Back to Journals » Cancer Management and Research » Volume 18

A Novel Prognostic Model Based on Prognostic Nutritional Index and Systemic Immune-Inflammation Index for Cancer Patients Treated with Immune Checkpoint Inhibitors
Authors Mao J, Guo H, Yang J ![]() , Wang J, Tao M, Wang Y, Yan X, Li M
, Wang J, Tao M, Wang Y, Yan X, Li M
Received 10 April 2026
Accepted for publication 16 June 2026
Published 10 July 2026 Volume 2026:18 611679
DOI https://doi.org/10.2147/CMAR.S611679
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Professor Seema Singh
Jingxian Mao,1,* Huaijuan Guo,1,* Jingjing Yang,1,* Jiaxin Wang,1 Mingyang Tao,1 Ying Wang,1 Xuebing Yan,1 Min Li2
1Department of Oncology, The Affiliated Hospital of Yangzhou University, Yangzhou University, Yangzhou, People’s Republic of China; 2Department of Anesthesiology, The Affiliated Hospital of Yangzhou University, Yangzhou University, Yangzhou, People’s Republic of China
*These authors contributed equally to the manuscript writing
Correspondence: Min Li, Department of Anesthesiology, The Affiliated Hospital of Yangzhou University, Yangzhou University, Yangzhou, People’s Republic of China, Email [email protected] Xuebing Yan, Department of Oncology, The Affiliated Hospital of Yangzhou University, Yangzhou University, Yangzhou, People’s Republic of China, Email [email protected]
Objective: The prognostic nutritional index (PNI) and systemic immune-inflammation index (SII) have both been reported as important indicators of prognosis in cancer patients. This study sought to construct and evaluate a combined PNI-SII score for predicting outcomes in patients undergoing immune checkpoint inhibitor (ICI) therapy.
Methods: A total of 350 cancer patients treated with ICI-based therapy were retrospectively enrolled, with overall survival (OS) and progression-free survival (PFS) defined as the primary endpoints. The PNI-SII scoring model was developed as follows: score 0 (low SII and high PNI), score 1 (high SII or low PNI), score 2 (high SII and low PNI).
Results: In the entire cohort, patients with high PNI level tended to have a significantly longer OS and PFS than those with low PNI level (both p< 0.001), while the opposite was for patients with high SII level as compared with those with low SII level (OS, p< 0.001; PFS, p=0.004). Consistently, the PNI-SII model was found to effectively stratify both OS and PFS in the entire cohort (both p< 0.001), which was then confirmed in the subgroups stratified by cancer type, age, and smoking history. In addition, the PNI-SII score was associated with short-term treatment response and therapy-related adverse events.
Conclusion: The PNI-SII model may serve as a convenient prognostic indicator for cancer patients receiving ICI therapy. Due to the limitations of the present study, further clinical investigations are necessary to validate its efficacy.
Keywords: cancer, immune checkpoint inhibitor, prognostic nutritional index, systemic immune-inflammation index and prognosis
Introduction
The immunotherapy has recently revolutionized the traditional anti-cancer modalities and achieved encouraging results in accumulating clinical trials.1 The representative drugs of cancer immunotherapy, known as immune checkpoint inhibitors (ICIs), inhibit the expression of programmed cell death protein 1 (PD-1) or its ligand PD-L1 or cytotoxic T-lymphocyte-associated protein 4 (CTLA-4), to stimulate the T cell-based anti-cancer immune system.2–4 However, not all the patients have favorable response to ICI therapy which is partly attributed to inherent and environmental factors.5–8 Moreover, unfavorable responses to ICI therapy may be influenced by tumor-intrinsic features, immune-suppressive components of the tumor microenvironment, impaired antigen presentation, and adaptive activation of alternative immune checkpoints.2,9 These factors may partly explain the heterogeneous responses to ICIs across different cancer types and individual patients. The advancing sequencing techniques have provided numerous circulating biomarkers for predicting ICI efficacy, but sufficient clinical validations are lacking and their high cost inhibits their actual application.10 Therefore, it is an urgent task to identify and validate low-cost and highly accessible predictive biomarkers that contribute to more precise decisions for ICI-based therapy.
Nutritional and inflammatory status are closely associated with antitumor immune responses, and together they regulate host antitumor immunity.11 Serum protein levels reflect nutritional status, and hypoalbuminemia may impair immune cell function.12 Peripheral lymphocyte count directly reflects host immune competence, while platelet and neutrophil counts represent the degree of systemic inflammation.13 These factors may influence the efficacy of ICIs by affecting both the quality and magnitude of antitumor immune responses. The prognostic nutritional index (PNI), derived from serum albumin and peripheral lymphocyte counts, was originally introduced as a perioperative risk indicator in gastrointestinal surgery.14 A recent meta-analysis has found reduced PNI is linked to unfavorable outcomes in patients with advanced non-small cell lung cancer (NSCLC) receiving first-line immunotherapy.15 In our previous work, PNI showed superior prognostic performance compared with body mass index (BMI) and albumin alone for overall survival (OS) in lung cancer patients treated with ICIs.16 Different from our previous study focusing on PNI alone in lung cancer patients, the present study further integrates PNI with systemic immune-inflammation index (SII) and evaluates the combined PNI-SII score in a multi-cancer cohort receiving ICI-based therapy. The SII, integrating platelet counts and the neutrophil-to-lymphocyte balance, was initially invented to predict the prognosis of hepatocellular carcinoma but then found to play a similar predictive role in other cancers and nonmalignant diseases.17 A recent meta-analysis has indicated that elevated SII is associated with poorer OS and progression-free survival (PFS) in ICI-treated cancer patients.18 Taken together, these findings strongly support that both PNI and SII have great potential to be an actionable prognostic biomarker for cancer patients who received ICI-based therapies.
Despite their potential prognostic value, a comprehensive validating work has found both PNI and SII were only moderately associated with the clinical outcome of metastatic NSCLC patients who received first-line ICIs, doubting their actual predictive performance.19 In addition, considering complexity of patients, any single index was unable accurately predict the clinical outcome. Therefore, combination of multiple biomarkers may increase the accuracy of prognosis prediction. A recent retrospective study has successfully combined PNI and SII in predicting the PFS of locally advanced gastric cancer patients who received neoadjuvant chemoimmunotherapy, suggesting the potential value of integrating nutritional and inflammatory markers.20 However, its applicability beyond a single cancer type and treatment setting remains unclear. Although PNI and SII reflect nutritional and inflammatory status respectively, both may influence ICI efficacy by modulating host antitumor immunity. Therefore, developing an integrated prognostic model in a heterogeneous cancer population may have broader clinical applicability, although sufficient cross-tumor validation is still required. Based on this rationale, a combined PNI-SII score was developed and evaluated in a retrospective multi-cancer cohort of 350 patients receiving immune checkpoint inhibitors.
Methods and Materials
Study Cohort
The patients who received ICI-based therapies between January 2018 and December 2023 at the Affiliated Hospital of Yangzhou University were screened for eligibility. The inclusion criteria were as follows: (1) pathologically confirmed cancer; (2) age over 18 years old; (3) patients underwent ICI treatment either as monotherapy or in combination with chemotherapy, radiotherapy, or targeted therapy; (4) available results of baseline laboratory tests. Patients were excluded if they had any of the following conditions: (1) the presence of multiple active primary tumors; (2) fewer than two cycles of ICI therapy; (3) incomplete clinical information, missing follow-up data, or absence of informed consent; (4) adjuvant ICI therapy after radical surgery; (5) suspected ICI-related hyperprogression. As a result, a total of 350 patients were included in this retrospective study, and the flowchart of patient recruitment was shown in Figure 1. The study protocol was reviewed and approved by the Ethics Committee of the Hospital (No. 2022-YKL11-Class 05). This study was conducted as a retrospective analysis, and all included patients were adults (≥18 years old). At the time of hospital admission, patients had signed a general informed consent form allowing the use of their anonymized clinical data for research purposes. This study was conducted in accordance with the Declaration of Helsinki.
 |
Figure 1 Flowchart of patient recruitment in the retrospective study. |
Definition of the PNI-SII Score
Peripheral venous blood was collected for baseline laboratory assessment within 24 hours prior to the first administration of ICIs. The PNI was calculated using the following formula: PNI = albumin (g/L) + 5 × peripheral serum lymphocyte count (109/L). SII was computed using the formula (platelet count × neutrophil count)/lymphocyte count. The optimal cut-off values for PNI and SII were determined by receiver operating characteristic (ROC) analyses with OS status as the outcome (Figure S1A and B). To assess the internal validity and robustness of the PNI-SII model and reduce potential overfitting, bootstrap resampling was performed with 1000 repetitions based on the original dataset. As a result, the high and low PNI were determined as those more and less than 47.625, respectively, while the high and low SII were determined as those more and less than 1004.145, respectively. The PNI-SII score was defined as follows: score 0 (low SII and high PNI score), score 1 (high SII or low PNI) and score 2 (high SII and low PNI).20,21
Therapeutic Regimens
The ICI drugs were administered intravenously every three weeks or subcutaneously every two weeks (envafolimab). The administered ICI drugs were as follows: sintilimab (n=139), camrelizumab (n=81), tirelizumab (n=71), pembrolizumab (n=19), toripalimab (n=15), serplulimab (n=9), nivolumab (n=7), durvalumab (n=3), envafolimab (n=3), penpulimab (n=1), cadonilimab (n=1) and atezolizumab (n=1). The irAEs were monitored using physical examination, laboratory and radiological detection. The management of irAEs was carried out based on National Comprehensive Cancer Network (NCCN) guidelines, where ICI therapy was considered to be permanently discontinued in case that grade 3 or 4 irAE was observed. Chemotherapy and radiotherapy were administered to 254 and 25 patients, respectively. Targeted therapy was given to 84 patients, including anlotinib (n=21), apatinib (n=18), lenvatinib (n=15), bevacizumab (n=11), trastuzumab (n=5), sorafenib (n=5), sulfatinib (n=3), regorafenib (n=3), pyrotinib (n=1), fruquintinib (n=1), and nimotuzumab (n=1).
Oncological Assessment
For oncological assessment, serum tumor marker measurement and radiological assessments were carried out every two to three treatment cycles. The therapy response was determined using Response Evaluation Criteria in Solid Tumors (RECIST) 1.1 criteria and classified into complete response (CR), partial response (PR), progressive disease (PD), and stable disease (SD). The clinical outcome was assessed using OS and PFS, where OS was defined as the time interval from the first ICI initiation to death caused by any reason or the last follow-up, and PFS was defined as the time interval from the first ICI initiation to disease progression or the last follow-up.
Statistical Analysis
All statistical analyses were performed using SPSS (version 26.0), and figures were generated with GraphPad Prism (version 10.0). Associations between PNI/SII and clinicopathological variables were examined using the chi-square test. Survival curves were estimated by the Kaplan–Meier method and compared with the Log rank test. Potential prognostic factors were evaluated using univariate and multivariable Cox proportional hazards regression models. A two-sided p value < 0.05 was considered statistically significant.
Results
Clinical Characteristics of the Patients
After applying the predefined inclusion and exclusion criteria, 350 patients were ultimately included in the retrospective cohort, and their clinicopathological characteristics are summarized in Table 1. None of the patients received the drugs that potentially induce cancer before initial diagnosis. The cohort had a median age of 68 years, with ages ranging between 30 and 86 years. In detail, the age distribution was as follows: 18–49 years old (n=15, 4.29%), 50–59 years old (n=66, 18.86%), 60–69 years old (n=129, 36.86%), 70–79 years old (n=117, 33.43%) and over 80 years old (n=23, 6.57%). In total, 267 (76.29%) and 83 (23.71%) patients were male and female, respectively. About 281 (80.2%) patients were found to have no HIV/HCV/HBV infection, with 5 HBV and 2 HCV cases. The serological virus history was missing in 62 cases (17.7%). The cancer types included NSCLC (n=128, 36.57%) and digestive system cancer (n=222, 63.43%). Among the patients, 114 were classified as stage III and 236 as stage IV. A total of 324 patients underwent combined therapies, whereas the others received ICI monotherapy. A total of 127 patients had smoking history, and 202 patients had alcohol consumption history. According to the cut-off values, 104 and 246 patients had high and low PNI, respectively, while 107 and 243 patients had high and low SII, respectively. The correlation analysis demonstrated PNI was uncorrelated with any clinical feature, however SII was significantly with cancer type, surgery history and smoking.
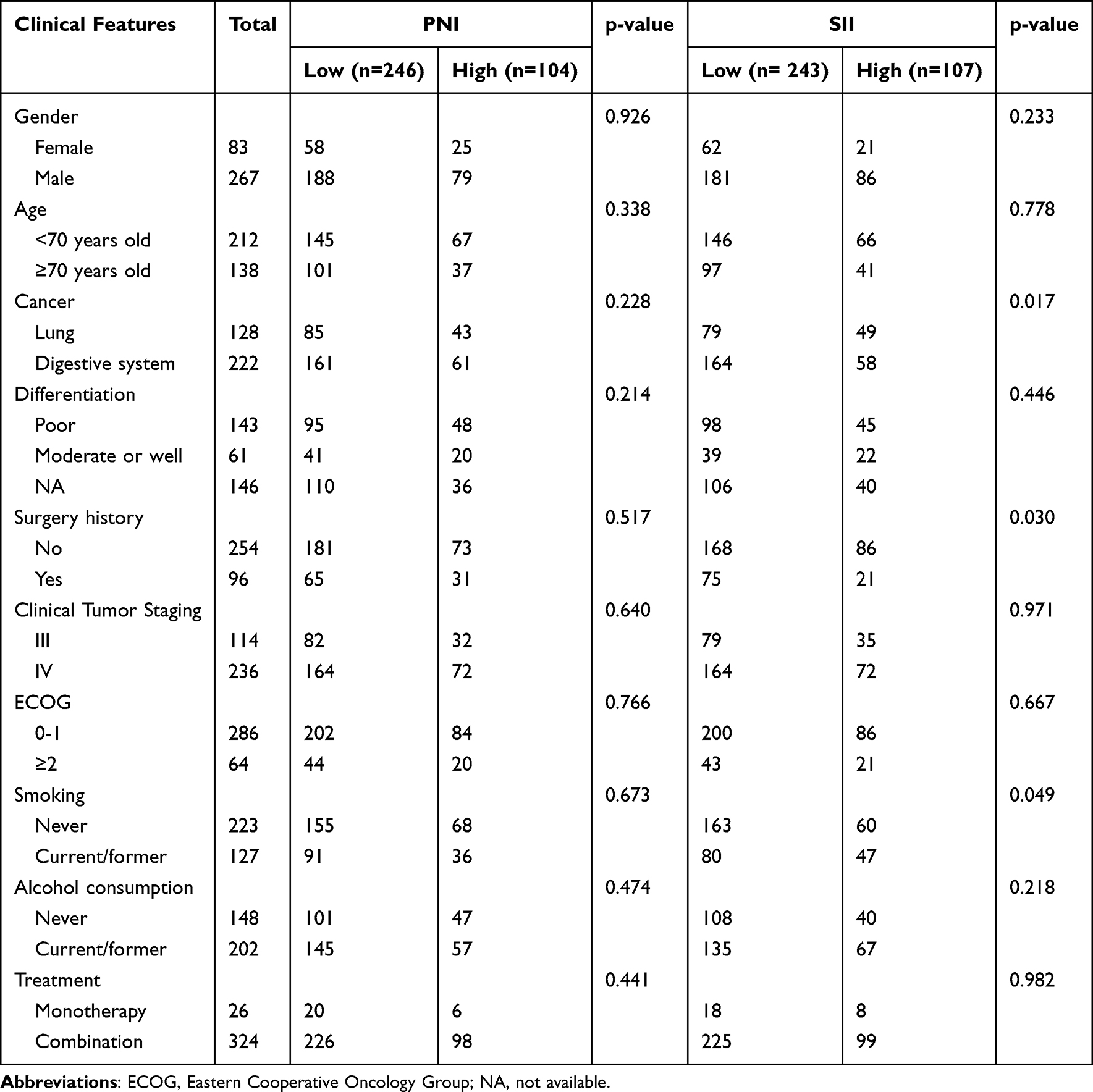 |
Table 1 Baseline Characteristics of the Entire Cohort |
Prognostic Significance of PNI and SII in ICI-Treated Cancer Patients
For the entire cohort, high PNI was significantly correlated with better OS (p<0.001, Figure 2A) and PFS (p<0.001, Figure 2B) of ICI-treated cancer patients. In contrast, high SII was significantly correlated with worse OS (p<0.001, Figure 2C) and PFS (p=0.004, Figure 2D). The univariate analysis demonstrated that age, cancer type, smoking, PNI and SII were significant prognostic factors for OS, while cancer type, age, PNI and SII were independent prognostic factors in the multivariate analysis (Table S1). In terms of PFS, PNI and SII were significant prognostic factors in the univariate analysis, both of which were also confirmed in the multivariate analysis (Table S2).
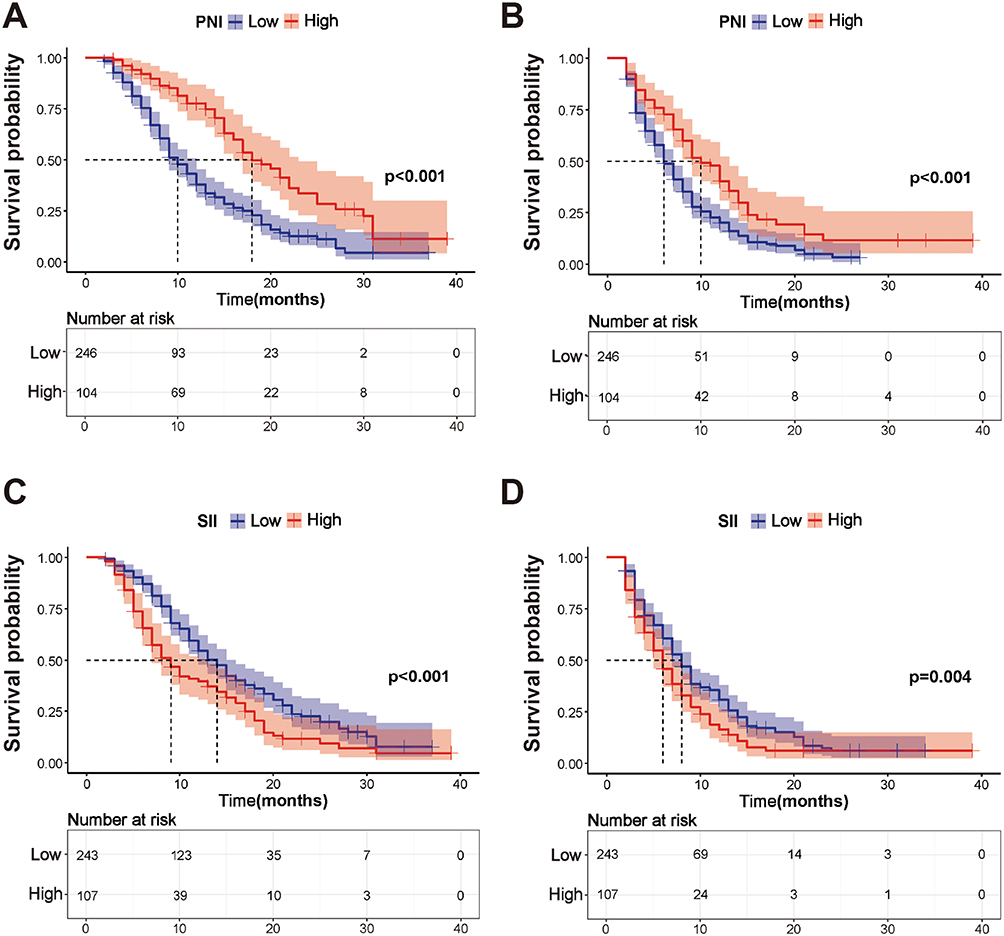 |
Figure 2 Prognostic significance of PNI and SII in cancer patients receiving immune checkpoint inhibitors (ICIs). (A and B) Kaplan–Meier curves for the association of PNI with overall survival (OS) (A) and progression-free survival (PFS) (B) in cancer patients receiving ICIs. (C and D) Kaplan–Meier curves for the association of SII with OS (C) and PFS (D) in cancer patients receiving ICIs. |
Prognostic Significance of PNI and SII in the Selected Subgroups
A total of 128 patients with NSCLC were enrolled in the entire cohort, and their clinical features were summarized in Table S3. The survival analysis demonstrated a positive correlation between high PNI and better clinical outcome (OS, p<0.001, Figure S2A; PFS, p=0.003, Figure S2B). The opposite result was observed in the patients with high SII (OS, p<0.001, Figure S2C; PFS, p=0.01, Figure S2D).
For digestive system cancers, 222 patients were analyzed and their clinical features were summarized in Table S4. Patients in the high-PNI group experienced significantly longer OS (p<0.001) and PFS (p=0.001) compared with those with low PNI (Figure S3A and B). However, SII did not show a statistically significant association with either OS (p=0.083) or PFS (p=0.16) in this subgroup (Figure S3C and D).
In patients with smoking history (n=127), high PNI was significantly correlated with better OS (p<0.001, Figure S4A) and PFS (p=0.008, Figure S4B), whereas high SII showed the opposite trend (OS, p<0.001, Figure S4C; PFS, p=0.023, Figure S4D). In patients without smoking history (n=223), the correlations of PNI with clinical outcome were still statistically significant (all p<0.05, Figure S4E and F), but not for SII (all p>0.05, Figure S4G and H).
Prognostic Significance of the PNI-SII Score in ICI-Treated Cancer Patients
For better utilization of PNI and SII in prognosis prediction, both the indexes were then integrated to form a PNI-SII score. According to the scoring system, the entire cohort was divided into three groups (score 0, n=82; score 1, n=183; score 2, n=85). The PNI-SII model achieved an AUC of 0.650 (95% CI: 0.583–0.716) in the original dataset. After 1,000 bootstrap resampling repetitions, the optimism-corrected AUC was 0.649 (95% CI: 0.622–0.666), indicating relatively stable model performance with moderate discriminative ability (Figure S5A and B). The survival analysis demonstrated that the PNI-SII score effectively stratified the OS (Figure 3A) and PFS (Figure 3B), where patients with score 0 had the best prognosis and the opposite was for those with score 2.
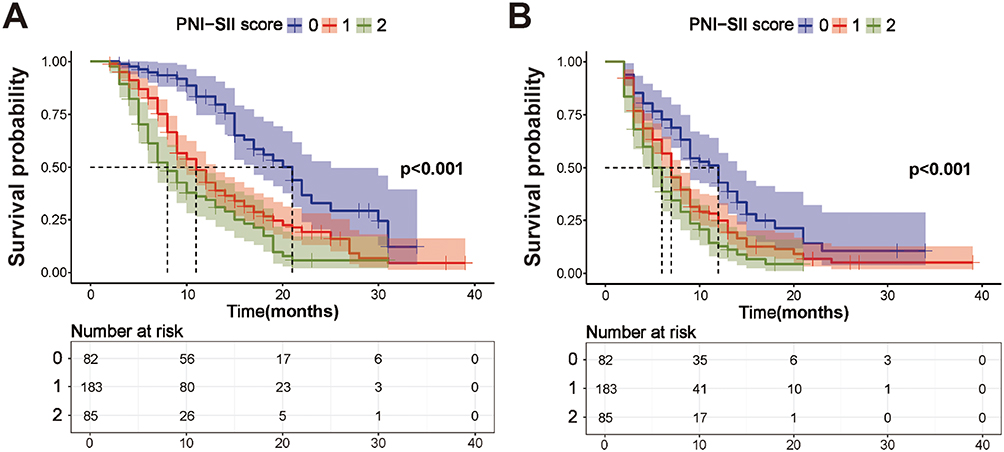 |
Figure 3 Prognostic significance of PNI-SII score in cancer patients receiving immune checkpoint inhibitors (ICIs). Kaplan–Meier curves for the association of PNI-SII score with overall survival (A) and progression-free survival (B) in cancer patients receiving ICIs. Number-at-risk tables are shown below each Kaplan–Meier curve. Median survival times with corresponding 95% confidence intervals were reported for each PNI-SII score group. For OS, the median survival times were 20.0 months (95% CI: 16.50–23.49) for score 0, 11.0 months (95% CI: 9.21–12.79) for score 1, and 8.0 months (95% CI: 6.14–9.86) for score 2. For PFS, the median survival times were 12.0 months (95% CI: 9.65–14.36) for score 0, 7.0 months (95% CI: 6.31-7.69) for score 1, and 5.0 months (95% CI: 4.00–6.00) for score 2. |
For further clarifying its prognostic value, the subgroup analysis was conducted across cancer types. The PNI-SII score effectively stratified the OS (p<0.001) and PFS (p=0.002) in NSCLC (Figure 4A-B). The similar results were also observed in patients with digestive cancers (OS, p<0.001, Figure 4C; PFS, p=0.005, Figure 4D). To investigate whether the prognostic value of the PNI-SII score was attributable to an interaction between PNI and SII, an interaction analysis was performed in the digestive cancer subgroup. No significant interaction was observed for either OS (p for interaction = 0.443) or PFS (p for interaction = 0.846).
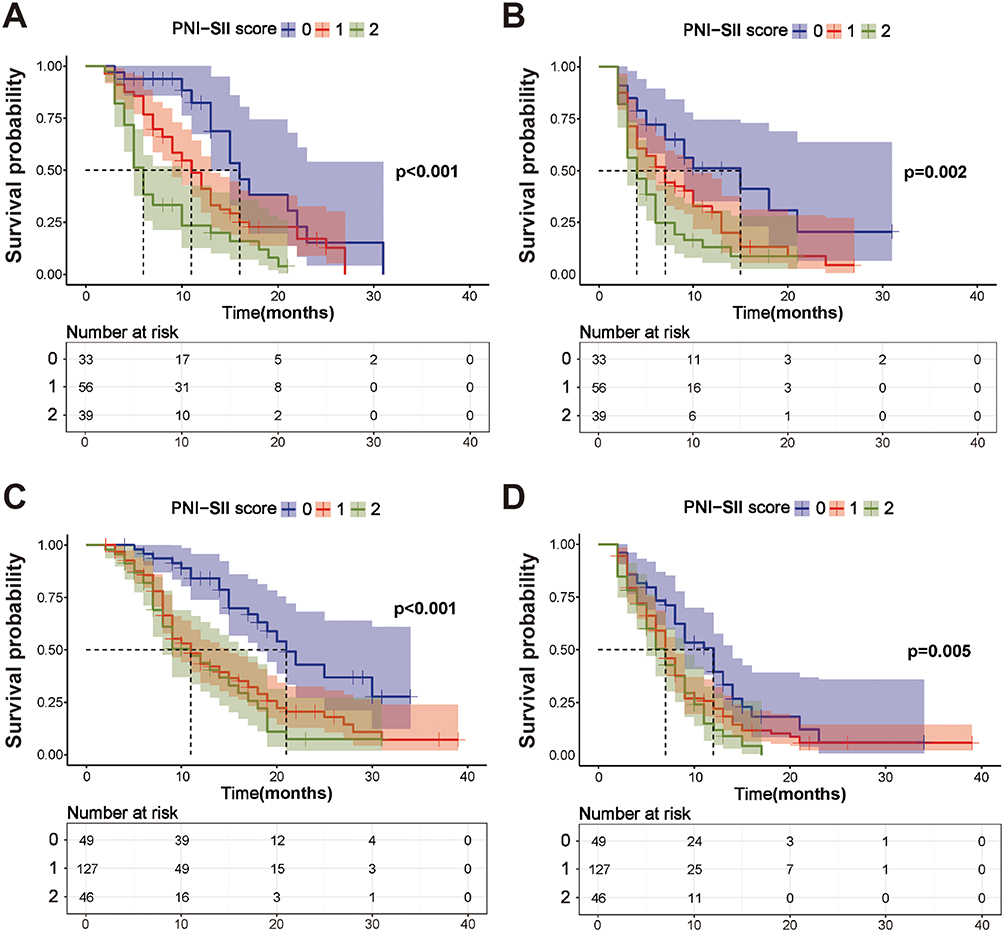 |
Figure 4 Prognostic significance of PNI-SII score in non-small cell lung cancer and digestive cancer patients receiving immune checkpoint inhibitors (ICIs). (A and B) Kaplan–Meier curves for the association of PNI-SII score with overall survival (OS) (A) and progression-free survival (PFS) (B) in non-small cell lung cancer patients receiving ICIs. (C and D) Kaplan–Meier curves for the association of PNI-SII score with OS (C) and PFS (D) in digestive cancer patients receiving ICIs. |
In patients aged over 70 years old (n=138), patients with high PNI-SII score had a significantly worse OS (p<0.001, Figure 5A) and PFS (p=0.013, Figure 5B) compared with those with low PNI-SII score. The same result was observed in patients aged below 70 years old (n=212, OS, p<0.001, Figure 5C; PFS, p<0.001, Figure 5D). Stratified by smoking status, the association between the PNI–SII score and outcomes remained significant in patients with a smoking history (n=127) (OS, p<0.001, Figure 6A; PFS, p=0.006, Figure 6B). For patients without smoking history (n=223), this correlation still reached statistical significance in OS (p<0.001, Figure 6C) and PFS (p=0.002, Figure 6D).
 |
Figure 5 Prognostic significance of PNI-SII score in the subgroup analysis based on age. (A and B) Kaplan–Meier curves for the association of PNI-SII score with overall survival (OS) (A) and progression-free survival (PFS) (B) in patients aged over 70 years old. (C and D) Kaplan–Meier curves for the association of PNI-SII score with OS (C) and PFS (D) in patients aged below 70 years old. |
 |
Figure 6 Prognostic significance of PNI-SII score in the subgroup analysis based on smoking history. (A and B) Kaplan–Meier curves for the association of PNI-SII score with overall survival (OS) (A) and progression-free survival (PFS) (B) in patients current or former smoking. (C and D) Kaplan–Meier curves for the association of PNI-SII score with OS (C) and PFS (D) in patients never smoking. |
Furthermore, to assess the prognostic performance of the PNI-SII score within a prevalent treatment regimen, we performed a subgroup analysis in patients receiving anti–PD-1–based combination therapy. As illustrated in Supplementary Figure 6, the PNI-SII score effectively discriminated survival outcomes in this subset, with significant differences in both OS (p < 0.001, Figure S6A) and PFS (p < 0.001, Figure S6B). These results indicate that the prognostic value of the PNI-SII score remains robust even in a more homogeneous patient population defined by a specific immunotherapeutic strategy.
Correlation of the PNI-SII Score with Short-Term Tumor Response and Therapy Related Adverse Events
As shown in Figure 7, within four treatment cycles, there were 48 PR, 16 PD and 18 SD cases in patients with score 0, compared with 63 PR, 57 PD and 63 SD cases in patients with score 1 and 22 PR, 34 PD and 29 SD cases in patients with score 2, respectively. The objective response rate (ORR) of patients with score 0 was 58.54%, which was higher than that of patients with score 1 (34.43%) or 2 (25.88%). The disease control rate (DCR) of patients with score 0 was 80.49%, which was also higher than that of patients with score 1 (68.85%) or 2 (60.00%).
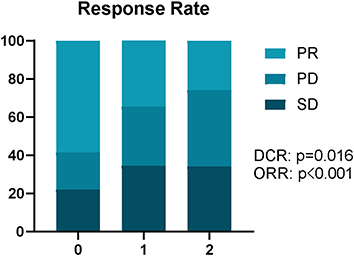 |
Figure 7 Correlations of PNI-SII score with therapy response within four treatment cycles in solid cancer patients receiving immune checkpoint inhibitors (ICIs). |
The correlation of the PNI-SII score with short-term (within four cycles) therapy related adverse events was summarized in Table S5 and Table S6. For patients receiving ICI monotherapy (n=26, Table S5), higher incidence of dermatologic toxicity and endocrine toxicity was observed in patients with a PNI-SII score of 0. For patients receiving combined therapies (n=324, Table S6), dermatologic and endocrine toxicities also tended to be more frequent in patients with a PNI-SII score of 0.
Discussion
Previous studies have provided numerous predictive biomarkers for ICI therapy, while some limitations restrict their actual application. For example, PD-L1 expression is commonly identified as a powerful prognostic indicator for ICI-treated cancer patients.22 However, its actual predictive role in some cancers still needs to be validated.23,24 In addition, different immunohistochemistry techniques for PD-L1 detection may result in discrepant conclusions.25 The alterations of gut microbiome have been linked with the efficacy of ICI drugs in numerous cancer types, while how to developing one or more bacteria in reliable clinical detectable biomarkers is extremely challenging.25,26 The tumor mutational burden (TMB) can also be utilized to predict the response to ICI therapy, but the high cost of gene sequencing limits its actual use.27,28 Recently, increasing studies have identified several nutritional or inflammatory markers as potential predictors for ICI therapy, representatively known as PNI and SII.15,29 However, considering the complexity of oncological evaluation, single nutritional or inflammatory marker may be far from sufficient to accurately predict patient outcome. To our knowledge, few studies are currently available to assess the predictive performance of combined nutritional and inflammatory markers. Therefore, the PNI-SII score may provide a simple supplementary approach for baseline prognostic assessment using routinely available laboratory parameters, rather than replacing established biomarkers such as PD-L1 expression, TMB, or gut microbiome-related markers.
In this study, the prognostic significance of PNI and SII in ICI-treated cancer patients was investigated. As a result, in the entire cohort, high PNI level was significantly correlated with better OS and PFS, while the opposite was for high SII level. This finding is consistent with several published meta-analysis highlighting their prognostic significance in ICI-treated cancer patients.18,30–32 However, there are some evidences against their prognostic values. For instance, a meta-analysis demonstrated no significant correlation between PNI and OS in NSCLC patients receiving ICIs combined with chemotherapy or as the first-line therapy.33 Another study also found PNI was unrelated with the PFS of lung cancer patients receiving anti-PD-1 therapy.16 In gastric cancer, the 5-year survival predictive sensitivity and specificity of SII were only 66.7% and 62.7%, respectively, which was far from acting as a reliable biomarker.34 These inconsistent findings suggest that the prognostic value of single nutritional or inflammatory markers may vary across different clinical contexts.
Subgroup analyses further showed that the prognostic performance of SII was not consistent across different clinical contexts. Although PNI and SII both stratified survival outcomes in NSCLC patients, only PNI retained prognostic significance in the digestive cancer subgroup. Similarly, SII showed attenuated prognostic value in never-smokers, whereas PNI remained informative. The prognostic value of SII in gastrointestinal malignancies has weakened, which may be related to the differences in the inflammatory tumor microenvironment among various cancer types. The causes of gastrointestinal malignancies are diverse (such as Helicobacter pylori infection, Barrett’s esophagus, adenoma-carcinoma sequence), and each cause will form a unique tumor microenvironment.35–38 The tumor microenvironment of gastrointestinal cancers undergoes a dynamic evolution from an early pro-inflammatory state to a late immunosuppressive state.39 Elevated systemic inflammatory markers may therefore reflect non-tumor-specific inflammation caused by intestinal dysbiosis-related barrier dysfunction, rather than tumor-driven inflammation.40 This heterogeneity of the microenvironment reduces the tumor specificity of SII as a prognostic marker for gastrointestinal malignancies. Smoking is associated with elevated systemic inflammatory markers, including CRP, IL-6, and neutrophils, accompanied by impaired NK cell function and altered lymphocyte composition.41,42 Such smoking-related chronic inflammation and immune remodeling may influence the prognostic relevance of SII, whereas its discriminatory ability may be attenuated in never-smokers with relatively lower baseline systemic inflammation.43 Given the context-dependent performance of SII and the relatively consistent prognostic value of PNI, we further integrated these two indices into a combined PNI-SII score to improve risk stratification.
As a result, PNI combined with SII not only effectively stratified the PFS and OS of the entire cohort but also could be used for predicting the short-term tumor response. Subsequent subgroup analyses confirmed its predictive performance in patients with NSCLC or digestive cancer. Additionally, it was also found to perform well regardless of age and smoking history. To our knowledge, there are numerous studies that have already proved the prognostic value of the combined index in cancer patients receiving other anti-cancer therapies. For instance, PNI combined with SII was found to predict the OS of esophageal cancer patients who received radical surgery and had a pathological TNM stage of T3N0M0.44 This combination was also utilized to predict the clinical outcome of advanced NSCLC patients receiving platinum-doublet chemotherapy.45 In locally advanced gastric cancer, the combined index was associated with sarcopenia and acted as an independent predictive factor for both OS and DFS.21
The improved prognostic value of the combined PNI-SII score may be attributed to the complementary information provided by PNI and SII. PNI mainly reflects nutritional status and immune competence, whereas SII captures systemic inflammatory burden related to neutrophil and platelet activation.46,47 For example, in patients with relatively preserved nutritional and lymphocyte-mediated immune status, the adverse impact of systemic inflammation may be partly buffered.48 Therefore, the PNI-SII score integrates both impaired host immune-nutritional status and enhanced tumor-promoting inflammation, providing a more comprehensive assessment of patient prognosis than either index alone. Collectively, based on our findings and previous evidences, PNI combined with SII has great potential to be used as a novel prognostic biomarker for ICI-treated patients.
Interestingly, although SII alone was not significantly associated with OS or PFS in the digestive cancer subgroup, the combined PNI-SII score remained prognostically significant. Interaction analysis showed no significant interaction between PNI and SII for either OS (p for interaction = 0.443) or PFS (p for interaction = 0.846), suggesting that the value of the combined score was unlikely to be driven by a synergistic interaction effect. Instead, it may reflect complementary prognostic information from nutritional status and systemic inflammation.
Nevertheless, this study mainly focused on the prognostic significance of the PNI-SII score, and its incremental predictive value beyond clinical variables such as tumor stage and ECOG performance status, or beyond PNI/SII alone, should be further quantified in future studies using metrics such as the concordance index, net reclassification improvement, and integrated discrimination improvement.
In addition to survival outcomes, therapy-related adverse events are commonly observed during anti-cancer therapy, which may lead to therapy discontinuation and drug dose reduction. Several previous studies have closely linked PNI or SII with therapy-related adverse events. For instance, high PNI level was associated with higher incidence of immune-related adverse events (irAEs) as compared with low PNI level (<45) in SCLC patients receiving first-line chemoimmunotherapy.49 This finding was also confirmed by another retrospective work that demonstrated the incidence of irAEs in high PNI group was nearly the double of that in low PNI group.50 The ICI-treated microsatellite instability-high metastatic colorectal cancer patients who had lower pretreatment SII level were more likely to suffer from irAEs.29 The low SII was significantly correlated with higher frequency of any grade or grade 1–2 irAEs in advanced NSCLC patients receiving chemoimmunotherapy.51 In this study, for both the monotherapy and combined therapy group, patients with high PNI and low SII were observed to have high incidence of irAEs such as dermatologic toxicity. This result can be partly explained by the fact that the occurrence of irAEs commonly indicated better therapy response to ICI drugs.52,53 Patients with high PNI and low SII may have better anti-cancer immune response, which may also trigger an autoimmune reaction in irrelevant organs such as thyroid and skin.54 In terms of biological mechanisms, the tumor-reactive T cells are known to display affinity for both tumor neoantigens and self-antigens from healthy tissues. In case that ICI-induced tumor-specific response is weaker than the cross-reactive response in some healthy organs, irAEs are likely to occur.55 On the other hand, due to the limited sample size and short term follow-up, only a few patients with irAEs were included for analysis. Therefore, the actual predictive role of the model in irAEs needs further validations in future.
Some mechanism investigations can be used for explaining the correlation of PNI or SII with ICI efficacy. PNI is determined by the level of albumin and lymphocyte, while SII is determined by the level of platelet, neutrophil and lymphocyte. The increased level of albumin was found to associate with improved efficacy of ICI drugs in a dose-dependent manner, which can be partly attributed to its regulatory role in the general catabolism of therapeutic IgG antibodies.56 The human serum albumin can be utilized as an effective carrier for the nanovaccine to enhance the T-cell mediated anti-cancer immune response.57 The platelets not only promote tumor invasion and migration through inducing epithelial mesenchymal transition but also protect circulating tumor cells from immune surveillance.58 Accordingly, aspirin as a well-known anti-platelet drug has been proved to upregulate CD80 expression and increase CD8/CD3 ratio, resulting activated immune surveillance in colorectal cancer.59 The activated neutrophils can impair T cell function through upregulating PD-L1 expression and have been widely used in predicting the prognosis of ICI-treated cancer patients.60 Emerging evidences have linked their immunosuppressive role with the formation of neutrophil extracellular traps in tumor microenvironment, which influences the function of CD8+ T cells and CD4+ T cells.61 Considering the potential impact of these factors on ICI therapy, they were integrated into a novel predictive model that was then successfully validated in our cohort. The present findings confirmed their prognostic significance in ICI-treated cancer patients and suggested the necessity of further investigation into their role in tumor immunity.
As a retrospective study, some inherent limitations should be mentioned. Firstly, the cut-off values of PNI and SII were determined by the various methods according to previous studies, which may directly impact the results. Although bootstrap internal validation was performed to assess model robustness, external validation in independent prospective cohorts is still required. Secondly, due to limited sample size, some cancer types such as small cell lung cancer, head and neck cancer and gynecological cancer were not included in our study. The actual clinical significance of PNI and SII in these cancers needs further investigations. Thirdly, the heterogeneity of ICI agents and treatment strategies may have influenced clinical outcomes and therapy-related adverse events. In particular, most patients received anti-PD-1 therapy, whereas the sample sizes of non-PD-1 therapy and ICI monotherapy subgroups were small, limiting reliable subgroup analyses according to ICI class and treatment strategy. Fourthly, the exclusion of patients with suspected ICI-related hyperprogression may have introduced selection bias. In addition, the lack of PD-L1 expression and TMB data limited direct comparison between the PNI-SII score and established immunotherapy biomarkers. Finally, the correlation of the model with long-term therapy-related adverse events remains unclear and needs to be clarified based on our updated follow-up records. In addition, our study focused on the prognostic impact of pretreatment levels of PNI and SII, but whether their dynamic changes during ICI therapy have any clinical significance is currently unknown and worthy of further investigation.
In conclusion, our study demonstrated that both PNI and SII could serve as reliable prognostic biomarkers for ICI-treated cancer patients. In addition, a novel model based on PNI and SII was developed for more accurate prediction of clinical outcome. These findings collectively highlight the crucial role of nutrition and inflammation in tumor immunity.
Acknowledgments
We would like to thank HOME for Researchers for providing English language editing and reviewing services for this manuscript.
Author Contributions
Jingxian Mao, Huaijuan Guo and Jingjing Yang contributed equally to this work and should be considered co-first authors. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was financially supported by the China National Natural Science Foundation (No. 81902422), Jiangsu Natural Science Foundation (No. BK20231245), Program of Jiangsu Commission of Health (No. M2020024), Program of Yangzhou Commission of Health (No. 2023-2-01 and 2024-2-08), Clinical Translational Foundation of Yangzhou University (No. AHYZUZHXM 202104) and Postgraduate Practice Innovation Program of Jiangsu Province (No. KYCX23_3621).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Chen Z, Hu T, Zhou J, et al. Overview of tumor immunotherapy based on approved drugs. Life Sci. 2024;340:122419. doi:10.1016/j.lfs.2024.122419
2. Wang H, Xie J, Li N, et al. Unraveling immunotherapy resistance in solid tumors: decoding mechanisms and charting future therapeutic landscapes. Oncol Res. 2025;33(12):3789–15. doi:10.32604/or.2025.067592
3. Zhang M, Xu J, Zheng Z, et al. The role of immune checkpoint molecules in cancers. Front Immunol. 2026;16:1674818. doi:10.3389/fimmu.2025.1674818
4. Meng L, Wu H, Wu J, et al. Mechanisms of immune checkpoint inhibitors: insights into the regulation of circular RNAS involved in cancer hallmarks. Cell Death Dis. 2024;15(1):3. doi:10.1038/s41419-023-06389-5
5. Ouyang P, Wang L, Wu J, et al. Overcoming cold tumors: a combination strategy of immune checkpoint inhibitors. Front Immunol. 2024;15:1344272. doi:10.3389/fimmu.2024.1344272
6. Yang M, Wang Y, Yuan M, et al. Antibiotic administration shortly before or after immunotherapy initiation is correlated with poor prognosis in solid cancer patients: an up-to-date systematic review and meta-analysis. Int Immunopharmacol. 2020;88:106876. doi:10.1016/j.intimp.2020.106876
7. Liu C, Guo H, Mao H, et al. An up-to-date investigation into the correlation between proton pump inhibitor use and the clinical efficacy of immune checkpoint inhibitors in advanced solid cancers: a systematic review and meta-analysis. Front Oncol. 2022;12:753234. doi:10.3389/fonc.2022.753234
8. Guo H, Li Y, Lin J, et al. A novel investigation into the negative impact of opioid use on the efficacy of immune checkpoint inhibitors in advanced non-small cell lung cancer patients. Int Immunopharmacol. 2024;129:111611. doi:10.1016/j.intimp.2024.111611
9. Zou Y, Wu J, Yuan Z, et al. Targeting the neuro-immune crosstalk in breast cancer brain metastases. J Immunother Cancer. 2026;14(4):e014134. doi:10.1136/jitc-2025-014134
10. Spagnolo CC, Pepe F, Ciappina G, et al. Circulating biomarkers as predictors of response to immune checkpoint inhibitors in NSCLC: are we on the right path? Crit Rev Oncol Hematol. 2024;197:104332. doi:10.1016/j.critrevonc.2024.104332
11. Sambataro D, Politi MR, Messina A, et al. Relationship of inflammatory parameters and nutritional status in cancer patients. Anticancer Res. 2023;43(6):2821–2829. doi:10.21873/anticanres.16451
12. Wang Y, Huang K, Chen C, et al. The predictive value of baseline systemic inflammation response index and systemic immune-inflammation index for the risk of infection within 6 months following initial immunosuppressive treatment in patients with ANCA-associated vasculitis. Front Immunol. 2026;17:1718901. doi:10.3389/fimmu.2026.1718901
13. Chen H, Mo Q, Huang M-T, et al. Systemic immune-inflammation index predicts acute histologic chorioamnionitis pathologic staging and neonatal respiratory distress syndrome in women with preterm premature rupture of membranes: a retrospective cohort study. BMC Pregnancy Childbirth. 2025;25(1):1244. doi:10.1186/s12884-025-08446-7
14. Buzby GP, Mullen JL, Matthews DC, et al. Prognostic nutritional index in gastrointestinal surgery. Am J Surg. 1980;139(1):160–167. doi:10.1016/0002-9610(80)90246-9
15. Yang J, Li H, Li L, et al. Prognostic role of pretreatment prognostic nutritional index in advanced lung cancer patients receiving first-line immunotherapy: a meta-analysis. Cureus. 2024;16(1):e52720. doi:10.7759/cureus.52720
16. Yan X, Wang J, Mao J, et al. Identification of prognostic nutritional index as a reliable prognostic indicator for advanced lung cancer patients receiving immune checkpoint inhibitors. Front Nutr. 2023;10:1213255. doi:10.3389/fnut.2023.1213255
17. Zeng QY, Qin Y, Shi Y, et al.Systemic immune-inflammation index and all-cause and cause-specific mortality in sarcopenia: a study from national health and nutrition examination survey 1999-2018.Front Immunol.2024.15;1376544. doi:10.3389/fimmu.2024.1376544
18. Wang Y, Ni Q. Prognostic and clinicopathological significance of Systemic Immune-Inflammation Index in cancer patients receiving immune checkpoint inhibitors: a meta-analysis. Ann Med. 2023;55(1):808–819. doi:10.1080/07853890.2023.2181983
19. Mahiat C, Bihin B, Duplaquet F, et al. Systemic inflammation/nutritional status scores are prognostic but not predictive in metastatic non-small-cell lung cancer treated with first-line immune checkpoint inhibitors. Int J Mol Sci. 2023;24(4):3618. doi:10.3390/ijms24043618
20. Ding P, Guo H, Sun C, et al. Combined systemic immune-inflammatory index (SII) and prognostic nutritional index (PNI) predicts chemotherapy response and prognosis in locally advanced gastric cancer patients receiving neoadjuvant chemotherapy with PD-1 antibody sintilimab and XELOX: a prospective study. BMC Gastroenterol. 2022;22(1):121. doi:10.1186/s12876-022-02199-9
21. Ding P, Lv J, Sun C, et al. Combined systemic inflammatory immunity index and prognostic nutritional index scores as a screening marker for sarcopenia in patients with locally advanced gastric cancer. Front Nutr. 2022;9:981533. doi:10.3389/fnut.2022.981533
22. Kuang X, Xu R, Li J. Association of PD-L1 expression with survival benefit from PD-1/PD-L1 inhibitors in advanced cancer: systematic review and meta-analysis of Phase III randomized clinical trials. Crit Rev Oncol Hematol. 2024;198:104357. doi:10.1016/j.critrevonc.2024.104357
23. Maiorano BA, Di Maio M, Cerbone L, et al. Significance of PD-L1 in metastatic urothelial carcinoma treated with immune checkpoint inhibitors: a systematic review and meta-analysis. JAMA Netw Open. 2024;7(3):e241215. doi:10.1001/jamanetworkopen.2024.1215
24. Fitzsimmons TS, Singh N, Walker TDJ, et al. Immune checkpoint inhibitors efficacy across solid cancers and the utility of PD-L1 as a biomarker of response: a systematic review and meta-analysis. Front Med. 2023;10:1192762. doi:10.3389/fmed.2023.1192762
25. de Ruiter EJ, Mulder FJ, Koomen BM, et al. Comparison of three PD-L1 immunohistochemical assays in head and neck squamous cell carcinoma (HNSCC). Mod Pathol. 2021;34(6):1125–1132. doi:10.1038/s41379-020-0644-7
26. Oh B, Boyle F, Pavlakis N, et al. The gut microbiome and cancer immunotherapy: can we use the gut microbiome as a predictive biomarker for clinical response in cancer immunotherapy? Cancers. 2021;13(19):4824. doi:10.3390/cancers13194824
27. Li Y, Ji L, Zhang Y, et al. The combination of tumor mutational burden and T-cell receptor repertoire predicts the response to immunotherapy in patients with advanced non-small cell lung cancer. MedComm. 2024;5(6):e604. doi:10.1002/mco2.604
28. Klümper N, Grünwald V, Hartmann A, et al. The role of microsatellite instability/dna mismatch repair deficiency and tumor mutational burden as biomarkers in predicting response to immunotherapy in castration-resistant prostate cancer. Eur Urol. 2024;86(5):388–390. doi:10.1016/j.eururo.2024.04.026
29. Yi J, Xue J, Yang L, et al. Predictive value of prognostic nutritional and systemic immune-inflammation indices for patients with microsatellite instability-high metastatic colorectal cancer receiving immunotherapy. Front Nutr. 2023;10:1094189. doi:10.3389/fnut.2023.1094189
30. Zhang L, Ma W, Qiu Z, et al. Prognostic nutritional index as a prognostic biomarker for gastrointestinal cancer patients treated with immune checkpoint inhibitors. Front Immunol. 2023;14:1219929. doi:10.3389/fimmu.2023.1219929
31. Ni L, Huang J, Ding J, et al. Prognostic nutritional index predicts response and prognosis in cancer patients treated with immune checkpoint inhibitors: a systematic review and meta-analysis. Front Nutr. 2022;9:823087. doi:10.3389/fnut.2022.823087
32. Tian BW, Yang YF, Yang CC, et al. Systemic immune-inflammation index predicts prognosis of cancer immunotherapy: systemic review and meta-analysis. Immunotherapy. 2022;14(18):1481–1496. doi:10.2217/imt-2022-0133
33. Xia H, Zhang W, Zheng Q, et al. Predictive value of the prognostic nutritional index in advanced non-small cell lung cancer patients treated with immune checkpoint inhibitors: a systematic review and meta-analysis. Heliyon. 2023;9(8):e17400. doi:10.1016/j.heliyon.2023.e17400
34. Uzunoglu H, Kaya S. Does systemic immune inflammation index have predictive value in gastric cancer prognosis? North Clin Istanb. 2023;10(1):24–32. doi:10.14744/nci.2021.71324
35. Barchi A, Dell’Anna G, Massimino L, et al. Unraveling the pathogenesis of Barrett’s esophagus and esophageal adenocarcinoma: the “omics” era. Front Oncol. 2025;14:1458138. doi:10.3389/fonc.2024.1458138
36. Chen J, Ye J, Lai R. A lipid metabolism-related gene signature reveals dynamic immune infiltration of the colorectal adenoma-carcinoma sequence. Lipids Health Dis. 2023;22(1):92. doi:10.1186/s12944-023-01866-4
37. Zhou B, Liu Q, Huang C, et al. Progressively altered genes in colorectal carcinogenesis link oncogenesis immune cycle and tumor microenvironment. Sci Rep. 2025;15(1):37495. doi:10.1038/s41598-025-21401-y
38. Duan Y, Xu Y, Dou Y, et al. Helicobacter pylori and gastric cancer: mechanisms and new perspectives. J Hematol Oncol. 2025;18(1):10. doi:10.1186/s13045-024-01654-2
39. Greten FR, Grivennikov SI. Inflammation and Cancer: triggers, Mechanisms, and Consequences. Immunity. 2019;51(1):27–41. doi:10.1016/j.immuni.2019.06.025
40. Garrett WS. Cancer and the microbiota. Science. 2015;348(6230):80–86. doi:10.1126/science.aaa4972
41. Elisia I, Lam V, Cho B, et al. The effect of smoking on chronic inflammation, immune function and blood cell composition. Sci Rep. 2020;10(1):19480. doi:10.1038/s41598-020-76556-7
42. Aloe C, Wang H, Vlahos R, et al. Emerging and multifaceted role of neutrophils in lung cancer. Transl Lung Cancer Res. 2021;10(6):2806–2818. doi:10.21037/tlcr-20-760
43. Feier CVI, Muntean C, Faur AM, et al. Exploring inflammatory parameters in lung cancer patients: a retrospective analysis. J Pers Med. 2024;14(6):552. doi:10.3390/jpm14060552
44. Ma H, Liu Y, Ye H, et al. The prognostic value of preoperative laboratory data indicators in patients with esophageal carcinoma: an observational study. Medicine. 2024;103(24):e38477. doi:10.1097/md.0000000000038477
45. Fan R, Chen Y, Xu G, et al. Combined systemic immune-inflammatory index and prognostic nutritional index predict outcomes in advanced non-small cell lung cancer patients receiving platinum-doublet chemotherapy. Front Oncol. 2023;13:996312. doi:10.3389/fonc.2023.996312
46. Keskinkilic M, Semiz HS, Ataca E, et al. The prognostic value of immune-nutritional status in metastatic colorectal cancer: prognostic Nutritional Index (PNI). Support Care Cancer. 2024;32(6):374. doi:10.1007/s00520-024-08572-6
47. Wu Y, Huang Y, Wu Y, et al. Systemic immune-inflammation index as a versatile biomarker in autoimmune disorders: insights from rheumatoid arthritis, lupus, and spondyloarthritis. Front Immunol. 2025;16:1621209. doi:10.3389/fimmu.2025.1621209
48. Niccolai E. Advancing patient care: the role of nutrition in immune-mediated diseases, spanning from cancer to autoimmunity. Nutrients. 2025;17(23):3632. doi:10.3390/nu17233632
49. Zhang B, Chen J, Yu H, et al. Prognostic nutritional index predicts efficacy and immune-related adverse events of first-line chemoimmunotherapy in patients with extensive-stage small-cell lung cancer. J Inflamm Res. 2024;17:1777–1788. doi:10.2147/jir.S450804
50. Furuno T, Sogawa R, Hashimoto T, et al. Association between the prognostic nutritional index and the occurrence of immune-related adverse events. Biol Pharm Bull. 2024;47(2):361–365. doi:10.1248/bpb.b23-00760
51. Anpalakhan S, Huddar P, Behrouzi R, et al. Immunotherapy-related adverse events in real-world patients with advanced non-small cell lung cancer on chemoimmunotherapy: a Spinnaker study sub-analysis. Front Oncol. 2023;13:1163768. doi:10.3389/fonc.2023.1163768
52. Ma S, Nie H, Wei C, et al. Association between immune-related adverse events and prognosis in patients with advanced non-small cell lung cancer: a systematic review and meta-analysis. Front Oncol. 2024;14:1402017. doi:10.3389/fonc.2024.1402017
53. Curkovic NB, Bai K, Ye F, et al. Incidence of cutaneous immune-related adverse events and outcomes in immune checkpoint inhibitor-containing regimens: a systematic review and meta-analysis. Cancers. 2024;16(2):340. doi:10.3390/cancers16020340
54. Ding P, Liu P, Meng L, et al. Mechanisms and biomarkers of immune-related adverse events in gastric cancer. Eur J Med Res. 2023;28(1):492. doi:10.1186/s40001-023-01365-3
55. Yoest JM. Clinical features, predictive correlates, and pathophysiology of immune-related adverse events in immune checkpoint inhibitor treatments in cancer: a short review. Immunotargets Ther. 2017;6:73–82. doi:10.2147/itt.S126227
56. Zheng M. Serum albumin: a pharmacokinetic marker for optimizing treatment outcome of immune checkpoint blockade. J Immunother Cancer. 2022;10(12):e00567. doi:10.1136/jitc-2022-005670
57. Zheng A, Ning Z, Wang X, et al. Human serum albumin as the carrier to fabricate STING-activating peptide nanovaccine for antitumor immunotherapy. Mater Today Bio. 2024;(25):100955. doi:10.1016/j.mtbio.2024.100955
58. Zhou L, Zhang Z, Tian Y, et al. The critical role of platelet in cancer progression and metastasis. Eur J Med Res. 2023;28(1):385. doi:10.1186/s40001-023-01342-w
59. Simoni O, Scarpa M, Castagliuolo I, et al. IMMUNOREACT 7: regular aspirin use is associated with immune surveillance activation in colorectal cancer. Cancer. 2024;130(13):2272–2286. doi:10.1002/cncr.35297
60. Guo Y, Xiang D, Wan J, et al. Focus on the dynamics of neutrophil-to-lymphocyte ratio in cancer patients treated with immune checkpoint inhibitors: a meta-analysis and systematic review. Cancers. 2022;14(21):5297. doi:10.3390/cancers14215297
61. Fang Q, Stehr AM, Naschberger E, et al. No NETs no TIME: crosstalk between neutrophil extracellular traps and the tumor immune microenvironment. Front Immunol. 2022;13:1075260. doi:10.3389/fimmu.2022.1075260
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.