Back to Journals » Journal of Pain Research » Volume 19
A Novel Single-Puncture Ultrasound-Guided Approach for Radiofrequency Treatment of the Articular Branches of Femoral and Obturator Nerves
Authors Bao Y ![]() , Lai J
, Lai J ![]() , Lu G, Xie X
, Lu G, Xie X ![]() , Fang W, Yang L, Yang J, Gao H, Zhou X, Xiang Y
, Fang W, Yang L, Yang J, Gao H, Zhou X, Xiang Y
Received 5 January 2026
Accepted for publication 21 April 2026
Published 16 May 2026 Volume 2026:19 593693
DOI https://doi.org/10.2147/JPR.S593693
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Andrea Tinnirello
Yang Bao, Jinyu Lai, Guoqiang Lu, Xiaofang Xie, Wei Fang, Liang Yang, Jiaxuan Yang, Hongyi Gao, Xiaofeng Zhou, Yong Xiang
Department of Pain, Taihe Hospital, Hubei University of Medicine, Hubei, People’s Republic of China
Correspondence: Yong Xiang, Department of Pain, Taihe Hospital, Hubei University of Medicine, Hubei, 442000, People’s Republic of China, Tel +86-719-13972451941, Email [email protected]
Purpose: Current management of hip pain primarily involves pharmacotherapy, conservative treatment, and surgical intervention, with pulsed radiofrequency (PRF) treatment of articular branches gaining increasing attention. Previous PRF treatments have radiation risk and poor vascular visibility. This study introduces a novel single-puncture combined ultrasound-guided PRF technique targeting the articular branches of both the obturator and femoral nerves and evaluates its efficacy and safety in patients with chronic hip pain.
Patients and Methods: A retrospective analysis was conducted on six patients with chronic hip pain treated at the Pain Department of Taihe Hospital, Shiyan, Hubei Province, between January 2024 and August 2025. All patients underwent the single-puncture combined ultrasound-guided PRF procedure. The position of the needle tip relative to the articular branches was verified using C-arm fluoroscopy. Pain intensity was assessed before and after the procedure using the Numerical Rating Scale (NRS).
Results: Under ultrasound guidance, the target anatomy was clearly visualized, and successful needle placement was achieved in all six patients. No serious complications occurred during the procedure. The median NRS score decreased from 8.0 (IQR 7.0– 8.0) at baseline to 1.5 (IQR 1.0– 2.0) at 8 weeks post‑procedure (Friedman test, χ2 = 15.95, df = 3, p = 0.0012). Following treatment, all patients showed varying degrees of improvement, as reflected by reduced NRS scores.
Limitations: Retrospective study, small sample size.
Conclusion: The single-puncture combined ultrasound-guided PRF technique targeting the articular branches of the obturator and femoral nerves is a safe and effective short-term treatment for chronic hip pain.
Keywords: ultrasound guidance, hip pain, femoral nerves, obturator nerves, pulsed radiofrequency
Introduction
Hip pain is a common clinical presentation, categorized anatomically as anterior, lateral, or posterior based on the pain location. Etiologies of chronic hip pain include osteoarthritis (OA), rheumatoid arthritis, osteonecrosis, femoroacetabular impingement, infectious coxarthrosis, and post-total hip arthroplasty (THA) pain. Chronic hip pain is a refractory condition that frequently leads to significant functional impairment, particularly in cases of advanced OA or femoral head osteonecrosis. Hip OA is a leading cause of disability among the elderly and the most prevalent arthropathy in the United States, affecting approximately 5% of individuals over 65 years of age.1,2 The corresponding surgical burden is substantial, with annual expenditures for total hip arthroplasty (THA) in the U.S. exceeding tens of billions of dollars.3 Conventional management—including pharmacotherapy, physiotherapy, rehabilitation, and intra-articular injections—provides only transient symptomatic relief. Furthermore, long-term analgesic use is associated with potential adverse effects. Surgical intervention, namely THA, is contingent upon specific indications and carries risks of perioperative complications and persistent post-surgical pain. Consequently, there is a pressing clinical need to develop safer, more cost-effective therapeutic modalities with superior risk profiles for elderly patients with significant comorbidities who are suboptimal candidates for arthroplasty.
In recent years, minimally invasive interventional techniques for pain management have gained widespread acceptance. For instance, the ultrasound-guided Pericapsular Nerve Group (PENG) block4 provides effective short-term analgesia for chronic hip pain.5 However, while its immediate efficacy is satisfactory, the long-term therapeutic benefits remain uncertain. Pulsed radiofrequency (PRF) application to the articular branches of hip innervation is emerging as a viable therapeutic strategy for chronic hip pain. PRF represents an established neuromodulatory modality for various pain conditions, functioning through the delivery of pulsed electrical energy to peripheral neural structures. The therapeutic mechanism involves multimodal neuromodulation, including regulation of inflammatory responses, cellular signaling pathways, and pain-related gene expression, alongside effects on protein synthesis, ion channel function, and neurotransmitter dynamics.6 Clinical evidence confirms that PRF not only provides sustained hip pain relief but also significantly reduces dependency on systemic analgesic regimens.7
Previous studies on PRF treatment of hip articular branches have predominantly utilized fluoroscopic guidance,8–10 which relies on anatomical landmarks to target the femoral nerves (FN) and obturator nerves (ON) articular branches. However, this approach presents two significant limitations: inherent radiation exposure and inadequate real-time visualization of the femoral artery, increasing potential vascular injury risk during needle placement. In contrast, ultrasound guidance enables dynamic, real-time visualization without radiation, enhancing both safety and operational efficiency. Although ultrasound has been increasingly utilized for nerve blocks targeting these articular branches, its application in PRF procedures remains limited. This study introduces a novel single-puncture combined ultrasound-guided technique for PRF ablation of both the FN and ON articular branches, offering advantages in real-time visualization, radiation exposure, and procedural precision.
We conducted a retrospective analysis of clinical data from six patients treated with this combined ultrasound-guided technique at our institution’s pain department to evaluate its efficacy and safety in managing hip joint pain.
Materials and Methods
General Information
This retrospective clinical analysis received approval from the Ethics Committee of Taihe Hospital, Hubei University of Medicine (Approval No: 2025KS107). All patient data were anonymized, and medical records remained confidential. We retrospectively analyzed clinical data from six patients with hip pain who underwent radiofrequency treatment at our pain clinic between January 2024 and August 2025. Symptom duration ranged from 3 to 36 months (mean ± SD: 11.50 ± 12.36 months). The cohort comprised 3 male and 3 female patients, aged 58 to 73 years (mean ± SD: 64.50 ± 6.09 years).
All patients provided written informed consent after comprehensive explanation of the study purpose and postoperative care requirements. Inclusion criteria included: (1) Characteristic hip pain symptoms, (2) Confirmatory physical examination findings, (3) Imaging evidence supporting hip pathology diagnosis. All patients underwent orthopedic evaluation before radiofrequency treatment, with either no surgical indications or refusal of surgical intervention. Exclusion criteria comprised: psychiatric comorbidities affecting compliance, coagulopathies, or active skin infection at the procedure site.
Procedure
The Localization of the Articular Branches of FN and ON
Chronic hip pain primarily originates from the hip joint capsule, which receives complex innervation. The posterior capsule is innervated by the nerve to quadratus femoris, the superior gluteal nerve, and potentially the sciatic and inferior gluteal nerves. In contrast, the anterior capsule is supplied mainly by the ON, accessory obturator, and FN. Neuroanatomical studies have established the FN and ON as the dominant sources of anterior capsular innervation, with reported prevalence rates of 83–98% for the ON and 75–95% for the FN.11–13 Dissection of 13 specimens confirmed FN and ON contributions in all cases, while the accessory obturator nerve was present in only 7 (54%).11 Consequently, PRF for chronic hip pain focuses on the FN and ON. The ON are classified as high (originating proximal to or within the obturator canal) or low (arising from its posterior division).11 The ON are located close to the inferomedial acetabulum. The most consistent landmark for these branches is the region of bone thickening at the inferomedial acetabulum.11 The FN are categorized relative to the inguinal ligament as high or low, with high branches being more numerous. All high branches traverse the periosteal surface of the pubis between the anterior inferior iliac spine (AIIS) and the medial aspect of the iliopubic eminence.11 The key landmarks for locating the FN articular branches are the AIIS and the superolateral acetabular rim.14,15 In summary, the articular branches of the ON and FN are the principal contributors to anterior hip joint innervation. Clinically, the radiographic “teardrop” is used to target the ON,15,16 while the AIIS or superolateral acetabular margin guides FN localization.14,15
Ultrasound-Guided Nerve Block and PRF for Articular Branches of FN and ON
Following orthopedic specialist consultation, the patient and family members opted for non-surgical management and provided written consent for the selected treatment approach. An initial diagnostic nerve block of the hip articular branches was performed, resulting in significant pain relief. After detailed discussion with the patient and family, informed consent for radiofrequency ablation was obtained. Preoperative preparations were completed utilizing the following equipment: an ultrasound system (SonoSite SII) with rC60xi/5-2 Mhz transducer, and Cosman RFG-4 radiofrequency ablation device, all confirmed to be in proper working condition. The procedure was performed by an experienced chief physician.
Initial ultrasound scanning was performed to map the entry point. We targeted the articular branches of ON and FN. The surface landmark, the anterior inferior iliac spine (AIIS), was first identified. The ultrasound probe was positioned in the classic PENG plane, which served as the initial sonographic reference (Figure 1C, red dashed boxes in Figure 1A–1B). To target the ON articular branches, the probe was moved inferomedially from the PENG plane and rotated clockwise (relative to the patient’s caudal side) until an image showing the femoral head and the inferomedial acetabulum was obtained. This identified a transitional ultrasound location (Figure 1D, green dashed box in Figure 1A). The probe was then shifted parallelly in a caudal direction to the point where the acetabulum just disappeared. The final ultrasound plane is used to guide the puncture needle for the ON articular branches (Figure 1E, solid green box in Figure 1A). This sonographic plane and the corresponding skin entry point were marked. Subsequently, for the FN articular branches, the probe was returned to the initial PENG plane. It was then rotated clockwise approximately 90° (relative to the patient’s caudal side), perpendicular to the original PENG plane orientation, to establish the guidance plane for FN articular branches (Figure 1F, solid blue box in Figure 1B). This plane was also marked, confirming the use of the same skin entry point (red stars in Figure 1A–Figure 1B).
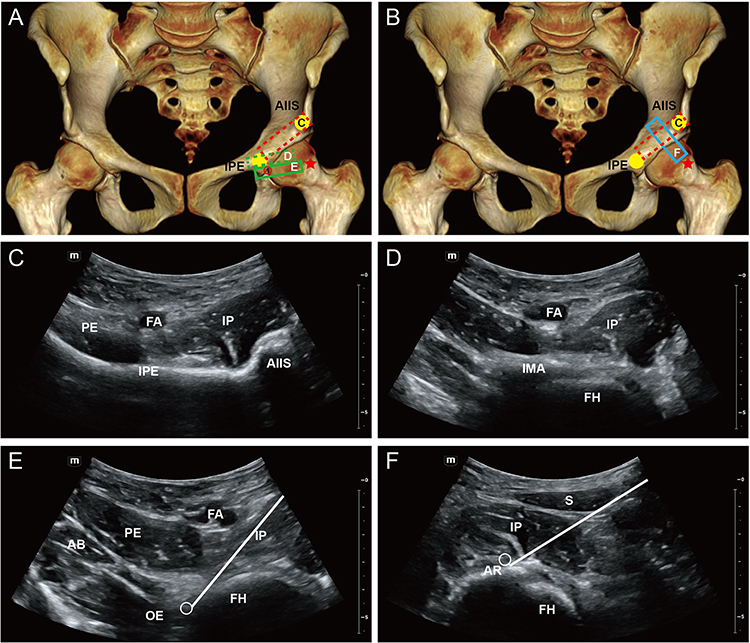 |
Figure 1 Single-puncture combined ultrasound-guided PRF of the ON and FN articular branches. (A) Schematic diagram of the position of the ultrasound probe during PRF of ON articular branches. The red dashed box indicates the initial PENG-scan plane. The green dashed box indicates an intermediate position after inferomedial probe adjustment until the inferomedial acetabulum are visualized. The green solid box indicates the final needle-guided probe position, achieved by moving the probe further down until the inferomedial acetabulum just disappears. (B) Schematic diagram of the position of the ultrasound probe during PRF of FN articular branches. The red dashed box indicates the initial PENG-scan plane. The solid blue box shows the final probe position for needle guidance, perpendicular to the initial PENG plane. (C) Planar ultrasound image of PENG scan. (D) Ultrasound image of the femoral head and inferomedial acetabulum. (E) Ultrasound image of the puncture-guided section during PRF of ON articular branches. (F) Ultrasound image of the puncture-guided section during PRF of FN articular branches. Solid white lines represent needle paths, and hollow circles represent target points. The red stars represent the puncture point, and the yellow circles represents the IPE. Abbreviations: AIIS, anterior inferior iliac spine; PE, pectineus muscle; AB, adductor brevis; FH, femoral head; IPE, the iliopubic eminence; OE, obturator externus-muscle; FA, femoral artery; IMA, inferomedial acetabulum; IP, Iliopsoas complex; S, sartorius; AR, acetabular rim. |
Following standard surgical disinfection and draping, a sterile ultrasound probe was utilized. Local anesthesia (2.5 mL of 2% lidocaine hydrochloride mixed with 2.5 mL of 0.9% sodium chloride) was administered via subcutaneous infiltration at the marked entry point (Figure 1A and B, red star). Notably, the injection was kept superficial to avoid compromising subsequent electrical stimulation. A 16-gauge, 10-cm radiofrequency cannula with a 5-mm active tip was advanced under real-time in-plane ultrasound guidance. The probe was maneuvered to maintain the femoral head in the center of the view, clearly display vascular structures, and ensure continuous visualization of the needle path. The ON articular branches were targeted first (Figure 1C–E). The needle was advanced through the iliopsoas complex, avoiding the femoral artery, to the femoral head margin. Needle position was verified using C-arm fluoroscopy (Figure 2A and B). After correct positioning, sensory stimulation at 50 Hz was performed to elicit paresthesias or pain sensation in the hip joint by the patient at 0.6 V. Two Hz stimulation was then performed to exclude the involvement of motor fibers. PRF was then applied to the target nerves for 300 seconds each, tip temperature was limited to 42°C. Intraoperative imaging of PRF is shown in Figure 2A. Then slowly injected 5 mL of anti-inflammatory solution (20 mg methylprednisolone dissolved in 10 mL of physiological saline). The FN articular branches were targeted next by returning the probe to the PENG plane and rotating it 90° to the target position (Figure 1F). From the same entry point, the needle was redirected through the iliopsoas complex to the superolateral acetabular rim. Position confirmation and PRF application followed the same protocol as for the ON articular branches, with C-arm verification (Figure 2C) and subsequent injection of 5 mL anti-inflammatory solution. The needle was withdrawn without complications. The puncture site was covered with sterile gauze, and the patient was transferred to the recovery room in stable condition. The operation flow chart is shown in Figure 3.
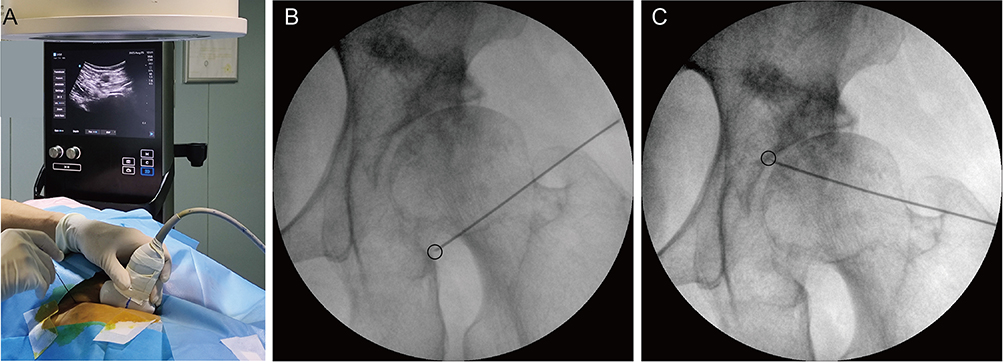 |
Figure 2 Intraoperative images and C-arm verification of PRF. (A) Intraoperative image of PRF. (B) Projection verification of ON articular branches via the C-arm. (C) Projection verification of FN articular branches via the C-arm. hollow circles represent target points. |
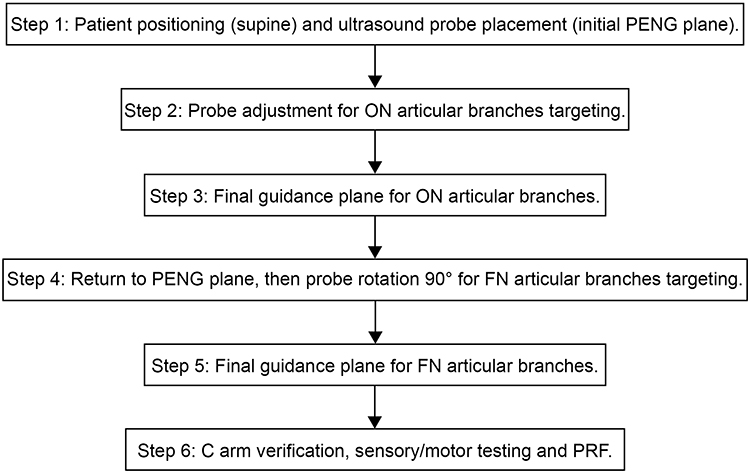 |
Figure 3 Technical workflow of the single‑puncture combined ultrasound‑guided PRF procedure. |
Results
The novel single-puncture approach successfully targeted the articular branches of both the FN and ON in all six patients. Fluoroscopic imaging in one representative case confirmed proper needle placement adjacent to the target nerves, demonstrating a favorable parallel alignment. Correct positioning for all patients was further verified by successful diagnostic stimulation prior to PRF.
A total of six patients were included. The median (IQR) NRS scores were 8.0 (7.0–8.0) at baseline, 3.0 (3.0–4.0) on postoperative day 1, 2.0 (2.0–3.0) at postoperative week 1, and 1.5 (1.0–2.0) at postoperative week 8 (Table 1). All patients demonstrated a reduction in NRS scores from baseline to each follow‑up time point (Table 2). The Friedman test revealed a statistically significant difference across the four time points (χ2 = 15.95, df = 3, p = 0.0012), indicating a significant decrease in pain scores after the procedure.
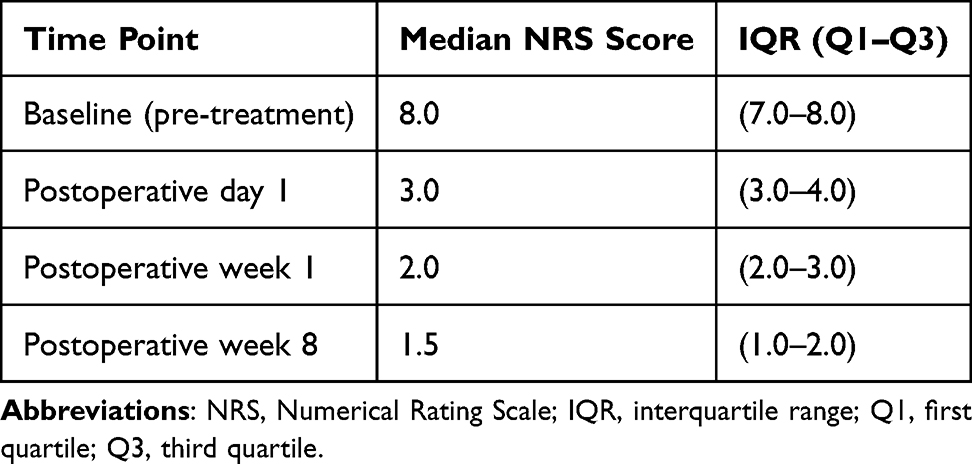 |
Table 1 NRS Scores Over Time (Median and IQR) |
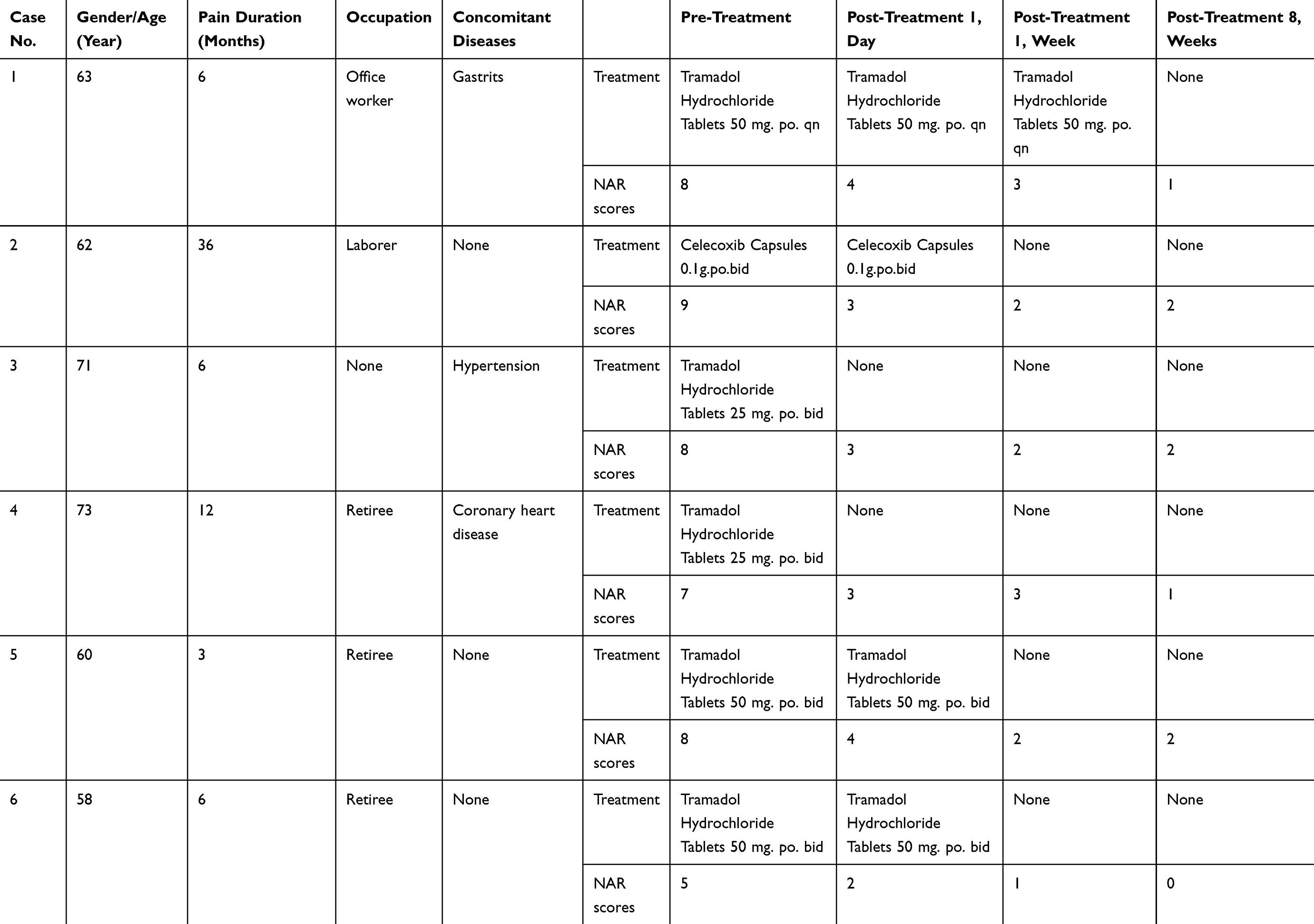 |
Table 2 Patient Basic Information and Clinical Parameters |
Preliminary findings from this small case series indicate that the single‑puncture combined ultrasound‑guided radiofrequency ablation technique for the articular branches of the FN and ON demonstrates an acceptable safety profile and potential short‑term efficacy in reducing chronic hip pain. However, given the methodological limitations, these observations should be considered hypothesis‑generating. Further prospective, controlled studies with larger sample sizes and longer follow‑up are warranted to confirm the safety and clinical utility of this approach.
Discussion
All six patients in this study underwent successful ultrasound-guided needle placement without intraoperative complications such as nerve injury, hemorrhage, or intravascular injection. Pain improved significantly at postoperative day 1, week 1, and week 8. No major complications or motor function limitations were observed during follow-up, confirming the procedure’s high safety profile under ultrasound guidance. Intraoperative C-arm fluoroscopy confirmed appropriate anatomical needle positioning. The radiofrequency needle was aligned parallel to the courses of both the FN and ON articular branches, resulting in broader ablation coverage. In this small‑sample preliminary study, the single‑puncture combined ultrasound‑guided radiofrequency ablation technique demonstrated favourable short‑term safety and a trend towards pain relief in patients with chronic hip pain.
Chronic hip pain represents a common condition in individuals aged 45 and older. Current treatment approaches primarily include pharmacotherapy, physical therapy, minimally invasive interventions, and surgical options. Among these, analgesic medications may induce gastrointestinal or cardiovascular side effects and are often unsuitable for long-term use in elderly patients with multiple comorbidities. While intra-articular injection is a widely adopted minimally invasive treatment, it has notable limitations. Studies indicate that the therapeutic effect of such injections is short-lived and fails to provide sustained relief for chronic hip pain over the long term.17,18 For patients with severe chronic hip pain who have not responded to conservative treatment, hip replacement surgery may be considered. Hip surgery can improve patients’ quality of life,19 but the costs involved are considerable. For young patients, elderly patients with high surgical risks, and patients who are unwilling to undergo surgery, a more economical method needs to be sought. Research reports that radiofrequency ablation is an effective treatment method for relieving hip pain in patients with persistent hip pain who have failed conservative treatment, have short-term effects after injection therapy, or are not suitable for surgery.20–22 Research has demonstrated that sensory innervation of the hip joint is primarily concentrated in the superior aspect of the anterior capsule and the acetabular labrum. Similarly to the distribution of nociceptors, mechanoreceptors exhibit a higher density in the anterior region compared to the posterior. Consequently, the anterior hip capsule is predominantly innervated by the articular branches of the FN and ON.23 In clinical practice, groin and medial thigh pain can be alleviated by targeting the articular branches of the ON, while lateral thigh and greater trochanter pain may be addressed by targeting the articular branches of the FN. Accordingly, the primary targets for PRF in managing chronic hip pain are the articular branches of the FN and ON.
The first application of radiofrequency (RF) for hip pain was reported by Akatov and Dreval in 1997.24 Using anatomical landmarks to localize the ON, their study showed that RF lesioning effectively alleviated hip pain. With technological advancements, fluoroscopic guidance was subsequently introduced, and several studies have reported the efficacy of fluoroscopy-guided RF treatment for hip pain.9,25–28 In the study by Mariconda et al,9 exercise rehabilitation combined with continuous radiofrequency (CRF) ablation of the articular branches of the FN and ON proved to be an effective alternative therapy for patients with severe hip osteoarthritis. In their protocol, CRF ablation of the FN was performed under fluoroscopic guidance using the superolateral edge of the acetabulum as a landmark. For the ON, the needle was inserted approximately 70° laterally to the femoral artery, using the “teardrop” as a landmark. The study concluded that the combination of exercise therapy and CRF ablation constitutes a viable therapeutic alternative.
With the increasing adoption of ultrasound, researchers have explored combined fluoroscopic and conventional radiofrequency thermocoagulation of FN and ON articular branches.20 These studies confirmed that conventional radiofrequency thermocoagulation of these branches effectively relieves chronic hip pain, improves hip function, and enhances quality of life. Another case report described ultrasound-guided RF ablation of the FN articular branches for pain relief.29 In a retrospective analysis of PRF treatment targeting the FN and ON for hip pain, the results demonstrated that PRF is a safe and effective modality for treating hip joint pain in the short and medium term. In that study, the articular branches of the FN and ON were localized under fluoroscopic guidance using systematic anatomical landmarks. At one year postoperatively, a significant reduction in NRS scores was observed in all 14 patients.30
Collectively, most earlier studies relied primarily on fluoroscopy for needle placement, with ultrasound occasionally used adjunctively to verify vascular anatomy. These fluoroscopy-guided methods demand considerable operator expertise, involve ionizing radiation exposure, and are difficult to widely implement in primary care settings due to equipment and training limitations.
This “two birds with one stone” approach enables real-time visualization of the femoral artery, effectively reducing vascular puncture risks while eliminating ionizing radiation and minimizing tissue trauma. The novel puncture trajectory offers three principal advantages. First, from an anatomical perspective, The needle alignment remains relatively parallel to the ON and FN articular branches, maximizing electrode-neural contact area and expanding the effective ablation zone. Second, ultrasound provides continuous real-time visualization of the femoral artery, preventing injury to critical neurovascular structures. Third, our single-puncture approach for dual nerve ablation eliminates the need for C-arm fluoroscopy, removing radiation exposure while reducing procedural trauma for both patients and medical personnel.
This study has several limitations. We acknowledge that the maximum follow‑up duration in this study was 8 weeks. Therefore, the observed pain relief should be interpreted as preliminary short‑term results. As a retrospective investigation, it features a small sample size and relatively simplistic outcome measures. Follow-up duration did not extend beyond six months, and assessment relied solely on NRS scores without more comprehensive metrics such as the Harris Hip Score or the Total Orthopedic and Musculoskeletal Assessment Criteria. Future directions include expanding the cohort size, incorporating multidimensional assessment tools, establishing control groups, and extending follow-up periods. Additionally, the procedure requires to be performed by senior, experienced operators, and we cannot exclude the possibility that complications or suboptimal outcomes might relate to technical inexperience. We acknowledge that the observed pain improvement cannot be solely attributed to the PRF treatment itself. Potential confounding factors include a placebo effect, the concurrent use of local anaesthetic and corticosteroid injections (which may provide independent analgesic and anti‑inflammatory effects), and the natural history of the underlying condition. The long‑term efficacy of this novel single‑puncture combined ultrasound‑guided PRF technique remains to be determined.
Abbreviations
PRF, Pulsed radiofrequency; NRS, numerical rating scale; FN, femoral nerves; ON, obturator nerves.
Data Sharing Statement
We agree to share all the data for this article. The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
This study is a retrospective clinical analysis and has been approved by the Ethics Committee of Taihe Hospital, Hubei University of Medicine (Approval No. 2025KS107). This study was conducted in accordance with the Declaration of Helsinki.
Consent for Publication
We all agree to share all the data for this article. The data that support the findings of this study are available from the corresponding author upon reasonable request.
Acknowledgments
Thank you to Dr. Yong Xiang for providing writing and operational guidance.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Taihe Hospital Funding Support (2025JJXM050).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lawrence RC, Helmick CG, Arnett FC, et al. Estimates of the prevalence of arthritis and selected musculoskeletal disorders in the United States. Arthritis Rheum. 1998;41(5):778–10. doi:10.1002/1529-0131(199805)41:5<778::Aid-art4>3.0.Co;2-v
2. Lane NE. Clinical practice. Osteoarthritis of the Hip. New Engl J Med. 2007;357(14):1413–1421. doi:10.1056/NEJMcp071112
3. Murphy L, Helmick CG. The impact of osteoarthritis in the United States: a population-health perspective. Am J Nurs. 2012;112(3 Suppl 1):S13–S19. doi:10.1097/01.Naj.0000412646.80054.21
4. Girón-Arango L, Peng PWH, Chin KJ, Brull R, Perlas A. Pericapsular Nerve Group (PENG) block for hip fracture. Reg Anesth Pain Med. 2018;43(8):859–863. doi:10.1097/aap.0000000000000847
5. Ergün Demiröz B, Sarı S, Ekin Y, Ertuğrul HA, Aydın ON. Comparison of conventional radiofrequency thermocoagulation to femoral and obturatory nerve articular branches with intra-articular steroid injection and PENG block in chronic Hip pain. J Back Musculoskeletal Rehabilit. 2025;10538127251349152. doi:10.1177/10538127251349152
6. De la Cruz J, Benzecry Almeida D, Silva Marques M, Ramina R, Fortes Kubiak RJ. Elucidating the mechanisms of pulsed radiofrequency for pain treatment. Cureus. 2023;15(9):e44922. doi:10.7759/cureus.44922
7. Diwan S, Gupta A, Sancheti P, Sanghvi S, Panchawagh S. Kronik kalça ağrısı olan hastalarda konvansiyonel analjeziklere dirençli kalça eklemi artiküler sinirlerinin perkütan puls radyofrekans ablasyonu [Percutaneous pulsed radiofrequency ablation of articular nerves of the Hip joint in patients with chronic hip pain refractory to conventional analgesics]. Agri (Algoloji) Dernegi’nin Yayin organidir. 2024;36(2):83–91. Turkish. doi:10.14744/agri.2023.90236
8. Okada T, Goyagi T, Ohseto K. Successful treatment of hip osteoarthritis with radiofrequency ablation: a report of two cases. Cureus. 2025;17(3):e80122. doi:10.7759/cureus.80122
9. Mariconda C, Megna M, Farì G, et al. Therapeutic exercise and radiofrequency in the rehabilitation project for Hip osteoarthritis pain. Eur J Phys Rehabil Med. 2020;56(4):451–458. doi:10.23736/s1973-9087.20.06152-3
10. Kapural L, Naber J, Neal K, Burchell M. Cooled radiofrequency ablation of the articular sensory branches of the obturator and femoral nerves using fluoroscopy and ultrasound guidance: a large retrospective study. Pain Physician. 2021;24(5):E611–E617.
11. Short AJ, Barnett JJG, Gofeld M, et al. Anatomic study of innervation of the anterior hip capsule: implication for image-guided intervention. Reg Anesth Pain Med. 2018;43(2):186–192. doi:10.1097/aap.0000000000000701
12. Birnbaum K, Prescher A, Hessler S, Heller KD. The sensory innervation of the Hip joint--an anatomical study. Surg Radiologic Anatomy. 1997;19(6):371–375. doi:10.1007/bf01628504
13. Kampa RJ, Prasthofer A, Lawrence-Watt DJ, Pattison RM. The internervous safe zone for incision of the capsule of the Hip. A cadaver study. J Bone Joint Surg Br. 2007;89(7):971–976. doi:10.1302/0301-620x.89b7.19053
14. Cortiñas-Sáenz M, Salmerón-Velez G, Holgado-Macho IA. Bloqueo intraarticular y de ramas sensoriales de los nervios obturador y femoral en cuadro de osteonecrosis y artrosis de cabeza femoral [Joint and sensory branch block of the obturator and femoral nerves in a case of femoral head osteonecrosis and arthritis]. Revista espanola de cirugia ortopedica y traumatologia. 2014;58(5):319–324. Spanish. doi:10.1016/j.recot.2014.01.009
15. Chaiban G, Paradis T, Atallah J. Use of ultrasound and fluoroscopy guidance in percutaneous radiofrequency lesioning of the sensory branches of the femoral and obturator nerves. Pain Pract. 2014;14(4):343–345. doi:10.1111/papr.12069
16. Stone J, Matchett G. Combined ultrasound and fluoroscopic guidance for radiofrequency ablation of the obturator nerve for intractable cancer-associated Hip pain. Pain Physician. 2014;17(1):E83–E87.
17. Gazendam A, Ekhtiari S, Bozzo A, Phillips M, Bhandari M. Intra-articular saline injection is as effective as corticosteroids, platelet-rich plasma and hyaluronic acid for Hip osteoarthritis pain: a systematic review and network meta-analysis of randomised controlled trials. Br J Sports Med. 2021;55(5):256–261. doi:10.1136/bjsports-2020-102179
18. Lai WC, Arshi A, Wang D, et al. Efficacy of intraarticular corticosteroid Hip injections for osteoarthritis and subsequent surgery. Skeletal Radiol. 2018;47(12):1635–1640. doi:10.1007/s00256-018-3052-z
19. Kumar P, Sen RK, Aggarwal S, Jindal K, Rajnish RK. Assessment and reliability of the World Health Organisation quality of life (WHO QOL-BREF) questionnaire in total Hip replacement patients. J Clinl Orthopaedics Trauma. 2020;11(Suppl 5):S756–S759. doi:10.1016/j.jcot.2020.07.020
20. Hernández-González L, Calvo CE, Atkins-González D. Peripheral nerve radiofrequency neurotomy: hip and knee joints. Phys Med Rehabilit Clinics North Am. 2018;29(1):61–71. doi:10.1016/j.pmr.2017.08.006
21. Karaoğlu S, Sari S, Ekin Y, Özkan Y, Aydin ON. The effect of conventional radiofrequency thermocoagulation of femoral and obturator nerves’ articular branches on chronic Hip pain: a prospective clinical study. Pain Med. 2024;25(7):444–450. doi:10.1093/pm/pnae016
22. Tran A, Reiter D, Wong PK, et al. Alternative treatment of Hip pain from advanced hip osteoarthritis utilizing cooled radiofrequency ablation: single institution pilot study. Skeletal Radiol. 2022;51(5):1047–1054. doi:10.1007/s00256-021-03927-0
23. Laumonerie P, Dalmas Y, Tibbo ME, et al. Sensory Innervation of the hip joint and referred pain: a systematic review of the literature. Pain Med. 2021;22(5):1149–1157. doi:10.1093/pm/pnab061
24. Akatov OV, Dreval ON. Percutaneous radiofrequency destruction of the obturator nerve for treatment of pain caused by coxarthrosis. Stereot Funct Neurosurg. 1997;69(1–4 Pt 2):278–280. doi:10.1159/000099888
25. Gupta G, Radhakrishna M, Etheridge P, Besemann M, Finlayson RJ. Radiofrequency denervation of the Hip joint for pain management: case report and literature review. US Army Med Dep J. 2014;2014:41–51.
26. Kumar P, Hoydonckx Y, Bhatia A. A review of current denervation techniques for chronic hip pain: anatomical and technical considerations. Curr Pain Headache Rep. 2019;23(6):38. doi:10.1007/s11916-019-0775-z
27. Correia R, Oliveira L, Andrade I, et al. Ultrasound-guided radiofrequency ablation for chronic hip pain due to osteoarthritis. Cureus. 2024;16(2):e53743. doi:10.7759/cureus.53743
28. Yildiz G, Baran M, Sahin S, Akcaboy EY, Celik S. Ultrasound-guided radiofrequency denervation and pericapsular nerve group block for chronic Hip joint pain in a patient diagnosed with Duchenne muscular dystrophy. Korean J Anesthesiol. 2023;76(4):389–390. doi:10.4097/kja.23015
29. Kim DJ, Shen S, Hanna GM. Ultrasound-guided radiofrequency lesioning of the articular branches of the femoral nerve for the treatment of chronic post-arthroplasty hip pain. Pain Physician. 2017;20(2):E323–E327.
30. Tinnirello A, Todeschini M, Pezzola D, Barbieri S. Pulsed radiofrequency application on femoral and obturator nerves for hip joint pain: retrospective analysis with 12-month follow-up results. Pain Physician. 2018;21(4):407–414.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.