risk patients in the post-program group was 51.6%, significantly higher than the 33.9% in the pre-program group (Table 3). Multivariate adjustment for confounding factors confirmed the independent protective effect of the program (OR 0.223, 95% CI 0.093–0.535) (Table 2).
Role of Caprini Score and Digital Tools in Precision Management
In accordance with the 2023 CHEST Guideline and ACCP Consensus,25,26 our study employed the Caprini Risk Assessment Model (RAM) through VTE-IDSS for automated VTE risk stratification in surgical populations. This selection aligns with evidence from Spencer et al, whose multicenter cohort study established a dose-response relationship between Caprini scores and VTE incidence (β = 1.32, 95% CI 1.18–1.47; p < 0.001).27 Notably, while current literature proposes elevated risk thresholds (8–10 points) for major orthopedic trauma patients with pelvic/hip fractures – given that these injuries intrinsically contribute 5 points on the Caprini scale28–30 – we maintained the guideline-recommended 5-point threshold to prioritize pharmaceutical care accessibility.
The utilization of an auxiliary decision-making system has been considered to enhance the prevention rate and reduce the incidence of VTE.31–34 In our study, clinical pharmacists reviewed the Caprini score calculated by the Dr. Breath system and found overestimations. The post-program group reviewed by clinical pharmacists had fewer high-risk VTE patients compared to the pre-program group (57.8% vs 76.1%, p < 0.01), and a higher proportion of moderate-risk patients (42.2% vs 23.9%, p < 0.01) (see Supplementary Table 1). The discrepancies stemmed from three factors: 1) the system assumed all surgical patients had bed rest or restricted mobility; 2) glucocorticoids use for anti-inflammatory purposes was misclassified as hormone replacement therapy; and 3) chronic ischemic stroke was incorrectly categorized as acute stroke (within 1 month). Consequently, the high-risk VTE proportion significantly decreased in the clinical pharmacist post-program group compared to the pre-program group (57.8% vs 76.1%, p < 0.001). These findings align with previous studies35 demonstrating that computerized VTE risk stratification based solely on Electronic Medical Records (EMR) data tends to be inaccurate, reinforcing that the face-to-face discussion Caprini score remains the most reliable method.36 While our intervention utilized a digital decision-support tool for efficiency, its core—standardized VTE risk assessment and pharmaceutical monitoring by trained clinical pharmacists—can be transferred to non-digital settings. Automated assessment and monitoring records can be substituted with standardized paper-based screening forms, structured medication reconciliation, and focused staff education to ensure feasibility, requiring additional personnel effort but demonstrating the program’s adaptability even in resource-limited environments.
The Value of Pharmacist Interventions
In the PL-VTEMP group, 38% of surgical patients with moderate-to-high VTE risk received pharmacological prophylaxis. This rate was notably lower than the 98.81% reported by Shang et al for postoperative TJA.9 The observed discrepancies may be attributed to multiple factors: 1) inclusion of diverse surgical procedures; 2) non-exclusion of patients with high bleeding risk; 3) omission of pharmacological prophylaxis for early mobilization (≤24 hours postoperatively); 4) limited intervention duration; and 5) insufficient clinical pharmacist staffing. Notably, among high-risk VTE patients, the PL-VTEMP demonstrated significantly improved pharmacological prophylaxis rates (51.6% vs 33.9%, p < 0.01), highlighting the clinical value of specialized pharmaceutical care. Although current prophylaxis rates remain suboptimal, the observed VTE incidence (2.7%) was substantially lower than the 29.6% reported in the previous literature.37 The enhanced outcomes may be partially explained by China’s national VTE prevention initiatives. Through policies established by the National Health Commission and Chinese Hospital Association, medical staff awareness has significantly increased. Consequently, basic preventive measures – including health education, ankle pump exercises, early ambulation, avoidance of lower extremity venous catheters, and breathing exercises – have become standard practice in our trauma and orthopedic units.38 Although the pre-program group VTE incidence was 7.8%, it was reduced to 2.7% after the implementation of the PL-VTEPM, corresponding to an absolute risk reduction of approximately 5 events per 100 patients. This not only markedly improves patient safety but also translates to substantial cost savings, averting over $60,000 in treatment costs alone given that each VTE event costs $12400-13900 to manage, further demonstrating the benefits of pharmacist-led anticoagulation management in cost-effectiveness and patient outcomes.39
In our study, no major bleeding events occurred in either group. Minor bleeding incidence showed no statistically significant difference between groups (urine occult blood positivity: 2.2% vs 7.3%, p = 0.09; stool occult blood positivity: 0% vs 2.4%, p = 0.13). Notably, the post-program group demonstrated numerically higher bleeding occurrences. This trend may reflect intensified monitoring through PL-VTEMP, where increased surveillance frequency naturally elevates detection rates. Importantly, clinical pharmacists’ expertise in anticoagulant management effectively counterbalanced this detection bias, maintaining comparable bleeding outcomes between groups - a protective effect well documented in existing literature.9,17,40,41
According to a meta-analysis,42 the peak risk of VTE occurs within two weeks following major orthopedic surgery and persists for five weeks postoperatively. Current evidence-based guidelines recommend pharmacological prophylaxis durations of 10–35 days.25 In our study, both groups had an average treatment duration of approximately one week, with no statistically significant difference (6.80 days vs 7.18 days, p = 0.870). In our study, both groups demonstrated comparable short-term prophylaxis (mean 6.80 vs 7.18 days, p = 0.870), potentially caused by similar lengths of stay (10.88 vs 11.18 days, p = 0.660). The absence of pharmacological prophylaxis in some patients stemmed from initial low-risk classifications via RAM. Post-discharge oral anticoagulant continuation rates emerged as a surrogate marker for prophylaxis duration, revealing dramatic intergroup disparity: post-program group patients demonstrated 8.9-fold higher compliance than pre-program group (29.4% vs 3.3%, p < 0.001). This improvement directly demonstrates the PL-VTEMP program’s potential in discharge medication reconciliation, personalized OAC adherence monitoring, and scheduled telemedicine consultations.
Study Limitations and Future Perspectives
Our study has five limitations. Firstly, the retrospective observational design inherently restricted data comprehensiveness, particularly regarding unmeasured confounders. Certain biases cannot be avoided. Secondly, short intervention duration hindered full assessment of longitudinal effects and late-onset complications. Extended-duration studies were needed to evaluate treatment outcomes’ long-term sustainability. Thirdly, pharmacist workforce constraints limited full protocol adherence monitoring, as evidenced by the intervention data in Supplementary Table 2. It is important to note that these same constraints also meant we could not implement a structured follow-up timeline. Fourthly, the regression analysis did not comprehensively consider potential factors influencing VTE occurrence, nor did it systematically assess the appropriateness of drug selection or the timing of initiation during the perioperative period, which may have constrained the optimization effectiveness of the PL-VTEMP. Fifth, the constraints of the electronic data extraction system precluded the collection of granular data on individual VTE risk factors, thereby necessitating our reliance on the aggregated Caprini risk scores rather than their specific components. We are currently conducting prospective clinical studies to address these limitations and to validate the impact of PL-VTEMP.
Conclusion
In summary, the PL-VTEMP implementing exhibited clinically meaningful outcomes in trauma and orthopedic populations. Clinical pharmacists have the potential to be core members of the VTE management team. Prospective multicenter studies are warranted to establish its clinical utility as a standardized thromboprophylaxis strategy.
Ethics Approval and Consent to Participate
This study was conducted with approval from the Ethical Committee of the Third Affiliated Hospital of Chongqing Medical University (Approval No. 2023-26) and adhered to the principles of the Declaration of Helsinki. The Ethics Committee granted a waiver of informed consent due to the retrospective nature of the clinical data and minimal study risks (no greater than routine health screenings).
Acknowledgments
We thank all the medical staff from The Orthopedic Department of Third Affiliated Hospital of Chongqing Medical University for their support during the project.
Funding
This work was supported by Technical Foresight and Institutional Innovation Project from The Science and Technology Bureau of Yuzhong District, Chongqing, China [grant number: 20210102], Medical Research Program under the Chongqing Municipal Health Commission [grant number: 2025WSJK101], The Clinical Pharmacy Priority Construction Project of The Chongqing Health Commission, and the Chongqing Graduate Student Research Innovation Project from Chongqing Municipality Education Commission [grant number: CYS240329].
Disclosure
The authors report no conflicts of interest in this work.
References
1. Zhai Z, Kan Q, Li W, et al. VTE risk profiles and prophylaxis in medical and surgical inpatients: the identification of Chinese hospitalized patients’ risk profile for venous thromboembolism (DissolVE-2)-A cross-sectional study. Chest. 2019;155(1):114–122. doi:10.1016/j.chest.2018.09.020
2. Piovella F, Wang CJ, Lu H, et al. Deep-vein thrombosis rates after major orthopedic surgery in Asia. An epidemiological study based on postoperative screening with centrally adjudicated bilateral venography. J Thromb Haemost. 2005;3(12):2664–2670. doi:10.1111/j.1538-7836.2005.01621.x
3. Shahi A, Bradbury TL, Guild GN, Saleh UH, Ghanem E, Oliashirazi A. What are the incidence and risk factors of in-hospital mortality after venous thromboembolism events in total Hip and knee arthroplasty patients? Arthroplast Today. 2018;4(3):343–347. doi:10.1016/j.artd.2018.02.014
4. Kahn SR, Morrison DR, Diendéré G, et al. Interventions for implementation of thromboprophylaxis in hospitalized patients at risk for venous thromboembolism. Cochrane Database Syst Rev. 2018;4(4):CD008201. doi:10.1002/14651858.CD008201.pub3
5. Zhang S, Htet KS, Tan XY, Wang X, Wang W, Chua W. Short-duration chemoprophylaxis might reduce incidence of deep vein thrombosis in Asian patients undergoing total knee arthroplasty. Knee Surg Relat Res. 2020;32(1):58. doi:10.1186/s43019-020-00077-w
6. Lovely JK, Hyland SJ, Smith AN, Nelson G, Ljungqvist O, Parrish RH. Clinical pharmacist perspectives for optimizing pharmacotherapy within enhanced recovery after surgery (ERAS((R))) programs. Int J Surg. 2019;63:58–62. doi:10.1016/j.ijsu.2019.01.006
7. Parrish RH, Findley R, Elias KM, et al. Pharmacotherapeutic prophylaxis and post-operative outcomes within an enhanced recovery after surgery (ERAS®) program: a randomized retrospective cohort study. Ann Med Surg Lond. 2022;73:103178. doi:10.1016/j.amsu.2021.103178
8. Quintens C, Verhamme P, Vanassche T, et al. Improving appropriate use of anticoagulants in hospitalised patients: a pharmacist-led check of medication appropriateness intervention. Br J Clin Pharmacol. 2022;88(6):2959–2968. doi:10.1111/bcp.15184
9. Shang J, Ning W, Gong J, Su D, Jia X, Wang Y. Impact of clinical pharmacist services on anticoagulation management of total joint arthroplasty: a retrospective observational study. J Clin Pharm Ther. 2021;46(5):1301–1307. doi:10.1111/jcpt.13428
10. Lachuer C, Benzengli H, Do B, Rwabihama JP, Leglise P. Oral anticoagulants: interventional pharmaceutical study with reminder of good practices, and iatrogenic impact. Ann Pharm Fr. 2021;79(4):409–417. doi:10.1016/j.pharma.2021.01.004
11. Kiracı ZK, Yalçın N, Cennet Ö, Demirkan K, Yorgancı K. Education and clinical pharmacist-led management strategies for the risk and prophylaxis of venous thromboembolism in general surgery. Thromb J. 2023;21(1):86. doi:10.1186/s12959-023-00530-2
12. Liu X, Xiao Q, Li Y, Hu G, Kun W, Xu W. Effect of post-discharge pharmacist-led follow-up on drug treatment in patients with deep venous thrombosis in primary hospitals in China. Pak J Pharm Sci. 2022;35(3):785–791.
13. Hyland SJ, Kramer BJ, Fada RA, Lucki MM. Clinical pharmacist service associated with improved outcomes and cost savings in total joint arthroplasty. J Arthroplasty. 2020;35(9):2307–2317.e1. doi:10.1016/j.arth.2020.04.022
14. Cronin M, Hill T, Reich DA, Pinard B, Krauss ES. Implementation of a multidisciplinary, pharmacy-led, thromboprophylaxis program in total-joint arthroplasty patients. Am J Health Syst Pharm. 2009;66(2):171–175. doi:10.2146/ajhp070660
15. Tortolano L, Misandeau Q, Inouri T, et al. Patient information pathway in orthopedic surgery: roles of ERAS and pharmacists. Orthop Traumatol Surg Res. 2023;109(8):103576. doi:10.1016/j.otsr.2023.103576
16. Karajizadeh M, Hassanipour S, Sharifian R, Tajbakhsh F, Saeidnia HR. The effect of information technology intervention on using appropriate VTE prophylaxis in non-surgical patients: a systematic review and meta-analysis. Digit Health. 2022;8:20552076221118828. doi:10.1177/20552076221118828
17. Hou K, Yang H, Ye Z, Wang Y, Liu L, Cui X. Effectiveness of pharmacist-led anticoagulation management on clinical outcomes: a systematic review and meta-analysis. J Pharm Pharm Sci. 2017;20(1):378–396. doi:10.18433/J3SQ0B
18. Li D, Dong J, Xi X, et al. Impact of pharmacist active consultation on clinical outcomes and quality of medical care in drug-induced liver injury inpatients in general hospital wards: a retrospective cohort study. Front Pharmacol. 2022;13:972800. doi:10.3389/fphar.2022.972800
19. Du Q, Xi X, Dong J, et al. The impact of pharmacist early active consultation (PEAC) on multidrug resistance organism treatment outcomes: a prospective historically controlled study. Front Pharmacol. 2023;14:1128219. doi:10.3389/fphar.2023.1128219
20. Tong K, Liu H, Qin J, et al. Current status survey of the extramural hospital management of venous thromboembolism after total Hip and knee arthroplasty in China. BMC Musculoskelet Disord. 2021;22(1):787. doi:10.1186/s12891-021-04663-1
21. Bassa B, Little E, Ryan D, et al. VTE rates and risk factors in major trauma patients. Injury. 2024;55(12):111964. doi:10.1016/j.injury.2024.111964
22. Saragas NP, Ferrao PN, Saragas E, Jacobson BF. The impact of risk assessment on the implementation of venous thromboembolism prophylaxis in foot and ankle surgery. Foot Ankle Surg. 2014;20(2):85–89. doi:10.1016/j.fas.2013.11.002
23. Zhang X, Hao A, Lu Y, Huang W. Deep vein thrombosis and validation of the Caprini risk assessment model in Chinese orthopaedic trauma patients: a multi-center retrospective cohort study enrolling 34,893 patients. Eur J Trauma Emerg Surg. 2023;49(4):1863–1871. doi:10.1007/s00068-023-02265-1
24. Lobastov K, Urbanek T, Stepanov E, et al. The thresholds of caprini score associated with increased risk of venous thromboembolism across different specialties: a systematic review. Ann Surg. 2023;277(6):929–937. doi:10.1097/SLA.0000000000005843
25. Falck-Ytter Y, Francis CW, Johanson NA, et al. Prevention of VTE in orthopedic surgery patients: antithrombotic therapy and prevention of thrombosis, 9th ed: American college of chest physicians evidence-based clinical practice guidelines. Chest. 2012;141(2 Suppl):e278S–e325S. doi:10.1378/chest.11-2404
26. Anderson DR, Morgano GP, Bennett C, et al. American society of hematology 2019 guidelines for management of venous thromboembolism: prevention of venous thromboembolism in surgical hospitalized patients. Blood Adv. 2019;3(23):3898–3944. doi:10.1182/bloodadvances.2019000975
27. Wilson S, Chen X, Cronin M, et al. Thrombosis prophylaxis in surgical patients using the caprini risk score. Curr Probl Surg. 2022;59(11):101221. doi:10.1016/j.cpsurg.2022.101221
28. Qiao L, Yao Y, Wu D, et al. The validation and modification of the caprini risk assessment model for evaluating venous thromboembolism after joint arthroplasty. Thromb Haemost. 2024;124(3):223–235. doi:10.1055/a-2122-7780
29. Qiao L, Yao Y, You X, et al. Identifying high-risk groups for deep vein thrombosis after primary total knee arthroplasty using preoperative Caprini scores and D-dimer levels. J Orthop Surg Res. 2024;19(1):616. doi:10.1186/s13018-024-05074-3
30. Krauss ES, Segal A, Cronin M, et al. Implementation and validation of the 2013 caprini score for risk stratification of arthroplasty patients in the prevention of venous thrombosis. Clin Appl Thromb Hemost. 2019;25:1076029619838066. doi:10.1177/1076029619838066
31. Umscheid CA, Hanish A, Chittams J, Weiner MG, Hecht TEH. Effectiveness of a novel and scalable clinical decision support intervention to improve venous thromboembolism prophylaxis: a quasi-experimental study. BMC Med Inform Decis Mak. 2012;12(1):92. doi:10.1186/1472-6947-12-92
32. Bahl V, Moote MJ, Hu HM, Campbell DA. Impact of clinical decision support with mandatory versus voluntary venous thromboembolism risk assessment in hospitalized patients. TH Open. 2024;8(3):e317–e328. doi:10.1055/s-0044-1790519
33. Galanter WL, Thambi M, Rosencranz H, et al. Effects of clinical decision support on venous thromboembolism risk assessment, prophylaxis, and prevention at a university teaching hospital. Am J Health Syst Pharm. 2010;67(15):1265–1273. doi:10.2146/ajhp090575
34. Borab ZM, Lanni MA, Tecce MG, Pannucci CJ, Fischer JP. Use of computerized clinical decision support systems to prevent venous thromboembolism in surgical patients: a systematic review and meta-analysis. JAMA Surg. 2017;152(7):638–645. doi:10.1001/jamasurg.2017.0131
35. He L, Luo L, Hou X, et al. Predicting venous thromboembolism in hospitalized trauma patients: a combination of the Caprini score and data-driven machine learning model. BMC Emerg Med. 2021;21(1):60. doi:10.1186/s12873-021-00447-x
36. Pannucci CJ, Fleming KI. Comparison of face-to-face interaction and the electronic medical record for venous thromboembolism risk stratification using the 2005 Caprini score. J Vasc Surg Venous Lymphat Disord. 2018;6(3):304–311. doi:10.1016/j.jvsv.2017.10.016
37. Sun N, Yang F, Li Y, Liu J, Liu Y, Wang M. Study of a preoperative deep venous thrombosis predictor score for patients with fresh lower extremity fractures. Zhonghua Wai Ke Za Zhi. 2015;53(2):101–105.
38. Gonzalez Della Valle A, Shanaghan KA, Nguyen J, et al. Multimodal prophylaxis in patients with a history of venous thromboembolism undergoing primary elective Hip arthroplasty. Bone Joint J. 2020;102-B(7_Supple_B):71–77. doi:10.1302/0301-620X.102B7.BJJ-2019-1559.R1
39. Howell CW, Walroth TA, Beam DM, et al. Pharmacoeconomic, medication access, and patient-satisfaction analysis of a pharmacist-managed VTE clinic compared to primary care physician outpatient therapy. J Pharm Pract. 2020;35(2):212–217. doi:10.1177/0897190020966210
40. Bailly R, Wuyts S, Toelen L, et al. Introducing a pharmacist-led transmural care program to reduce drug-related problems in orthogeriatric patients: a prospective interventional study. BMC Geriatr. 2024;24(1):47. doi:10.1186/s12877-023-04591-w
41. Xie C, Mu X, Hu Z, et al. Impact of pharmaceutical care in the orthopaedic department. J Clin Pharm Ther. 2020;45(3):401–407. doi:10.1111/jcpt.13091
42. Sobieraj DM, Lee S, Coleman CI, et al. Prolonged versus standard-duration venous thromboprophylaxis in major orthopedic surgery: a systematic review. Ann Intern Med. 2012;156(10):720–727. doi:10.7326/0003-4819-156-10-201205150-00423
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.