Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
A Maltese Study in Determining the Presence of Chronic Obstructive Pulmonary Disease in Metabolic Syndrome
Authors Gauci J, Gauci Pullicino S, Caruana E, Petroni Magri V, Formosa MM, Fenech AG, Fava S, Montefort S, Fsadni P
Received 12 March 2026
Accepted for publication 29 May 2026
Published 11 June 2026 Volume 2026:21 608737
DOI https://doi.org/10.2147/COPD.S608737
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Zijing Zhou
Jonathan Gauci,1,2 Stephanie Gauci Pullicino,1,2 Emma Caruana,2 Vanessa Petroni Magri,3,4 Melissa M Formosa,3,5 Anthony G Fenech,3,5 Stephen Fava,1,2 Stephen Montefort,2 Peter Fsadni1,2
1Department of Medicine, Mater Dei Hospital, Msida, Malta; 2Department of Medicine, Faculty of Medicine & Surgery, University of Malta, Msida, Malta; 3Centre for Molecular Medicine and Biobanking, University of Malta, Msida, Malta; 4Department of Clinical Pharmacology and Therapeutics, Faculty of Medicine & Surgery, University of Malta, Msida, Malta; 5Department of Applied Biomedical Science, Faculty of Health Sciences, University of Malta, Msida, Malta
Correspondence: Jonathan Gauci, Department of Medicine, Faculty of Medicine & Surgery, University of Malta, Msida, Malta, Email [email protected]
Introduction: Both Chronic Obstructive Pulmonary Disease (COPD) and Metabolic Syndrome (MetS) are pro-inflammatory states, and while the diagnosis of MetS in COPD has been extensively studied, the diagnosis of COPD in MetS is poorly studied. The study focuses on determining the presence of COPD in persons living with diabetes and MetS in Malta, and aims to identify differences in biomarkers between MetS subjects with and without COPD.
Materials and Methods: Diabetic MetS subjects at Malta’s main general hospital were assessed through St George’s Respiratory Questionnaire for COPD (SGRQ-C), modified Medical Research Council scale (mMRC), COPD Assessment Test (CAT), Centre for Epidemiological Studies Depression scale (CES-D), Functional Assessment of Chronic Illness Therapy (FACIT) Fatigue scale, Spirometry, Six Minute Walk Test (6MWT), BODE index (composed of Body Mass Index, Obstruction, Dyspnoea, Exercise capacity) and routine blood tests. They were divided into three groups: the main study group consisted of MetS subjects with COPD, one control group consisted of MetS subjects with a smoking history but not COPD, and the other control group consisted of diabetic MetS subjects with no smoking history.
Results: A total of 67 MetS subjects were included. Those with COPD had significantly worse outcomes in SGRQ-C scores, mMRC, CAT, spirometry, BODE, CES-D and FACIT Fatigue scale than smokers without COPD and non-smokers. 25-hydroxy-vitamin D levels were significantly lower in MetS subjects with COPD compared to smokers without COPD (p=0.030) and non-smokers (p=0.043). C-reactive protein (p=0.036), triglycerides (p=0.023) and total cholesterol (p=0.039) were significantly higher in MetS subjects with COPD compared to smokers without COPD.
Discussion: Screening for depression and fatigue in subjects with COPD and MetS is recommended. Low vitamin D, high CRP, high triglyceride and high total cholesterol levels are correlated with a COPD diagnosis within the local MetS population, and monitoring these parameters would enable timely management.
Keywords: chronic obstructive pulmonary disease, metabolic syndrome, biomarkers
Introduction
Research on biomarkers in Chronic Obstructive Pulmonary Disease (COPD) is beneficial because it may lead to the emergence of future treatments. The Evaluation of COPD Longitudinally to Identify Predictive Surrogate End-points (ECLIPSE) study was a multi-centre research project which identified numerous COPD biomarkers. The cases in the ECLIPSE study were Global Initiative for Chronic Obstructive Lung Disease (GOLD) stage II–IV COPD patients aged between 40 and 75 years, and the two control groups consisted of smokers without COPD and non-smokers.1
COPD and Metabolic Syndrome (MetS) are both pro-inflammatory states which appear to be linked.2 MetS is a multi-faceted disease comprising several interrelated components that increase the risk of atherosclerosis and type 2 diabetes.3 The American Heart Association (AHA) and National Heart Lung and Blood Institute (NHLBI) define MetS as three out of five of abdominal obesity, high triglycerides (or on triglyceride-lowering treatment), low levels of high density lipoprotein (HDL) cholesterol (or on HDL-improving treatment), high blood pressure (or on anti-hypertensive treatment), and high fasting glucose (or on glucose-lowering treatment).4
The diagnosis of MetS in COPD has been previously studied to a significant degree. In contrast, international data on COPD in MetS is lacking. The study therefore aimed to focus on COPD in MetS, which is of particular importance in Malta, where one quarter of the adult population is obese and one-tenth is diabetic.5,6 The presence of COPD actually worsens MetS through increased systemic inflammation, chronic oxidative stress, physical inactivity and the consequences of systemic steroids.7 This results in worse respiratory and cardiovascular outcomes for people living with both conditions.7
The study aimed to identify differences in biomarkers in Maltese MetS subjects with and without COPD. A similar approach to the ECLIPSE study was adopted, within the context of diabetics with MetS in Malta. The study hypothesis was that there is a significant difference in clinical and blood parameters when comparing MetS subjects with COPD and MetS subjects without COPD.
Materials and Methods
Research Study Enrolment
Research subjects were enrolled into the study from the Diabetes clinic at the main general hospital in Malta. The enrolment period was from March 2021 to December 2022, and the convenience sampling method was used. Using a sample size calculator, it was determined that at least 66 participants were required (66 from an estimated diabetic adult population of 35,000 gives a margin of error of 9.93%).
The study included all persons living with type 2 diabetes aged 40 to 75 years who were willing to participate in the research project. All participants were fully informed about the study’s purpose, and formal written consent was obtained.
Each subject was interviewed to check for any exclusion criteria. The exclusion criteria comprised a history of respiratory disease, diabetes or pre-diabetes other than type 2 diabetes, malignancy in the past 5 years, other inflammatory disorders, and infection or use of systemic steroids in the past 4 weeks. Individuals receiving vitamin D supplementation were also excluded, as were those unable to give consent.
Following this initial step, the remaining participants were invited to attend for the respiratory assessment session which was scheduled shortly after the date of enrolment.
Respiratory Assessment Session
Assessment of all research subjects was performed at the outpatients department of the main general hospital, following an overnight fast of eight hours. Demographics, drug history, smoking history and exacerbation history were recorded. The St George’s Respiratory Questionnaire for COPD patients (SGRQ-C)8 was carried out, followed by the COPD Assessment Test (CAT)9 and the modified Medical Research Council (mMRC) score.10 Risk for depression was evaluated using the Centre for Epidemiological Studies – Depression (CES-D) scale,11 and fatigue was evaluated using the Functional Assessment of Chronic Illness Therapy (FACIT) Fatigue scale.12
The following parameters were measured: waist circumference (at upper part of iliac crests following expiration), blood pressure (using manual sphygmomanometer), height (using stadiometer) and weight. The six-minute walking distance (6MWD) was obtained following a six-minute walk test (6MWT) in accordance with the local hospital protocol based on the American Thoracic Society 2002 guidelines.13 Spirometry was performed using a portable Medical International Research® Spirolab III® spirometer in accordance with the 2019 joint American Thoracic Society and European Respiratory Society Technical Statement on Standardisation of Spirometry.14 Reversibility testing was performed in order to obtain the post-bronchodilator FEV1 (Forced Expiratory Volume in 1 second), FVC (Forced Vital Capacity) and FEV1/FVC ratio. Fractional Exhaled Nitric Oxide (FeNO) testing was performed using a portable Bedfont® NObreath® FeNO monitor. Body Mass Index (BMI) was calculated from height and weight. BODE index was calculated from BMI, Obstruction (FEV1 from spirometry), Dyspnoea (mMRC scale) and Exercise capacity (6MWD).
Venous blood was analysed in the same local laboratory. Phlebotomy was performed in accordance with the Clinical and Laboratory Standards Institute recommendations.15 The following blood tests were requested: complete blood count (CBC), erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), renal profile, procalcitonin, ferritin, fibrinogen, 25-hydroxy-vitamin D, liver function tests, lipid profile, glycosylated haemoglobin (HbA1c), fasting blood glucose, N-terminal pro brain natriuretic peptide (NT-proBNP) and creatine kinase (CK).
Through this assessment, persons living with type 2 diabetes were screened for MetS and for COPD. The diagnosis of MetS was based on AHA and NHLBI criteria.4 The diagnosis of COPD was based on the GOLD definition, which is a fixed ratio of post-bronchodilator FEV1/FVC < 0.7.16 However, later in the analysis COPD was also defined as FEV1/FVC < LLN (Lower Limit of Normal), and a sensitivity analysis using the LLN instead of the fixed ratio was performed in order to identify true obstruction, particularly since several participants were obese. The Global Lung Function Initiative (GLI) 2012 equations were used to calculate the predicted FEV1/FVC ratio and the LLN.17 As in the ECLIPSE study, there were three study groups. Study Group 1 was the main study group, which consisted of MetS subjects with COPD. Study Group 2 consisted of MetS subjects with a smoking history but not COPD. Study Group 3 consisted of diabetic MetS subjects with no smoking history.
Statistical Analysis
Data analysis was carried out through the Statistical Package for the Social Sciences (SPSS®) Version 29.0.0.0. Two study groups at a time were compared using the independent samples t-test or the Mann Whitney U-test, where a p-value of <0.05 indicated that there was a statistically significant difference between the two groups. The normality of the clinical or blood parameter was checked using the Shapiro–Wilk test, where a Shapiro–Wilk p-value of >0.05 indicated a normal distribution. The independent samples t-test was used when the parameter was normally distributed in both study groups, while the Mann Whitney U-test was used when the parameter was not normally distributed in both study groups. Both tests were used when the parameter was normally distributed in one group but not in the other. Levene’s p-value was noted in order to check if the variances were significantly different, where a Levene’s p-value of >0.05 indicated that the variances were not significantly different and therefore the independent samples t-test p-value where equal variances assumed was noted. The results of the comparison were displayed with an error bar graph. However the method used to determine the presence of a statistically significant difference was the p-value of the hypothesis test rather than whether or not there was an overlap in confidence intervals on the error bar graph (the latter method may lead to type II errors).
Results
Enrolment Process
104 persons at Diabetes clinic aged 40–75 years accepted to participate in the study. Of these, 37 were excluded from the study in view of one or more exclusion criteria (Figure 1). There were no eligible participants who were unable to give consent.
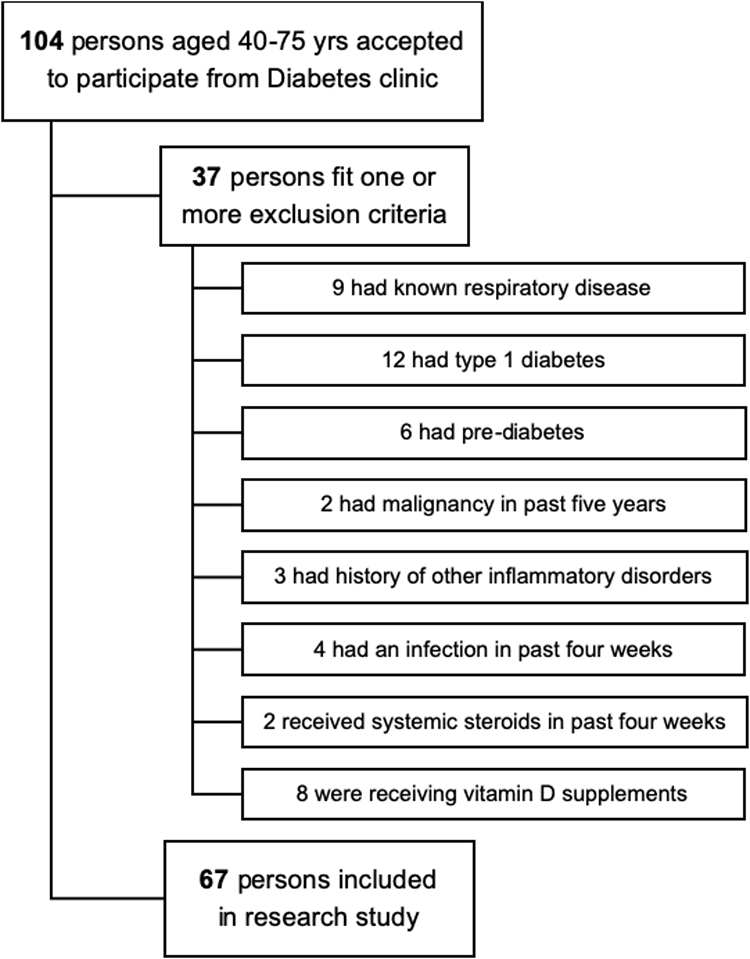 |
Figure 1 Study Participant Enrolment Process. |
Demographics
A total of 67 persons living with type 2 diabetes were recruited into the study (Figure 1). All of these were found to meet the criteria for MetS since they all received a statin and an anti-hypertensive agent. The participants were divided into three study groups, as shown in Table 1. This table also shows the gender distribution and the smoking status of participants in each study group.
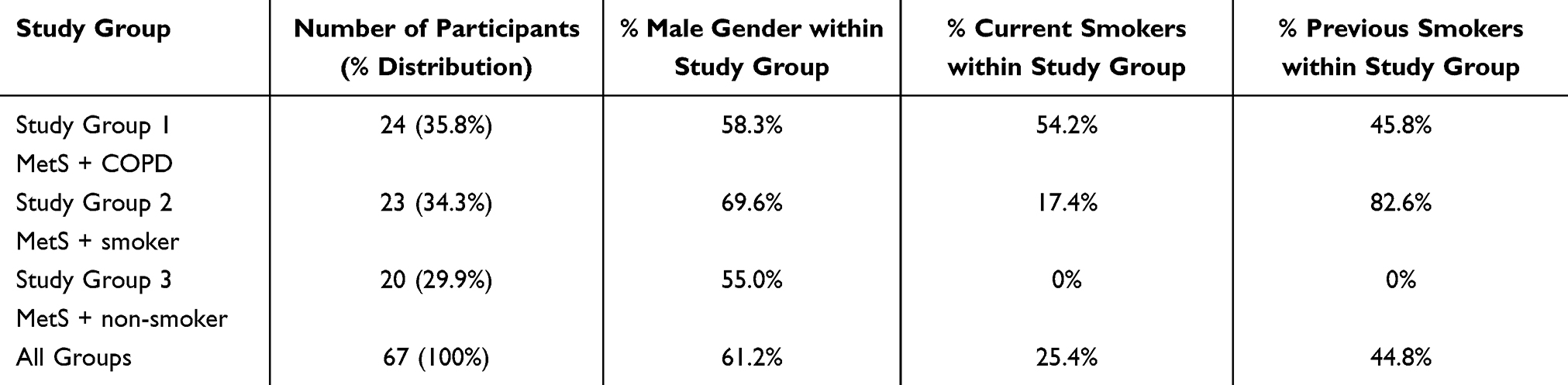 |
Table 1 Distribution of Participants According to Study Group |
Study Groups 1 vs 2
Table 2 compares the clinical and blood parameters in Study Group 1 vs 2, with the statistically significant p-values shown in bold.
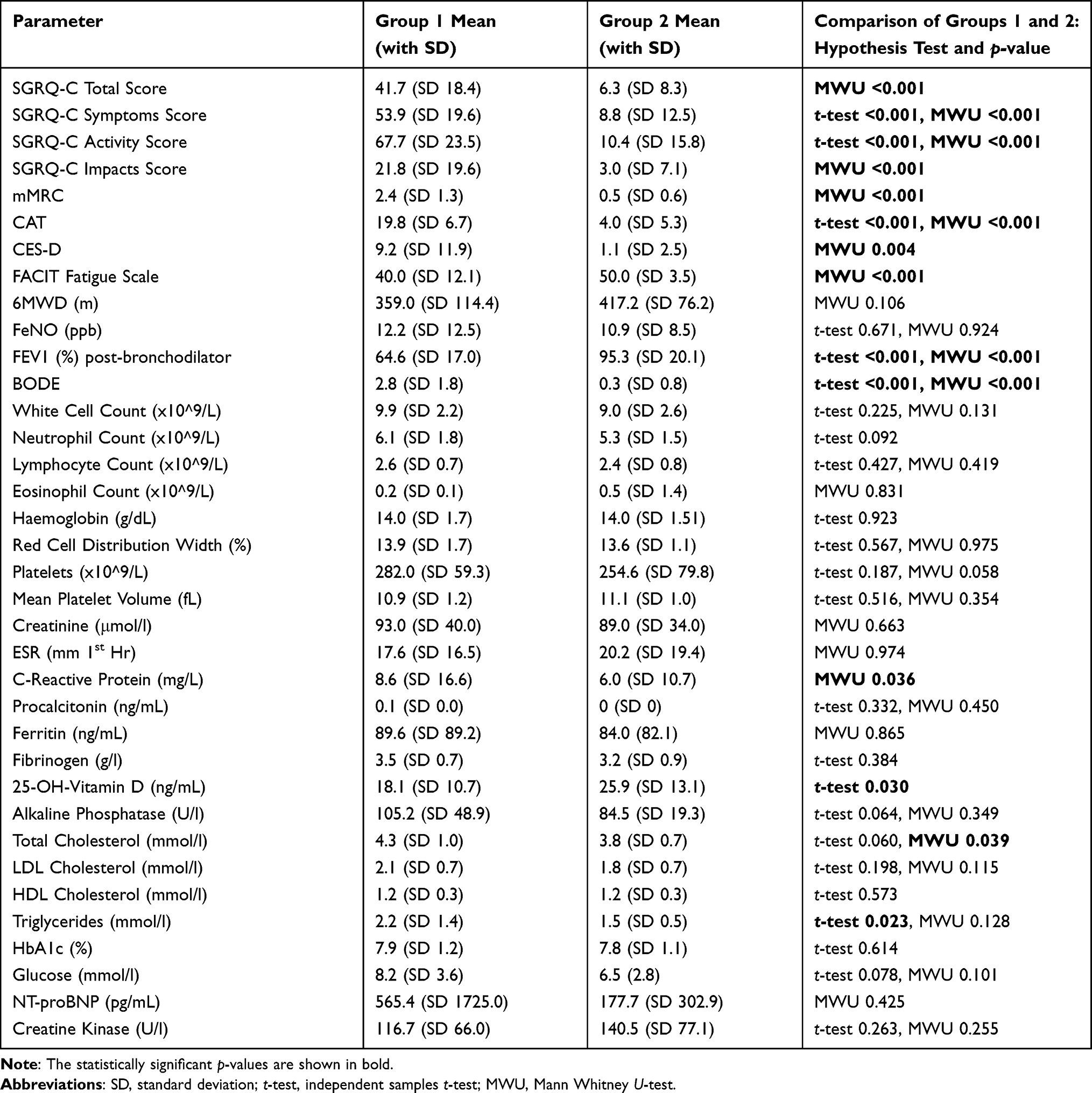 |
Table 2 Comparison of All Parameters Between Study Groups 1 (MetS + COPD) and 2 (MetS + Smoker) |
Figures 2–5 are graphs displaying the comparison of CRP, 25-hydroxy-vitamin D, triglycerides, and total cholesterol levels respectively between Study Groups 1 and 2. The error bars represent 95% confidence intervals.
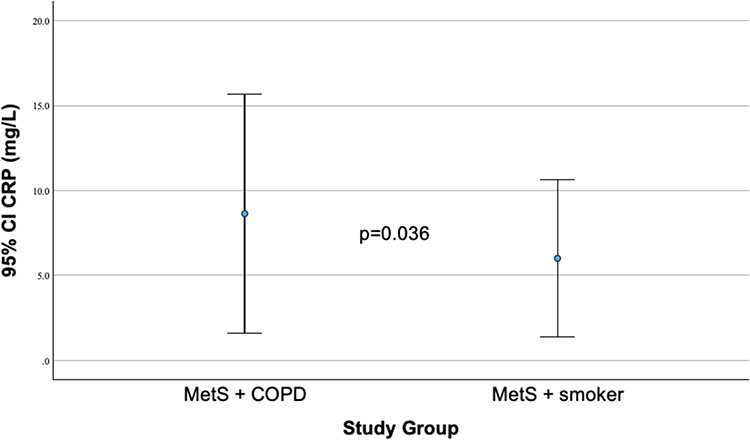 |
Figure 2 Comparison of CRP between MetS + COPD (Study Group 1) and MetS + smoker (Study Group 2). |
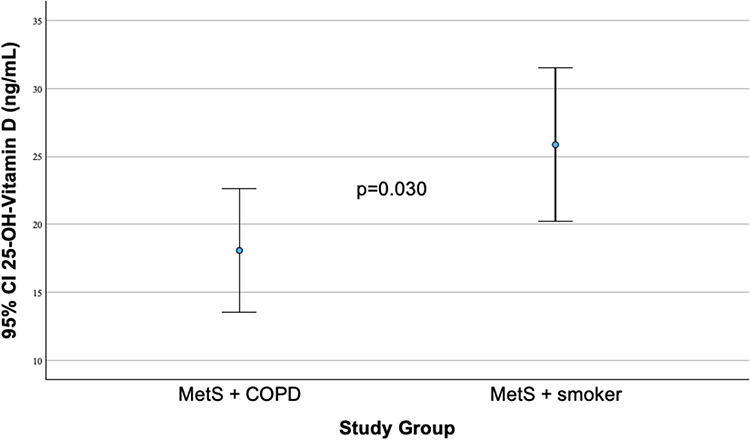 |
Figure 3 Comparison of 25-hydroxy-Vitamin D between MetS + COPD (Study Group 1) and MetS + smoker (Study Group 2). |
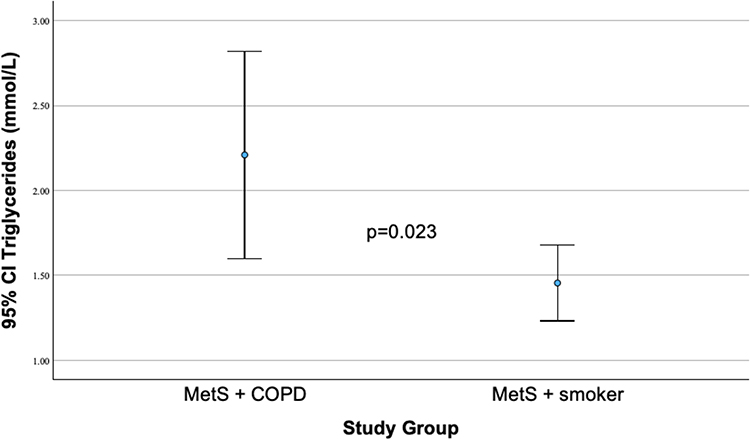 |
Figure 4 Comparison of Triglycerides between MetS + COPD (Study Group 1) and MetS + smoker (Study Group 2). |
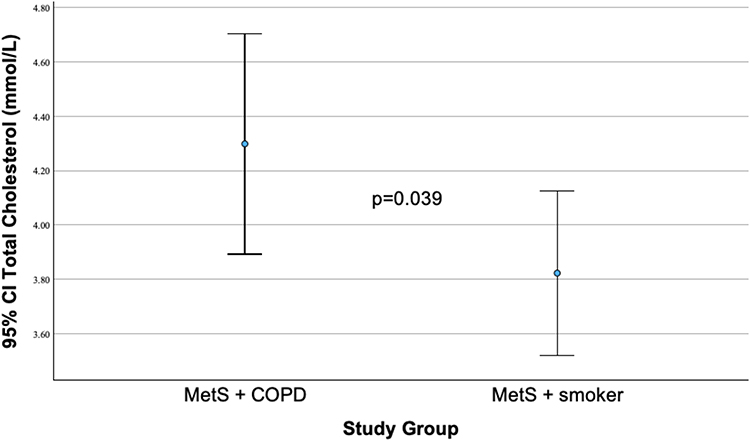 |
Figure 5 Comparison of Total Cholesterol between MetS + COPD (Study Group 1) and MetS + smoker (Study Group 2). |
Study Groups 1 vs 3
Table 3 compares the clinical and blood parameters in Study Group 1 vs 3, with the statistically significant p-values shown in bold.
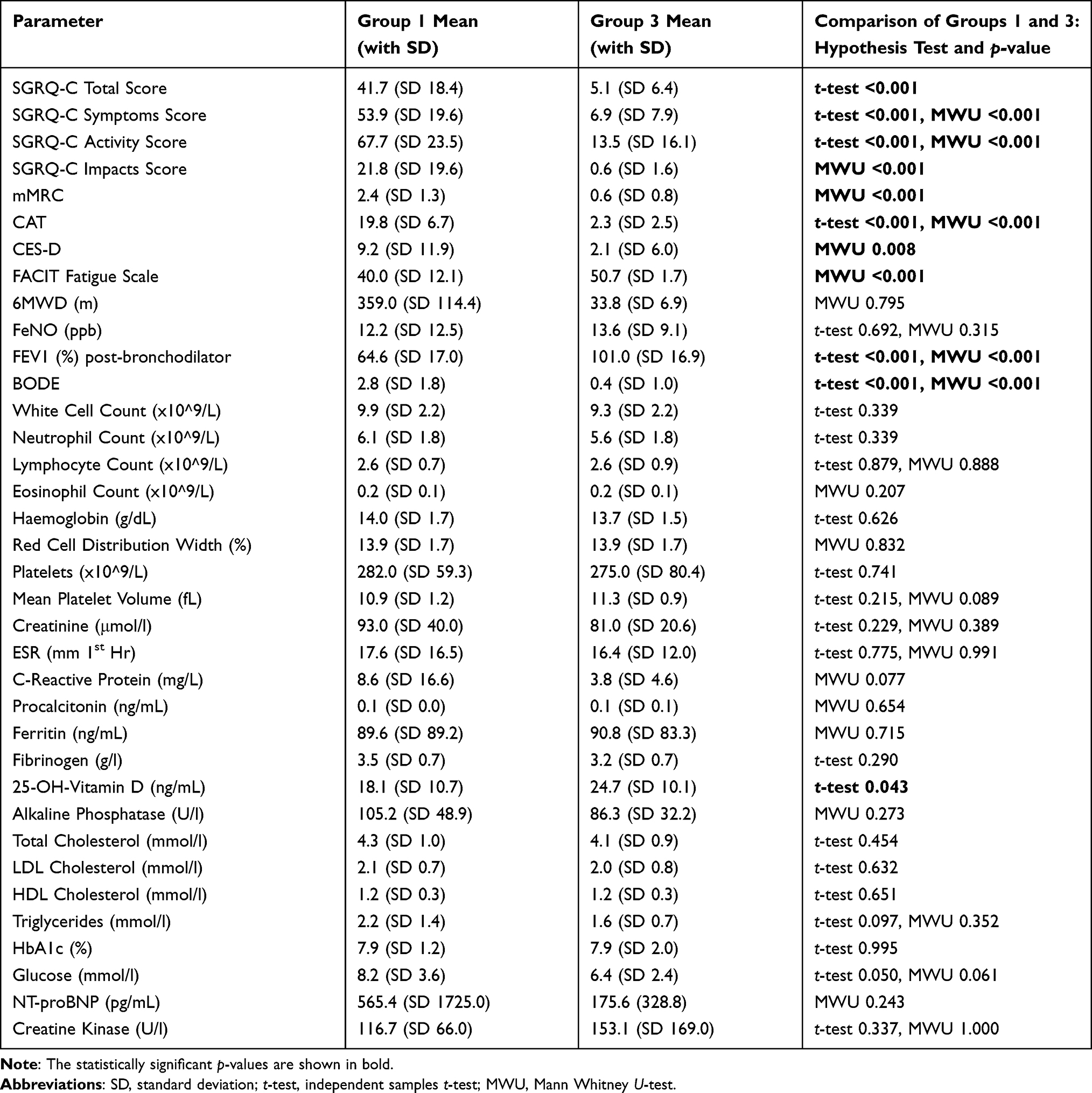 |
Table 3 Comparison of All Parameters Between Study Groups 1 (MetS + COPD) and 3 (MetS + Non-Smoker) |
Figure 6 is a graph displaying the comparison of 25-hydroxy-vitamin D levels between Study Groups 1 and 3. The error bars represent 95% confidence intervals.
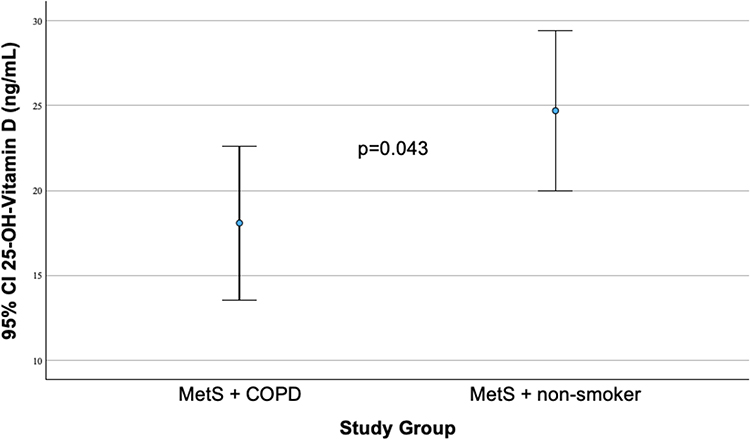 |
Figure 6 Comparison of 25-hydroxy-Vitamin D between MetS + COPD (Study Group 1) and MetS + non-smoker (Study Group 3). |
Study Groups 2 vs 3
There were no significant differences in the clinical and blood parameters between Study Groups 2 and 3.
Discussion
In order to study the presence of COPD in MetS, one can analyse the results of Study Groups 1 (COPD and MetS subjects) vs 2 (MetS subjects who did not have COPD but had a smoking history) as well as the results of Study Groups 1 vs 3 (MetS subjects who did not have COPD and were non-smokers).
Subjects with both COPD and MetS had significantly higher SGRQ-C Total, Symptoms, Activity and Impacts scores than the other two study groups. Similarly, they also had a higher mMRC score and CAT score than the controls. These respiratory symptom score differences are likely to be due to the airflow obstruction which is characteristic of COPD.
An interesting finding is that subjects with both COPD and MetS also had a higher CES-D score (reflecting increased risk for depression) and a lower FACIT Fatigue score (reflecting more fatigue) than the control groups. Depression is known to be a common co-morbidity in COPD, and a 2017 systematic review on COPD reported a depression prevalence of 30%.18 There may therefore be a role for screening COPD patients for depression and referring for treatment in order to improve quality of life. Fatigue has also been found to be widely prevalent in COPD previously; a 2021 systematic review on COPD reported a fatigue prevalence of 17–95%.19 Screening for fatigue is important because this condition may have economic and social repercussions which may need addressing.
Subjects in the main study group (COPD and MetS) had a significantly lower FEV1 value than Study Groups 2 and 3 – this can also be explained by the persistent airflow obstruction characteristic of COPD. Since the BODE index reflects FEV1 and mMRC, then it follows that Study Group 1 had a significantly higher BODE index than Study Groups 2 and 3.
CRP was found to be significantly higher in participants with COPD and MetS than in MetS subjects who did not have COPD but had a smoking history. For more than two decades, CRP has been extensively studied as a biomarker of systemic inflammation, which is characteristic of COPD.20–23 Chandatre et al showed in a 2025 Indian study that mean CRP level was significantly higher in stable COPD patients compared to controls, and that CRP increases with GOLD stages24 Participants with recent exacerbations were excluded in both the local study and the Indian study, and therefore both studies conclude that high CRP levels in the clinically stable phase of COPD are due to persistent low-grade systemic inflammation irrespective of acute triggers. Even small rises in CRP are clinically meaningful because they indicate low-grade inflammation and increased cardiovascular risk.25 Chandratre et al suggest that CRP may be used to monitor the progression of COPD, and that it may aid COPD therapy decisions, though clinical trials are needed in this respect.24
Levels of 25-hydroxy-vitamin D were lower in the main study group (COPD and MetS) than in the two control groups who did not have COPD. A high prevalence of vitamin D deficiency has been described in COPD and is due to several factors such as lack of sunlight exposure, smoking, poor diet, co-morbidities and persistent inflammation.26,27 This is particularly relevant to the study population since exposure to sunlight in Malta is usually above average due to the Mediterranean climate (Köppen classification).28 Vitamin D levels were inversely associated with risk and severity of COPD according to a 2016 systematic review and meta-analysis,29 suggesting a role for screening for vitamin D deficiency in COPD patients and in smokers, and consequently supplementing Vitamin D if deficient.
Triglyceride levels were higher in COPD and MetS subjects than in MetS participants who did not have COPD but had a smoking history. The finding of higher triglyceride levels in COPD patients has been previously described.30 High serum triglyceride levels are associated with increased insulin resistance, which contributes to COPD progression through several mechanisms, including the activation of inflammatory pathways resulting in small airway fibrosis and alveolar wall destruction.31,32 Another theory is that high serum triglyceride levels may lead to increased intracellular lipid molecules and therefore increased rigidity of the lung parenchyma, resulting in increased airway resistance and airflow limitation, though this mechanism is not fully understood.33 These relationships suggest there may be a role for screening for and treating high triglyceride levels in COPD clinic. A 2020 Taiwanese study concluded that statins and fibrates reduced COPD risk in hyperlipidaemic patients in a dose-dependent manner.34
Total cholesterol levels were higher in COPD and MetS cases than in smoking controls with MetS but not COPD. The low density lipoprotein (LDL) cholesterol and HDL cholesterol components did not show significant differences. The authors hypothesize that remnant cholesterol (the portion of cholesterol which is not found in LDL or HDL cholesterol) is responsible for this relationship with COPD risk. A 2025 Chinese study by Feng et al also showed an association between high remnant cholesterol and increased COPD risk, possibly because remnant cholesterol accumulates in arterial walls, resulting in local and systemic inflammation, increasing risk of inflammatory conditions including COPD.35,36 Feng et al recommend lifestyle changes to lower remnant cholesterol levels and consequently decrease COPD risk, though this approach requires further investigation.35
Taken together, the results provide further evidence that increased systemic inflammation and metabolic disturbances are connected and central to the pathophysiology of COPD in MetS. Although spirometric screening for COPD in the asymptomatic general population is generally not recommended (since early detection of COPD was not found to alter the prognosis), there is no guidance on screening for COPD in people living with MetS, both symptomatic and asymptomatic.37 Further studies are recommended to evaluate whether an earlier diagnosis of COPD in MetS is associated with better outcomes.
We note that there was a statistically significant difference in CRP, triglycerides and total cholesterol between Groups 1 and 2 but not between Groups 1 and 3. This is likely to be due to the heterogeneity in statin use across the study population: different statins would affect the CRP, triglycerides and total cholesterol to a different extent.
Strengths and Limitations
This study is important because there is a lack of data on the diagnosis and presence of COPD in MetS, both in the local population and internationally. Although the total number of participants was not large, each participant was assessed in great detail through several robust tools. Moreover, the presence of two control groups allowed for contrast between the three sample populations, through the utilisation of the independent samples t-test or the Mann Whitney U-test which compared two groups at a time.
An important limitation is the small sample population size, which may decrease statistical power. This was partly due to the exclusion criteria, which were essential to decrease confounding factors. Furthermore, the coronavirus disease 19 pandemic may have affected the research study enrolment phase. While excluding participants on vitamin D supplementation was done to reduce confounding, this may reduce generalizability, since several COPD patients receive vitamin D supplementation.
The cross-sectional design signifies that the study can measure correlations, but not determine causality. An element of bias may have been introduced by the convenience sampling method, and by confounding factors such as age, gender, smoking status and drug history. Moreover, those with a smoking history may have been more likely to accept to participate in the study than non-smokers, as the former may have been more concerned about the possibility of smoking-related lung disease and may have viewed the study as a health check-up.
Another limitation was due to the potential reduction in FVC due to obesity in MetS subjects, which would result in a higher FEV1/FVC ratio, potentially missing a true diagnosis of COPD.38 The sensitivity analysis using the LLN (rather than the fixed FEV1/FVC ratio ratio) for COPD diagnosis identified 2 obese smokers who were likely underdiagnosed with COPD.
A further limitation was due to the AHA and NHLBI criteria for MetS. Whereas the researchers adhered to this definition, we believe that some type 2 diabetics were misclassified as MetS simply because they were receiving a statin and an angiotensin converting enzyme inhibitor (ACEI) for prognostic benefit and therefore fulfilled at least three AHA and NHLBI criteria. Moreover, the heterogeneity in statin use across the study population may have an impact on the results; we suggest further studies with possible subgroup analyses to evaluate the effects of statins.
Conclusions
The presence of COPD in MetS is correlated with higher levels of respiratory symptoms, depression, fatigue, CRP, triglycerides and total cholesterol, as well as lower lung function and 25-hydroxy-vitamin D levels. Monitoring CRP and screening for depression, fatigue, high triglycerides, low vitamin D, and high remnant cholesterol levels may be beneficial in people with MetS and COPD.
Abbreviations
COPD, Chronic Obstructive Pulmonary Disease; ECLIPSE, Evaluation of COPD Longitudinally to Identify Predictive Surrogate End-points; GOLD, Global Initiative for Chronic Obstructive Lung Disease; MetS, Metabolic Syndrome; AHA, American Heart Association; NHLBI, National Heart Lung and Blood Institute; HDL, High Density Lipoprotein; SGRQ-C, St George’s Respiratory Questionnaire for COPD patients; CAT, COPD Assessment Test; mMRC, modified Medical Research Council; CES-D, Centre for Epidemiological Studies – Depression; FACIT, Functional Assessment of Chronic Illness Therapy Fatigue scale.; 6MWD, Six-Minute Walking Distance; 6MWT, Six-Minute Walk Test; FEV1, Forced Expiratory Volume in 1 second; FVC, Forced Vital Capacity; FeNO, Fractional Exhaled Nitric Oxide; BMI, Body Mass Index; BODE, Body Mass Index, Obstruction, Dyspnoea and Exercise capacity; CBC, Complete Blood Count; ESR, Erythrocyte Sedimentation Rate; CRP, C-Reactive Protein; HbA1c, Glycosylated Haemoglobin; NT-proBNP, N-Terminal pro Brain Natriuretic Peptide; CK, Creatine Kinase; LLN, Lower Limit of Normal; GLI, Global Lung function Initiative; SPSS, Statistical Package for the Social Sciences; SD, Standard Deviation; MWU, Mann Whitney U; LDL, Low Density Lipoprotein; ACEI, Angiotensin Converting Enzyme Inhibitor; 25-OH-Vitamin D, 25-hydroxy-Vitamin D; CI, Confidence Intervals.
Ethics Approval and Informed Consent
The study complies with the Declaration of Helsinki and was approved by the Research Ethics Committee of the Faculty of Medicine and Surgery at the University of Malta (Reference Number FRECMDS_1819_125).
Acknowledgment
The results of Study Group 1 were published in an article entitled ‘Chronic Obstructive Pulmonary Disease and Metabolic Syndrome: A Maltese Study on Biomarkers and Clinical Implications’ by the same authors.39
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors received financial support from the Department of Medicine, Faculty of Medicine & Surgery, University of Malta and from Malta Enterprise, Malta’s economic development agency.
Disclosure
All authors declare that they have no conflicts of interest for this work.
References
1. Vestbo J, Anderson W, Coxson HO, et al. Evaluation of COPD Longitudinally to Identify Predictive Surrogate End-points (ECLIPSE). Eur Respir J. 2008;31(4):869–12. doi:10.1183/09031936.00111707
2. Vujic T, Nagorni O, Maric G, Popovic L, Jankovic J. Metabolic syndrome in patients with chronic obstructive pulmonary disease: frequency and relationship with systemic inflammation. Hippokratia. 2016;20(2):110–114.
3. Kassi E, Pervanidou P, Kaltsas G, Chrousos G. Metabolic syndrome: definitions and controversies. BMC Med. 2011;9(1):48. doi:10.1186/1741-7015-9-48
4. Grundy SM, Cleeman JI, Daniels SR, et al; American Heart Association; National Heart, Lung, and Blood Institute. Diagnosis and management of the metabolic syndrome: an American Heart Association/National Heart, Lung, and Blood Institute Scientific Statement. Circulation. 2005;112(17):2735–2752. doi:10.1161/CIRCULATIONAHA.105.169404
5. European Observatory on Health Systems and Policies. Malta health system review. Health Syst Trans. 2017;19(1):1–37.
6. International Diabetes Federation. IDF Diabetes Atlas.
7. Naik D, Joshi A, Paul TV, Thomas N. Chronic obstructive pulmonary disease and the metabolic syndrome: consequences of a dual threat. Indian J Endocrinol Metab. 2014;18(5):608–616. doi:10.4103/2230-8210.139212
8. Jones PW, Forde Y. St George’s Respiratory Questionnaire for COPD patients (SGRQ-C) Manual Version No.1.3; 2016.
9. Jones PW, Harding G, Berry P, Wiklund I, Chen WH, Kline Leidy N. Development and first validation of the COPD assessment test. Eur Respir J. 2009;34(3):648–654. doi:10.1183/09031936.00102509
10. Mahler DA, Wells CK. Evaluation of clinical methods for rating dyspnea. Chest. 1988;93(3):580–586. doi:10.1378/chest.93.3.580
11. Radloff LS. The CES-D scale: a self report depression scale for research in the general population. Appl Psychol Meas. 1977;1(3):385–401. doi:10.1177/014662167700100306
12. Webste K, Cella D, Yost K. The functional assessment of chronic illness therapy (FACIT) measurement system: properties, applications and interpretation. Health Qual Life Outcomes. 2003;1(79):1–7. doi:10.1186/1477-7525-1-1
13. American Thoracic Society. Available from: http://www.thoracic.org.
14. Graham BL, Steenbruggen I, Milleri MR, et al. Standardization of Spirometry 2019 Update. An Official American Thoracic Society and European Respiratory Society Technical Statement. Am J Respir Crit Care Med. 2019;200(8):e70–e88. doi:10.1164/rccm.201908-1590ST
15. Clinical and Laboratory Standards Institute. GP41 Collection of Diagnostic Venous Blood Specimens.
16. Global Initiative for Chronic Obstructive Lung Disease. 2026 GOLD Report; 2026.
17. Quanjer PH, Stanojevic S, Cole TJ, et al; ERS Global Lung Function Initiative. Multi-ethinic reference values for spirometry for the 3–95 yr ago range: the global lung function 2012 equations. Eur Respir J. 2012;40(6):1324–1343. doi:10.1183/09031936.00080312
18. Bock K, Bendstrup E, Hilberg O, Lokke A. Screening tools for evaluation of depression in Chronic Obstructive Pulmonary Disease (COPD). A systematic review. Eur Clin Respir J. 2017;4(1):1332931. doi:10.1080/20018525.2017.1332931
19. Ebadi Z, Goertz YMJ, Van Herck M, et al. The prevalence and related factors of fatigue in patients with COPD: a systematic review. Eur Respir Rev. 2021;30(160):200298. doi:10.1183/16000617.0298-2020
20. Gan WQ, Man SF, Senthilselvan A, Sin DD. Association between chronic obstructive pulmonary disease and systemic inflammation: a systematic review and a meta-analysis. Thorax. 2004;59(7):574–580. doi:10.1136/thx.2003.019588
21. Karadag F, Kirdar S, Karul AB, Ceylan E. The value of C-reactive protein as a marker of systemic inflammation in stable chronic obstructive pulmonary disease. Eur J Intern Med. 2008;19(2):104–108. doi:10.1016/j.ejim.2007.04.026
22. Aksu F, Capan N, Aksu K, et al. C-reactive protein levels are raised in stable Chronic obstructive pulmonary disease patients independent of smoking behaviour and biomass exposure. J Thoracic Dis. 2013;5(4):414–421.
23. Leuzzi G, Galeone C, Taverna F, Suatoni P, Morelli D, Pastorino U. C-reactive protein level predicts mortality in COPD: a systematic review and meta-analysis. Eur Respir Rev. 2017;26(143):160070. doi:10.1183/16000617.0070-2016
24. Chandratre S, Trivedi B, Somani AO. Quantifying C-reactive protein in clinically stable chronic obstructive pulmonary disease patients. EJCM. 2025;15(4):266–269.
25. Luan YY, Yao YM. The clinical significance and potential role of C-reactive protein in chronic inflammatory and neurodegenerative diseases. Front Immul. 2018;9:1302. doi:10.3389/fimmu.2018.01302
26. Sun M, Qian Y, Cai C, et al. The role and clinical significance of vitamin D in chronic obstructive pulmonary disease. Int J Chron Obstruct Pulm Dis. 2025;20:2023–2033. doi:10.2147/COPD.S520795
27. Janssens W, Lehouck A, Decramer M, Gayan-Ramirez G. Vitamin D and chronic obsructive pulmonary disease. Vitamin D Lung. 2012;3:239–260.
28. Department of Information - Government of Malta. The Maltese Islands. Department of Information – Malta; 2009. Available from: http://www.doi.gov.mt/en/islands/location.asp.
29. Zhu M, Wang T, Wang C, Ji Y. The association between vitamin D and COPD risk, severity, and exacerbation: an updated systematic review and meta-analysis. Int J Chron Obstruct Pulm Dis. 2016;11:2597–2607. doi:10.2147/COPD.S101382
30. Xuan L, Han F, Gong L, et al. Association between chronic obstructive pulmonary disease and serum lipid levels: a meta-analysis. Lipids Health Dis. 2018;17(1):263. doi:10.1186/s12944-018-0904-4
31. Chen J, Chen A, Yang S, et al. Association of triglyceride glucose and obesity indices with chronic obstructive pulmonary disease in US adults: data from 2013 to 2018 NHANES. BMC Pulm Med. 2025;25(1):268. doi:10.1186/s12890-025-03738-2
32. Xu J, Zeng Q, Li S, Su Q, Fan H. Inflammation mechanisms and research progress of COPD. Front Immunol. 2024;15:1404615. doi:10.3389/fimmu.2024.1404615
33. Rafie S, Moitra S, Brashier BB. Association between the serum metabolic profile and lung function on chronic obstructive pulmonary disease. Turk Thorac J. 2018;19(1):13–18. doi:10.5152/TurkThoracJ.2017.17043
34. Lei YF, Lin HC, Lin HL, Uang YS, Cheng HW, Wang LH. Association between use of antihyperlipidemic agents and chronic obstructive pulmonary disease in patients with hyperlipademia: a population-based retrospective cohort study. Int J Chron Obstruct Pulm Dis. 2020;15:2573–2581. doi:10.2147/COPD.S267017
35. Feng WY, Zheng JH, Xiao JQ, et al. Risk of remnant cholesterol and chronic obstructive pulmonary disease: a mendelian randomization study. J Thorac Dis. 2025;17(7):5122–5132. doi:10.21037/jtd-24-1894
36. Bernelot Moens SJ, Verweij SL, Schnitzler KG, et al. Remnant cholesterol elicits arterial wall inflammation and a multilevel cellular immune response in humans. Arterioscler Thromb Vasc Biol. 2017;37(5):969–975. doi:10.1161/ATVBAHA.116.308834
37. Lin JS, Webber EM, Thomas RG. Screening for Chronic Obstructive Pulmonary Disease: A Targeted Evidence Update for the US Preventive Services Task Force. Rockville (MD): Agency for Healthcare Research and Quality (US); 2022.
38. Shengyu W, Xiuzhen S, Te-Chun H, Xiaboo L, Manziang L. The effects of body mass index on spirometry tests among adults in Xi’an China. Medicine. 2017;96(15):e6596. doi:10.1097/MD.0000000000006596
39. Gauci J, Gauci Pullicino S, Caruana E, et al. Chronic obstructive pulmonary disease and metabolic syndrome: a maltese study on biomarkers and clinical implications. Diabetes Metab Syndr Obes. 2025;18:2463–2476. doi:10.2147/DMSO.S515061
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Pyroptosis-Related Genes as Diagnostic Markers in Chronic Obstructive Pulmonary Disease and Its Correlation with Immune Infiltration
Shu HM, Lin CQ, He B, Wang W, Wang L, Wu T, He HJ, Wang HJ, Zhou HP, Ding GZ
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:1491-1513
Published Date: 27 June 2024
Identification of Oxidative Stress-Associated Biomarkers in Chronic Obstructive Pulmonary Disease: An Integrated Bioinformatics Analysis
Jiang X, Wang M, Li H, Liu Y, Dong X
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:841-855
Published Date: 26 March 2025
Integrating Bioinformatics Analysis with RT-qPCR Experimental Validation to Investigate Immune Cell and Telomere-Related Biomarkers in Chronic Obstructive Pulmonary Disease
Wang S, Tang W, Yang H
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:3839-3854
Published Date: 28 November 2025
Identification of Th17 Cell-Associated Biomarkers and Their Potential Regulatory Mechanisms in Chronic Obstructive Pulmonary Disease Through Integrated Bioinformatics Analysis and Machine Learning
Li Q, Xue D, Yu J, Yang M, Zhang Y, Obuli R
International Journal of Chronic Obstructive Pulmonary Disease 2026, 21:596649
Published Date: 11 June 2026