Back to Journals » Neuropsychiatric Disease and Treatment » Volume 10
A novel five-category multimodal T1-weighted and T2-weighted magnetic resonance imaging-based stratification system for the selection of spinal arachnoid cyst treatment: a 15-year experience of 81 cases
Received 5 August 2013
Accepted for publication 13 September 2013
Published 19 March 2014 Volume 2014:10 Pages 499—506
DOI https://doi.org/10.2147/NDT.S52517
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Ji Qi, Jun Yang, Guihuai Wang
Department of Neurosurgery, Beijing Tiantan Hospital, Capital Medical University, Beijing, People's Republic of China
Background: Idiopathic spinal arachnoid cysts are rare cystic masses of the spinal canal generally classified as intra- or extradural, based on anatomical presentation. However, this system may not effectively indicate treatment.
Objective: To investigate the incidence, resection modality, and prognosis of spinal arachnoid cyst in a 15-year case series.
Patients and methods: A retrospective study was conducted in 81 spinal arachnoid cyst patients (male:female 34:47, mean age 36.5 years, age range 6–66 years) classified using a novel five-category T1-weighted and T2-weighted magnetic resonance imaging (MRI) classification system (intramedullary, subdural extramedullary, subdural/epidural, intraspinal epidural, or intraspinal/extraspinal). Conservative treatment failed in all patients. They underwent spinal surgery between January 1995 and December 2010 and were followed up for 69 (range 3–187) months. Performance outcomes were assessed using the Fugl-Meyer (FM) scale 90 days after operation. Recurrences and deaths were recorded.
Results: Subdural/epidural and intraspinal epidural cysts accounted for 66.7% (54 of 81) of patients, but exhibited relatively lower rates of postsurgical improvement using FM, with only 66.7% (36 of 54) of patients showing improvements. Excellent outcomes using the FM scale were reached in 100% (eight of eight) of intramedullary, intraspinal/extraspinal, and subdural extramedullary cyst patients, 86.7% (13 of 15) of subdural extramedullary cyst patients, and 66.7% (36 of 54) of epidural intraspinal cyst patients.
Conclusion: The proposed five-category multimodal MRI-based stratification system for spinal arachnoid cyst patients may more effectively allow clinicians to select the appropriate surgical intervention, and may help to predict outcomes.
Keywords: spinal arachnoid cyst, classification, intramedullary, extramedullary, subdural, epidural, spinal surgery
Introduction
Spinal arachnoid cysts are relatively rare, variable, nonspecific, and nonmalignant cystic masses that occur in the spinal canal, generally classified as either intra- or extradural, based on anatomical presentation.1 The incidence of spinal arachnoid cysts is low, with most cases being incidentally detected by magnetic resonance imaging (MRI) before or after manifestation of pain or neuropathy due to spinal compression.2,3 In many cases, the disease remains undetected for a long period of time in asymptomatic patients, and is only treated when symptoms emerge, such as radiculalgia, limb spasm, weakness, upper-limb pain, and defecation and urination dysfunction.4 Thus, the relatively little available information pertaining to spinal arachnoid cyst treatment is generally based on reviews of isolated case reports that are not widely representative of the majority of spinal arachnoid cyst patients.5,6 Unfortunately, for many patients, anatomical presentation at symptoms’ onset does not fully indicate the effects on the subarachnoid space,7 resulting in selection of suboptimal surgical intervention strategies that can lead to poor prognosis and failure to alleviate symptoms.
The etiology of spinal arachnoid cysts is complex, involving congenital, idiopathic, and acquired cases that are secondary to bleeding, inflammation, infections, or puncture-related traumas.8 Incidental asymptomatic cysts are usually treated with conservative methods. However, in cases of failure of conservative treatment, a surgery may be selected. To better select treatment strategies, several systems have been designed for classification of these patients based on anatomical characteristics of the lesions, including intra/extradural,1 subdural/epidural,9,10 and Nabors’ classification.11 Of these, the Nabors classification was developed in 1988 and remains the most widely used strategy for classifying spinal arachnoid cyst patients, defining type I as extradural meningeal cysts without neural tissue, type II as extradural meningeal cysts containing neural tissue, and type III as intradural spinal arachnoid cysts.12 However, each of these systems makes basic assumptions about the formation of spinal subdural cysts, failing to consider abnormalities due to defects, spinal protrusion, endorrhachis, and cysticercosis.10 Thus, many practitioners select the surgery based on a type that does not accurately consider all factors of the patient’s status, necessitating the development of more accurate, individualized, and comprehensive treatment-selection strategies for these patients who consider both anatomical and pathological classifications.
In order to evaluate a novel five-category system for classification of spinal arachnoid cyst patients, an extensive case series spanning a 15-year period was retrospectively examined. Outcomes of patients with spinal arachnoid cysts classified as intramedullary, subdural extramedullary, subdural/epidural, intraspinal epidural, or intraspinal/extraspinal, based on the anatomical location and abnormalities detected by MRI were examined. This strategy fills a critical need for an improved classification of spinal arachnoid cyst patients, potentially improving treatment selection and overall prognosis.
Patients and methods
Study design
A total of 81 spinal arachnoid cyst patients (male:female 34:47, mean age 32 years) undergoing surgery in Beijing Tiantan Hospital from January 1995 to December 2010 were retrospectively studied. The study protocol was approved by the Ethics Committee of Beijing Tiantan Hospital. Written informed consent was obtained from all patients or from guardians for patients less than 18 years old.
Patients
Inclusion criteria were: 1) diagnosis of idiopathic or congenital spinal arachnoid cyst based on MRI and clinical features, using the diagnostic criteria provided by Hughes et al1; 2) aged 6–70 years at the time of treatment; and 3) conservative-treatment failure, and patient still exhibiting a baseline preoperative Fugl-Meyer (FM) score of <50 after conservative treatment. Exclusion criteria were: 1) diagnosis of another disease requiring clinical intervention or impairing routine operative care, including spinal tuberculosis or tumor; 2) undergoing treatment for diabetes mellitus or other chronic diseases; or 3) had been diagnosed with arachnoid cysts secondary to trauma, including hemorrhage, inflammation, surgery, or lumbar puncture.
Preoperative examinations
All patients underwent routine MRI examinations. Spinal arachnoid cysts were identified based on apparent low-signal regions in T1-weighted images. Similarly, high signals were used to indicate cerebrospinal fluid without enhancement in T2-weighted images. All examinations were conducted in accordance with previously published guidelines.1
Classification using the five-category system
Both anatomical location and abnormalities observed by MRI were assessed for each patient. Surgical procedure of spinal arachnoid cysts was determined before the year 1995 in our department. Spinal arachnoid cysts were subdivided into five types: 1) intramedullary cysts/syrinxes, 2) subdural extramedullary, 3) subdural/epidural, 4) intraspinal epidural, or 5) intraspinal/extraspinal (Figure 1). If surgical observation was inconsistent with preoperative evaluation by MRI, the surgical procedure was modified according to intraoperative observations.
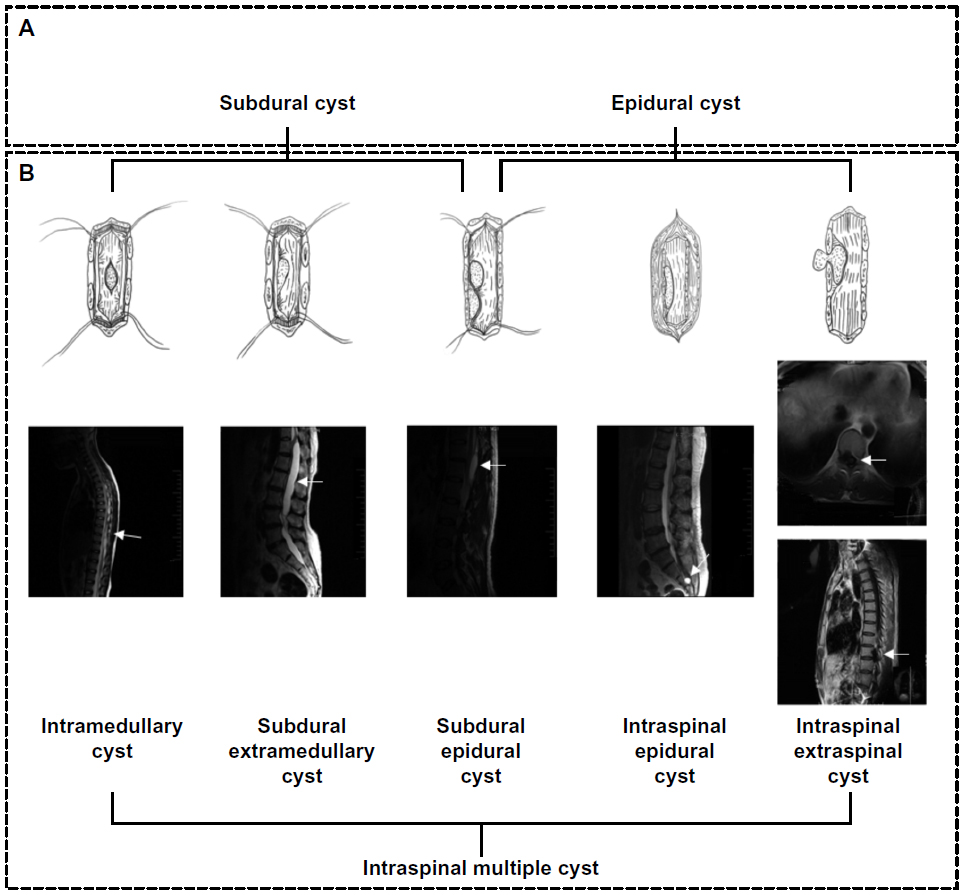 | Figure 1(A and B) Classification of spinal arachnoid cysts. (A) Two anatomical types of spinal arachnoid cysts; (B) novel five-type classification system determined by magnetic resonance imaging (MRI). |
Surgical procedures
Surgical treatment was selected based on spinal arachnoid cyst type and conducted by a team of two trained surgeons and two assistants. All surgeries were conducted at the same facility. The use of total or partial resection was recorded for each patient.
Intramedullary cyst treatment
For patients with this kind of cyst, experimental puncture was performed to identify the location of the cysts, then an incision along the posterior median sulcus was made to achieve cyst opening (the length of the incision varied according to the size of the cyst). For some patients with dense adhesion between the cyst wall and spinal cord, the separation of the cyst was not continued if it was very difficult to separate. On the contrary, the clinicians removed the parts that could be separated or sutured the pia mater to the cyst wall and ensured the connection of the cyst cavity and the subarachnoid space to prevent the recurrence of the cyst.
Subdural extramedullary cyst treatment
Subdural extramedullary spinal arachnoid cysts feature abnormal thickening and adhesion of the arachnoid caused by congenital aplasia and/or inflammatory responses. These abnormalities are commonly found at the ventral and ventrolateral spinal cord. Posterior shifting of the spinal cord is generally found in patients with cysts at the ventral and ventrolateral spinal cord, and thickening and adhesion of the arachnoid that could lead to dense adhesion between the spinal cord and the endorrhachis. Thus the incision of the endorrhachis should be carefully performed with the assistance of endoscopy to avoid injuries to the spinal cord. The long-term pressure on the spinal cord could result in the adhesion and thickening of the adjacent arachnoid and poor spinal cord pulsation. Thus the adhesive arachnoid between the spinal cord and the adjacent endorrhachis was separated carefully and removed as much as possible to release the spinal cord. However, the operational view of the surgical procedures on the cysts at the ventral spinal cord is generally limited, and traction of the spinal cord should be avoided as much as possible to avoid damage to the spinal cord nerves and adjacent vessels.
Subdural/epidural cyst treatment
Subdural/epidural cysts were treated by resection of the cyst wall. If no dense adhesion between the cyst wall and the endorrhachis or nerve root was found, the cyst was separated until the neck of the cyst, and then tight suturing was performed after resection of the cyst. In contrast, if dense adhesion between the cyst wall and nerve root made the separation of the cyst very difficult, partial removal of the cyst was performed, and then tight suturing was performed after the connecting hole had been filled with a section of free muscle mass. For cysts not connected with the subarachnoid space, the cyst wall was removed as much as possible. In cases of dense adhesion between nerve root and the cyst, the cyst wall was partially resected for drainage and decompression before tight overlapping suturing. A section of free muscle mass was then positioned on the dura at the site of the cyst and fixed by suture and inward pressure to prevent new cyst formation.
Intraspinal epidural cyst treatment
Intraspinal epidural cysts were treated by ligation of the cervix. In some cases, the muscle mass was isolated and used to plug the access hole prior to suturing of the cyst walls. If the nerve root or dural adhesion was weak, the cyst was mobilized to the neck, resected, and sutured tightly. However, in cases of very strong nerve root or dural adhesion the cyst wall was partially resected and a piece of free muscle mass was used to plug the access hole prior to tight suturing.
Intraspinal/extraspinal cyst treatment
Intraspinal and extraspinal cysts were removed through enlarged intervertebral foramina. Extraspinal cysts are easy to be treated. Operation of intraspinal cysts is similar to subdural/epidural cysts. If no dense adhesion between the cyst wall and the endorrhachis or nerve root was found, the cyst was separated until the neck of the cyst, and then tight suturing was performed after resection of the cyst. If dense adhesion between the cyst wall and nerve root made the separation of the cyst difficult, partial removal of the cyst was performed, and then tight suturing was performed with a section of free muscle mass. For cysts not connected with the subarachnoid space, the cyst wall was removed.
Postoperative follow-up
All patients were followed up, with a mean period of 69 months (range 3–187 months). Cases of recurrence, death, or second surgery were recorded.
Fugl-Meyer scale assessments
FM scores were assessed preoperatively and at postoperative day 90 on a 0- to 99-point scale. As previously described,13,14 FM scores were assessed as severe or marked motor impairment (0–84), moderate motor impairment (85–95 points), and slight motor impairment (96–99 points).
Preoperative FM scores of all patients were less than 50 points after conservative therapy. Significant improvement was determined when postoperative FM score achieved 96–99, and clinical symptoms disappeared with incident pain or numbness; patients had a normal life and work. Improvement was determined when postoperative FM score achieved 85–95, and parts of symptoms disappeared but some moderate motor impairment still remained. No improvement was determined when postoperative FM score remained 0–84.
Results
Patients’ demographic and clinical characteristics
Among the 81 included patients, 34 were males and 47 were females, with a mean age of 36.5 years (ranging from 6 to 66 years) (Table 1). Intraspinal epidural cysts were significantly more frequent than other types – 66.7% (54 of 81). Ten (12.4%) patients developed multiple lumbar and lumbosacral segment intraspinal cysts. Intraspinal epidural cysts were predominantly located in the lumbar and lumbosacral segments (83.3%, 45 of 54) and in the thoracic and thoracolumbar segments (18.5%, 15 of 81). The incidence of subdural extramedullary cysts was 18.5% (15 of 81), with cysts located primarily in the thoracic and thoracolumbar segments (93.3%, 14 of 15). Eight patients had intramedullary cysts in the cervical and cervicothoracic segments (62.5%, five of eight) and the thoracic and thoracolumbar segments (37.5%, three of eight). Intraspinal/extraspinal cyst (three of 81) occurrence was rare, occurring in significantly fewer patients than other types (Table 1).
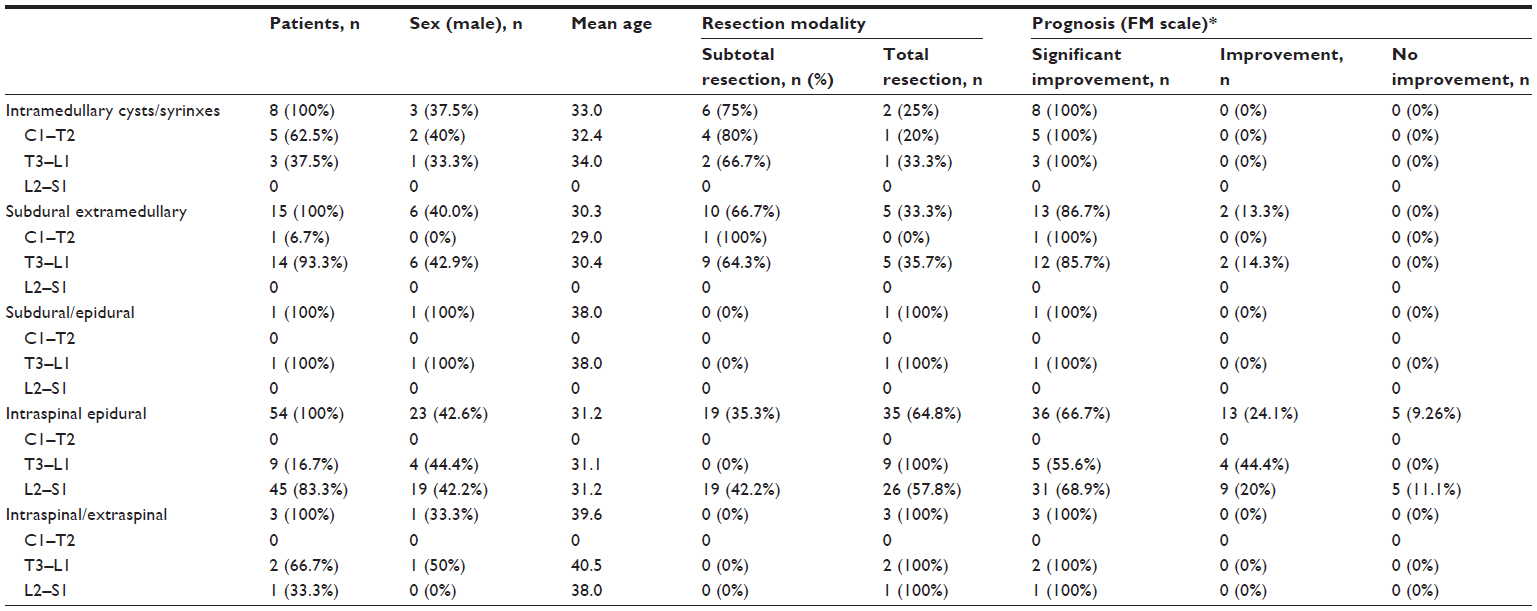 | Table 1 Incidence, resection modality, and prognosis of the five types of spinal arachnoid cysts |
The clinical symptoms of the patients with spinal arachnoid cyst varied with the location of the cyst. For patients with the cyst at the cervical level, the symptoms were mainly pain at the neck, shoulder, and upper limbs; weakness of the upper limbs could also be observed. For patients with the cyst at the thoracic level, the major symptoms were pain in the chest and back, as well as spastic paralysis of the lower limbs. For patients with the cyst at the lumbosacral level, lumbosacral pain and lower-limb pain could occur when abdominal pressure increased. As some cysts are connected with the subarachnoid space, the cerebrospinal fluid could flow into the cyst cavity when the abdominal pressure increased and caused enlargement of the cyst, which could compress the nerve root and aggravate the symptoms. When the patients were put in the horizontal position, the cyst shrank, relieving the symptoms. Sphincter dysfunction could be observed in the late period of the disease, and urination- and defecation-function impairment could also occur in some cases that needed more time to recover after the operation.
Surgical difficulty varied according to type and anatomical location
Total resection was not performed in 55.6% (45 of 81) of patients due to surgical difficulties. Compared to all other types, patients with intramedullary and subdural extramedullary cysts were more difficult to surgically handle. For these patients, subtotal resection was significantly more common than total resection (intramedullary, six versus two; subdural extramedullary, ten versus five). Notably, 100% (ten of ten) of patients with multiple intraspinal cysts experienced surgical difficulties and thus underwent subtotal resection. Total resection was performed in 100% (ten of ten) of patients with subdural/epidural cysts. In patients with intraspinal epidural cysts, total resection was significantly more common than subtotal resection, applicable in 100% (nine of nine) of cases affecting thoracic and thoracolumbar segments and in 57.8% (26 of 45) of cases affecting lumbar and lumbosacral segments.
FM scores
All patients (100%, eight of eight) with intramedullary cysts/syrinxes reported slight FM-score improvement. The majority of subdural extramedullary cyst patients experienced slight improvements (13 of 15, 86.7%), and none of these patients reported no improvement. All subdural/epidural (100%, one of one) and intraspinal/extraspinal (100%, three of three) reported improvements. Notably, in the largest patient group, intraspinal epidural cyst patients, only 66.7% (36/54) of patients reported slight improvements, and 9.26% (five of 54) reported no improvement, making these patients significantly more likely to experience no postoperative improvement in FM score.
Outcomes and recurrence
Two patients suffered from an intramedullary cyst recurrence. Their first surgery was posterior myelotomy and cyst opening. Recurrence was observed 2 months after operation in both patients. During the second operation, the incision of the spinal cord was found to be connected by scars, which led to the recurrence of the cyst. These two patients recovered after the cysts were totally removed, and no recurrence was identified by the end of the follow-up. No death was observed in any patient.
Discussion
The current study used a novel five-category classification system for spinal arachnoid cysts. Intraspinal epidural spinal arachnoid cysts were significantly more common than other cyst types, followed by subdural extramedullary and intramedullary cysts/syrinxes. Notably, conventional classification systems that only use anatomical location for diagnosis fail to consider intraspinal epidural spinal arachnoid cysts as a distinct type, despite the current indications that these patients are much more likely to have limited or no improvement following routine surgical intervention. Thus, the use of the five-category classification system for spinal arachnoid cysts clearly indicated that some patients were at greater risk for poor outcomes following surgery, requiring more careful treatment planning. Wider use of the five-category classification may allow a better clinical assessment of patients at risk for poor surgical outcomes after failure of a conservative treatment.
Though conventional classification of spinal arachnoid cysts may be effective in most patients, the present study indicates that there is a distinct subpopulation of patients that will have no evidence of symptom improvement after surgery. A number of previous clinical studies have identified characteristics of this at-risk population,14–19 including patients with slight adherence of the nerve root and cyst, separation of the cervical region of the cyst, and close adherence between the nerve root and cyst during resection, complicating separation or leading to partial resection. Hamamcioglu et al20 reported a case of extradural cyst, unusual in size, location, and clinical features, that complicated a routine surgery, due to the required movement of muscle mass to close the dural defect after excision. Similarly, Lee and Cho21 reported that while complete surgical excision was the best treatment for a variety of spinal arachnoid cyst types, the pleural cavity or right atrium modality should be based on MRI findings rather than on anatomical classifications. Thus, the additional benefits of identifying and stratifying spinal arachnoid cysts based on both anatomical classification and MRI findings have been increasingly reported, and the current study offers the first system for standardizing these recommendations.
The current study observed that intraspinal epidural spinal arachnoid cysts were the most common. Though intraspinal cyst cases have been previously reported,22 the intraspinal epidural classification is unique to the proposed system. The present study demonstrated that these cases are more likely to experience poor surgical outcomes as well as limited functional improvements and symptom alleviation, consistent with a previous report that these cases are often afflicted with complications, such as spinal disk herniation.22 Additionally, though subdural/epidural cysts (one patient) and intraspinal multiple cysts (ten patients) were relatively rare in this study, examination of larger cohorts of these patients may reveal that they are similarly at risk, due to the unique nature of these lesions and potential for complications, particularly when they occur in ventral locations.23 Additionally, trauma and labor in females can result in multiple spinal arachnoid cysts, where the presence of more than one lesion complicates treatment even further.24 Thus, classification schemes that use only anatomical location may increase the risk of poor surgical outcomes in many patient subpopulations. Therefore, these patients should be identified early in the treatment process, and specific surgical procedures and treatment plans should be developed based on MRI as well as anatomical findings.
While the proposed five-category classification system is based on MRI findings of cyst manifestation, other researchers have employed stratification by clinical signs and symptoms.24,25 Wang et al23 reported that patients with preoperative neuropathic pain or numbness were much less likely to benefit from surgery than those with myelopathy or weakness, suggesting that surgical success could also be improved by the use of intraoperative ultrasound to guide aggressive surgical treatment. Based on size and clinical symptoms, it may be possible to determine more readily whether complete resection, shunting, or duraplasty will most optimally result in a high rate of cyst and syrinx obliteration without symptom recurrence,24 particularly in the case of giant spinal arachnoid cysts.25 Thus, further study will be required to determine whether the current five-category system is significantly related to alleviation of certain symptoms, requiring investigation before wide implementation of these findings.
Cysts could also be classified according to their etiology. However, such classifications need to be validated, because cysts at different locations could have the same causes, and the same kinds of cysts could also have different causes. Nevertheless, the predilection sites vary with the types of cysts. In the present study, all the subdural extramedullary cysts were found at the cervicothoracic level, while the extradural cysts were mainly located at the lumbosacral level. However, there were nine patients with extradural cysts located at the cervicothoracic level. Several similar clinical symptoms were found between the patients with subdural extramedullary and extradural cysts at the cervicothoracic vertebra. For patients with the cysts located at the thoracic or thoracolumbar level, numbness, weakness, and pain of lower extremities were generally observed. For patients with cysts located at the lumbosacral level, radiculalgia, extremity spasticity, and weakness were generally observed, and urination- and defecation-function disturbances were also found in some patients.
Considering these findings, the retrospective nature, wide time intervals between treatments, and the possibility of unrecognized selection and recall biases must be considered. A selection bias might be due to the fact that all included patients did not respond to conservative treatment and had to undergo surgery. In addition, due to the retrospective nature of the study, FM scores were not available for all patients, since scores were assessed in patients with obvious symptoms at admission. Furthermore, considerable changes in surgical technology from 1995 to now may further complicate the interpretation of these findings. However, the rarity of the condition necessitates a long study period to achieve a relevant number of cases. In addition, the group of selected patients all had a preoperative FM score <50 after conservative treatment. Surgery is only an alternative treatment, and many patients did not improve their FM score after surgery, indicating that the surgical strategies could still be improved and that a careful selection of patients for surgery could improve surgical outcomes. Nevertheless, validation in larger sample sizes is required, potentially as a multicenter effort.
After failure of a conservative treatment, patients with the most common cyst type, intraspinal epidural cysts, were the most likely to exhibit poor outcomes following conventional resection surgery. By using combined MRI imaging and anatomical findings, the proposed five-category classification provides a critically needed means for classifying spinal arachnoid cyst patients at risk for poor treatment outcomes or symptom alleviation, thereby allowing for divergent surgical intervention for specific cyst types. This may lead to a greater standardization of care and improved overall prognoses for spinal arachnoid cyst patients. Despite these positive preliminary indications of the effectiveness of this system, larger multicenter prospective studies will be required to confirm these observations, particularly in rarely reported spinal arachnoid cyst subtypes.
Disclosure
The authors report no conflicts of interest in this work.
References
Hughes G, Ugokwe K, Benzel EC. A review of spinal arachnoid cysts. Cleve Clin J Med. 2008;75:311–315. | |
Pradilla G, Jallo G. Arachnoid cysts: case series and review of the literature. Neurosurg Focus. 2007;22:E7. | |
Bitaraf MA, Zeinalizadeh M, Meybodi AT, Meybodi KT, Habibi Z. Multiple extradural spinal arachnoid cysts: a case report and review of the literature. Cases J. 2009;2:7531. | |
Zhou JY, Pu JL, Chen S, Hong Y, Ling CH, Zhang JM. Mirror-image arachnoid cysts in a pair of monozygotic twins: a case report and review of the literature. Int J Med Sci. 2011;8:402–405. | |
Oberbauer RW, Haase J, Pucher R. Arachnoid cysts in children: a European co-operative study. Childs Nerv Syst. 1992;8:281–286. | |
Rengachary SS, Watanabe I. Ultrastructure and pathogenesis of intracranial arachnoid cysts. J Neuropathol Exp Neurol. 1981;40:61–83. | |
Choi JY, Kim SH, Lee WS, Sung KH. Spinal extradural arachnoid cyst. Acta Neurochir (Wien). 2006;148:579–585; discussion 585. | |
Brant WE, Helms CA. The Brant and Helms Solution: Fundamentals of Diagnostic Radiology. 3rd ed. Philadelphia: Lippincott Williams and Wilkins; 2006. | |
Go KG, Hew JM, Kamman RL, Molenaar WM, Pruim J, Blaauw EH. Cystic lesions of the brain. A classification based on pathogenesis, with consideration of histological and radiological features. Eur J Radiol. 1993;17:69–84. | |
Galassi E, Tognetti F, Gaist G, Fagioli L, Frank F, Frank G. CT scan and metrizamide CT cisternography in arachnoid cysts of the middle cranial fossa: classification and pathophysiological aspects. Surg Neurol. 1982;17:363–369. | |
Nabors MW, Pait TG, Byrd EB, et al. Updated assessment and current classification of spinal meningeal cysts. J Neurosurg. 1988;68:366–377. | |
Neurosurgical Video Gallery. Intraspinal cysts. Available from: http://www.neurosurgery.tv/intraspinalcysts.html. Accessed March 27, 2013. | |
Clancey JK. Karnofsky performance scale. J Neurosci Nurs. 1995;27:220. | |
Mor V, Laliberte L, Morris JN, Wiemann M. The Karnofsky Performance Status Scale. An examination of its reliability and validity in a research setting. Cancer. 1984;53:2002–2007. | |
Raeder MB, Helland CA, Hugdahl K, Wester K. Arachnoid cysts cause cognitive deficits that improve after surgery. Neurology. 2005;64:160–162. | |
Jallo GI, Woo HH, Meshki C, Epstein FJ, Wisoff JH. Arachnoid cysts of the cerebellopontine angle: diagnosis and surgery. Neurosurgery. 1997;40:31–37; discussion 37–38. | |
Koch CA, Voth D, Kraemer G, Schwarz M. Arachnoid cysts: does surgery improve epileptic seizures and headaches? Neurosurg Rev. 1995;18:173–181. | |
Gangemi M, Maiuri F, Colella G, Sardo L. Endoscopic surgery for large posterior fossa arachnoid cysts. Minim Invasive Neurosurg. 2001;44:21–24. | |
Kunz U, Mauer UM, Waldbaur H. Lumbosacral extradural arachnoid cysts: diagnostic and indication for surgery. Eur Spine J. 1999;8:218–222. | |
Hamamcioglu MK, Kilincer C, Hicdonmez T, Simsek O, Birgili B, Cobanoglu S. Giant cervicothoracic extradural arachnoid cyst: case report. Eur Spine J. 2006;15 Suppl 5:595–598. | |
Lee HJ, Cho DY. Symptomatic spinal intradural arachnoid cysts in the pediatric age group: description of three new cases and review of the literature. Pediatr Neurosurg. 2001;35:181–187. | |
Kono K, Nakamura H, Inoue Y, Okamura T, Shakudo M, Yamada R. Intraspinal extradural cysts communicating with adjacent herniated disks: imaging characteristics and possible pathogenesis. AJNR Am J Neuroradiol. 1999;20:1373–1377. | |
Wang MY, Levi AD, Green BA. Intradural spinal arachnoid cysts in adults. Surg Neurol. 2003;60:49–55; discussion 55–46. | |
Ergun T, Lakadamyali H. Multiple extradural spinal arachnoid cysts causing diffuse myelomalacia of the spinal cord. Neurologist. 2009;15:347–350. | |
Kumar S, Chauresia P, Singh D, Singh H. Giant thoracolumbar intradural multilobulated arachnoid cyst. Neurol India. 2012;60:134–135. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.