Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 19
A Multi-Omics Study of Comorbid Mechanisms Between Depression and Inflammatory Dermatoses Identifies FADS1 and TMEM258 as Therapeutic Targets
Authors Feng Y ![]() , Chen X, Qiu X, Zhang R, Cui Z, Mo X, Ju Q
, Chen X, Qiu X, Zhang R, Cui Z, Mo X, Ju Q
Received 6 March 2026
Accepted for publication 5 May 2026
Published 15 May 2026 Volume 2026:19 607365
DOI https://doi.org/10.2147/CCID.S607365
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Yibo Feng,1,* Xiang Chen,1,* Xinlan Qiu,1,* Runlin Zhang,2 Zhiyu Cui,3 Xiaohui Mo,1 Qiang Ju1
1Department of Dermatology, Renji Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, People’s Republic of China; 2Department of Dermatology, The First Affiliated Hospital of Harbin Medical University, Harbin, People’s Republic of China; 3Medical College, Shanxi Datong University, Datong, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiaohui Mo, Department of Dermatology, Renji Hospital, Shanghai Jiao Tong University School of Medicine, Pujian Road 160, Shanghai, 200127, People’s Republic of China, Email [email protected] Qiang Ju, Department of Dermatology, Renji Hospital, Shanghai Jiao Tong University School of Medicine, Pujian Road 160, Shanghai, 200127, People’s Republic of China, Email [email protected]
Background: Emerging evidence indicates a robust association between inflammatory dermatoses and mental disorders, likely driven by their combined impact on health and shared pathogenic mechanisms.
Purpose: Establishing the causal relationships between these two types of diseases and investigating their comorbid mechanisms.
Methods: We performed two-sample Mendelian randomization (TSMR) analyses using genome-wide association study (GWAS) summary statistics, examining causal links between six mental disorders and seven inflammatory dermatoses. To elucidate the underlying molecular basis, we implemented an integrative multi-omics framework comprising summary data-based Mendelian randomization (SMR), three-step SMR, TSMR, Bayesian colocalization, gene enrichment analysis and RNA sequencing data analysis.
Results: Meta-analysis and multiple testing correction revealed that genetic predisposition to depression increases the risk of psoriasis, while atopic dermatitis is causally associated with a higher risk of depression. Furthermore, we identified 14 genes potentially mediating the comorbidity between inflammatory dermatoses and mental disorders. Functional enrichment analyses and immune cell colocalization suggested the involvement of immunological pathways. Differential expression of several candidate genes was validated in transcriptomic datasets derived from affected tissues. Mediation analyses identified specific mediators and established their causal relationships with the identified genes. Finally, using genetic evidence and druggability assessments, we prioritized the therapeutic potential of these genes.
Conclusion: Causal relationships exist between various inflammatory dermatoses and mental disorders, with the most significant associations observed between depression and psoriasis, as well as between atopic dermatitis and depression. Fourteen genes are implicated in their comorbid mechanisms, with FADS1 and TMEM258 exhibiting the greatest potential as therapeutic targets.
Plain Language Summary: Psychodermatological disorders refer to skin diseases that are triggered or exacerbated by the interaction between skin conditions and psychological factors. These disorders include skin symptoms caused by psychological factors and psychological issues triggered by skin diseases. Both aspects intertwine, creating a vicious cycle. To date, no research has comprehensively explained the causal relationships and potential mechanisms behind the comorbidity of inflammatory skin diseases and mental disorders.
Our study aims to further investigate these disorders. We examined six common mental disorders—anxiety, depression, bipolar disorder, schizophrenia, post-traumatic stress disorder, and obsessive-compulsive disorder—and seven high-prevalence inflammatory skin diseases, including acne, rosacea, hidradenitis suppurativa, atopic dermatitis, contact dermatitis, eczema, and psoriasis. Through a comprehensive analysis of 26 Genome-Wide Association Study datasets from European populations, we confirmed that depression increases the risk of psoriasis, and that there is a causal relationship between atopic dermatitis and the high risk of depression. We then used Summary-based Mendelian Randomization analysis to identify 14 genes associated with these two comorbidities. The functions of these genes were validated through a series of data at the cellular, DNA, and RNA transcription levels. Finally, we evaluated the druggability of these genes using multiple drug databases. We identified Fatty Acid Desaturase 1 (FADS1) and Transmembrane Protein 258 (TMEM258) as the most promising therapeutic targets.
In summary, our findings provide new insights into the comorbid mechanisms between inflammatory skin diseases and mental disorders, paving the way for the development of targeted treatment strategies. The infographic titled ’Causal Multi-omics Framework’ outlines a series of steps involved in the framework. The first step, ’Bidirectional TSMR’, involves 26 GWAS studies focusing on conditions like psoriasis, depression and atopic dermatitis. The second step, ’SMR analysis’, examines 5 tissues and 14 selected genes. The third step, ’Sensitivity analysis’, includes 2 analyses: colocalization and TSMR. The fourth step, ’Multi-omics validation’, uses 3 methods: KEGG and GO, immune cell colocalization and RNA sequencing. The fifth step, ’Mediation analysis’, identifies 2 mediators: insomnia and unsaturated fatty acids. The final step, ’Priority ranking’, categorizes into 3 tiers based on scores: Tier 1 (score greater than or equal to 6), Tier 2 (score between 4.5 and 6) and Tier 3 (score less than 4.5), with a visual representation of total scores across tiers.Causal multi-omics: TSMR, SMR, sensitivity, validation, mediation, ranking.
Keywords: inflammatory dermatoses, mental disorders, summary data-based Mendelian randomization, atopic dermatitis, psoriasis, depression
Background
Inflammatory dermatoses are immune-mediated skin conditions without an infectious etiology, including disorders like acne vulgaris, eczema, psoriasis, rosacea, etc.1 These conditions can be triggered by various factors, such as infections, drug-induced hypersensitivity, autoimmune reactions, and environmental perturbations.2 Many patients with these diseases suffer from comorbidities, with mental disorders being increasingly recognized in recent studies.3 For instance, a meta-analysis encompassing 106 studies found that patients with atopic dermatitis (AD) are more likely to experience depression and suicidality, with approximately one in six patients with AD affected by clinical depression.4 Yi et al found altered brain activity in psoriasis patients similar to that in individuals with bipolar disorder (BD)5 Additionally, a meta-analysis by Chang et al confirmed that rosacea patients are more susceptible to anxiety and depression.6
As highlighted in the 2023 European White Paper on Psychodermatology, psychological factors significantly influence the progression and severity of various dermatological disorders.7 However, the mechanisms behind the comorbidity of inflammatory dermatoses and mental disorders remain poorly understood. While hypotheses suggest shared pathways like systemic inflammation and the brain-skin axis, there is limited genetic evidence supporting these theories.8,9 Recent Mendelian randomization studies have provided insights into this comorbidity.10–14 Despite these advances, the molecular mechanisms driving this comorbidity need further investigation.
This study explores the comorbidity of six mental disorders—namely, anxiety disorder, depression, BD, schizophrenia, post-traumatic stress disorder (PTSD), and obsessive-compulsive disorder (OCD)—with seven inflammatory dermatoses, including acne vulgaris, rosacea, hidradenitis suppurativa (HS), AD, contact dermatitis (CD), eczema, and psoriasis. Using two sets of consolidated genome-wide association study (GWAS) datasets, we conducted a two-sample Mendelian randomization (TSMR) study, meta-analysis and LD score regression (LDSC), confirming causal relationships between depression and both psoriasis and AD. We then integrated multi-omics data, including expression quantitative trait loci (eQTL), methylation quantitative trait loci (mQTL), and GWAS data. By employing a systematic approach, we combined TSMR, summary-data-based Mendelian randomization (SMR), colocalization methods and several other studies to delineate the genetic pathways connecting depression with these skin conditions.
By combining these approaches, we provided a more comprehensive understanding of the molecular mechanisms underlying the comorbidity between inflammatory dermatoses and mental disorders, paving the way for targeted therapeutic strategies.
Study Design
The research framework is depicted in Figure 1. We initially employed bidirectional TSMR to investigate the causal relationships between mental disorders and inflammatory dermatoses, utilizing GWAS data from the FinnGen study, large-scale European datasets, and the Psychiatric Genomics Consortium (PGC). GWAS datasets were selected according to phenotype relevance, sample size, ancestry information, and the availability of complete variant-level information. Before downstream analyses, summary statistics from different sources were standardized and harmonized by aligning variant identifiers, genomic coordinates, effect alleles, and effect directions where applicable. A meta-analysis was subsequently conducted to synthesize these findings, confirming the causal relationships between depression and psoriasis, as well as between AD and depression. LDSC analysis was further performed to assess cross-trait genetic correlation and provide complementary evidence for shared genetic architecture.
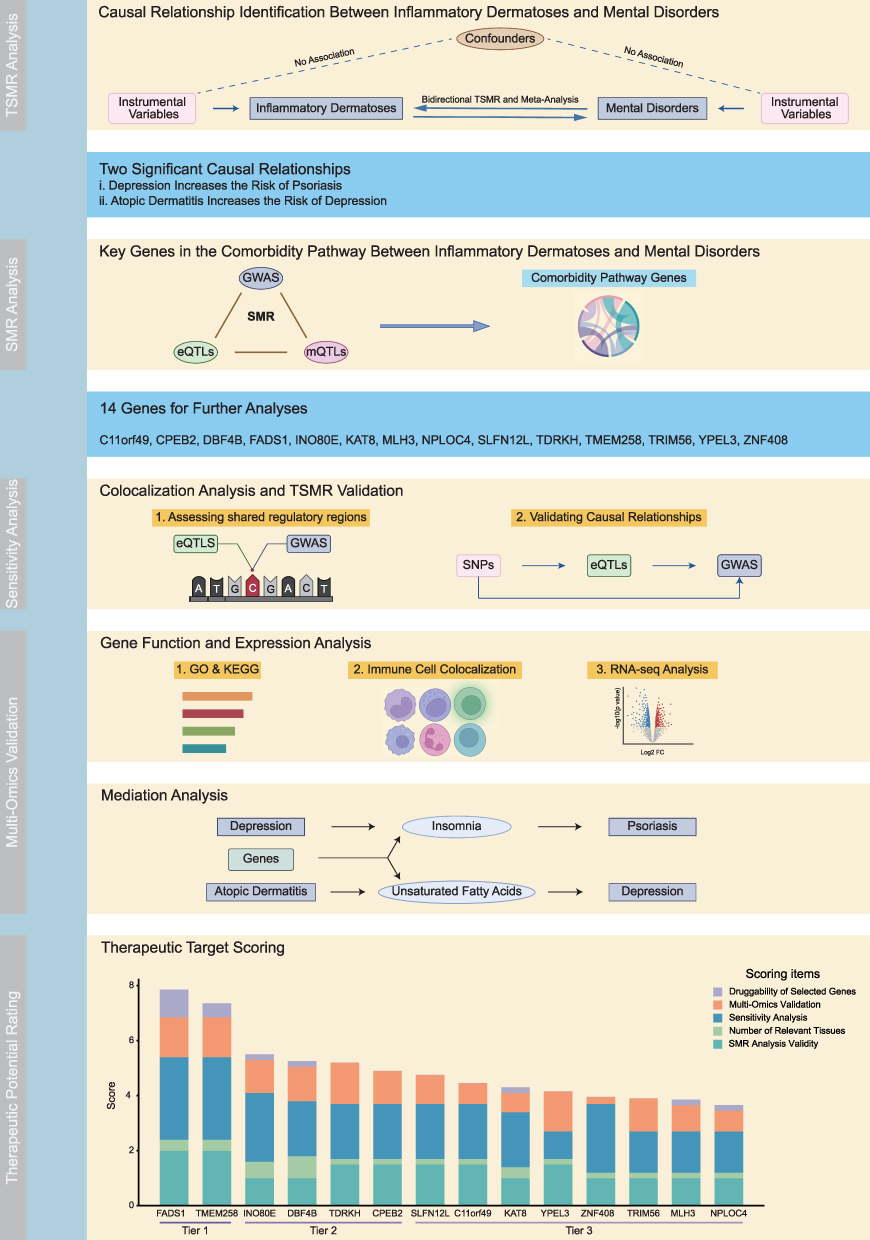 |
Figure 1 Overview of the study design. Created with BioRender.com. Abbreviations: eQTL, expression quantitative trait loci; GWAS, genome-wide association study; GO, gene ontology; KEGG, Kyoto Encyclopedia of Genes and Genomes; mQTL, methylation quantitative trait loci; RNA-seq, RNA sequencing; SMR, summary-data-based Mendelian randomization; TSMR, two-sample Mendelian randomization. |
Following this, eQTL instrumental variables derived from whole blood, skin, and brain, in conjunction with GWAS data for depression, psoriasis, and AD, were utilized to perform SMR and heterogeneity in dependent instruments (HEIDI) tests to identify genes significantly associated with the two related diseases. The tissue-specific eQTL datasets were selected based on their biological relevance to inflammatory dermatoses, mental disorders, and the brain-skin axis. To explore the epigenetic dimension, a three-step SMR analysis was applied, incorporating mQTLs associated with the GWAS of the three diseases, as well as mQTLs in relation to eQTLs, to identify methylation-regulated genes potentially involved in gene-expression regulation and disease susceptibility. Bayesian colocalization and TSMR were then employed to further validate the identified genes and reduce the likelihood that the observed associations were driven by linkage disequilibrium or inconsistent causal directions.
A total of 14 genes were selected for comprehensive functional analysis, including Gene Ontology (GO), Kyoto Encyclopedia of Genes and Genomes (KEGG) analysis, and immune cell-specific eQTL analysis. We also identified the mediating factors underlying the causal effects of depression on psoriasis and AD on depression, and applied TSMR to confirm the causal relationships between the target genes and mediating factors. Furthermore, publicly available GEO transcriptomic datasets for depression, psoriasis, and AD were analyzed to assess the differential expression of target genes across disease contexts. Finally, a multi-omics evidence-based scoring system was used to prioritize potential therapeutic targets by integrating evidence from MR, SMR, colocalization, methylation regulation, pathway enrichment, immune cell specificity, transcriptomic validation, and mediation analyses.
Detailed information on data sources, preprocessing procedures, software tools, parameter settings, and statistical thresholds is provided in the Supplementary Methods.
Results
TSMR and Meta-Analysis Identify Causal Relationships Between Inflammatory Dermatoses and Mental Disorders
A summary of the GWAS findings on inflammatory dermatoses and mental disorders is provided in Table 1. This study utilized genetic instruments, with each SNP showing an F-statistic exceeding the threshold of 10. Our findings on the causal relationships between inflammatory dermatoses and mental disorders are illustrated in Figure 2a and b.
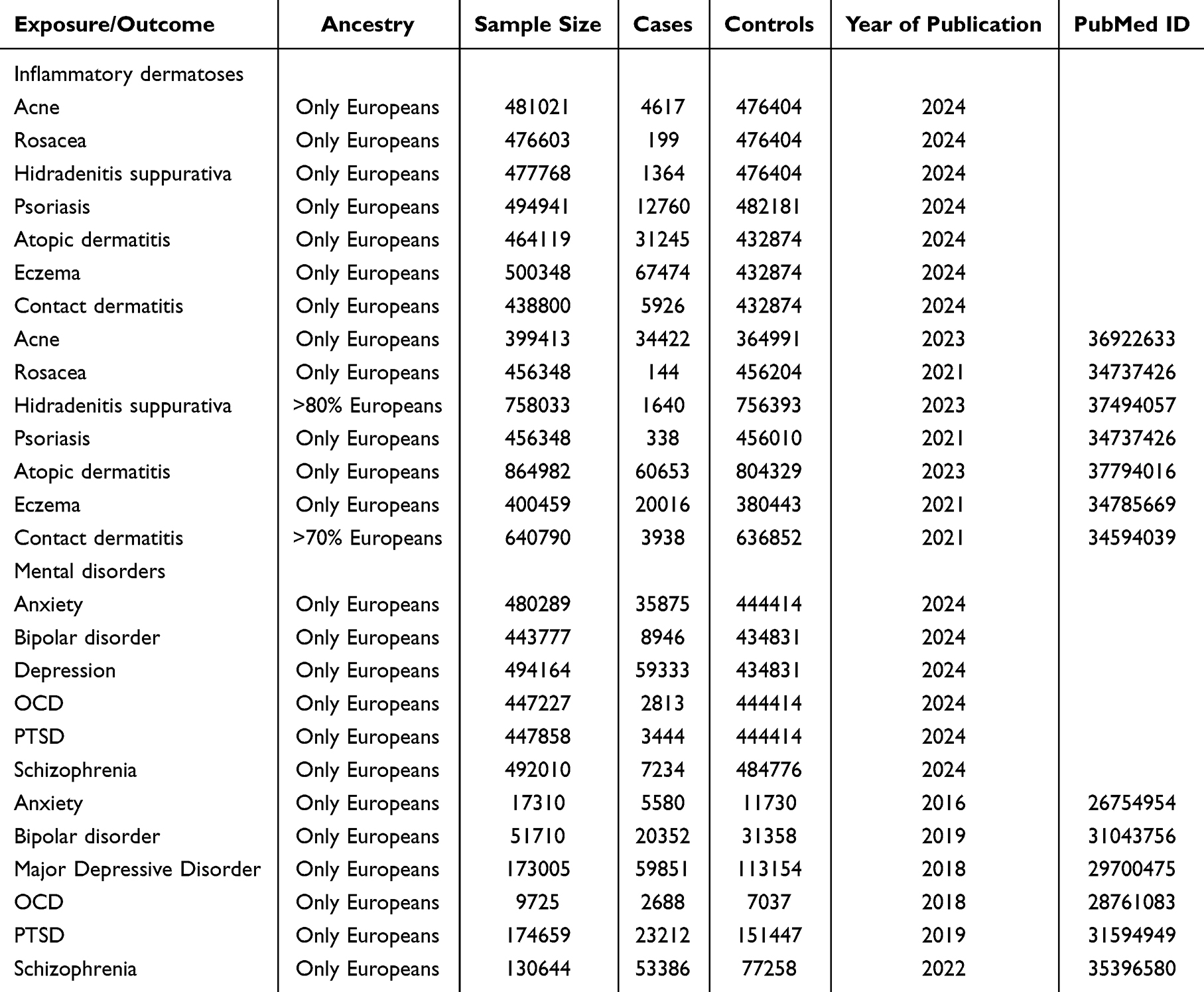 |
Table 1 Brief Description of Each GWAS Summary Statistics |
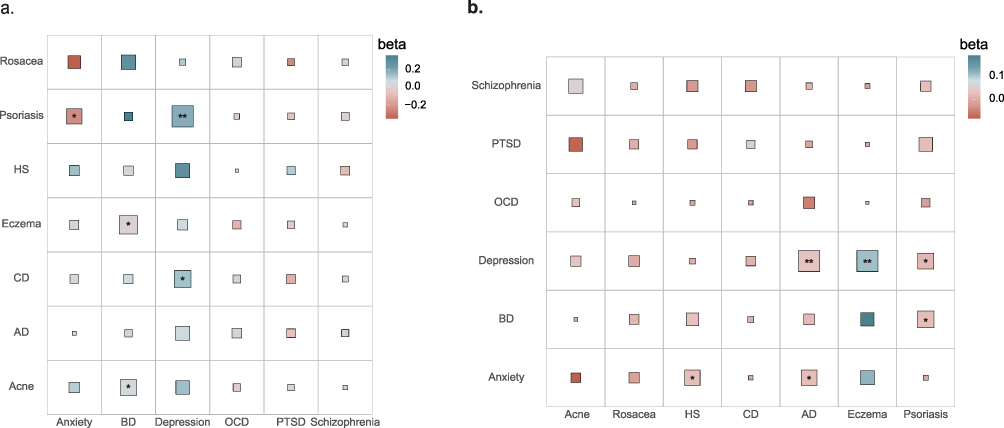 |
Figure 2 Bidirectional TSMR results between inflammatory dermatoses and mental disorders. (a) The TSMR results of mental disorders on inflammatory dermatoses. (b) The TSMR results of inflammatory dermatoses on mental disorders. “*” indicates FDR < 0.1, and “**” indicates FDR < 0.05. Square size reflects the strength of statistical evidence, with larger squares indicating smaller P values. Abbreviations: AD, atopic dermatitis; BD, bipolar disorder; CD, contact dermatitis; HS, hidradenitis suppurativa; OCD, obsessive-compulsive disorder; PTSD, post-traumatic stress disorder; TSMR, two-sample Mendelian randomization. |
We identified five significant causal associations (P < 0.05) between psychiatric disorders and skin diseases (Figures S1 and S2). Genetically predicted depression was found to significantly increase the risk of psoriasis (OR = 1.199, P < 0.001, FDR < 0.001). Depression and CD, BD and acne vulgaris and eczema, and anxiety disorder and psoriasis showed potential causal links. No significant associations were found between inflammatory skin diseases and OCD, PTSD, or schizophrenia (P > 0.05).
On the flip side, we also assessed the causal influence of skin diseases on psychiatric conditions. Six significant causal relationships (P < 0.05) were identified (Figures S3 and S4). Genetically predicted AD was shown to significantly increase depression risk (OR = 1.032, P = 0.001, FDR = 0.006), and eczema was associated with an increased risk of depression (OR = 1.113, P < 0.001, FDR < 0.001). A suggestive causal link was observed between AD and anxiety disorders, hidradenitis suppurativa and anxiety disorders, and eczema with both BD and depression. No correlations were found between acne vulgaris, rosacea, or CD and psychiatric disorders (P > 0.05). Detailed results are provided in Tables S1 and S2.
Our sensitivity analysis confirmed consistency with the primary findings, with robust results supported by random and fixed effects models. We identified depression as a risk factor for psoriasis and AD as a risk factor for depression. Further exploration of these comorbid relationships follows.
LDSC Analysis of TSMR Findings
We conducted LDSC analysis on the TSMR results to assess the genetic correlation between depression and both psoriasis and AD. The LDSC findings revealed a significant genetic correlation between depression and psoriasis (h2 = 0.019, rg = 0.202, P < 0.001), as well as between AD and depression (h2 = 0.039, rg = 0.202, P < 0.001), with detailed results provided in Table S3.
SMR and Three-Step SMR Identify Key Genes Underlying the Comorbid Pathways Between Inflammatory Dermatoses and Mental Disorders
To minimize bias from linkage disequilibrium, both multi-SNP and single-SNP SMR analyses were performed, with a focus on the latter.15 Significant associations (FDR < 0.1) were found for 167, 60, and 97 genes related to psoriasis, AD, and depression, respectively. The HEIDI test (P_HEIDI > 0.05) indicated that these associations were not due to horizontal pleiotropy.
We identified FADS1 and TMEM258 as key loci with significant cross-trait associations with both depression and AD. TMEM258 consistently showed positive associations across tissues, while FADS1 exhibited tissue-specific effects—positive in blood, negative in brain and fibroblasts. These findings highlight the tissue-dependent role of fatty acid metabolism. No genes were associated with depression and psoriasis simultaneously. The SMR results are detailed in Tables S4–S6.
Epigenetic regulation plays a critical role in the development of both inflammatory dermatoses and mental disorders.16–18 Using a three-step SMR framework, we integrated DNA methylation, gene expression, and disease-associated variants to uncover shared regulatory pathways. This identified KAT8, MLH3, TDRKH, and TRIM56 for psoriasis, and C11orf49, CPEB2, DBF4B, INO80E, and ZNF408 for depression. Several CpG sites showed joint associations with eQTLs and both diseases, supporting a methylation-dependent regulatory axis. These findings are visualized in Figure 3b and detailed in Tables S7–S10.
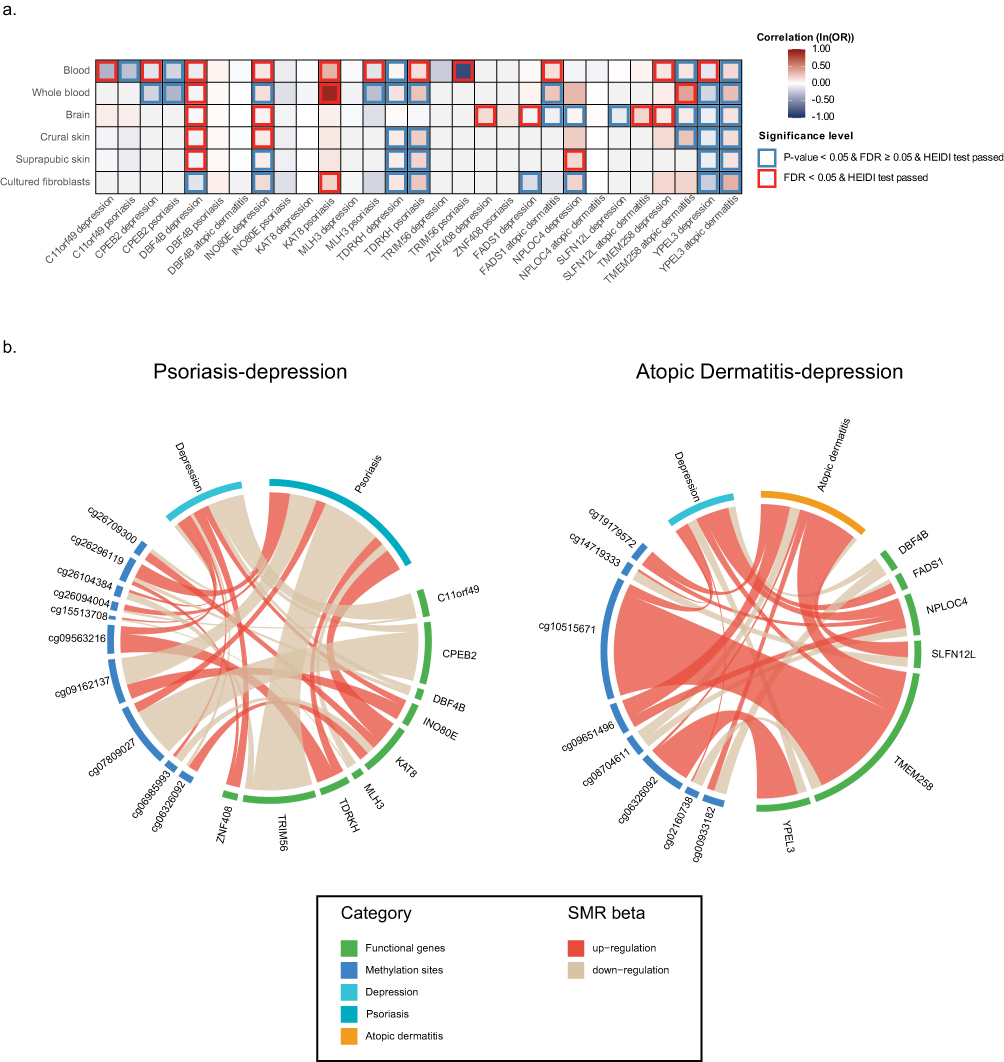 |
Figure 3 Identification of comorbidity-associated genes between inflammatory dermatoses and mental disorders through three-step SMR. (a) SMR significant results linking tissue eQTLs with psoriasis, atopic dermatitis, and depression. Red shading indicates increased risk, while blue shading denotes reduced risk, with darker shades reflecting stronger effects. Genes with significant SMR results, validated by the HEIDI test, are outlined in blue. Genes with significant FDR results and validated by the HEIDI test are outlined in red. (b) Associations between genes, CpGs, and diseases established through three-step SMR. The thickness of each line reflects the strength of the SMR association, while the line color indicates the direction of regulation: red represents upregulation, and beige represents downregulation. Abbreviations: CpG, Cytosine-phosphate-Guanine; eQTL, expression quantitative trait loci; FDR, false discovery rate; HEIDI, heterogeneity in dependent instrument; SMR, summary-data-based Mendelian randomization. |
Functionally, TMEM258 and SLFN12L were linked to AD risk, while KAT8 and TDRKH were associated with psoriasis. For depression, NPLOC4, INO80E, and ZNF408 increased risk, while others were protective. The tissue-specific expression suggests that the local microenvironment shapes the functional relevance of these genes in comorbid disease mechanisms. The eQTL and mQTL data utilized in the study are presented in Table 2. And the SMR results of the selected genes are shown in Figure 3a.
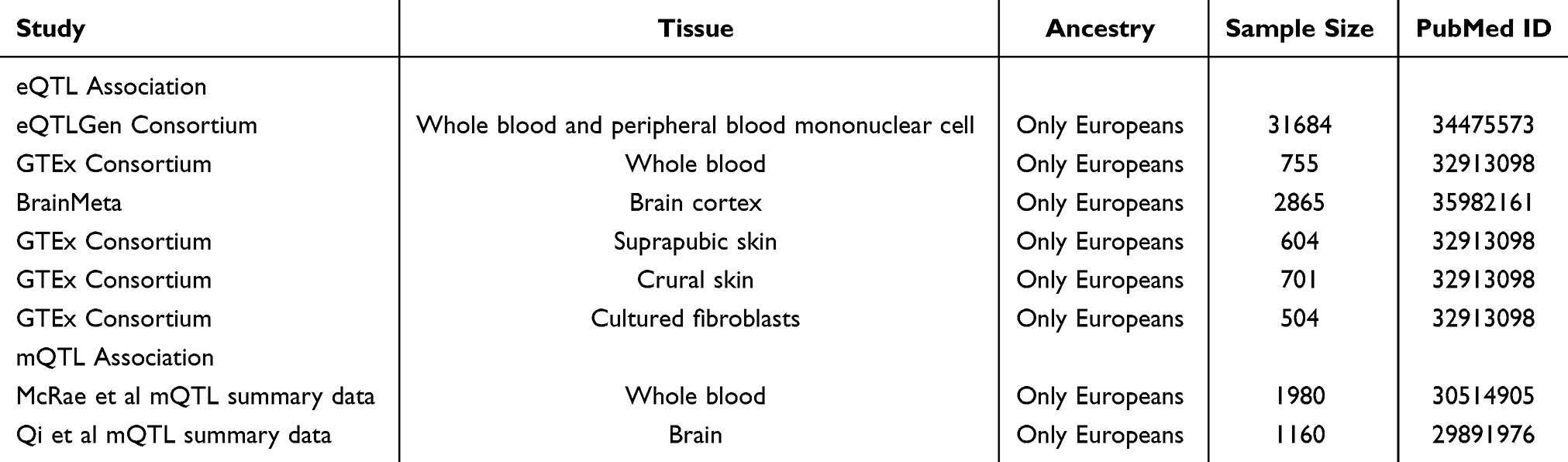 |
Table 2 Brief Information on eQTL and mQTL Data |
Bayesian Colocalization Analysis of SMR-Identified Associations
Bayesian colocalization analysis was performed to assess shared genetic variants in SMR-identified associations. As illustrated in Figure 4a–c and detailed in Tables S11–S13, FADS1 and TMEM258 showed strong colocalization (posterior probability of hypothesis 4, PP.H4 > 75%) with AD (blood) and depression (brain), while KAT8, MLH3, TDRKH, and TRIM56 colocalized with psoriasis in target tissues. SLFN12L colocalized with AD in blood, and C11orf49, CPEB2, INO80E, NPLOC4, and ZNF408 colocalized with depression. Beyond shared-variant associations, we also observed associations driven by distinct causal variants (PP.H3 > 75%).
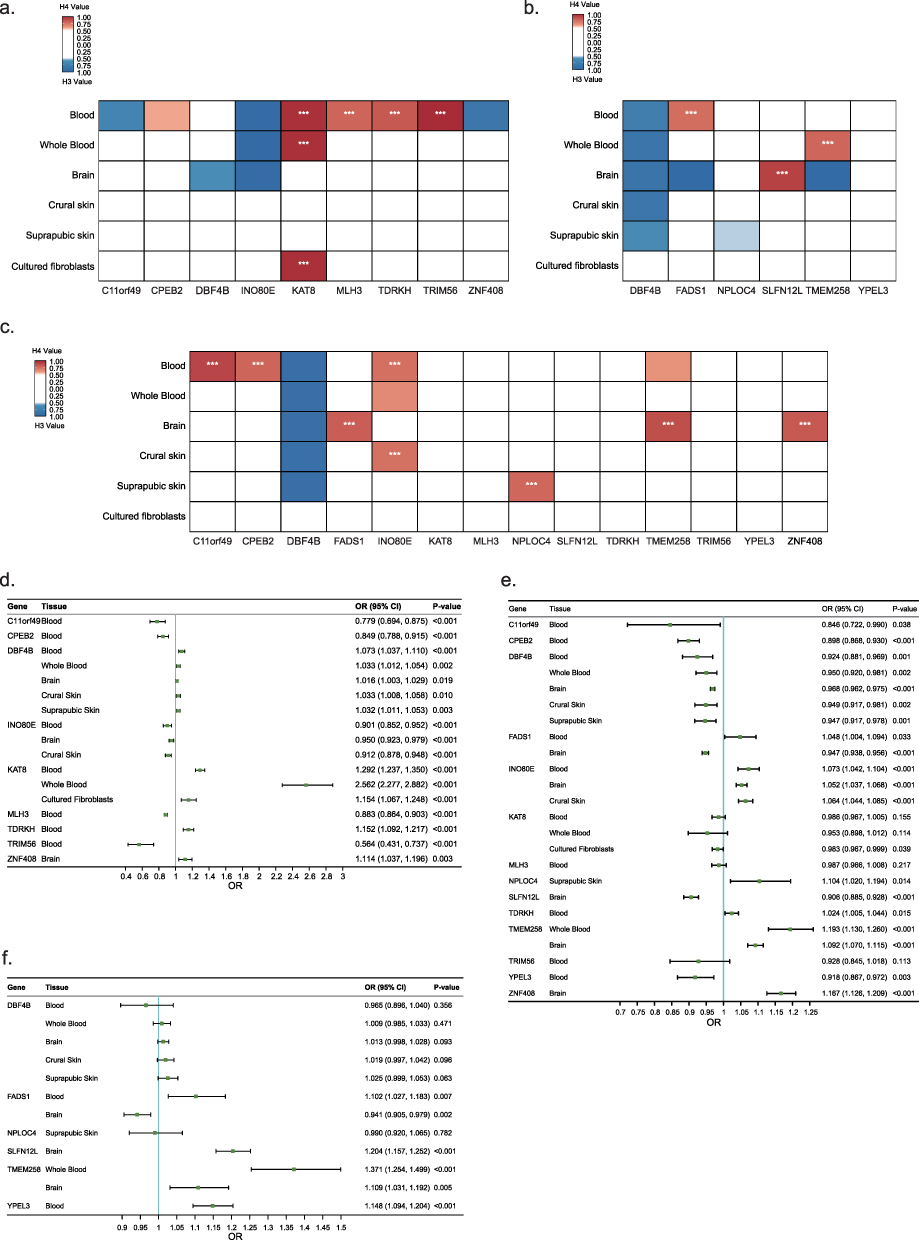 |
Figure 4 The colocalization and TSMR results for significant SMR genes. (a–c) Colocalization results of tissue-specific eQTLs with psoriasis (a), atopic dermatitis (b), and depression (c). Red indicates colocalization (PP.H4 > 0.5), while blue represents non-colocalized genetic associations (PP.H3 > 0.5). Darker shades indicate stronger associations. “***” denotes strong colocalization (PP.H4 ≥ 0.75). (d–f) TSMR forest plots show the association results between tissue-specific eQTLs and psoriasis (d), atopic dermatitis (e), and depression (f), including gene names, tissue types, OR, CI, and P values. Abbreviations: CI, confidence interval; eQTL, expression quantitative trait loci; OR, Odds Ratio; PP.H3, posterior probability of hypothesis 3; PP.H4, posterior probability of hypothesis 4; SMR, summary-data-based Mendelian randomization; TSMR, two-sample Mendelian randomization. |
TSMR Confirms the Causal Roles of Candidate Genes in Disease Risk
TSMR validated the causal associations identified by SMR, confirming that genes linked to psoriasis significantly influenced disease risk, with consistent effect directions. TMEM258, SLFN12L, YPEL3, and FADS1 were causally linked to AD. FADS1 showed tissue-specific effects. KAT8, MLH3, and TRIM56 did not affect depression, but other genes showed significant associations with depression. The detailed results are presented in Figure 4d–f and Tables S14–S16.
Functional Pathways of Candidate Genes
KEGG and GO analyses revealed the biological functions of candidate genes. Genes linked to depression and psoriasis were involved in type I interferon signaling, meiotic processes, transcription regulation, and mismatch repair, meiosis. Genes associated with depression and AD were involved in fatty acid metabolism, immune signaling, and endoplasmic reticulum (ER) function. Key findings from the over-representation analysis are presented in Figure 5a and b, and the full dataset is available in Tables S17–S20.
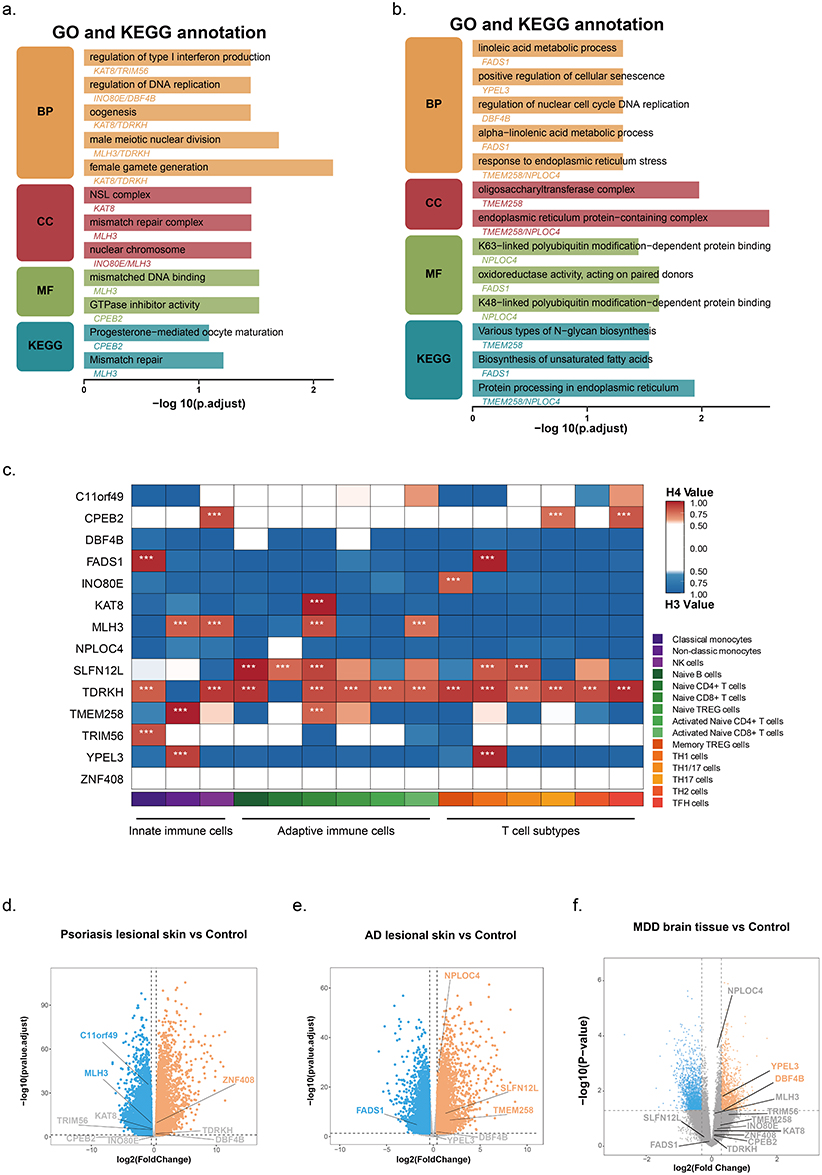 |
Figure 5 Multi-omics analysis of selected genes. (a and b) GO and KEGG functional classification of comorbidity-associated genes for depression–psoriasis (a) and atopic dermatitis–depression (b). GO analysis was performed across three functional categories: BP, CC, and MF. Orange indicates BP, red indicates CC, green indicates MF, and cyan indicates KEGG pathways. (c) Colocalization analysis of selected genes with immune cell specificity. Red indicates colocalization (PP.H4 > 0.5), while blue indicates non-colocalized genetic associations (PP.H3 > 0.5), with darker shades representing stronger associations. “***” denotes strong colocalization (PP.H4 ≥ 0.75). The different colors along the bottom axis represent different immune cell types, providing a detailed view of cell-specific associations. (d–f) RNA-seq volcano plots showing differentially expressed genes in psoriasis lesional skin (d), atopic dermatitis lesional skin (e), and MDD brain tissue (f) compared with healthy controls. Gray represents insignificant genes, blue indicates significantly downregulated genes, and orange represents significantly upregulated genes. Abbreviations: BP, biological process; CC, cellular component; GO, gene ontology; KEGG, Kyoto Encyclopedia of Genes and Genomes; MDD, major depressive disorder; MF, molecular function; PP.H3, posterior probability of hypothesis 3; PP.H4, posterior probability of hypothesis 4; RNA-seq, RNA sequencing. |
Immune Cell–Specific Colocalization of Candidate Genes
To explore the immunogenetic context, we assessed colocalization between candidate gene eQTLs and 15 immune cell types. FADS1 colocalized with monocytes and TFH cells, TMEM258 with non-classical monocytes and naïve CD4⁺ T cells, and TDRKH with 13 immune cell types, showing the strongest colocalization. These results are illustrated in Figure 5c and comprehensively detailed in Table S21.
Transcriptomic Profiling of Candidate Genes in Inflammatory Dermatoses and Depression
RNA sequencing analysis revealed significant differential expression (p.adjust < 0.05) of C11orf49, MLH3, and ZNF408 in psoriasis lesions, FADS1, NPLOC4, SLFN12L, and TMEM258 in AD skin. YPEL3 and DBF4B exhibited differential expression in MDD. The differential expression of these genes is visualized in Figure 5d–f and comprehensively reported in Tables S22–S24.
Mediation Analysis of Causal Relationships Between Inflammatory Dermatoses and Mental Disorders
TSMR identified insomnia and the omega-6/omega-3 fatty acid ratio as mediators in the pathways from depression to psoriasis and AD to depression. The mediation effect of insomnia was 0.023 (11.8% of the total effect), and for the omega-6/omega-3 ratio, it was 0.0015 (5.2% of the total effect). Further TSMR analysis revealed C11orf49, CPEB2, DBF4B, INO80E, TDRKH, and TRIM56 as genes linked to insomnia, with INO80E and TRIM56 promoting it. DBF4B, FADS1, SLFN12L, TMEM258, and YPEL3 were associated with the omega-6/omega-3 ratio. Notably, FADS1 displayed tissue-specific heterogeneity consistent with findings from the SMR analysis. These results are presented in Figure S5 and summarized in Tables S25–S27.
Prioritization of Therapeutic Targets for Comorbid Inflammatory Dermatoses and Mental Disorders
To identify promising therapeutic targets for the treatment of comorbid inflammatory dermatoses and mental disorders, we developed a prioritization framework based on five criteria: (i) SMR analysis validity, (ii) the number of relevant tissues, (iii) sensitivity analysis, (iv) multi-omics validation and (v) druggability.
Fourteen candidate genes were evaluated and systematically scored according to these criteria. Based on total scores, genes were grouped into three tiers. FADS1 and TMEM258 emerged as top-priority targets (score ≥ 6.0), reflecting their strong therapeutic potential. Five genes were assigned intermediate priority (score between 4.5 and 6.0), and the remaining genes were classified as lower-priority candidates. Notably, FADS1 achieved the highest overall score (7.85), with robust support across all evaluation domains. TMEM258 also ranked highly (score = 7.35), supported by multiple independent lines of evidence. Based on these findings, we propose FADS1 and TMEM258 as high-priority target genes for the treatment of comorbid inflammatory dermatoses and mental disorders. Final prioritization results are presented in Figure 6.
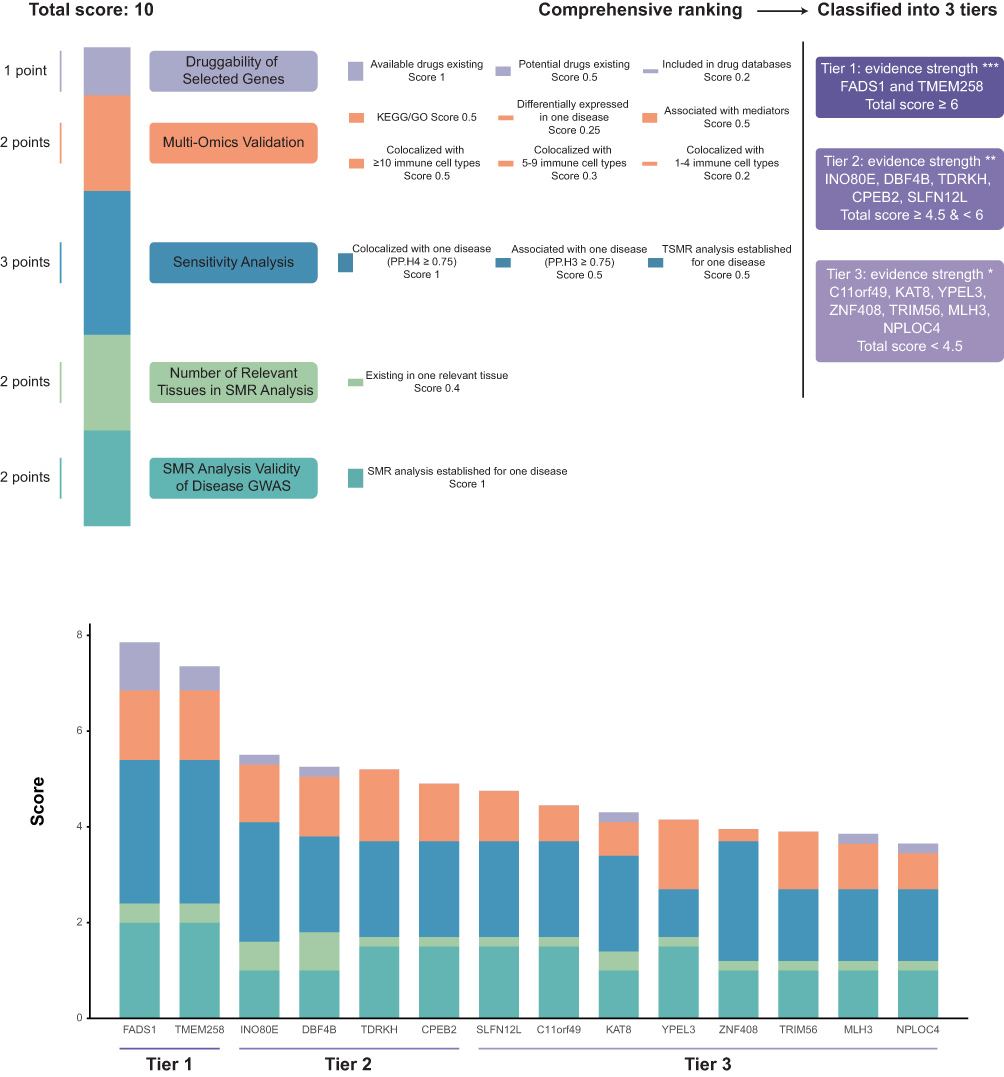 |
Figure 6 Evaluation of candidate drug targets for comorbid inflammatory dermatoses and mental disorders based on the results of this study. The prioritization of drug targets is based on five evidence components, with a total score of 10. Dark green (total score 2): evidence from SMR analysis of genes. Light green (total score 2): number of tissues showing statistical significance. Blue (total score 3): sensitivity analysis, including colocalization and TSMR. Orange (total score 2): evidence from KEGG/GO pathways, immune cell signaling, RNA-seq data, and mediation analysis. Purple: evidence from druggability across multiple databases. Gene targets are categorized into three tiers based on their total scores. Tier 1: total score ≥6, including FADS1 and TMEM258. Tier 2: total score ≥4.5 and <6, including INO80E, DBF4B, TDRKH, CPEB2, and SLFN12L. Tier 3: total score <4.5, including C11orf49, KAT8, YPEL3, ZNF408, TRIM56, MLH3, and NPLOC4. In the tier labels, “***”, “**”, and “*” indicate decreasing levels of evidence strength from Tier 1 to Tier 3. Abbreviations: GO, Gene Ontology; KEGG, Kyoto Encyclopedia of Genes and Genomes; RNA-seq, RNA sequencing; SMR, summary-data-based Mendelian randomization; TSMR, two-sample Mendelian randomization. |
Discussion
Psychodermatology, a growing field at the intersection of dermatology and psychiatry, has gained significant attention in the European Academy of Dermatology and Venereology. Several studies highlight the profound psychological impact of skin diseases, particularly AD and psoriasis, which are linked to psychological stressors like anxiety and depression.19–21 Current research recognizes that the pathogenesis of numerous skin disorders is influenced by both biological mechanisms and psychological factors. While cross-sectional studies have established a correlation between psychological stress and both the emergence and intensification of symptoms in various skin conditions, the molecular mechanisms underlying the comorbidity remain poorly understood.22,23 Through comprehensive causal inference and multi-omics analyses, we identified 14 genes implicated in shared pathogenic pathways. After assessing drug target potential, FADS1 and TMEM258 emerged as promising therapeutic targets, providing critical insights into the molecular basis of this comorbidity.
Comorbidity Between Depression and Psoriasis
Depression is common among individuals with psoriasis, with studies showing a significant association between psoriasis severity, mood disorders, and impaired quality of life.24 A meta-analysis found psoriasis patients have a higher incidence of depressive symptoms (SMD = 1.16; OR 1.57) compared to the general population.25 Over 10% of psoriasis patients experience clinical depression. Shared inflammatory mechanisms, such as the activation of IL-23 and IL-17 in psoriasis, contribute to the pathogenesis.26 Depression also increases inflammatory cytokines, which are linked to worse depression symptoms.27 Inflammatory cytokines in psoriasis may disrupt the HPA axis, reducing serotonin and promoting depression.9 This inflammatory overlap may be modulated by the gut-brain-skin axis.
In contrast to earlier studies, which often focused on surface-level associations, our investigation offers an in-depth examination of the molecular underpinnings linking depression and psoriasis. We identified a set of four genes—CPEB2, DBF4B, INO80E, and ZNF408—that appear to orchestrate key aspects of this comorbidity. Functionally, these genes converge on fundamental cellular processes such as cell cycle regulation, DNA replication, and transcription, and colocalize with pro-inflammatory immune subsets including Th17 cells. Among them, CPEB2 is particularly important in the nervous system, where it regulates both presynaptic and postsynaptic translation, thereby influencing synaptic plasticity and memory formation.28 Moreover, CPEB2 has been implicated in epithelial-mesenchymal transition (EMT) and metastasis in hepatocellular carcinoma through the HIF-1α/miR-210-3p/CPEB2 signaling axis.29 INO80E, on the other hand, has been associated with schizophrenia and alcohol use disorder in previous studies.30
In addition, we identified insomnia as a mediating factor in the causal pathway between depression and psoriasis. This phenotype exhibited causal relationships with several of the aforementioned genes. Epigenetic studies have revealed that individuals with short sleep duration or chronic insomnia exhibit distinct DNA methylation patterns, which may influence biological processes related to neuroplasticity and neurodegeneration.31,32 DNA methylation represents a shared molecular thread across both disorders: in psoriasis, methylation changes in lesional skin are strongly associated with disease severity and pathological gene expression; in depression, altered methylation at the BDNF locus has been proposed as a state marker.33,34 These findings collectively point to an epigenetic mechanism through which sleep disruption may amplify immune dysregulation and facilitate comorbidity between depression and psoriasis. Furthermore, reduced melatonin secretion in depressed individuals might influence the levels of TNF-α, IL-6, and IL-8, as well as other components of the inflammatory cascade, potentially triggering psoriasis.35
Finally, we identified KAT8, MLH3, TDRKH, and TRIM56 as potential therapeutic targets for psoriasis. KAT8, in particular, enhances pro-inflammatory chemokine secretion through H4K16 acetylation, exacerbating psoriatic inflammation.36 However, no direct link to depression has been established.
Biologics targeting inflammatory markers effectively reduce depressive symptoms in psoriasis patients. Ustekinumab reduced depression risk by 55% (HADS), and brodalumab improved HADS scores in Phase III trials.37,38 In contrast, psychotropic drugs’ effects on psoriasis are less studied, with maprotiline showing improvements in lesions and psychiatric symptoms.39 Gabapentin and pregabalin also improved psoriasis.40 Regular psychological assessments and monitoring of skin manifestations, especially in patients with risk factors like obesity and smoking, are crucial.26
Comorbidity Between Depression and AD
Our study also suggests that AD (OR = 1.032, P = 0.001, FDR = 0.006) and eczema (OR = 1.113, P < 0.001, FDR < 0.001) increase the risk of depression. National Health and Nutrition Examination Survey (NHANES) (2005–2006) found that 31% of AD patients reported depressive symptoms.41 Factors such as severe itching, sleep disturbances, and social isolation contribute to higher depression rates in AD.42 Th2-type immune activation and elevated inflammatory cytokines in AD may increase depression risk, similar to psoriasis.43
Our study identified FADS1 as a key gene mediating the comorbidity between AD and depression. FADS1 (fatty acid desaturase 1) encodes a rate-limiting enzyme involved in the biosynthesis of ω-3 and ω-6 polyunsaturated fatty acids (PUFAs).44 Genetic variants associated with reduced FADS1 expression have been linked to lower circulating levels of eicosapentaenoic acid (EPA), which aligns with our transcriptomic findings from the GEO database.45 Notably, we found that the imbalance between ω-6 and ω-3 fatty acids acts as a mediating factor between AD and depression. ω-3 PUFAs possess anti-inflammatory properties, contribute to the regulation of epidermal lipid composition, and reinforce skin barrier function by reducing transepidermal water loss.46 Mechanistically, ω-3 PUFAs suppress Th2 cytokine expression by inhibiting GATA transcription factors, thereby alleviating the symptoms of AD.47 In the central nervous system, ω-3 PUFAs have been shown to promote synaptogenesis and stress adaptation by upregulating the expression of BDNF.48 Multiple clinical studies have reported an inverse correlation between ω-3 fatty acid levels and the risk of depression.49 Taken together, these findings suggest that PUFA imbalance due to dysregulated FADS1 expression may serve as a common pathological link between AD and depression. Moreover, ω-3 supplementation emerges as a potential preventive strategy for comorbid AD and depression. Clinical trials have demonstrated notable improvements in pediatric AD following ω-3 supplementation, although its therapeutic efficacy in depression remains inconclusive.50
In addition, two endoplasmic reticulum (ER) stress-related genes, TMEM258 and NPLOC4, have been implicated in both depression and AD. Dysregulation of the unfolded protein response (UPR) and excessive ER stress have been associated with a broad range of skin disorders, including rosacea and vitiligo.51,52 Experimental studies have shown that activation of IRE1 and PERK signaling pathways within the UPR can exacerbate inflammation in murine models of contact hypersensitivity.53 In the central nervous system, ER stress amplifies neuroinflammatory responses by affecting neurons, microglia, and astrocytes, ultimately impairing synaptic plasticity—a mechanism thought to contribute to the pathophysiology of depression.54 TMEM258 and NPLOC4 are key regulators of ER stress. TMEM258 is an essential component of the oligosaccharyltransferase complex, which modulates protein glycosylation and governs ER stress responses; it plays a critical role in intestinal inflammation.55 While NPLOC4 is involved in ubiquitin-dependent pathways, particularly ER-associated degradation (ERAD), which clears misfolded proteins from the ER.56 Given their functional involvement in ER stress pathways, TMEM258 and NPLOC4 may serve as molecular bridges contributing to the shared pathogenesis of depression and AD through ER stress-mediated immune and neuroinflammatory mechanisms.
Biologics for AD, such as dupilumab and abrocitinib, may reduce depression incidence.57,58 Phase III trials showed dupilumab improved depressive symptoms, and abrocitinib reduced depression scale scores compared to placebo.59,60
Conclusions
Our study integrated epigenetic data and multi-omics resources to comprehensively investigate the bidirectional causal relationships and shared comorbid mechanisms between six mental disorders and seven inflammatory dermatoses. Despite limitations related to cohort ancestry information and the use of summary-level data, our findings provided evidence supporting causal links between depression and psoriasis, as well as between AD and depression. We identified 14 genes associated with these comorbid mechanisms, primarily implicating neuroinflammation, dysregulated lipid metabolism, and endoplasmic reticulum stress, with FADS1 and TMEM258 emerging as the most promising therapeutic targets. In addition, our results suggest the clinical relevance of monitoring sleep status and serum fatty acid levels in patients with psoriasis and AD. Collectively, this study provides new insights into the clinical management of patients with inflammatory dermatoses and lays a foundation for the development of targeted therapeutic strategies for psychodermatological comorbidities.
Abbreviations
AD, atopic dermatitis; BD, bipolar disorder; BDNF, brain-derived neurotrophic factor; CD, contact dermatitis; eQTL, expression quantitative trait loci; ER, endoplasmic reticulum; FDR, false discovery rate; GO, Gene Ontology; GWAS, genome-wide association study; HEIDI, heterogeneity in dependent instruments; KEGG, Kyoto Encyclopedia of Genes and Genomes; LDSC, linkage disequilibrium score regression; mQTL, methylation quantitative trait loci; OCD, obsessive-compulsive disorder; OR, odds ratio; PGC, Psychiatric Genomics Consortium; PP.H4, posterior probability of hypothesis 4; PTSD, post-traumatic stress disorder; PUFAs, polyunsaturated fatty acids; SMD, standardized mean difference; SMR, summary data-based Mendelian randomization; TSMR, two-sample Mendelian randomization.
Data Sharing Statement
All data utilized in this MR study are publicly available from the original genome-wide association studies (GWAS) cited in the manuscript. Detailed information of the database is provided in Table 1. The datasets supporting the conclusions of this article are included within the article and Additional File.
Ethics Approval and Consent to Participate
All data used in this study were obtained from legally acquired, publicly available databases and did not involve any individually identifiable information. The original data collection for the source databases had been approved by the respective ethics committees, and informed consent had been obtained from all participants by the original investigators. In accordance with Article 32, items (1) and (2), of the Measures for Ethical Review of Life Science and Medical Research Involving Human Subjects (China, February 18, 2023), studies using legally obtained public data or anonymized information data that do not cause harm to human participants and do not involve sensitive personal information or commercial interests may be exempt from ethics review. After assessment by the ethics department of the corresponding author’s institution, this study was determined to meet the criteria for exemption from institutional ethics review and approval. Therefore, no additional ethics approval or informed consent was required for this study.
Acknowledgments
Yibo Feng, Xiang Chen, and Xinlan Qiu are co-first authors for this study. We want to acknowledge the participants and investigators of the FinnGen Biobank and Psychiatric Genomics Consortium.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors declare financial support was received for the research. This research was funded by the National Natural Science Foundation of China (82373506) and the National Key Research and Development Program of China (2023YFC2509000).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Penn L, Rothman L, Sutton AM, Brinster NK, Vidal CI. What’s new in dermatopathology: inflammatory dermatoses. Adv Anat Pathol. 2019;26(1):40–17. doi:10.1097/PAP.0000000000000210
2. Liu TJ, Lin LL, McMeniman E, et al. Cytokine/Chemokine assessment as a complementary diagnostic tool for inflammatory skin diseases. Front Immunol. 2022;13:1028435. doi:10.3389/fimmu.2022.1028435
3. Farzanfar D, Dowlati Y, French LE, Lowes MA, Alavi A. Inflammation: a contributor to depressive comorbidity in inflammatory skin disease. Skin Pharmacol Physiol. 2018;31(5):246–251. doi:10.1159/000490002
4. Patel KR, Immaneni S, Singam V, Rastogi S, Silverberg JI. Association between atopic dermatitis, depression, and suicidal ideation: a systematic review and meta-analysis. J Am Acad Dermatol. 2019;80(2):402–410. doi:10.1016/j.jaad.2018.08.063
5. Yi X, Wang X, Fu Y, et al. Altered brain activity and cognitive impairment in patients with psoriasis. J Eur Acad Dermatol Venereol. 2024;38(3):557–567. doi:10.1111/jdv.19685
6. Chang HC, Huang YC, Lien YJ, Chang YS. Association of rosacea with depression and anxiety: a systematic review and meta-analysis. J Affect Disord. 2022;299:239–245. doi:10.1016/j.jad.2021.12.008
7. White paper on psychodermatology in Europe: a position paper from the EADV Psychodermatology Task Force and the European Society for Dermatology and Psychiatry (ESDaP) - PubMed. Available from: https://pubmed.ncbi.nlm.nih.gov/37615377/.
8. Marek-Jozefowicz L, Czajkowski R, Borkowska A, et al. The brain–skin axis in psoriasis—psychological, psychiatric, hormonal, and dermatological aspects. Int J Mol Sci. 2022;23(2):669. doi:10.3390/ijms23020669
9. Koo J, Marangell LB, Nakamura M, et al. Depression and suicidality in psoriasis: review of the literature including the cytokine theory of depression. J Eur Acad Dermatol Venereol. 2017;31(12):1999–2009. doi:10.1111/jdv.14460
10. Liu L, Xue Y, Chen Y, et al. Acne and risk of mental disorders: a two-sample Mendelian randomization study based on large genome-wide association data. Front Public Health. 2023;11:1156522. doi:10.3389/fpubh.2023.1156522
11. Baurecht H, Welker C, Baumeister SE, et al. Relationship between atopic dermatitis, depression and anxiety: a two-sample Mendelian randomization study. Br J Dermatol. 2021;185(4):781–786. doi:10.1111/bjd.20092
12. Cao S, Zhang Z, Liu L, et al. Causal relationships between atopic dermatitis and psychiatric disorders: a bidirectional two-sample Mendelian randomization study. BMC Psychiatry. 2024;24(1):16. doi:10.1186/s12888-023-05478-1
13. Wang Y, Wang X, Gu X, et al. Evidence for a causal association between psoriasis and psychiatric disorders using a bidirectional Mendelian randomization analysis in up to 902,341 individuals. J Affect Disord. 2023;337:27–36. doi:10.1016/j.jad.2023.05.059
14. Chu M, Shen S, Zhu Z, et al. Association of psoriasis with depression, anxiety, and suicidality: a bidirectional two-sample Mendelian randomization study. J Dermatol. 2023;50(12):1629–1634. doi:10.1111/1346-8138.16941
15. Wu Y, Zeng J, Zhang F, et al. Integrative analysis of omics summary data reveals putative mechanisms underlying complex traits. Nat Commun. 2018;9(1):918. doi:10.1038/s41467-018-03371-0
16. Schmidt AD, de Guzman Strong C. Current understanding of epigenetics in atopic dermatitis. Exp Dermatol. 2021;30(8):1150–1155. doi:10.1111/exd.14392
17. Mateu-Arrom L, Puig L. Genetic and Epigenetic Mechanisms of Psoriasis. Genes. 2023;14(8):1619. doi:10.3390/genes14081619
18. Vialou V, Feng J, Robison AJ, Nestler EJ. Epigenetic mechanisms of depression and antidepressant action. Annu Rev Pharmacol Toxicol. 2013;53:59–87. doi:10.1146/annurev-pharmtox-010611-134540
19. Reich A, Hrehorów E, Szepietowski JC. Pruritus is an important factor negatively influencing the well-being of psoriatic patients. Acta Derm Venereol. 2010;90(3):257–263. doi:10.2340/00015555-0851
20. Silverberg JI, Margolis DJ, Boguniewicz M, et al. Validation of five patient-reported outcomes for atopic dermatitis severity in adults. Br J Dermatol. 2020;182(1):104–111. doi:10.1111/bjd.18002
21. Strouphauer E, Stolar A, Tollefson M. Manifestation of anxiety and depression among pediatric patients with psoriasis: a review. Pediatr Dermatol. 2023;40(1):11–18. doi:10.1111/pde.15185
22. Schut C, Mollanazar NK, Sethi M, et al. Psychological stress and skin symptoms in college students: results of a cross-sectional web-based questionnaire study. Acta Derm Venereol. 2016;96(4):550–551. doi:10.2340/00015555-2291
23. Stewart TJ, Schut C, Whitfeld M, Yosipovitch G. Cross-sectional study of psychological stress and skin symptoms in Australian university students. Australas J Dermatol. 2018;59(1):e82–e84. doi:10.1111/ajd.12640
24. Boehncke WH, Schön MP. Psoriasis. Lancet. 2015;386(9997):983–994. doi:10.1016/S0140-6736(14)61909-7
25. Dowlatshahi EA, Wakkee M, Arends LR, Nijsten T. The prevalence and odds of depressive symptoms and clinical depression in psoriasis patients: a systematic review and meta-analysis. J Invest Dermatol. 2014;134(6):1542–1551. doi:10.1038/jid.2013.508
26. Mrowietz U, Sümbül M, Gerdes S. Depression, a major comorbidity of psoriatic disease, is caused by metabolic inflammation. J Eur Acad Dermatol Venereol. 2023;37(9):1731–1738. doi:10.1111/jdv.19192
27. Prinz I, Sandrock I, Mrowietz U. Interleukin-17 cytokines: effectors and targets in psoriasis-A breakthrough in understanding and treatment. J Exp Med. 2020;217(1):e20191397. doi:10.1084/jem.20191397
28. Lu WH, Chang TT, Chang YM, et al. CPEB2-activated axonal translation of VGLUT2 mRNA promotes glutamatergic transmission and presynaptic plasticity. J Biomed Sci. 2024;31(1):69. doi:10.1186/s12929-024-01061-2
29. You R, Yang Y, Yin G, et al. CPEB2 suppresses hepatocellular carcinoma epithelial-mesenchymal transition and metastasis through regulating the HIF-1α/miR-210-3p/CPEB2 axis. Pharmaceutics. 2023;15(7):1887. doi:10.3390/pharmaceutics15071887
30. Hu B, Yin MY, Zhang CY, et al. The INO80E at 16p11.2 locus increases risk of schizophrenia in humans and induces schizophrenia-like phenotypes in mice. EBioMedicine. 2025;114:105645. doi:10.1016/j.ebiom.2025.105645
31. Ämmälä AJ, Hancox TPM, Qiuyu F, et al. Daily rhythm in DNA methylation and the effect of total sleep deprivation. J Sleep Res. 2025;34(4):e14438. doi:10.1111/jsr.14438
32. Lahtinen A, Puttonen S, Vanttola P, et al. A distinctive DNA methylation pattern in insufficient sleep. Sci Rep. 2019;9(1):1193. doi:10.1038/s41598-018-38009-0
33. Pan J, Chen S, Chen X, Song Y, Cheng H. Histone modifications and DNA methylation in psoriasis: a cellular perspective. Clin Rev Allergy Immunol. 2025;68(1):6. doi:10.1007/s12016-024-09014-1
34. Januar V, Ancelin ML, Ritchie K, Saffery R, Ryan J. BDNF promoter methylation and genetic variation in late-life depression. Transl Psychiatry. 2015;5(8):e619. doi:10.1038/tp.2015.114
35. Tohid H, Aleem D, Jackson C. Major depression and psoriasis: a psychodermatological phenomenon. Skin Pharmacol Physiol. 2016;29(4):220–230. doi:10.1159/000448122
36. Xiang Y, Jiang Y, Wang Z, et al. Targeting KAT8 alleviates self-RNA-driven skin inflammation by modulating histone H4 lysine 16 acetylation in psoriasis. Cell Death Differ. 2025. doi:10.1038/s41418-025-01547-y
37. Langley RG, Feldman SR, Han C, et al. Ustekinumab significantly improves symptoms of anxiety, depression, and skin-related quality of life in patients with moderate-to-severe psoriasis: results from a randomized, double-blind, placebo-controlled phase III trial. J Am Acad Dermatol. 2010;63(3):457–465. doi:10.1016/j.jaad.2009.09.014
38. Papp KA, Reich K, Paul C, et al. A prospective Phase III, randomized, double-blind, placebo-controlled study of brodalumab in patients with moderate-to-severe plaque psoriasis. Br J Dermatol. 2016;175(2):273–286. doi:10.1111/bjd.14493
39. Alpsoy E, Ozcan E, Cetin L, et al. Is the efficacy of topical corticosteroid therapy for psoriasis vulgaris enhanced by concurrent moclobemide therapy? A double-blind, placebo-controlled study. J Am Acad Dermatol. 1998;38(2 Pt 1):197–200. doi:10.1016/s0190-9622(98)70240-3
40. Boyd ST, Mihm L, Causey NW. Improvement in psoriasis following treatment with gabapentin and pregabalin. Am J Clin Dermatol. 2008;9(6):419. doi:10.2165/0128071-200809060-00012
41. Association between Atopic Dermatitis and Depression in US Adults - PubMed. Available from: https://pubmed.ncbi.nlm.nih.gov/26316069/.
42. Silverberg JI. Comorbidities and the impact of atopic dermatitis. Ann Allergy Asthma Immunol. 2019;123(2):144–151. doi:10.1016/j.anai.2019.04.020
43. Guttman-Yassky E, Renert-Yuval Y, Brunner PM. Atopic dermatitis. Lancet. 2025;405(10478):583–596. doi:10.1016/S0140-6736(24)02519-4
44. Reyes-Pérez SD, González-Becerra K, Barrón-Cabrera E, Muñoz-Valle JF, Armendáriz-Borunda J, Martínez-López E. FADS1 genetic variant and Omega-3 supplementation are associated with changes in fatty acid composition in red blood cells of subjects with obesity. Nutrients. 2024;16(20):3522. doi:10.3390/nu16203522
45. Tanaka T, Shen J, Abecasis GR, et al. Genome-wide association study of plasma polyunsaturated fatty acids in the InCHIANTI Study. PLoS Genet. 2009;5(1):e1000338. doi:10.1371/journal.pgen.1000338
46. Balić A, Vlašić D, Žužul K, Marinović B, Bukvić Mokos Z. Omega-3 versus Omega-6 polyunsaturated fatty acids in the prevention and treatment of inflammatory skin diseases. Int J Mol Sci. 2020;21(3):741. doi:10.3390/ijms21030741
47. Park BK, Park S, Park JB, Park MC, Min TS, Jin M. Omega-3 fatty acids suppress Th2-associated cytokine gene expressions and GATA transcription factors in mast cells. J Nutr Biochem. 2013;24(5):868–876. doi:10.1016/j.jnutbio.2012.05.007
48. Liu B, Zhang Y, Yang Z, et al. ω-3 DPA protected neurons from neuroinflammation by balancing microglia M1/M2 polarizations through inhibiting NF-κB/MAPK p38 signaling and activating Neuron-BDNF-PI3K/AKT pathways. Mar Drugs. 2021;19(11):587. doi:10.3390/md19110587
49. Serefko A, Jach ME, Pietraszuk M, Świąder M, Świąder K, Szopa A. Omega-3 Polyunsaturated Fatty Acids in Depression. Int J Mol Sci. 2024;25(16):8675. doi:10.3390/ijms25168675
50. Niseteo T, Hojsak I, Ožanić Bulić S, Pustišek N. Effect of Omega-3 polyunsaturated fatty acid supplementation on clinical outcome of atopic dermatitis in children. Nutrients. 2024;16(17):2829. doi:10.3390/nu16172829
51. Melnik BC. Rosacea: the blessing of the celts - an approach to pathogenesis through translational research. Acta Derm Venereol. 2016;96(2):147–156. doi:10.2340/00015555-2220
52. Shimasaki S, Koga T, Shuto T, et al. Endoplasmic reticulum stress increases the expression and function of toll-like receptor-2 in epithelial cells. Biochem Biophys Res Commun. 2010;402(2):235–240. doi:10.1016/j.bbrc.2010.09.132
53. Gendrisch F, Völkel L, Fluck M, et al. IRE1 and PERK signaling regulates inflammatory responses in a murine model of contact hypersensitivity. Allergy. 2022;77(3):966–978. doi:10.1111/all.15024
54. Sprenkle NT, Sims SG, Sánchez CL, Meares GP. Endoplasmic reticulum stress and inflammation in the central nervous system. Mol Neurodegener. 2017;12(1):42. doi:10.1186/s13024-017-0183-y
55. Graham DB, Lefkovith A, Deelen P, et al. TMEM258 is a component of the oligosaccharyltransferase complex controlling ER stress and intestinal inflammation. Cell Rep. 2016;17(11):2955–2965. doi:10.1016/j.celrep.2016.11.042
56. Blythe EE, Olson KC, Chau V, Deshaies RJ. Ubiquitin- and ATP-dependent unfoldase activity of P97/VCP•NPLOC4•UFD1L is enhanced by a mutation that causes multisystem proteinopathy. Proc Natl Acad Sci U S A. 2017;114(22):E4380–E4388. doi:10.1073/pnas.1706205114
57. Langan SM, Irvine AD, Weidinger S. Atopic dermatitis. Lancet. 2020;396(10247):345–360. doi:10.1016/S0140-6736(20)31286-1
58. Paller A, Jaworski JC, Simpson EL, et al. Major Comorbidities of Atopic Dermatitis: beyond Allergic Disorders. Am J Clin Dermatol. 2018;19(6):821–838. doi:10.1007/s40257-018-0383-4
59. Silverberg JI, Simpson EL, Thyssen JP, et al. Efficacy and safety of abrocitinib in patients with moderate-to-severe atopic dermatitis: a randomized clinical trial. JAMA Dermatol. 2020;156(8):863–873. doi:10.1001/jamadermatol.2020.1406
60. Simpson EL, Bieber T, Guttman-Yassky E, et al. Two Phase 3 trials of dupilumab versus placebo in atopic dermatitis. N Engl J Med. 2016;375(24):2335–2348. doi:10.1056/NEJMoa1610020
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Elevated C-Reactive Protein and Erythrocyte Sedimentation Rate Correlates with Depression in Psoriasis: A Chinese Cross-Sectional Study
Tan M, Luo Y, Hu J, Hu K, Li X, Yang J, Chen J, Zhu W, Kuang Y
Clinical, Cosmetic and Investigational Dermatology 2023, 16:397-405
Published Date: 13 February 2023
Health-Related Behaviors and Psychological Status of Adolescent Patients with Atopic Dermatitis: The 2019 Korea Youth Risk Behavior Web-Based Survey
Park JH, Prochnow T, Chang J, Kim SJ
Patient Preference and Adherence 2023, 17:739-747
Published Date: 18 March 2023
Transcriptome Analysis Identifies Biomarkers for the Diagnosis and Management of Psoriasis Complicated with Depression
Xia X, Yu H, Li Y, Liang Y, Li G, Huang F
Clinical, Cosmetic and Investigational Dermatology 2023, 16:1287-1301
Published Date: 18 May 2023
Advances in Relationship Between Alcohol Consumption and Skin Diseases
Liu L, Chen J
Clinical, Cosmetic and Investigational Dermatology 2023, 16:3785-3791
Published Date: 29 December 2023
Advancements in Dermatological Applications of Curcumin: Clinical Efficacy and Mechanistic Insights in the Management of Skin Disorders
Mo Z, Yuan J, Guan X, Peng J
Clinical, Cosmetic and Investigational Dermatology 2024, 17:1083-1092
Published Date: 13 May 2024