Back to Journals » Nature and Science of Sleep » Volume 18

A Nomogram Model for Predicting Moderate to Severe OSA in Western China: A Retrospective Analysis
Authors Gul A, Talifu A, Aili M, Xie X, Kuerban Y, Wusiman Z, Wushuer P, Huang F, Dong J ![]() , Li Z
, Li Z ![]()
Received 8 January 2026
Accepted for publication 26 May 2026
Published 25 June 2026 Volume 2026:18 592761
DOI https://doi.org/10.2147/NSS.S592761
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Marco Veneruso
Aman Gul,1– 3,* Ainiwaer Talifu,4,* Maimaiti Aili,1 Xuejiao Xie,5 Yilifanjiang Kuerban,1 Zulipikaer Wusiman,1 Palidan Wushuer,6,* Fuxian Huang,1 Jingcheng Dong,2,3,* Zhijian Li1,*
1Department of Clinical Basic Research Center, Uyghur Medicines Hospital of Xinjiang Uyghur Autonomous Region, Urumqi, 830000, People’s Republic of China; 2Department of Integrative Medicine, Huashan Hospital, Fudan University, Shanghai, 200040, People’s Republic of China; 3Institute of Integrated Traditional Chinese and Western Medicine, Fudan University, Shanghai, 200040, People’s Republic of China; 4People’s Hospital of Xinjiang Uyghur Autonomous Region Xinjiang Uyghur Autonomous Region, Urumqi, 830001, People’s Republic of China; 5College of Chinese Medicine, Hunan University of Chinese Medicine, Changsha, Hunan, 410208, People’s Republic of China; 6Xinjiang Uyghur Autonomous Region Hospital of Traditional Chinese Medicine, Urumqi, 830000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jingcheng Dong, Department of Integrative Medicine, Huashan Hospital, Fudan University, Shanghai, 200040, People’s Republic of China, Email [email protected] Zhijian Li, Uyghur Medicines Hospital of Xinjiang Uyghur Autonomous Region, Urumqi, 830049, People’s Republic of China, Email [email protected]
Objective: To develop an interpretable nomogram model for predicting moderate-to-severe obstructive sleep apnea (OSA).
Methods: This retrospective study analyzed 11,030 OSA patients who underwent polysomnography between 2012 and 2020. Patients were randomly divided into a modeling cohort (n=7,721) and a validation cohort (n=3,309) in a 7:3 ratio. Based on disease severity, patients were further classified into mild and moderate-to-severe subgroups. General clinical data were collected. Independent risk factors were identified using multivariate logistic regression, and a nomogram prediction model was constructed using the R “rms” package.
Results: Univariate analysis showed significant differences in age, BMI, neck circumference, gender, hypertension, diabetes, smoking status, alcohol consumption, and coronary heart disease between the mild and moderate-to-severe groups in both cohorts (all P < 0.05). Multivariate logistic regression identified age, BMI, neck circumference, male gender, hypertension, and diabetes as independent risk factors for moderate-to-severe OSA (all P < 0.05). The nomogram model demonstrated good fit (Hosmer-Lemeshow test: modeling cohort χ2=10.754, P=0.216; validation cohort χ2=8.383, P=0.397). Decision curve analysis confirmed the model’s clinical utility within specific risk thresholds. The area under the ROC curve was 0.676 (95% CI: 0.664– 0.688) for the modeling cohort and 0.613 (95% CI: 0.593– 0.632) for the validation cohort, indicating strong predictive performance.
Conclusion: The nomogram model based on age, BMI, neck circumference, gender, hypertension, and diabetes provides a valuable tool for predicting and assessing moderate-to-severe OSA, offering important strategic guidance for clinical practice.
Keywords: obstructive sleep apnea, sleep-disordered breathing, nomogram
Introduction
Obstructive sleep apnea (OSA) is characterized by repeated collapse of the upper airway during sleep, which can cause apnea and hypopnea. The prevalence of OSA continues to increase with obesity and aging, and is closely related to complications such as cardiovascular and cerebrovascular diseases and diabetes.1–4 About 936 million people aged 30–69 years are affected globally, and about 425 million people are moderately or severely affected, with about 176 million patients in China.5,6 The 5-year mortality rate of untreated severe OSA is 11%-13%, and patients with moderate to severe OSA have a higher risk of poor prognosis, so early identification is particularly important.7 Polysomnography (PSG) is the gold standard for the diagnosis of OSA, which can monitor more than 10 kinds of physiological indicators such as electroencephalogram (EEG) and respiration, distinguish sleep stages, record key data such as apnea and blood oxygen saturation, and provide objective diagnostic basis.However, PSG is a resource-intensive examination that is complex to operate, expensive, and has a long waiting period, particularly in areas with limited medical resources. This seriously restricts the early diagnosis and intervention of OSA.8 Although alternative diagnostic methods including the home sleep apnea test (HSAT), type IV sleep monitoring devices, and assessment tools like the Epworth Sleepiness Scale (ESS), STOP-BANG questionnaire, and Berlin Questionnaire (BQ) have been introduced, each method has unique advantages and limitations that restrict their effectiveness as standalone diagnostic tools for OSA.9 Most of the existing sleep apnea screening scales have problems such as imbalance of sensitivity and specificity, poor suitability to the population, and inability to accurately predict moderate to severe risk, which is difficult to meet the needs of efficient screening in primary care. Compared with the existing studies, this study is the first to construct an OSAHS prediction model based on a large sample of real-world data in western China, with a larger sample size and stronger regional specificity. The core clinical indicators used in this study are simpler and easier to obtain, and more suitable for primary care screening in areas with limited medical resources, which can improve the shortcomings of the previous model in the western population. Nomograms, as a clinically practical risk prediction tool, integrate multidimensional clinical variables and transform complex regression models into an intuitive scoring system. They can accurately predict individual disease risk and clearly display the contribution weight of each variable, offering new possibilities for precise stratified management of OSA. This study aims to identify the risk factors for moderate or severe OSA as per clinical data from the population in western China. We will establish and validate a practical nomogram prediction model, providing evidence-based support for optimizing regional OSA screening strategies, improving patients’ quality of life, and reducing the healthcare burden.
Materials and Methods
General Information
A total of 11,853 patients diagnosed with OSA through PSG were initially enrolled. After applying exclusions, 11,030 individuals were randomly split into a modeling cohort (n = 7,721) and a verification cohort (n = 3,309) with 70% of the patients assigned to the modeling cohort. This cohort was further subdivided into a mild cohort (n = 2,802) and a moderate to severe cohort (n = 4,919) based on the severity of their conditions. The verification cohort was further split into a mild cohort (n = 1,201) and a moderate to severe cohort (n = 2,108) for subsequent analysis. Inclusion criteria: (1) Age of 18 years or above; (2) Underwent overnight PSG monitoring at the sleep center of this hospital, with a total monitoring time of at least 4 hours; (3) Complete clinical medical records. Exclusion criteria: (1) Suffering from a neuromuscular disease; (2) Having previously received treatment for sleep apnea; (3) Diagnosed with central sleep apnea by PSG; (4) Long-term use of medications that affect sleep quality (such as sedatives and hypnotics); (5) Missing key data in the medical record.
Methods
Data Preprocessing
For the initial collection of 11,853 records were cleaned. 105 duplicate entries were identified and deleted. Missing data were addressed, including 2 missing snoring records. 233 entries, 3 missing data points for fatigue and drowsiness. Of the 233 observed apnea data points, 700 were missing. The imputation of missing values was conducted through multiple imputation by chained equations, resulting in 11,030 complete data points for subsequent analysis.
Feature Variable Collection
The following three categories of characteristic variables came from the medical record system: (1) Demographic characteristics and lifestyle habits: age, gender, BMI, neck circumference, smoking history, Heart failure and drinking history; (2) Comorbidities and laboratory indicators: hypertension, diabetes, coronary heart disease, arrhythmia, ischemic stroke, hypothyroidism, fatty liver, chronic obstructive pulmonary disease, abnormal airway anatomy, hyperhomocysteinemia, hyperuricemia, benign prostatic hyperplasia, FT3, FT4, ALP, BUN,CREF, LDL, and VLDL; (3) Clinical symptoms and vital signs: including total bed rest time, core temperature, breathing rate, and systolic and diastolic blood pressure. In total, 29 items were entered into the research database along with the polysomnography monitoring results.
Diagnostic Criteria
(1) OSA: Diagnostic criteria: AHI exceeds 5 times per hour; Grading criteria are as follows: OSA severity was defined as follows: mild (AHI: 5–15 times/hour), moderate (AHI: > 15–30 times/hour), and severe (AHI: > 30 times/hour).10 (2) Diabetes: In accordance with the 2020 Chinese Guideline,11 diabetes is diagnosed if any of the following conditions are satisfied: fasting blood glucose (FBG) > 7.0 mmol/L; a 2-hour OGTT blood glucose > 11.0 mmol/L from an oral glucose tolerance test; or currently receiving hypoglycemic drug treatment. (3) Hypertension: Hypertension is defined by blood pressure: 140–159/90-99 mmHg for Grade 1, 160–179/100-109 mmHg for Grade 2, and values exceeding 180/110 mmHg for Grade 3.12
Statistical Methods
Data processing was performed with SPSS 27.0, and the level of statistical significance was defined as α = 0.05. The Kolmogorov–Smirnov and Levene tests were utilized to examine normality and variance homogeneity. Continuous data with normal distribution were shown as mean ± SD, and t-tests were used for between-group comparisons. Categorical data are presented as n (%), and the χ2 test was used for comparisons. Logistic regression analysis was performed for multivariate regression analytical approach. A nomogram prediction model was created with R 4.2.1, and calibration curves were generated. The Hosmer-Lemeshow test was employed to evaluate the model’s goodness of fit. The bootstrap method was adopted to internal validation, and the C-index served as a measure of discriminative performance. Receiver operating characteristic (ROC) curves were used to evaluate power.
Results
General Comparison
According to the univariate analysis results presented in Tables 1 and 2, no significant differences in moderate-to-severe OSA prevalence were noted between the modeling group and the experimental group regarding arrhythmia, ischemic stroke, hypothyroidism, fatty liver disease, chronic obstructive pulmonary disease, abnormal airway anatomy, hyperhomocysteinemia, hyperuricemia, benign prostatic hyperplasia, total bed rest duration, core temperature, breathing rate, blood pressure (systolic and diastolic), FT3, FT4, ALP, BUN, LDL, and VLDL (all P > 0.05). However, the prevalence of moderate-to-severe OSA significantly associated with age, gender, BMI, neck circumference, hypertension, diabetes mellitus, smoking history, alcohol consumption history, and coronary heart disease (all P < 0.05).
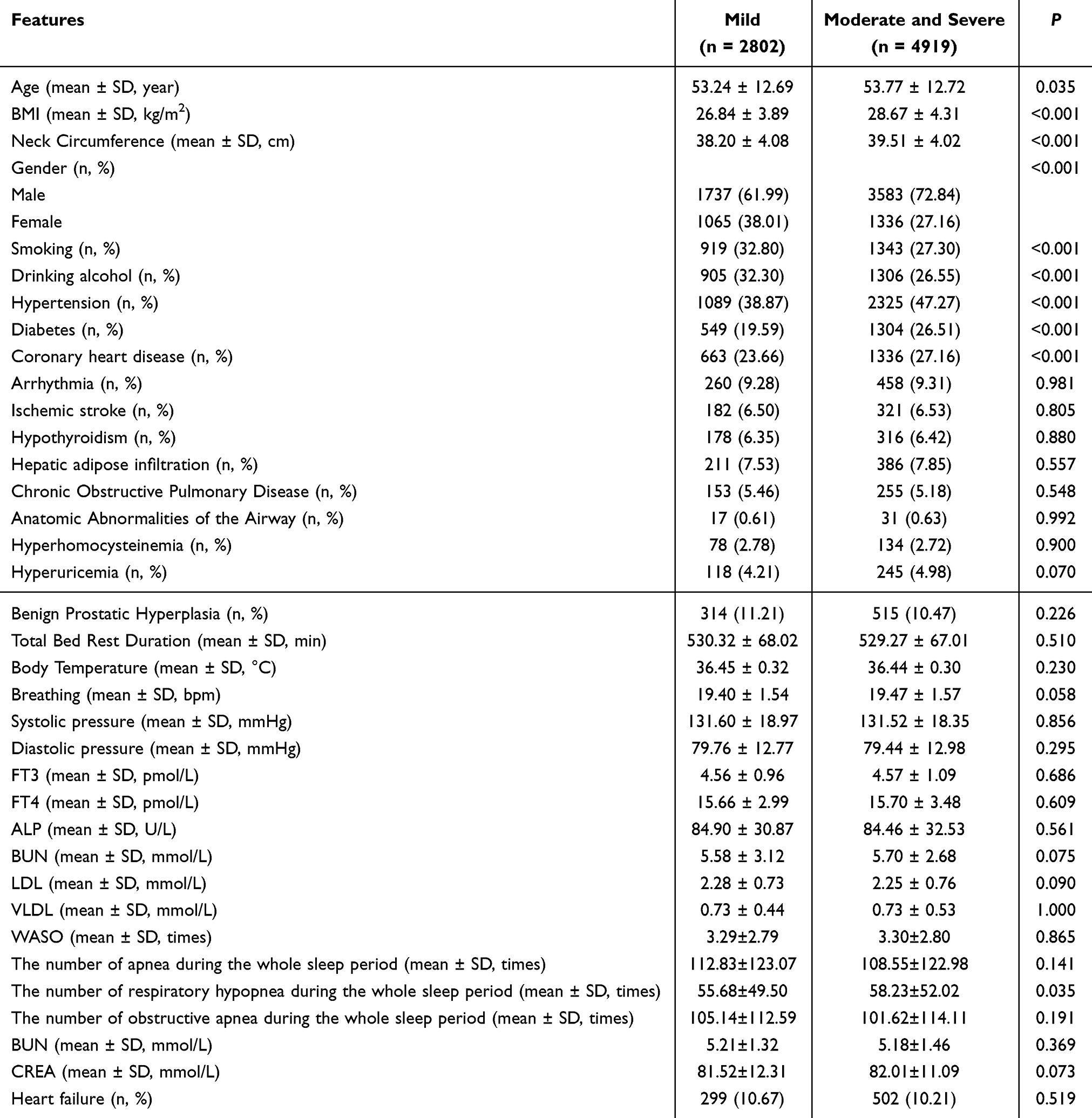 |
Table 1 Comparison of General Data of the Modeling Group |
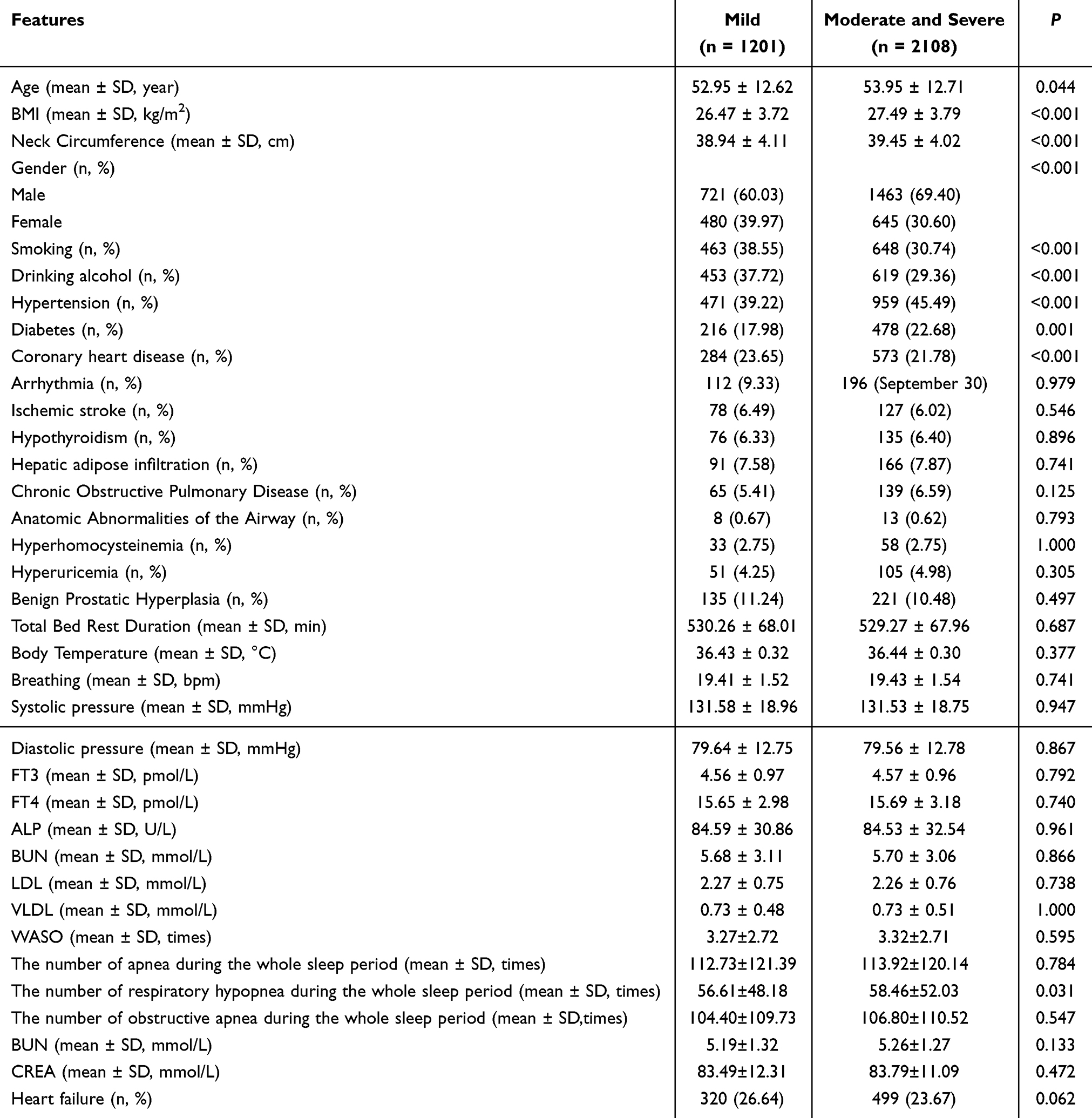 |
Table 2 Comparison of General Data of the Test Modules |
Multifactor Logistic Regression Model Analysis
The statistically significant differences presented in Table 1 were analyzed using the following indicators: the occurrence of moderate-to-severe OSA as the dependent variable (moderate and severe groups = 1, mild group = 0), and the independent variables of Age (original value), BMI (original value), neck circumference (NC, original value), Gender (Male = 1, Female = 2), Smoking status (Yes=1, No=0), Alcohol consumption (Yes = 1, No = 0), Hypertension (Yes = 1, No = 0), Diabetes (Yes = 1, No = 0), and Coronary heart disease (Yes = 1, No = 0),The number of respiratory hypopnea during the whole sleep period (original value) as independent variables. The results indicated that the primary influencing factors for the severity of moderate to severe OSA were age, BMI, NC, gender, hypertension, and diabetes (P < 0.05). Refer to Table 3 for details.
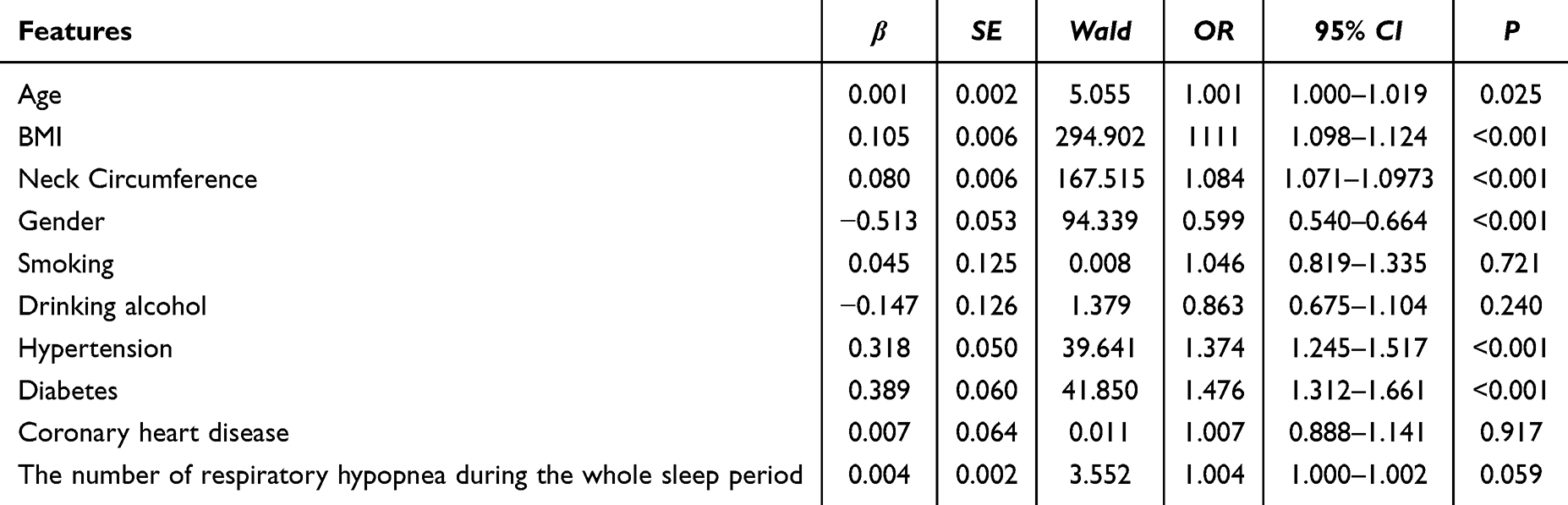 |
Table 3 Results of Multivariate Logistic Regression Model Analysis |
Constructing a Nomogram Prediction Model for Moderate-to-Severe OSA Patients
According to the outcomes of the multivariate analysis, this research identified six key variables with independent predictive significance. Using age, BMI, neck circumference, gender, hypertension, and diabetes as predictive factors, a nomogram prediction model was established to stratify the severity of OSA in patients with moderate to severe conditions, as presented in Figure 1.
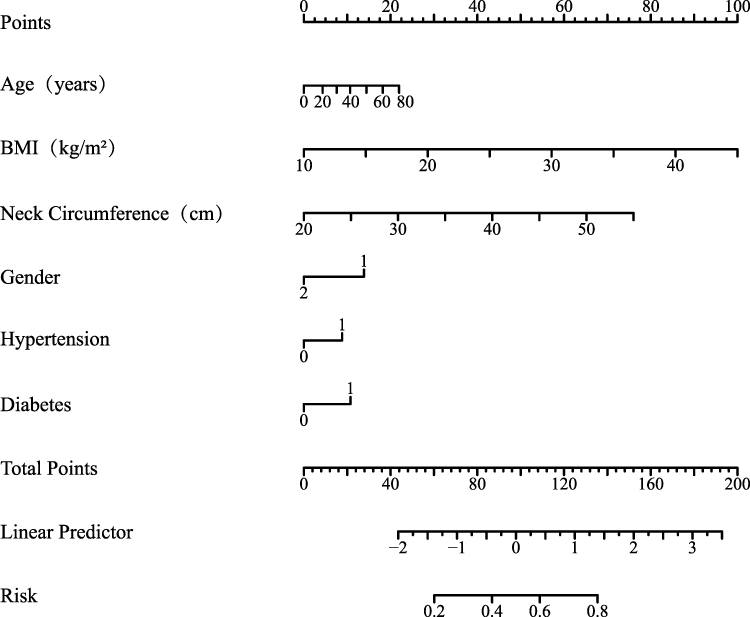 |
Figure 1 Nonograph prediction model for OSA patients with moderate-to-severe disease severity. The nomogram is designed to quickly assess the risk of moderate to severe obstructive sleep apnea (OSA). It is easy to operate and does not require calculation. The specific steps are as follows: 1. Determine the patient’s age, BMI, neck circumference, gender, hypertension and diabetes. 2. Find the patient’s numerical position on the corresponding index axis, and make the vertical line upward to obtain the corresponding score; 3. The total score was obtained by adding the scores of the six indicators, locating on the axis of the total score and making a vertical line downward; 4. The intersection of the vertical line and the risk axis is the predicted risk probability of moderate to severe OSA in this patient, and the higher the value, the higher the risk. |
Validation of the Nomogram Prediction Model
Calibration Curve and Clinical Net Benefit Analysis of the Nonograph Prediction Model
Internal model validation was conducted using Bootstrap, while external model validation was performed with a validation cohort. Calibration curve analysis revealed that the nomogram prediction model achieved a C-index of 0.676 (95% CI 0.663–0.688) in the modeling cohort and 0.613 (95% CI 0.593–0.633) in the validation cohort; the calibration plot closely aligned with the perfect diagonal. The Hosmer-Lemeshow goodness-of-fit test results indicated that the modeling group had χ2 = 10.754, P = 0.216, and the validation group had χ2 =8.383, P = 0.397. These findings suggest that the prediction model is reasonably consistent and provides a good fit, as shown in Figure 2. Decision curve analysis demonstrated that the predictive model could yield significant additional clinical net benefits when the risk threshold for the modeling cohort exceeded greater than 0.6 and when the risk threshold for the validation cohort ranged between 0.60 and 0.90 (Figure 3).
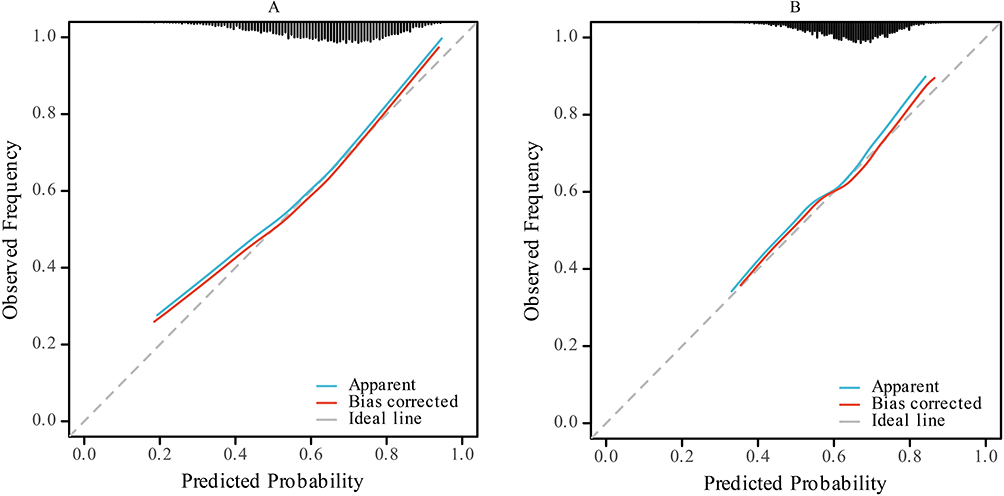 |
Figure 2 Calibration curve evaluation nomogram prediction model. (A) Modeling Group; (B) Model Verification Group. |
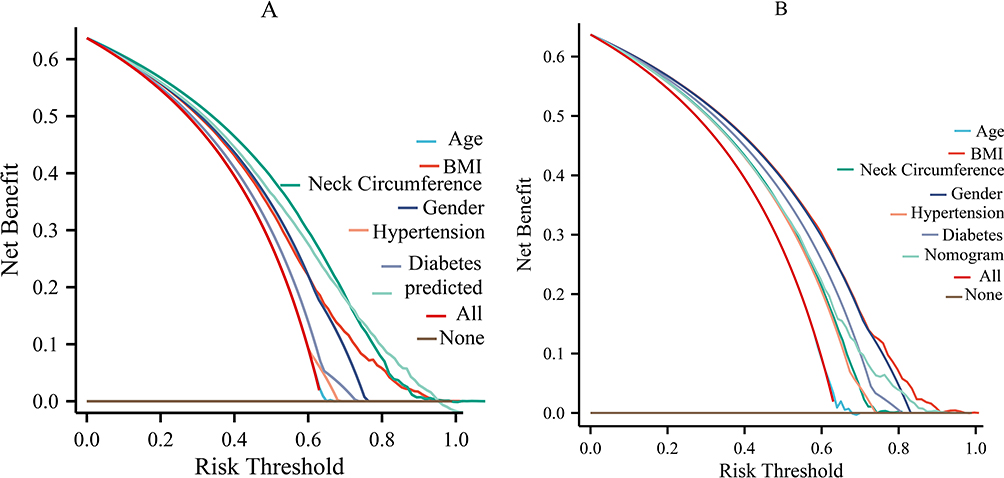 |
Figure 3 Decision Curve Evaluation Novologram Prediction Model. (A) Modeling Group; (B) Model Verification Group. |
Evaluation of Predictive Performance
The ROC curve analysis revealed an AUC of 0.676 for the modeling group, with a 95% confidence interval ranging from 0.664 to 0.688. This indicates a strong predictive ability for moderate and severe OSA. The experimental group achieved an AUC of 0.613, with a 95% confidence interval of 0.593 to 0.632. This analysis reveals that the nomogram model developed in this study has strong discriminatory capability and forecasting accuracy (Figure 4).
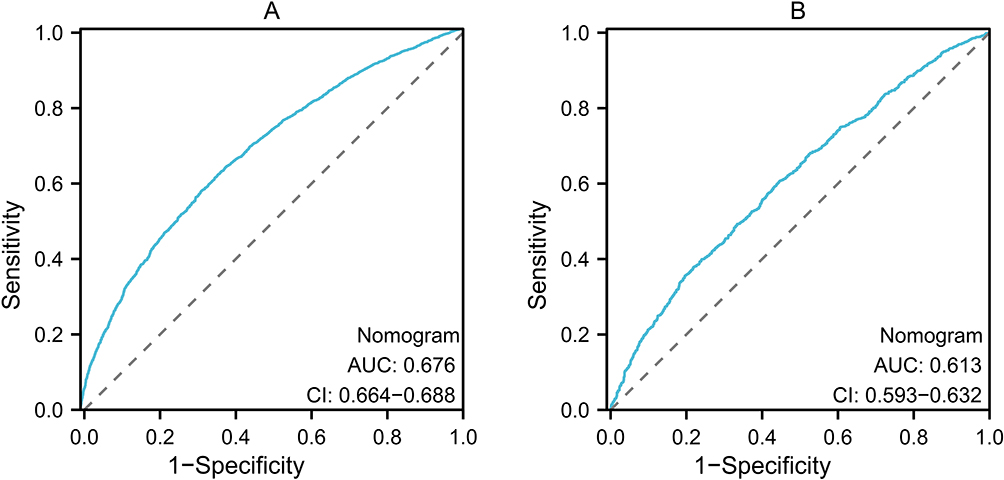 |
Figure 4 The nomogram’s ROC curve. (A) Modeling Group; (B) Model Verification Group. |
Discussion
Early identification of OSA, particularly screening for moderate to severe OSA, is crucial for improving patient prognosis and optimizing the allocation of medical resources.13 A nomogram prediction model was developed and validated in this study, utilizing a large-scale clinical cohort in western China. Unlike previous models that focused on populations in Europe, the United States, or the eastern coastal areas of China, this study is the first to concentrate on the population in western China. It takes into account the region’s unique genetic background, living environment, and distribution of medical resources, thereby ensuring the model’s regional applicability.This model effectively addresses the gap in OSA risk prediction tools in western China.14,15 This is a very simple tool to use. It can be easily integrated into the primary health care system, where only a few PSG tools are currently available. It quickly identifies individuals who may be at risk and facilitates proper referrals. This can lead to a better allocation of medical resources, ultimately improving patient outcomes.
Univariate analysis revealed significant differences in age, gender, BMI, neck circumference, smoking history, alcohol history, hypertension, diabetes, and CHD across OSA severity subgroups (P < 0.05). These variables were initially identified as potential risk predictors. Further screening using logistic regression was conducted to construct a nomogram containing the core predictors. This study confirmed that the nomogram model, which includes six features (age, BMI, neck circumference, gender, hypertension, and diabetes), demonstrated excellent discriminative ability in predicting moderate to severe OSA. Calibration curve analysis revealed that the nomogram model exhibited a C-index of 0.868, demonstrating robust consistency and precision in its predictive performance.
Age is a significant risk factor for OSA.16,17 Advanced age is an important independent predictor of moderate to severe OSA. As individuals age, they are more likely to experience airway collapse due to reduced of upper airway muscle tone and fat redistribution, increasing the likelihood of moderate to severe OSA. Therefore, clinical screening for OSA should pay more attention to the middle-aged and elderly population. BMI and neck circumference are key indicators of obesity and fat distribution. This study confirmed that both are independent predictors of OSA, consistent with previous research.18,19 Neck circumference, as a key marker of upper body subcutaneous fat deposition, is closely related to increased lipolytic activity in the neck. A substantial hepatic influx of free fatty acids can lead to hepatic lipid deposition and insulin resistance. Additionally, neck fat secretes inflammatory factors, such as TNF-α and IL-6, which disrupt signaling pathways by blocking insulin receptor phosphorylation.20 Neck fat accumulation compresses the upper airway, exacerbating airway collapse and leading to recurrent hypoxemia and sleep fragmentation. OSA further worsens insulin resistance through a dual mechanism: intermittent hypoxia activates HIF-1α, inhibiting glucose transport, while sympathetic nerve activation increases catecholamine and cortisol secretion, creating a self-reinforcing cycle of metabolic disorders.21,22 Neck circumference not only indicates the risk of upper airway mechanical compression but also serves as a primary marker for metabolic disorders. Neck fat releases inflammatory substances that impair the body’s insulin response via blood circulation, and the lack of oxygen during the night due to OSA exacerbates these issues. This bidirectional pathophysiological mechanism illustrates why neck circumference offers unique predictive value for moderate to severe OSA beyond BMI.
Furthermore, this study found that metabolic comorbidities, such as hypertension and diabetes, were significantly more prevalent in the moderate to severe OSA group (P < 0.001), consistent with earlier research. These comorbidities share risk factors, such as obesity, with OSA and may worsen the disease process by impacting autonomic nerve function and other pathways. The morning hypertension observed in OSA patients, hypertension, and diabetes is strongly associated with sympathetic nerve activation resulting from repeated nocturnal hypoxia. Additionally, abnormal glucose metabolism arises from hypoxia-induced inhibition of the insulin signaling pathway. These metabolic abnormalities not only result from OSA but can also exacerbate upper airway instability by affecting autonomic nerve function and increasing the systemic inflammatory state, creating a vicious cycle. Diabetes risk in older patients with hypertension and OSA is significantly influenced by NC, and these two comorbid conditions can also influence the severity of OSA.23,24 Therefore, in clinical practice, incorporating NC measurement into routine physical examinations can significantly enhance the screening efficiency of OSA.
This study identified male gender as a significant risk factor (P < 0. 001), aligning with previous findings.25 The differences in fat distribution, upper airway structure, and hormone levels between men and women may contribute to this disparity.26,27 This study cohort revealed a higher percentage of males in the moderate to severe OSA group compared to females, further supporting this relationship. The mechanisms underlying gender differences may extend beyond traditional anatomical explanations. In addition to the known variations in upper airway structure, the regulatory role of gender hormones on respiratory control pathways must also be considered. Testosterone is believed to affect respiratory stability by altering the chemoreceptivity of the carotid body, offering a new physiological perspective for understanding the high incidence of OSA in men.28 Estrogen enhances the contraction of the genioglossus muscle, stabilizing the upper airway, while progesterone acts as a potent respiratory stimulant that significantly increases ventilation drive and counteracts hypercapnia.29 In addition, estrogen affects metabolism by regulating leptin sensitivity and reduces oxidative stress damage caused by intermittent hypoxia through antioxidant mechanisms. Together, these factors form a physiological protective barrier for premenopausal women.30
The nomogram model of moderate to severe obstructive sleep apnea constructed in this study has significant clinical advantages and practical value, but has certain limitations. Compared with the classical screening tools such as STOP-BANG and Berlin questionnaire, this nomogram only includes six routine clinical indicators, such as age, BMI, neck circumference, gender, hypertension and diabetes, which are easily available in primary care. It does not require professional equipment, complex calculation or subjective scoring, and can quickly quantify individual risk of disease in a visual and intuitive scoring way. The procedure is simpler and the results are more objective and accurate, especially suitable for rapid stratified screening in areas with limited medical resources. The model has been verified in and outside of a large sample with excellent discrimination efficiency and good fitting. It has been confirmed by decision curve analysis that it has clear net clinical benefit, which can more efficiently identify high-risk patients and guide accurate referral, making up for the shortcomings of traditional questionnaire’s unstable prediction efficiency and limited population applicability. However, this study still has limitations. As a single-center retrospective study, there is selection and information bias. The model was constructed only for the western Chinese population, and further validation is needed when extrapolated to populations in other regions. Moreover, sleep-related subjective symptoms and other indicators were not included, and the risk assessment dimensions were relatively limited.
In clinical application, the nomogram can be used as a primary screening tool to prioritize polysomnography for high-risk individuals, so as to optimize the allocation of medical resources and improve the early detection rate of moderate to severe OSA. In the future, multi-center prospective studies can be carried out to further improve the model and expand the applicable population.
In summary, the current study successfully developed and validated a feasible nomogram that demonstrates strong performance in predicting moderate to severe OSA risk in a western Chinese population by multivariate analysis. This tool offers valuable insights for predicting patients at risk for moderate to severe OSA.
Data Sharing Statement
The data presented in this article are available from the corresponding author upon reasonable request. The data are not publicly available due to privacy.
Ethics Approval and Participation Consent
The Ethics Committee of Xinjiang Uyhgur Autonomous Region Traditional Chinese Medicine Hospital passed on May 27, 2020, with certificate number 2020XE-GS003.All study procedures were conducted in strict accordance with the relevant ethical guidelines of the Declaration of Helsinki.The patients gave their written informed consent.
Author Contributions
Aman Gul: Conceptualization, Investigation, Writing-original draft;
Maimaiti Aili:Methodology; Conceptualization; Funding acquisition; Writing-original draft
Xuejiao Xie:Data curation; Investigation; Project administration; validation; visualization Ainiwaer Talifu:Formal analysis; Investigation; Supervision;
Fuxian Huang:Visualization; Formal analysis; conceptualization, methodology, supervision
Yilifanjiang Kuerban:Validation; Formal analysis, data curation
Zhijian Li:Conceptualization;Writing-original draft; Project administration, Supervision;Writing – review & editing
Jingcheng Dong:Conceptualization Writing-review&editing.
All authors took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Tianchi Talents Project of the Xinjiang Uyhgur Autonomous Region from department of Human Resources and Social Security of Xinjiang Uyhgur Autonomous Region. Supported by the Project for Cultivating Talents in Traditional Chinese Medicine-Special Project for Young Scientific and Technological Talents (grant numbers ZYQ2025018) from Administration of Traditional Chinese Medicine of Xinjiang Uyghur Autonomous Region.
Disclosure
The Authors have no conflicting interests relating to this work.
References
1. Tobias LA, Pisani MA. Sleep and sleep disorders in older adults. Clin Geriatr Med. 2025;41(4):569–11. doi:10.1016/j.cger.2025.07.010
2. Sun WL, Chen YH. Impact and management of comorbidities in patients with chronic obstructive pulmonary disease and obstructive sleep apnea. Zhonghua Jie He He Hu Xi Za Zhi. 2025;48(4):392–395. doi:10.3760/cma.j.cn112147-20250208-00071
3. Frosztega W, Sroczynski M, Michalek M, Wieckiewicz M, Madziarska K, Martynowicz H. Gallstones, obesity, insulin resistance, and obstructive sleep apnea - current knowledge on the topic: a literature review. Dent Med Probl. 2025;62(5):987–992. doi:10.17219/dmp/204402
4. Luong TV, Hoang TA, Tran DH, et al. Continuous positive airway pressure therapy for patients with obstructive sleep apnea and coronary artery disease. World J Cardiol. 2025;17(10):107750. doi:10.4330/wjc.v17.i10.107750
5. Hirani R, Smiley A. A scoping review of sleep apnea: where do we stand? Life. 2023;13(2):387. doi:10.3390/life13020387
6. Holfinger SJ, Lyons MM, Keenan BT, et al. Diagnostic performance of machine learning-derived OSA prediction tools in large clinical and community-based samples. Chest. 2022;161(3):807–817. doi:10.1016/j.chest.2021.10.023
7. Zhan X, Gao Y, Sun Z, et al. Screening obstructive sleep apnea in chinese adults: optimizing STOP-Bang and NoSAS cutoff values. Med Sci Monit. 2025;31:e947544. doi:10.12659/MSM.947544
8. Rani S, Gao EY, Ong JZE, et al. Multichannel machine learning for polysomnographic diagnosis of obstructive sleep apnea: a Bayesian meta-analysis. Eur Arch Otorhinolaryngol. 2025.
9. Munoz-Pindado C, Bonich-Juan R, Munoz-Pindado C, et al. Diagnostic utility of screening tools (Epworth scale, Berlin questionnaire, and STOP-Bang questionnaire) in moderate-to-severe obstructive sleep apnea supported by simple home-based diagnostic methods in primary care. Semergen. 2025;51(9):102581. doi:10.1016/j.semerg.2025.102581
10. Force USPST, Mangione CM, Barry MJ, et al. Screening for obstructive sleep apnea in adults: US preventive services task force recommendation statement. JAMA. 2022;328(19):1945–1950. doi:10.1001/jama.2022.20304
11. P. Chinese Elderly Type 2 Diabetes, G. Treatment of Clinical Guidelines Writing, E. Geriatric, S. Metabolism Branch of Chinese Geriatric, E.Geriatric,S. Metabolism branch of chinese geriatric health care, F. Geriatric Professional Committee of Beijing Medical Award, D. National Clinical Medical Research Center for Geriatric. Clinical guidelines for prevention and treatment of type 2 diabetes mellitus in the elderly in China (2022 edition). Zhonghua Nei Ke Za Zhi. 2022;61(1):12–50. doi:10.3760/cma.j.cn112138-20211027-00751
12. Johnson PA, Johnson JC. Enhancing hypertension diagnosis: embracing ambulatory monitoring for global standards. J Family Community Med. 2024;31(4):358–359. doi:10.4103/jfcm.jfcm_197_24
13. Sharma S, Stansbury R, Srinivasan P, et al. Early recognition and treatment of OSA in hospitalized patients and its impact on health care utilization in rural population: a real-world study. J Clin Sleep Med. 2024;20(8):1313–1319. doi:10.5664/jcsm.11146
14. Liu W, Sun X, Huang J, et al. Development and validation of a genomic nomogram based on a ceRNA network for comprehensive analysis of obstructive sleep apnea. Front Genet. 2023;14:1084552. doi:10.3389/fgene.2023.1084552
15. Haghighat S, Joghatayi M, Issa J, et al. Diagnostic accuracy of artificial intelligence for obstructive sleep apnea detection: a systematic review. BMC Med Inform Decis Mak. 2025;25(1):278. doi:10.1186/s12911-025-03129-x
16. Azarian M. Age matters: the differential impact of OSA on metabolic health by age group. J Clin Sleep Med. 2025;21(8):1335–1336. doi:10.5664/jcsm.11796
17. Kasmaoui FE, Abdelhafid B, Harsi EME, Mansoury O, Amine M. Prevalence of obstructive sleep apnea and its associated factors in primary health care in Morocco. Sleep Breath. 2024;28(5):1929–1937. doi:10.1007/s11325-024-03077-2
18. Yao X, Zhou K, Jiang W, Heizhati M, Tuerxun S, Wang L. Neck circumference predicts the incident cardiac events of obese hypertension with obstructive sleep apnea. Am J Prev Cardiol. 2025;23:101048. doi:10.1016/j.ajpc.2025.101048
19. Li S, Huang J, Xiao Z, Fan C. Advances in machine learning prediction models for the screening of obstructive sleep apnea in adults. Nat Sci Sleep. 2025;17:2575–2595. doi:10.2147/NSS.S526631
20. Titu IM, Vulturar DM, Chis AF, Oprea A, Manea A, Todea DA. Impact of obstructive sleep apnea in surgical patients: a systematic review. J Clin Med. 2025;14(14):5095. doi:10.3390/jcm14145095
21. Zhu Z, Wu Y, Qu L, et al. Evaluation of nocturnal apnea and airflow limitation as indicators for cognitive dysfunction in patients with chronic obstructive pulmonary disease/obstructive sleep apnea hypopnea syndrome overlap syndrome. Chron Respir Dis. 2024;21:14799731241236492. doi:10.1177/14799731241236492
22. Bellebe Y, Elie R. Poor developing country threatened. Haitian nurses and physicians in a battle against AIDS. Interview by Mats Ulbult. Sykepleien. 1987;74(17):22–27.
23. Nithitsutthibuta K, Sonsuwan N, Uthaikhup S, Kiatwattanacharoen S, Kunritt J, Pratanaphon S. Effects of obstructive sleep apnea on vascular structure and function in adults with obesity and type 2 diabetes: a comparative study. Cardiovasc Endocrinol Metab. 2025;14(3):e00342. doi:10.1097/XCE.0000000000000342
24. Oscullo G, Pengo MF, Gomez-Olivas JD, Lombardi C, Parati G, Martinez-Garcia MA. Refractory hypertension and obstructive sleep apnea. J Hypertens. 2025;43(12):1937–1944. doi:10.1097/HJH.0000000000004166
25. Gunes ZY, Gunaydin FM, Yildirim S. Comparisons of obstructive - central respiratory events with body mass index and neck-waist circumference measurements according to gender in patients with obstructive sleep apnea syndrome. Sleep Breath. 2025;29(6):330. doi:10.1007/s11325-025-03510-0
26. Braga PGS, Giampa SQC. Good night’s sleep, good arterial health: are there differences between men and women living with obstructive sleep apnoea? J Physiol. 2024;602(21):5973–5974. doi:10.1113/JP286370
27. Roger-Casals N, Munoz-Fernandez AM, Munoz-Pindado C. Differences in clinical profile between men and women with obstructive sleep apnoeas. Med Clin. 2025;165(1):106975. doi:10.1016/j.medcli.2025.106975
28. Li L, Xue W, Yang Q, et al. Multifactorial relationships among the waist-to-Hip ratio, insulin resistance, and obstructive sleep apnea in men: a large-scale cohort study. Nutr Metab. 2025;22(1):121. doi:10.1186/s12986-025-01020-0
29. Sung ER, Collop N. Obstructive sleep apnoea in women: what do we know and what don’t we know? Respirology. 2025;30(12):1127–1130. doi:10.1002/resp.70136
30. Dunietz GL, Chervin RD, Tauman R, Shaklai S, Sankari A. OSA in women: associations with reproductive aging and screening challenges. Chest. 2025.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.