Back to Journals » Psychology Research and Behavior Management » Volume 19
A Network Analysis of the Interrelationships Between Depression, Anxiety, Insomnia and Non-Suicidal Self-Injury in Middle School Students
Authors Qian H, Zhang J, Duan X, Wu TM, Xie YF, Yang BX, Luo D, Liu LZ, Yu P
Received 16 October 2025
Accepted for publication 7 January 2026
Published 12 January 2026 Volume 2026:19 570928
DOI https://doi.org/10.2147/PRBM.S570928
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mei-Chun Cheung
Hang Qian,1,* Juan Zhang,2,* Xiang Duan,3 Tai-Min Wu,2 Yao-Fei Xie,2 Bing-Xiang Yang,4 Dan Luo,4 Lian-Zhong Liu,5 Ping Yu2
1Tongji Medical College of Huazhong University of Science and Technology, Wuhan, People’s Republic of China; 2Affiliated Wuhan Mental Health Center, Tongji Medical College of Huazhong University of Science and Technology, Wuhan, People’s Republic of China; 3Department of Psychology, Institute of Education, China University of Geosciences, Wuhan, People’s Republic of China; 4Center for Wise Information Technology of Mental Health Nursing Research, School of Nursing, Wuhan University, Wuhan, People’s Republic of China; 5Wuhan Wudong Hospital (Wuhan Second Mental Hospital), Wuhan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Lian-Zhong Liu, Email [email protected] Ping Yu, Email [email protected]
Purpose: Depression, anxiety and Insomnia are common among middle school students. Non-suicidal self-injury (NSSI) has become an important mental health issue in this group. This study explores the comorbid relationship between depression, anxiety, and insomnia symptoms among junior high school students from a network perspective and investigates the associations between these symptoms and NSSI.
Patients and Methods: This study was a cross-sectional design with convenience sampling, and students from junior high schools in Wuhan, China, were selected in October 2023 (N=8244) as survey respondents. An online questionnaire was used to collect data. The Patient Health Questionnaire, Generalized Anxiety Disorder Scale and Insomnia Severity Index were used to assess depression, anxiety and insomnia. Whether NSSI behaviors occurred in the last 1 year was obtained by self-report. Network analysis was used to assess core and bridge symptoms of the depression, anxiety and insomnia co-morbidity network and associations with NSSI.
Results: The results revealed that GAD2 “Control Worry”, GAD3 “Excessive Worry” (EI = 1.040), ISI2 “SleepMaint” (EI=1.025) and PHQ2 “Hopeless” (EI=1.018) were the central symptoms of the network, exhibiting the highest expected influence values. GAD5 “restlessness” (BEI=0.376) and PHQ4 “Lack of Energy” (BEI=0.351), PHQ6 “self feeling” (BEI=0.325) and GAD1 “Nervous” (BEI=0.296) were the bridge symptoms. PHQ9 “Suicidal Ideation” (edge weight = 0.33) showed the strongest connection to NSSI. The network comparison test results indicated a more densely connected symptom network in the NSH group than in the NSSI group.
Conclusion: Symptoms related to worry are core factors in the network of depression, anxiety, and insomnia among junior high school students. Suicidal ideation is directly and closely associated with NSSI. These symptoms may serve as key targets for early screening and intervention, while the strong link between suicidal ideation and NSSI underscores the need for timely prevention efforts in this vulnerable population.
Keywords: adolescent, mental health, self-injurious behavior, network analysis
Introduction
During middle school, the initial stage of adolescence following childhood, adolescents experience a critical period marked by rapid physical and psychological development.1,2 Although their sense of independence increases, insufficient cognitive maturity and limited self-regulation strategies make them more vulnerable to stressors and adverse events, leading to heightened mood swings, anxiety, depression, or self-perceptual conflicts, and potentially resulting in behavioral issues such as substance abuse, self-injury, or even suicide.3 Given these challenges, it is essential to investigate middle school students to better understand and address emerging mental health risks during this vulnerable period.
Depression, anxiety, and insomnia are the most common psychological disturbances in early adolescence, with the potential to persist into adulthood.4 A study involving Chinese adolescents aged 12–17 years reported prevalence rates of 25.6% for depressive symptoms and 26.9% for anxiety symptoms.5 Large-scale reviews indicate a combined prevalence of depressive symptoms of 24.15% among junior high school students and an anxiety prevalence of 13.89%,6,7 both higher than those observed in high school students from the same studies. Moreover, accumulating evidence points to an upward trend in the prevalence of depression and anxiety among adolescents.8 Adolescents are particularly vulnerable to insomnia due to circadian rhythm shifts and exposure to external stressors. Within China’s educational context, sleep disturbances represent a frequent complaint among adolescents.9 Early meta-analyses have shown that 53% of school-attending students sleep less than 8 hours per night and 36% report difficulties falling asleep.10,11 Epidemiological studies confirm a close association between depression, anxiety, and insomnia during adolescence, with these conditions frequently exhibiting high rates of comorbidity,12–14 underpinned by specific biological, psychological, and social mechanisms.15 Research conducted in adolescent samples has demonstrated that mood disorders (depression and anxiety) and insomnia often act as reciprocal predictors, exacerbating the severity of each disorder.16–18 These conditions contribute, to varying degrees, to academic underperformance,19,20 interpersonal difficulties,21,22 and behavioral problems in adolescents.20,23,24
Numerous factors influence mood and sleep disorders, with gender differences representing one of the most consistently reported findings.25,26 Multiple large-scale studies indicate that, beginning in adolescence, female adolescents exhibit significantly higher prevalence rates of depressive and anxiety symptoms compared to males,27–29 and are also more likely to report insomnia-related symptoms.30 Furthermore, only children in China may benefit from greater educational investment and access to family resources; however, they may simultaneously face heightened parental expectations and academic pressure. Epidemiological research has yielded inconsistent findings regarding differences in emotional problems and sleep conditions between only children and those with siblings.31,32 In addition, escalating academic pressure during the transition to higher grades, peer relationships, and family environment are widely recognized as being closely associated with depression, anxiety, and sleep problems among junior high school adolescents.33,34
In early adolescence, difficulties in emotion regulation associated with symptoms of anxiety, depression, and sleep problems may heighten the likelihood of adopting non-suicidal self-injury (NSSI) as a maladaptive coping strategy.35 Non-suicidal self-injury (NSSI) is the direct, repetitive, and intentional infliction of bodily harm without suicidal intent or resulting in death.36 NSSI behavior typically begins in early childhood,37 persists throughout adolescence, and can even continue into adulthood. Notably, adolescence is a period when the incidence of NSSI increases dramatically, with recent review surveys indicating a detection rate of 22% among adolescent students.38 NSSI poses serious harm to individuals, adversely affecting the academic and social functioning of adolescent students, and is significantly associated with suicidal behavior.39 Furthermore, NSSI is strongly associated with a wide range of psychosocial health problems and behavioral disorders in adulthood.40 Research indicates that for adolescents in the junior high school stage (ages 11–15), NSSI frequently exhibits a highly intertwined pattern of comorbidity with depression, anxiety, and insomnia/sleep problems.41,42 Elevated levels of depressive and anxiety symptoms are commonly regarded as critical psychological risk factors for NSSI, with longitudinal evidence from large samples of Chinese children and adolescents indicating that depressive/anxiety symptoms predict the onset, persistence, or trajectory of NSSI behaviors.43 This suggests that emotional distress may increase the risk of self-injury by impairing stress coping and emotion regulation capacities. Furthermore, studies conducted across multiple junior and senior high schools in China have revealed that sleep problems can predict subsequent NSSI in adolescents.44,45
Previous research has predominantly examined the interrelationships among depression, anxiety, and insomnia symptoms, typically employing traditional statistical approaches such as regression analysis, structural equation modeling, or mediation analysis.46 However, these methods have limitations in capturing interactive effects among symptoms and accurately modeling complex multivariate relationships. Network theory offers a novel perspective, positing that psychopathological phenomena arise from dynamic interactions among symptoms, where strong connections form distinct feedback loops that facilitate the onset and maintenance of disorders.47 Network analysis has been widely applied in comorbidity studies of mood and insomnia disorders across various populations. For instance, one study on anxiety-depression and insomnia comorbidity in university students (including depressive symptoms) identified low energy, the impact of sleep on daytime functioning, and difficulty relaxing as central symptoms.48 In a sample of Macau residents, difficulties maintaining sleep, sleep-related daytime dysfunction, and difficulty relaxing emerged as central symptoms.49 However, such investigations have not specifically targeted middle school students. The present study employs comorbidity network analysis to investigate symptom-level associations among depression, anxiety, and insomnia in middle school students. Centrality indices are used to identify core symptoms and bridge symptoms, which may serve as critical targets for intervention. The study also utilizes the EBICglasso method and the Network Comparison Test (NCT) to evaluate between-group differences. Furthermore, this research examines symptoms associated with non-suicidal self-injury (NSSI) and conducts network comparison analyses of the depression-anxiety-insomnia comorbidity network stratified by NSSI engagement, gender, and only-child status. These analyses aim to elucidate inter-symptom interconnections and provide empirical foundations for strategies to mitigate risks of depression, anxiety, insomnia, and NSSI in adolescents.
Materials and Methods
Data and Sample
This study was conducted in October 2023 in Wuhan, China. Using convenience sampling, four junior high schools were selected from four different regions of the city, and questionnaires were administered to middle school students in grades one through third at these schools. The enumerators received standardized training and administered the survey on-site with the cooperation of the schools during class time. Before the survey, students were informed about the purpose and nature of the study and were provided with instructions on how to complete the questionnaire. Participants accessed the relevant service cloud platform to complete the anonymous self-report questionnaire and submitted it on the website, resulting in 8244 valid questionnaires with no missing information being included in the analysis. To ensure response validity, several quality checks were implemented. Specifically, questionnaires with excessive missing data, implausibly short completion times, or uniform response patterns were excluded from the analysis. In addition, data collection was conducted in a supervised school setting, which reduced the likelihood of inattentive responding. The Ethics Committee of the Affiliated Wuhan Mental Health Center approved the study.
Measurements
Sociodemographic Data
The researcher designed a questionnaire to collect socio-demographic information, including gender (male/female), age, grade (first, second, or third year), and whether the respondent was an only child (yes/no).
Depression Symptoms
Depressive symptoms among students were assessed using the Patient Health Questionnaire-9 (PHQ-9).50 Items are rated on a 4-point Likert scale (0 = not at all, 1 = several days, 2 = more than half the days, 3 = nearly every day). Total scores range from 0 to 27, with scores of 5 or higher indicating the presence of depressive symptoms. In the present study, the Cronbach’s alpha for the PHQ-9 was 0.905, demonstrating excellent internal consistency.
Anxious Symptoms
The Chinese version of the Generalized Anxiety Disorder Scale (GAD-7) was used for anxiety screening and assessment of symptom severity. The GAD-7 consists of a total of 7 items, with each item scored from “0” (not at all) to 3 (almost every day) and a total score ranging from 0 to 21. The GAD-7 was used to assess the severity of symptoms and the severity of symptoms.51 Individuals with a total GAD score of ≥5 were considered to be “experiencing symptoms of anxiety”,52 with a Cronbach’s α of 0.931.
Insomnia Symptoms
Sleep status was investigated using the Insomnia Severity Index (ISI) to survey students’ sleep status.53 This scale is one of the most widely used scales for assessing insomnia in clinical practice. The ISI consists of seven items rated on a scale from “0” (none) to “4” (very severe), with a total score ranging from 0 to 28.54 Individuals with a total score of ≥8 were considered to “have symptoms of insomnia”, with a Cronbach’s α of 0.882.
Occurrence of NSSI
This survey used a history of self-injurious behavior as a screen for self-injurious behavior (In the past 12 months, have you intentionally injured yourself, but not with the intent to kill yourself? (Yes/No). If the answer was yes, the population was defined as self-injurious.
Statistical Analysis
Web Estimation
Mean scores and standard deviations (SDs) for the Patient Healthy Questionnaire (PHQ-9), Insomnia Severity Index (ISI), and Generalized Anxiety Disorder-7 (GAD-7) were calculated using IBM SPSS Statistics (version 27.0). The RStudio program (version 4.4.3) was used to perform network analyses.
The network was estimated using the bootnet package in R, and the qgraph package was employed for visualization. First, the Gaussian graphical model (GGM), a Gaussian graph-based regularization method including the glasso (graph minimum absolute contraction and control of false positive edges) process, was used to estimate the depression-anxiety-insomnia network, and the Extended Bayesian Information Criterion (EBIC) was used to select the best-fitting model. The “mgm” package was used to estimate the predictability of each node. To further explore the association of NSSI with depression, anxiety and insomnia symptoms, the “flow” feature of the qgraph package was used, which allows for the identification of symptoms with the greatest relevance.
Centrality Estimation
In order to quantify the degree of centrality of nodes in the network, we calculated the expected influence value in the centrality index using the function “centrality Plot” from the R package “qgraph”. Additionally, we calculated the bridge centrality index to quantify the degree of association between symptoms of different diseases; symptoms with higher bridge centrality indicate that the symptom has a strong activation in the network.
The accuracy and stability of network edge weights and centrality indices were conducted by the R package “bootnet”,55 applying a nonparametric bootstrap to assess the accuracy of the edges, and constructing a 95% CI by resampling and replacing the data, with narrower constructed CIs indicating high network confidence. We used the case-drop bootstrap to check the estimation accuracy of centrality indices.56 The program checks for stability by examining the correlation of estimated centrality in the original and subset samples. Centrality indices are considered stable if they do not vary significantly in the smallest subsample (randomly excluding 70% of the data in the original data set). The correlation stability (CS) coefficient was calculated to quantify stability according to.57 It is recommended that the CS coefficient should be more than 0.5 but not less than 0.25.
Network Comparisons
We divided the sample into non-sucidual self-injury group (NSSI group) (N=1183) and non-self-injury group (NSH group) (N=7061), into genders (4441 males, 3803 females), and into only children (N=4557) and non-only children (N=3687). Then we performed the comparison of Gaussian-model-based network analyses of depression-anxiety-insomnia comorbidities. We used the R package “Network Comparison Test” (NCT) to examine the differences in network structure between two estimated models. The different networks are visualized with the same layout in the function “Average Layout” in the R package “qgraph”. The invariance of the global intensity and edge weights is calculated to characterize the difference between global and local features. The global intensity is the sum of all edges.58 In symptom networks, overall intensity can reveal disease vulnerability. Higher values of overall strength indicate stronger links between symptoms.59
Results
Study Sample
The demographic characteristics of the full sample are shown in Table 1. The NSSI detection rate is 14.35%. Demographic characteristics as shown in the Table 1, the average age of the middle school students surveyed was 14.40 years old, the number of female students was 3803 (46.1%), and the number of only children was 4557 (55.3%) and the ratio of the grades in which they were enrolled was 3077 (37.3%) in the first year, 2718 (33.0%) in the second year. The mean total PHQ-9 score for the whole sample was 4.02, the mean total GAD-7 score for the whole sample was 3.50, and the mean total ISI score was 4.09. Mean scores and standard deviations for each of the PHQ9, GAD7 and ISI entries are shown in Table 2.
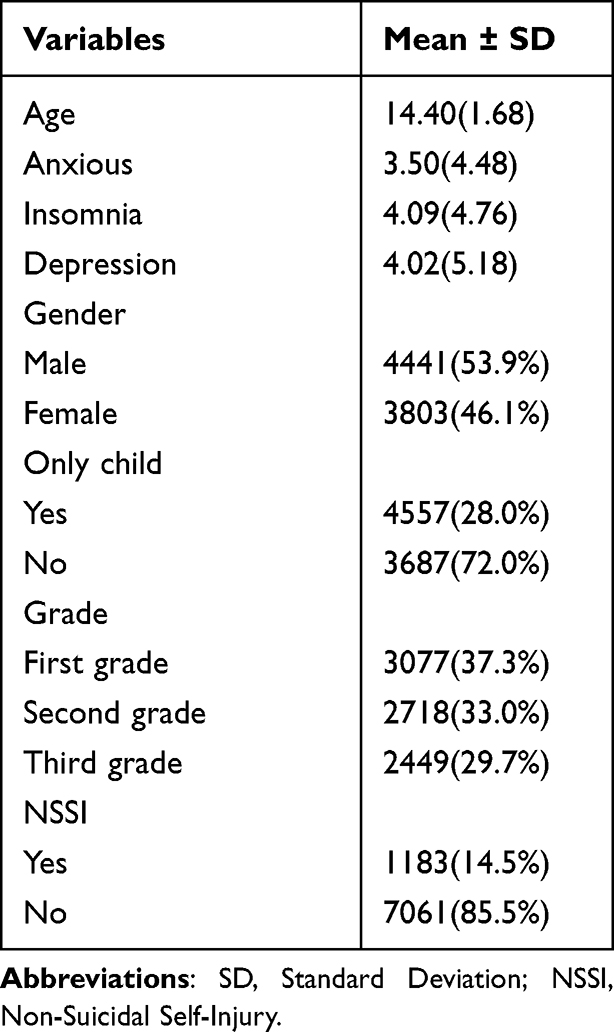 |
Table 1 Sample Characteristics |
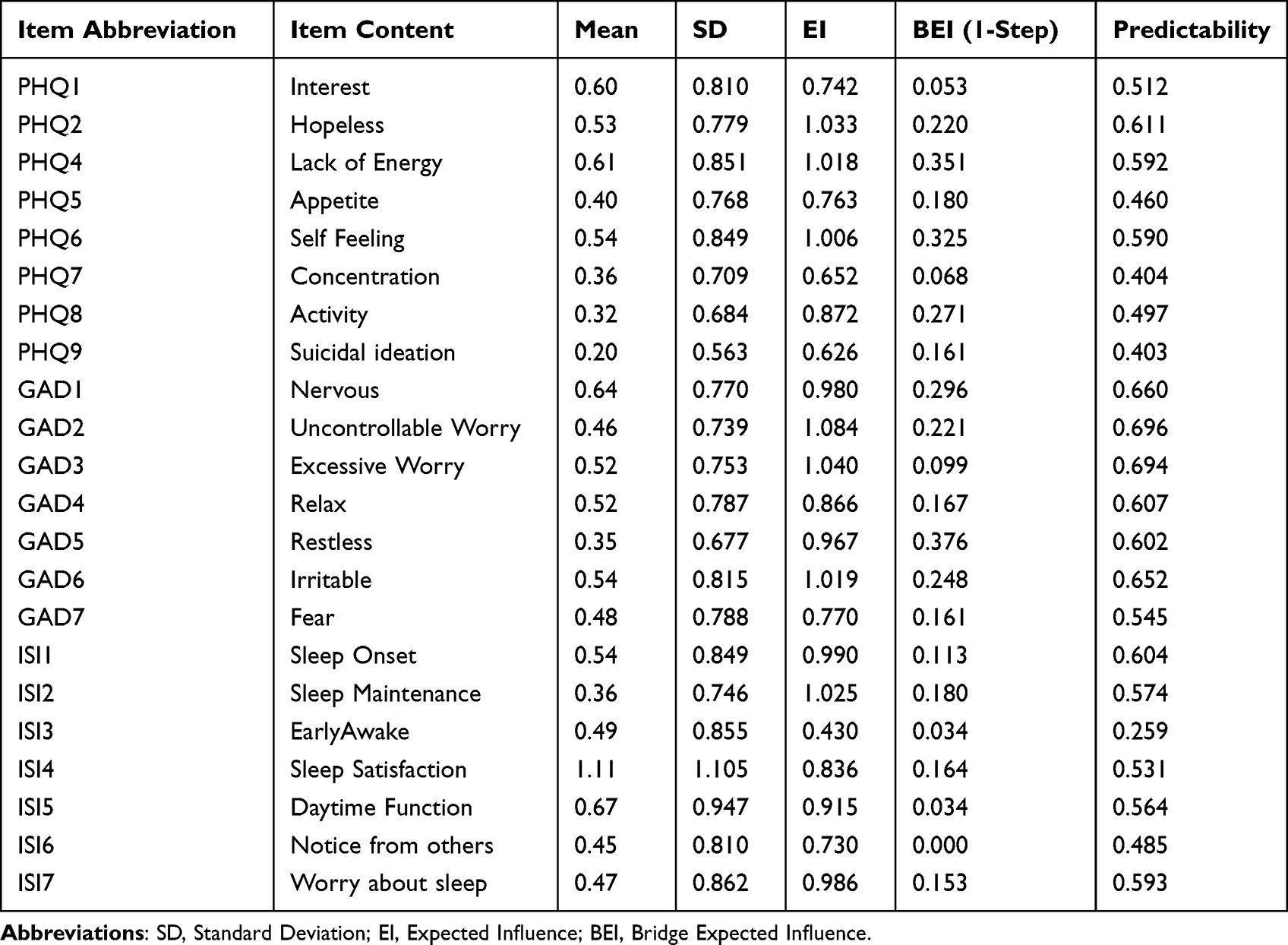 |
Table 2 Original Values of Mean, SD, Predictability, EI, and BEI for Each Node |
Network Structure
Symptom comorbidity networks of the full sample are available in Figure 1, annulus around the periphery of each symptom node are used to represent the predictability of the nodes, the mean predictability is 0.538 (range from 0.260–0.697), and mean scores on each item of the PHQ9, GAD-7 and ISI, while the predictability of each symptom are shown in Table 2. The network diagram shows that among the possible 231 edges, there are 102 non-zero edges, indicating a network density of 44.2%. The thickest edges within the entire network exist within individual communities, such as between ISI1 “sleep onset” and ISI2 “sleep maintenance” (edge weight = 0.41), GAD2 “control worry” and GAD3 “excessive worry” (edge weight = 0.29), and PHQ1 “interest decreased” and PHQ2 “hopeless” (edge weight = 0.32). The strongest cross-community connecting edges are between PHQ8 “Activity” and GAD5 “restlessness” (edge weight = 0.18), PHQ4 “lack of energy” and ISI4 “Sleep Satisfaction” (edge weight = 0.10), and GAD7 “fear” and PHQ6 “self feeling” (edge weight = 0.10).
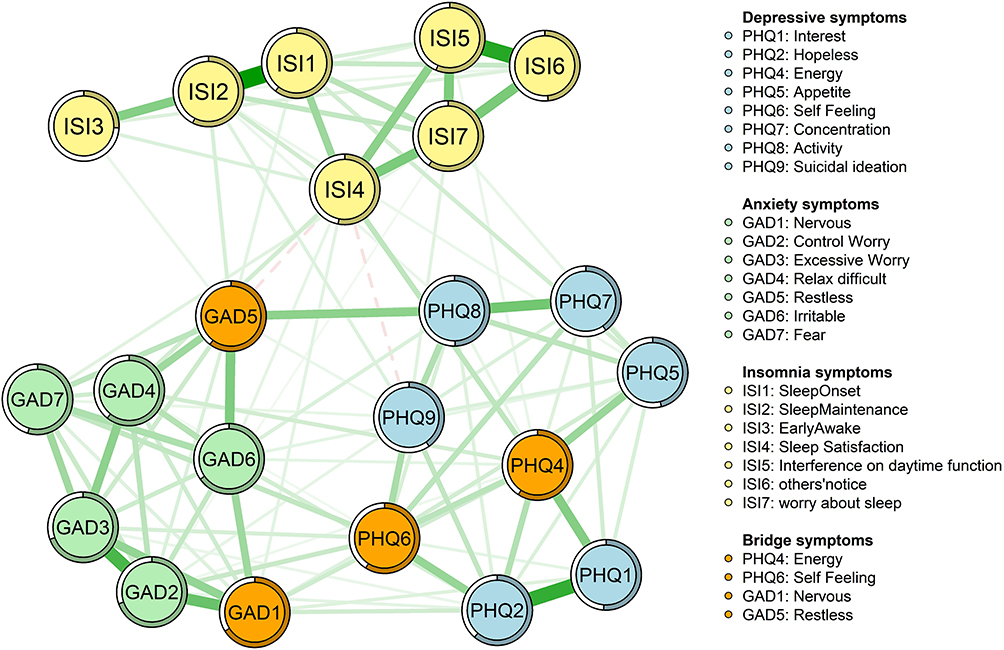 |
Figure 1 The network structure of depression, anxiety and insomnia symptoms. |
Network Centrality
In the analysis of network centrality, expected influence is used to measure centrality in symptom networks containing negatively correlated symptoms, and is often preferred to the commonly used “intensity” index. The node centrality results (Figure 2A) indicated that GAD2 “control worry” had the highest expected influence value (EI = 1.084), followed by GAD3 “excessive worry” (EI = 1.040), ISI2 “sleep maintenance” (EI=1.025), and PHQ2 “hopeless” (EI=1.018). Bridge symptoms are the symptoms with the highest bridge centrality in the network and represent the most influential symptoms in the comorbidity network. Additionally, as shown in Figure 2B, GAD5 “restlessness” (BEI=0.376) and PHQ4 “lack of energy” (BEI=0.351), PHQ6 “self feeling” (BEI=0.325) and GAD1 “nervous” (BEI=0.296) had the highest bridge expected influence value, playing an important role in linking anxiety and insomnia within the network. The original values of expected influence and the bridge’s expected influence values are visible in Table 2.
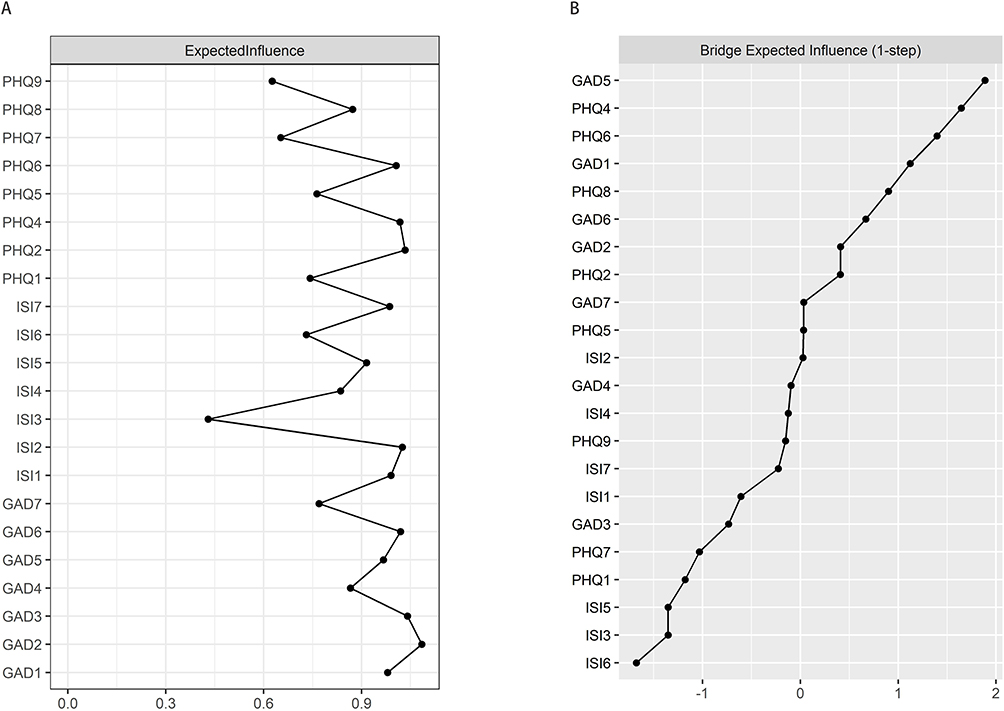 |
Figure 2 Centrality and Bridge Centrality of the Network. (A) EI of the Network; (B) BEI of the Network. |
Network Accuracy and Stability
As shown in Figure 3, the large overlap between the 95% confidence intervals of the edge weights obtained by the bootstrap method was sufficient to indicate that the estimates of the insomnia and anxiety symptom networks were sufficiently accurate. In Figure 4, the stability test of the network centrality metrics for expected influence and bridge expected influence yielded very high results, with a CS mean of 0.75, indicating that the structure of the network remained unchanged when 75% of the samples were discarded.
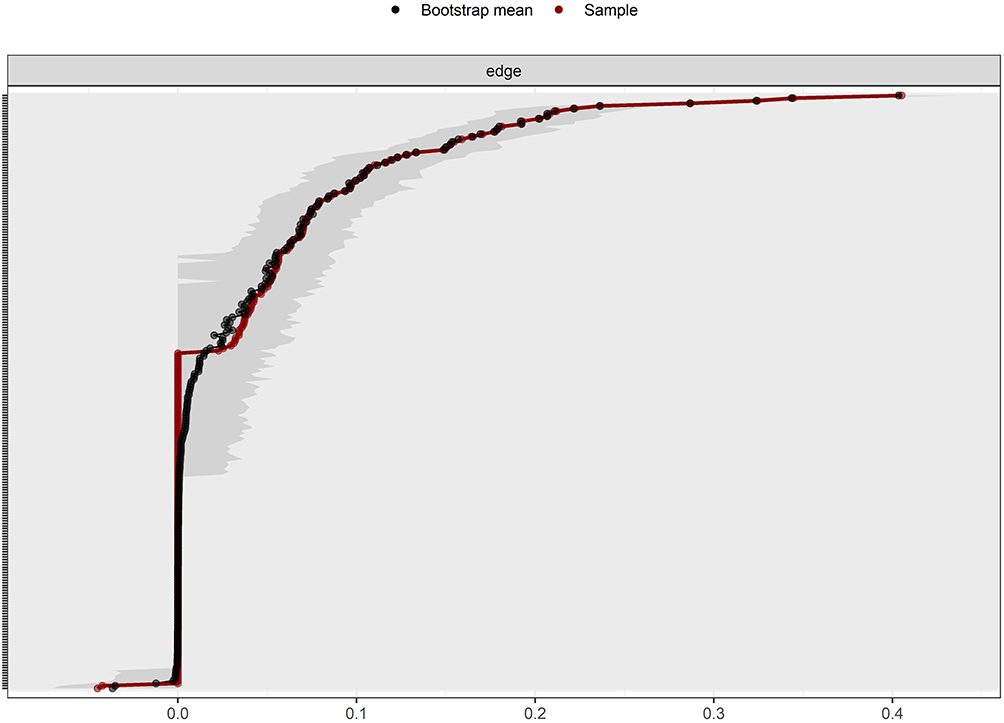 |
Figure 3 Bootstrapped confidence intervals of estimated edge weights. Notes: Red lines indicate the edge weights in the study sample, black lines represent the average edge weights estimated by the bootstrap, and the gray area represents the confidence intervals derived from the bootstrap. |
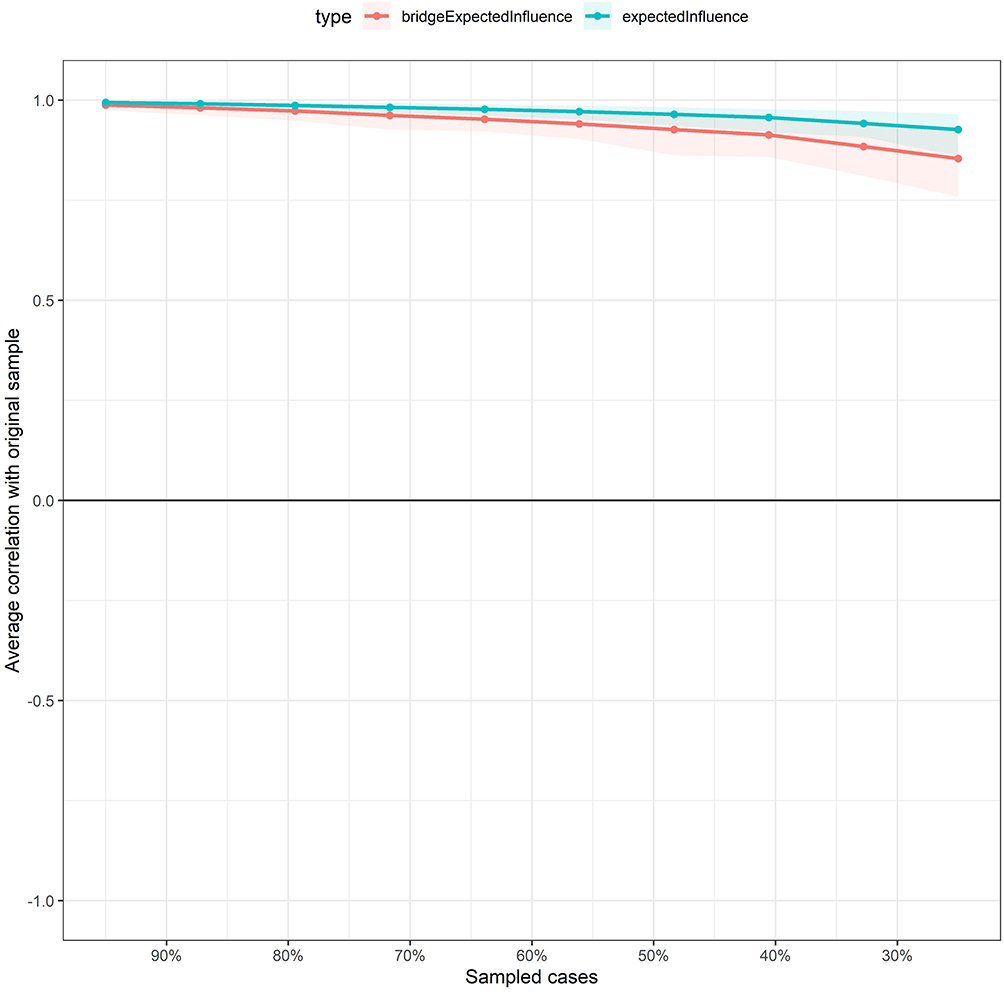 |
Figure 4 Stability of centrality and bridge centrality using the case-drop bootstrap. |
Flow Network Diagram of the NSSI
Figure 5 depicts a flowchart of the network structure of NSSI about insomnia and anxiety symptoms. Seven nodes located in the diagram are directly related to NSSI, and each of the remaining nodes is indirectly related to NSSI. Specifically, it indicated that PHQ9 “suicidal ideation” (edge weight = 0.33), PHQ6 “self feeling” (edge weight = 0.09) were more strongly associated with NSSI.
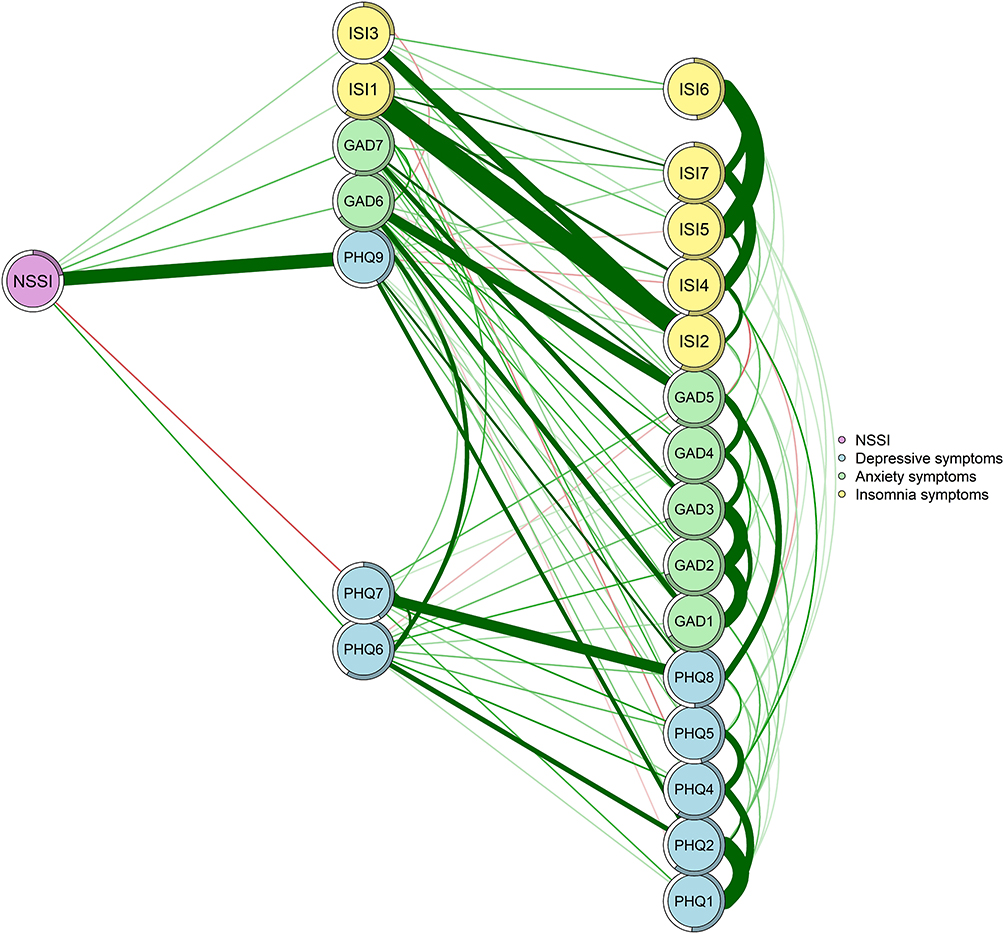 |
Figure 5 Flow network diagram of NSSI. |
Network Comparison
The network structures across subgroups after network comparison are visualized in Figure 6. Notably, all subnetworks exhibited clustering of symptoms within distinct communities, with the strongest edges consistently occurring within the same fixed communities across networks. Results from network invariance tests indicated that, after Benjamini-Hochberg (BH) correction, the global network structure did not significantly differ between the NSSI and non-NSSI (NSH) groups (M = 0.10, p = 0.715). However, a significant difference was observed in global strength (S = 0.384, p = 0.023), with the NSH group demonstrating higher overall connectivity (10.488 vs 10.104 in the NSSI group). This suggests stronger inter-node associations and more tightly interconnected symptoms in adolescents without self-injury. Network comparisons by gender showed no significant differences between boys and girls in global network structure (M = 0.08, p = 0.361) or global strength (males: 10.272 vs females: 10.436; S = 0.16, p = 0.274). Comparisons between only-child and non-only-child subgroups likewise revealed no significant differences in global network structure (M = 0.08, p = 0.551) or global strength (only-child: 10.446 vs non-only-child: 10.335; S = 0.11, p = 0.452).
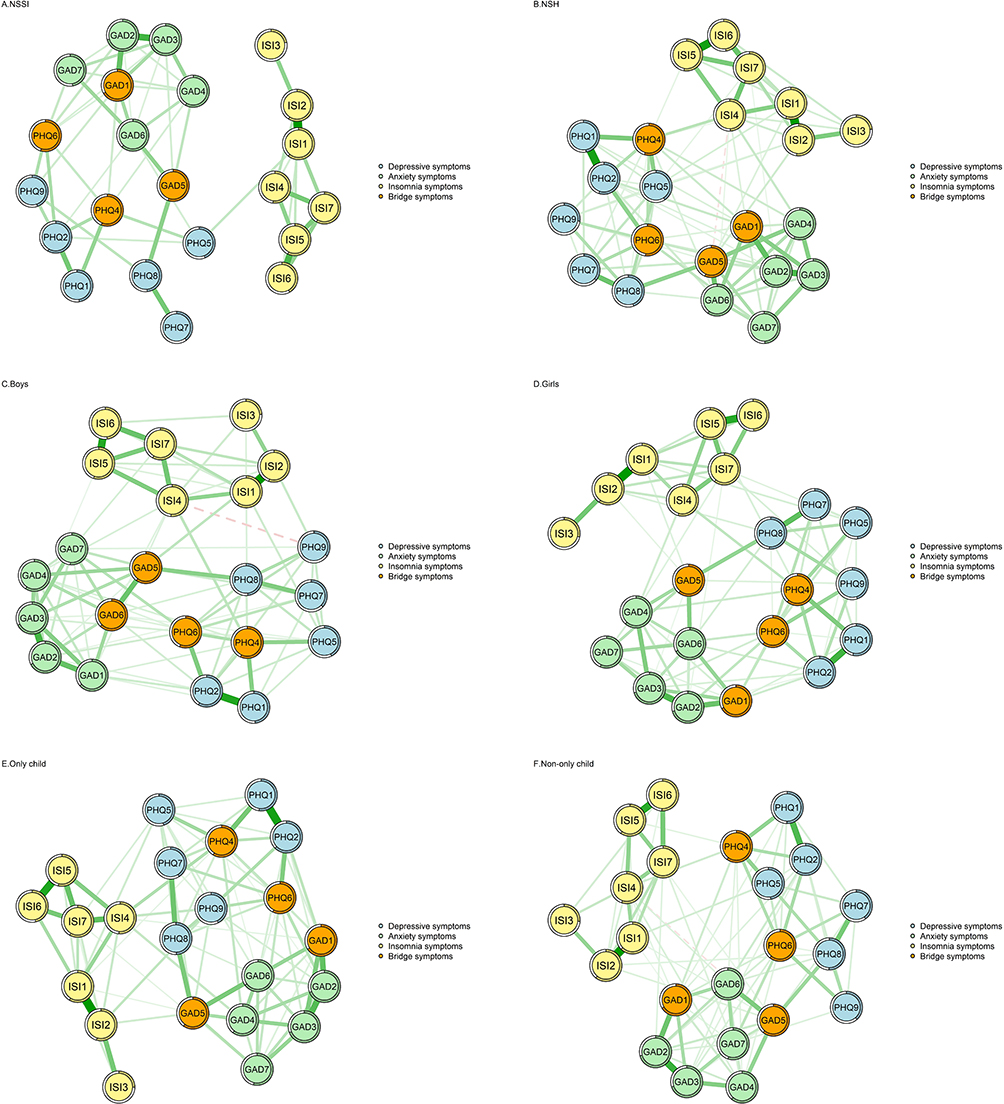 |
Figure 6 Comparison of sub-network structure. Notes: (A) Network structure of the NSH group. (B) Network structure of the NSSI group. (C) Network structure of boys. (D) Network structure of girls. (E) Network structure of only child. (F) Network structure of non-only-child. |
Discussion
In the present study, we constructed a symptom network of depression, anxiety and insomnia among junior high school students. The results indicated that worry-related symptoms, difficulty maintaining sleep and feelings of hopelessness emerged as the most influential nodes in the network. Bridge symptoms included restlessness, low energy, negative self-feeling and feeling nervous. Furthermore, the network symptom connections were denser in the NSH group compared to the NSSI group. Additionally, suicidal ideation exhibited the strongest association with NSSI.
Worry-related symptoms (uncontrollable worry and excessive worry) emerged as central symptoms in the network. Elevated worry represents a hallmark feature of generalized anxiety disorder, reflecting negative beliefs about potential threats and uncertainty.60 Prior research has provided mechanistic evidence supporting the central role of worry in generalized anxiety disorder among children and adolescents.61–63 Moreover, worry transcends multiple internalizing problems and has been identified as a repetitive negative thinking process that predicts risk for both anxiety and depression. Some studies have also suggested that worry tends to intensify at bedtime in adolescents, thereby impairing sleep onset and continuity.64 These theoretical and empirical findings robustly account for the prominent role of worry within the overall network. During adolescence, worries related to academic performance and interpersonal relationships commonly arise; addressing such worries is therefore crucial for preventing the escalation of further internalizing psychopathology and supporting healthy adolescent development. Related cognitive behavioral therapy interventions have demonstrated considerable efficacy.65
Difficulty maintaining sleep emerged as one of the strongest central symptoms in the model. It is typically characterized by nocturnal sleep fragmentation and difficulty returning to sleep after awakening, often resulting in sleep deprivation.66 This is consistent with prior network-analytic findings in insomnia, anxiety, and depression.67,68 Collectively, these results suggest that difficulty maintaining sleep may play a broadly important role in the psychopathological development of depression, anxiety, and insomnia across different populations. Insufficient sleep duration is common among adolescents. Sleep disturbances during neurodevelopment may disrupt neural plasticity and functional connectivity in the developing brain, thereby affecting the maturation of brain regions involved in emotion generation and emotion regulation and increasing vulnerability to affective disorders.12 In addition, hopelessness emerged as another core symptom. Middle-school students experience a developmental period marked by heightened academic evaluation, intensified peer comparison, and rapid changes in identity formation,69 and start to explore the concept of self and establish a foundation for self-awareness.70 They may become especially sensitive to whether they can meet their own expectations, making hopeless thoughts more likely under external influences. Hopelessness can undermine perceived control and motivation, thereby increasing the risk of affective disorders such as depression and generalized anxiety.71,72 Our findings further indicate that hopelessness functions as a key “activating” node within the overall symptom network. Therefore, identifying and correcting maladaptive hopeless beliefs in adolescents is both necessary and clinically meaningful.
Restlessness emerged as the most important bridge symptom in the network model, consistent with previous findings.49,73 This result suggests that restlessness may serve as a transdiagnostic marker of symptom severity within the internalizing spectrum and may function as a shared indicator of anxiety and insomnia among adolescents with emotional disorders.74 Mechanistically, restlessness may inhibit relaxation through exaggerated stress responses and physiological hyperarousal, thereby increasing the risk of insomnia in adolescents.75 Fatigue also exhibited high bridge centrality in the model, in line with prior studies in adolescent populations identifying fatigue as a transitional symptom linking depression and anxiety.73 This association may be related to dysfunctions in neuromodulatory systems involved in ascending arousal and motivational regulation, including noradrenaline, dopamine, acetylcholine, and histamine.76–78 Such dysregulation may further facilitate the broader co-occurrence and mutual reinforcement of depression, anxiety, and insomnia.79,80 Low self-worth and tension indicate that negative self-evaluation and heightened arousal states in adolescents warrant particular attention and should be prioritized as key targets for intervention. The bridging roles of low self-worth and tension indicate that negative self-evaluation and heightened arousal states in adolescents warrant particular attention and should be prioritized as key targets for intervention.
Flow network analyses of NSSI indicated that NSSI among adolescents was positively associated with multiple symptoms of depression, anxiety, and insomnia. Among these associations, suicidal ideation exhibited the strongest link with NSSI. This finding is consistent with a previous network analysis conducted in Chinese adolescents, which identified suicidal ideation as the symptom most strongly associated with NSSI.81 Prior research has further demonstrated that NSSI and suicidal behaviors are mutually predictive and frequently co-occur.82–84 The close association between these two phenomena was further confirmed in the present study. These findings suggest that, among middle-school students, NSSI and suicidal ideation do not occur in isolation but are jointly embedded within a broader psychological risk network characterized by depressive, anxious, and sleep-related problems. Accordingly, risk assessment and intervention strategies targeting this population should explicitly address the co-occurring risk of NSSI and suicidal ideation.
The overall patterns of symptom associations were largely similar between the NSSI and NSH groups. However, individuals with NSSI exhibited significantly lower connectivity among psychological symptoms compared to those without NSSI. This difference may reflect the high heterogeneity of psychological problems within the NSSI population. Previous research has shown that NSSI can occur across a wide range of psychological contexts and does not depend on any fixed constellation of symptoms.85,86 Accordingly, at the population level, individuals with NSSI may present with diverse types and severities of psychological symptoms that do not necessarily co-occur in a highly synchronized manner. In contrast, among individuals without NSSI but with psychological problems, symptoms of depression, anxiety, and insomnia tend to co-occur and mutually reinforce one another. These findings have significant implications, suggesting that in NSSI populations, the presence of a single symptom may be insufficient to capture overall psychological burden. Screening and risk assessment strategies based solely on comorbidity assumptions may therefore require more individualized and fine-grained approaches.
This study had a large sample size and applied network analysis to explore the comorbidity of insomnia and anxiety among Chinese middle school students. Some limitations should be noted. Our data are based on self-reports from middle school students and, therefore, may be subject to reporting biases. Subsequent studies may extend interviews or assessments by others to assess symptoms. A cross-sectional survey study employed undirected network analysis, which does not permit inferences about causal relationships or dynamics between individual symptoms. Further research should take cohort longitudinal studies to further explore the causal relationship between symptoms, thus reinforcing the reliability of the findings.
Conclusion
This study used network analysis to examine the relationships among anxiety, depression, insomnia, and NSSI. The results identified difficulty controlling worry, excessive worry, sleep maintenance problems, and hopelessness as core symptoms with the strongest centrality in the network. Restlessness, lack of energy, negative self-feeling, and nervousness emerged as core bridge symptoms linking different symptom domains. Notably, suicidal ideation showed the strongest association with NSSI. Additionally, the symptom network was more densely connected in the NSH group than in the NSSI group, indicating greater symptom interdependence. These findings highlight potential targets for early intervention and clinical prevention strategies.
Ethics Approval and Informed Consent
Hereby, the authors of this paper do consciously assure that this study has followed the guidelines and principles as set forth by the following ethical statement:
1. The body of work comprising this paper is entirely original and none of it has been previously published.
2. Prior to the start of the study, we obtained informed consent from the parents or legal guardians of all underage participants. At the same time, we also obtained informed consent from the underage participants themselves.
3. This study’s research methodology, the data collected, and findings were all conducted without anything being falsified or purposefully altered.
4. This study was approved by the Wuhan Medical Scientific Research Ethics Committee (Wuhan Municipal Health Commission, China). The ethics approval reference number is KY2021.11.01.
All procedures were conducted in accordance with relevant ethical guidelines and the Declaration of Helsinki.
Acknowledgments
We would like to thank all participants.
Funding
This research was supported by the National Natural Science Foundation of China (grant numbers: 72174152); Fundamental Research Funds for the Central Universities (grant numbers: 2042022kf1218 and 2042022kf1037).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Patton GC, Sawyer SM, Santelli JS, et al. Our future: a lancet commission on adolescent health and wellbeing. Lancet. 2016;387(10036):2423–16. doi:10.1016/S0140-6736(16)00579-1
2. Holder MK, Blaustein JD. Puberty and adolescence as a time of vulnerability to stressors that alter neurobehavioral processes. Front Neuroendocrinol. 2014;35(1):89–110. doi:10.1016/j.yfrne.2013.10.004
3. Cameron S, Brown VJ, Dritschel B, Power K, Cook M. Understanding the relationship between suicidality, current depressed mood, personality, and cognitive factors. Psychol Psychother. 2017;90(4):530–549. doi:10.1111/papt.12123
4. Uccella S, Cordani R, Salfi F, et al. Sleep deprivation and insomnia in adolescence: implications for mental health. Brain Sci. 2023;13(4):569. doi:10.3390/brainsci13040569
5. Zhang X, Yang H, Zhang J, Yang M, Yuan N, Liu J. Prevalence of and risk factors for depressive and anxiety symptoms in a large sample of Chinese adolescents in the post-COVID-19 era. Child Adolesc Psychiatr Ment Health. 2021;15(1):80. doi:10.1186/s13034-021-00429-8
6. Zhou J, Liu Y, Ma J, et al. Prevalence of depressive symptoms among children and adolescents in China: a systematic review and meta-analysis. Child Adolesc Psychiatr Ment Health. 2024;18(1):150. doi:10.1186/s13034-024-00841-w
7. Xu Q, Mao Z, Wei D, et al. Prevalence and risk factors for anxiety symptoms during the outbreak of COVID-19: a large survey among 373216 junior and senior high school students in China. J Affect Disord. 2021;288:17–22. doi:10.1016/j.jad.2021.03.080
8. Thapar A, Eyre O, Patel V, Brent D. Depression in young people. Lancet. 2022;400(10352):617–631. doi:10.1016/S0140-6736(22)01012-1
9. Zhang Y, Ye H, Huang M, et al. Changes in insomnia symptoms among compulsory education students in China after the “Double Reduction” policy: a two-wave longitudinal study. BMC Psychiatry. 2024;24(1):945. doi:10.1186/s12888-024-06414-7
10. Crowley SJ, Acebo C, Carskadon MA. Sleep, circadian rhythms, and delayed phase in adolescence. Sleep Med. 2007;8(6):602–612. doi:10.1016/j.sleep.2006.12.002
11. Gradisar M, Gardner G, Dohnt H. Recent worldwide sleep patterns and problems during adolescence: a review and meta-analysis of age, region, and sleep. Sleep Med. 2011;12(2):110–118. doi:10.1016/j.sleep.2010.11.008
12. Chellappa SL, Aeschbach D. Sleep and anxiety: from mechanisms to interventions. Sleep Med Rev. 2022;61:101583. doi:10.1016/j.smrv.2021.101583
13. Avenevoli S, Swendsen J, He JP, Burstein M, Merikangas KR. Major depression in the national comorbidity survey-adolescent supplement: prevalence, correlates, and treatment. J Am Acad Child Adolesc Psychiatry. 2015;54(1):37–44e2. doi:10.1016/j.jaac.2014.10.010
14. Alfano CA, Zakem AH, Costa NM, Taylor LK, Weems CF. Sleep problems and their relation to cognitive factors, anxiety, and depressive symptoms in children and adolescents. Depress Anxiety. 2009;26(6):503–512. doi:10.1002/da.20443
15. Blake MJ, Trinder JA, Allen NB. Mechanisms underlying the association between insomnia, anxiety, and depression in adolescence: implications for behavioral sleep interventions. Clin Psychol Rev. 2018;63:25–40. doi:10.1016/j.cpr.2018.05.006
16. Palmer CA, Bower JL, Cho KW, et al. Sleep loss and emotion: a systematic review and meta-analysis of over 50 years of experimental research. Psychol Bull. 2024;150(4):440–463. doi:10.1037/bul0000410
17. Haugland BSM, Hysing M, Baste V, et al. Sleep Duration and Insomnia in Adolescents Seeking Treatment for Anxiety in Primary Health Care. Front Psychol. 2021;12:638879. doi:10.3389/fpsyg.2021.638879
18. Gao T, Tao Y, Wang Q, et al. A bibliometric analysis of insomnia in adolescent. Front Psychiatry. 2023;14:1246808. doi:10.3389/fpsyt.2023.1246808
19. Verboom CE, Sijtsema JJ, Verhulst FC, Penninx BW, Ormel J. Longitudinal associations between depressive problems, academic performance, and social functioning in adolescent boys and girls. Dev Psychol. 2014;50(1):247–257. doi:10.1037/a0032547
20. Mathew GM, Reichenberger DA, Master L, Buxton OM, Chang AM, Hale L. Actigraphic sleep dimensions and associations with academic functioning among adolescents. Sleep. 2024;47(7). doi:10.1093/sleep/zsae062
21. Chiu K, Clark DM, Leigh E. Prospective associations between peer functioning and social anxiety in adolescents: a systematic review and meta-analysis. J Affect Disord. 2021;279:650–661. doi:10.1016/j.jad.2020.10.055
22. Wang M, Zheng H, Song L, Wang M, Zhou Y, Liu Z. Relational victimization, coping styles and depressive symptoms: a test of bidirectional associations in adolescence. J Youth Adolesc. 2025;54(5):1314–1325. doi:10.1007/s10964-024-02134-z
23. Liu X. Emotion dysregulation mediates the relationship between sleep problems and externalizing symptoms in early adolescents: a four-wave longitudinal study. J Affect Disord. 2024;363:221–229. doi:10.1016/j.jad.2024.07.058
24. Brieant A, Cai T, Ip KI, Holt-Gosselin B, Gee DG. Heterogeneity in developmental trajectories of internalizing and externalizing symptomatology: associations with risk and protective factors. Child Psychiatry Hum Dev. 2025. doi:10.1007/s10578-024-01804-0
25. Bone JK, Lewis G, Lewis G. The role of gender inequalities in adolescent depression. Lancet Psychiatry. 2020;7(6):471–472. doi:10.1016/S2215-0366(20)30081-X
26. Kaplan V. Gender sensitive psychiatry and feminist therapy. Cyp Turk J Psychiatry Psychol. 2021;3(3). doi:10.35365/ctjpp.21.3.22
27. Tang X, Tang S, Ren Z, Wong DFK. Prevalence of depressive symptoms among adolescents in secondary school in mainland China: a systematic review and meta-analysis. J Affect Disord. 2019;245:498–507. doi:10.1016/j.jad.2018.11.043
28. McLaughlin KA, King K. Developmental trajectories of anxiety and depression in early adolescence. J Abnorm Child Psychol. 2015;43(2):311–323. doi:10.1007/s10802-014-9898-1
29. Racine N, McArthur BA, Cooke JE, Eirich R, Zhu J, Madigan S. Global prevalence of depressive and anxiety symptoms in children and adolescents during COVID-19: a meta-analysis. JAMA Pediatr. 2021;175(11):1142–1150. doi:10.1001/jamapediatrics.2021.2482
30. Zhang J, Chan NY, Lam SP, et al. Emergence of sex differences in insomnia symptoms in adolescents: a large-scale school-based study. Sleep. 2016;39(8):1563–1570. doi:10.5665/sleep.6022
31. Chi X, Huang L, Wang J, Zhang P. The prevalence and socio-demographic correlates of depressive symptoms in early adolescents in china: differences in only child and non-only child groups. Int J Environ Res Public Health. 2020;17(2):438. doi:10.3390/ijerph17020438
32. He J, Zhong Y, Song Y, et al. The impact of only-child status on adolescent mental health: a multi-center cross-sectional study using propensity score matching in Western China. BMC Public Health. 2025;25(1):2140. doi:10.1186/s12889-025-23383-y
33. Sun J, Dunne MP, Hou X-Y. Academic stress among adolescents in China. Australas epidemiol. 2012;19(1):9–12.
34. Chen Z, Ren S, He R, et al. Prevalence and associated factors of depressive and anxiety symptoms among Chinese secondary school students. BMC Psychiatry. 2023;23(1):580. doi:10.1186/s12888-023-05068-1
35. Wolff JC, Thompson E, Thomas SA, et al. Emotion dysregulation and non-suicidal self-injury: a systematic review and meta-analysis. Eur Psychiatry. 2019;59:25–36. doi:10.1016/j.eurpsy.2019.03.004
36. Giletta M, Scholte RH, Engels RC, Ciairano S, Prinstein MJ. Adolescent non-suicidal self-injury: a cross-national study of community samples from Italy, the Netherlands and the United States. Psychiatry Res. 2012;197(1–2):66–72. doi:10.1016/j.psychres.2012.02.009
37. Baker AC, Wallander JL, Elliott MN, Schuster MA. Non-suicidal self-injury among adolescents: a structural model with socioecological connectedness, bullying victimization, and depression. Child Psychiatry Hum Dev. 2023;54(4):1190–1208. doi:10.1007/s10578-022-01319-6
38. Xiao Q, Song X, Huang L, Hou D, Huang X. Global prevalence and characteristics of non-suicidal self-injury between 2010 and 2021 among a non-clinical sample of adolescents: a meta-analysis. Front Psychiatry. 2022;13:912441. doi:10.3389/fpsyt.2022.912441
39. Liu S, You J, Ying J, Li X, Shi Q. Emotion reactivity, nonsuicidal self-injury, and regulatory emotional self-efficacy: a moderated mediation model of suicide ideation. J Affect Disord. 2020;266:82–89. doi:10.1016/j.jad.2020.01.083
40. Borschmann R, Becker D, Coffey C, et al. 20-year outcomes in adolescents who self-harm: a population-based cohort study. Lancet Child Adolesc Health. 2017;1(3):195–202. doi:10.1016/S2352-4642(17)30007-X
41. Liu RT, Steele SJ, Hamilton JL, et al. Sleep and suicide: a systematic review and meta-analysis of longitudinal studies. Clin Psychol Rev. 2020;81:101895. doi:10.1016/j.cpr.2020.101895
42. Jia Q, Wu Z, Liu B, et al. Exploring the longitudinal relationships between non-suicidal self-injury and depressive symptoms in adolescents: a cross-lagged panel network analysis. BMC Psychiatry. 2025;25(1):358. doi:10.1186/s12888-025-06806-3
43. Chen Y, Hu R, Xu X, et al. The effect of mental health status and family function on nonsuicidal self-injury: a longitudinal analysis of chinese children and adolescents. Psychol Res Behav Manag. 2023;16:4491–4500. doi:10.2147/PRBM.S429748
44. Liu X, Liu ZZ, Chen RH, et al. Nightmares are associated with future suicide attempt and non-suicidal self-injury in adolescents. J Clin Psychiatry. 2019;80(4). doi:10.4088/JCP.18m12181
45. Bauducco SV, Tilton-Weaver L, Gradisar M, Hysing M, Latina D. Sleep trajectories and frequency of non-suicidal self-injury in adolescents: a person-oriented perspective over two years. Sci Rep. 2025;15(1):1734. doi:10.1038/s41598-025-85779-5
46. Jiao T, Guo S, Zhang Y, et al. Associations of depressive and anxiety symptoms with non-suicidal self-injury and suicidal attempt among Chinese adolescents: the mediation role of sleep quality. Front Psychiatry. 2022;13:1018525. doi:10.3389/fpsyt.2022.1018525
47. McNally RJ. Can network analysis transform psychopathology? Behav Res Ther. 2016;86:95–104. doi:10.1016/j.brat.2016.06.006
48. Sun C, Zhu Z, Zhang P, et al. Exploring the interconnections of anxiety, depression, sleep problems and health-promoting lifestyles among Chinese university students: a comprehensive network approach. Front Psychiatry. 2024;15:1402680. doi:10.3389/fpsyt.2024.1402680
49. Bai W, Zhao YJ, Cai H, et al. Network analysis of depression, anxiety, insomnia and quality of life among Macau residents during the COVID-19 pandemic. J Affect Disord. 2022;311:181–188. doi:10.1016/j.jad.2022.05.061
50. Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606–613. doi:10.1046/j.1525-1497.2001.016009606.x
51. Plummer F, Manea L, Trepel D, McMillan D. Screening for anxiety disorders with the GAD-7 and GAD-2: a systematic review and diagnostic metaanalysis. Gen Hosp Psychiatry. 2016;39:24–31. doi:10.1016/j.genhosppsych.2015.11.005
52. Spitzer RL, Kroenke K, Williams JB, Lowe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006;166(10):1092–1097. doi:10.1001/archinte.166.10.1092
53. Morin CM, Belleville G, Belanger L, Ivers H. The insomnia severity index: psychometric indicators to detect insomnia cases and evaluate treatment response. Sleep. 2011;34(5):601–608. doi:10.1093/sleep/34.5.601
54. Smith MT, Wegener ST. Measures of sleep: the insomnia severity index, Medical Outcomes Study (MOS) sleep scale, Pittsburgh Sleep Diary (PSD), and Pittsburgh Sleep Quality Index (PSQI). Arthritis Care Res. 2003;49(S5):S184–S196. doi:10.1002/art.11409
55. Borsboom D, Robinaugh DJ, Psychosystems G, Rhemtulla M, Cramer AOJ. Robustness and replicability of psychopathology networks. World Psychiatry. 2018;17(2):143–144. doi:10.1002/wps.20515
56. Epskamp S, Borsboom D, Fried EI. Estimating psychological networks and their accuracy: a tutorial paper. Behav Res Methods. 2018;50(1):195–212. doi:10.3758/s13428-017-0862-1
57. van Borkulo CD, van Bork R, Boschloo L, et al. Comparing network structures on three aspects: a permutation test. Psychol Methods. 2023;28(6):1273–1285. doi:10.1037/met0000476
58. Opsahl T, Agneessens F, Skvoretz J. Node centrality in weighted networks: generalizing degree and shortest paths. Social Networks. 2010;32(3):245–251. doi:10.1016/j.socnet.2010.03.006
59. Van de geer S, Bühlmann P, Ritov Y, Dezeure R. On asymptotically optimal confidence regions and tests for high-dimensional models. Ann Stat. 2014;42(3). doi:10.1214/14-aos1221
60. Shipp L, Leigh E, Laverton A, Percy R, Waite P. Cognitive aspects of generalised anxiety disorder in adolescents: exploring intolerance of uncertainty, cognitive avoidance, and positive beliefs about worry. Child Psychiatry Hum Dev. 2025. doi:10.1007/s10578-025-01809-3
61. Songco A, Hudson JL, Fox E. A cognitive model of pathological worry in children and adolescents: a systematic review. Clin Child Fam Psychol Rev. 2020;23(2):229–249. doi:10.1007/s10567-020-00311-7
62. Ellis DM, Hudson JL. The metacognitive model of generalized anxiety disorder in children and adolescents. Clin Child Fam Psychol Rev. 2010;13(2):151–163. doi:10.1007/s10567-010-0065-0
63. Gosselin P, Langlois F, Freeston MH, Ladouceur R, Laberge M, Lemay D. Cognitive variables related to worry among adolescents: avoidance strategies and faulty beliefs about worry. Behav Res Ther. 2007;45(2):225–233. doi:10.1016/j.brat.2006.03.001
64. Heath M, Johnston A, Dohnt H, Short M, Gradisar M. The role of pre-sleep cognitions in adolescent sleep-onset problems. Sleep Med. 2018;46:117–121. doi:10.1016/j.sleep.2018.03.002
65. Hirsch CR, Beale S, Grey N, Liness S. Approaching cognitive behavior therapy for generalized anxiety disorder from a cognitive process perspective. Front Psychiatry. 2019;10:796. doi:10.3389/fpsyt.2019.00796
66. Babson KA, Trainor CD, Feldner MT, Blumenthal H. A test of the effects of acute sleep deprivation on general and specific self-reported anxiety and depressive symptoms: an experimental extension. J Behav Ther Exp Psychiatry. 2010;41(3):297–303. doi:10.1016/j.jbtep.2010.02.008
67. Mathew GM, Li X, Hale L, Chang AM. Sleep duration and social jetlag are independently associated with anxious symptoms in adolescents. Chronobiol Int. 2019;36(4):461–469. doi:10.1080/07420528.2018.1509079
68. Cai H, Zhao YJ, Xing X, et al. Network analysis of comorbid anxiety and insomnia among clinicians with depressive symptoms during the late stage of the COVID-19 pandemic: a cross-sectional study. Nat Sci Sleep. 2022;14:1351–1362. doi:10.2147/NSS.S367974
69. Li J, Zhang N, Yao M, Xing H, Liu H. Academic social comparison and depression in Chinese adolescents: the mediating role of basic psychological needs satisfaction. School Mental Health. 2021;13(4):719–729. doi:10.1007/s12310-021-09436-8
70. Pfeifer JH, Berkman ET. The development of self and identity in adolescence: neural evidence and implications for a value-based choice perspective on motivated behavior. Child Dev Perspect. 2018;12(3):158–164. doi:10.1111/cdep.12279
71. Liu RT, Kleiman EM, Nestor BA, Cheek SM. The hopelessness theory of depression: a quarter century in review. Clin Psychol. 2015;22(4):345–365. doi:10.1111/cpsp.12125
72. Scherer KR. Learned helplessness revisited: biased evaluation of goals and action potential are major risk factors for emotional disturbance. Cogn Emot. 2022;36(6):1021–1026. doi:10.1080/02699931.2022.2141002
73. He Y, Wu C, LeMoult J, et al. Exploring symptom-level associations between anxiety and depression across developmental stages of adolescence: a network analysis approach. BMC Psychiatry. 2023;23(1):941. doi:10.1186/s12888-023-05449-6
74. Aitken M, Andrade BF. Attention problems and restlessness as transdiagnostic markers of severity and treatment response in youth with internalizing problems. Res Child Adolesc Psychopathol. 2021;49(8):1069–1082. doi:10.1007/s10802-021-00797-x
75. Norell-Clarke A, Hagstrom M, Jansson-Frojmark M. Sleep-Related Cognitive Processes And The Incidence Of Insomnia Over Time: Does Anxiety And Depression Impact The Relationship? Front Psychol. 2021;12:677538. doi:10.3389/fpsyg.2021.677538
76. Kok A. Cognitive control, motivation and fatigue: a cognitive neuroscience perspective. Brain Cogn. 2022;160:105880. doi:10.1016/j.bandc.2022.105880
77. Van Egroo M, Koshmanova E, Vandewalle G, Jacobs HIL. Importance of the locus coeruleus-norepinephrine system in sleep-wake regulation: implications for aging and Alzheimer’s disease. Sleep Med Rev. 2022;62:101592. doi:10.1016/j.smrv.2022.101592
78. Sulaman BA, Zhang Y, Matosevich N, et al. Emerging functions of neuromodulation during sleep. J Neurosci. 2024;44(40). doi:10.1523/JNEUROSCI.1277-24.2024
79. Jesulola E, Micalos P, Baguley IJ. Understanding the pathophysiology of depression: from monoamines to the neurogenesis hypothesis model - are we there yet? Behav Brain Res. 2018;341:79–90. doi:10.1016/j.bbr.2017.12.025
80. Ross JA, Van Bockstaele EJ. The locus coeruleus- norepinephrine system in stress and arousal: unraveling historical, current, and future perspectives. Front Psychiatry. 2020;11:601519. doi:10.3389/fpsyt.2020.601519
81. Ma M, Xiao C, Ou W, et al. Depression and anxiety symptoms associated with internet addiction and non-suicidal self-injury in Chinese adolescent students - a network analysis. BMC Psychiatry. 2025;25(1):731. doi:10.1186/s12888-025-07131-5
82. Asarnow JR, Porta G, Spirito A, et al. Suicide attempts and nonsuicidal self-injury in the treatment of resistant depression in adolescents: findings from the TORDIA study. J Am Acad Child Adolesc Psychiatry. 2011;50(8):772–781. doi:10.1016/j.jaac.2011.04.003
83. Xu Z, Li N, Kong Y, et al. Nonsuicidal self-injury as the gateway and consequence of suicidal ideation among adolescents: a cross-lagged regression analysis. Front Psychiatry. 2024;15:1434191. doi:10.3389/fpsyt.2024.1434191
84. Hamza CA, Stewart SL, Willoughby T. Examining the link between nonsuicidal self-injury and suicidal behavior: a review of the literature and an integrated model. Clin Psychol Rev. 2012;32(6):482–495. doi:10.1016/j.cpr.2012.05.003
85. Kruzan KP, Hentges E, Ramirez I, Washburn JJ. Identifying subgroups of nonsuicidal self-injury: a systematic review. PLOS Ment Health. 2025;2(4). doi:10.1371/journal.pmen.0000291
86. de Neve-Enthoven NGM, Ringoot AP, Jongerling J, et al. Adolescent nonsuicidal self-injury and suicidality: a latent class analysis and associations with clinical characteristics in an at-risk cohort. J Youth Adolesc. 2024;53(5):1197–1213. doi:10.1007/s10964-023-01922-3
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Attention-Dominated Cognitive Dysfunction May Be a Biological Marker for Distinguishing SA from SI in Adolescents: A Network Analysis Study Based on Adolescent Depression
Wang Q, Wen M, Fan S, Liu J, Wang X, Guo W, Hu J, Zhang J, Li B, Zhang L, Zhang Y, Li K
Psychology Research and Behavior Management 2024, 17:945-956
Published Date: 6 March 2024
Internet Use Behavior and Adolescent Mental Health: The Mediating Effects of Self-Education Expectations and Parental Support
Du W, Fan Z, Li D, Wu M
Psychology Research and Behavior Management 2024, 17:1163-1176
Published Date: 13 March 2024
A Network Structure of Mental Health and Problematic Mobile Phone Use Among Middle School Students
Zhou M, Dong X, Wu W, Li Y
Psychology Research and Behavior Management 2024, 17:3533-3542
Published Date: 15 October 2024
Improving Diagnostic Strategies for Pediatric Anxiety Disorders: Advice for the Clinician
Hilliard W, Kearney K, Lucas S, Flores MED
Psychology Research and Behavior Management 2024, 17:4035-4042
Published Date: 25 November 2024
Food Intake and Mental Health Among Middle School Students in Shandong Province: A Network Analysis
Yao Y, Liao B, Feng J, Tang S, Zhang Z, Yang D, Yin X, Xie J, Yang L, Yin W
Psychology Research and Behavior Management 2025, 18:1839-1852
Published Date: 1 September 2025