Back to Journals » Advances in Medical Education and Practice » Volume 14
A Multi-Institutional Study of Yemeni Final Year Undergraduate Pharmacy Students’ Understanding, Attitudes, and Perceived Barriers Toward Provision of Pharmaceutical Care: A Cross-Sectional Study
Authors Hatem NAH ![]() , Mohamed Ibrahim MI
, Mohamed Ibrahim MI ![]() , Halboup A
, Halboup A ![]() , Kubas M
, Kubas M ![]()
Received 11 October 2022
Accepted for publication 24 January 2023
Published 11 February 2023 Volume 2023:14 Pages 109—121
DOI https://doi.org/10.2147/AMEP.S392886
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Najmaddin AH Hatem,1 Mohamed Izham Mohamed Ibrahim,2 Abdulsalam Halboup,3,4 Mohammed Kubas5,6
1Department of Pharmacy Practice, College of Clinical Pharmacy, Hodeidah University, Alhodeidah, Yemen; 2Department of Clinical Pharmacy and Practice, College of Pharmacy, QU Health, Qatar University, Doha, Qatar; 3Department of Clinical Pharmacy and Pharmacy Practice, Faculty of Pharmacy, University of Science and Technology, Sana’a, Yemen; 4Discipline of Clinical Pharmacy, University Sains Malaysia, Penang, Malaysia; 5Clinical Pharmacy Department, University of Science and Technology Hospital, Sana’a, Yemen; 6Clinical Pharmacy Department, School of Pharmacy, Lebanese International University, Sana’a, Yemen
Correspondence: Najmaddin AH Hatem, Department of Pharmacy Practice, College of Clinical Pharmacy, Hodeidah University, P.O. 3114, Alhodeidah, Yemen, Tel +967 775040472, Email [email protected]
Introduction: Pharmaceutical care (PC) is the philosophy of the pharmacist’s practice to achieve a better health-related outcome by designing, implementing and monitoring the therapeutic plans. It is in its infancy in Yemen. Hence, the study objectives were to examine the barriers to PC provision as perceived by Yemen pharmacy students and to assess their level of understanding of PC and their attitudes toward PC.
Methodology: A cross-sectional study was conducted among ten pharmacy colleges in Yemen, offering undergraduate pharmacy programs. A stratified sample of 518 students from the included universities were surveyed using a well-structured, validated and self-administered questionnaire. Chi-square, Mann–Whitney U, and Kruskal–Wallis tests were conducted at an alpha level of 0.05.
Results: Four hundred and seventy-five (475) participants were included (92.9% response rate). More than 17% (n=84) of participants were involved in Pharm.D program, and nearly 29.9% (n=142) preferred pharmaceutical marketing as a career after graduation. About 65% of participants recognized the purpose of PC, and pharmacists’ role within PC. However, only 43.8% (n=208) knew the difference between clinical pharmacy and PC. About 82% of respondents showed very good attitudes toward PC. Pharm.D students showed higher attitudes’ total scores, median (IQR): 4.3 (4.1– 4.4), 4.2 (4– 4.2) and 4 (3.9– 4.2) for Pharm.D, bachelor of pharmacy and bachelor of clinical pharmacy respectively, (p-value = 0.032). Moreover, students who currently employed in pharmacy-related job during their study were also associated with high attitudes scores compared to unemployed students, median (IQR): 4.2 (4– 4.4) and 4(3.9– 4.1) respectively (p-value = 0.023). “Lack of access to the patient medical record in the pharmacy” and “inadequate (hospital and community pharmacy) internship period” were the top reported barriers with 81.5% (n=387) agreement.
Conclusion: Although PC is in its infancy in Yemen, pharmacy students showed positive attitudes toward practicing PC. Educational institutions should exert efforts for curricular revision to improve understanding, and overcome the reported barriers in the future.
Keywords: clinical pharmacy, evaluation research, pharmaceutical care, pharmacy curriculum, Yemeni pharmacy education
Introduction
The pharmacist’s job has gradually changed through PC services over the 20th century from drug-focused to patient-focused. For many pharmacists worldwide, it has evolved into a standard type of practice.1 The board of Pharmaceutical Care Network Europe (PCNE) announced a workshop for all members and other pharmaceutical care experts in 2013. The consensus in this workshop was to redefine pharmaceutical care (PC) as: “the pharmacist contribution to care of the individual in order to optimize medicines use and improve health outcome”.2
Pharmaceutical care is a philosophy of the pharmacist’s practice to collaborate closely with other health care professionals and the patient to achieve a better health-related outcome by designing, implementing and monitoring the therapeutic plan.3 Due to poly-pharmacy, an increase in age, and an increase in chronic diseases, patients may experience a potential or actual drug-related problems (DRPs) during treatment. In this case, the pharmacist plays a critical role in ① Identifying those DRPs ② resolving actual DRPs and Preventing any potential DRPs.4 According to numerous pieces of research, evaluating the effects of PC in various settings, offering PC has a favorable effect on reducing hospital stay, improving patient quality of life, and patient adherence, decreasing mortality or hospitalization rates and reducing medication errors.5 Moreover, providing PC has positive outcomes in many diseases, particularly hypertension, diabetes, cardiovascular diseases, asthma and chronic obstructive pulmonary disease (COPD).6–9 In areas of the world with more advanced medical facilities, PC is frequently practiced.10 However, the situation might differ in some Arab nations, where pharmacist orientation is still primarily centered on selling medicines.11
The University of Sana’a’s Faculty of Medicine and Health Sciences established a pharmacy department in 1987, and other universities and institutions soon followed. Yemen’s undergraduate pharmacy curricula continue to be influenced by traditional pharmaceutical curriculum and only sometimes applying knowledge to patient care, despite Yemen having received pharmacy education earlier than other Arabic nations.11 Currently, seven governmental universities and more than 12 private colleges and universities provide three different types of undergraduate pharmacy programs: Bachelor of Pharmacy, Bachelor of clinical pharmacy, and Pharm.D. In 2011 Hodeidah university established a Bachelor of clinical pharmacy program in which an entry-to-practice degree with a duration of five years and a half, including 6-month internships (4.5 years of academic study and 6-months hospital ward internship) It is the first governmental university that establishes a new patient-oriented curriculum.11 Implementing the new patient-oriented curriculum has gradually transitioned from traditional drug dispensing to a patient-centered approach in pharmacy practice. Most pharmacy schools and colleges offer PC as a stand-alone theory course or as a component of other curricula. As long as the pharmacist is the most accessible medical professional in Yemen. Hence, pharmacists can play an extremely important role in promoting and preserving public health, especially during the continuing crisis.12 Nevertheless, pharmacists have not yet included PC practices in their routine practice. The provision of PC is uncommon and even less common in hospitals.11
The participant students had worked or trained in an actual pharmacy practice setting. Therefore, it is essential to comprehend pharmacy students’ preparedness to provide PC and determine pharmacy students’ attitudes toward PC and barriers that could affect their practice. Several related studies have been carried out internationally,13–15 as well as in the Middle East in Saudi Arabia,16 Kuwait,17 Qatar,18 and the UAE.19 Baral et al reported that positive attitude towards PC was indicated by the Nepalese students despite having several barriers.14 Similar findings was also shown by the Cuban university pharmacy students.15 Al-Arifi’s study in King Saud University, Saudi Arabia also reported that students have positive attitudes toward PC and it was significantly related to age, gender and marital status of the students.16 A study in Kuwait by Katoue et al established another evidence that the Kuwaiti pharmacy students while recognizing barriers, understood and supported the PC implementation in the health care settings.17 In addition, studies in Qatar and UAE, indicated similar results.18,19
Therefore, it is important to assess if Yemeni pharmacy students are receiving adequate instruction and preparation to foster a positive attitude toward PC. Therefore, the purpose of this study was to outline the understanding and attitudes of Yemeni pharmacy students concerning PC and address the barriers that could hinder future pharmacists from providing such service. Furthermore, keeping track of this crucial data will help to monitor the nation’s efforts to teach future pharmacy healthcare professionals.
Materials and Methods
Study Design and Setting
A cross-sectional study was conducted in Yemen based on a validated self-administered bilingual questionnaire (S1 File). Of more than 12 private and six public universities in Yemen,11 five public and five private universities that offer undergraduate pharmacy programs and have students in their final year were selected and the questionnaire was distributed among them. These universities are located in major cities in Yemen. They were selected in order to cover both the private and public sectors. Also, the majority of pharmacy students graduated from these institutions.
Study Population, Sample Size Calculation and Sampling Method
Representative pharmacy students in each university were approached to know the number of final-year pharmacy students. In all participating universities, There were 1227 undergraduate pharmacy students. The sample size was calculated using the Raosoft sample size online calculator (http://www.raosoft.com/samplesize.html). Using the obtained target population size and assuming a margin of error of 5%, a confidence interval of 99% and a 20% were added to account for the non-response rate. The ultimate sample size was 518.
A cluster random sampling method was used to enrol a demographically stratified proportionate sample from each college. The stratified sample for each college was calculated by dividing the sample size (n=518) by the total population (N=1227) and then multiplying it by the number of final-year pharmacy students in each university. Each college was treated as a cluster, and the appropriate sample was drawn from each of them using simple random sampling. Before distributing the questionnaires, we gathered information regarding the number of males and females in the final year at each university. The total number was 269 females (21.9%) and 958 males (78.1%). The investigators aimed to obtain a proportionate sample from each university by distributing the questionnaires according to that ratio.
Inclusion and Exclusion Criteria
Final year pharmacy, clinical pharmacy and Pharm.D students from the above-mentioned universities were included in this study since they have almost been exposed to the concept of PC. Therefore, we believe that final-year students are familiar with this concept, particularly those who have completed or done an academic internship in hospitals or practical training in community pharmacies. Therefore, pharmacy students from different levels were excluded.
Study Tool Development and Validation
A self-administered questionnaire was distributed among final-year pharmacy students at the included universities. On the opening page of the questionnaire, the study’s goals and a thank you message were mentioned. The first section of the questionnaire contained participants’ socio-demographic characteristics and other data that were gathered to learn more about Yemen’s actual pharmaceutical scenario. The second part contained twelve true/false statements about pharmacy students’ understanding of PC’s idea, purpose, and function and the pharmacist’s involvement in the PC process. Six of the incorporated questions were misleading statements, according to previous studies.20–22 The third part contained 13 items of the standard Pharmaceutical Care Attitudes Survey (PCAS) instrument, which Chisholm and Martin23 originally developed to examine pharmacy students’ attitudes regarding the PC. The participants were required to rate the items on a five Likert scale (5= strongly agree, 4= agree, 3= neutral, 2= disagree and 1= strongly disagree). The final part contains the barriers to implementing PC. Final-year pharmacy students were asked to rate the items on a five-point Likert scale (5= strongly agree, 4= agree, 3= neutral, 2= disagree and 1= strongly disagree) on how much each of the 11 potential barriers would hinder their provision of PC in the future. Eleven barrier-related items were incorporated based on previous research.14–18,18,19 This instrument was selected since it has been widely used around the world, such as in USA,13 Saudi Arabia,16 Kuwait,17 Qatar,18 UAE,19 Cuba,15 Malaysia,24 and Pakistan.25
After the principal investigator was granted electronic permission to use the PCAS by Bradley C. Martin, forward translation from English into Arabic was performed. For validation, the Arabic-translated version of the structured tool was sent to two faculty members who are familiar with quantitative studies and have much expertise in cross-sectional studies in the pharmacy field. Another clinical pharmacist (Ph.D. candidate) was involved in the validation process. The relevancy, clarity, conciseness of the items and readability of the questions were all examined for the questionnaire. The final draft of the questionnaire was created after reviewing experts’ comments. The reliability of the study tool was assessed by piloting the validated survey among 10 final-year pharmacy students who were excluded from the final analysis. The values for Cronbach’s alpha for attitudes and barriers were 0.847 and 0.750, respectively.
Data Collection Procedure
After obtaining permission from the selected universities the questionnaire was distributed among students at the beginning of the main lectures in the selected universities. The time expected to fill up the questionnaire was ten minutes. The participants were informed about the study’s objectives and verbal consent for participation was obtained. The principal investigator and two other clinical pharmacy students collected the data. Unfortunately, we could not distribute the study survey to one of the universities because they were in their academic clerkship in the hospital. Thus, we created an online copy of the questionnaire using Google form and sent it to 80 students as they were a representative proportionate sample from that university.
Data Analysis
The data were entered and analyzed using IBM SPSS statistics version 26.0 for windows (IBM Corp., Armonk, NY, USA). Categorical variables, such as socio-demographic data, understanding, attitudes, and perceived barriers, were reported as frequency and percentage.
The Kolmogorov–Smirnov result for data normality was statistically significant (P < 0.05), indicating that the data followed non-normal distribution. Mann–Whitney U and Kruskal–Wallis tests were used to assess the differences between the scores of understanding, attitudes, and barriers items and the participants’ characteristics. Chi square test was used to assess association between categorical variables. A p value of less than 0.05 was considered statistically significant.
Results
Of 518 pharmacy students were invited to participate, 481 surveys were returned with a response rate of 92.9%. Six surveys were excluded in which more than three questions were not answered. Total valid responses were, therefore 475. The vast majority of respondents were male (80.8%, n=384), and they were widely distributed within the age group 25 years old and less (68%, n=323), and (82.9%, n=394) were single. The respondents were grouped based on the type of pharmacy program, with the Bachelor of Pharmacy recording the highest proportion (75.8%, n=360), followed by Pharm.D (17.7%, n=84), and Bachelor of Clinical Pharmacy program (6.5%, n=31). Additional socio-demographic factors are listed in Table 1.
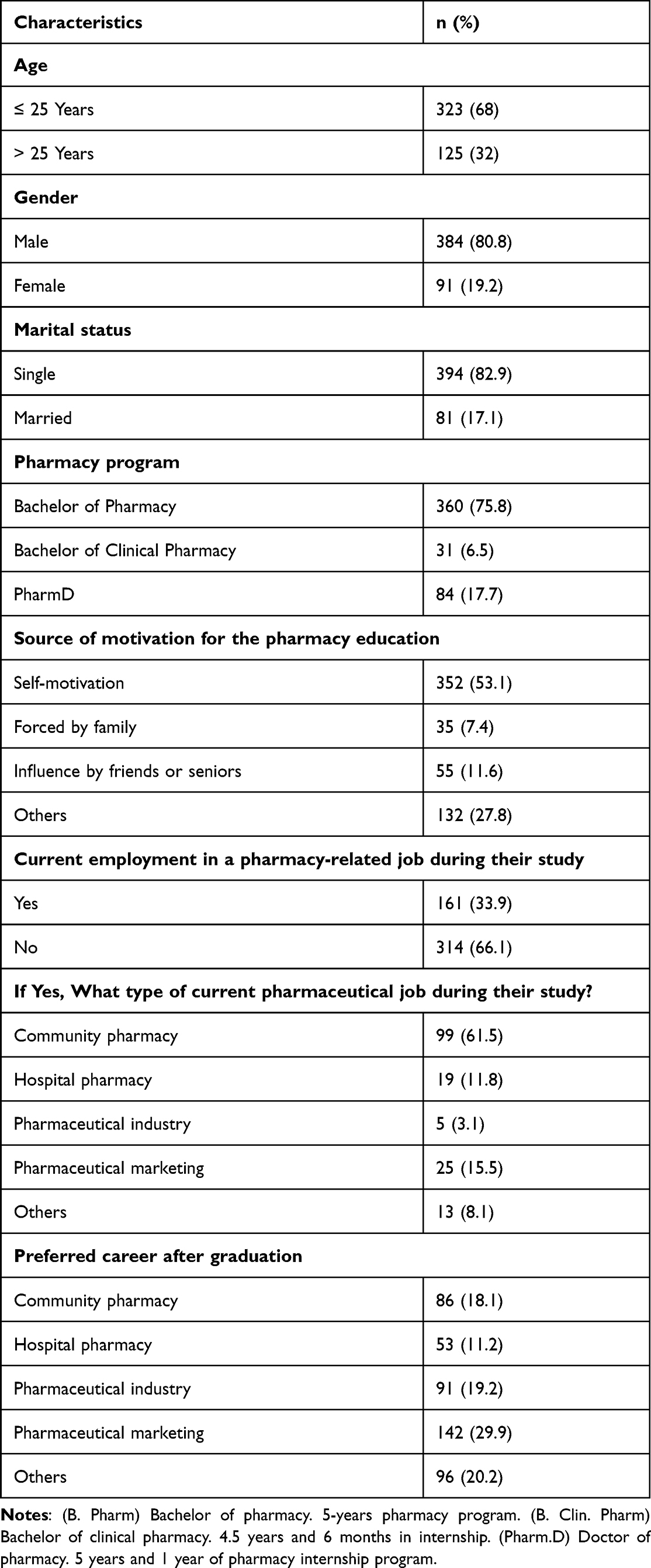 |
Table 1 Pharmacy Students’ Socio-Demographic Characteristics |
Understanding of PC
The goal of this section was to establish students’ general understanding of PC. The majority of the respondents (64%) had an overall correct understanding of the PC process. Through assessing statements 1, 6 and 7, over 80% of pharmacy students correctly understood the role and responsibilities of PC practitioners and the PC process. Moreover, (96.2%, n=457,) of pharmacy students correctly thought maintaining and improving patient quality of life was the main goal of PC. Barely, (44%, n=208,) respondents correctly thought there was a difference between PC and clinical pharmacy. More details can be found in Table 2.
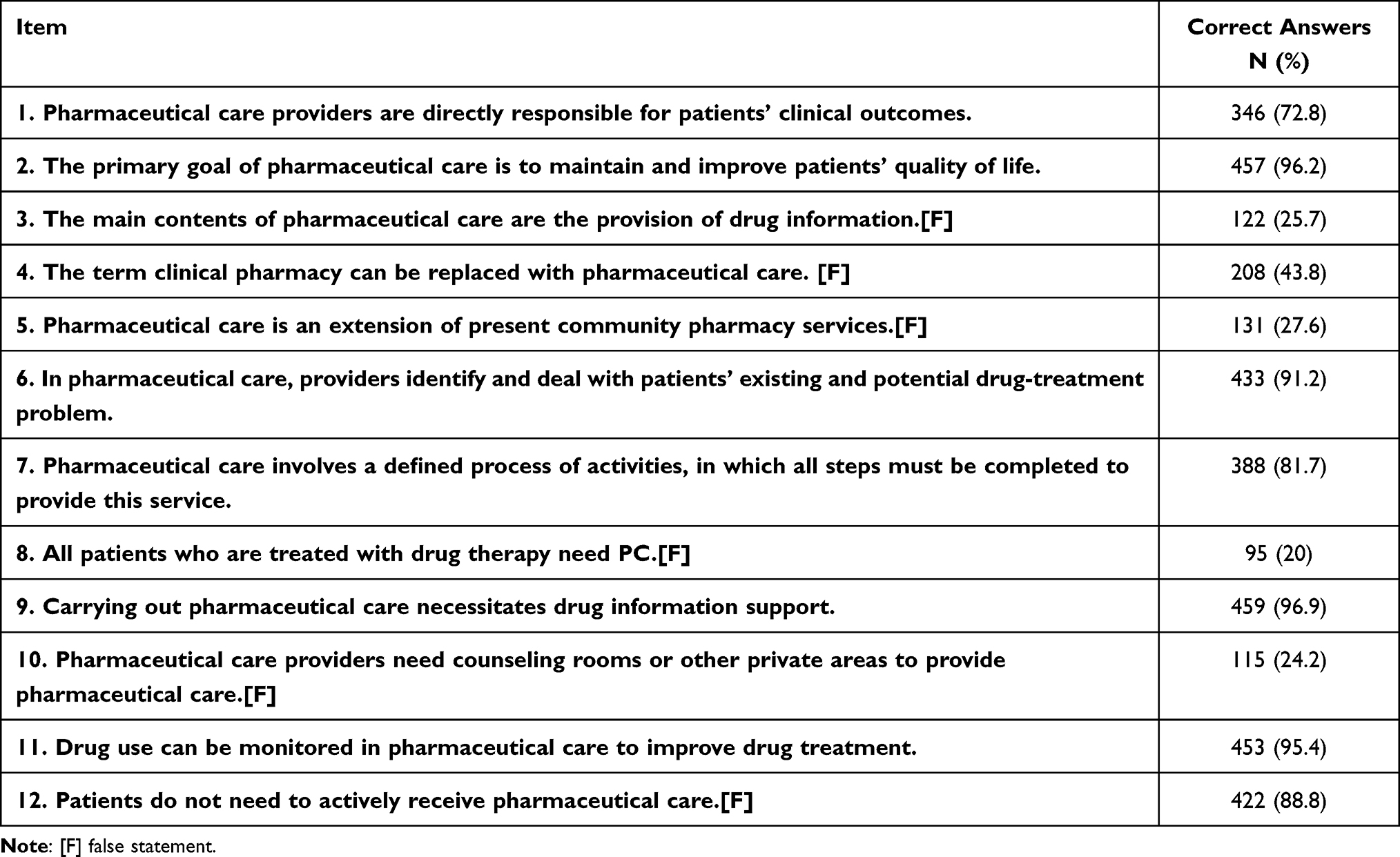 |
Table 2 Pharmacy Students Understanding of the Concept of Pharmaceutical Care |
The overall score of understanding of PC was not significantly affected by socio-demographic characteristics except for the gender group in which male students had a higher level of understanding than females (P = 0.049). In S1 Table Statements 7, 8 and 10 were statistically significant with gender group whereas females had a higher level of understanding than males in statements 7 and 8 (P = 0. 012, P = 0. 047, and P = 0.009), respectively. Moreover, Pharm.D students had less understanding than other pharmacy students on the need for a counseling room or private space to provide PC (P = 0.006).
Attitudes Toward the Provision of PC
The vast majority of respondents (80%) had an overall positive attitude toward providing PC. About 94.5% (n=449,) of the respondents supported that the PC movement will improve patient health, 81.5% (n=387) strongly agree/agree that all pharmacists should perform PC, and 87.6% (n=416,) thought that the primary responsibility of pharmacists in a health care setting should be to prevent and solve medication-related problems. However, only 17% (n=81) strongly disagree/disagree that “providing PC takes too much time and effort”, and 31.8% (n=151) strongly agree/agree “providing PC is not worth the additional workload that it places on the pharmacist” (Table 3).
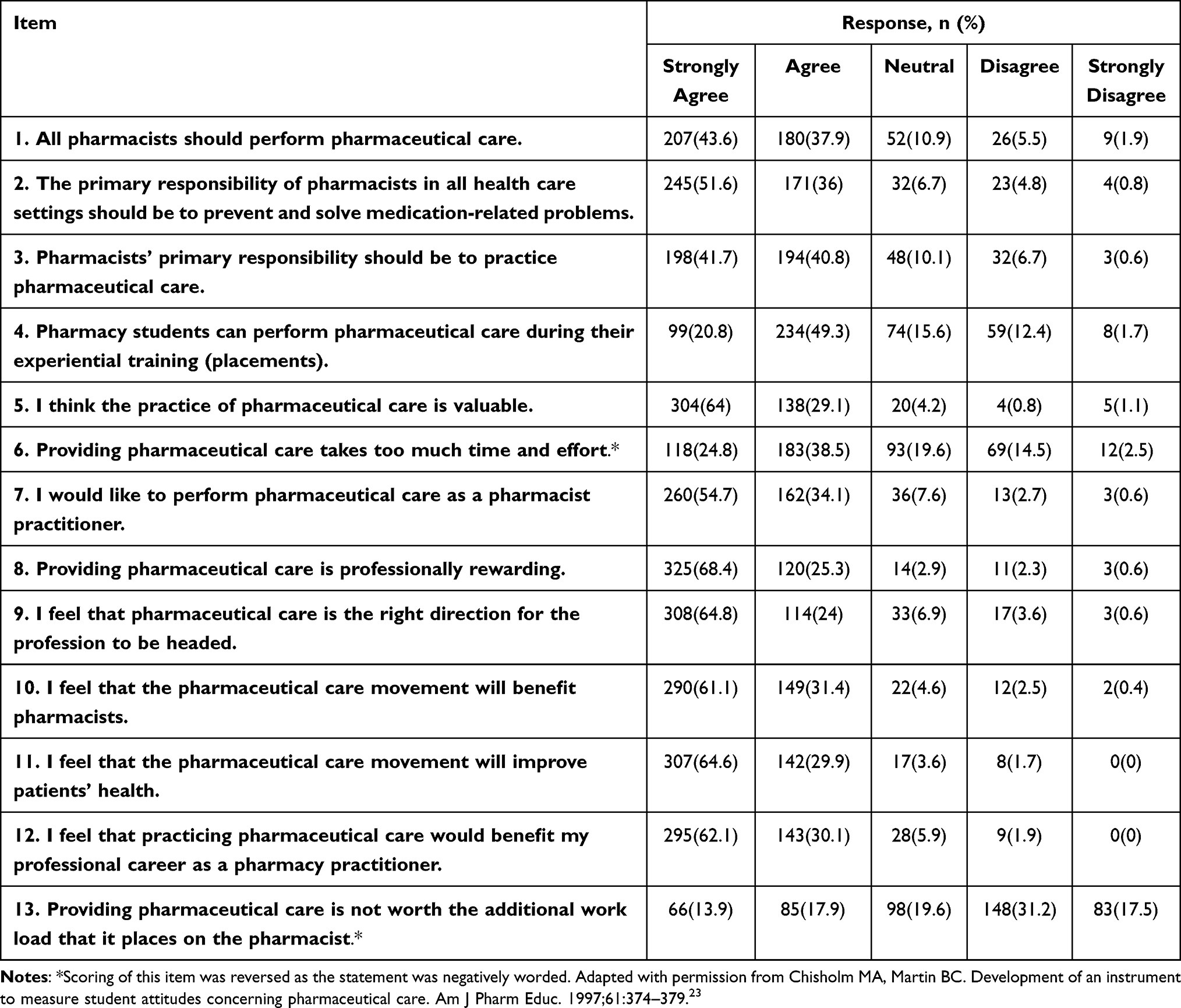 |
Table 3 Pharmacy Students’ Attitudes Toward the Provision of Pharmaceutical Care |
In contrast, students in the Pharm.D program recorded higher attitudes scores with median and IQR 4.3 (4.1–4.4) than those in other programs (p = 0.032). Interestingly, in Table 4, current employed pharmacy students with median and IQR 4.2 (4–4.4) had higher positive attitudes than unemployed students with median and IQR 4 (3.9–4.1), (p = 0.023). Also, in S2 Table they recorded higher attitudes in association with the PCAS per scale “Professional Benefit, Professional Duty, and Return on Effort” (P = 0.001, P = 0.008, P = 0.009) respectively. The S3 Table lists the attitudes items that significantly influenced the characteristic. The Kruskal–Wallis test showed statistical significance in the type of pharmacy students program with statements 2, 6, 9, and 10 whereas, the PharmD program recorded the highest positive scores (p = 0.033, p = 0.001, p = 0.003, p = 0.003) respectively.
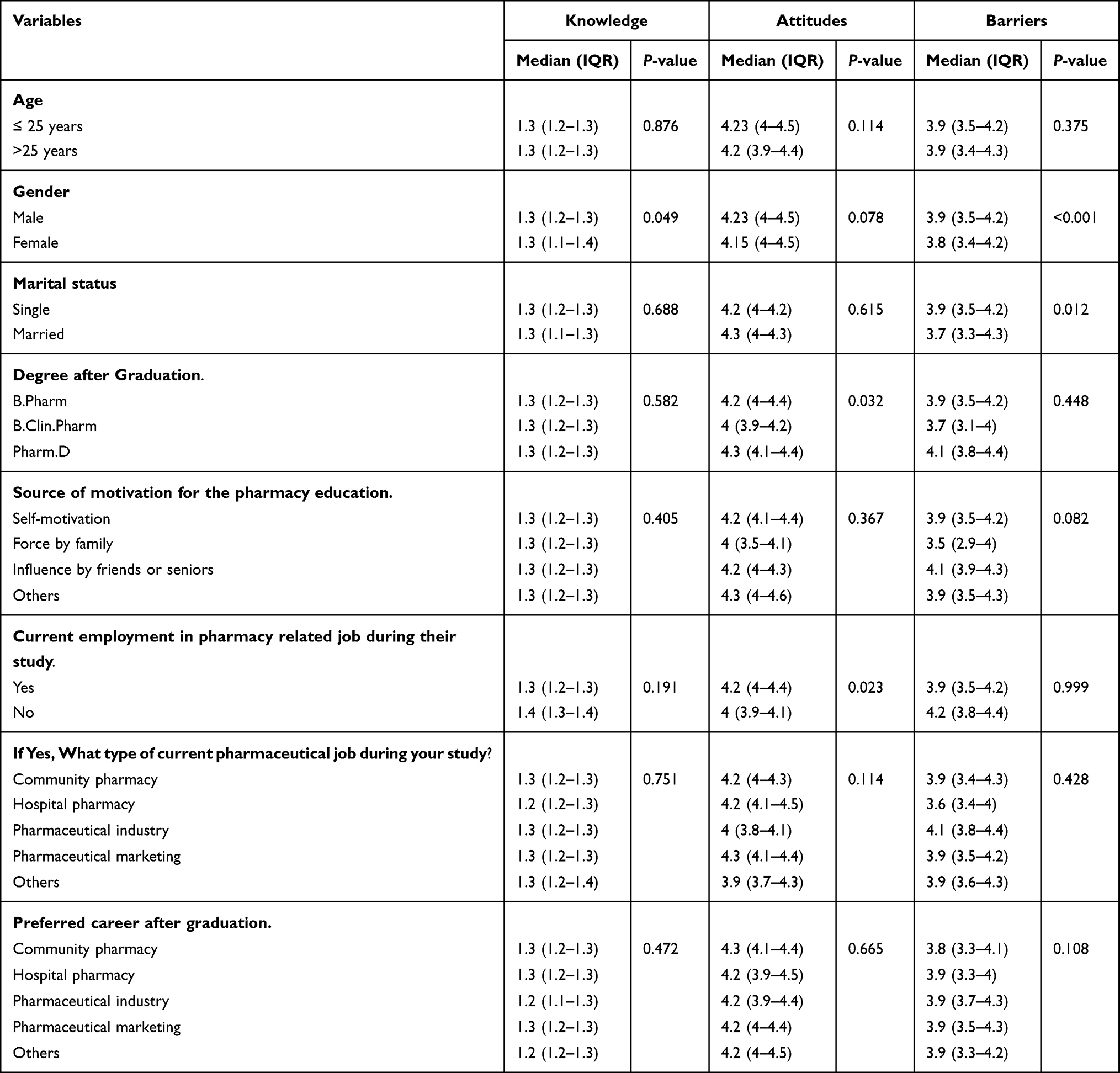 |
Table 4 Differences Between Demographic Variables and Pharmacy Students’ Understanding, Attitudes and Barriers |
Barriers Toward PC Provision
The Table 5. shows that pharmacy students strongly agree or agree that “Lack of access to the patient medical record in the pharmacy” (n=387, 81.5%), “Inadequate internship period” (n=387, 81.5%), “Lack of private counseling area, space, or inappropriate pharmacy layout” (n=363, 76.4%), “Lack of therapeutic knowledge and clinical problem-solving skills” (n=352, 74.1%), and “Lack of understanding of PC” (n=351, 73.9%), were perceived as the top five barriers to provide the PC in their daily practice. “Lack of confidence” received disagreement (n=161, 33.9%), making it the perceived barrier with the highest disagreement. Furthermore, the characteristic did not significantly affect the perceived barriers’ score except gender and marital status (p = < 0.001, and p = 0.012), respectively (see Table 4).
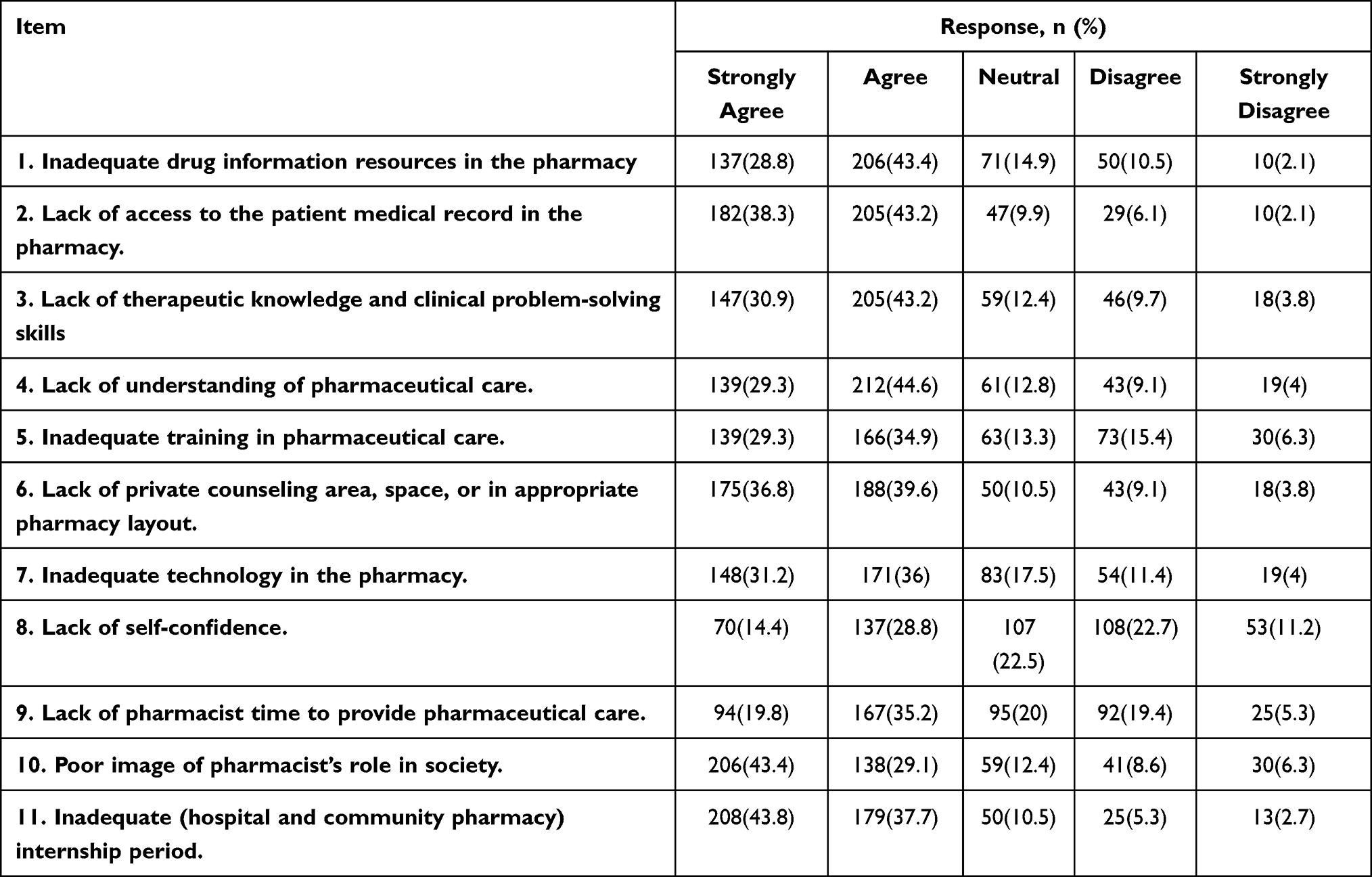 |
Table 5 Pharmacy Students Preserved Barriers Toward the Provision of Pharmaceutical Care |
Discussion
In the current study the respondents had a moderate understanding of the newly introduced concept of PC. They expressed a very good attitude and willingness to implement PC. Pharm.D and employed students displayed more positive attitudes. Lack of access to the patient medical record in the pharmacy and inadequate (hospital and community pharmacy) internship period were the main barriers identified, among other barriers. In general, this study’s findings were consistent with other studies, especially in the Arab region.
Most pharmacy students were self-motivated to undertake pharmacy education, and less than twenty percent were females; this was lower than reported studies in Kuwait, Malaysia, Nepal, and UEA.14,17,19,25 Furthermore, their preferred career after graduation was in pharmaceutical marketing, followed by the pharmaceutical industry. The availability of 500 foreign pharmaceutical companies and more than 13,000 brand medicines registered in this country could have influenced their choice of pharmaceutical marketing.26 Moreover, it is considered the highest-paid pharmaceutical sector in Yemen. Medication counseling, drug information center, pharmacovigilance, and drug dispensing are some employment placement sites for pharmacists in hospital pharmacies. In spite of that, hospital pharmacy in the current study received the lowest percentage among preferred pharmaceutical careers. The Yemeni Ministry of Public Health and Population (MoPH) in 2020 published the first national guide of clinical pharmacy, which states clinical pharmacist responsibilities and job description along with the presence of at least one clinical pharmacist for every ten hospitals’ beds.27 We expect this endeavor to serve as a framework for building a concrete career foundation for pharmacists working in hospital pharmacies in the following years.
Understanding of PC
The current study demonstrated that pharmacy students in Yemen moderately understood the basic concept of PC. However, the results stress that students’ understanding is still not optimal. Therefore, the current curriculum for pharmacy (B.Sc) degrees should be revised and should include more training in PC. In addition, the current Pharm.D and clinical pharmacy B.Sc curriculum must highlight the new responsibilities and stress the impact of implementing PC in pharmacist daily practice. This result was in line with previous studies conducted among pharmacists in New Zealand, Thailand, Jordan, and Qatar.20–22,28
In fact, less than half of participants correctly thought that clinical pharmacy and PC could be used interchangeably. Clinical pharmacy and PC are mutually complementary ideas but have different goals. Clinical pharmacy describes a practice of pharmacy that contributes to a larger PC system. Understanding clinical pharmacy can improve the technical quality of PC. On the other hand, understanding PC can broaden the philosophy and practice of clinical pharmacy. PC is often discussed as a system, but none of the definitions of clinical pharmacy mention systems. The two concepts also seem to differ in their philosophical bases. Evidently, the basis for clinical pharmacy is more in science than in relationship ethics.3
Community pharmacists are in a unique position to provide various services, since they are the most accessible healthcare member in this country.12 However, pharmacists are still concerned about dispensing medical prescriptions and marketing only. Over four decades, PC has been adopted in many countries worldwide. As a result, pharmacists globally have been given more responsibilities within PC, such as interviewing patients to establish a direct relationship, obtaining -related information, and clarifying and augmenting other available information to prevent, detect, and resolve medication therapy recommendations.1 In the current study, nearly thirty percent of students thought that “PC is an extension of present community pharmacy services”. As a result, the Yemeni pharmacy curriculum must highlight those responsibilities within PC and stress the impact of adopting them in daily practice.
Attitudes Toward the Provision of PC
The present study has found that pharmacy students have high positive attitudes. This is in line with similar studies in Saudi, Kuwait, Qatar, USA, Nigeria, Nepal, Ethiopia, Cuba, Pakistan, and UAE.13–19,25,29,30 Even though many colleges’ pharmacy curricula do not offer a separate course on PC, it did not appear necessary to foster the students’ positive views. Our findings imply that existing pharmacy college courses in Yemen are beneficial in improving pharmacy students’ positive attitudes regarding PC.
About respondents’ attitudes toward the constructs of the PCAS more than fourth-fifth were mostly positive to “Professional benefit”, and “Professional duty”. However, more than half of the respondents negatively thought about the two items in “Return of effort” respectively. In this study, many students thought that “Pharmacy students can perform PC during their experiential training (placement)”. Pharmacy students should be allowed to offer PC directly to actual patients while being observed by experienced preceptors as part of their training experience. Moreover, pharmacy students must be involved in the full patient care process, from assessment to documentation and follow-up evaluation. The main goal of pharmacy students’ involvement is to assess them in establishing a patient care process (assessment, care plan, evaluation abilities), and to teach students the value of understanding their vital role.
Interestingly, in our study the item “Providing PC takes too much time and effort” received less than one-fifth disagreement. In studies conducted in USA and UAE reported higher disagreement. However, studies in Saudi, Kuwait, Cuba, Qatar, and Ethiopia reported lower disagreement than our results.15–18,31 A possible explanation may be the high number of patients visiting pharmacies and increased the number of prescriptions, and major pharmacist involvement in dispensing instead of hiring pharmacy technicians to perform this task. In Yemen, the pharmacist must be more patient-oriented by providing PC and conducting patient care, instead of performing the traditional tasks. Moreover, the lines between pharmacy technician duties and the pharmacist must be well established. Some routine dispensing activities are being transferred to skilled pharmacy technicians under supervision. As a result, Yemeni pharmacists will have more time and attention to devote to cognitive services. In fact, Strand and Cipolle had concluded that pharmacists could not perform both tasks simultaneously and in the same place; also, they stated that both tasks must be kept separate.31
Nearly half of the participants in our study disagreed that “Providing PC is not worth the additional workload that it a place on pharmacist”. The concept of PC in Yemen is still in its infancy, the traditional pharmacy curriculum still influences the patient-oriented pharmacy programs, and the PC is not almost implemented in most pharmacy practice settings yet. We believe that if students complete their internship or training in a setting where PC services are well-implemented, pharmacy students will recognize the significance of PC, particularly the health benefits and influence on clinical outcomes. Many studies have reported higher positive attitudes concerning this item, while others reported negative ones. These disparities could be attributable to the extent to which the PC care services were implemented in students trained and daily health care settings.
This study, the first of its kind, has evaluated different pharmacy programs (patient-oriented and traditional pharmacy programs) as contributing factors. Data in our study reveal that Pharm.D students had more positive attitudes toward providing PC compared to other pharmacy programs. Furthermore, they were more positively to items “The primary responsibility of pharmacist in all health care should be to prevent and solve medication-related problems”, “providing PC takes too much time and effort”, “I feel that PC is the right direction for the profession to be headed”, and “I feel that the PC movement will benefit pharmacist”. These findings may explain that Pharm.D program is more patient-oriented and more focused on clinical pharmacy education and provision of PC. It gives hope for Yemen’s clinical pharmacy future professional practice.
We have added “Do you currently work in any related pharmacy field?” as a counteracting factor to recognize that the universities curriculum matches the real-life pharmacy practice in this country. Interestingly, students who were employed had more positive attitudes compared to unemployed. Further, employed students responded more positively to the items “Pharmacists’ primary responsibility should be to practice PC”, “Pharmacy students can perform PC during their experiential training (placement)”, and “Providing PC takes too much time and effort”. In addition, our data results demonstrated that those employed were more positive on “PB”, “PD”, and “RE”. These findings show that pharmacy students in real-life pharmacy practice settings have realized the importance of implementing PC and generally feel well-prepared to implement it in daily pharmacy practice. Moreover, these shows that universities’ curricula were not far enough from daily practice.
Barriers to Provide PC
In order to expand the practice of PC, it is essential to identify the barriers that impede its implementation and plan strategies to overcome them. These barriers are not unique to Yemenis’ pharmacy students but are also widely reported in many other studies.13,18,19 Most respondents “strongly agree” or “agree” that the lack of access to the patient medical records in the pharmacy was highly perceived as a barrier to PC provision. This is consistent with studies in Qatar.8 In Yemen medical records are available only in hospitals, usually found as paper files. According to a study in the USA by Gernant, pharmacists’ access to medical records helps identify the drug-related problems.32
“Inadequate (hospital and community pharmacy) internship period” was also highly perceived as a barrier. This finding was expected since the Bachelor of Pharmacy program included only four months of community pharmacy internship, and many students do it on their own without direct supervision from the university. On the other hand, most Yemeni universities which provide Pharm.D and Bachelor of Clinical Pharmacy programs had 30, and 15 credits respectively limited to hospital wards.11 Moreover, most universities have not established their educational hospitals yet. In such a case, one or two governmental hospitals may serve as training settings for more than three universities’ medical students from different specializations. This overload could affect the quality of supervision that preceptors provide. This emphasizes the need to upgrade the Yemeni pharmacy curriculum by decreasing the excessive basic science load, introducing more patient-oriented courses, and establishing further introductory pharmacy practice experiences (IPPE) earlier in their pharmacy curriculum. Furthermore, oblige establishing educational hospitals for any university that will provide any medical specialty and hire skilled preceptors to suit the number of trained students.
In our study results, the lack of a private counseling area or appropriate pharmacy layout was perceived as a barrier. These results in line with studies in Qatar, Nepal, UAE.14,18,19 In Yemen, the pharmacy design should be changed to accompany the new pharmacist role. Establishing a private or semi-private counseling space would help encourage a confidential and comfortable counseling atmosphere. Most importantly, it will allow the pharmacist to contribute effectively to direct patient care.
In addition, PC provision requires therapeutic knowledge and clinical problem-solving skills. However, most respondents thought that they did not have enough such skills. In Thailand pharmacists reported a similar finding.21 The results could be attributed to the traditional pharmacy curriculum that still generally influences pharmacy programs in Yemen.
Study Strengths and Limitations
To the best of our knowledge, this study was the first in Yemen to study the understanding, attitudes, and perceived barriers of pharmacy students toward PC. Also this study is the first in the region to investigate pharmacy students’ understanding of PC. Moreover, many studies have recommended comparing understanding and attitudes among different pharmacy programs. Hence, this study has covered this issue. This study recruited a larger sample size and had cover five out of six governmental universities; from major cities of the country; thus study results could be generalized.
However, various potential limitations should be considered. Firstly, this study used a cross-sectional design, making it impossible to draw specific conclusions about the causal links between the dependent and independent variables. Second, like most self-administered questionnaire surveys, individuals may over-report socially favorable activities while under-reporting socially negative behaviors. Furthermore, it is possible that the participants answering questions in one hall could have influenced their responses.
Study Implications
Although the current curriculum seems effective in raising positive attitudes toward PC, more effort should be exerted on developing the current Yemeni pharmacy curriculum (eg inclusion of interprofessional education and experiential learning activities) rather than on adopting different programs without proper preparation. Moreover, this emphasizes the need to revise the Yemeni pharmacy curriculum by decreasing the excessive basic science load, introducing more patient-oriented courses, and establishing different introductory pharmacy practice experiences (IPPE) earlier in their journey. Furthermore, oblige establishing educational hospitals for any university that will provide any medical specialty and hire skilled preceptors to suit the number of trained students. In addition, action must be taken around the country to raise the level of awareness toward the role of the pharmacist to improve the image of pharmacists among other health care team members and the general public.
Conclusions
In the current study, pharmacy students had a moderate understanding of the newly introduced concept of PC. They expressed a very good attitude and willingness to implement PC. Pharm.D and employed students displayed positive attitudes compared to other groups. Lack of access to the patient medical record in the pharmacy and inadequate (hospital and community pharmacy) internship period were the main barriers identified. More effort should be exerted on developing the current Yemeni pharmacy curriculum rather than on adopting different pharmacy programs without proper preparation. The present study generates interest in future research that assesses the practiced pharmacists’ understanding, attitudes and perceived barriers toward PC.
Acknowledgments
We would like to acknowledge Dr. Mohammed Alshakka who obtained the ethical approval for this study and passed away with COVID-19 before he participated in this work. Also we would like to acknowledge final-year clinical pharmacy students (Mohammed Al-Adlani, Wigdan Adel) for helping in the data collection. Furthermore, special thanks to College of Clinical Pharmacy, Hodeidah University, for helping in conducting this study as it was the Bachelors’ degree research graduation for the principal investigator (Najmaddin).
Ethics Approval and Consent to Participate
The study protocol was approved by Ethics Research Committee at the Faculty of Medicine and Health Sciences, Aden University with research code (REC-116-2022) in compliances with the international conference of Harmonization (ICH). Verbal informed consent was acceptable and approved by the ethics committee. All participants were informed about the study objectives and they were also told that they could withdraw from the study at any time.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Berenguer B, La Casa C, de la Matta MJ, Martín-Calero MJ. Pharmaceutical care: past, present and future. Curr Pharm Des. 2004;10(31):3931–3946. doi:10.2174/1381612043382521
2. Allemann SS, van Mil JW, Botermann L, Berger K, Griese N, Hersberger KE. Pharmaceutical care: the PCNE definition 2013. Int J Clin Pharm. 2014;36(3):544–555. doi:10.1007/s11096-014-9933-x
3. Hepler CD. Clinical pharmacy, pharmaceutical care, and the quality of drug therapy. Pharmacotherapy. 2004;24(11):1491–1498. doi:10.1592/phco.24.16.1491.50950
4. Cipolle R, Strand L, Morley P. Pharmaceutical Care Practice: The Patient-Centered Approach to Medication Management. McGrawHill Medical; 2012. ISBN-13: 978-0071756389.
5. Lin G, Huang R, Zhang J, Li G, Chen L, Xi X. Clinical and economic outcomes of hospital pharmaceutical care: a systematic review and meta-analysis. BMC Health Serv Res. 2020;20(1):487. doi:10.1186/s12913-020-05346-8
6. Cazarim Mde S, de Freitas O, Penaforte TR, Achcar A, Pereira LR. Impact assessment of pharmaceutical care in the management of hypertension and coronary risk factors after discharge. PLoS One. 2016;11(6):e0155204. doi:10.1371/journal.pone.0155204
7. Shao H, Chen G, Zhu C, et al. Effect of pharmaceutical care on clinical outcomes of outpatients with type 2 diabetes mellitus. Patient Prefer Adherence. 2017;11:897–903. doi:10.2147/PPA.S92533
8. Babar ZU, Kousar R, Murtaza G, Azhar S, Khan SA, Curley L. Randomized controlled trials covering pharmaceutical care and medicines management: a systematic review of literature. Res Social Adm Pharm. 2018;14(6):521–539. doi:10.1016/j.sapharm.2017.06.008
9. Shanmugam S, Varughese J, Nair MA, et al. Pharmaceutical care for asthma patients: a developing country’s experience. J Res Pharm Pract. 2012;1(2):66–71. doi:10.4103/2279-042X.108373
10. Xi X, Huang Y, Lu Q, Ung COL, Hu H. Community pharmacists’ opinions and practice of pharmaceutical care at chain pharmacy and independent pharmacy in China. Int J Clin Pharm. 2019;41(2):478–487. doi:10.1007/s11096-019-00802-w
11. Al-Worafi YMA. Chapter.14—pharmacy practice in Yemen. In: Fathelrahman AI, Ibrahim MIM, Wertheimer AI, editors. Pharmacy Practice in Developing Countries. Boston: Academic Press; 2016.
12. Yousuf SA, Alshakka M, Badulla WFS, Ali HS, Shankar PR, Mohamed Ibrahim MI. Attitudes and practices of community pharmacists and barriers to their participation in public health activities in Yemen: mind the gap. BMC Health Serv Res. 2019;19(1):304. doi:10.1186/s12913-019-4133-y
13. Martin BC, Chisholm MA. Cross-validation of an instrument measuring students attitudes toward pharmaceutical care. Am J Pharm Educ. 1999;63:46–51.
14. Baral SR, Parajuli DR, Shrestha S, et al. Undergraduate pharmacy students’ attitudes and perceived barriers toward provision of pharmaceutical care: a multi-institutional study in Nepal. Integr Pharm Res Pract. 2019;8:47–59. doi:10.2147/IPRP.S203240
15. Martinez Sanchez ADLM, delSol AB. Assessment of attitudes of Cuban university pharmacy students toward pharmaceutical care. Indian J Pharm Educ. 2016;50(4):504–511. doi:10.5530/ijper.50.4.1
16. Al-Arifi MN. Pharmacy students attitudes toward pharmaceutical care in Riyadh region Saudi Arabia. Pharm World Sci. 2009;31(6):677–681. doi:10.1007/s11096-009-9331-y
17. Katoue MG, Awad AI, Schwinghammer TL, Kombian SB. Pharmaceutical care education in Kuwait: pharmacy students’ perspectives. Pharm Pract. 2014;12(3):411. doi:10.4321/s1886-36552014000300002
18. ElHajj MS, Hammad AS, Afifi HM. Pharmacy students’ attitudes toward pharmaceutical care in Qatar. Ther Clin Risk Manag. 2014;10:121–129. doi:10.2147/TCRM.S56982
19. Tawfiq AM, Alomar MJ, Hassan N, Palaian S, MacLure K. Nationwide survey on attitudes and perceived barriers toward provision of pharmaceutical care among final year undergraduate pharmacy students in the United Arab Emirates. PLoS One. 2021;16(2):e0246934. doi:10.1371/journal.pone.0246934
20. Dunlop JA, Shaw JP. Community pharmacists’perspectives on pharmaceutical care implementation in New Zealand. Pharm World Sci. 2002;24(6):224–230. doi:10.1023/A:1021526425458
21. Ngorsuraches S, Li SC. Thai pharmacists’ understanding, attitudes, and perceived barriers related to providing pharmaceutical care. Am J Health Syst Pharm. 2006;63(21):2144–2150. doi:10.2146/ajhp060054
22. El Hajj MS, Al-Saeed HS, Khaja M. Qatar pharmacists’ understanding, attitudes, practice and perceived barriers related to providing pharmaceutical care. Int J Clin Pharm. 2016;38(2):330–343. doi:10.1007/s11096-016-0246-0
23. Chisholm MA, Martin BC. Development of an instrument to measure student attitudes concerning pharmaceutical care. Am J Pharm Educ. 1997;61:374–379.
24. Elnaem MH, Jamshed SQ, Elkalmi RM. The future of pharmaceutical care in Malaysia: pharmacy students’ perspectives. Pharm Educ. 2017;17(1):215–222.
25. Hussain I, Rasool MF, Imran I, et al. Assessment of undergraduate pharmacy students’ attitude towards pharmaceutical care in Pakistan: practice implications. J Multidiscip Healthc. 2020;13:1517–1525. doi:10.2147/JMDH.S282776
26. Al-Worafi YM. Pharmacy practice and its challenges in Yemen. Australas Med J. 2014;7(1):17–23. doi:10.4066/AMJ.2014.1890
27. Ministry of Public Health and Population. National guide of clinical pharmacy. Available from: https://moh.gov.ye/nc_archive_files.aspx?id=1.
28. Aburuz S, Al-Ghazawi M, Snyder A. Pharmaceutical care in a community-based practice setting in Jordan: where are we now with our attitudes and perceived barriers? Int J Pharm Pract. 2012;20(2):71–79. doi:10.1111/j.2042-7174.2011.00164.x
29. Ubaka CM, Ekwunife OI, Adibe MO. Does the clinical clerkship course improve students’ attitudes towards pharmaceutical care? Int J Pharm Pract. 2012;20(4):272–274. doi:10.1111/j.20427174.2012.00191.x
30. Tsega B, Bhagavathula AS, Sarkar BR, Melaku T, Shewamene Z. Impact of clerkship attachments on students’ attitude toward pharmaceutical care in Ethiopia. Adv Med Edu Pract. 2015;6:385–391. doi:10.2147/AMEP.S80802
31. Strand LM, Cipolle RJ, Morley PC, Frakes MJ. The impact of pharmaceutical care practice on the practitioner and the patient in the ambulatory practice setting: twenty-five years of experience. Curr Pharm Des. 2004;10(31):3987–4001. doi:10.2174/1381612043382576
32. Gernant SA, Zillich AJ, Snyder ME. Access to medical records’ impact on community pharmacist-delivered medication therapy management: a pilot from the medication safety research network of Indiana (Rx-SafeNet). J Pharm Pract. 2018;31(6):642–650. doi:10.1177/0897190017735422
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.