Back to Journals » Advances in Medical Education and Practice » Volume 16
A Novel Multidimensional Fidelity Framework for Cardiac Surgery Simulation: A Thematic Literature Review
Authors Alharbi MA, Muller Moran HR, Maurice-Ventouris M, Harley JM, Lachapelle KJ
Received 6 October 2025
Accepted for publication 10 December 2025
Published 25 December 2025 Volume 2025:16 Pages 2419—2430
DOI https://doi.org/10.2147/AMEP.S572421
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sateesh Arja
Mohammed A Alharbi,1 Hellmuth R Muller Moran,2 Meagane Maurice-Ventouris,2 Jason M Harley,2 Kevin J Lachapelle2
1Department of Surgery, Imam Abdulrahman bin Faisal University, Dammam, Saudi Arabia; 2Department of Surgery, McGill University, Montreal, QC, Canada
Correspondence: Kevin J Lachapelle, Department of Surgery, McGill University, 1650 Cedars Av, L9, Montreal, QC, H4A 3J1, Canada, Tel +1 514 934-1934, ext. 36873, Fax +1 514 843-1602, Email [email protected]
Introduction: Simulation-based training is increasingly being adopted in cardiac surgery to train future surgeons. Although low- and high-fidelity cardiac surgical simulations have been described previously, simulation fidelity or the degree to which a simulation replicates reality is poorly defined and not well established. This study examines the literature on the themes of fidelity using a novel multidimensional surgical framework.
Methods: A keyword-based literature review was conducted to retrieve published cardiac surgical simulation studies using MEDLINE and EMBASE, from January 2000 to February 2020. The search was limited to the date of publication and not by type. Within predefined dimensions, the included articles were thematically analyzed using a hybrid coding approach to identify fidelity themes and subthemes.
Results: Twenty-six articles were included in the thematic analysis after duplicate removal, screening, and eligibility assessment based on the inclusion and exclusion criteria. Seven themes were identified within physical, surgical, and interactional dimensions. They were derived from environmental, equipment, anatomical, physiological, procedural, perceptual, and psychological simulation components. Subthemes for three levels of realism were generated for each theme by using an iterative process.
Conclusion: This fidelity framework provides educators with actionable guidance for designing cost-effective cardiac surgical simulation for competency-based training by enabling selective fidelity utilization. Educators can apply this framework through aligning learning objectives, fidelity dimensions and levels accordingly. The framework facilitates optimal resource allocation by designing effective and fit for learner simulations.
Keywords: surgical education, surgical simulation, cardiovascular surgery, thematic analysis, surgical fidelity
Introduction
Simulation-based cardiac surgery training is a valuable tool to teach complex, invasive, and high-stake procedures in safe environments. Since the beginning, cardiac surgeons have used simulations to practice procedures on animals or cadavers before performing them on humans.1 Recent advances in surgical simulation have motivated training bodies to adapt simulations to resident training. Considering that surgical education is transforming into competency-based training rather than the Halstedian apprenticeship model, simulation-based training could certainly be advantageous.2 Such transition puts pressure on surgical educators to advance simulation-based training curricula and instructional design, and calls for further funding in simulation research.
The literature on cardiac surgical simulation is rich, with several publications documenting significant efforts to design and validate simulators, build simulation experience, and assess their educational value. Notably, the literature presented a multitude of simulation experimentation, from bench-top, low-cost, and do-it-yourself simulators to sophisticated complex simulation programs by major academic centers.1,3,4 Frequently, researchers described their simulators as having low or high fidelity based on their complexity and technical abilities. It is indisputable that increasing simulator functions would increase the cost to design, and operate them.5 As a result, without financial backing, access to so-called “high fidelity” simulators would become limited. Furthermore, this unidimensional approach fails to capture the complexity of surgical training needs which include importance for continuous access to simulation training and the dynamic nature of surgical environments. Because simulation operational costs have become a challenge to simulation-based training, many medical educators have questioned the concept of fidelity.6–8 This prompted educators to study fidelity as a construct and add further controversy.9,10 This led to inconsistent definitions, terminology, and application in the literature, hampering a systematic and clear fidelity conceptualization across disciplines.
In surgical simulation, the relationship between the trainee and simulator is unique and essential. This relationship cannot be characterized exclusively in terms of engineering or simulator functions and capabilities. Surgical simulation fidelity emerges from several aspects of reality around the trainee, including physical elements, procedures, and simulation interactions. Here, the concept of dimensional simulation fidelity by Beaubien et al becomes more relevant and dynamic in surgical simulation design.11 This approach is particularly relevant to surgical simulation where selective use of fidelity may be more important that global high fidelity. In fact, surgical educators can design simulation experiences with fit-for-purpose fidelity and cost efficiency in mind.12 Furthermore, enhancing simulation design by utilizing fidelity could address learner needs and streamline their training and assessment.
Despite growing cardiac surgical simulations, no previous effort has systematically studied how fidelity is conceptualized and reported in the literature. This thematic literature review intends to expand the dimensional fidelity concept by mapping and identifying its themes in cardiac surgical simulation.
Theoretical Framework and Aim
Pragmatically, overarching fidelity dimensions may be derived from actual surgical practice. Kneebone et al demonstrated this in their circles of focus simulation concept.13 In The innermost circle encompasses the surgical field in which surgery is actively been performed, thus establishing a surgical field dimension. Lies outside that circle, the surrounding environment, and its elements; hence, a physical dimension was added. Finally, the outermost least-focused circle represents the general context of the disease. In addition, the trainee’s interaction with the simulation itself could be a major modifier for enhancing simulation authenticity. Rystedt et al advocated considering this interaction as an indication of simulation fidelity. Therefore, we included an interactional dimension14 Importantly, simulation authenticity is defined as the subjective experience of a simulation activity to be relevant to a learner’s reality.
The aim of this thematic review was to identify fidelity themes according to a multidimensional framework expanded from Kneebone et al and Rystedt et al work and to generate subthemes that determine the level of realism (low, intermediate, and high) for each theme within cardiac surgical simulation. The research questions were as follows: (1) What are the fidelity themes in cardiac surgical simulations according to the predefined fidelity dimensions? (2) What subthemes determine their level of realism?
Methods
Study Design and Search Strategy
A literature review was conducted using MEDLINE (January 2000–February 2020) and EMBASE (January 2000–February 2020). Medical Subject Heading (MeSH) terms and keywords were identified using the Population, Interest and Context (PICo) framework for qualitative research. The search strategy was formulated using population (cardiac surgery trainees), interest (surgical simulation), and context (training) (Box A.1 in the appendix). The search covered simulated publications in English, and a search was conducted on the retrieved studies for cited references. Duplicates were removed using MEDLINE and EMBASE database advanced tools.
Screening
Our initial search identified 880 sources of evidence, and 425 article abstracts were retrieved after removing duplicates. Screening of titles and abstracts yielded 99 articles for full-text analysis. Of these, 76 articles did not meet the inclusion and exclusion criteria. Subsequently, 23 articles were included, and three were added from a reference search for a total of 26 articles. The PRISMA flowchart in Figure 1 depicts the screening and assessment processes.
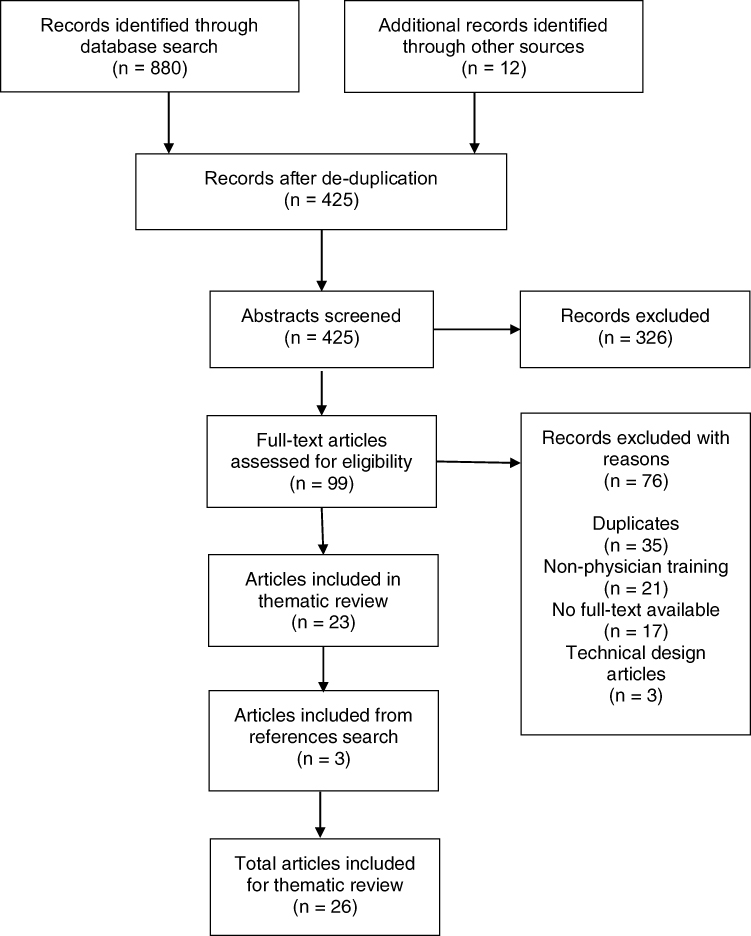 |
Figure 1 PRISMA flowchart of screening and assessment process. |
The full-text review of 99 articles determined eligibility according to predetermined criteria, which included 1) simulation-based training with a defined outcome; 2) involving cardiovascular training; 3) trainees including residents, fellows or attendings 4) including cardiac surgical procedures; 5) all simulator modalities; and 6) including a description of the simulation design. Articles offering a technical description of simulation technology were excluded.
Analysis and Coding
Thematic analysis was conducted to identify themes and subthemes using a hybrid approach with deductive and inductive coding. One author (M.A.) examined the articles’ text, photographs, and video-based data. This process was accomplished by the following established steps: familiarization by reading and viewing data from articles and generating initial codes manually using an iterative process. Themes and subthemes were then identified, the initial results were reviewed by the authors (K.L., J.H., H.M, and M.M)., and a thematic map was created. After the final analysis by the authors (M.A., K.L., and J. H)., themes were organized, renamed, and defined to generate a final report. The coding process included initial deductive coding, where three overarching dimensions (physical, surgical field, and interactional) were examined within the data. This resulted in identifying the initial codes manually and inductive coding, followed by consolidating the extracted codes into 13 initial themes and an extensive search for subthemes. The retrieved subthemes were aimed at identifying the patterns of gradual simulation realism within the data. The review process involved analyzing and testing the final themes and subthemes.
Results
Studies Characteristics
The years of publication of the included studies ranged from 2008 to 2020. Studies were conducted in the United States (n=14), Canada (n=4), China (n=2), Turkey (n=2), and other countries (n=4). The publications were empirical articles, with comparative studies being the most prevalent (single group, pre-post test (n=9), single group, post-test (n=5), randomized controlled trials (n=4), observational studies (n=4), and others (n=4)). Table A.1 in the appendix summarizes other descriptive characteristics, such as simulators utilized, simulator modality, targeted competencies or skills, and outcomes. Targeted cardiac surgical competencies included coronary artery bypass grafting (n=8), aortic and venous cannulation, cardiopulmonary bypass or extracorporeal membrane oxygenation management (n=6), aortic or mitral valve procedures (n=4), multiple cardiac surgical procedures (n=3), heart transplant and left ventricular assist device insertion (n=2), congenital procedures (n=2), and aortic anastomosis (n=1).
Thematic Analysis
The three predefined overarching fidelity dimensions, physical, surgical field, and interactional dimensions by Kneebone et al and Rystedt et al, were the starting point of the analysis by the author (M.A). The deductive coding process started by reading the articles in search of patterns of meaning that might be coded. The initial codes were noted manually and included features that fit under predefined dimensions (eg, physical elements: surgical lights, conversations, alarms, colors, and surgical instruments). This proceeded inductively by looking for themes that aggregated the codes, yielding 13 primary themes (eg, sounds and equipment under the physical dimension). Subsequently, subthemes that generated meanings of gradual increases or reductions in realism (low, intermediate, and high realism) commenced. This was followed by a continuous review of themes and subthemes to ensure consistency across articles. As a result, seven themes generated after redefinition, renaming, and subthemes were reviewed again within the articles to refine and update them (Figure 2). Finally, two themes were identified and reported for the physical dimension: (1) the simulation environment and (2) simulation equipment. Three themes were identified in the surgical field dimension: (3) surgical anatomy, (4) surgical physiology or pathology, and (5) procedural steps. Finally, the two themes for the interactional dimension: (6) perceptual interactions, and (7) psychological interactions. The results of thematic analysis are presented in Tables1–3.
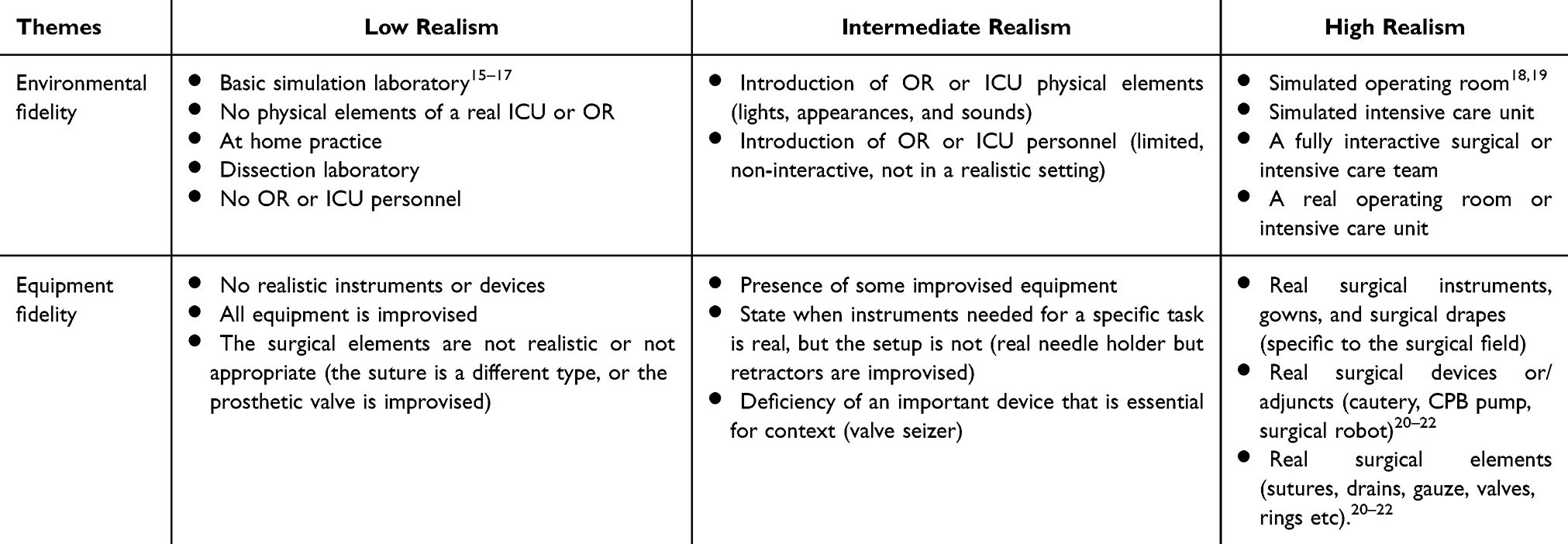 |
Table 1 Physical Dimension Themes and Subthemes |
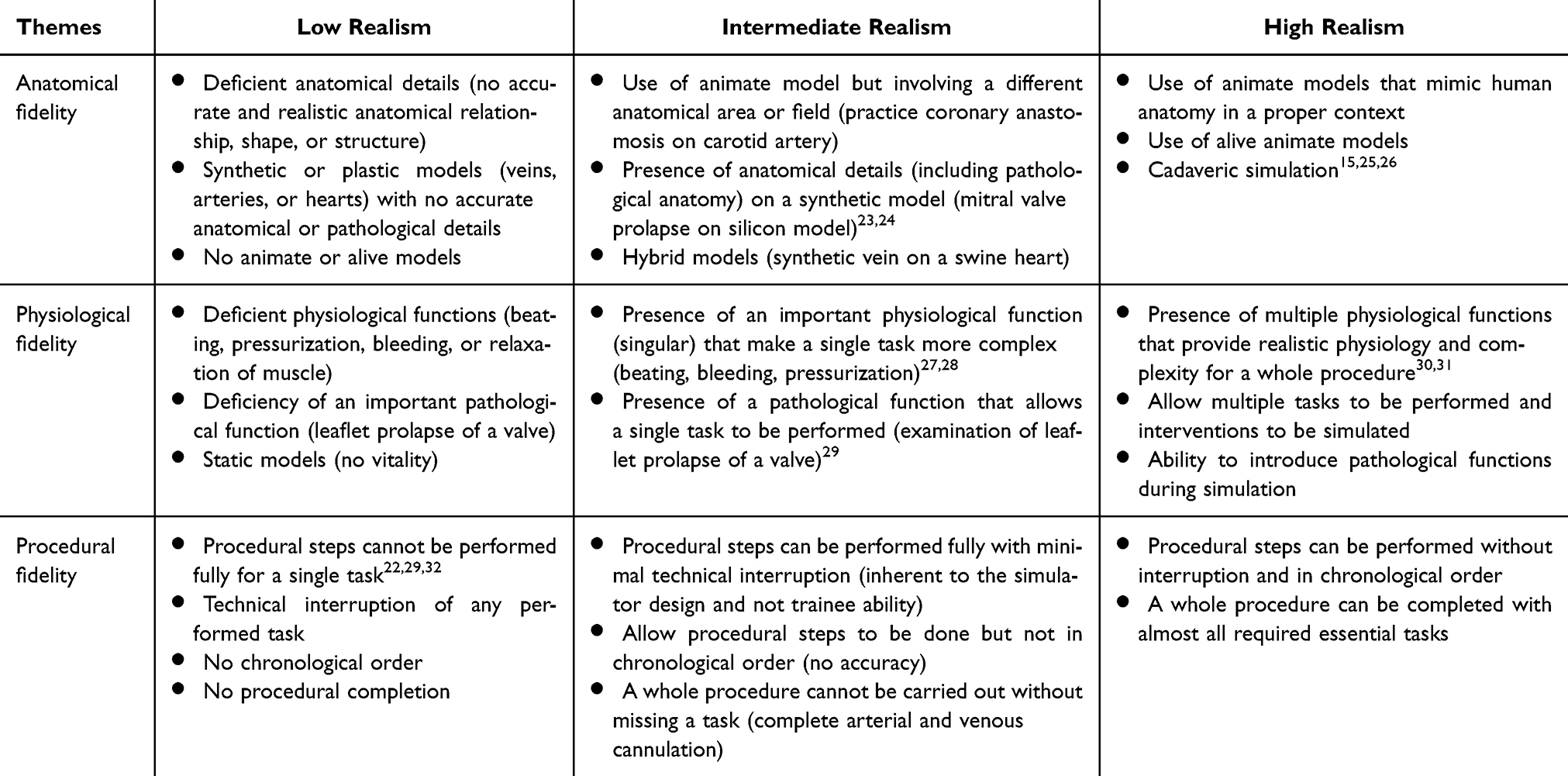 |
Table 2 Surgical Field Dimension Themes and Subthemes |
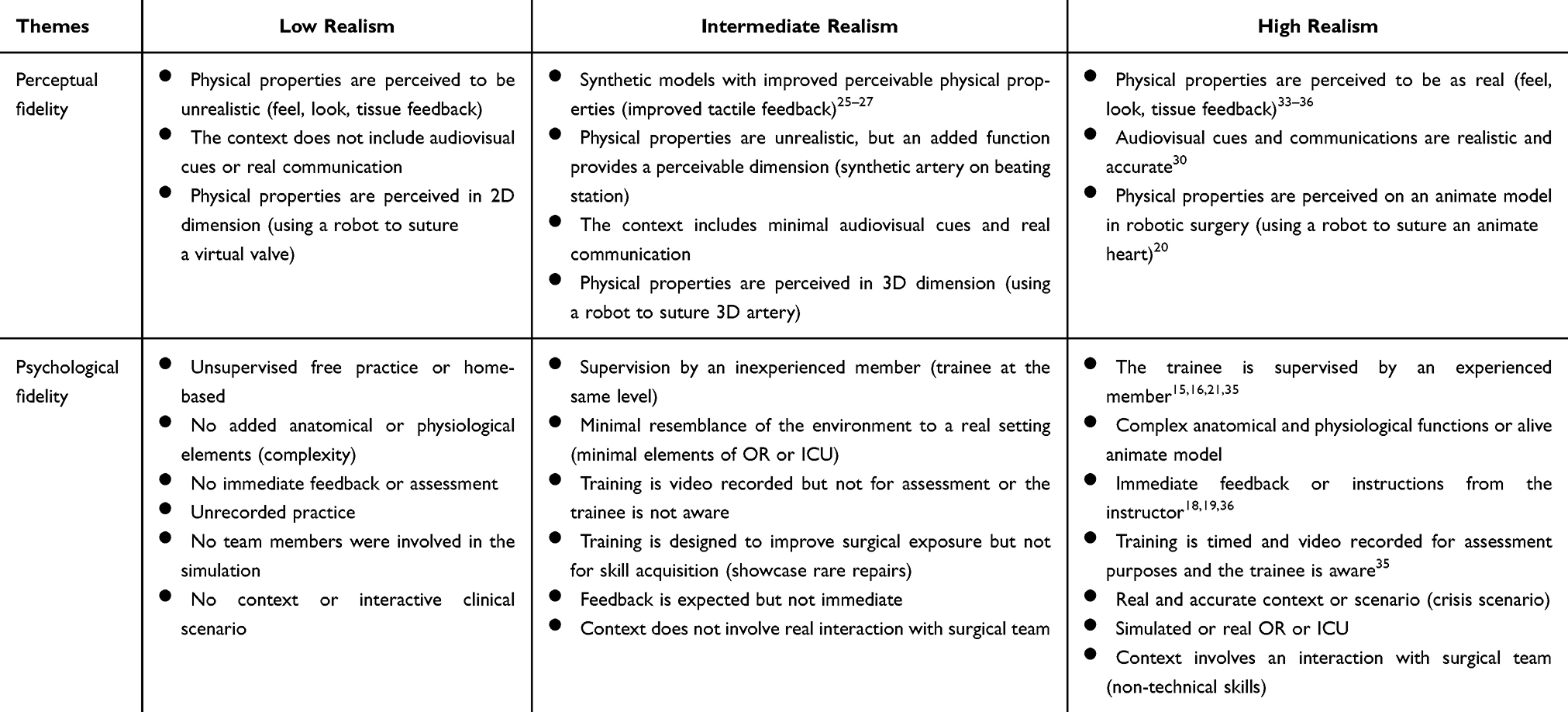 |
Table 3 Interactional Dimension Themes and Subthemes |
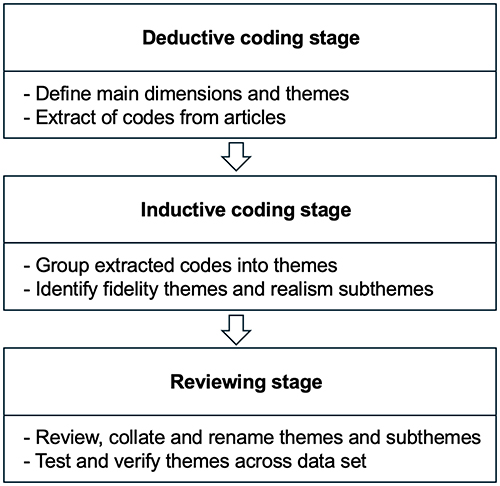 |
Figure 2 Hybrid thematic analysis stages. |
Themes
Physical Themes
In the Simulation environment, almost all studies (n = 24) described the environment surrounding the simulated activities in a variety of ways. The majority reported a detailed description of the physical space in which the activity was performed, as well as environmental elements such as sounds, light, functions, and appearances. In fact, realism is closely related to those elements; for instance, low realism in a physical space would equal practicing at home or a basic simulation laboratory without operating room physical cues.15–17 Advancing levels of realism would provide a greater resemblance to the real surgical zone around the trainee, such as a simulated operating room or an actual operating room.18,19 Simulation equipment, The majority of the studies (n = 23) mentioned the equipment used in their simulation exercises. Multiple studies emphasized the use of real surgical instruments to train skills, some studies described the use of specific devices that are crucial to the simulation context (eg use of a surgical robot, cardiopulmonary bypass pump, and prosthetic heart valves).20–22 The level of realism was primarily determined by the degree of improvised items, the presence of devices or elements essential to context and most importantly the use of real surgical-grade instruments. Surgical equipment contributes significantly to the authenticity of the experience as it provides a unique surgical simulation theme.
Surgical Field Themes
Surgical anatomy, All the studies addressed the anatomical features of the surgical field. Meanings were retrieved from descriptive simulation designs or from attached photos and videos. Some articles referenced the use of simulators based on previously published technical descriptions. These publications were retrieved for verification, if needed. The levels of realism of the simulated field ranged from a lack of accurate anatomical details to absolute realism by using human cadavers.15,25,26 Furthermore, the use of three-dimensional printing to create synthetic models with accurate pathological anatomy significantly increased the level of realism.23,24 Surgical physiology and pathology, each study (n = 26) was successfully mapped for physiological and pathological surgical field functions by extracting multiple codes from text, photos, and videos. The most coded physiological functions simulated a beating heart to increase realism and induce pathological reactions during surgical scenarios to add complexity.27,28,37 Some simulations were created with only one needed physiological or pathological function, resulting in a higher level of realism.29 Other simulators used complex technology to simulate multiple physiological functions, providing a realistic clinical scenario.30,31 In Surgical procedural steps, all studies (n = 26) included a description of the procedural tasks that were supposed to be simulated by trainees. Some studies intended to teach non-technical cardiac surgical scenarios but did not address surgical skills.22,29,32,38 As a result, trainees were evaluated based on their ability to perform complete clinical assessments and provide a management plan. For these simulations, the ability to perform complete assessments and management steps was considered the degree of realism. For simulated technical procedures, the ability to perform all tasks with minimal interruption was deemed high in realism. Incompleteness or frequent interruptions in the performance of these tasks confer a lower level of realism. Additionally, the following chronological order was considered higher realism and vice versa.
Interactional Themes
The perceptual interactions, all studies (n = 26) characterized the perceptual relationship of the trainee with the simulator to some extent. The majority of them have shown that employing surgical models with great anatomical details improves perceptual reactions (eg, animate models or cadaveric tissues), as they provide a realistic appearance and tissue feedback and react to surgical tasks accurately.25–27,33–36 Alternatively, some studies have created highly interactive surgical scenarios with realistic audiovisual cues that were perceived as authentic by trainees as real.30 On the other hand, virtual reality training on robots was not regarded as realistic. However, the use of animate models with robots markedly boosted realism perceptually.20 The psychological interaction, most of the studies (n = 25) were mapped for triggers that result in greater psychological or affective responses as a consequence of interaction with simulation experiences. For example, home practice and surgeon-supervised simulation sessions have different experiences for each trainee. The combination of video recording and awareness of assessment has placed trainees in a more psychologically demanding situation.15,16,21,35 Immediate and repetitive feedback from surgeons simulated a real trainee-instructor interaction throughout the procedure.18,19,36 Multifunctional complex simulators involving team interaction elicited far more realistic affective responses.
Discussion
This literature review and thematic analysis used multidimensional fidelity to establish seven major themes of cardiac surgical simulation fidelity. The detected themes were developed based on expansive dimensions from the studies of Kneebone et al and Rystedt et al. Given that our research question aimed to identify fidelity themes and subthemes, this review successfully met its objectives. As most of the included studies have been published over the past decade, this thematic framework was formulated using recent data from a growing field of surgical simulation. As a result, the dimensional fidelity themes established may guide future simulation and instructional design in cardiac surgical simulation-based training and facilitate the uniformity of fidelity definitions.
The analysis generated two themes by expanding the physical dimension, which encompassed all major physical triggers outside the surgical field for trainees. Consequently, we compiled many codes under an environmental fidelity theme that included the location of the simulation exercise and its elements (ie, home or simulation laboratory without the physical elements of the actual operating room or personnel in a real simulated operating room with dedicated staff). This theme was closely related to the psychological theme, where interaction with the simulation in a low environmental fidelity setting (eg, home or residents’ lounge) resulted in reduced psychological responses and vice versa. In addition, the analysis revealed that environmental fidelity often correlated with training objective, basic skills training required minimal realism while team training was performed in maximum realism. The other is the equipment fidelity theme, which maps physical tools and instruments (ie, improvised items, surgical tools, and elements to real ones). It is often associated with perceptual themes in which improvised items do not provide more perceptual realism. This also holds true for anatomical fidelity, where realistic equipment resulted in the simulation being perceived as authentic (eg, using cautery and retractors on cadaveric tissue). All of these intertwined relationships between themes necessitated that while designing a certain simulation exercise, one may consider how these themes would interact with one another and whether it is necessary. For example, using real surgical instruments in low realism environments or anatomical models was proved cost-effective.16
Three themes specific to the surgical site were identified under the surgical field dimension, which was developed from Kneebone’s innermost circle of focus. The anatomical theme corresponded to the accuracy of anatomical details and relationships. It was evident that the level of realism increased when synthetic materials were replaced with hybrid and animate models. Rich anatomical features are sometimes necessary to replicate a surgical field but might be overlooked when the attention is on a strictly technical task requiring repetitive movements and deliberate practice (eg, practicing complex suturing techniques and instrument manipulation). This theme is relevant when high anatomical realism presents a distraction rather than a requirement for novice learners training on basic surgical skill (eg, repetitive suturing). The second theme is physiological fidelity, which was mapped from models that replicated a normal or abnormal function, and was critical when educators incorporated bleeding and beating functions or used live animals to simulate a real surgical field. This translated into better authenticity and engagement, as well as produced complexity (eg, practicing cardiopulmonary bypass on beating the animate heart to observe the physiological responses). It is important to highlight increased cost with higher physiological realism especially when requiring higher realism in other themes (eg, environmental, anatomical, equipment). Finally, the procedural fidelity theme was dependent on the completion, interruption, and chronological order for any given task or procedure. This provided an important simulation feature that might have a detrimental effect on learning outcomes if the trained tasks are not performed completely or in order. As observed, procedural fidelity depends on the desired objectives (ie, subthemes related to levels of realism were consistent when it was a simple singular task or a procedure with many tasks). Notably, non-procedural tasks such as situational awareness could not be accounted for because this theme is exclusive to performing surgical acts. In addition, novice learners need low procedural realism as they acquire deconstructed skills and then advance into higher levels when training on full procedures. Finally, the three themes interacted with the interactional dimension when their realism was enhanced (eg, the addition of physiological functions, such as bleeding, would boost psychological fidelity).
The interactional dimension, as proposed by Rystedt et al, generated two themes: a perceptual fidelity theme, in which the simulation is perceived by the trainee to be realistic or unrealistic. It was evident that the accurate features of animate models provided better perceptual fidelity and were regarded as better than synthetic non-animate models. In addition, audiovisual cues, such as alarms, conversations, and gray noise, enhance realism. This theme is relevant to surgical simulation because it enhances the authenticity of the surgical sense and physical interaction of the trainee with the model (eg, inserting a cannula in a pressurized animal aorta has higher perceptual fidelity than a plastic tube). Finally, the psychological fidelity theme featured stimuli that might heighten the trainees’ affective responses. Certainly, low anatomical, physiological, and environmental fidelity is associated with low complexity and psychological interaction, and vice versa. Additional subthemes included supervision by a staff surgeon and instantaneous feedback as a genuine stimulus for trainees in real practice. Likewise, simulating a complicated urgent situation involving interactions with multiple teams elicits a real psychological response. This theme provided elements that could be manipulated during simulation to raise or reduce psychological fidelity for trainees, thereby aiding in the design of exercises suited to the trainee level and task required (eg, less stressful exercises for novices to enable skill acquisition, followed by increasing the psychological load as they advance). Altogether, the seven surgical fidelity themes are not mutually exclusive because their presence depends on their level of realism for a given design rather than on the present or absent dichotomy.39 The complex interaction between themes revealed that high realism in one dimensions did not necessarily require higher realism in others. For instance, the coronary anastomosis trainer benefited from high procedural and perceptual fidelity but required minimal environmental realism.16 Conversely, team training on emergency scenarios demanded high environmental and psychological fidelity but tolerated lower anatomical and procedural domains.
Certainly, fidelity is not a well-established concept, and the published surgical education literature does not define it consistently.10 In fact, cardiothoracic surgery educators have urged for robust educational research since there is a paucity of high-quality research.40 By mapping meanings of surgical fidelity beyond prior definitions and further extending previous simulation educators’ work, this analysis can provide educators with universal definitions and standard operational frameworks.5,13,14,41 This effort has the potential to bring consistency to the field with the indirect goal of improving simulation research through the use of uniform terminology and themes. Depending on their top-priority surgical fidelity themes and level of realism, educators may compare various simulations and their outcomes better. Additionally, the cost-benefit of healthcare simulation is understandably a limiting issue, with no clear evidence of a return on investment.42 In fact, there is no strong evidence to back up the use of expensive, high-fidelity simulation for strong and tangible outcomes.11 Alternatively, utilizing the framework of dimensional fidelity, augmentation of low-realism and affordable simulation may be a valid solution. As an illustration, adding pertinent perceptual fidelity elements (eg, adding a synthetic tissue with actual feedback to a simple coronary anastomosis trainer or using progressive anatomical fidelity to teach skills on a synthetic valve model before fine-tuning it on an animate heart) may enhance authenticity.
It is impossible to overlook the fundamental change in surgical education toward competency-based instruction and assessment.2 In real practice, trainees must develop certain competencies that they would not have encountered throughout their training and may need simulation to fill in gaps. To achieve this, the simulation instructional design and desirable outcomes or competencies must be aligned. We propose a guide for dimensional fidelity to flexibly help modify various simulation designs to target specific competencies more effectively, Table 4. For example, a competency that requires pure technical skills can be exercised using a simulation design that prioritizes equipment and procedural fidelity, while maintaining cost efficiency. This implies that rather than seeking simulation that resembles the aviation industry in healthcare, surgical instructors should strive for fit-for-purpose design.43 It is enticing to aim for high technological properties in simulation design in surgical training, although this may provide advanced technological functions, this may not translate into better training outcome.8 This is due to the fact that surgical simulation is unique to its discipline with many unpredictable clinical scenarios and different technical approaches. Compared to aviation, surgical simulation design must be adaptable to train various surgical skills and procedures within limited time and resources. However, this simplistic approach to fidelity should not persuade educators to depend solely on it to enhance simulation. In fact, the fidelity is only one facet of the overall simulation mosaic. A recent systematic review identified the features that promote fidelity and authenticity in simulation-based education. They included featuring real-life content, feedback, performance expectations, logical scenarios, cueing and other elements.44 This model while developed for cardiac surgery, non-cardiac surgical disciplines can apply the dimensional fidelity framework and modify its themes according to their domains, while maintaining the principle of selective fidelity. Finally, the findings of this research, which support calls not to abandon fidelity as a simulation principle, further broaden understanding of dimensional fidelity from previous descriptions. They also supported skill training via a cost-efficient design by offering an operational fidelity framework in the era of competency-based cardiac surgical education. While acknowledging uncertainty of surgical simulation costs and return of investment, this framework could democratize simulation training by reducing cost barriers while maintaining simulation quality and authenticity.
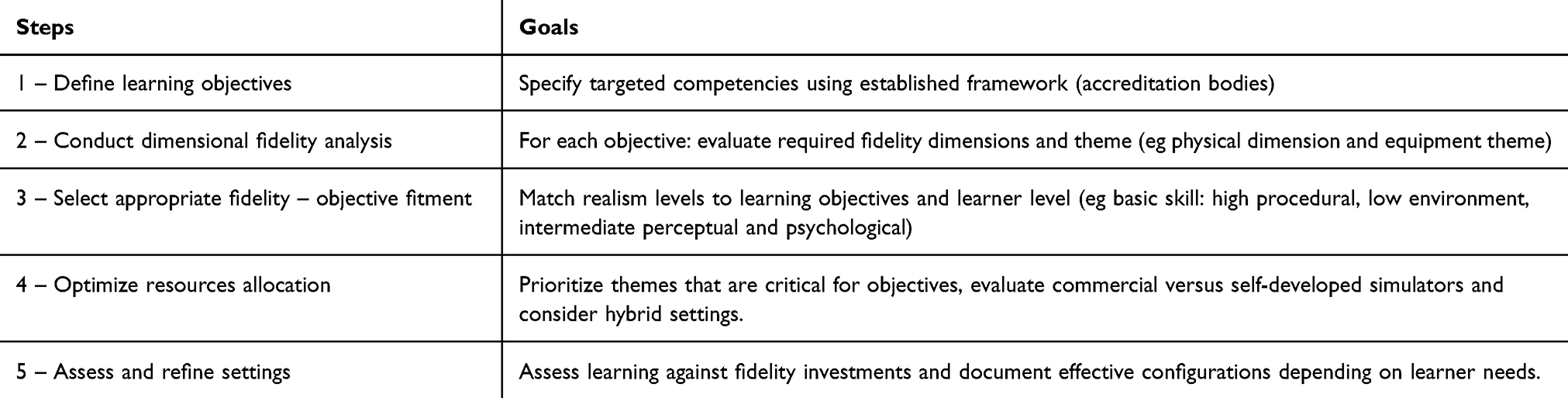 |
Table 4 Dimensional Fidelity Framework Implementation Guide for Educators |
Limitations
This literature review utilized deductive and inductive thematic analysis, which provides a flexible and reliable methodology to extract meanings from a large body of data, and highlights the similarities and subtleties of fidelity. This strategy increased the overall mapping of diverse literature and generated new findings, but not without limitations. First, quality appraisal was not performed because the included articles had high heterogeneity in methodology and varying reporting of the simulation design. Since our aim was limited to mapping the existing literature for fidelity themes, we decided not to exclude any studies after the application of inclusion and exclusion criteria, which helped capture broader meanings. Finally, theme extraction was dependent on the quality of reporting of the simulation design, conduct, and results, which varied across the articles.
Conclusion
A multidimensional framework was used to thematically map fidelity in the cardiac surgery simulation. The analysis generated seven fidelity dimensional themes and various subthemes that reflected their level of realism. This novel dimensional fidelity concept challenges prevailing assumptions about fidelity, demonstrating that selective enhancement of specific fidelity dimensions may achieve educational goals more efficiently than pursuing uniform higher uniform fidelity. This framework can be utilized in curriculum design by defining learning objectives, selecting dimensional themes and levels, matching them appropriately and allocating resources as needed. Barriers to implementation include faculty training, and institutional support. Future research should validate the framework and explore optimal fidelity dimensions configurations for specific educational competencies.
Abbreviations
MEDLINE, Medical Literature Analysis and Retrieval System Online; EMBASE, Excerpta Medica database; PICo, Population, Interest, Context; OPCAB, Off-pump coronary artery bypass; OR, Operating room; ICU, Intensive care unit.
Acknowledgment
The authors acknowledge that this manuscript is based on research initially conducted for the master’s thesis of Mohammed A. Alharbi at McGill University and portions of this paper are drawn from it.45
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. Trehan K, Kemp CD, Yang SC. Simulation in cardiothoracic surgical training: where do we stand? J Thorac Cardiovasc Surg. 2014;147(1):18–24e2. doi:10.1016/j.jtcvs.2013.09.007
2. Canada R. Competence by Design. Available from: https://www.royalcollege.ca/rcsite/cbd/competence-by-design-cbd-e.
3. Hossien A. Low-fidelity simulation of mitral valve surgery: simple and effective trainer. J Surg Educ. 2015;72(5):904–909. doi:10.1016/j.jsurg.2015.04.010
4. Verberkmoes NJ, Verberkmoes-Broeders EM. A novel low-fidelity simulator for both mitral valve and tricuspid valve surgery: the surgical skills trainer for classic open and minimally invasive techniques. Interact Cardiovasc Thoracic Surg. 2013;16(2):97–101. doi:10.1093/icvts/ivs451
5. Maran NJ, Glavin RJ. Low- to high-fidelity simulation - a continuum of medical education? Med Educ. 2003;37(1):22–28. doi:10.1046/j.1365-2923.37.s1.9.x
6. Massoth C, Roder H, Ohlenburg H, et al. High-fidelity is not superior to low-fidelity simulation but leads to overconfidence in medical students. BMC Med Educ. 2019;19(1):29. doi:10.1186/s12909-019-1464-7
7. Finan E, Bismilla Z, Whyte HE, Leblanc V, McNamara PJ. High-fidelity simulator technology may not be superior to traditional low-fidelity equipment for neonatal resuscitation training. J Perinatol. 2012;32(4):287–292. doi:10.1038/jp.2011.96
8. Norman G, Dore K, Grierson L. The minimal relationship between simulation fidelity and transfer of learning. Med Educ. 2012;46(7):636–647. doi:10.1111/j.1365-2923.2012.04243.x
9. Cook DA, Hatala R, Brydges R, et al. Technology-enhanced simulation for health professions education: a systematic review and meta-analysis. JAMA. 2011;306(9):978–988. doi:10.1001/jama.2011.1234
10. Hamstra SJ, Brydges R, Hatala R, Zendejas B, Cook DA. Reconsidering fidelity in simulation-based training. Acad Med. 2014;89(3):387–392. doi:10.1097/ACM.0000000000000130
11. Beaubien JM. The use of simulation for training teamwork skills in health care: how low can you go? Qual Saf Health Care. 2004;13(Suppl suppl_1):i51–6. doi:10.1136/qshc.2004.009845
12. Matsumoto ED, Hamstra SJ, Radomski SB, Cusimano MD. The effect of bench model fidelity on endourological skills: a randomized controlled study. J Urol. 2002;167(3):1243–1247.
13. Kneebone R. Simulation, safety and surgery. Qual Saf Health Care. 2010;19(3):i47–52. doi:10.1136/qshc.2010.042424
14. Rystedt H, Sjöblom B. Realism, authenticity, and learning in healthcare simulations: rules of relevance and irrelevance as interactive achievements. Instructional Sci. 2012;40(5):785–798.
15. Price J, Naik V, Boodhwani M, Brandys T, Hendry P, Lam BK. A randomized evaluation of simulation training on performance of vascular anastomosis on a high-fidelity in vivo model: the role of deliberate practice. J Thoracic Cardiovasc Surg. 2011;142(3):496–503. doi:10.1016/j.jtcvs.2011.05.015
16. Enter DH, Lee R, Fann JI, et al. “Top Gun” competition: motivation and practice narrows the technical skill gap among new cardiothoracic surgery residents. Ann Thorac Surg. 2015;99(3):870–875. doi:10.1016/j.athoracsur.2014.09.051
17. Helder MR, Rowse PG, Ruparel RK, et al. Basic cardiac surgery skills on sale for $22.50: an aortic anastomosis simulation curriculum. Ann Thorac Surg. 2016;101(1):316–322. doi:10.1016/j.athoracsur.2015.08.005
18. Spooner AJ, Faulkner CM, Novick RJ, Kent WDT. Optimizing Surgical Skills in Cardiac Surgery residents with cardiac transplant in the high-fidelity porcine model. Innovations. 2019;14(1):37–42. doi:10.1177/1556984519828016
19. Zhang LF, Feng HB, Yu ZG, Jing S, Wan F. Surgical training improves performance in minimally invasive left ventricular assist device implantation without cardiopulmonary bypass. J Surg Educ. 2018;75(1):195–199. doi:10.1016/j.jsurg.2017.06.029
20. Valdis M, Chu MWA, Schlachta C, Kiaii B. Evaluation of robotic cardiac surgery simulation training: a randomized controlled trial. J Thoracic Cardiovasc Surg. 2016;151(6):1498–1505. doi:10.1016/j.jtcvs.2016.02.016
21. Greenhouse DGMD, Grossi EAMD, Dellis SBA, et al. Assessment of a mitral valve replacement skills trainer: a simplified, low-cost approach. J Thoracic Cardiovasc Surg. 2013;145(1):54–59. doi:10.1016/j.jtcvs.2012.09.074
22. Fouilloux V, Doguet F, Kotsakis A, Dubrowski A, Berdah S. A model of cardiopulmonary bypass staged training integrating technical and non-technical skills dedicated to cardiac trainees. Perfusion. 2015;30(2):132–139. doi:10.1177/0267659114534287
23. Hermsen JLMD, Yang RMD, Burke TMP, et al. Development of a 3-D printing-based cardiac surgical simulation curriculum to teach septal myectomy. J Thoracic Cardiovasc Surg. 2018;156(3):1139–1148. doi:10.1016/j.jtcvs.2017.09.136
24. Sardari Nia P, Heuts S, Daemen JHT, Olsthoorn JR, Chitwood WR, Maessen JG. The EACTS simulation-based training course for endoscopic mitral valve repair: an air-pilot training concept in action. Interact CardioVascul Thorac Surg. 2020;30(5):691–698. doi:10.1093/icvts/ivz323
25. Baker CJ, Sinha R, Sullivan ME. Development of a cardiac surgery simulation curriculum: from needs assessment results to practical implementation. J Thorac Cardiovasc Surg. 2012;144(1):7–16. doi:10.1016/j.jtcvs.2012.03.026
26. Joyce DLMD, Dhillon TSBS, Caffarelli ADMD, et al. Simulation and skills training in mitral valve surgery. J Thoracic Cardiovasc Surg. 2011;141(1):107–112. doi:10.1016/j.jtcvs.2010.08.059
27. Hicks GL Jr, Gangemi J, Angona RE Jr, Ramphal PS, Feins RH, Fann JI. Cardiopulmonary bypass simulation at the boot camp. J Thoracic Cardiovasc Surg. 2011;141(1):284–292. doi:10.1016/j.jtcvs.2010.03.019
28. Ito J, Shimamoto T, Sakaguchi G, Komiya T. Impact of novel off-pump coronary artery bypass simulator on the surgical training. Gen Thoracic Cardiovasc Surg. 2013;61(5):270–273. doi:10.1007/s11748-013-0211-y
29. Cristancho S, Moussa F, Dubrowski A. Simulation-augmented training program for off-pump coronary artery bypass surgery: developing and validating performance assessments. Surgery. 2012;151(6):785–795. doi:10.1016/j.surg.2012.03.015
30. Burkhart HMMD, Riley JBCCP, Hendrickson SEMA, et al. The successful application of simulation-based training in thoracic surgery residency. J Thoracic Cardiovasc Surg. 2010;139(3):707–712. doi:10.1016/j.jtcvs.2009.10.029
31. Joyce DL, Lahr BD, Maltais S, et al. Integration of simulation components enhances team training in cardiac surgery. J Thoracic Cardiovasc Surg. 2018;155(6):2518–2524. doi:10.1016/j.jtcvs.2018.01.076
32. Burkhart HM, Riley JB, Lynch JJ, et al. Simulation-based postcardiotomy extracorporeal membrane oxygenation crisis training for thoracic surgery residents. Ann Thorac Surg. 2013;95(3):901–906. doi:10.1016/j.athoracsur.2012.12.015
33. Fann JIMD, Calhoon JHMD, Carpenter AJMDP, et al. Simulation in coronary artery anastomosis early in cardiothoracic surgical residency training: the boot camp experience. J Thoracic Cardiovasc Surg. 2010;139(5):1275–1281. doi:10.1016/j.jtcvs.2009.08.045
34. Tavlasoglu M, Durukan AB, Arslan Z, Kurkluoglu M, Amrahov A, Jahollari A. Evaluation of skill-acquisition process in mitral valve repair techniques: a simulation-based study. J Surg Edu. 2013;70(3):318–325. doi:10.1016/j.jsurg.2013.01.009
35. Tavlasoglu M, Durukan AB, Gurbuz HA, Jahollari A, Guler A. Skill acquisition process in vascular anastomosis procedures: a simulation-based study. Eur J Cardiothorac Surg. 2015;47(5):812–818. doi:10.1093/ejcts/ezu288
36. Liu XMD, Yang YMD, Meng QMD, et al. A secure and high-fidelity live animal model for off-pump coronary bypass surgery training. J Surg Edu. 2016;73(4):583–588. doi:10.1016/j.jsurg.2016.02.004
37. Fann JI, Caffarelli AD, Georgette G, et al. Improvement in coronary anastomosis with cardiac surgery simulation. J Thoracic Cardiovasc Surg. 2008;136(6):1486–1491. doi:10.1016/j.jtcvs.2008.08.016
38. Smelt JLC, Phillips S, Hamilton C, et al. Simulator teaching of cardiopulmonary bypass complications: a prospective, randomized study. J Surg Edu. 2016;73(6):1026–1031. doi:10.1016/j.jsurg.2016.05.009
39. Hontvedt M, Øvergård KI. Simulations at work —a framework for configuring simulation fidelity with training objectives. Computer Support Cooperat Work. 2020;29(1):85–113. doi:10.1007/s10606-019-09367-8
40. Antonoff MB, Nguyen S, Nguyen TC, Odell D. Conducting high-quality research in cardiothoracic surgical education: recommendations from the Thoracic Education Cooperative Group. J Thoracic Cardiovasc Surg. 2019;157(2):820–827. doi:10.1016/j.jtcvs.2018.09.117
41. Bland AJ, Topping A, Tobbell J. Time to unravel the conceptual confusion of authenticity and fidelity and their contribution to learning within simulation-based nurse education. A discussion paper. Nurse Educ Today. 2014;34(7):1112–1118. doi:10.1016/j.nedt.2014.03.009
42. Stephen M, Terry H. Issues of cost-benefit and cost-effectiveness for simulation in health professions education. Advanc Simulation. 2016;1(1):13. doi:10.1186/s41077-016-0020-3
43. Gogalniceanu PMMPF, Calder FMF, Callaghan CMPF, Sevdalis NP, Mamode NMMDF. Surgeons are not pilots: is the aviation safety paradigm relevant to modern surgical practice? J Surg Edu. 2021;78(5):1393–1399. doi:10.1016/j.jsurg.2021.01.016
44. Lavoie P, Deschênes M-F, Nolin R, et al. Beyond technology: a scoping review of features that promote fidelity and authenticity in simulation-based health professional education. Clin Simul Nurs. 2020;42:22–41. doi:10.1016/j.ecns.2020.02.001
45. Alharbi MA. A Model for Competency-based Simulation Training in Cardiac Surgery Utilizing Dimensional Fidelity. Master’s thesis. McGill University; 2023.
46. Allan CK, Pigula F, Bacha EA, et al. An extracorporeal membrane oxygenation cannulation curriculum featuring a novel integrated skills trainer leads to improved performance among pediatric cardiac surgery trainees. Simul Healthcare. 2013;8(4):221–228. doi:10.1097/SIH.0b013e31828b4179
47. Mavroudis CD, Mavroudis C, Jacobs JP, DeCampli WM, Tweddell JS. Simulation and deliberate practice in a porcine model for congenital heart surgery training. Ann Thorac Surg. 2018;105(2):637–643. doi:10.1016/j.athoracsur.2017.10.011
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.