Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
A Multidimensional Perspective on COPD: How Coping Styles and Self-Esteem Relate to Psychological Distress and Functional Capacity
Authors Pescaru CC, Crisan AF ![]() , Maritescu A, Tudorache E, Oancea C
, Maritescu A, Tudorache E, Oancea C
Received 9 September 2025
Accepted for publication 17 December 2025
Published 27 December 2025 Volume 2025:20 Pages 4143—4157
DOI https://doi.org/10.2147/COPD.S561817
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jill Ohar
Camelia Corina Pescaru,1,2 Alexandru Florian Crisan,2,3 Adelina Maritescu,2,4 Emanuela Tudorache,1,5 Cristian Oancea1,5
1Center for Research and Innovation in Personalized Medicine of Respiratory Diseases (CRIPMRD), “Victor Babes” University of Medicine and Pharmacy Timisoara, Timisoara, Romania; 2Pulmonary Rehabilitation Center, Clinical Hospital of Infectious Diseases and Pulmonology, “Victor Babes”, Timisoara, Romania; 3Research Center for Assessment of Human Motion, Functionality, and Disability, “Victor Babes” University of Medicine and Pharmacy Timisoara, Timisoara, Romania; 4Doctoral School, “Victor Babes” University of Medicine and Pharmacy Timisoara, Timisoara, Romania; 5Pulmonology Clinic, Clinical Hospital of Infectious Diseases and Pulmonology, “Victor Babes”, Timisoara, Romania
Correspondence: Alexandru Florian Crisan, Center for Research and Innovation in Personalized Medicine of Respiratory Diseases (CRIPMRD), “Victor Babes” University of Medicine and Pharmacy Timisoara, Timisoara, Romania, Email [email protected]
Purpose: Emerging evidence indicates that psychological resources may influence clinical outcomes and disease burden in chronic obstructive pulmonary disease (COPD), but their interactions are still not well understood. This study examined how coping strategies and self-esteem are connected to psychological distress, symptom impact, and functional capacity in moderate and severe COPD.
Patients and Methods: A cross-sectional study was conducted between December 2024 and July 2025 at a tertiary pulmonary center. Ninety-three patients with stable COPD were enrolled and classified into moderate (n = 43) and severe (n = 50) groups according to GOLD criteria. Assessments included spirometry, 6-minute walk test (6MWT), COPD Assessment Test (CAT), modified Medical Research Council (mMRC) scale, Hospital Anxiety and Depression Scale (HADS), Rosenberg Self-Esteem Scale (RSES), and the COPE inventory. Statistical analyses comprised group comparisons, correlation analyses with Benjamini–Hochberg correction, and multiple linear regression to identify independent predictors of coping styles.
Results: Severe COPD was associated with lower self-esteem (median RSES 18.5 vs 21, p < 0.0001), reduced 6MWT (203 m vs 300 m, p < 0.0001), higher anxiety (HADS-A 9.5 vs 7, p = 0.0001), and greater symptom burden (CAT 25 vs 19, p < 0.0001). These patients relied less on problem- (27 vs 31, p < 0.0001) and emotion-focused coping (23 vs 27, p < 0.0001), but more on avoidant coping (21 vs 19, p < 0.0001). Correlations showed that problem- and emotion-focused coping were linked to higher self-esteem and better 6MWT performance, whereas avoidant coping was related to greater dyspnea, higher CAT, and lower self-esteem. Regression analyses identified dyspnea severity (mMRC, p = 0.018) and lower FEV1% (p = 0.0003) as predictors of avoidant coping, while self-esteem (p = 0.036) and 6MWT % (p = 0.015) predicted adaptive coping.
Conclusion: Severe COPD is associated with greater psychological distress, reduced self-esteem, and reliance on avoidant coping. In contrast, higher self-esteem and better functional capacity favor adaptive coping strategies.
Plain Language Summary: Chronic obstructive pulmonary disease (COPD) is a long-lasting lung condition that makes breathing hard and impacts many parts of daily life. People with COPD often experience physical symptoms like breathlessness and reduced ability to exercise, along with psychological challenges such as anxiety, depression, and low self-esteem. How patients handle these challenges plays a key role in their overall well-being.
In this study, we examined how people with moderate and severe COPD cope with their illness. We included 93 patients and measured lung function, walking distance over six minutes, symptoms, levels of anxiety and depression, self-esteem, and coping strategies. Coping strategies are ways people try to manage stress and can be categorized into three types: problem-focused (actively dealing with challenges), emotion-focused (regulating feelings), and avoidant (withdrawing or ignoring problems).
We discovered that patients with severe COPD were more likely to depend on avoidant coping, which was associated with increased breathlessness and poorer lung function. Conversely, patients with higher self-esteem and better walking capacity tended to use more adaptive coping methods, such as problem- or emotion-focused strategies.
These findings suggest that, in addition to treating physical symptoms, it is crucial to support patients’ psychological resources. Enhancing self-esteem and promoting active coping could help people with COPD manage their condition more effectively, lessen distress, and improve their quality of life. Pulmonary rehabilitation programs, which combine exercise, education, and psychological support, may be the best way to accomplish this.
Keywords: COPD, coping strategies, self-esteem, anxiety, functional capacity, quality of life
Introduction
Chronic obstructive pulmonary disease (COPD) is a progressive respiratory condition marked by persistent airflow limitation and a considerable impact on patients’ physical and mental health.1 In addition to respiratory symptoms and functional limitations, patients with COPD often experience emotional disorders, especially depression and anxiety, which contribute to decreased quality of life and poorer prognosis.2,3 A study performed on over 200 patients with COPD has shown that some of these patients exhibit low levels of self-esteem.4 Moreover, patients’ coping strategies vary significantly, influencing their perception of the disease, how they adapt to imposed limitations, and their psychological well-being.5
An exploratory qualitative study found that patients with COPD adopt various coping strategies, and their ability to adapt varies widely regardless of lung function severity. Some patients manage well despite respiratory deterioration, while others experience significant impacts on their quality of life, indicating that psychological factors differently influence how they perceive the disease.6 A qualitative meta-analysis found that COPD patients have significant emotional needs (frustration, depression, anxiety) and that the self-management process is lengthy and tailored, emphasizing differences in adaptation based on context and cultural resources.7
How patients cope with stress and symptoms affects their adherence to treatment, participation in pulmonary rehabilitation, and health-related behaviors. Certain coping styles (eg, active/problem-focused coping) are linked to better quality of life and more positive functional outcomes, while avoidant-focused or emotional-focused coping may be related to social isolation, depression, and worse clinical results.6,8 Recognizing dominant coping strategies allows for the customization of psychological and educational interventions for each patient.
In this context, assessing self-esteem and coping strategies, along with examining psychological and functional status, can offer a comprehensive view of how COPD patients adjust to their disease and the factors that impact their quality of life. Unlike our previous study,9 which focused on self-compassion, guilt, shame, and self-efficacy, the present research addresses coping strategies (problem-focused, emotion-focused, avoidant) and self-esteem. To our knowledge, this is the first study to systematically investigate the interplay between coping strategies, self-esteem, psychological distress, and functional outcomes in patients with moderate and severe COPD.
The objective of this study was to investigate coping patterns and their association with psychological status, symptom severity, and functional capacity in patients with moderate and severe COPD.
Materials and Methods
This observational, cross-sectional study was conducted at the Clinical Hospital for Infectious Diseases and Pneumophthisiology “Dr. Victor Babeș” in Timișoara, between December 2024 and July 2025. Patients were consecutively enrolled as they presented for scheduled follow-up visits, and only those with a confirmed diagnosis of COPD, established according to the Global Initiative for Chronic Obstructive Lung Disease (GOLD) criteria, were included.10
All patients were clinically stable during evaluation, with no exacerbations or therapy changes in the past four weeks. Maintenance inhaled treatment adhered to current GOLD guidelines, consisting of long-acting bronchodilators (LABA/LAMA) or triple therapy (ICS/LABA/LAMA) based on disease severity and clinical indications.
Patients were eligible for inclusion if they were aged 40 years or older, had a confirmed diagnosis of COPD according to the GOLD 2024 criteria, were in a clinically stable condition defined as the absence of exacerbations during the previous four weeks, and were able to complete all functional and psychological assessments specified in the protocol.10 Exclusion criteria included the presence of other chronic respiratory diseases, such as bronchial asthma, extensive bronchiectasis, or pulmonary fibrosis, as well as major neurological, psychiatric, or cognitive disorders that could interfere with test performance. Patients with severe locomotor disabilities preventing completion of the 6-minute walk test, those with unstable cardiovascular disease, or those unable to provide informed consent were also excluded.
Disease severity was classified based on post-bronchodilator FEV1 values (% of predicted value), according to the GOLD staging, with patients divided into moderate COPD and severe COPD groups.10
Demographic data, lung volumes (FVC, FEV1), COPD Assessment Test (CAT), and modified Medical Research Council (mMRC) scores, along with the distance walked on the 6-minute walk test (6MWT), were collected from each participant. Additionally, psychological assessments were performed using the Hospital Anxiety and Depression Scale (HADS), Rosenberg Self-Esteem Scale (RSES), and the COPE questionnaire for coping strategies. All assessments took place during a single study visit. After obtaining informed consent, demographic and clinical data were recorded first, followed by spirometry and the psychological questionnaires in a quiet and comfortable setting. The 6-minute walk test was conducted at the end of the session to prevent fatigue from affecting the questionnaire results.
Since one of the main goals of the study was to compare clinical, functional, and psychological features between moderate and severe COPD, all descriptive and comparative analyses were stratified based on GOLD-defined severity. Data on home non-invasive ventilation (nNIV) use and individual inhaled pharmacological treatment regimens were not collected, as these variables were outside the scope of the study. All patients were, however, receiving stable maintenance inhaled therapy according to GOLD recommendations.
The study was approved by the Ethics Committee of the Clinical Hospital for Infectious Diseases and Pneumophthisiology “Dr. Victor Babeș” Timișoara (no. 12197/17.12.2024), and all patients signed informed consent before inclusion in the research.
Sample Size Calculation
The minimum sample size was estimated using G*Power 3.1 software, for an independent samples t-test analysis, with the total coping score as the main variable. The calculated parameters were based on an expected mean difference according to the data reported in the literature for patients with COPD of different severities, a significance level of α = 0.05 and a statistical power of 80% (1–β = 0.80). The result indicated the need for a minimum number of 40 patients per group. 43 patients with moderate COPD and 50 with severe COPD were included in the study, exceeding the estimated minimum size.
Spirometry Assessment
Pulmonary function was evaluated using a COSMED Quark PFT system (COSMED, Rome, Italy), which was calibrated daily according to the manufacturer’s instructions. Measurements were performed following the recommendations of the American Thoracic Society and European Respiratory Society (ATS/ERS) standardization for spirometry.11 Forced vital capacity (FVC), forced expiratory volume in one second (FEV1), and the FEV1/FVC ratio were obtained from flow–volume curves recorded after the administration of a short-acting bronchodilator. Results were expressed as absolute values and as percentages of predicted values based on reference equations.
Functional Capacity
The 6-minute walk test (6MWT) was used to assess the functional capacity of patients with COPD, as recommended by the American Thoracic Society (ATS).12 The test measures the maximum distance a person can comfortably walk on a hard, flat surface within six minutes. The assessment was performed indoors, in a temperature-controlled environment, on a 30 m long straight corridor marked at regular intervals. A trained physiotherapist supervised all tests and provided standardized verbal encouragement at each minute according to ATS protocol. The total distance walked was recorded in meters. In patients with COPD, a distance of less than 350 m is frequently associated with severe functional limitations and poor prognosis.13
Anxiety and Depression Evaluation
Levels of anxiety and depression were assessed using the Hospital Anxiety and Depression Scale (HADS), a self-report questionnaire consisting of 14 items, each rated on a 4-point Likert scale (0–3).14 The questionnaire is divided into two subscales: anxiety (HADS-A) and depression (HADS-D), each containing seven items, with the score for each subscale ranging from 0 to 21. Scores between 8 and 10 indicate the presence of symptoms of moderate intensity, and scores ≥11 suggest significant symptomatology, compatible with a possible clinical diagnosis.14 The total score results from the summation of the two subscales and reflects the global level of emotional impairment.
Self-Esteem Assessment
Self-esteem was assessed using the Rosenberg Self-Esteem Scale (RSES), a commonly used psychometric instrument for measuring an individual’s overall evaluation of themselves.15 The questionnaire consists of 10 items formulated as statements, each rated on a 4-point Likert scale, from 0 (“totally disagree”) to 3 (“totally agree”). Five of the items assess positive aspects of self-esteem, and the other five target negative aspects, which are scored in reverse. The total score ranges from 0 to 30, with higher values indicating higher levels of self-esteem.16
Coping Strategies
Coping strategies were assessed using the Coping Orientation to Problems Experienced (COPE) Inventory, the 60-item extended version, developed by Carver et al. This questionnaire is a self-report instrument that measures a wide range of cognitive and behavioral responses used by individuals to cope with stressful situations.17 The items are grouped into 15 subscales, each subscale containing four questions. Responses are recorded on a 4-point Likert scale, from 1 (“I usually don’t do this at all”) to 4 (“I usually do this a lot”), with higher scores indicating more frequent use of the respective strategy.
In the literature, these subscales are often aggregated into three major dimensions: problem-focused coping, emotion-focused coping, and avoidant-focused coping.18 Scores for each dimension are obtained by summing the values of the corresponding items, with higher values reflecting a more intense use of that coping strategy.
In the present study, these three coping patterns were analyzed based on the theoretical framework proposed by Carver et al. Problem-focused coping, which includes active coping, planning, and the use of instrumental support, reflects efforts aimed at solving or managing the problem causing distress. Emotion-focused coping, encompassing positive reinterpretation, acceptance, humor, and the use of emotional support, aims to regulate emotional responses to stress. Avoidant-focused coping, which includes denial, behavioral disengagement, and substance use, represents strategies of withdrawal or escape from the stressor rather than directly managing it.18
Symptom Impact Assessment
The impact of symptoms on quality of life was assessed using the COPD Assessment Test (CAT), a validated and easy-to-administer questionnaire for patients with COPD.19 It contains 8 items covering aspects such as cough, sputum production, chest tightness, dyspnea on exertion, limitations in daily activities, confidence to leave the house, sleep quality and energy level. Each item is rated from 0 to 5, resulting in a total score ranging from 0 to 40, where higher scores indicate a more severe impact of the disease. The impact classification is as follows: low impact (0–9 points), moderate impact (10–20 points), high impact (21–30 points) and very high impact (31–40 points).20
Severity of dyspnea was assessed using the Modified Medical Research Council Dyspnea Scale (mMRC), a standardized instrument commonly used in clinical practice for patients with COPD.21 The mMRC scale comprises five grades, from 0 to 4, each corresponding to a description of the limitation caused by dyspnea in daily activities. Grade 0 indicates that dyspnea occurs only with strenuous exercise, while grade 1 refers to feeling short of breath when walking quickly or climbing a slight incline. Grade 2 describes walking slower than people of the same age due to dyspnea or having to stop to breathe while walking at a normal pace. At grade 3, the patient must stop to breathe after about 100 meters or after a few minutes of walking on level ground, and grade 4 reflects dyspnea so severe that it prevents leaving the house or occurs with very light activities, such as getting dressed or undressed.21
Statistical Analysis
Continuous variables were expressed as mean ± standard deviation or median [interquartile range – IQR], depending on the distribution assessed by normality tests and inspection of graphs. Normality of distributions was tested using the Shapiro–Wilk test, and homogeneity of variances was assessed using Levene’s test. Categorical variables were presented as absolute frequencies and percentages.
Comparison of clinical and psychological characteristics between patients with moderate and severe COPD was performed using Student’s t test for normally distributed variables, Mann–Whitney U for nonparametric distributions and χ2-test for categorical variables. Differences in coping scores between ordinal clinical categories defined by level of anxiety (HADS), depression (HADS), impact of illness (CAT) and dyspnea (mMRC) were assessed by one-way ANOVA, followed by post-hoc analyses with correction for multiple testing, reporting F statistics, degrees of freedom and p-values.
Correlations between coping strategies and clinical/psychological measures were evaluated using Spearman’s rank correlation coefficient (ρ), with 95% confidence intervals (CI). To control for the false discovery rate (FDR) given multiple testing, the Benjamini–Hochberg (BH) correction was applied to correlation p-values. Multiple linear regression models were then constructed to identify predictors of avoidant-, emotion-focused, and problem-focused coping. For each model, unstandardized coefficients (B), standardized coefficients (β), standard errors (SE), and p-values were reported. Model performance was expressed as R2, adjusted R2, F statistic, and model p-value. Statistical significance was set at p < 0.05 after correction.
Cronbach’s α coefficient showed good internal consistency for the Rosenberg Self-Esteem Scale (α = 0.88), the HADS anxiety subscale (α = 0.81), the HADS depression subscale (α = 0.83), and the COPD Assessment Test (α = 0.86), and acceptable consistency for the COPE questionnaire (α = 0.79).
Results
Sample Characteristics
The study included 93 patients, of whom 43 had moderate COPD and 50 had severe COPD. Significant clinical and psychological differences were observed between the two groups. Patients with severe COPD presented a higher symptom burden, more comorbidities, and greater levels of anxiety and overall psychological distress. Notably, self-esteem scores were significantly lower in the severe group. In terms of coping profiles, severe COPD was associated with reduced use of problem- and emotion-focused strategies and a greater reliance on avoidant coping (Table 1).
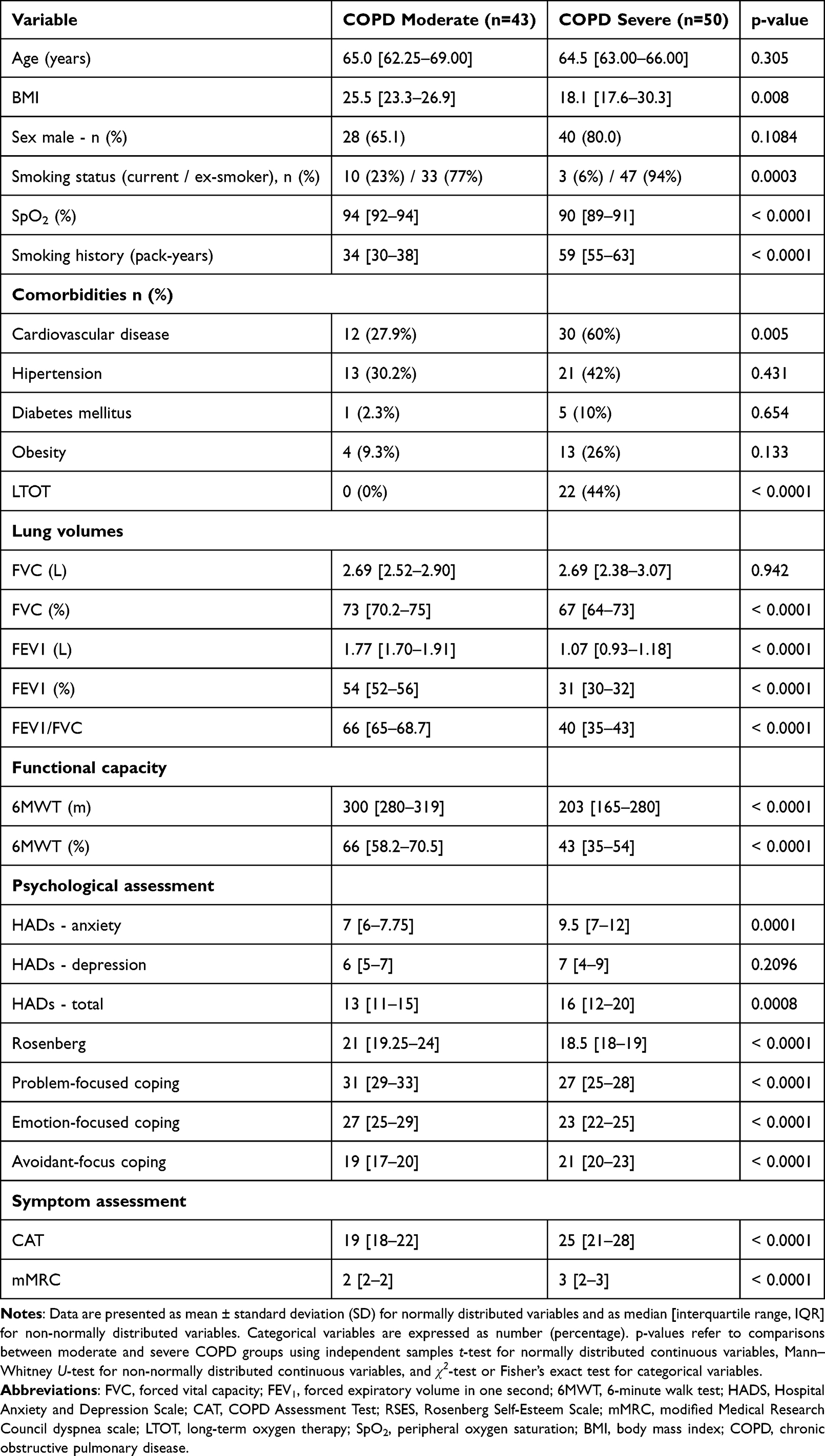 |
Table 1 Demographic, Clinical, Functional, and Psychological Characteristics of Participants, Stratified by COPD Severity |
Correlations Between Coping Strategies and Clinical Variables
As shown in Table 2 and visually depicted in Figure 1, the correlation analyses revealed consistent and clinically meaningful patterns connecting coping styles with psychological health, symptom severity, lung function, and functional capacity. Problem-focused coping aligned with a healthier clinical profile, being linked to lower anxiety and psychological distress, higher self-esteem, and better exercise performance and lung function. Emotion-focused coping showed a similarly positive pattern, associated with improved functional capacity, higher self-esteem, and reduced symptom burden and dyspnea. In contrast, avoidant coping consistently correlated with a less favorable profile, strongly associated with increased dyspnea, higher symptom burden, lower self-esteem, decreased lung function, and poorer performance on the 6-minute walk test.
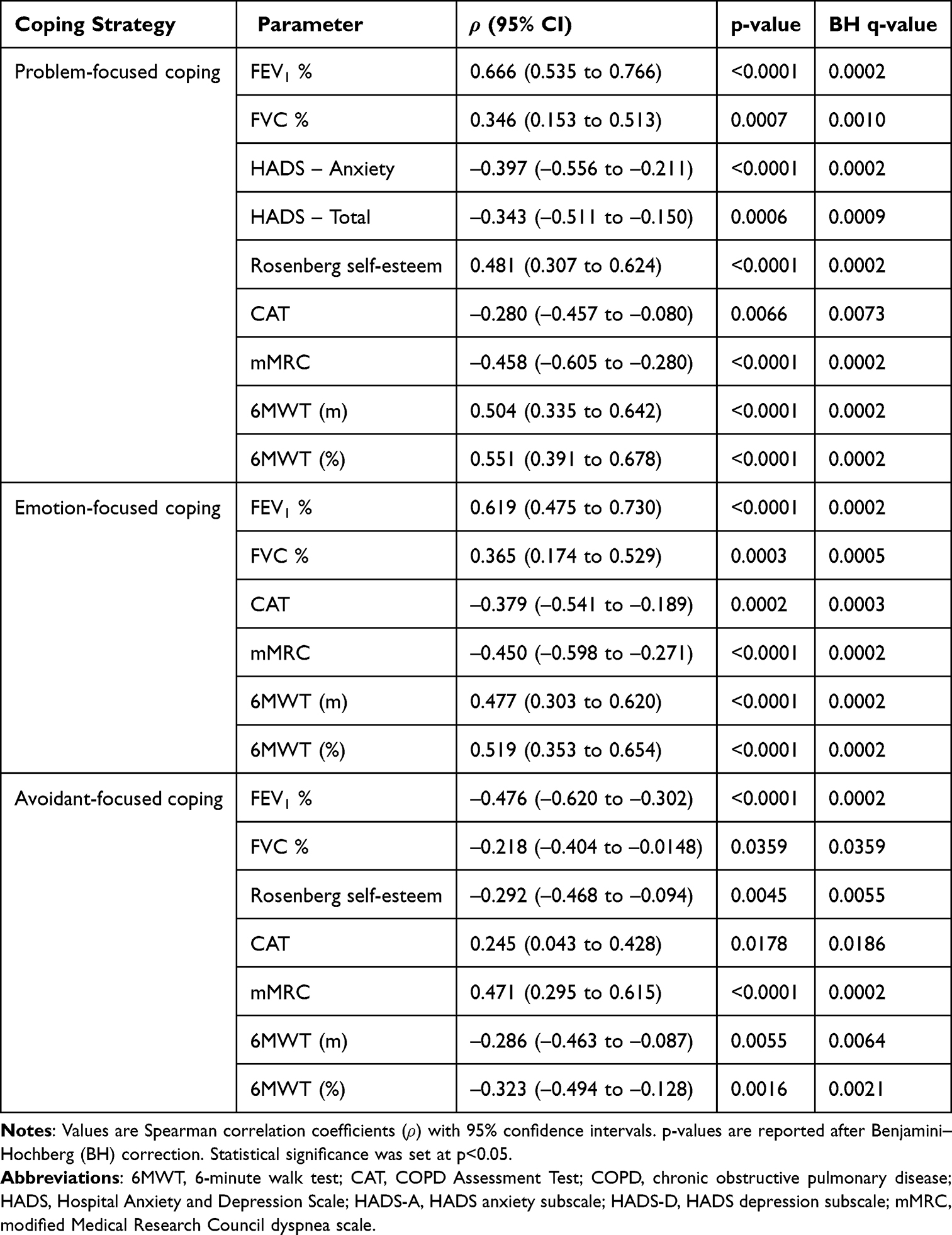 |
Table 2 Correlations Between Coping Strategies and Psychological, Symptomatic and Functional Parameters |
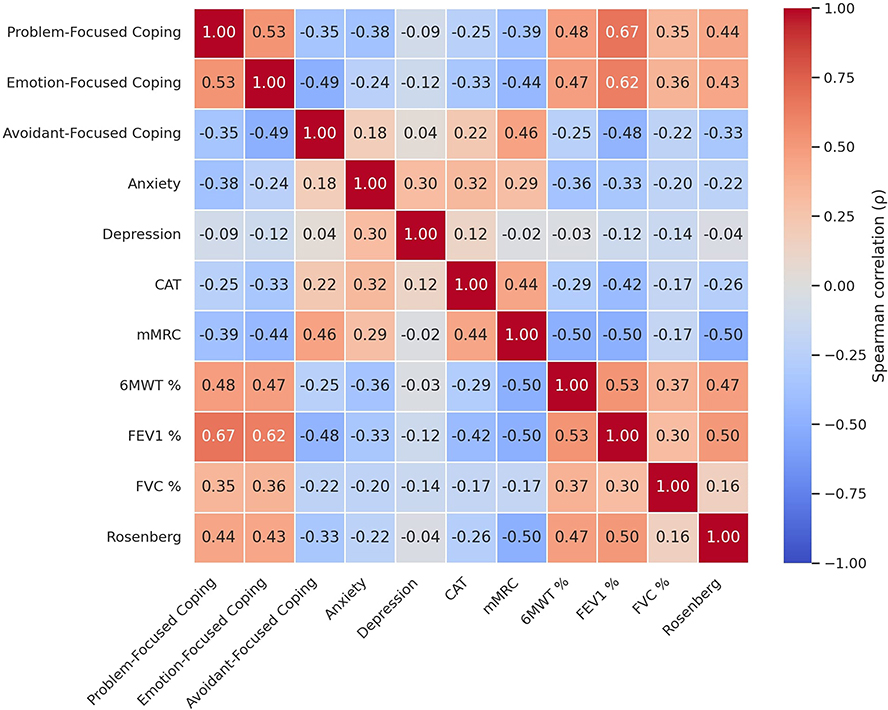 |
Figure 1 Correlations between coping strategies and psychological, symptomatic and functional parameters. |
Multiple Regression Analyses of Predictors of Coping Strategies
In the adjusted regression analyses, distinct predictors emerged for each coping strategy (Table 3).
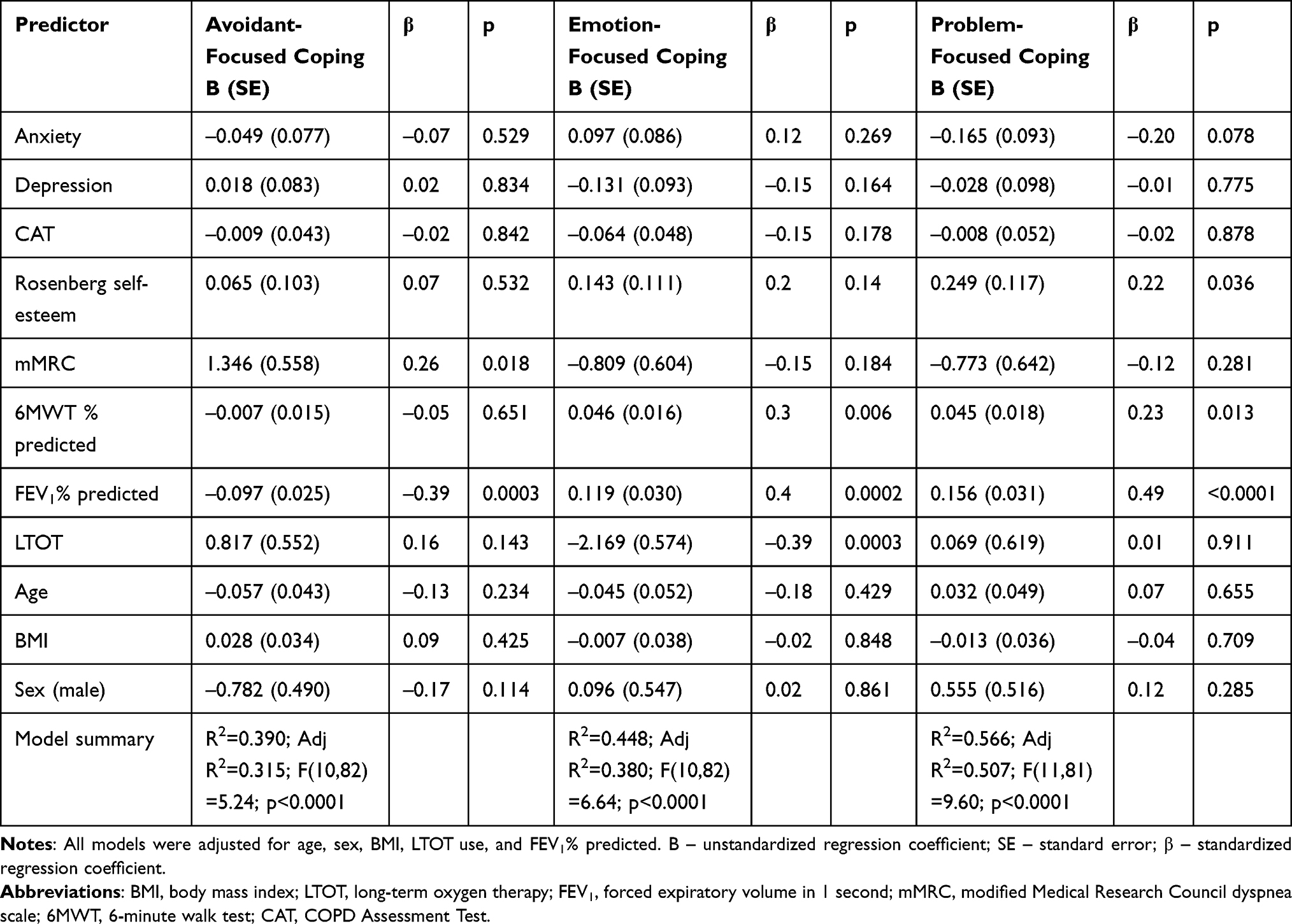 |
Table 3 Predictors of Avoidant-Focused, Emotion-Focused, and Problem-Focused Coping Identified Through Multiple Linear Regression |
For avoidant-focused coping, higher dyspnea severity (mMRC; B = 1.35, p = 0.018) and lower FEV1% predicted (B = –0.097, p = 0.0003) were significant independent predictors, accounting for 31.5% of the variance (Adj. R2 = 0.315, p < 0.0001).
For emotion-focused coping, lower FEV1% predicted (B = 0.119, p = 0.0002), use of LTOT (B = –2.17, p = 0.0003), and higher functional capacity (6MWT % predicted; B = 0.046, p = 0.006) were significant predictors. The model explained 38.0% of the variance (Adj. R2 = 0.380, p < 0.0001).
For problem-focused coping, higher self-esteem (Rosenberg; B = 0.249, p = 0.036), greater exercise capacity (6MWT % predicted; B = 0.045, p = 0.013), and higher FEV1% predicted (B = 0.156, p < 0.0001) independently predicted greater use of this strategy. The model explained the largest proportion of variance (Adj. R2 = 0.507, p < 0.0001).
Differences in Coping Strategies Across Psychological and Clinical Severity Levels
Patients were stratified according to official severity thresholds:
Anxiety and depression were classified using HADS scores as Normal (0–7), Borderline (8–10), and Abnormal (≥11).14
Disease impact was assessed with the CAT and categorized into Low (0–10), Medium (11–20), High (21–30), and Very high (31–40).20
Dyspnea severity was evaluated with the mMRC scale and grouped as Moderate (score 2) and Severe (score 3).21
Patients in the Normal anxiety group (HADS-A ≤7) reported significantly higher use of problem-focused and emotion-focused coping compared to those in the Abnormal group (HADS-A ≥11). For depression, emotion-focused coping was greater in the Normal group (HADS-D ≤7) compared to the Abnormal group (HADS-D ≥11).
Regarding disease impact, patients with medium CAT scores (11–20) reported significantly greater use of emotion-focused coping compared to those with high impact (21–30), while no significant differences were observed for the very high CAT group (≥31).
Regarding dyspnea, patients with severe symptoms (mMRC = 3) exhibited significantly higher avoidant-focused coping than those experiencing moderate dyspnea (mMRC = 2). Conversely, emotion-focused and problem-focused coping were more prominent in patients with moderate dyspnea compared to those with severe dyspnea. These differences are summarized in Table 4, which presents the distribution of coping strategies according to the severity of anxiety, depression, disease impact, and dyspnea. These differences are detailed in Supplementary Table 1.
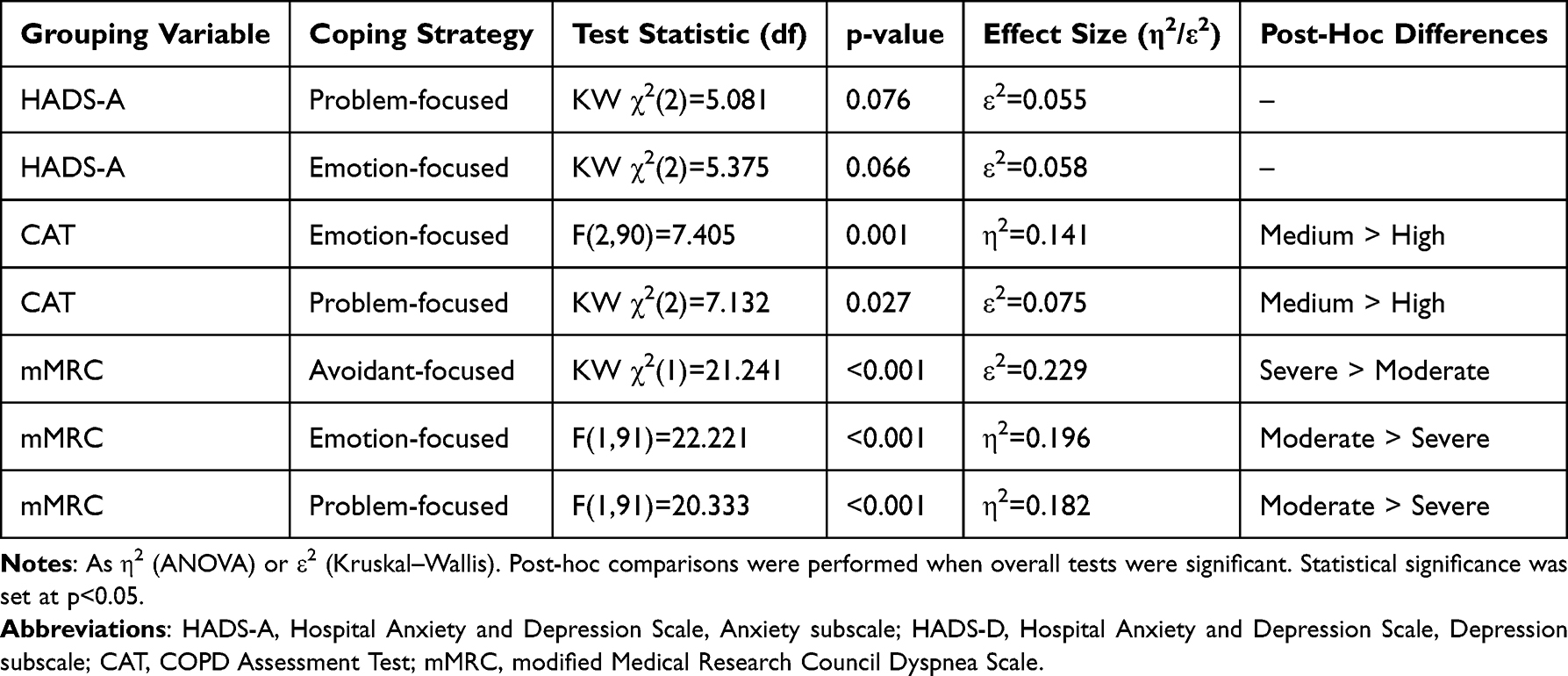 |
Table 4 Differences in Coping Strategies Depending on the Severity of Anxiety, Depression, Disease Impact, and Dyspnea |
Discussion
The primary goal of this study was to explore the coping strategies employed by patients with moderate and severe COPD and to analyze how these are related to psychological health, disease impact, and functional ability. Previous research from our group has shown that COPD severity is associated with self-conscious emotions such as guilt and shame, as well as with self-compassion and self-efficacy.9 The present study builds on that work by focusing instead on coping strategies (problem-focused, emotion-focused, avoidant) and self-esteem. By addressing these distinct psychological constructs, our analysis provides novel insights into the interplay between coping, self-esteem, symptom burden, and functional outcomes in COPD. We observed a clear and internally consistent pattern across clinical and psychological measures. Problem-focused and emotion-focused coping showed positive correlations with preserved lung function (FEV1%, FVC%), greater functional capacity (6MWT m and 6MWT%), and higher self-esteem, whereas avoidant-focused coping correlated with greater dyspnea severity (mMRC), higher symptom burden (CAT), and reduced exercise capacity. Self-esteem demonstrated positive associations with both adaptive coping styles and functional performance, while anxiety correlated moderately with higher CAT scores, higher mMRC levels, and lower 6MWT performance.
Coping is the collection of mental and behavioral strategies that individuals use to handle stress and respond to internal or external demands they perceive as surpassing their resources.22
Alongside coping, self-esteem is another crucial psychological resource, reflecting an individual’s overall sense of self-worth and competence.23 In patients with chronic diseases, including COPD, self-esteem is closely linked to emotional adjustment and health outcomes: higher self-esteem correlates with lower anxiety and depression,3 better treatment adherence, and greater participation in rehabilitation, while low self-esteem can increase psychological distress and decrease quality of life.24 Emerging evidence suggests that self-esteem can serve as a mediator in the pathway from psychosocial resources to psychological outcomes in chronic illness. For example, in a clinical population, self-esteem (along with self-efficacy) fully mediated the positive relationship between functional social support and mental well-being.25 Similarly, in a prospective study of end-stage renal disease, self-esteem mediated the effects of social and problematic support on depression and optimism.26 Extrapolating to COPD, these data suggest that enhancing self-esteem may attenuate the impact of maladaptive coping on psychological outcomes and engagement with rehabilitation.
In chronic diseases like COPD, coping mechanisms, defined as mental and behavioral strategies for adjusting to stress and demands, are crucial for managing the physical, psychological, and social limitations caused by the disease. These strategies are usually categorized into three types: problem-focused, emotion-focused, and avoidant-focused.17,27 Across chronic illnesses, coping strategies are key to psychological and social adjustment.28 In COPD specifically, coping styles are linked to psychological distress and patient-reported outcomes.29
Our results showed that patients with severe COPD had higher levels of anxiety and greater disease impact compared to those with moderate forms. When examining independent predictors, multivariable regression analyses showed that higher dyspnea severity (mMRC) and lower lung function (FEV1%) were the strongest predictors of avoidant-focused coping, while higher self-esteem and better exercise capacity (6MWT%) independently predicted the use of problem- and emotion-focused coping strategies.
These findings are consistent with data from the international literature. Brien et al showed that patients with COPD choose different coping strategies depending on the severity of the disease, which supports the differences observed in our cohort.6 One explanation is that as COPD advances, increasing symptom burden and functional limitations weaken patients’ perceived control, leading a shift away from active, problem-focused strategies toward emotion-focused or avoidant coping.30
Papava et al also reported that avoidant-focused coping is linked to higher levels of anxiety and depression, while problem-focused strategies are connected with better functional outcomes and higher self-esteem, results consistent with our findings on the role of 6MWT and Rosenberg scores.31 Avoidant coping can maintain psychological distress by fostering withdrawal, inactivity, and rumination, reinforcing a cycle of distress and reduced activity; whereas problem-focused coping enhances self-efficacy and treatment adherence, supporting functional improvement.32
At the same time, the observations of Rzadkiewicz et al, which indicate that adaptive strategies (active planning, distraction) contribute to post-rehabilitation benefits and a positive psychological state, confirm the importance of using problem- and emotion-focused strategies identified in our analysis.33 Adaptive coping strengthens psychological resilience by enhancing cognitive reframing and self-regulation, which in turn promotes engagement in rehabilitation and mental well-being.34
Although only a limited number of studies have explored coping in COPD,27 some nuances become apparent when our findings are compared with the existing literature. First, several sources suggest that the effects of emotion-focused coping are not consistent: in some contexts of chronic illness, it is described as potentially helpful (eg, humor, emotional expression for short-term regulation),22 while in other studies, it has been linked to worse psychological outcomes.35 Second, not all research has found clear links between coping styles and disease-related factors: for example, some reports found no significant relationship between coping and disease-specific health status,36 while others indicated that cognitive and perceptual factors were more strongly associated with psychological distress than disease severity itself.37
Mechanistically, these data indicate a circuit where physiological limitations (dyspnea, reduced respiratory function) trigger frustration and emotional distress, which in turn foster reliance on avoidant coping. Conversely, preserved exercise capacity and higher self-esteem appear to promote adaptive problem- and emotion-focused strategies. In contrast, avoidant strategies do not promote engagement in physical activity, potentially resulting in further physiological deconditioning and increased symptoms, including heightened perception of dyspnea. These psychological mechanisms coexist with biological pathways influenced by smoking exposure, including oxidative stress, which has recently been highlighted as a relevant contributor to COPD progression.38
Beyond its psychological importance, self-esteem may influence COPD stability and prognosis through changeable behavioral pathways. Lower self-esteem often comes with increased psychological distress and weaker self-management, which can lead to lower adherence to medications and non-drug treatments, delays in seeking help during symptom worsening, and less engagement in physical activity and rehabilitation. Psychological distress has been independently linked to a higher risk of acute exacerbations, hospitalizations, and death in COPD.39 In contrast, structured self-management and patient education programs that boost psychological engagement and confidence have been shown to lower hospital use and readmissions after exacerbations.40–42
The GOLD guidelines and recent research mainly focus on the prevalence and impact of anxiety and depression in COPD, but aspects like self-esteem and coping styles are less addressed. Our findings therefore complement existing data and underscore the importance of integrating these psychological factors into the comprehensive management of COPD.1,5,32,37,43
Given these psychological mechanisms, pulmonary rehabilitation (PR) serves as an ideal framework to address not only functional impairment but also maladaptive coping and low self-esteem in COPD. Pulmonary rehabilitation is a multidisciplinary intervention that combines exercise training, education, and psychosocial support, with well-established benefits in exercise capacity, dyspnea, and quality of life.44–48 Beyond physical improvements, PR has been shown to lessen anxiety and depression, partly by encouraging more adaptive coping strategies like problem-focused planning and acceptance.49 The study by Jacob et al showed that systematic psychological screening and personalized counseling (such as psychiatric support or by pulmonologists) in the context of PR can decrease psychological distress and enhance functional outcomes (FEV1, 6MWT) and quality of life.50 Recent guidelines from ATS/ERS highlight the importance of personalized approaches that incorporate psychological resources along with medical and functional assessments.51
Our study employed a multidimensional approach, combining objective assessments of lung function and functional capacity with validated psychometric tools for self-esteem, coping strategies, anxiety, and depression. This integrated analysis enabled us to understand the complex relationship between clinical and psychological factors in COPD. By comparing patients with moderate and severe disease, our findings offer valuable insights for customizing pulmonary rehabilitation programs, tailoring them not only to the physiological severity of the disease but also to the individual’s psychological profile.
Our study employed a multidimensional approach, combining objective assessments of lung function and functional capacity with validated psychometric tools for self-esteem, coping strategies, anxiety, and depression. This integrated analysis enabled us to understand the complex relationship between clinical and psychological factors in COPD. By comparing patients with moderate and severe disease, our findings offer valuable insights for customizing pulmonary rehabilitation programs, tailoring them not only to the physiological severity of the disease but also to the individual’s psychological profile.
This study has several limitations to consider when interpreting the results. First, the relatively small sample size and the selection of participants from a single tertiary center may limit how well the findings apply to the broader population with COPD. Second, the observational and cross-sectional design does not allow for establishing a cause-and-effect relationship between coping strategies, psychological status, and functional outcomes. Third, the absence of longitudinal follow-up prevents assessment of changes over time in coping styles or their potential response to interventions. Additionally, the interpretation of coping scores should be approached with caution, considering the self-reported nature of the questionnaire and possible influences from response bias or the participants’ momentary emotional states.
Future research should further investigate how self-esteem and coping strategies interact with disease impact and functional capacity in COPD. Since our findings showed that low self-esteem and the frequent use of avoidant strategies were linked to greater dyspnea severity and reduced lung function (FEV1%), as well as decreased 6MWT performance, longitudinal studies are necessary to determine if changes in self-esteem or coping styles predict clinical deterioration over time. Additionally, intervention studies should examine whether boosting self-esteem and encouraging problem-focused coping can reduce anxiety and depression, improve adherence to treatment, and support functional improvements during pulmonary rehabilitation. Tailored rehabilitation programs that include psychological screening and targeted support could thus be an effective way to enhance outcomes for patients with moderate and severe COPD.
Conclusion
Patients with severe COPD exhibited greater symptom burden, reduced functional capacity, and lower self-esteem. Regression analyses identified dyspnea severity and decreased FEV1% as key predictors of avoidant coping. Conversely, higher self-esteem and better 6MWT performance predicted more adaptive coping, highlighting the importance of incorporating psychological assessment into COPD management and rehabilitation.
Abbreviations
6MWT, Six-Minute Walk Test; ATS, American Thoracic Society; BH, Benjamini–Hochberg; BMI, Body Mass Index; CAT, COPD Assessment Test; CI, Confidence Interval; COPE, Coping Orientation to Problems Experienced; COPD, Chronic Obstructive Pulmonary Disease; ERS, European Respiratory Society; FEV1, Forced Expiratory Volume in one second; FVC, Forced Vital Capacity; GOLD, Global Initiative for Chronic Obstructive Lung Disease; HADS, Hospital Anxiety and Depression Scale; HADS-A, Hospital Anxiety and Depression Scale, Anxiety Subscale; HADS-D, Hospital Anxiety and Depression Scale, Depression Subscale; IQR, Interquartile Range; LTOT, Long-Term Oxygen Therapy; mMRC, Modified Medical Research Council Dyspnea Scale; PR, Pulmonary Rehabilitation; R2, Coefficient of Determination; RSES, Rosenberg Self-Esteem Scale; SE, Standard Error; SPSS, Statistical Package for the Social Sciences.
Data Sharing Statement
The datasets generated and analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
This cross-sectional study was conducted in accordance with the principles of the Declaration of Helsinki and received approval from the Ethics Committee of the Clinical Hospital for Infectious Diseases and Pneumophthisiology “Dr. Victor Babeș”, Timișoara (no. 12197/17.12.2024). All participants were informed about the study procedures and provided written informed consent prior to enrollment.
Consent for Publication
All authors have read and approved the final version of the manuscript and give their consent for its publication.
Acknowledgments
The publication costs of the present article were covered by “Victor Babes” University of Medicine and Pharmacy Timisoara.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. GOLD Report - Global Initiative for Chronic Obstructive Lung Disease - GOLD. 2025.
2. Yohannes AM, Alexopoulos GS. Depression and anxiety in patients with COPD. Eur Respir Rev. 2014;23(133):345–349. doi:10.1183/09059180.00007813
3. Rahi MS, Thilagar B, Balaji S, et al. The impact of anxiety and depression in chronic obstructive pulmonary disease. Adv Respir Med. 2023;91(2):123. doi:10.3390/arm91020011
4. Bonsaksen T, Fagermoen MS, Lerdal A. Factors associated with self-esteem in persons with morbid obesity and in persons with chronic obstructive pulmonary disease: a cross-sectional study. Psychol Health Med. 2015;20(4):431–442. doi:10.1080/13548506.2014.959529
5. Huang LM, Tan CY, Chen X, Jiang YJ, Zhou YR, Zhao H. A qualitative study on illness perception and coping behaviors among patients with chronic obstructive pulmonary disease: implications for intervention. Int J Chron Obstruct Pulmon Dis. 2024;19:2467–2479. doi:10.2147/COPD.S473790
6. Brien SB, Lewith GT, Thomas M. Patient coping strategies in COPD across disease severity and quality of life: a qualitative study. NPJ Prim Care Respir Med. 2016;26:16051. doi:10.1038/npjpcrm.2016.51
7. Russell S, Ogunbayo OJ, Newham JJ, et al. Qualitative systematic review of barriers and facilitators to self-management of chronic obstructive pulmonary disease: views of patients and healthcare professionals. NPJ Prim Care Respir Med. 2018;28(1):1–13. doi:10.1038/s41533-017-0069-z
8. Panagioti M, Scott C, Blakemore A, Coventry PA. Overview of the prevalence, impact, and management of depression and anxiety in chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2014;9:1289. doi:10.2147/COPD.S72073
9. Crisan AF, Pescaru CC, Maritescu A, Stoicescu ER, Carunta V, Oancea C. The impact of chronic obstructive pulmonary disease severity on psychological and functional outcomes: a cross-sectional analysis. J Clin Med. 2025;14(6):1865. doi:10.3390/jcm14061865
10. Venkatesan P. GOLD COPD report: 2024 update. Lancet Respir Med. 2024;12(1):15–16. doi:10.1016/S2213-2600(23)00461-7
11. Graham BL, Steenbruggen I, Barjaktarevic IZ, et al. Standardization of spirometry 2019 update. an official American Thoracic Society and European Respiratory Society technical statement. Am J Respir Crit Care Med. 2019;200(8):E70–E88. doi:10.1164/rccm.201908-1590ST
12. Crapo RO, Casaburi R, Coates AL, et al. ATS statement: guidelines for the six-minute walk test. Am J Respir Crit Care Med. 2002;166(1):111–117.
13. Cote CG, Casanova C, Marín JM, et al. Validation and comparison of reference equations for the 6-min walk distance test. Eur Respir J. 2008;31(3):571–578. doi:10.1183/09031936.00104507
14. Zigmond AS, Snaith RP. The Hospital Anxiety and Depression Scale. Acta Psychiatr Scand. 1983;67(6):361–370. doi:10.1111/j.1600-0447.1983.tb09716.x
15. Rosenberg M. Society and the Adolescent Self-Image. Princeton University Press; 1965.
16. Schmitt DP, Allik J. Simultaneous administration of the rosenberg self-esteem scale in 53 nations: exploring the universal and culture-specific features of global self-esteem. J Pers Soc Psychol. 2005;89(4):623–642. doi:10.1037/0022-3514.89.4.623
17. Carver CS, Scheier MF, Weintraub JK. Assessing coping strategies: a theoretically based approach. J Pers Soc Psychol. 1989;56(2):267–283. doi:10.1037/0022-3514.56.2.267
18. Litman JA. The COPE inventory: dimensionality and relationships with approach- and avoidance-motives and positive and negative traits. Pers Individ Dif. 2006;41(2):273–284. doi:10.1016/j.paid.2005.11.032
19. Jones PW, Harding G, Berry P, Wiklund I, Chen WH, Kline Leidy N. Development and first validation of the COPD assessment test. Eur Respir J. 2009;34(3):648–654. doi:10.1183/09031936.00102509
20. Gupta N, Pinto LM, Morogan A, Bourbeau J. The COPD assessment test: a systematic review. Eur Respir J. 2014;44(4):873–884. doi:10.1183/09031936.00025214
21. Bestall JC, Paul EA, Garrod R, Garnham R, Jones PW, Wedzicha JA. Usefulness of the Medical Research Council (MRC) dyspnoea scale as a measure of disability in patients with chronic obstructive pulmonary disease. Thorax. 1999;54(7):581–586. doi:10.1136/thx.54.7.581
22. Algorani EB, Gupta V. Coping mechanisms. Sexual Violence Abuse. 2023;1-2(1):102–104.
23. Bedrov A, Bulaj G. Improving self-esteem with motivational quotes: opportunities for digital health technologies for people with chronic disorders. Front Psychol. 2018;9(OCT):2126. doi:10.3389/fpsyg.2018.02126
24. Ji P, Zhang L, Gao Z, et al. Relationship between self-esteem and quality of life in middle-aged and older patients with chronic diseases: mediating effects of death anxiety. BMC Psychiatry. 2024;24(1):1–11. doi:10.1186/s12888-023-05459-4
25. Rippon D, Shepherd J, Wakefield S, Lee A, Pollet TV. The role of self-efficacy and self-esteem in mediating positive associations between functional social support and psychological wellbeing in people with a mental health diagnosis. J Ment Health. 2024;33(6):721–730. doi:10.1080/09638237.2022.2069695
26. Symister P, Friend R. The influence of social support and problematic support on optimism and depression in chronic illness: a prospective study evaluating self-esteem as a mediator. Health Psychol. 2003;22(2):123–129. doi:10.1037/0278-6133.22.2.123
27. Łuc M, Pawłowski M, Jaworski A, et al. Coping of chronically-ill patients during the COVID-19 pandemic: comparison between four groups. Int J Environ Res Public Health. 2023;20(6):4814. doi:10.3390/ijerph20064814
28. Bishop M, Park S, Livneh H, Rumrill P. Psychosocial adaptation to chronic illness and disability: a primer for counselors. Psychological Social Impact Chronic Illness Disability.
29. Soyseth TS, Dew MA, Lund MB, Haugstad GK, Soyseth V, Malt UF. Coping patterns and emotional distress in patients with chronic obstructive lung disease who are undergoing lung transplant evaluation. Prog Trans. 2020;30(3):228–234. doi:10.1177/1526924820933817
30. Shchaslyvyi AY, Antonenko SV, Telegeev GD. Comprehensive review of chronic stress pathways and the efficacy of behavioral stress reduction programs (BSRPs) in managing diseases. Int J Environ Res Public Health. 2024;21(8):1077. doi:10.3390/ijerph21081077
31. Papava I, Oancea C, Enatescu VR, et al. The impact of coping on the somatic and mental status of patients with COPD: a cross-sectional study. Int J COPD. 2016;11(1):1343–1351. doi:10.2147/COPD.S106765
32. Achury-Saldaña D, Duran De-Villalobos MM, Fuentes-Ramirez A. Self‐Efficacy in people with chronic disease: an evolutionary concept analysis. Nurs Open. 2025;12(7):e70276. doi:10.1002/nop2.70276
33. Rzadkiewicz M, Nasiłowski J. Psychosocial interventions for patients with severe COPD—an up-to-date literature review. Medicina. 2019;55(9):597. doi:10.3390/medicina55090597
34. Stepanian N, Larsen MH, Mendelsohn JB, Mariussen KL, Heggdal K. Empowerment interventions designed for persons living with chronic disease - a systematic review and meta-analysis of the components and efficacy of format on patient-reported outcomes. BMC Health Serv Res. 2023;23(1):911. doi:10.1186/s12913-023-09895-6
35. Hinch R, Sirois M, Sirois FM. A meta-analysis of coping strategies and psychological distress in rheumatoid arthritis. Br J Health Psychol. 2024;29(3):771–787. doi:10.1111/bjhp.12726
36. Stoilkova A, Janssen DJA, Franssen FME, Spruit MA, Wouters EFM. Coping styles in patients with COPD before and after pulmonary rehabilitation. Respir Med. 2013;107(6):825–833. doi:10.1016/j.rmed.2013.03.001
37. Thakur ER, Sansgiry S, Petersen NJ, et al. Cognitive and perceptual factors, not disease severity, are linked with anxiety in COPD: results from a cross-sectional study. Int J Behav Med. 2018;25(1):74–84. doi:10.1007/s12529-017-9663-2
38. Pezzuto A, Ricci A, Tammaro A. Oxidative stress in smokers with and without COPD: what variables are associated? Minerva Med. 2025;116(5).
39. Kham-Ai P, Heaton K, Xiao C, Wheeler P. Systematic review and meta-analysis of psychological distress and acute exacerbation of chronic obstructive pulmonary disease and consequences. Nurs Res. 2024;73(1):62–71. doi:10.1097/NNR.0000000000000694
40. Bourbeau J, Julien M, Maltais F, et al. Reduction of hospital utilization in patients with chronic obstructive pulmonary disease: a disease-specific self-management intervention. Arch Intern Med. 2003;163(5):585–591. doi:10.1001/archinte.163.5.585
41. Gadoury MA, Schwartzman K, Rouleau M, et al. Self-management reduces both short- and long-term hospitalisation in COPD. Eur Respir J. 2005;26(5):853–857. doi:10.1183/09031936.05.00093204
42. Jonkman NH, Westland H, Trappenburg JCA, et al. Do self-management interventions in COPD patients work and which patients benefit most? An individual patient data meta-analysis. Int J Chron Obstruct Pulmon Dis. 2016;11(1):2063–2074. doi:10.2147/COPD.S107884
43. Wang J, Ly L, Barson E, Smallwood N. Perceived barriers and facilitators to managing psychological distress in COPD: the perspectives of patients and carers – a qualitative study using the theoretical domains framework (TDF). NPJ Prim Care Respir Med. 2025;35(1):1–13. doi:10.1038/s41533-025-00430-0
44. Arnold MT, Dolezal BA, Cooper CB. Pulmonary rehabilitation for chronic obstructive pulmonary disease: highly effective but often overlooked. Tuberc Respir Dis. 2020;83(4):257. doi:10.4046/trd.2020.0064
45. Sohanpal R, Pinnock H, Steed L, et al. Tailored, psychological intervention for anxiety or depression in people with chronic obstructive pulmonary disease (COPD), TANDEM (Tailored intervention for ANxiety and DEpression Management in COPD): protocol for a randomised controlled trial. Trials. 2020;21(1):1–12. doi:10.1186/s13063-019-3800-y
46. Prasad R, Verma SK, Tonga KO, Oliver BG. Effectiveness of pulmonary rehabilitation for chronic obstructive pulmonary disease therapy: focusing on traditional medical practices. J Clin Med. 2023;12(14):4815. doi:10.3390/jcm12144815
47. Holland AE, Singh SJ, Casaburi R, et al. Defining modern pulmonary rehabilitation. an official American thoracic society workshop report. Ann Am Thorac Soc. 2021;18(5):E12–E29. doi:10.1513/AnnalsATS.202102-146ST
48. Smith SMS, Sonego S, Ketcheson L, Larson JL. A review of the effectiveness of psychological interventions used for anxiety and depression in chronic obstructive pulmonary disease. BMJ Open Respir Res. 2014;1(1):42. doi:10.1136/bmjresp-2014-000042
49. Farver-Vestergaard I, Buksted EH, Sørensen D, et al. Changes in COPD-related anxiety symptoms during pulmonary rehabilitation: a prospective quantitative and qualitative study. Front Rehab Sci. 2024;5:1428893. doi:10.3389/fresc.2024.1428893
50. Jacob A, Garg K, Dutta K, Saini V, Aggarwal D, Sidana A. Role of detailed psychological evaluation and treatment in pulmonary rehabilitation programs for patients with chronic obstructive pulmonary disease. Monaldi Arch Chest Disease. 2024;95(1). doi:10.4081/monaldi.2024.2849
51. Wouters EFM, Wouters BBREF, Augustin IML, Houben-Wilke S, Vanfleteren LEGW, Franssen FME. Personalised pulmonary rehabilitation in COPD. Eur Respir Rev. 2018;27(147):170125. doi:10.1183/16000617.0125-2017
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.