Back to Journals » Journal of Hepatocellular Carcinoma » Volume 12
A Patient Charter to Improve Care for Hepatocellular Carcinoma
Authors Hassan Y, Kautz A, James C, Lee D, Langenbacher D, Bouffet E, Chakowa J, Hicks J, Ward JW, Kuschnereit LA ![]() , Allaire M, Zhang T
, Allaire M, Zhang T ![]() , Huang Chi Z
, Huang Chi Z
Received 4 March 2025
Accepted for publication 30 July 2025
Published 20 August 2025 Volume 2025:12 Pages 1849—1859
DOI https://doi.org/10.2147/JHC.S526170
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr David Gerber
Yasmine Hassan,1,* Achim Kautz,2,* Cary James,3,* Dee Lee,4,* Diane Langenbacher,2,* Eric Bouffet,5,* Jade Chakowa,6,* Jessica Hicks,3,* John W Ward,7,8,* Lili Anna Kuschnereit,9,* Manon Allaire,10,* Tingting Zhang,11,* Zeena Huang Chi1,*
1Department of Global Policy, Advocacy and Health Equity, AstraZeneca, Gaithersburg, MD, USA; 2International Liver Cancer Movement, Cologne, Germany; 3World Hepatitis Alliance, Geneva, Switzerland; 4Inno Asia, Guangzhou, People’s Republic of China; 5Division of Paediatric Oncology/Haematology, The Hospital for Sick Children, The University of Toronto, Toronto, Canada; 6The Hepatitis Fund, Geneva, Switzerland; 7Coalition for Global Hepatitis Elimination, Task Force for Global Health, Decatur, GA, USA; 8Hubert Department of Global Health, Rollins School of Public Health, Emory University, Atlanta, GA, USA; 9Digestive Cancers Europe, Brussels, Belgium; 10Service d’Hépato-gastroentérologie, Hôpital Universitaire Pitié-Salpêtrière, AP-HP Sorbonne Université, Paris, France; 11Hear2Care, Spokane, WA, USA
*These authors contributed equally to this work
Correspondence: Zeena Huang Chi, AstraZeneca, 1 MedImmune Way, Gaithersburg, MD, 20878, USA, Email [email protected]
Purpose: To establish a patient charter that articulates the principles of quality care for individuals living with hepatocellular carcinoma (HCC), aiming to improve patient outcomes and survival rates globally.
Methods: A multidisciplinary group comprising healthcare professionals, patient advocacy representatives, and policymakers convened to identify the critical areas of unmet need in HCC care. The group shared patient experiences, barriers, and insights – particularly with input from Patient Advocacy Groups (PAGs) – to better understand the challenges faced by patients. They reviewed existing literature, current care practices, and patient experiences to formulate a patient charter that outlines the principles of quality care for HCC.
Results: The patient charter identifies the seven principles of quality care that people with HCC or at risk of developing HCC should expect to receive in order to benefit from improved outcomes and increased survival. These principles address the need for policy prioritization, early diagnosis, multidisciplinary care, personalized treatment, shared decision-making, stigma-free access to services and increased research funding.
Conclusion: The patient charter serves as a call to action for stakeholders to unite in enhancing the care and treatment of HCC, with the ultimate goal of improving health outcomes for patients.
Keywords: hepatocellular carcinoma, liver cancer, patient care, health policy, multidisciplinary team
Introduction
HCC represents a significant global health challenge, accounting for approximately 80% of primary liver cancer diagnoses,1 with an estimated 866,136 new cases reported in 2022 and 758,725 deaths worldwide.2,3 The disease has a marked gender disparity, with men being two to four times more likely to develop HCC than women and also experience higher mortality rates.4
The pathogenesis of HCC is closely linked to chronic liver disease, particularly cirrhosis. Major risk factors for cirrhosis and HCC include metabolic syndrome (diabetes mellitus, Metabolic dysfunction-associated steatotic liver disease (MASLD), previously termed Non-Alcoholic Fatty Liver Disease (NAFLD), obesity, excessive alcohol consumption or chronic Hepatitis B (HBV) and Hepatitis C virus (HCV) infection.5 Additionally, individuals with HBV infection who are coinfected with hepatitis D virus (HDV) often experience accelerated liver disease progression, leading to an earlier onset of HCC compared to monoinfection with other hepatitis viruses.6
Despite the existence of treatment strategies that offer a good likelihood of cure when initiated at early stages,7 the majority of HCC patients are diagnosed at advanced stages of the disease.8 This is particularly concerning given that risk populations are well-defined and diagnostic tools are both available and affordable.
The objective of this patient charter is to outline the principles of quality care that individuals with HCC should expect to receive, with the aim of enhancing outcomes and survival rates. It serves as a call to action for governments, healthcare providers, policymakers, medical societies, guideline panels, patient advocacy groups, and those affected by HCC to collectively address the unmet needs and burdens associated with HCC. Through collaborative efforts, we aim to achieve meaningful improvements in HCC care now and for future generations.
The patient charter outlines seven key principles aimed at improving care for individuals with HCC. The patient charter’s principles address the need for policy prioritization, early diagnosis, multidisciplinary care, personalized treatment, shared decision-making, stigma-free access to services, and increased research funding.
Material and Methods
Working Group Formation
The HCC patient charter was developed through a series of multidisciplinary consultations and roundtable discussions with clinicians, patient advocacy groups and healthcare professionals from across the globe. The aim was to ensure a comprehensive and representative set of principles that reflect the needs and experiences of individuals affected by HCC. The International Liver Cancer Movement (ILCM) played a pivotal role in this process, collaborating closely with us to create the charter and contributing their expertise as chairs of discussions during one of the roundtables.
Literature Review, Advocacy Advisory Board and Formulation of the Patient Charter
A literature review was conducted with the objectives of identifying current unmet needs in HCC care worldwide, understanding existing advocacy efforts, and examining best practices from other disease areas where patient charters have successfully driven change. This review provided a foundational understanding to inform the development of the patient charter.
In April 2024, an Advocacy Advisory Board was formed, comprising representatives from PAGs. The board discussed the major unmet needs in HCC as reported by the patient, clinical and advocacy community to develop specific principles to be included in the patient charter. The board reached a consensus on priority areas of unmet need, which were subsequently addressed in the patient charter’s principles.
Following this, desk research was conducted to draft these principles. To validate and refine the draft principles, two multidisciplinary roundtables were held in September 2024 at the European Society for Medical Oncology (ESMO) and the World Cancer Congress (WCC). The goal was to align the patient charter with the broader HCC community’s perspectives and initiate planning for its launch and dissemination.
Results
Principle 1: Patients Need Liver Cancer to Be Prioritized by Policymakers and Addressed in National Cancer Strategies. This Includes Grasping the Opportunity to Prevent Many HCC Cases by Eliminating Viral Hepatitis as a Public Health Threat by 2030, Which Would Significantly Reduce Mortality, Improve Quality of Life and Lower Healthcare Costs
Despite HCC being the most common type of primary liver cancer,9 few policymakers prioritize HCC prevention, screening and treatment. In countries such as the United Kingdom (UK) and United States (US) – as in much of the world – HCC is often overshadowed by other cancers with more established advocacy, such as breast, colorectoral and lung cancers.10 Yet, HCC is among the most preventable cancers. A coordinated, strategic response is essential to address this growing public health challenge.
Effective national strategies should begin with prevention and early detection. Public health campaigns must raise awareness of key risk factors, including harmful alcohol use and metabolic syndrome, while ensuring equitable access to preventive services. Central to these efforts are widespread HBV vaccination and the scaling up of testing and treatment for HBV, HDV, and HCV. These measures are not only cost-effective but lifesaving. For example, large-scale HBV vaccination and HCV antiviral therapy programs in regions such as sub-Saharan Africa, Hong Kong, Shanghai, Japan, Taiwan, Egypt and Singapore have already contributed to a 20% reduction in HCC incidence.11,12 Despite this progress, the World Health Organization (WHO) has acknowledged that the global community is falling short of its 2030 viral hepatitis elimination targets. This highlights the need for urgent policy action. National cancer control plans must integrate HCC prevention, including expanded vaccination programs, access to curative antiviral therapies, investment in research and innovation, and public education campaigns. Without such concerted efforts, the global burden of HCC will continue to rise, and the opportunity to save thousands of lives will be lost.
Principle 2: Patients Need Timely Access to an Early and Accurate Diagnosis and Assessment of Their HCC, Leading to Timely Intervention and with That Improved Survival
HCC is frequently diagnosed at an advanced stage, with studies estimating that 25% to 70% of patients are identified too late, rendering the disease incurable.13 This underscores the critical need for effective national screening programs targeting high-risk populations, which can significantly improve early detection, survival outcomes and reduce the overall disease burden. Moreover, timely diagnosis through structured surveillance may help address persistent ethnic, racial and socioeconomic disparities in HCC outcomes.14,15
In the US, for instance, HCC disproportionately affects racial and ethnic minority groups – often linked to broader social determinants of health and systemic barriers, including limited healthcare access in immigrant and underserved communities.16 Establishing comprehensive screening and surveillance systems is essential to mitigate these disparities and ensure more equitable care.14
The success of HCC surveillance depends on several factors: the availability and acceptability of reliable diagnostic tools, timely access to treatment, healthcare provider awareness, and seamless integration into routine clinical workflows.17 While the evidence base for HCC surveillance remains limited, the consistently high mortality associated with late-stage diagnosis has led leading international societies including European Association for the Study of the Liver (EASL),18 American Association for the Study of Liver Disease (AASLD),19 Asia-Pacific Association for the Study of the Liver (APASL)20 and Asociación Latinoamericana para el Estudio del Hígado (ALEH)21 – to recommend routine surveillance in at-risk individuals. This typically involves ultrasound imaging every six months, often coupled with - alpha-fetoprotein (AFP) blood testing.19 Eligible populations include individuals with chronic liver disease, viral hepatitis,19 MASLD, or a family history of HCC.22
Despite these guidelines, HCC surveillance remains underutilized in practice.23,24 Screening uptake is frequently suboptimal or absent altogether, particularly in regions lacking formal national programs.25 Disparities in implementation between specialized and non-specialized centers further contribute to delayed diagnoses. In response, EASL has urged the European Commission to incorporate HCC screening into Europe’s Beating Cancer Plan, aiming to establish consistent, continent-wide surveillance protocols.26
Principle 3: Patients Need Access to a Multidisciplinary Team to Provide Comprehensive Care, Considering Both the Liver Condition and Cancer Treatment
Multidisciplinary teams or at least its principles are critical in HCC care. They can provide a comprehensive evaluation of the HCC, develop personalized treatment plans and have been shown to improve patient quality of life and overall outcomes.27 These teams enable thorough assessment of both liver function and tumor burden, allowing for tailored therapeutic strategies. Core members typically include epidemiologists, hepatologists or gastroenterologists, radiologists, interventional radiologists, pathologists, transplant and hepatobiliary surgeons, oncologists, surgical oncologists, endoscopists, clinical pharmacologists, nutritionists, palliative care specialists, psychologists, physiotherapists, and nurse navigators.28 Patient support groups and advocacy organizations also play a critical role in patient empowerment and shared decision-making.
Multidisciplinary care can be delivered at varying levels of complexity and integration. At its most basic, it involves coordinated access to relevant subspecialists within the same health system, facilitating sequential consultations. A more structured model is the multidisciplinary tumor board, in which cases are collaboratively reviewed by experts across disciplines to develop consensus treatment plans. The most integrated model features co-located multidisciplinary HCC clinics, where real-time interaction among specialists enhances communication, speeds up decision-making, and streamlines care delivery.18,19,29,30
Each level of multidisciplinary engagement offers benefits, and health systems should aim to implement the highest level of integration possible, adapted to local resources and patient needs. Major clinical guidelines – including those from the AASLD, Barcelona Clinic Liver Cancer (BCLC) group, the APASL, and the EASL – emphasize the central role of multidisciplinary care in HCC management.18,19,29,30 These guidelines consistently associate multidisciplinary care with improved treatment efficacy and patient-centered outcomes.
Despite its recognized value, access to multidisciplinary care remains uneven due to systemic barriers, including funding constraints, workforce shortages, and limited institutional capacity.31,32 Furthermore, key operational details – such as identifying which patient populations benefit most, the optimal team composition, and measurable clinical outcomes – require further clarification.33
Access to multidisciplinary care should be guaranteed for all patients with HCC, regardless of geographic location.34 In regions where in-person multidisciplinary teams are not feasible, telemedicine and virtual tumor boards can help extend this collaborative model of care to underserved areas, improving equity and access to high-quality treatment.
Principle 4: Patients Need Personalized Care Which Considers Their Unique Needs and Preferences: Considering Personal Milestones and Treatment Goals
Personalized care is fundamental to optimizing outcomes for patients with HCC. Recognizing that every patient is unique, this approach tailors treatment plans to align with each individual’s specific needs, preferences and circumstances.
Personalized care for people with HCC involves crafting management strategies that consider multiple factors: a patient’s overall health status, liver function (whether cirrhotic or non-cirrhotic, and whether compensated or decompensated), the size, location, and spread of the cancer, co-morbidities, mental health needs, lifestyle and social circumstances.35 Personalized care in HCC must be grounded in a thorough understanding of patient characteristics and preferences that directly inform treatment selection. While HCC predominantly affects older adults – the mean ages of diagnosis with HCC were 55–59 years in China and 63–65 years in Europe and North America12 – there is a notable subset of younger patients, particularly in regions with endemic hepatitis B, where a greater number of HCC cases may occur in individuals at earlier ages.12 For these younger patients, long-term life planning considerations, such as fertility preservation, can significantly influence treatment choices.36 Cultural background, language proficiency, health literacy, and individual beliefs also shape treatment preferences and engagement.37 By integrating these factors into care planning, clinicians can ensure that treatment strategies align not only with clinical needs but also with what matters most to each patient.
Successful implementation of personalized approaches can lead to improved health outcomes, more efficient healthcare service use, and a reduction in health inequalities.38 Personalized care can also lead to reduced anxiety, quicker recovery and improved adherence to treatment programs, especially in cases where accepting language is effectively utilized.35
Every patient diagnosed with HCC should have access to an individualized care plan that reflects their unique medical and personal context, ensuring that clinical decisions are made not only for patients – but with them. Given the heterogeneity of HCC, a one-size-fits-all approach is insufficient.39 Tailored care allows patients to receive treatments that are better suited to their specific disease state and personal goals.
Healthcare professionals should be equipped to deliver care that is both clinically appropriate and emotionally supportive. This includes training in communication, cultural sensitivity and shared decision making.40 Maintaining patient privacy and dignity, particularly during sensitive discussions, is crucial.
Empowering patients through supported self-management is also vital. Education about the disease, symptom management, and treatment options enables individuals to play an active role in their care, improving quality of life and treatment engagement. Connecting patients with peer mentors, survivor networks, or support groups further reinforces agency and confidence in the care process.
Principle 5: Patients Need Shared Decision-Making to Be Recognized and Implemented During Their Treatment Pathway
Shared decision-making is a collaborative and empowering process where HCPs and patients jointly make care and treatment decisions, considering the diagnosis, specific disease features, personal circumstances, lifestyle and preferences. This is a continuous process, as preferences and needs can change over time.
Effective shared decision-making is essential for optimizing outcomes in HCC. Leading guidelines from the AASLD,19 the EASL,18 the APASL,41 BCLC29 and the ALEH,21 suggest that HCC care decisions should be made collaboratively, considering individual preferences, overall health and treatment goals.9
Research indicates that shared decision-making can significantly enhance patient quality of life, improve clinical outcomes, increase adherence to treatment plans, and even prolong survival.42,43 By engaging patients in the decision-making process, healthcare providers can ensure that treatment strategies align with the patient’s values, priorities, and long-term goals.
Despite the benefits, many patients with HCC do not feel adequately informed to participate in their care decisions. Studies have found that up to two-thirds of people with HCC report not receiving enough information about their condition.44 This knowledge gap can prevent patients from engaging meaningfully in discussions about their treatment options.
To enable effective shared decision-making, patients must be fully informed about the risks, benefits and alternatives of each treatment option. Open dialogue should be encouraged to address patient concerns and questions. Providing clear, patient-centered information is crucial – this includes using language that is understandable, accommodating different languages or dialects, and utilizing visual aids where necessary to support comprehension.44
Patients should also be connected to support networks, such as survivor groups or peer mentors, who can provide additional guidance and information. These resources should be integrated into the patient care pathway to support ongoing decision-making.
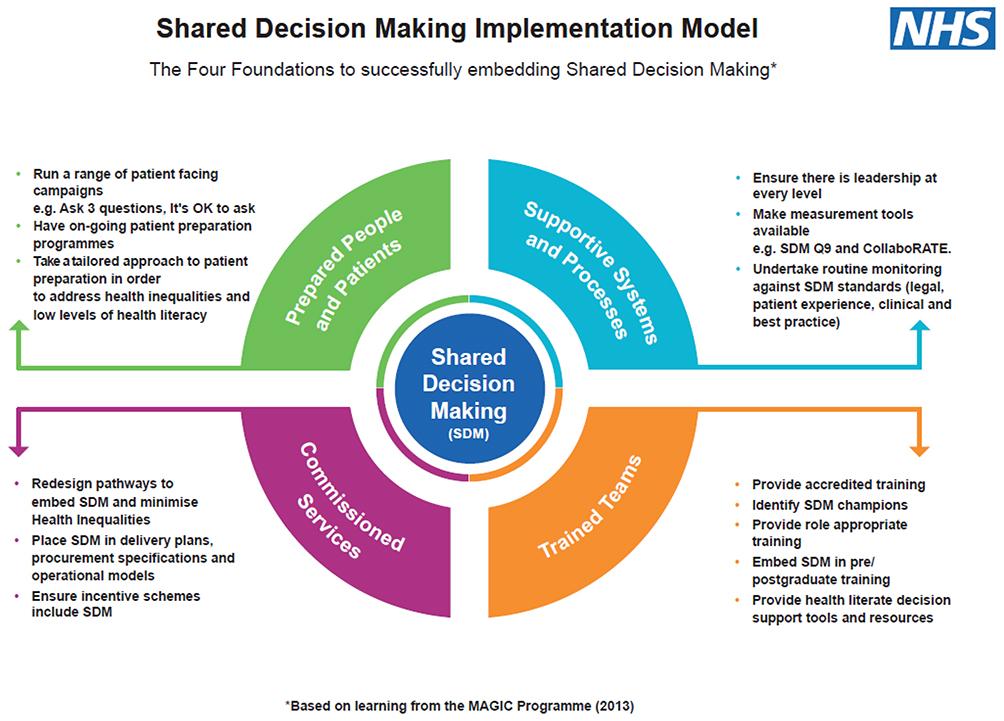 |
Figure 1 Example of a Shared Decision-Making Implementation Model – NHS England. Reprinted from NHS England. How to make shared decision making happen. 2025. Available from: https://www.england.nhs.uk/personalisedcare/shared-decision-making/how-to-make-shared-decision-making-happen/. Creative Commons.45 |
Healthcare providers should implement shared decision-making tools to facilitate discussions about patient preferences, values, and priorities (see Figure 1 for an example of a shared decision-making implementation model45). Information and decision aids, such as brochures, videos, audio resources, and online tools, can empower patients, caregivers, and families to actively participate in decision-making.9
Principle 6: Patients Need Access to Early Detection Services, Care, and Treatment Without Being Stigmatized
Access to early detection and timely care for HCC should not be hindered by stigma. However, stigma remains a significant barrier for many patients, often rooted in widespread misconceptions about the causes of HCC.
Many people associate HCC with lifestyle factors, such as heavy alcohol use, injection drug use, obesity or smoking.46 These misconceptions can perpetuate negative stereotypes, making patients reluctant to seek help due to fear of judgment or social stigma. This can discourage individuals from undergoing necessary screening and surveillance for liver disease, delaying diagnosis and leading to higher mortality.47,48
Stigma not only impacts the psychological well-being of patients but also places a social and economic burden on their families. The fear of being judged can prevent patients from accessing essential healthcare services, ultimately contributing to poorer health outcomes. Storytelling and shared experiences can play a powerful role in reducing stigma and amplifying awareness. Programs like the Hepatitis B Foundation’s #justB and B the Voice campaigns49 have demonstrated the impact of sharing real-life stories from patients and caregivers. These initiatives humanize the experience of living with hepatitis B and liver disease, helping to break down misconceptions and promote understanding.
Reducing stigma requires sustained public education to correct false beliefs and emphasize that liver disease affects people of all backgrounds – not just those with certain behaviors. Normalizing routine screening and early surveillance for at-risk populations is key to reducing disparities and improving outcomes.
Emotional support is also critical. Patient advocacy groups, support networks, and survivor communities offer vital psychosocial resources that help individuals and families navigate the emotional impact of diagnosis, including depression and isolation.50
Comprehensive care must also address nutritional needs. Proper dietary guidance can slow disease progression, prevent complications, and improve quality of life.51 Addressing the financial challenges faced by patients and caregivers is equally important, as economic strain can further compromise access to care and health outcomes.52
Principle 7: Patients Need a Commitment to Increased Funding and Further Research for HCC
HCC requires increased research funding and resources to drive advances in care. Despite being one of the deadliest cancers, HCC remains underfunded compared to other cancers (as shown in Figure 2),53 which hampers progress in improving patient outcomes.
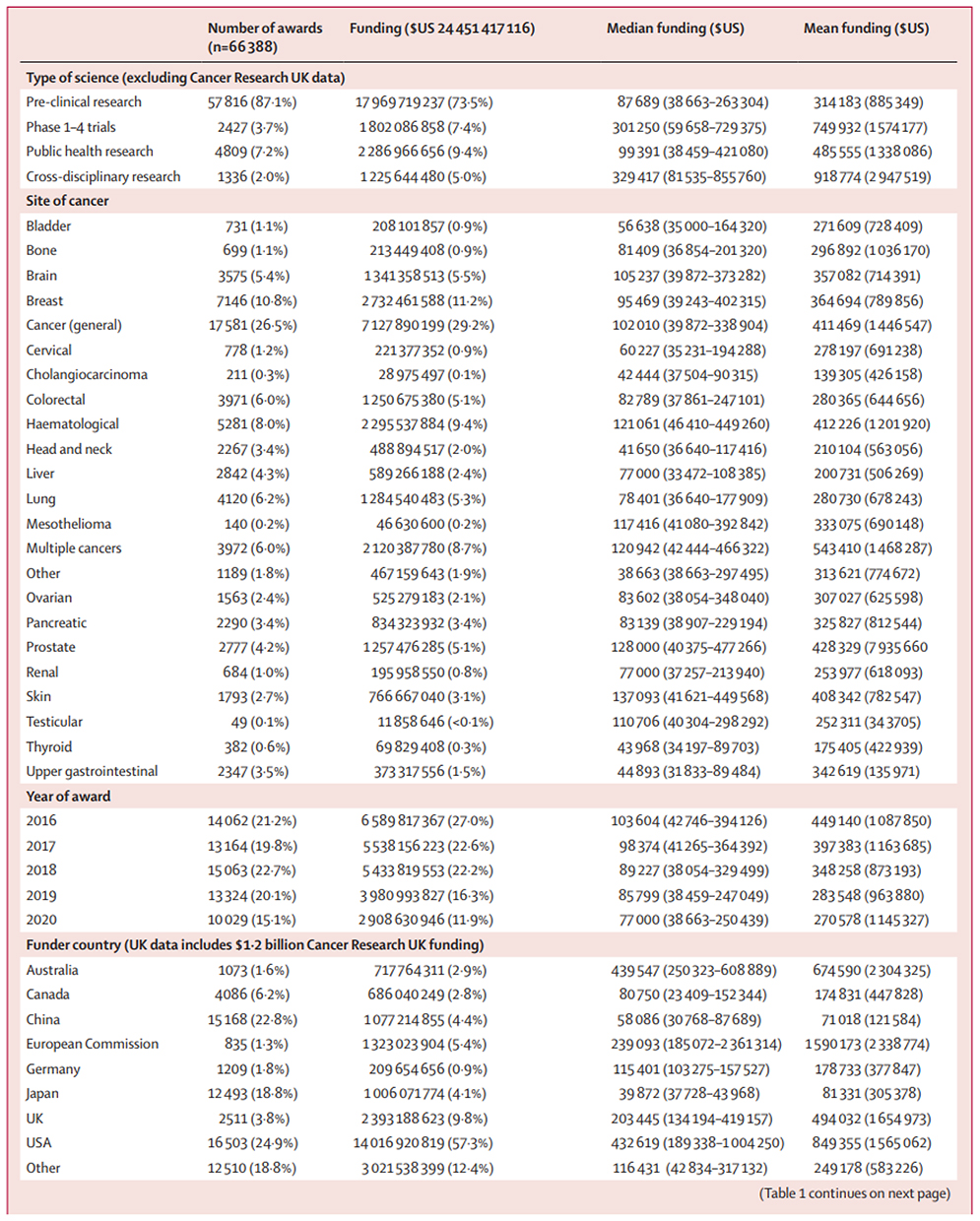 |
Figure 2 Awards for cancer research between Jan 1, 2016 and Dec 31, 2020. Adapted from McIntosh SA, Alam F, Adams L, et al. Global funding for cancer research between 2016 and 2020: a content analysis of public and philanthropic investments. Lancet Oncol. 2023;24(6):636–645. Creative Commons.53 |
Current investment in HCC research is disproportionately low, especially in low- and middle-income countries, where the burden of liver cancer is highest. The majority of research funding for cancer biology is concentrated in high-income countries, yet regional differences in HCC suggest that findings from these studies may not be universally applicable.53 Prioritizing HCC research on a global scale is essential to address disparities and ensure that advancements benefit all populations.
Addressing gaps in diagnostics, treatments and data collection is crucial to advancing care for HCC. Currently, there is no consensus on the most effective screening methods for early detection of HCC. This gap highlights the urgent need for additional research to validate novel biomarkers, genetic tests and advanced imaging techniques that could improve early diagnosis. Early detection remains key to optimizing patient outcomes, as a significant proportion of HCC cases are diagnosed at advanced stages, when curative options are limited. In parallel, research into targeted therapies, particularly systemic and immune-based treatments, is progressing; however, there remains insufficient data linking specific molecular profiles to the most effective therapies. This limitation underscores the need for personalized approaches in HCC treatment, where care can be tailored based on the genetic and molecular characteristics of a patient’s tumor. To achieve this, more studies are required to delineate how distinct molecular signatures influence treatment responses, allowing clinicians to select the most appropriate therapies for each patient.
Moreover, enhancing data collection through comprehensive national and international registries is essential to improving our understanding of treatment outcomes. Currently, there is limited data on how various clinical factors, such as underlying liver disease etiology – whether viral hepatitis or MASLD – affect responses to HCC treatments. Systematic collection of this information will not only inform evidence-based guidelines but also support the development of tailored management strategies. Investing in robust data infrastructure will enable a deeper analysis of real-world patient outcomes, therefore refining therapeutic approaches and improving long-term survival rates for HCC patients.54
Limitations
The development of this patient charter was shaped by a collaborative process involving clinical experts, patient advocates, and stakeholders, including industry representatives. While this inclusive approach enriched the content and ensured a broad perspective, it also introduced certain limitations. Although every effort was made to maintain the independence and integrity of the charter’s content, the potential for bias arising from industry involvement cannot be entirely excluded. Additionally, while the charter reflects current best practices and expert consensus, it may not capture the full diversity of experiences across all regions, healthcare systems, or patient populations. Further validation through wider public and professional engagement is encouraged to enhance the charter’s applicability and inclusivity.
Conclusion
HCC represents a major burden for millions of people worldwide, significantly affecting their quality of life, mental health, and overall well-being. It also places considerable strain on healthcare systems, with late-stage diagnoses and inconsistent access to effective treatments exacerbating the issue.
The principles and recommendations outlined in this paper highlight the essential components of quality care for people living with HCC. We urge healthcare providers, policymakers, and health systems globally to adopt and implement comprehensive strategies that prioritize HCC prevention, early diagnosis, multidisciplinary care, personalized treatment, and equitable access to therapies. In doing so, we can ensure that the latest advancements in HCC care reach those who need them most, ultimately improving outcomes and reducing the global impact of this disease.
Data Sharing Statement
Data sharing is not applicable as no datasets generated and/or analyzed for this study.
Ethics Approval and Informed Consent
Not applicable for this study. This article is based on previously conducted studies and does not contain any new studies with human participants or animals performed by any of the authors.
Acknowledgments
While no authors received payment for their contribution to the charter, as part of the development process, the ILCM received compensation for chairing one roundtable meeting held in 2024. ILCM is granted financial support by AstraZeneca, Bayer Healthcare and Hofman La Roche, AstraZeneca is a corporate member of ILCM. The Task Force for Global Health receives support for the Coalition for Global Hepatitis Elimination from governmental, philanthropic, individual, and industry partners (Abbott Laboratories, AbbVie, Cepheid, Dynavax, Gilead Sciences, Merck, Pharco, Roche Diagnostics, Siemens, VBI Vaccines, and Zydus Life Sciences).
Funding
Funding for this study, the article processing charges, and the open access charge were provided by AstraZeneca.
Disclosure
Dr Diane Langenbacher reports grants from Astra Zeneca UK Ltd., F.Hofmann-La Roche AG, and Bayer Healthcare, outside the submitted work. Dr Eric Bouffet reports grants from Roche; advisory committee for Novartis, Alexion, Servier, and Fore, outside the submitted work. Mrs Zeena Huang Chi is an employee of AstraZeneca, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Rumgay H, Ferlay J, de Martel C, et al. Global, regional and national burden of primary liver cancer by subtype. Eur J Cancer. 2022;161:108–118. doi:10.1016/j.ejca.2021.11.023. Epub 2021 Dec 20. PMID: 34942552.
2. World Cancer Research Fund International. Liver cancer statistics. Available from: https://www.wcrf.org/cancer-trends/liver-cancer-statistics/#:~:text=Latest%20liver%20cancer%20data,ASR%20%3D%20age%2Dstandardised%20rates.
3. International Agency for Research on Cancer World Health Organisation. Cancer Today – datavis. Available from: https://gco.iarc.fr/today/en/dataviz/pie?mode=cancer&cancers=11&group_populations=1&types=1&sort_by=value1.
4. Fa A, Danos DM, Maniscalco L, et al. Is There Really a Difference in Outcomes between Men and Women with Hepatocellular Cancer? Cancers. 2023;15(11):2892. doi:10.3390/cancers15112892. PMID: 37296854; PMCID: PMC10251901.
5. Asafo-Agyei KO, Samant H. Hepatocellular Carcinoma. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2024. Available from https://www.ncbi.nlm.nih.gov/books/NphBK559177/.
6. Mentha N, Clément S, Negro F, Alfaiate D. A review on hepatitis D: from virology to new therapies. J Adv Res. 2019;17:3–15. doi:10.1016/j.jare.2019.03.009
7. Tojjari A, Saeed A, Singh M, Cavalcante L, Sahin IH, Saeed A. A comprehensive review on cancer vaccines and vaccine strategies in hepatocellular carcinoma. Vaccines. 2023;11(8):1357. doi:10.3390/vaccines11081357
8. Yang C, Zhang H, Zhang L, et al. Evolving therapeutic landscape of advanced hepatocellular carcinoma. Nat Rev Gastroenterol Hepatol. 2023;20(4):203–222. doi:10.1038/s41575-022-00704-9
9. Gordan J, Kennedy EB, Abou-Alfa GK, et al. Systemic Therapy for Advanced Hepatocellular Carcinoma: ASCO Guideline Update. J Clin Oncol. 2024;42(15):1830–1850. doi:10.1200/JCO.23.02745
10. Liao W, Coupland CAC, Innes H, et al. Disparities in care and outcomes for primary liver cancer in England during 2008-2018: a cohort study of 8.52 million primary care population using the QResearch database. EClinicalMedicine. 2023;59:101969. doi:10.1016/j.eclinm.2023.101969
11. Kim E, Viatour P. Hepatocellular carcinoma: old friends and new tricks. Exp Mol Med. 2020;52(12):1898–1907. doi:10.1038/s12276-020-00527-1
12. El-Serag HB. Epidemiology of viral hepatitis and hepatocellular carcinoma. Gastroenterology. 2012;142(6):1264–1273.e1. doi:10.1053/j.gastro.2011.12.061. PMID: 22537432; PMCID: PMC3338949.
13. Park JW, Chen M, Colombo M, et al. Global patterns of hepatocellular carcinoma management from diagnosis to death: the BRIDGE Study. Liver Int. 2015;35(9):2155–2166. doi:10.1111/liv.12818
14. Sherman M. How to improve HCC surveillance outcomes. JHEP Rep. 2019;1(6):460–467. doi:10.1016/j.jhepr.2019.10.007
15. Rich NE, Hester C, Odewole M, et al. Racial and Ethnic Differences in Presentation and Outcomes of Hepatocellular Carcinoma. Clin Gastroenterol Hepatol. 2019;17(3):551–559e1. doi:10.1016/j.cgh.2018.05.039
16. Kim NJ, Cravero A, VoPham T. Addressing racial and ethnic disparities in US liver cancer care. Hepatol Commun. 2023;7(7):e00190. doi:10.1097/HC9.0000000000000190
17. International Liver Cancer Movement. The INTERNATIONAL LIVER CANCER NETWORK asks for reinforced efforts to improve patient outcomes: PREVENTION, EARLY DETECTION and ACCESS TO CARE. 2021. Available from: https://ilcm.global/files/ilcm_layout/RESOURCES/ILCN%20White%20Paper_2021.pdf.
18. European Association for the Study of the Liver. Electronic address: [email protected]; European Association for the Study of the Liver. EASL Clinical Practice Guidelines: management of hepatocellular carcinoma, J Hepatol. 2018;69(1):182–236. doi:10.1016/j.jhep.2018.03.019. Epub 2018 Apr 5. Erratum in: J Hepatol. 2019;70(4):817. doi: 10.1016/j.jhep.2019.01.020. PMID: 29628281
19. Singal AG, Llovet JM, Yarchoan M, et al. AASLD Practice Guidance on prevention, diagnosis, and treatment of hepatocellular carcinoma. Hepatology. 2023;78(6):1922–1965. doi:10.1097/HEP.0000000000000466
20. Shiina S, Gani RA, Yokosuka O, et al. APASL practical recommendations for the management of hepatocellular carcinoma in the era of COVID-19. Hepatol Int. 2020;14(6):920–929. doi:10.1007/s12072-020-10103-4. Epub 2020 Nov 11. PMID: 33174159; PMCID: PMC7655459.
21. Arab JP, Dirchwolf M, Álvares-da-silva MR, et al. Latin American Association for the study of the liver (ALEH) practice guidance for the diagnosis and treatment of non-alcoholic fatty liver disease. Ann Hepatol. 2020;19(6):674–690. doi:10.1016/j.aohep.2020.09.006. Epub 2020 Oct 5. PMID: 33031970.
22. Acharya SK, Bopanna S. Hepatocellular Carcinoma Screening and Nonalcoholic Fatty Liver Disease: how is it Different? J Clin Experiment Hepatol. 2020;10(5):518–524. doi:10.1016/j.jceh.2020.04.004
23. McMahon B, Cohen C, Brown Jr RS, et al. Opportunities to address gaps in early detection and improve outcomes of liver cancer. JNCI Cancer Spectr. 2023;7(3). doi:10.1093/jncics/pkad034
24. Digestive Cancers Europe. Insights and Key Findings: hepatocellular Carcinoma Prevention and Diagnosis Mapping Project, 2024. Available from: https://digestivecancers.eu/wp-content/uploads/2024/10/executive-summary-lcam2024.pdf.
25. Singal AG, Lok AS, Feng Z, Kanwal F, Parikh ND. Conceptual Model for the Hepatocellular Carcinoma Screening Continuum: current Status and Research Agenda. Clin Gastroenterol Hepatol. 2022;20(1):9–18. doi:10.1016/j.cgh.2020.09.036
26. Qurashi M, Sharma R, et al. Improving hepatocellular carcinoma surveillance in the United Kingdom: challenges and solutions Qurashi, Maria et al. Lancet Regional Health. 2024;43:100963. doi:10.1016/j.lanepe.2024.100963
27. Kinsey E, Lee HM. Management of Hepatocellular Carcinoma in 2024: the Multidisciplinary Paradigm in an Evolving Treatment Landscape. Cancers. 2024;16(3):666. doi:10.3390/cancers16030666
28. Zhu H, Patel MS, Gopal P, Parikh ND, Yopp AC, Singal AG. Multidisciplinary care for patients with HCC: a systematic review and meta-analysis. Hepatol Commun. 2023;7(5):1.
29. Reig M, Forner A, Rimola J, et al. BCLC strategy for prognosis prediction and treatment recommendation: the 2022 update. J Hepatol. 2022;76(3):681–693. doi:10.1016/j.jhep.2021.11.018
30. Cho Y, Kim BH, Park JW. Overview of Asian clinical practice guidelines for the management of hepatocellular carcinoma: an Asian perspective comparison. Clin Mol Hepatol. 2023;29(2):252–262. doi:10.3350/cmh.2023.0099. Epub 2023 Mar 10. PMID: 36907570; PMCID: PMC10121305.
31. Sinn DH, Choi G-S, Park HC, et al. Multidisciplinary approach is associated with improved survival of hepatocellular carcinoma patients. PLoS One. 2019;14(1):e0210730. doi:10.1371/journal.pone.0210730
32. Naugler WE, Alsina AE, Frenette CT, et al. Building the multidisciplinary team for management of patients with hepatocellular carcinoma. Clin Gastroenterol Hepatol. 2015;13(5):827–835. doi:10.1016/j.cgh.2014.03.038
33. Harrington C. Composition of An Ideal Medical Care Team. Dela J Public Health. 2022;8(5):150–153. doi:10.32481/djph.2022.12.033. PMID: 36751608; PMCID: PMC9894047.
34. Association of Community Cancer Centres. Multidisciplinary Hepatocellular Carcinoma Care. 2021. Available from: https://www.accc-cancer.org/docs/projects/hcc/hcc-pub_web.pdf?sfvrsn=fdd53564_0.
35. NHS. Long Term Plan. 2019. Available from: https://www.longtermplan.nhs.uk/wp-content/uploads/2019/08/nhs-long-term-plan-version-1.2.pdf.
36. Loren AW, et al. Fertility Preservation in People With Cancer: ASCO Guideline Clinical Insights. JCO Oncol Pract. 2025;2025:1. doi:10.1200/OP-25-00223
37. Elwyn G, Frosch D, Thomson R, et al. Shared Decision Making: a Model for Clinical Practice. J GEN INTERN MED. 2012;27(10):1361–1367. doi:10.1007/s11606-012-2077-6
38. Johnson L, Kirk H, Clark B, et al. Improving personalised care, through the development of a service evaluation tool to assess, understand and monitor delivery. BMJ Open Qual. 2023;12(3):e002324. doi:10.1136/bmjoq-2023-002324
39. Sun H, Yang H, Mao Y. Personalized treatment for hepatocellular carcinoma in the era of targeted medicine and bioengineering. Front Pharmacol. 2023;14:1150151. doi:10.3389/fphar.2023.1150151. PMID: 37214451; PMCID: PMC10198383.
40. NICE. Home care: delivering personal care and practical support to older people living in their own homes. 2015. Available from: https://www.nice.org.uk/guidance/ng21/chapter/recommendations.
41. Lau G, Obi S, Zhou J, et al. APASL clinical practice guidelines on systemic therapy for hepatocellular carcinoma-2024. Hepatol Int. 2024;18(6):1661–1683. doi:10.1007/s12072-024-10732-z
42. ClinicalTrials.gov. Sharing Decision-making Program for HCC Patients Treatment Decisions. 2021. Available from: https://clinicaltrials.gov/study/NCT03926039.
43. European Cancer Organisation. Shared Decision Making. Available from: https://www.europeancancer.org/content/the-code-shared-decision-making.html#:~:text=A%20treatment%20preference%20may%20be,should%20improve%20QoL%20and%20survival.
44. Gill J, Baiceanu A, Clark PJ, et al. Insights Into the Hepatocellular Carcinoma Patient Journey: results of the First Global Quality of Life Survey. Future Oncol. 2018;14(17):1701–1710. doi:10.2217/fon-2017-0715
45. NHS England. How to make shared decision making happen. 2025. Available from: https://www.england.nhs.uk/personalisedcare/shared-decision-making/how-to-make-shared-decision-making-happen/.
46. Cancer Support Community. 3 Ways to Shatter the Stigma of Liver Cancer & Find Healing. 2023. Available from: https://www.cancersupportcommunity.org/blog/shatter-stigma-liver-cancer-find-healing.
47. Liver Cancer UK. New data shows how liver cancer hits vulnerable groups hardest. 2024. Available from: https://livercanceruk.org/news/new-data-shows-how-liver-cancer-hits-vulnerable-groups-hardest/.
48. Health Awareness. How stigma can delay liver disease diagnosis. 2021. Available from: https://www.healthawareness.co.uk/liver/how-stigma-can-delay-liver-disease-diagnosis/.
49. Hepatitis B Foundation. Storytelling: the lived experience of having hepatitis B. 2024. Available from: https://www.hepb.org/research-and-programs/patient-story-telling-project/.
50. Canadian Cancer Liver Network. Liver Cancer Stigma. Available from: https://survivornet.ca/hcc-portal/liver-cancer-primary/living-well-primary-liver-cancer/liver-cancer-stigma/.
51. Jamioł-Milc D, Gudan A, Kaźmierczak-Siedlecka K, et al. Nutritional Support for Liver Diseases. Nutrients. 2023;15(16):3640. doi:10.3390/nu15163640
52. Ufere NN, Lai JC, Lai JC, Serper M, Serper M. Financial burden in adults with chronic liver disease: a scoping review. Liver Transpl. 2022;28(12):1920–1935. doi:10.1002/lt.26514
53. McIntosh SA, Alam F, Adams L, et al. Global funding for cancer research between 2016 and 2020: a content analysis of public and philanthropic investments. Lancet Oncol. 2023;24(6):636–645. doi:10.1016/S1470-2045(23)00182-1
54. Singal AG, Kudo M, Bruix J. Breakthroughs in hepatocellular carcinoma therapies. Clin Gastroenterol Hepatol. 2023;21(8):2135–2149. doi:10.1016/j.cgh.2023.01.039
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Understanding the Role of Metabolic Syndrome as a Risk Factor for Hepatocellular Carcinoma
Chavez-Tapia NC, Murúa-Beltrán Gall S, Ordoñez-Vázquez AL, Nuño-Lambarri N, Vidal-Cevallos P, Uribe M
Journal of Hepatocellular Carcinoma 2022, 9:583-593
Published Date: 5 July 2022
Changes in Presentation, Treatment, and Survival of Patients with Hepatocellular Carcinoma in Damietta, Egypt, 2007–2019: A Retrospective Monocentric Cohort Study
Jean K, Tawheed A, Luong Nguyen LB, Heikal T, Eldaly U, Elhadidy N, Elghaieb A, Aboudonia A, Tondeur L, Dublineau A, Fontanet A, El-Kassas M
Journal of Hepatocellular Carcinoma 2023, 10:99-111
Published Date: 25 January 2023
A Comparison of Presentation, Treatment, and Survival After Hepatocellular Carcinoma of Viral and Non-Viral Etiology in Damietta, Egypt, 2007–2019
Jean K, Tawheed A, Luong Nguyen LB, Heikal T, Eldaly U, Elhadidy NG, Elghaieb A, Aboudonia A, Tondeur L, Dublineau A, Fontanet A, El-Kassas M
Journal of Hepatocellular Carcinoma 2024, 11:997-1004
Published Date: 31 May 2024
Real-World Effectiveness of First Line Lenvatinib Therapy in Advanced Hepatocellular Carcinoma: Current Insights
Biachi de Castria T, Kim RD
Pragmatic and Observational Research 2024, 15:79-87
Published Date: 10 June 2024
Delivery of Avocado Seed Extract Using Novel Charge-Switchable Mesoporous Silica Nanoparticles with Galactose Surface Modified to Target Sorafenib-Resistant Hepatocellular Carcinoma

Basu A, Sae-be A, Namporn T, Suriyaphan O, Sithisarn P, Leanpolchareanchai J, Plommaithong P, Chatsukit A, Sa-ngiamsuntorn K, Naruphontjirakul P, Ruenraroengsak P
International Journal of Nanomedicine 2024, 19:10341-10365
Published Date: 14 October 2024