")
Back to Journals » OncoTargets and Therapy » Volume 17
A Novel Intergenic Region (chr2: 30,316,870)-ALK Fusion in a Patient with Lung Adenocarcinoma Responding to Crizotinib Combined with Pemetrexed Treatment: A Case Report
Authors Zhou D, Ying J, Hu S, Li J, Liu H
Received 13 October 2023
Accepted for publication 19 March 2024
Published 27 March 2024 Volume 2024:17 Pages 261—265
DOI https://doi.org/10.2147/OTT.S444624
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Yong Teng
Danfei Zhou, Jun Ying, Shanshan Hu, Jiangdong Li, Haijian Liu
Department of Respiratory and Critical Care Medicine, Ningbo No.2 Hospital, Ningbo, People’s Republic of China
Correspondence: Haijian Liu, Department of Respiratory and Critical Care Medicine, Ningbo No.2 Hospital, NO. 41, Xibei Street, Ningbo, 315000, People’s Republic of China, Email [email protected]
Background: Anaplastic lymphoma kinase (ALK) rearrangements have been reported as an important oncogenic driver in 5– 7% non-small cell lung cancer (NSCLC) patients. Reports about the intergenic region (IGR) as an ALK fusion partner are rare. In this study, we report a novel IGR (chr2: 30,316,870)-ALK fusion in an advanced lung adenocarcinoma patient that responded effectively to crizotinib combined with pemetrexed.
Case Presentation: A 68-year-old Chinese female was diagnosed with stage IV right lung adenocarcinoma (cT3N3M1c). The targeted next-generation sequencing (NGS) of 14 cancer-related genes identified an IGR (chr2: 30,316,870)-ALK fusion. Her lung lesions have been successfully converted from a partial response to a complete response after administrating crizotinib for 1 year combined with 6 cycles of chemotherapy with pemetrexed. So far, her progression-free-survival has reached 21 months.
Conclusion: In this case, we firstly report a novel IGR (chr2: 30,316,870)-ALK fusion by using targeted NGS, and highlight the efficacy of crizotinib combined with pemetrexed to reduce unbearable gastrointestinal adverse reactions. It provides valuable clinical guidance for the treatment of similar cases in the future.
Keywords: NSCLC, IGR-ALK, NGS, crizotinib, pemetrexed
Introduction
Non-small-cell lung cancer (NSCLC) accounts for approximately 80% of lung cancers and is associated with high mortality worldwide.1 Anaplastic lymphoma kinase (ALK) rearrangements, an oncogenic driver, have been identified in 5–7% NSCLC patients.2 Echinoderm microtubule-associated like 4 (EML4) is the first identified and the canonical partner of ALK gene.3 With the development of next‐generation sequencing (NGS) technology, an increasing number of novel ALK fusions have been discovered. However, reports of the intergenic region (IGR) as an ALK fusion partner are still rare. Several ALK tyrosine kinase inhibitors (ALK‐TKIs), including crizotinib, ceritinib, alectinib, brigatinib and lorlatinib, have been approved for treating ALK‐rearranged NSCLC patients, and their efficacy may be affected by the ALK variant status.4 The sensitivity of these IGR-ALK fusions to ALK targeted therapies is also not clear.5 In this study, we present the case of a patient with advanced lung adenocarcinoma patient harboring a rare IGR (chr2: 30,316,870)-ALK fusion, who showed enduring clinical response to crizotinib combined with pemetrexed, with a 21-month progression-free survival (PFS).
Case Presentation
In April 2019, a 68-year-old Chinese female with no smoking history was referred to the respiratory department of our hospital after a routine physical examination at a healthcare center. She complained that pulmonary lesions had been discovered, despite not experiencing any discomfort in the past. Her chest computed tomography (CT) scan revealed a 34 mm × 37 mm × 56 mm mass in the right upper lobe with metastases to mediastinal and right hilar lymph nodes (Figure 1A and B). Further cranial MRI confirmed there was no brain metastasis. The whole-body emission computed tomography (ECT) revealed lesions with increased radioactivity in patients’ right shoulder and left coxa. Hematoxylin and eosin (HE) staining of endobronchial ultrasound-guided needle aspiration specimen of the mass in the right upper lobe revealed a typical adenocarcinoma histology (Figure 2A and B). Based on the imaging examinations, histopathology and immunohistochemical profile, the patient was diagnosed with stage IV (cT3N3M1c) lung adenocarcinoma according to UICC 8th edition TNM staging (Figure 1A).
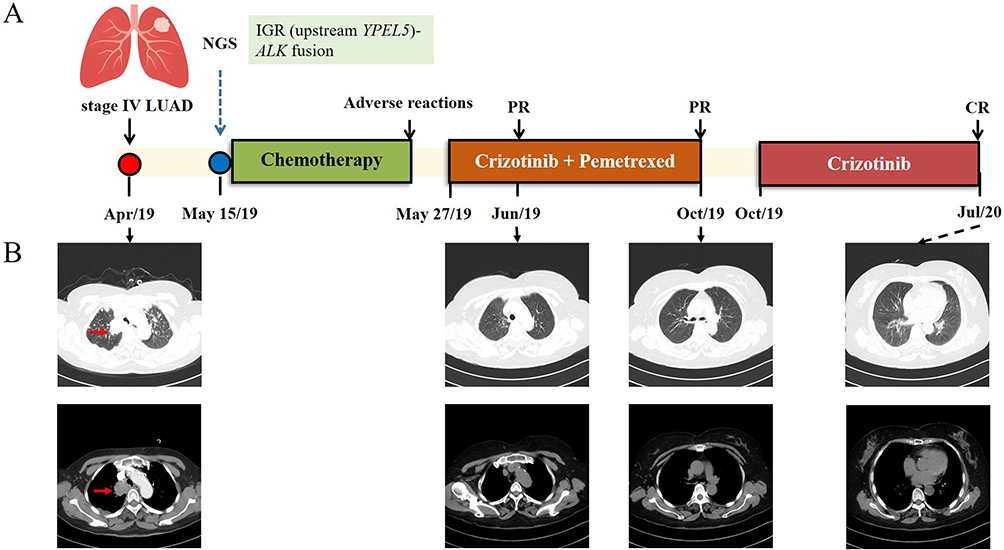 |
Figure 1 Schematic of patients’ treatment histories. (A) The treatment timeline of the patient. (B) Images of the chest CT are provided with lung tumors indicated with red arrows. Abbreviations: LUAD, lung adenocarcinoma; NGS, next-generation sequencing; IGR, intergenic region; PR, partial response; CR, complete response. |
 |
Figure 2 Pathology results. (A and B) Hematoxylin-eosin staining of endobronchial ultrasound-guided transbronchial needle aspiration biopsy specimen showed lung adenocarcinoma (10×). |
Subsequent targeted NGS of 14 cancer-related genes analysis (Nanjing Geneseeq Technology Inc., Nanjing, Jiangsu, China) of her aspiration biopsy identified an IGR (chr2: 30,316,870)-ALK fusion (Figure 3), but no other oncogenic alterations were found. The test results suggested that there was no known sensitive targeted medicine for this type of fusion. Therefore, the patient was treated with chemotherapy with nedaplatin (50 mg on d1-2) and pemetrexed (0.8 g on d1, q4w) on May 15, 2019. After the first cycle of the chemotherapy, the patient reported intolerable severe gastrointestinal adverse reactions with dizziness, amaurosis and weakness. Therefore, a combined treatment of crizotinib (250 mg bid) and maintenance chemotherapy with pemetrexed (0.8 g on d1, q4w) were administrated on May 27, 2019 and achieved a partial response (PR), as indicated by chest CT scan one month later which showed a remarkable shrinkage of the right upper lung lesion and multiple nodules in the two lungs (Figure 1B). Since the monthly chest CT scan in the following 6 months indicated a remarkable shrinkage of the right upper lung lesion and multiple nodules in the two lungs (Figure 1B), the patient was only given crizotinib as maintenance treatment on October 31, 2019. In July 2020, the patient’s chest CT scan showed that multiple nodules in both lungs were benign nodules (Figure 1B). The patient’s lung lesions were successfully converted from PR to complete response (CR) and remained progression-free-survival (PFS) on crizotinib for 21 months up to the most recent follow-up. During the targeted therapy, the patient experienced mild adverse reactions such as visual disturbance, dizziness, fatigue, and rash, which were well tolerated.
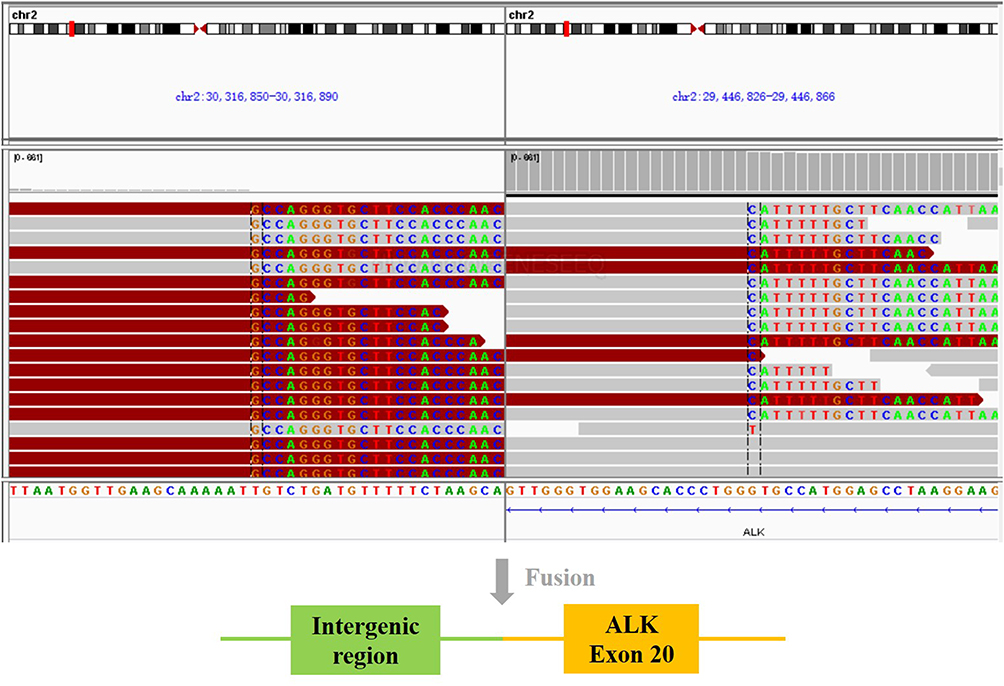 |
Figure 3 Sequencing reads of IGR and ALK were visualized by the Integrative Genomics Viewer (IGV). The schematic below shows the IGR (upstream YPEL5-) ALK fusion. |
Discussion
Approximately 5–7% of patients with NSCLC exhibit ALK gene rearrangements, which define a unique molecular subgroup within NSCLC.6 Multiple types of ALK fusions have been identified in patients with NSCLC, among which, different fusion partners may affect the response to ALK-TKIs.4 Therefore, it is necessary to determine the sensitivity of different ALK fusions to different ALK inhibitors for the purpose of making therapeutic decisions. To our knowledge, this is the first report of an IGR (chr2: 30,316,870)-ALK fusion as identified by targeted NGS and was successfully treated with crizotinib. The wide use of NGS testing has facilitated the detection of rare ALK fusions, including those with one IGR breakpoint.7 The shortcoming of traditional Fluorescence in situ hybridization (FISH) and IHC methods is that the specific variants of ALK fusion could not be determined.8 DNA-based NGS can also be performed on both tissue samples and liquid biopsies. While IGR-ALK at the genomic level may not always produce detectable fusion transcripts, many studies have indicated that unconventional ALK fusion at the DNA level can generate functional fusion due to mRNA splicing.9 In our case, the aspiration biopsy sample was not successfully tested with RNA-based NGS owing to sample poor quality. However, our case suggests that additional validation testing using targeted deep RNA-seq may be necessary to identify patients with intergenic-breakpoint fusion, who could benefit from ALK TKIs treatment. In addition, due to the unavailability of tissue samples, we were unable to conduct IHC and/or FISH tests, which is a limitation of our case.
In intergenic-ALK fusions, one breakpoint occurs at an intergenic position while the other is situated within the ALK gene. To date, over 20 intergenic ALK fusion genes have been reported, and only a few of these cases were sensitive to ALK-TKIs, including CENPA/DPYSL5, CENPA, CHRNA7, SLC8A1/LINC01913, and Linc00308/D21S2088E.5,7,9,10 In this case, we identified a novel IGR (chr2: 30,316,870)-ALK fusion. The breakpoints were located in the upstream intergenic region of Yippee-like 5 (YPEL5) and exon 20 of the ALK gene. YPEL5 is a component of the CTLH E3 ubiquitin-protein ligase complex that selectively accepts ubiquitin from UBE2H and mediates ubiquitination and subsequent proteasomal degradation of the transcription factor HBP1. This process is essential for the normal proliferation of cells. The kinase domain was preserved in ALK exon 20 and fused with the upstream intergenic region of YPEL5 to generate the IGR (upstream YPEL5)-ALK fusion. It was reported that a fusion between the intergenic region of YPEL5 (chr2: 30,193,816) and ALK gene in a female NSCLC case responded well to alectinib, a second-generation ALK TKI.11 Moreover, given that this fusion type retains a complete ALK kinase domain, it is theoretically possible that our patient may respond to ALK TKIs, such as crizotinib or alectinib. Indeed, our patient received a remarkable response following crizotinib therapy. This case report has expanded the spectrum of ALK fusions and offered valuable information for the precise administration of ALK inhibitor in the future. Pemetrexed, an antifolate, is commonly used in chemotherapy. Previous study has shown that the addition of pemetrexed had similar clinical response in ALK-positive and ALK-negative patients.12 Nevertheless, the PROFILE 1014 clinical trial has demonstrated that ALK-positive NSCLC patients exhibit an enhanced sensitivity to pemetrexed.13 In the light of NGS result and clinical guidelines, the patient was administered crizotinib combined with pemetrexed as a second-line treatment due to the severe adverse reactions of the first-line chemotherapy with nedaplatin and pemetrexed. Surprisingly, the second-line treatment yielded a good response so far with mild adverse reactions. This intergenic ALK fusion was sensitive for the combination of pemetrexed and crizotinib, which was feasible and may be an alternative for second generation ALK-TKI like alectinib.11 Further clinical studies are needed to verify our findings and clinical outcomes of crizotinib versus crizotinib combined with pemetrexed can be further studied.
Conclusion
Based on the literature retrieval, this study illustrated the first case of a lung adenocarcinoma patient carrying a novel IGR (chr2: 30,316,870)-ALK fusion and reported that the patient benefited from the treatment of crizotinib combined with pemetrexed. The functions of the novel ALK fusion in oncogenesis and drug resistance need to be further investigated to better inform treatment decisions and prognosis predictions. Our study provides the first clinical evidence of ALK‐TKI efficacy in such patients, and highlights the importance of targeted NGS to guide treatment decision-making.
Date Availability
All datasets generated for this study are included in the manuscript.
Ethics Approval and Consent for Publication
The studies involving human participants were reviewed and approved by The Ethics Committee of Ningbo No.2 Hospital. Written informed consent was obtained from the patient for publication of this report.
Acknowledgment
Thanks for the technical support provided by Nanjing Geneseeq Technology Inc.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Supported by Ningbo Clinical Research Center for Respiratory Diseases (Grant No. 2022L004); Supported by Ningbo Health Branding Subject Fund (Grant No. PPXK2018-05); Supported by Medical Scientific Research Foundation of Zhejiang Province, China (Grant No.2019KY593); Supported by Ningbo Natural Science Foundation, China (Grant No.202003N4277).
Disclosure
The authors declare that they have no conflict of interest.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. Ca a Cancer J Clinicians. 2021;71(3):209–249. doi:10.3322/caac.21660
2. Devarakonda S, Morgensztern D, Govindan R. Genomic alterations in lung adenocarcinoma. Lancet Oncol. 2015;16(7):e342–351. doi:10.1016/S1470-2045(15)00077-7
3. Soda M, Choi YL, Enomoto M, et al. Identification of the transforming EML4-ALK fusion gene in non-small-cell lung cancer. Nature. 2007;448(7153):561–566. doi:10.1038/nature05945
4. Yoshida T, Oya Y, Tanaka K, et al. Differential crizotinib response duration among ALK fusion variants in ALK-positive non-small-cell lung cancer. J Clin Oncol. 2016;34(28):3383–3389. doi:10.1200/JCO.2015.65.8732
5. Ou SI, Zhu VW, Nagasaka M. Catalog of 5’ Fusion Partners in ALK-positive NSCLC Circa 2020. JTO Clin Res Rep. 2020;1(1):100015. doi:10.1016/j.jtocrr.2020.100015
6. Barlesi F, Mazieres J, Merlio JP, et al. Routine molecular profiling of patients with advanced non-small-cell lung cancer: results of a 1-year nationwide programme of the French Cooperative Thoracic Intergroup (IFCT). Lancet. 2016;387(10026):1415–1426. doi:10.1016/S0140-6736(16)00004-0
7. Zhang J, Zou C, Zhou C, et al. A Novel Linc00308/D21S2088E intergenic region ALK fusion and its enduring clinical responses to crizotinib. J Thorac Oncol. 2020;15(6):1073–1077. doi:10.1016/j.jtho.2020.03.009
8. Pekar-Zlotin M, Hirsch FR, Soussan-Gutman L, et al. Fluorescence in situ hybridization, immunohistochemistry, and next-generation sequencing for detection of EML4-ALK rearrangement in lung cancer. Oncologist. 2015;20(3):316–322. doi:10.1634/theoncologist.2014-0389
9. Li W, Liu Y, Li W, Chen L, Ying J. Intergenic breakpoints identified by DNA sequencing confound targetable kinase fusion detection in NSCLC. J Thorac Oncol. 2020;15(7):1223–1231. doi:10.1016/j.jtho.2020.02.023
10. Wang C, Chen S, He Q, Sun T, Xu P. A novel SLC8A1/LINC01913 intergenic region-ALK fusion identified by NGS and validated by IHC and FISH in a stage IIB lung adenocarcinoma patient who remains relapse-free during the treatment of crizotinib: a case report. Invest New Drugs. 2022;40(6):1350–1353. doi:10.1007/s10637-022-01262-2
11. Wang T, Du G, Niu M, Liu R. A novel intergenic region (chr2: 30,193,816)-ALK fusion shows sensitivity to Alectinib in lung adenocarcinoma. BMC Pulm Med. 2023;23(1):60. doi:10.1186/s12890-023-02351-5
12. Shaw AT, Varghese AM, Solomon BJ, et al. Pemetrexed-based chemotherapy in patients with advanced, ALK-positive non-small cell lung cancer. Ann Oncol. 2013;24(1):59–66. doi:10.1093/annonc/mds242
13. Noonan SA, Camidge DR. PROFILE 1014: lessons for the new era of lung cancer clinical research. Transl Lung Cancer Res. 2015;4(5):642–648. doi:10.3978/j.issn.2218-6751.2015.05.02
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.