Back to Journals » OncoTargets and Therapy » Volume 19
A Nomogram Integrating HOXA9 Expression and Clinicopathological Factors for Predicting Postoperative Recurrence in Gastric Cancer: A Single-Center Retrospective Study
Authors Weng J, Ying J, Xia M, Xie Y
Received 14 January 2026
Accepted for publication 27 May 2026
Published 6 June 2026 Volume 2026:19 596270
DOI https://doi.org/10.2147/OTT.S596270
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sanjay Singh
Jianze Weng,1 Jingwen Ying,1 Minming Xia,2 Yijie Xie3
1Department of Pharmacy, The Affiliated People’s Hospital of Ningbo University, Ningbo, Zhejiang, 315000, People’s Republic of China; 2Department of Gastrointestinal Minimally Invasive Surgery, The Affiliated People’s Hospital of Ningbo University, Ningbo, Zhejiang, 315000, People’s Republic of China; 3Department of Dermatology, The Affiliated People’s Hospital of Ningbo University, Ningbo, Zhejiang, 315000, People’s Republic of China
Correspondence: Jianze Weng, Department of Pharmacy, The Affiliated People’s Hospital of Ningbo University, No. 251 Baizhang East Road, Yinzhou District, Ningbo, Zhejiang, 315000, People’s Republic of China, Email [email protected]
Objective: To develop a nomogram integrating HOXA9 expression with clinicopathological indicators for predicting postoperative recurrence risk in gastric cancer.
Methods: This single-center retrospective study enrolled 152 gastric cancer patients who underwent radical surgery (June 2023–March 2024) with 18-month follow-up. Patients were divided into recurrence (n=58) and non-recurrence (n=94) groups. HOXA9 expression was assessed by immunohistochemistry. Clinicopathological parameters including age, gender, tumor size, location, differentiation, invasion depth, lymph node metastasis, TNM stage, vascular invasion, and perineural invasion were collected. Univariate and multivariate Cox regression and ROC analyses were used to identify independent risk factors and evaluate predictive value.
Results: The recurrence rate was 38.16%. The recurrence group had significantly larger tumor size, higher proportions of poor differentiation, lymph node metastasis, TNM stage III, vascular invasion, perineural invasion, and high HOXA9 expression (all P< 0.05). Multivariate Cox regression identified lymph node metastasis [HR=1.206 (1.042– 1.397)], TNM stage III [HR=1.598 (1.096– 2.328)], vascular invasion [HR=1.863 (1.093– 3.176)], and high HOXA9 expression [HR=2.076 (1.222– 3.525)] as independent risk factors (P< 0.05). The combined AUC was 0.798, significantly higher than each factor alone (Z=3.472– 3.305, all P< 0.01).
Conclusion: The model combining HOXA9 expression with TNM stage, lymph node metastasis, and vascular invasion demonstrates good performance in assessing postoperative recurrence risk and may serve as a practical tool for clinical risk stratification.
Keywords: gastric cancer, HOXA9, clinicopathological indicators, postoperative recurrence, risk prediction
Introduction
Gastric cancer is a highly prevalent malignant tumor of the digestive tract worldwide. Radical surgery is the preferred treatment for early and locally advanced gastric cancer; however, the postoperative recurrence rate remains as high as 30%-50%, and the five-year survival rate for patients with recurrence is less than 10%.1,2 Accurately predicting the risk of postoperative recurrence to implement intensified adjuvant therapy for high-risk patients and avoid overtreatment in low-risk patients is a core strategy for improving the prognosis of gastric cancer.3 In recent years, research on molecular prognostic markers has provided new directions for precision management of gastric cancer. As reviewed by Shi et al,4 although transcriptomics-based molecular subtyping can significantly improve prognostic prediction, its high cost and long turnaround time hinder routine clinical application. In contrast, protein markers detectable by immunohistochemistry, due to their simplicity, cost-effectiveness, and accessibility, remain the most clinically promising prognostic tools.
The homeobox (HOX) gene family encodes key transcription factors that regulate embryonic development and cellular differentiation, and their aberrant expression is closely associated with the occurrence and progression of various tumors. Homeobox A9 (HOXA9), a core member of the HOX gene family, plays a critical regulatory role in embryonic development and cellular differentiation. Recent studies have revealed that HOXA9 is aberrantly activated in multiple solid tumors, promoting tumor proliferation, invasion, and metastasis through pathways such as Wnt/β-catenin and PI3K/Akt.5 Previous research has confirmed the aberrant expression of HOXA9 in lung cancer, colorectal cancer, breast cancer, and other malignancies, where it is closely associated with tumor cell proliferation, invasion, and metastasis.6,7 In gastric cancer, HOXA9 overexpression has been linked to poor tumor differentiation, lymph node metastasis, and advanced TNM stage. However, its independent association with postoperative recurrence and predictive value remain controversial, and studies integrating HOXA9 into predictive models alongside clinicopathological parameters are lacking.8
Currently, the most commonly used tool for predicting gastric cancer recurrence is the TNM staging system, which relies solely on anatomical features and fails to distinguish recurrence risk among patients with the same stage but different molecular phenotypes, achieving an area under the curve (AUC) of only 0.6–0.7, indicating limited predictive efficacy.9 Although recent studies have developed predictive models incorporating molecular markers such as HER2 and PD-L1, the high cost and technical complexity of these assays limit their implementation in primary hospitals. In contrast, HOXA9 can be detected using routine immunohistochemistry, offering simplicity and cost-effectiveness suitable for widespread clinical application. Furthermore, postoperative adjuvant chemotherapy is a key measure to reduce the risk of recurrence in locally advanced gastric cancer; however, approximately 30% of patients with stage III disease still experience recurrence despite receiving standard adjuvant chemotherapy, underscoring the need for more precise biomarkers to identify truly high-risk populations.10 Based on these considerations, this study hypothesizes that high HOXA9 expression is an independent risk factor for postoperative recurrence of gastric cancer and that integrating HOXA9 with clinicopathological indicators can establish a more accurate predictive model for 18-month postoperative recurrence, thereby providing a novel basis for individualized clinical management.
Methods
Study Subjects
This retrospective cohort study included 152 gastric cancer patients who underwent radical surgery in the Affiliated People’s Hospital of Ningbo University from June 2023 to March 2024. Inclusion criteria: Age ≥18 years, regardless of gender; Postoperative histopathological confirmation of gastric adenocarcinoma; Indications for surgical treatment and voluntary acceptance of surgery; Complete clinicopathological data; Postoperative follow-up duration ≥18 months; Signed informed consent from the patient or family members. Exclusion criteria: Previous neoadjuvant radiotherapy, chemotherapy, targeted therapy, or immunotherapy; Concurrent other malignancies; Pathological types other than adenocarcinoma, such as squamous cell carcinoma, adenosquamous carcinoma, or neuroendocrine tumors; Preoperative imaging or intraoperative confirmation of distant metastasis; Loss to follow-up or missing key clinicopathological data during follow-up; Poor quality of tumor tissue samples, rendering them unsuitable for immunohistochemical testing. The study was approved by the Ethics Committee of the Affiliated People’s Hospital of Ningbo University (No.:2025–034) and informed consent was provided by all participants.
Experimental Methods and Observation Indicators
HOXA9 detection was performed using the immunohistochemical SP method. Postoperative paraffin-embedded tumor tissue samples from patients were collected, fixed in 4% paraformaldehyde for 24 hours, and then routinely processed through gradient dehydration, xylene clearing, and paraffin embedding. Continuous 4μm sections were mounted onto poly-lysine-coated slides and baked at 60°C for 2 hours for subsequent use. Experimental reagents included rabbit anti-human HOXA9 monoclonal antibody (Product # ab189730, Abcam, concentration 1mg/mL), SP immunohistochemistry kit (Product # PV-9000, Beijing Zhongshan Golden Bridge Biotechnology Co., Ltd)., DAB chromogen kit (Product: ZLI-9018, Beijing Zhongshan Golden Bridge Biotechnology Co., Ltd)., and citrate antigen retrieval solution (pH 6.0, Product: ZLI-9065, Beijing Zhongshan Golden Bridge Biotechnology Co., Ltd). The operating procedure strictly followed the instructions of the immunohistochemistry SP method kit. Result evaluation was performed by two pathologists, each with over five years of diagnostic experience, using a double-blind method and a semi-quantitative scoring system. The scoring criteria for the proportion of positive cells were: 0 points (<5%), 1 point (5–25%), 2 points (26–50%), 3 points (51–75%), and 4 points (>75%). The scoring criteria for staining intensity were: 0 points (no staining), 1 point (light yellow), 2 points (brown-yellow), and 3 points (brown). The total score was calculated as the product of the positive cell proportion score and the staining intensity score. A total score ≤ 3 was defined as low HOXA9 expression, and a score > 3 was defined as high HOXA9 expression. If the score difference between the two pathologists was >1 point, they jointly re-reviewed the slides to reach a consensus before recording the final result. The intraclass correlation coefficient (ICC) was used to assess inter-observer reliability, and the results showed an ICC of 0.89 (95% CI 0.83–0.93), indicating good inter-observer agreement.
Collection of Clinicopathological Indicators
Patient clinicopathological indicators were collected via the hospital electronic medical record system and pathology department information system. Indicators included age, gender, maximum tumor diameter, tumor location (gastric body, gastric antrum, other), differentiation degree (including well-differentiated, moderately differentiated, and poorly differentiated; well- and moderately-differentiated were combined into a high/moderate differentiation group, while poorly differentiated constituted a separate group), depth of invasion (categorized as T1–T2 or T3–T4 stages according to the AJCC 8th edition TNM staging criteria), lymph node metastasis [defined as present (number of metastatic lymph nodes ≥1) or absent (number of metastatic lymph nodes = 0) based on postoperative pathology reports], TNM stage (classified as stage I–II or stage III using the AJCC 8th edition gastric cancer staging criteria), presence of vascular invasion (defined as tumor cells invading blood or lymphatic vessels observed on pathological slides), and perineural invasion (defined as tumor cells invading gastric wall nerve fibers or plexuses).
Follow-Up Method
Postoperative follow-up was conducted using a combination of outpatient visits and telephone calls. Follow-ups were scheduled every 3 months in the first postoperative year and every 6 months in the second year. Follow-up content included detailed inquiry about patient symptoms, physical examination, gastroscopy, abdominal computed tomography (CT) scans, and tumor marker testing. The time of recurrence, recurrence sites, and survival status were recorded. The follow-up endpoint was set at 18 months post-surgery or the first confirmed recurrence. Based on the 18-month postoperative follow-up results, patients were divided into groups. The recurrence group was defined as patients with confirmed local recurrence, regional lymph node metastasis, or distant metastasis postoperatively via gastroscopy, abdominal CT, positron emission tomography-computed tomography (PET-CT), or pathological biopsy. The non-recurrence group was defined as patients with no evidence of the aforementioned recurrence events by 18 months post-surgery and no abnormal elevation of tumor markers.
Statistical Methods
Statistical analysis was performed using SPSS 26.0 software (IBM Corp., USA). For continuous variables, normality was first assessed using the Shapiro–Wilk test. Data conforming to a normal distribution were expressed as mean ± standard deviation (x±s), and comparisons between groups were performed using the independent samples t-test. Categorical data were expressed as number (percentage) [n(%)], and comparisons between groups were made using the χ2-test. Univariate and multivariate Cox proportional hazards regression models were used to analyze risk factors for postoperative recurrence of gastric cancer. Variables with P < 0.05 in the univariate analysis were included in the multivariate regression model. The variance inflation factor (VIF) was calculated for all included variables to exclude indicators with severe multicollinearity. Stepwise regression was applied to identify independent risk factors. The value of combined independent risk factors in predicting postoperative recurrence risk in gastric cancer patients was analyzed using receiver operating characteristic (ROC) curves and the area under the curve (AUC). A P-value < 0.05 was considered statistically significant. The event-per-variable ratio was 14.5:1, which exceeds the recommended minimum of 5–10 events per variable.
Results
Patient Baseline Characteristics and HOXA9 Expression
Among the 152 gastric cancer patients, 58 experienced recurrence within 18 months postoperatively (recurrence rate 38.16%). The recurrence group had significantly higher maximum tumor diameter, proportion of poor differentiation, lymph node metastasis rate, proportion of TNM stage III, rates of vascular invasion and perineural invasion, and rate of high HOXA9 expression compared to the non-recurrence group (all P < 0.05). There were no statistically significant differences between the two groups in terms of age, gender, tumor location, or depth of invasion (all P > 0.05), as shown in Table 1.
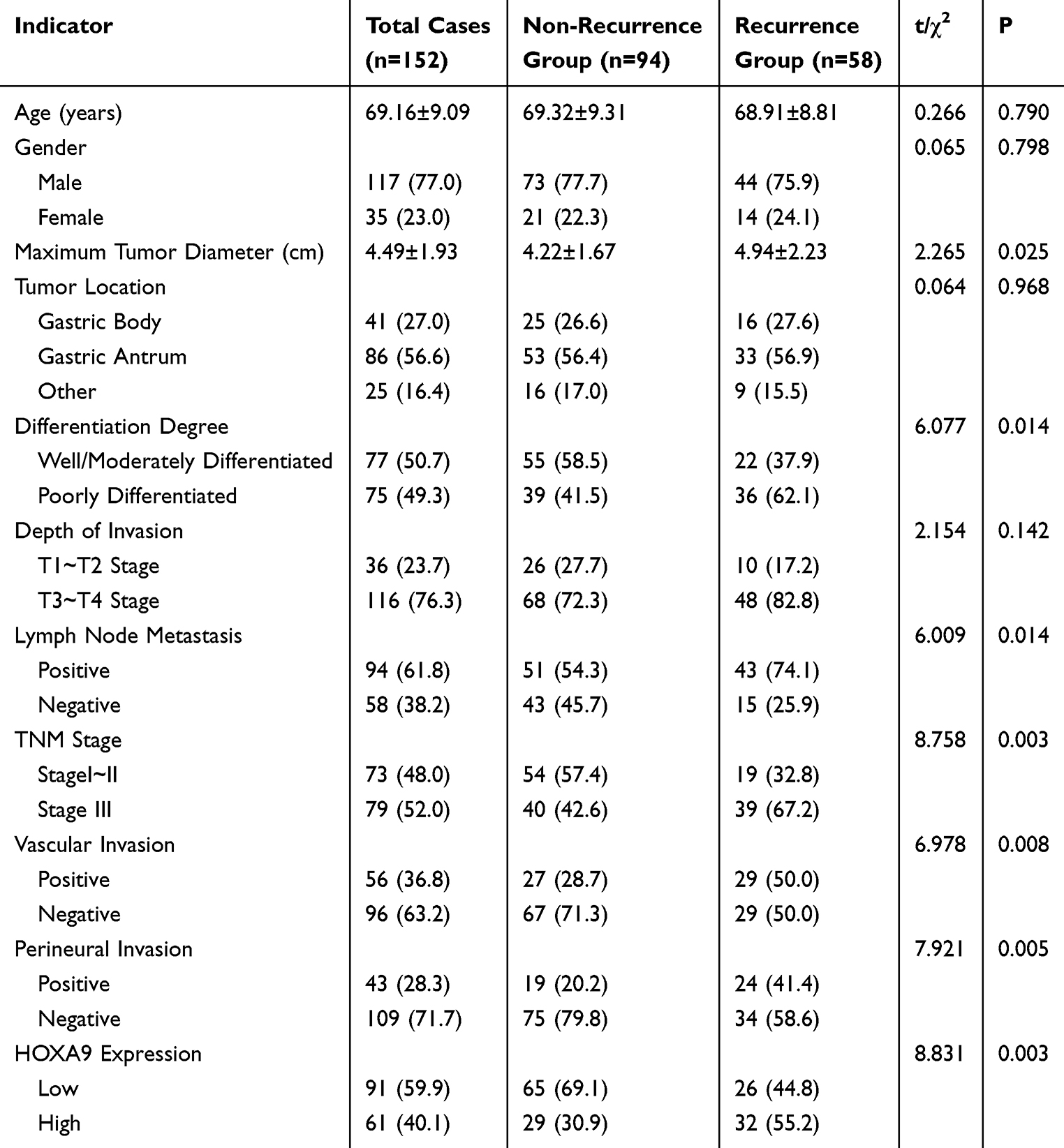 |
Table 1 Comparison of Baseline Characteristics and HOXA9 Expression Between the Two Groups [( |

Univariate and Multivariate Cox Regression Analysis of Risk Factors for Postoperative Recurrence in Gastric Cancer
The postoperative recurrence status of enrolled patients was set as the dependent variable, with assignments as follows: postoperative recurrence = 1, no postoperative recurrence = 0. Variables with P < 0.05 in intergroup univariate analysis were assigned as independent variables: maximum tumor diameter was assigned the original measured value, well/moderately differentiated = 0, poorly differentiated = 1, lymph node metastasis = 1, no lymph node metastasis = 0, TNM stage III = 1, TNM stage I–II = 0, vascular invasion = 1, no vascular invasion = 0, perineural invasion = 1, no perineural invasion = 0, high HOXA9 expression = 1, low HOXA9 expression = 0. Univariate Cox regression showed that maximum tumor diameter, poor differentiation, lymph node metastasis, TNM stage III, vascular invasion, perineural invasion, and high HOXA9 expression were all risk factors for postoperative recurrence in gastric cancer patients (P < 0.05), as shown in Table 2.
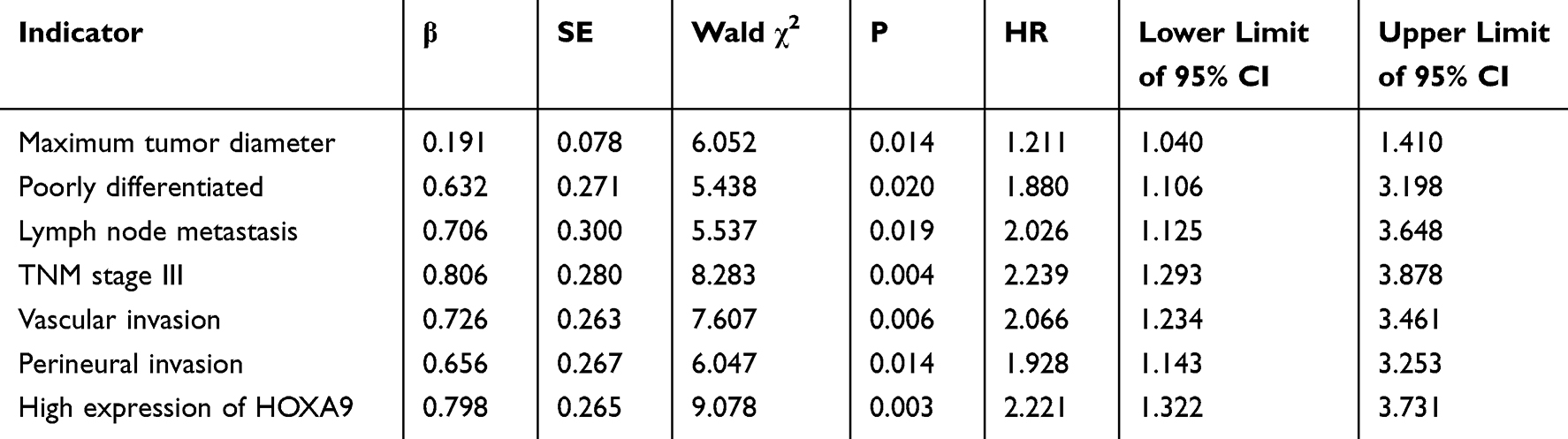 |
Table 2 Univariate Cox Regression Analysis of Risk Factors for Postoperative Recurrence in Gastric Cancer |
The VIF for all included variables was less than 2, indicating no severe multicollinearity among the potential influencing factors. Variables with P < 0.05 in the univariate Cox regression analysis were further included in the multivariate Cox regression analysis. The results indicated that lymph node metastasis [HR (95% CI) = 1.206 (1.042–1.397)], TNM stage III [HR (95% CI) = 1.598 (1.096–2.328)], vascular invasion [HR (95% CI) = 1.863 (1.093–3.176)], and high HOXA9 expression [HR (95% CI) = 2.076 (1.222–3.525)] were independent risk factors for postoperative recurrence (P < 0.05), as shown in Table 3.
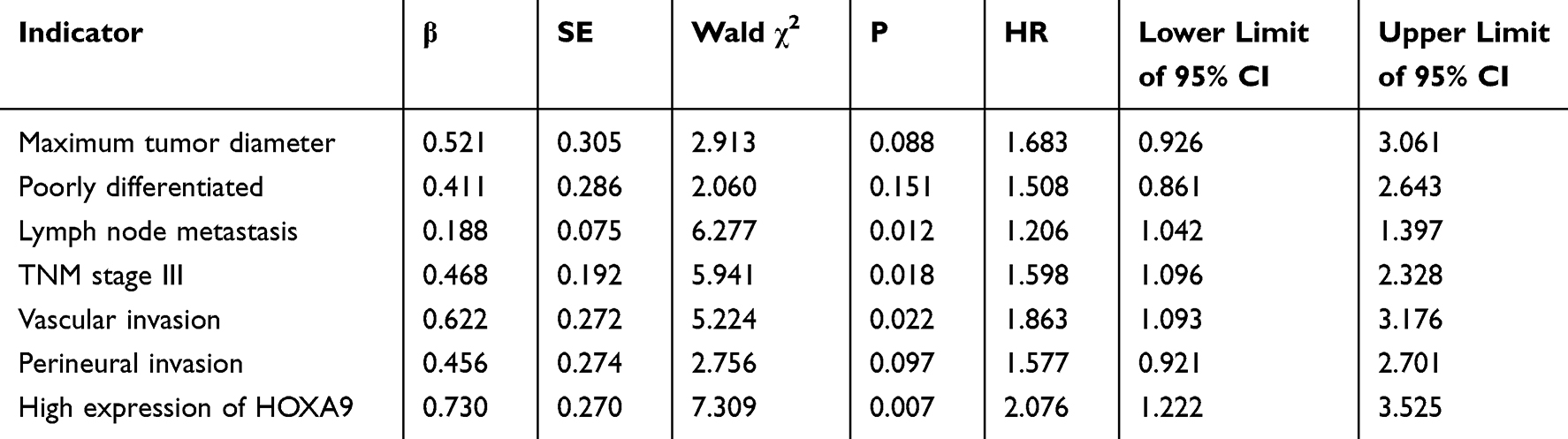 |
Table 3 Multivariate Cox Regression Analysis of Risk Factors for Postoperative Recurrence of Gastric Cancer |
Analysis of the Efficacy of Individual and Combined Risk Factors in Predicting Postoperative Recurrence Risk of Gastric Cancer
ROC analysis revealed that the AUCs for lymph node metastasis, TNM stage III, vascular invasion, and high HOXA9 expression—both individually and in combination—in predicting postoperative recurrence risk of gastric cancer were 0.599, 0.623, 0.606, 0.622, and 0.798, respectively. The predictive efficacy of the four factors combined was significantly higher than that of each factor alone (Z = 3.472, 2.938, 3.305, 2.899; P = 0.001, 0.003, 0.001, 0.004). At this point, the combined prediction demonstrated a sensitivity of 0.712, a specificity of 0.730, and a Youden index of 0.442, as shown in Table 4 and Figure 1. The bootstrap method with 1000 resampling iterations was used for internal validation. The results showed a corrected AUC of 0.776 (95% CI: 0.701–0.851), with a difference of less than 0.03 from the original AUC (0.798), indicating good model stability. The calibration curve demonstrated good agreement between predicted probabilities and actual recurrence probabilities (Hosmer-Lemeshow test: χ2 = 6.234, P = 0.621).
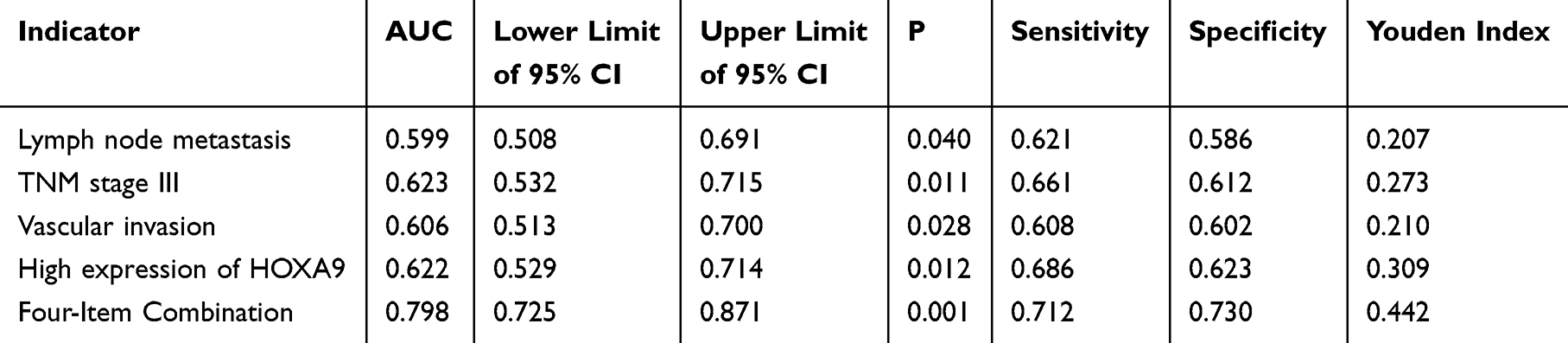 |
Table 4 Efficacy Analysis of Individual and Combined Risk Factors in Predicting Postoperative Recurrence Risk of Gastric Cancer |
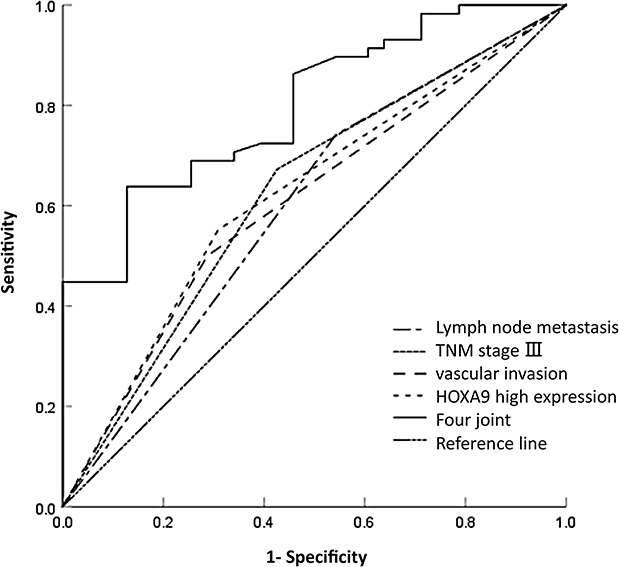 |
Figure 1 ROC analysis of independent and combined risk factors for predicting postoperative recurrence risk of gastric cancer. |
Discussion
This study, by integrating the molecular biomarker HOXA9 with clinicopathological indicators, confirmed that high HOXA9 expression combined with lymph node metastasis, TNM stage III, and vascular invasion significantly improves prediction accuracy, providing new evidence for the precise postoperative management of gastric cancer. As a core member of the homeobox gene family, the regulatory role of HOXA9 in tumorigenesis and progression has been confirmed in various solid tumors, but its specific mechanism and predictive value in postoperative recurrence of gastric cancer have not been fully elucidated.11,12 This study found that the high expression rate of HOXA9 in the gastric cancer recurrence group (55.17%) was significantly higher than in the non-recurrence group (29.79%), and it remained an independent risk factor for postoperative recurrence after multivariate adjustment, suggesting that high HOXA9 expression may be a key driver of gastric cancer progression and recurrence. HOXA9 can regulate the proliferation, invasion, and metastatic capabilities of gastric cancer cells through multiple signaling pathways: on one hand, HOXA9 can form heterodimers with PBX family proteins to activate the Wnt/β-catenin signaling pathway, promoting the expression of downstream target genes, accelerating tumor cell cycle progression, and enhancing proliferation activity;13 on the other hand, HOXA9 can inhibit tumor cell apoptosis by regulating the phosphorylation level of the PI3K/Akt pathway, while promoting the secretion of matrix metalloproteinases to degrade the extracellular matrix, thereby enhancing the invasive and metastatic capabilities of tumor cells.4 Furthermore, recent studies have confirmed that HOXA9 can participate in the epithelial-mesenchymal transition (EMT) process. By downregulating E-cadherin and upregulating N-cadherin and vimentin expression, tumor cells acquire a mesenchymal phenotype, making them more prone to breaking through the basement membrane barrier and leading to distant metastasis.14,15 This also explains why gastric cancer patients with high HOXA9 expression are more susceptible to postoperative recurrence.
This study also confirmed that lymph node metastasis, TNM stage III, and vascular invasion are independent risk factors for postoperative recurrence of gastric cancer. As a core indicator of gastric cancer staging, the presence of lymph node metastasis implies that tumor cells have acquired the ability for distant dissemination. Even after radical surgical resection, residual micrometastases may proliferate postoperatively, leading to recurrence.15 Patients with TNM stage III have deeper tumor infiltration, a broader scope of involvement, and a greater tumor burden. The probability of residual microscopic foci postoperatively is significantly higher than in stage I–II patients, which is the core reason for their increased recurrence risk.16 Vascular invasion indicates that tumor cells have invaded blood or lymphatic vessels, providing a direct pathway for distant metastasis. Previous studies have shown that gastric cancer patients with vascular invasion have an increased risk of distant metastasis and a significantly higher recurrence rate postoperatively.17 In this study, perineural invasion did not enter the final multivariate model, which may be related to sample size and follow-up duration. It also suggests that the predictive value of some clinicopathological indicators is diminished after integrating molecular biomarkers, further confirming the complementary roles of molecular biomarkers and clinicopathological indicators.
The combined prediction model integrating HOXA9 expression with clinicopathological indicators demonstrates significantly superior performance compared to any single indicator, highlighting the advantage of integrating molecular biomarkers with clinicopathological features. Traditional TNM staging only reflects the anatomical extent of the tumor and cannot distinguish the risk of recurrence among patients with different molecular phenotypes within the same stage.6 The AUC of the combined model in this study reached 0.798, which is significantly higher than the predictive efficacy of each individual indicator and is comparable to the performance of recently published gastric cancer recurrence prediction models incorporating multiple molecular biomarkers (AUC 0.75–0.82).16 Compared with other models, this model includes only one immunohistochemical indicator and three routine clinicopathological indicators, resulting in low detection costs and simple operation, making it potentially more suitable for promotion and application in primary hospitals. Furthermore, the findings of this study are mutually corroborated with previous related research while also exhibiting significant innovative aspects. The review by Tang et al5 pointed out that HOXA9 can serve as a biomarker of poor prognosis in solid tumors, but did not clarify its predictive value for postoperative recurrence of gastric cancer. The study by Bao et al6 confirmed that HOXA9 promotes proliferation and metastasis of hepatocellular carcinoma via the PI3K/Akt pathway, providing supporting evidence for the mechanistic analysis in this study. For the first time, this study integrates HOXA9 with clinicopathological indicators to construct a nomogram model for postoperative recurrence of gastric cancer, filling the research gap in the combined use of molecular biomarkers and clinical indicators to predict postoperative recurrence of gastric cancer.
The model constructed in this study can be used to assist clinical decision-making. For postoperative gastric cancer patients predicted by the model to be at high risk of recurrence, it is recommended to increase the frequency of postoperative follow-up from once every 3 months to once every 2 months. Routine contrast-enhanced abdominal CT and tumor marker testing should be performed at 6 and 12 months post-surgery, and PET-CT may be performed when necessary for early detection of recurrence. Additionally, targeted therapy or immunotherapy may be considered in combination with standard adjuvant chemotherapy to further reduce the risk of recurrence. For postoperative gastric cancer patients at low risk of recurrence, it is recommended to appropriately extend the follow-up interval to once every 4–6 months to avoid the medical burden and psychological stress associated with excessive testing.
However, this study has significant methodological limitations, and the results should be interpreted with caution. First, this was a single-center retrospective study, which may have introduced selection bias. Moreover, the study population was primarily from northern China, limiting the generalizability of the model. Second, the follow-up period was relatively short, assessing only early recurrence within 18 months post-surgery, and thus could not predict late recurrence risk beyond two years. In addition, adjuvant therapy status was not included as a covariate in the multivariate analysis. Adjuvant chemotherapy is a key factor influencing recurrence risk in patients with stage III gastric cancer, and its omission may have introduced confounding bias into the results. Furthermore, due to the limitations of the study design, no external validation of the developed prediction model was performed. The stability of the model was evaluated only through internal bootstrap validation, and its predictive performance in independent cohorts requires further validation. Additionally, the mRNA levels of HOXA9 and downstream signaling pathway molecules were not examined, and mechanistic analyses still need to be confirmed by basic experiments. These limitations suggest that the results of this study are preliminary and should not be used as the sole basis for clinical decision-making. Interpretation of the findings should be integrated with clinical guidelines, consensus, and real-world conditions.
Conclusion
In summary, this study confirms that high HOXA9 expression, lymph node metastasis, TNM stage III, and lymphovascular invasion are independent risk factors for 18-month postoperative recurrence in patients with gastric cancer. The prediction model incorporating these factors demonstrates good discrimination and stability. However, due to the limitations of a single-center retrospective design, a relatively short follow-up period, and lack of external validation, this model can currently serve only as a reference tool for preliminary clinical risk stratification. Its clinical utility requires further validation through multicenter, large-sample, prospective studies. Future research should adjust for the effect of adjuvant therapy and validate the generalizability of the model in independent cohorts, so as to provide higher-level clinical evidence for precision management of gastric cancer after surgery.
Data Sharing Statement
The data used to support the findings of this study are included within the article.
Ethics Statement
The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. The study was conducted in accordance with the Declaration of Helsinki (as revised in 2013). The study was approved by the Ethics Committee of the Affiliated People’s Hospital of Ningbo University (No.:2025-034) and informed consent was provided by all participants.
Funding
This research has received funding by the Yinzhou District Health Science and Technology Plan Project (NO.: 2025Y06) and the Zhejiang Provincial Science and Technology Plan for Disease Control and Prevention Project (NO.: 2025JK277).
Disclosure
The authors have no conflicts of interest to declare.
References
1. Yang WJ, Zhao HP, Yu Y, et al. Updates on global epidemiology, risk and prognostic factors of gastric cancer. World J Gastroenterol. 2023;29(16):2452–9. doi:10.3748/wjg.v29.i16.2452
2. Zheng C, Qian M, Huang T, et al. Exploring individualized follow-up of gastric cancer after radical surgery based on pTNM stage: a retrospective cohort study from China. Clin Med Insights Oncol. 2024;18:11795549241272654. doi:10.1177/11795549241272654
3. Yun JH, Choi YY, Cheong JH. The current evidence and future direction of adjuvant treatment for gastric cancer in the era of precision medicine. Cancer Res Treat. 2025;57(3):621–634. doi:10.4143/crt.2024.1222
4. Shi D, Yang Z, Cai Y, et al. Research advances in the molecular classification of gastric cancer. Cell Oncol. 2024;47(5):1523–1536. doi:10.1007/s13402-024-00951-9
5. Tang L, Peng L, Tan C, et al. Role of HOXA9 in solid tumors: mechanistic insights and therapeutic potential. Cancer Cell Int. 2022;22(1):349. doi:10.1186/s12935-022-02767-9
6. Bao G, Wei H, Yan J, et al. HOXA9 promotes proliferation, metastasis and prevents apoptosis in hepatocellular carcinoma. J Cancer Res Clin Oncol. 2024;150(9):422. doi:10.1007/s00432-024-05950-9
7. Watanabe Y, Saito M, Saito K, et al. Upregulated HOXA9 expression is associated with lymph node metastasis in colorectal cancer. Oncol Lett. 2018;15(3):2756–2762. doi:10.3892/ol.2017.7650
8. Ma YY, Zhang Y, Mou XZ, et al. High level of homeobox A9 and PBX homeobox 3 expression in gastric cancer correlates with poor prognosis. Oncol Lett. 2017;14(5):5883–5889. doi:10.3892/ol.2017.6937
9. Mantziari S, St Amour P, Abboretti F, et al. A comprehensive review of prognostic factors in patients with gastric adenocarcinoma. Cancers (Basel). 2023;15(5):1628. doi:10.3390/cancers15051628
10. Kanaji S, Suzuki S, Matsuda Y, et al. Recent updates in perioperative chemotherapy and recurrence pattern of gastric cancer. Ann Gastroenterol Surg. 2018;2(6):400–405. doi:10.1002/ags3.12199
11. Shenoy US, Adiga D, Alhedyan F, et al. HOXA9 transcription factor is a double-edged sword: from development to cancer progression. Cancer Metastasis Rev. 2024;43(2):709–728. doi:10.1007/s10555-023-10159-2
12. Jasim SA, Farhan SH, Ahmad I, et al. Role of homeobox genes in cancer: immune system interactions, long non-coding RNAs, and tumor progression. Mol Biol Rep. 2024;51(1):964. doi:10.1007/s11033-024-09857-z
13. LaRonde-LeBlanc NA, Wolberger C. Structure of HoxA9 and Pbx1 bound to DNA: hox hexapeptide and DNA recognition anterior to posterior. Genes Dev. 2003;17(16):2060–2072. doi:10.1101/gad.1103303
14. Shenoy US, Basavarajappa DS, Kabekkodu SP, Radhakrishnan R. Pan-cancer exploration of oncogenic and clinical impacts revealed that HOXA9 is a diagnostic indicator of tumorigenesis. Clin Exp Med. 2024;24(1):134. doi:10.1007/s10238-024-01389-x
15. Xu Q, Zhang Q, Dong M, et al. MicroRNA-638 inhibits the progression of breast cancer through targeting HOXA9 and suppressing Wnt/β-cadherin pathway. World J Surg Oncol. 2021;19(1):247. doi:10.1186/s12957-021-02363-7
16. Zhu Y, Chen H, Wu Y, et al. Novel nomogram and risk stratification for peritoneal recurrence after curative resection in gastric cancer. Sci Rep. 2024;14(1):19103. doi:10.1038/s41598-024-70349-y
17. Imai Y, Kurata Y, Ichinose M. Risk stratification for predicting postoperative recurrence of gastric cancer by grade of venous invasion. BMC Gastroenterol. 2023;23(1):189. doi:10.1186/s12876-023-02825-0
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Development of a Risk Prediction Model for Preoperative Pre-Frailty in Elderly Patients with Gastric Cancer
Yin C, Yin M, Zhen J, Xue C, Zhu Z
Clinical Interventions in Aging 2025, 20:2763-2772
Published Date: 28 December 2025