Back to Journals » Infection and Drug Resistance » Volume 16
A Nomogram for Predicting Delayed Viral Shedding in Non-Severe SARS-CoV-2 Omicron Infection
Authors Yu T ![]() , Dong J, Qi Q, Lv Q, Li J, Huang C, Cai X
, Dong J, Qi Q, Lv Q, Li J, Huang C, Cai X ![]()
Received 21 February 2023
Accepted for publication 19 April 2023
Published 27 April 2023 Volume 2023:16 Pages 2487—2500
DOI https://doi.org/10.2147/IDR.S407620
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Tianyu Yu,* Jiangnan Dong,* Qi Qi,* Qiang Lv, Jun Li, Chaojun Huang, Xiaoyan Cai
Department of General Surgery, Gongli Hospital of Shanghai Pudong New Area, Shanghai, 200135, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiaoyan Cai, Department of General Surgery, Gongli Hospital of Shanghai Pudong New Area, Shanghai, 200135, People’s Republic of China, Tel/Fax +86-21-58858730, Email [email protected]
Purpose: The Omicron variant of SARS-CoV-2 has emerged as a significant global concern, characterized by its rapid transmission and resistance to existing treatments and vaccines. However, the specific hematological and biochemical factors that may impact the clearance of Omicron variant infection remain unclear. The present study aimed to identify easily accessible laboratory markers that are associated with prolonged virus shedding in non-severe patients with COVID-19 caused by the Omicron variant.
Patients and Methods: A retrospective cohort study was conducted on 882 non-severe COVID-19 patients who were diagnosed with the Omicron variant in Shanghai between March and June 2022. The least absolute shrinkage and selection operator regression model was used for feature selection and dimensional reduction, and multivariate logistic regression analysis was performed to construct a nomogram for predicting the risk of prolonged SARS-CoV-2 RNA positivity lasting for more than 7 days. The receiver operating characteristic (ROC) curve and calibration curves were used to assess predictive discrimination and accuracy, with bootstrap validation.
Results: Patients were randomly divided into derivation (70%, n = 618) and validation (30%, n = 264) cohorts. Optimal independent markers for prolonged viral shedding time (VST) over 7 days were identified as Age, C-reactive protein (CRP), platelet count, leukocyte count, lymphocyte count, and eosinophil count. These factors were subsequently incorporated into the nomogram utilizing bootstrap validation. The area under the curve (AUC) in the derivation (0.761) and validation (0.756) cohorts indicated good discriminative ability. The calibration curve showed good agreement between the nomogram-predicted and actual patients with VST over 7 days.
Conclusion: Our study confirmed six factors associated with delayed VST in non-severe SARS-CoV-2 Omicron infection and constructed a Nomogram which may assist non-severely affected patients to better estimate the appropriate length of self-isolation and optimize their self-management strategies.
Keywords: SARS-CoV-2, COVID-19, Omicron, viral shedding time, nomogram
Introduction
Coronavirus disease 2019 (COVID-19) is an emerging and rapidly evolving global pandemic caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2).1 Among the various variants of SARS-CoV-2, the Omicron variant, first identified in South Africa on November 22, 2021, has emerged as a major concern due to its increased transmissibility, estimated to be 37.5% higher than the Delta variant.2,3 This variant has become the dominant strain in many parts of the world, accounting for approximately 99% of global gene sequencing data up to March 2022.4 In China, the Omicron variant was first detected on December 9, 2021, and rapidly spread in Shanghai by the end of February 2022.5 The Omicron variant in Shanghai belongs to the BA.2.2 sub-lineage. Although the Omicron variant generally induces milder acute disease manifestations in comparison to earlier variants, it possesses in excess of 30 mutations within the spike protein, enhancing its transmissibility and ability to evade the immune system.6,7
To date, several studies have investigated the relationships between clinical features and the virological course in persistently positive patients infected with SARS-CoV-2 original strain. Lee et al8 examined 1186 non-severe COVID-19 patients in Korea from Feb 21 to Apr 29, 2020, and found that respiratory symptoms were the most significant independent predictor of longer viral shedding time (VST), while age had no significant correlation. However, Hu et al9 supported that elderly and chest tightness were independent factors for delayed VST among hospitalized COVID-19 patients in China between Jan 29, 2020, and March 12, 2020. With the emergence of the Omicron variant, several recent studies have shed light on the unique clinical features of patients infected with this variant. For example, Saxena et al10 analyzed the transmission dynamic, effects on testing and immunity response of Omicron infection in a global perspective. Zhang et al11 confirmed that the number of inoculations and the Ct value of the SARS-CoV-2 ORF1ab gene were independently associated with prolonged Omicron VST. These well-designed studies have focused on the association between patient symptoms and prolonged Omicron VST. However, it remains unclear whether routine laboratory tests, such as hematological and biochemical parameters, are specific risk factors for delayed Omicron VST, and few studies have focused on this area.
The duration of self-isolation for people with COVID-19 varies depending on their level of infectiousness. With the increasing prevalence of the Omicron variant globally, numerous countries have adjusted their recommended quarantine periods for individuals infected with the virus. In August 2022, the US Centers for Disease Control and Prevention revised its guidelines, recommending a 5-day self-isolation period for individuals with COVID-19 and a 10-day period for those experiencing moderate or severe symptoms.12 In September 2022, Japan shortened the quarantine duration for symptomatic infected individuals from 10 days to 7 days, and for asymptomatic patients from 7 days to 5 days.13 Nonetheless, a Japanese study conducted in January 2022 on the Omicron variant revealed that 11.1% of infected individuals could still shed the virus after 7-day infection.14 Given the high transmissibility of the Omicron variant, ending isolation prematurely may pose a risk of exposing others to COVID-19 infection. Identifying risk factors for the duration of Omicron viral shedding is crucial in determining the appropriate patient self-isolation period and plays a vital role in controlling virus transmission.
Between March and May 2022, Shanghai witnessed a significant influx of SARS-CoV-2 Omicron variant cases. Within the context of the Chinese healthcare system, a policy emphasizing extensive patient admission and tailored treatment provision facilitated access to specialized care for numerous individuals, including those with mild symptoms. Given that most patients infected with Omicron variant do not present with severe symptoms, we focused on non-serious cases in order to explore risk factors for prolonged virus shedding. In this study, we aimed to identify easily accessible factors from routine laboratory tests that were associated with the duration of virus shedding in patients with COVID-19 caused by the Omicron variant. We used a retrospective cohort study design and employed statistical techniques such as least absolute shrinkage and selection operator (LASSO) regression model and multivariate logistic regression analysis to identify independent predictors of prolonged viral shedding. In light of numerous countries implementing an approximate 7-day isolation period for Omicron-infected patients, we also developed a nomogram for predicting the risk of virus shedding over than 7 days. Our study may help non-severely affected patients in enhancing their self-management strategies.
Materials and Methods
Patients
A total of 1235 Patients infected with SARS-CoV-2 Omicron diagnosed according to the the ninth version of Chinese guidelines for the diagnosis and treatment of COVID-1915 in Shanghai Pudong New Area Gongli Hospital, between April 13, 2022, and June 1, 2022, were available to enroll this retrospective study. All patients underwent hematological tests upon admission. The COVID-19 diagnosis was confirmed using transcriptase-polymerase chain reaction (RT-PCR) assay performed by the Laboratory of the Shanghai Pudong New Area Gongli Hospital, using a commercial kit (Yeason, China). The cycle threshold (Ct) values of SARS-CoV-2 ORF1ab and N genes < 35 were considered as a positive RNA test. If the result was negative (Ct ≥ 35), duplicate tests were performed at 24 hours.
The evaluation of a patient’s condition severity was also conducted in accordance with the ninth version of Chinese guidelines for the diagnosis and treatment of COVID-19.15 Patients classified as non-severe, based on a positive nucleic acid test result, were also required to present with at least one of the following Omicron infection manifestations: fever, dry cough, fatigue, nasal congestion, runny nose, sore throat, conjunctivitis, myalgia, diarrhea or radiographically-confirmed pneumonia. Throughout the disease course, patients were excluded if they exhibited any of the following severe clinical manifestations at any point: (1) tachypnea, characterized by a respiratory rate (RR) ≥ 30 breaths/min; (2) a resting oxygen saturation ≤ 93% while breathing room air; (3) an arterial partial pressure of oxygen (PaO2) to fractional inspired oxygen (FiO2) ratio ≤ 300 mmHg; or (4) progressive clinical deterioration, accompanied by pulmonary imaging indicative of lesion advancement exceeding 50% within a 24- to 48-hour period. Additionally, patients were also excluded if they met any of the following criteria: (1) younger than 18 years of age; or (2) possessing incomplete demographic, clinical, or epidemiological data. Finally, a total of 882 non-severe COVID-19 patients were included for further analysis. In addition, eight types of comorbidities were evaluated, including hypertension, diabetes, tumor, cardiovascular disease (such as rheumatic heart disease, coronary heart disease, atrial fibrillation, and cardiac insufficiency), respiratory disease (including bronchiectasis, bronchitis, chronic obstructive pulmonary disease, emphysema and asthma), rheumatic immune disease (like systemic lupus erythematosus and rheumatoid arthritis), hepatic disease (including fatty liver, hepatitis B, and liver cirrhosis) and Chronic kidney disease (CKD). Patients were then classified into comorbidity < 3 or comorbidity ≥ 3 based on the number of comorbidities.
Statistical Analysis
All enrolled 882 patients were randomized into training (70%, n = 618) and validation (30%, n = 264) cohorts to develop nomogram and perform internal validation. Given the number of events available, careful selection of variables was performed, considering clinically relevant hematological characteristics, liver and kidney function, as well as variables reported in previous studies with clinical significance. In total, 19 variables were incorporated into our study. For baseline analysis of patients, categorical variables were expressed as frequencies and percentages, and data were compared using chi-square test or Fisher’s exact test, while continuous data were expressed as median (interquartile range, IQR) and significant of differences were analyzed by Kruskal–Wallis test. Among the 19 variables incorporated, 14 were continuous variables. To pinpoint the most pertinent predictors, these continuous variables were further screened using LASSO regression. Employed as a regularization technique and chosen based on the minimum and 1-SE criteria, LASSO regression aimed to enhance the accuracy and interpretability of the regression models.16–18 To prevent over-fitting and increase model robustness, multivariate models were performed with substantiated 10-fold cross-validation and bootstrapping (1000 re-sampling).18 Restricted cubic spline (RCS) fits were performed on filtered continuous variables to test whether the nonlinear components were statistically significant.19 If nonlinearity was detected, the segmented regression was performed to fit a piecewise-linear relationship between continuous variables and odds of virus shedding at 7 days, and the threshold inflection point was calculated using a recursive algorithm.20 Then, the multivariate logistic regression was conducted to identify the risk factors for viral clearance. A nomogram was constructed based on statistically significant factors identified by multivariate analyses, using logistic regression to predict odds of virus shedding at 7-day. Both the training and validation cohort models were used to verify the effectiveness of nomogram. The discriminative ability of nomogram was assessed by the area under the curve (AUC) from receiver operating characteristic (ROC) curves, and the coincidence between the actual outcomes and the predicted probabilities was estimated by calibration curves using a bootstrap method with 1000 resamples.21 The prediction falling on the 45° diagonal in the calibration curve represents the most desirable case.
All analyses were conducted using R software Version 4.2.1 and the following R packages: “caret” for building training and validation cohorts, “glmnet” for LASSO regression, “rms” for RCS fits, “riskRegression” and “pROC” for generating ROC and calibration curves. A two-tailed P-value of less than 0.05 was considered statistically significant.
Results
Baseline Characteristics of Patients Infected with SARS-CoV-2 Omicron
A total of 1235 people were diagnosed with COVID-19 caused by the Omicron variant, of which 882 were included in the final analysis. The flow diagram of patient selection is detailed in Figure 1. The training and validation cohorts were found to be similar in most baseline characteristics, including SARS-CoV-2 nucleic acid test results at day 7, indicating that the groups were evenly distributed and suitable for internal verification (Table 1). As shown in Table 2, the baseline clinical features of the included patients were analyzed, with 45.35% of patients (n = 400) having detectable levels of viral RNA in their samples for at least 7 days, while 54.65% (n = 482) had negative results for viral detection over a period of less than 7 days. The average age of the patients was 66.43±18.53 years, and 427 of them (48.41%) were male. Approximately half of the patients (57.03%, 503/882) had abnormal chest CT scans indicative of viral pneumonia. The majority of the enrolled patients (60.32%, 532/882) were unvaccinated, while 20.75% (183/882) had received one or two doses of a vaccine and 18.93% (167/882) had received a third booster dose. Of all participants, 43.99% (388/882) of the patients had no comorbidities, while 4.20% (37/882) had more than three. None of the patients died during their hospitalization.
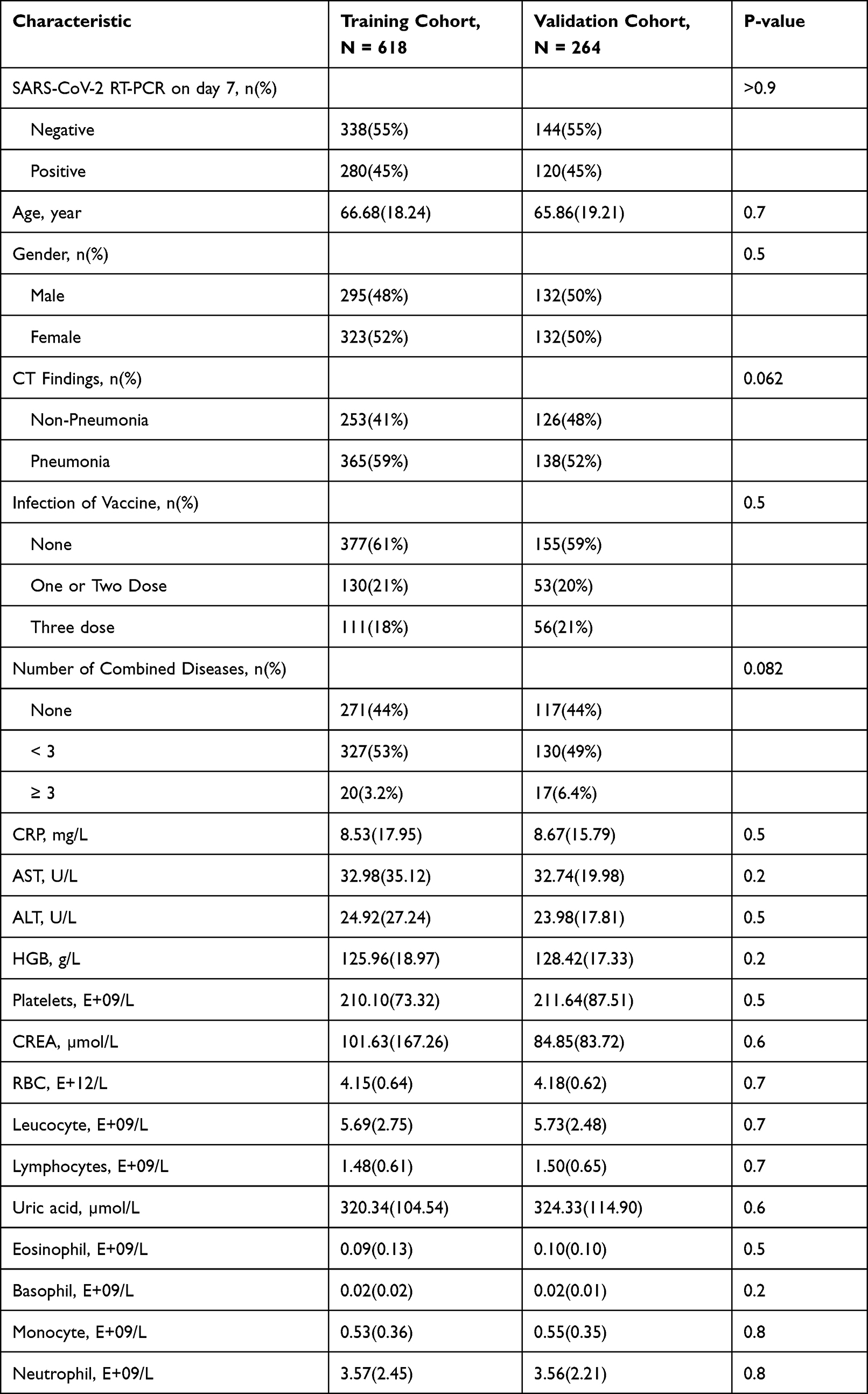 |
Table 1 Demographic Characteristics of Training Cohort and Validation Cohort |
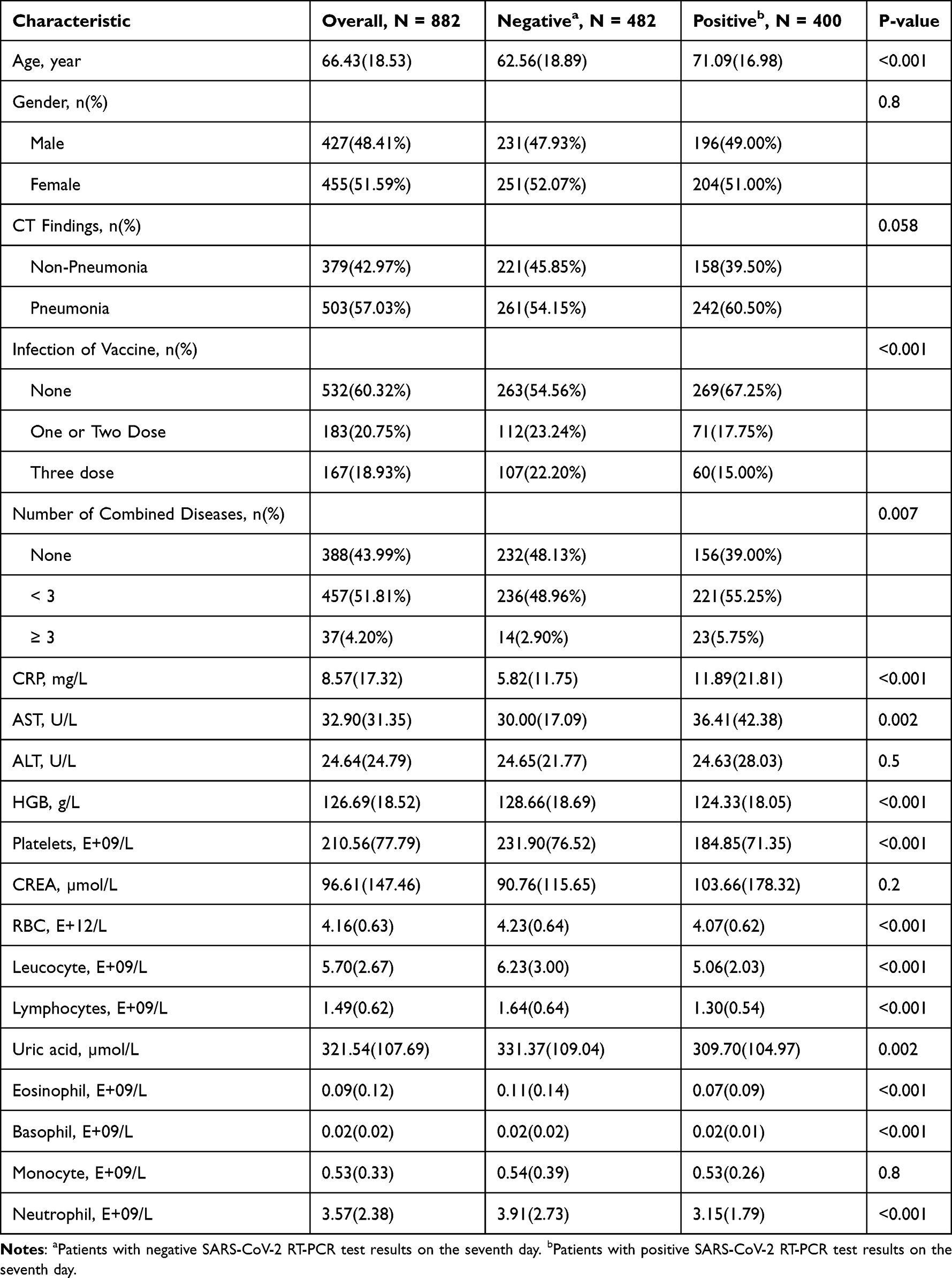 |
Table 2 Baseline Clinical Features of Patients with and without SARS-CoV-2 on Day 7 |
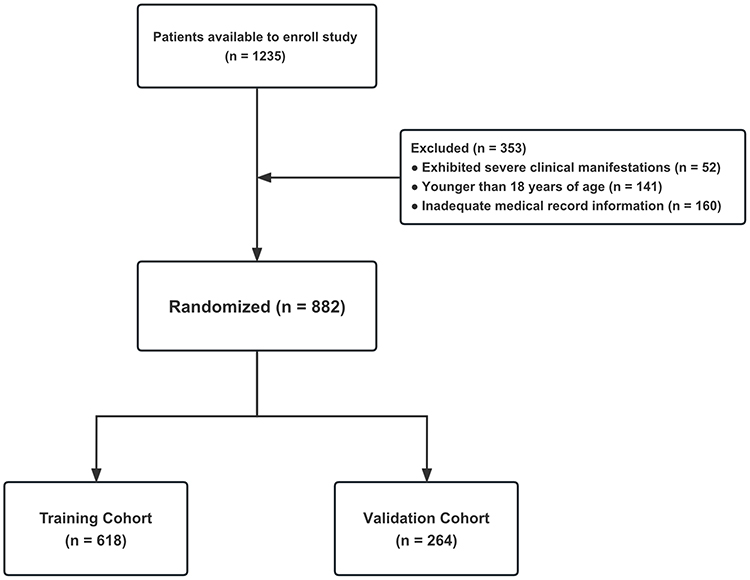 |
Figure 1 Flow diagram of patient selection. Among the 1235 patients, 52 were classified as presenting with severe COVID-19 upon admission or throughout the progression of their illness. Furthermore, 141 were minors under the age of 18 years, and 160 individuals possessed insufficient medical records. Finally, a cohort of 882 patients was incorporated into this study and stratified into the training cohort (n=618) and validation cohort (n=264) randomly. |
RCS Analysis of Nonlinear Associations Determined the Cutoff Values of Optimal Variables Reselected by LASSO Regression
The LASSO regression analysis indicated that the residual sum of squares was minimized at a lambda value of 0.04373 and log (λ) value of −3.147. Utilizing this information, seven optimal variables were identified as being predictive of the risk of VST > 7 days, including Age, C-reactive protein (CRP), as well as the counts of Platelets, Leucocyte, Lymphocytes, Eosinophil, and Basophil (Figure 2). Subsequently, a restricted cubic spline (RCS) regression model was employed to evaluate the nonlinearity relationships between each of the optimal variable and the risk of VST > 7 days. As shown in Figure 3, all seven variables were found to exhibit a nonlinear association with risk (with P values for nonlinearity < 0.001). These plots demonstrate a significantly lower risk at lower predicted values of Age and CRP, and at higher predicted values of platelet, leucocyte, lymphocyte, eosinophil, and basophil counts. The threshold inflection points were calculated using a recursive algorithm, indicating a clear increased risk when age > 68 years, CRP > 3.38mg/L, platelets < 205 E+09/L, leucocyte < 5.2 E+09/L, lymphocytes < 1.4 E+09/L, eosinophil < 0.06 E+09/L and basophil < 0.02 E+09/L.
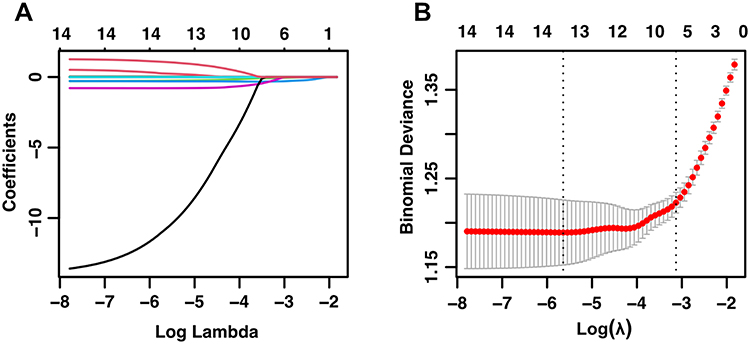 |
Figure 2 The selection of optimal variables for the model was carried out using LASSO regression. (A) LASSO model coefficient trendlines of the 14 variables for risk of SARS-Cov2 RNA positivity lasting longer than 7 days. (B) Tuning parameter (Lambda, λ) selection cross-validation error curve. Vertical lines were drawn at the optimal values given minimum criteria and 1-SE criteria, resulting in λ = 0.04373 and the optimization of six non-zero coefficients. Abbreviation: LASSO, Least absolute shrinkage and selection operator. |
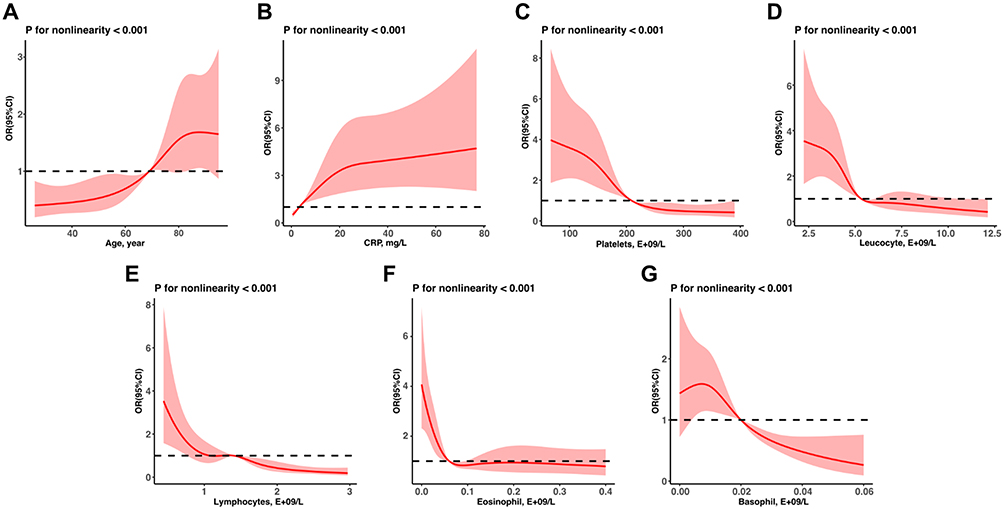 |
Figure 3 RCS mode evaluates the non-linearity relationship of age (A), CRP levels (B) and counts of platelets (C), leukocytes (D), lymphocytes (E), eosinophils (F) and basophils (G) to risk of SARS-Cov2 RNA positivity lasting longer than 7 days. Abbreviations: RCS, Restricted cubic spline; CRP, C-reactive protein. |
Univariate and Multivariable Logistic Regression for Optimal Variables
In order to further verify the association between the optimal variables identified by the LASSO regression and the outcome of interest, univariate and multivariable logistic regression analysis were conducted. The results of multivariable logistic regression, as presented in the Table 3, indicate that age greater than 68 years (odds ratio [OR]: 2.03; 95% confidence interval [CI]: 1.29–3.19; P = 0.002), CRP greater than 3.38 mg/L (OR: 2.27; CI: 1.56–3.32; P < 0.001), platelets less than 205 E+09/L (OR: 2.04; CI: 1.39–2.99; P < 0.001), leucocyte less than 5.2 E+09/L (OR: 2.1; CI: 1.42–3.11; P < 0.001) and eosinophil less than 0.06 E+09/L (OR: 1.95; CI: 1.33–2.85; P < 0.001) were found to be independently associated an increased risk of SARS-CoV-2 RNA positivity on day 7. These findings provide further evidence for the predictive value of these variables in identifying individuals with delayed viral clearance.
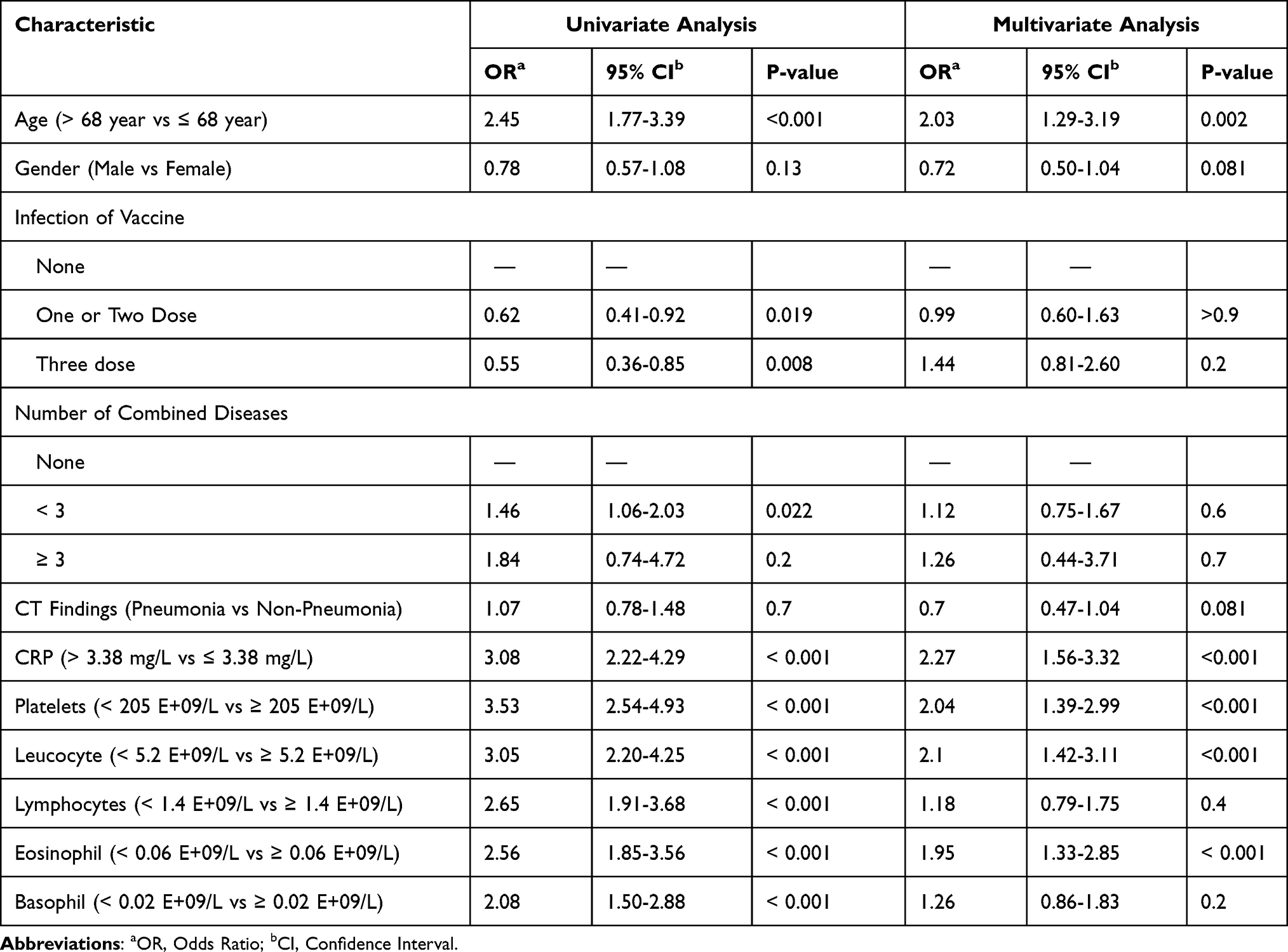 |
Table 3 Univariate and Multivariate Logistic Regression Analyses for Risk Factors of SARS-CoV-2 RNA Positivity Lasting Longer Than 7 Days in Training Cohort |
Construction and Validation of the Nomogram for Risk of SARS-CoV-2 RNA Positivity Lasting Longer Than 7 Days
Based on the results of the multivariate logistic regression analysis, a nomogram was developed to predict the risk of VST > 7 days. As shown in Figure 4, the nomogram incorporates six variables, with each clinical factor corresponding to a specific point value plotted on the Points axis. The total points can be calculated by summing these point values, and the corresponding probability of SARS-CoV-2 RNA positivity lasting longer than 7 days can be estimated by drawing a line straight down from the Total Points value to the Risk axis. The Nomogram was validated using both a training cohort and a validation cohort. The AUC for the Nomogram in the training cohort was 0.761 (95% CI: 0.724–0.799) and in the validation cohort was also high at 0.756 (95% CI: 0.697–0.816), indicating the Nomogram’s good discriminative ability (Figure 5A and C). Furthermore, in both the training and validation cohorts, the predicted viral shedding probability at 7 days closely matched the observed results, indicating a good calibration (Figure 5B and D).
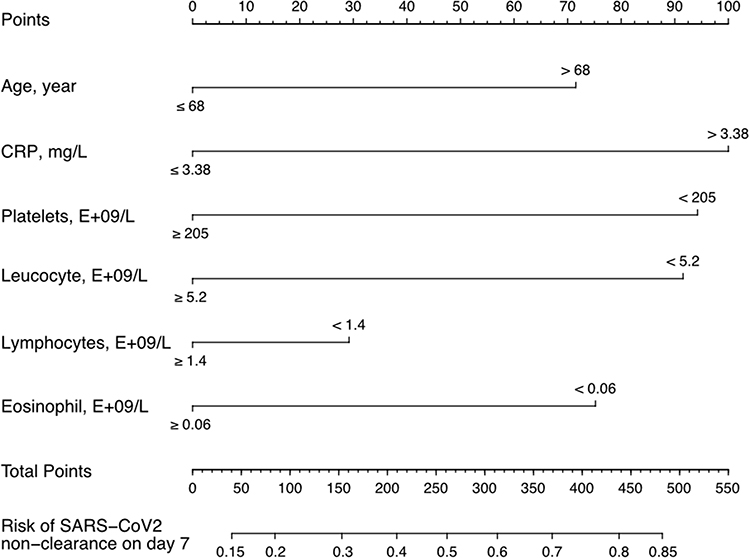 |
Figure 4 Nomogram to predict the probabilities of viral shedding at 7 days. For each clinicopathological factor, find the corresponding point by drawing a vertical line from that variable to the points axis. The sum of each variable score corresponds to probability of viral shedding at 7 days. |
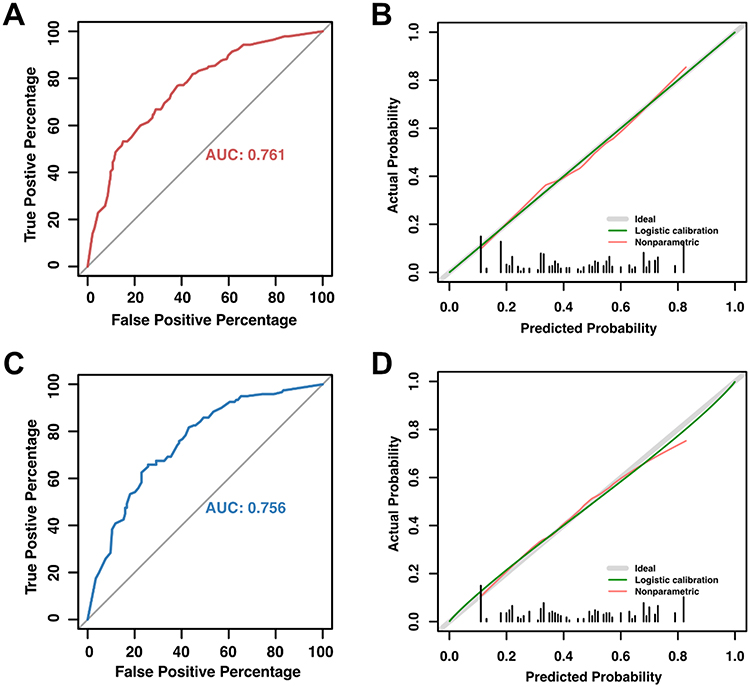 |
Figure 5 AUC curve and calibration plot of the nomogram for the risk of SARS-Cov2 RNA positivity lasting longer than 7 days. (A) The area under ROC curve (0.761, 95% CI: 0.724–0.799) was utilized to assess the accuracy of nomogram. (B) Calibration plot for judging the prediction of nomogram. The red line denotes bias, while the green diagonal line at a 45-degree angle represents perfect prediction. The nomogram is thought to be more reliable the closer these two lines are to one another. (C) The area under ROC curve (0.756, 95% CI: 0.697–0.816) of validation cohort. (D) Calibration plot for nomogram in validation cohort. Abbreviations: ROC, receiver operating characteristic curve; AUC, area under the curve. |
Discussion
The duration of viral shedding is important factor affecting the spread and transmission of the virus. Previous studies have investigated factors that may influence the duration of viral shedding in SARS-CoV-2, including the Alpha and Delta variants.22–27 However, there is currently a lack of models for predicting viral shedding time (VST) in the Omicron variant. In our study, we identified six factors - age, CRP, platelet count, leukocyte count, lymphocyte count and eosinophil count - that are readily amenable to laboratory investigation and associated with the duration of SARS-CoV-2 Omicron viral shedding in non-serious cases.
In this work, we found that individuals over the age of 68 are at an increased risk for extended viral shedding of the SARS-CoV-2 Omicron strain, which might be attributed to age-related changes in the immune system, such as decreased production of type I interferon, which in turn leads to an imbalance between M1 and M2 macrophages and impair natural killer cell activity, resulting in reduced virus clearance.28 According to an in vitro study, the Omicron virus can efficiently replicate to high titers in Angiotensin-converting enzyme 2 (ACE2) receptor-overexpressed cell lines,29 and the upregulation of ACE2 receptors in respiratory tract of elderly people may allow for more rapid virus replication.30,31 Furthermore, older individuals may have a lower tolerance for increased inflammation and pro-inflammatory cytokine production, which can result in cytokine storms.28 These factors may all contribute to slower viral clearance in older patients with Omicron infection.
Our study also revealed the impact of CRP upregulation on Omicron viral clearance. CRP is a pentameric protein produced in the liver in response to inflammation, primarily induced by interleukin-6 (IL-6). It is critical for the recognition and removal of foreign pathogens.32 In COVID-19 patients, high CRP levels have been linked to an increased risk of rapid progression to critical illness and in-hospital mortality. A retrospective analysis of 429 patients found that those with CRP levels higher than 64.75 mg/L were more likely to suffer severe complications.33 Similarly, CRP levels above 108mg/L were associated with disease severity and higher mortality in a cohort study of 2782 COVID-19 patients.34 A 1035-patient retrospective research also revealed that COVID-19 patients were more likely to experience a severe form of the illness if their CRP level was beyond 100 mg/L.35 Patients infected with the Omicron generally have lower CRP levels compared to those infected with the SARS-CoV-2 original strain.36 Additionally, there is no statistical difference in CRP levels between Omicron-infected patients and non-Omicron infected febrile patients.37 But interestingly, our study revealed that Omicron-infected patients had a considerably higher risk of delayed viral clearance even with mildly raised CRP levels (above 3.38 mg/L). Despite being a non-specific biomarker of inflammation, CRP is advantageous as a prognostic factor due to its wide availability and frequent testing compared to other biomarkers.
According to our study, SARS-CoV-2 Omicron-infected patients with low levels of certain hematological cells, including platelets, leukocytes, lymphocytes, and eosinophils, were at higher risk for slower viral clearance. A significant increase in risk is observed when these indicators drop below a certain threshold. While platelet counts are usually within normal range and severe thrombocytopenia is rare,38 the thrombocytopenia was common in patients with severe COVID-19 and was associated with a higher mortality rate.38–40 Despite differing reports on the direct interactions between SARS-CoV-2 and platelets, majority of studies agree that platelets are activated during COVID-19 and some of them further found viral RNA in platelets.41 The immune system’s response to viral infection, including the formation of microthrombi following cytokine storm, can lead to increased platelet depletion, and the activation of immune system can cause an antibody-mediated phagocytic response that increases platelet clearance,42,43 both contributing to thrombocytopenia in COVID-19 patients. This change in platelet counts appears to be specific to SARS-CoV-2 infection and has not been observed with other coronavirus strains.44 Collectively, these studies highlight the potentially intricate and crucial role of platelets during the progression of SARS-CoV-2 infection. In our study, we discovered that patients exhibiting lower platelet levels upon admission experienced protracted viral clearance times. This observation may suggest a correlation between platelet counts and the efficiency of viral clearance. Nevertheless, the exact interaction between SARS-CoV-2 (especially the Omicron strain) and platelets remains unclear and requires further study.
Lymphopenia may be caused by a reduction in CD4+ and some CD8+ T cells, upsetting the equilibrium between the innate and acquired immune systems.45 It has been noted that critically ill COVID-19 patients frequently experience a large drop in lymphocyte count.46 Direct infection of lymphoid organs,47 cytokine storm,48 metabolic disorders,49,50 epigenetic alteration and dysfunction of lymphocytes,51,52 and expression alteration of genes involved in lymphocyte proliferation and apoptosis53,54 may be the mechanisms underlying lymphopenia in COVID-19 patients. Although lymphocytes play an important role in the process of SARS-CoV-2 infection, in one study involving 31 patients infected with the SARS-CoV-2 original strain, no relationship was found between the viral shedding period and the duration of lymphopenia.55 But our investigation demonstrated that patients with low baseline lymphocyte counts during SARS-CoV-2 Omicron infection experienced an extended duration of viral shedding, which may suggest that the clearance of the Omicron variant is more reliant on lymphocyte activity in comparison to the original strain.
Eosinophils are mainly located in the gastrointestinal tract and lungs and have regulatory functions in protective immunity, organ growth and metabolism. Eosinophils are currently considered to have a protective role in the initial stage of COVID-19,56 and developing eosinopenia in the first compasses of COVID-19 is an indicator of poor prognosis and the worst disease course.57 According to one study, about half of the COVID-19 patients admitted to the hospital had eosinophilia, but for patients who were improving, eosinophil cell count gradually returns to normal.58,59 On the other hand, if eosinophil continues to decrease as the disease progresses, it may lead to serious consequences, including higher mortality, tissue damage, and a higher presence of coagulation disorder markers.60 Although the role of eosinophils in antiviral defense is not fully understood, our study found that low levels of eosinophils on admission may contribute to the slower SARS-CoV-2 Omicron virus clearance.
Neutrophilia, a sign of severe respiratory involvement and poor prognosis in COVID-19 patients,61 has been found in bronchoalveolar lavage fluid and circulation.62–64 But we did not observe the association between higher neutrophil counts and prolonged viral shedding in our investigation of non-severely symptomatic individuals with SARS-CoV-2 Omicron infection. This could be because only moderate inflammatory responses were generated in these patients.
Previous study has indicated that in elderly Omicron-infected patients over the age of 60, full vaccination can reduce the time to virus shedding and provide protection against serious infection.65 However, in our study, we discovered that vaccination status or the number of vaccine doses administered had no effect on the period of viral shedding, presumably due to the wide age range of our study population and the fact that only half were above 60 years old. Despite the fact that the Omicron variation has been demonstrated to evade immunity more easily than other VoCs, lowering the efficiency of clinically authorized vaccines such as mRNA and inactivated viral vaccines,66,67 vaccination remains a crucial preventive approach, particularly for older persons.
There are several limitations to our study. One is the lack of viral load data, which is critical for understanding the proliferation and spread of the virus. Another limitation is a lack of data on specific types of lymphocytes, such as CD4+ and CD8+ T cells, which play an important role in the immune response to SARS-CoV-2, including virus clearance and viral variant recognition.68 Moreover, our available data is limited to the 7-day positivity status of patients; hence, further investigations are required to determine if additional factors influence patients with viral clearance times exceeding 7 days. Furthermore, because our work is a single-center retrospective study, it needed to be validated in larger prospective studies.
Conclusion
In this study, we identified six factors that are associated with delayed viral shedding in non-severe SARS-CoV-2 Omicron infection, including advanced age, elevated CRP levels and reduced counts of platelets, leukocytes, lymphocytes, and eosinophils. Based on these findings, we developed a nomogram to predict the probability of viral shedding at 7 days for non-severe patients with SARS-CoV-2 Omicron infection. Our study may help non-severely affected patients to optimize their self-management strategies. For patients presenting the aforementioned high-risk factors, it is advisable to extend the typically prescribed quarantine period.
Ethics Statement
This study was conducted according to the guidelines laid down in the Declaration of Helsinki, and all the human participants were reviewed and approved by the Medical Ethics Committee of Shanghai Pudong New Area Gongli Hospital (GLYYls2022-025). All enrolled patients have signed informed consents from the study participants prior to study commencement.
Acknowledgments
May we pay tribute to the devoted healthcare workers who bravely battled the Omicron outbreak in Shanghai from March to June 2022. Their unwavering dedication, exceptional skills, and selfless sacrifices illuminated a path of hope amid the bleakest moments of the pandemic.
Funding
This study was funded by Outstanding Leaders Training Program of Pudong Health Bureau of Shanghai (Grant No. PWRl2022-06).
Disclosure
The authors no conflicts of interest in this work.
References
1. Bhattacharyya P, Das S, Aich S, Sarkar J. COVID-19: morphology and mechanism of the SARS-CoV-2, global outbreak, medication, vaccines and future of the virus. Frontiers Biosci. 2021;13(2):272. doi:10.52586/e884
2. Li J, Lai S, Gao GF, Shi W. The emergence, genomic diversity and global spread of SARS-CoV-2. Nature. 2021;600(7889):408–418. doi:10.1038/s41586-021-04188-6
3. Tian D, Sun Y, Xu H, Ye Q. The emergence and epidemic characteristics of the highly mutated SARS‐CoV‐2 Omicron variant. J Med Virol. 2022;94(6):2376–2383. doi:10.1002/jmv.27643
4. Prasad N, Derado G, Nanduri SA, et al. Effectiveness of a COVID-19 additional primary or booster vaccine dose in preventing SARS-CoV-2 infection among nursing home residents during widespread circulation of the omicron variant — United States, February 14–March 27, 2022. Morbidity Mortal Wkly Rep. 2022;71(18):633–637. doi:10.15585/mmwr.mm7118a4
5. Zhang X, Zhang W, Chen S. Shanghai’s life-saving efforts against the current omicron wave of the COVID-19 pandemic. Lancet Lond Engl. 2022;399(10340):2011–2012. doi:10.1016/s0140-6736(22)00838-8
6. Bálint G, Vörös-Horváth B, Széchenyi A. Omicron: increased transmissibility and decreased pathogenicity. Signal Transduct Target Ther. 2022;7(1):151. doi:10.1038/s41392-022-01009-8
7. Wang L, Cheng G. Sequence analysis of the emerging SARS‐CoV‐2 variant Omicron in South Africa. J Med Virol. 2022;94(4):1728–1733. doi:10.1002/jmv.27516
8. Lee YH, Hong CM, Lee TH, Hwang YJ, Kim DH, Lee J. Factors associated with prolonged viral detection in asymptomatic and mildly symptomatic patients with SARS-CoV-2 infection. J Infect Dev Ctries. 2022;16(02):291–297. doi:10.3855/jidc.15072
9. Hu X, Xing Y, Jia J, et al. Factors associated with negative conversion of viral RNA in patients hospitalized with COVID-19. Sci Total Environ. 2020;728:138812. doi:10.1016/j.scitotenv.2020.138812
10. Saxena SK, Kumar S, Ansari S, et al. Characterization of the novel SARS‐CoV‐2 Omicron (B.1.1.529) variant of concern and its global perspective. J Med Virol. 2022;94(4):1738–1744. doi:10.1002/jmv.27524
11. Zhang W, Zhou S, Wang G, et al. Clinical predictors and RT-PCR profile of prolonged viral shedding in patients with SARS-CoV-2 Omicron variant in Shanghai: a retrospective observational study. Frontiers Public Heal. 2022;10:1015811. doi:10.3389/fpubh.2022.1015811
12. CDC Online Newsroom | CDC. CDC streamlines COVID-19 guidance to help the public better protect themselves and understand their risk. Available from: https://www.cdc.gov/media/releases/2022/p0811-covid-guidance.html.
13. The Japan Times. Japan to shorten COVID-19 isolation period to seven days. Available from: https://www.japantimes.co.jp/news/2022/09/06/national/covid19-isolation-period-shortened/.
14. Center NC for GH and MNI of IDDC and P. Active Epidemiological Investigation on SARS‐CoV‐2 infection caused by omicron variant (Pango Lineage B. 1.1. 529) in Japan: preliminary report on infectious period; 2022.
15. National Health Care Commission of China. Diagnosis and treatment plan for COVID-19(trial version 9). Int J Epidemiol Infect Dis. 2022;49(02):73–80. doi:10.3760/cma.j.cn331340-20220325-00065
16. Zhang Y, Chen P, Zhou Q, et al. A novel immune-related prognostic signature in head and neck squamous cell carcinoma. Frontiers Genetics. 2021;12:570336. doi:10.3389/fgene.2021.570336
17. Lin Y, Wang M, Jia J, et al. Development and validation of a prognostic nomogram to predict recurrence in high-risk gastrointestinal stromal tumour: a retrospective analysis of two independent cohorts. Ebiomedicine. 2020;60:103016. doi:10.1016/j.ebiom.2020.103016
18. Su YS, Gelman A, Hill J, Yajima M. Multiple imputation with diagnostics (mi) in R: opening windows into the black box. J Stat Softw. 2011;45(2). doi:10.18637/jss.v045.i02
19. Harrell FE. Regression Modeling Strategies, with Applications to Linear Models, Logistic Regression, and Survival Analysis. Springer; 2001:465–507. doi:10.1007/978-1-4757-3462-1_19
20. Dauriz M, Targher G, Temporelli PL, et al. Prognostic impact of diabetes and prediabetes on survival outcomes in patients with chronic heart failure: a post‐hoc analysis of the GISSI‐HF (Gruppo Italiano per lo Studio della Sopravvivenza nella Insufficienza Cardiaca‐Heart Failure) trial. J Am Heart Assoc. 2017;6(7):e005156. doi:10.1161/jaha.116.005156
21. DeLong ER, DeLong DM, Clarke-Pearson DL. Comparing the areas under two or more correlated receiver operating characteristic curves: a nonparametric approach. Biometrics. 1988;44(3):837. doi:10.2307/2531595
22. Lin A, He ZB, Zhang S, Zhang JG, Zhang X, Yan WH. Early risk factors for the duration of severe acute respiratory syndrome coronavirus 2 viral positivity in patients with coronavirus disease 2019. Clin Infect Dis. 2020;71(16):2061–2065. doi:10.1093/cid/ciaa490
23. Xiao AT, Tong YX, Zhang S. Profile of RT-PCR for SARS-CoV-2: a preliminary study from 56 COVID-19 patients. Clin Infect Dis. 2020;71(16):2249–2251. doi:10.1093/cid/ciaa460
24. Xu K, Chen Y, Yuan J, et al. Factors associated with prolonged viral RNA shedding in patients with coronavirus disease 2019 (COVID-19). Clin Infect Dis. 2020;71(15):799–806. doi:10.1093/cid/ciaa351
25. Zheng S, Fan J, Yu F, et al. Viral load dynamics and disease severity in patients infected with SARS-CoV-2 in Zhejiang province, China, January-March 2020: retrospective cohort study. BMJ. 2020;369:m1443. doi:10.1136/bmj.m1443
26. Zou L, Ruan F, Huang M, et al. SARS-CoV-2 viral load in upper respiratory specimens of infected patients. New Engl J Med. 2020;382(12):1177–1179. doi:10.1056/nejmc2001737
27. Yuan S, Pan Y, Xia Y, et al. Development and validation of an individualized nomogram for early prediction of the duration of SARS-CoV-2 shedding in COVID-19 patients with non-severe disease. J Zhejiang Univ Sci B. 2021;22(4):318–329. doi:10.1631/jzus.b2000608
28. Bajaj V, Gadi N, Spihlman AP, Wu SC, Choi CH, Moulton VR. Aging, Immunity, and COVID-19: how Age Influences the Host Immune Response to Coronavirus Infections? Front Physiol. 2021;11:571416. doi:10.3389/fphys.2020.571416
29. Khatri R, Siddqui G, Sadhu S, et al. Intrinsic D614G and P681R/H mutations in SARS-CoV-2 VoCs Alpha, Delta, Omicron and viruses with D614G plus key signature mutations in spike protein alters fusogenicity and infectivity. Med Microbiol Immun. 2022:1–20. doi:10.1007/s00430-022-00760-7
30. Zhou F, Yu T, Du R, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. 2020;395(10229):1054–1062. doi:10.1016/s0140-6736(20)30566-3
31. Santesmasses D, Castro JP, Zenin AA, et al. COVID‐19 is an emergent disease of aging. Aging Cell. 2020;19(10):e13230. doi:10.1111/acel.13230
32. McWilliam S, Riordan A. How to use: c-reactive protein. Archives Dis Child Educ Pract Ed. 2010;95(2):55. doi:10.1136/adc.2009.174367
33. Sadeghi-Haddad-Zavareh M, Bayani M, Shokri M, et al. C-reactive protein as a prognostic indicator in COVID-19 patients. Interdiscip Perspect Infect Dis. 2021;2021:5557582. doi:10.1155/2021/5557582
34. Smilowitz NR, Kunichoff D, Garshick M, et al. C-reactive protein and clinical outcomes in patients with COVID-19. Eur Heart J. 2021;42(23):ehaa1103. doi:10.1093/eurheartj/ehaa1103
35. Bouayed MZ, Laaribi I, Chatar CEM, et al. C-Reactive Protein (CRP): a poor prognostic biomarker in COVID-19. Front Immunol. 2022;13:1040024. doi:10.3389/fimmu.2022.1040024
36. Zhang H, Chen W, Ye X, et al. Clinical characteristics of patients infected with novel coronavirus wild strain, Delta variant strain and Omicron variant strain in Quanzhou: a real-world study. Exp Ther Med. 2022;25(1):62. doi:10.3892/etm.2022.11761
37. Chang H, Li J. “Lymphocyte * Neutrophil” count decreased in SARS‐CoV‐2 Omicron patients in Shanghai with no significant change in CRP and SAA. J Clin Lab Anal. 2022;36(10):e24671. doi:10.1002/jcla.24671
38. Lippi G, Plebani M, Henry BM. Thrombocytopenia is associated with severe coronavirus disease 2019 (COVID-19) infections: a meta-analysis. Clin Chim Acta. 2020;506:145–148. doi:10.1016/j.cca.2020.03.022
39. Wool GD, Miller JL. The impact of COVID-19 disease on platelets and coagulation. Pathobiology. 2021;88(1):15–27. doi:10.1159/000512007
40. Jiang S, Huang Q, Xie W, Lv C, Quan X. The association between severe COVID‐19 and low platelet count: evidence from 31 observational studies involving 7613 participants. Brit J Haematol. 2020;190(1):e29–e33. doi:10.1111/bjh.16817
41. Bury L, Camilloni B, Castronari R, et al. Search for SARS-CoV-2 RNA in platelets from COVID-19 patients. Platelets. 2021;32(2):284–287. doi:10.1080/09537104.2020.1859104
42. Xu P, Zhou Q, Xu J. Mechanism of thrombocytopenia in COVID-19 patients. Ann Hematol. 2020;99(6):1205–1208. doi:10.1007/s00277-020-04019-0
43. Semple JW, Aslam R, Kim M, Speck ER, Freedman J. Platelet-bound lipopolysaccharide enhances Fc receptor–mediated phagocytosis of IgG-opsonized platelets. Blood. 2007;109(11):4803–4805. doi:10.1182/blood-2006-12-062695
44. Kim JK, Jeon J, Kim JW, Kim G. Correlation between abnormal platelet count and respiratory viral infection in patients from Cheonan, Korea. J Clin Lab Anal. 2016;30(3):185–189. doi:10.1002/jcla.21822
45. Liu PP, Blet A, Smyth D, Li H. The science underlying COVID-19: implications for the cardiovascular system. Circulation. 2020;142(1):68–78. doi:10.1161/circulationaha.120.047549
46. Huang C, Wang Y, Li X, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet Lond Engl. 2020;395(10223):497–506. doi:10.1016/s0140-6736(20)30183-5
47. Tabary M, Khanmohammadi S, Araghi F, Dadkhahfar S, Tavangar SM. Pathologic features of COVID-19: a concise review. Pathol Res Pract. 2020;216(9):153097. doi:10.1016/j.prp.2020.153097
48. Fathi N, Rezaei N. Lymphopenia in COVID‐19: therapeutic opportunities. Cell Biol Int. 2020;44(9):1792–1797. doi:10.1002/cbin.11403
49. Henry BM, Aggarwal G, Wong J, et al. Lactate dehydrogenase levels predict coronavirus disease 2019 (COVID-19) severity and mortality: a pooled analysis. Am J Emerg Med. 2020;38(9):1722–1726. doi:10.1016/j.ajem.2020.05.073
50. Chhetri S, Khamis F, Pandak N, Khalili HA, Said E, Petersen E. A fatal case of COVID-19 due to metabolic acidosis following dysregulate inflammatory response (cytokine storm). Idcases. 2020;21:e00829. doi:10.1016/j.idcr.2020.e00829
51. Xiong Y, Liu Y, Cao L, et al. Transcriptomic characteristics of bronchoalveolar lavage fluid and peripheral blood mononuclear cells in COVID-19 patients. Emerg Microbes Infec. 2020;9(1):761–770. doi:10.1080/22221751.2020.1747363
52. Ouyang Y, Yin J, Wang W, et al. Downregulated gene expression spectrum and immune responses changed during the disease progression in patients with COVID-19. Clin Infect Dis. 2020;71(16):2052–2060. doi:10.1093/cid/ciaa462
53. Corley MJ, Ndhlovu LC. DNA methylation analysis of the COVID-19 host cell receptor, Angiotensin I Converting Enzyme 2 Gene (ACE2) in the respiratory system reveal age and gender differences; 2020. doi:10.20944/preprints202003.0295.v1
54. Crimi E, Benincasa G, Figueroa-Marrero N, Galdiero M, Napoli C. Epigenetic susceptibility to severe respiratory viral infections and its therapeutic implications: a narrative review. Bja Br J Anaesth. 2020;125(6):1002–1017. doi:10.1016/j.bja.2020.06.060
55. Sadeghi S, Nasri P, Nasri E, et al. The correlation between viral shedding duration and blood biomarkers in COVID-19-infected patients. J Res Med Sci. 2022;27:43. doi:10.4103/jrms.jrms_401_21
56. Nair AP, Soliman A, Masalamani MAA, et al. Clinical outcome of eosinophilia in patients with COVID-19: a controlled study. Acta Bio Medica Atenei Parmensis. 2020;91(4):e2020165. doi:10.23750/abm.v91i4.10564
57. Xie G, Ding F, Han L, Yin D, Lu H, Zhang M. The role of peripheral blood eosinophil counts in COVID‐19 patients. Allergy. 2021;76(2):471–482. doi:10.1111/all.14465
58. Zhang J, Dong X, Cao Y, et al. Clinical characteristics of 140 patients infected with SARS‐CoV‐2 in Wuhan, China. Allergy. 2020;75(7):1730–1741. doi:10.1111/all.14238
59. Mu T, Yi Z, Wang M, et al. Expression of eosinophil in peripheral blood of patients with COVID‐19 and its clinical significance. J Clin Lab Anal. 2021;35(1):e23620. doi:10.1002/jcla.23620
60. Yan B, Yang J, Xie Y, Tang X. Relationship between blood eosinophil levels and COVID-19 mortality. World Allergy Organ J. 2021;14(3):100521. doi:10.1016/j.waojou.2021.100521
61. Blanch-Ruiz MA, Ortega-Luna R, Gómez-García G, Martínez-Cuesta MÁ, Álvarez Á. Role of neutrophil extracellular traps in COVID-19 progression: an insight for effective treatment. Biomed. 2021;10(1):31. doi:10.3390/biomedicines10010031
62. Hazeldine J, Lord JM. Neutrophils and COVID-19: active participants and rational therapeutic targets. Front Immunol. 2021;12:680134. doi:10.3389/fimmu.2021.680134
63. Liao M, Liu Y, Yuan J, et al. Single-cell landscape of bronchoalveolar immune cells in patients with COVID-19. Nat Med. 2020;26(6):842–844. doi:10.1038/s41591-020-0901-9
64. Chua RL, Lukassen S, Trump S, et al. COVID-19 severity correlates with airway epithelium–immune cell interactions identified by single-cell analysis. Nat Biotechnol. 2020;38(8):970–979. doi:10.1038/s41587-020-0602-4
65. Lu G, Zhang Y, Zhang H, et al. Geriatric risk and protective factors for serious COVID-19 outcomes among older adults in Shanghai Omicron wave. Emerg Microbes Infec. 2022;11(1):2045–2054. doi:10.1080/22221751.2022.2109517
66. Wilhelm A, Widera M, Grikscheit K, et al. Limited neutralisation of the SARS-CoV-2 Omicron subvariants BA.1 and BA.2 by convalescent and vaccine serum and monoclonal antibodies. Ebiomedicine. 2022;82:104158. doi:10.1016/j.ebiom.2022.104158
67. Wang K, Jia Z, Bao L, et al. Memory B cell repertoire from triple vaccinees against diverse SARS-CoV-2 variants. Nature. 2022;603(7903):919–925. doi:10.1038/s41586-022-04466-x
68. Moss P. The T cell immune response against SARS-CoV-2. Nat Immunol. 2022;23(2):186–193. doi:10.1038/s41590-021-01122-w
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Development and Validation of a Predictive Nomogram with Age and Laboratory Findings for Severe COVID-19 in Hunan Province, China
Jiang J, Zhong W, Huang W, Gao Y, He Y, Li X, Liu Z, Zhou H, Fu Y, Liu R, Zhang W
Therapeutics and Clinical Risk Management 2022, 18:579-591
Published Date: 17 May 2022
Old Age is an Independent Risk Factor for Pneumonia Development in Patients with SARS-CoV-2 Omicron Variant Infection and a History of Inactivated Vaccine Injection
Tong X, Huang Z, Zhang X, Si G, Lu H, Zhang W, Xue Y, Xie W
Infection and Drug Resistance 2022, 15:5567-5573
Published Date: 21 September 2022
The m7G Modification Level and Immune Infiltration Characteristics in Patients with COVID-19
Lu L, Zheng J, Liu B, Wu H, Huang J, Wu L, Li D
Journal of Multidisciplinary Healthcare 2022, 15:2461-2472
Published Date: 26 October 2022
Clinico-Epidemiological Profile of COVID-19 Patients with Omicron Variant Admitted in a Tertiary Care Center, South India
Ethirajan T, Natarajan G, Velayudham R, Jayakumaran P, Karnan I, Rajendran K, Doraisamy S, Chenakeswarar Sridhar S, Kumaran P, Kamaraj K, Kandasamy A, Natarajan M
International Journal of General Medicine 2023, 16:185-191
Published Date: 17 January 2023
A Nomogram for Predicting Survival in Patients with SARS-CoV-2 Omicron Variant Pneumonia Based on Admission Data
Yang Y, Li D, Nie J, Wang J, Huang H, Hang X
Infection and Drug Resistance 2025, 18:2093-2104
Published Date: 25 April 2025