Back to Journals » Neuropsychiatric Disease and Treatment » Volume 19
A Linear Regression Equation for Predicting the Residual Volume of Chronic Subdural Hematoma 1 Week After Surgery
Authors Yan C, Su C, Ye YF, Liu J
Received 19 September 2023
Accepted for publication 7 December 2023
Published 14 December 2023 Volume 2023:19 Pages 2787—2796
DOI https://doi.org/10.2147/NDT.S436127
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Richard J Porter
Chao Yan,1,* Chang Su,1,* Yu-fei Ye,2 Jin Liu1
1Department of Neurosurgery, the Sixth Affiliated Hospital of Wenzhou Medical University, Lishui, Zhejiang, 323000, People’s Republic of China; 2Department of Neurosurgery, Qingyuan People’s Hospital, Lishui, Zhejiang, 323800, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jin Liu, Department of Neurosurgery, the Sixth Affiliated Hospital of Wenzhou Medical University, 1188 Liyang Street, Liandu District, Lishui, Zhejiang Province, 323000, People’s Republic of China, Email [email protected]
Objective: The outcome of chronic subdural hematoma (CSDH) is influenced not only by the choice of treatment but also by various baseline characteristics. The main objective of this study is to identify the risk factors that can affect the prognosis of CSDH and develop a regression equation based on these risk factors.
Methods: A total of 212 patients with CSDH were included in the study. We collected clinical data including age, gender, and so on, and radiological data including preoperative hematoma volume (V1), effusion volume 1 day after surgery (V2), gas volume 1 day after surgery (V3), and so on. These were considered independent variables, while residual volume 1 week after surgery (V4) was the dependent variable. Univariate linear regression analysis was performed to identify factors that were significantly related. Subsequently, multivariate linear regression analysis was conducted to determine the relationship between each independent variable and the dependent variable. Multiple linear regression analysis was used to obtain a regression equation predicting V4.
Results: We have found that age (t = 3.109, P = 0.002), aspirin (t = 2.762, P = 0.006), hemostatic agents (haemocoagulase, t = 3.731, P < 0.001; vitamin K, t = 2.824, P = 0.005 < 0.05), V2 (t = 8.73, P < 0.001), and V3 (t = 5.968, P < 0.001) are significantly associated with V4. Furthermore, we have developed a regression equation that can predict this volume with CSDH. The fit of the model is robust with an R-squared value of 65.2% > 50%.
Conclusion: Age, aspirin, hemostatic agent, V2, and V3 are significantly associated with V4. We developed a regression equation to predict this volume with CSDH.
Keywords: CSDH, burr-hole and drainage, regression equation
Introduction
Chronic subdural hematoma (CSDH) is a prevalent neurosurgical condition. With the increase in the life expectancy of the population, the incidence of CSDH has also increased.1 The outcome of CSDH depends not only on the choice of treatment but also on baseline characteristics such as age, sex, comorbidities, severity of symptoms, medication use, and severity of baseline imaging abnormalities.2 Several randomized controlled trials are currently investigating the impact of various perioperative characteristics on outcomes.3 Many models have been established to predict the outcome of CSDH.4–7 These models attempted to predict outcome measures of CSDH such as mortality, risk of recurrence, and functional outcome after surgical treatment.2 Population differences and differences in the distribution of predictors between development and validation studies may affect model performance in the validation setting.2
The factors that affect prognosis may vary greatly at different follow-up times. Due to drain removal, a repeat head computed tomography (CT) 1 week after the burr hole and drainage tended to show an increased residual cavity volume. Furthermore, there were cases of patients who required a second surgery 1 week after the initial surgery due to an increase in symptoms. In various studies, the definition of recurrence varies and not all patients with recurrence necessarily require surgery again. This study specified the prognostic study timing was 1 week after surgery and used residual cavity volume as prognostic index. Investigating the correlation between each clinical characteristic and residual cavity volume 1 week after surgery, this study identified risk factors that affect the prognosis of CSDH and developed a regression equation based on these factors.
Materials and Methods
Clinical Data
A total of 212 patients with CSDH underwent burr hole and drainage from December 2010 to February 2022 at the Sixth Affiliated Hospital of Wenzhou Medical University and Qingyuan People’s Hospital.
Inclusion Criteria
- The patients must have received burr-hole and drainage surgery;
- Age: ≥18 years;
- Patients had not experienced major trauma, surgical treatment, inflammatory disease, or fever within 3 months;
- No lesions in the central nervous system other than CSDH.
Exclusion Criteria
- Patients who underwent craniotomy;
- Patients with bilateral chronic subdural hematoma and drainage of only one hematoma;
- Patients with ventriculo peritoneal (VP) shunts in situ;
- Patients with a history of stroke;
- Patients with hydrocephalus;
- Patients with calcified or ossified CSDH.8–10
The following data were collected: age, sex, duration of the study symptoms, history of trauma, diabetes mellitus, hypertension, antithrombotic agents, operative time, hemostatic agents, white blood cell count, lymphocyte count, monocyte count, granulocyte count, lymphocyte ratio, monocyte ratio, granulocyte ratio, red blood cell distribution width (RDW), platelets, neutrophil lymphocyte (NLR), platelet lymphocyte count ratio (PLR).
Treatment Methods
All patients underwent burr hole and drainage surgery in general anesthesia. Intraoperatively, we drill one hole for each hematoma and flush through this hole using warm saline, and the drainage tubes were left in place under the dura mater. In this study, patients with bilateral hematoma underwent bilateral drilling surgery. Drainage tubes were removed 48 hr after the surgery.
Antithrombotic drugs are usually discontinued 5 days before surgery and are re-used after the risk of postoperative bleeding is reduced (usually 48 hr after surgery).
Hemostatic drugs are usually applied within 24 hr after surgery. In this study, the following drugs can be selected: hemocoagulase (2U iv bid), vitamin K (10mg im bid), carbazochrome sodium sulfonate (80mg ivgtt bid), tranexamic acid (0.4g ivgtt bid), and medication chosen were decided by the attending physician.
Radiological Data
We used PSCS system to collect CT image data, including hematoma side, hole diameter, and difference in midline shift (MLS) before and 1 day after surgery. The type of preoperative hematoma was divided into 7 types as Nakaguchi et al11 proposed (Figure 1):
 |
Figure 1 Nagakuchi’s classification of CSDH: hypodensity type (A) isodensity type (B) hyperdensity type (C) laminar type (D) separated type (E) grading type (F) trabecular type (G). |
Hypodensity type (A): The density of this type of hematoma is lower than that of the surrounding white matter of the brain;
Isodensity type (B): The density of this type of hematoma is equal to the surrounding white matter of the brain;
Hyperdensity type (C): The density of this type of hematoma is higher than that of the surrounding white matter of the brain;
Laminar type (D): This type of hematoma has a high-density layered structure distributed along the inner membrane of the hematoma;
Separated type (E): This type of hematoma is composed of two parts with different densities, and there is a clear boundary between the two parts;
Grading type (F): This type is between the separated type and the uniform density type, and is a subtype of stratified hematoma, but there is no clear boundary between high and low density;
Trabecular type (G): This type of hematoma is a hypodensity type or Isodensity type hematoma with high-density fibrous trabecular structures located between the inner and outer membranes, separating the hematoma cavity.
We used computer-assisted volumetric analysis (CAVA) with 3D-Slicer software (Version 4.9) to calculate preoperative hematoma volume (V1), hole diameter, effusion volume 1 day after surgery (V2), gas volume 1 day after surgery (V3), and residual volume 1 week 1 day after surgery (V4).
Statistical Analysis
The study used SPSS 22.0 software (SPSS Inc., Chicago, IL, USA) to analyze correlation factors of V4. Age, sex, days from onset (the occurrence of symptoms), trauma history, diabetes mellitus history, hypertension history, anticoagulant use history, surgical time, hemostatic agents, white blood cell count, lymphocyte count, monocyte count, granulocyte ratio, monocyte ratio, granulocyte ratio, RDW, platelet, NLR, PLR, preoperative hematoma type, hole diameter, difference in midline shift (MLS) before and 1 day after surgery, V1, V2, and V3, these were considered independent variables, while V4 was the dependent variable. Univariate linear regression analysis was performed, and those factors, which were significantly related to V4 were selected, and multivariate linear regression analysis was conducted to clarify each variable’s relationship with the dependent variable.
Multiple linear regression analysis was employed to obtain a regression equation predicting V4. Statistical significance was determined as P < 0.05.
Result
A total of 212 patients were included in the study. The patients had an average age of 68.71(±13.01) years, with 174 males and 38 females. In this study, we define recurrence as a combination of radiological recurrence and recurrence of symptoms. Fifteen patients (15/212, 7.07%) experienced postoperative recurrence, six patients (6/212, 2.8%) experienced recurrence 1 week after surgery and underwent reoperation, five patients (5/212, 2.4%) experienced recurrence between 1 week and 1 month after surgery, and four patients (4/212, 1.9%) experienced recurrence between 1 month and 3 months after surgery.
Univariate Linear Regression Analysis
Based on univariate linear regression analysis, we have determined that several factors including age, diabetes mellitus, use of clopidogrel, aspirin, hemostatic agent, lymphocytes, monocytes, side and type of hematoma, as well as V1, V2, and V3, were significantly associated with V4. Specifically, increased age, use of clopidogrel and aspirin, and low lymphocytes and monocytes were significantly associated with higher V4. Furthermore, the use of hemostatic agents (hemagglutinase or sodium carbamazepine), a single left or right side of the hematoma, and a type G hematoma were other significant predictors of higher V4. Those with higher V1 and V2 were at increased risk of higher V4 (Table 1). These risk factors were included in multivariate linear regression analysis.
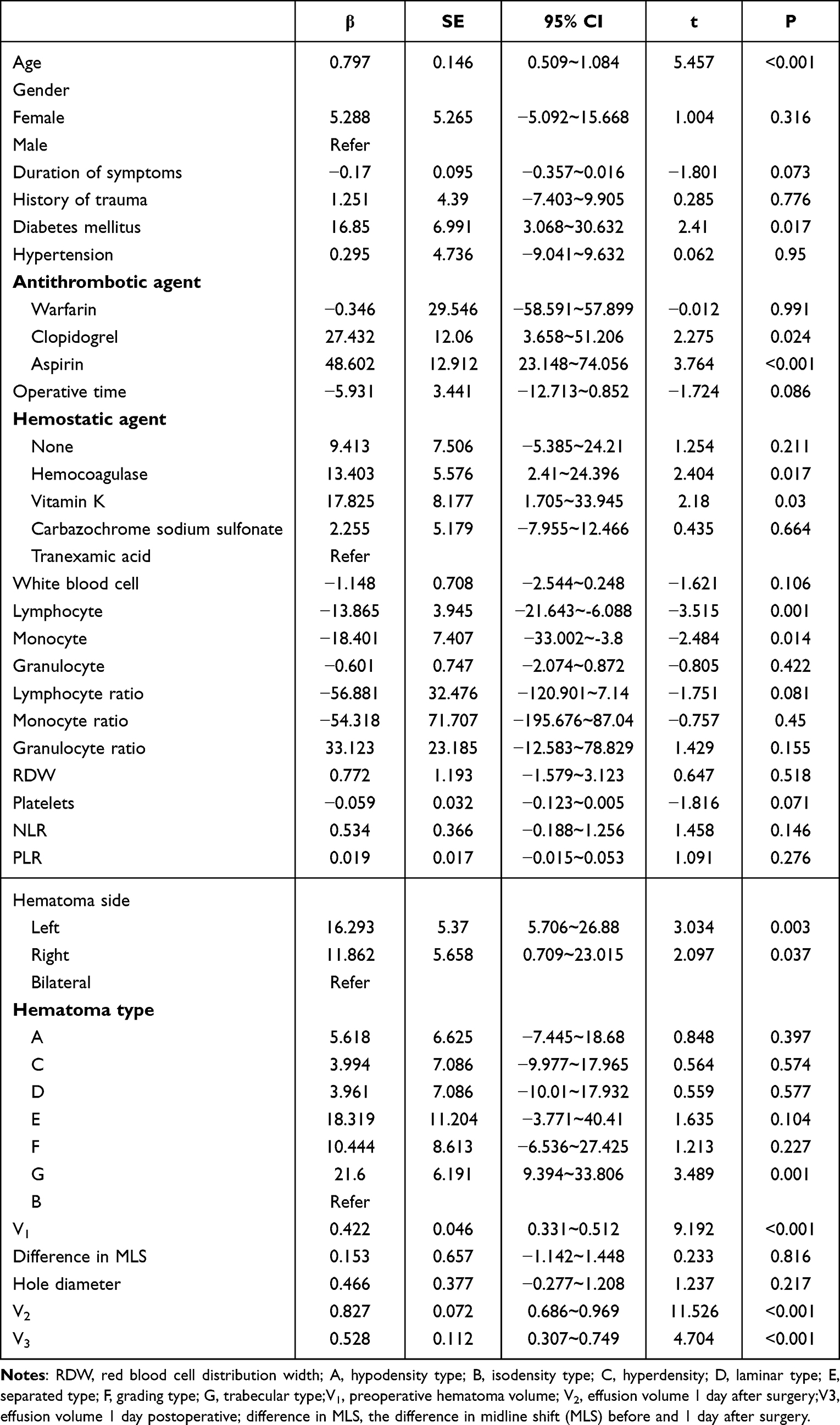 |
Table 1 Univariate Linear Regression Analysis |
Multivariate Linear Regression Analysis
After a multivariate linear regression analysis, we found that age, aspirin, hemostatic agent, V2, and V3 were significantly associated with V4.
Age was found to have a significant impact on the residual cavity 1 week post-surgery (t-value = 3.109, P = 0.002). Furthermore, the coefficient of age in the residual cavity was recorded as 0.375, indicating a positive correlation, which implies that an increase in age results in a higher V4.
The study found that aspirin has a notable impact on V4 (t = 2.762, P = 0.006). Additionally, the coefficient of the effect of aspirin on V4 was 28.876 > 0, indicating that the residual cavity was significantly larger in patients who took aspirin, compared to those who did not.
The use of hemostatic agent has a significant impact on V4. In comparison to tranexamic acid, the use of haemocoagulase (t = 3.731, P < 0.001) and vitamin K (t = 2.824, P = 0.005) show a higher coefficient of effect, with β values of 14.731 > 0 and 15.388 > 0, respectively. This implies that patients using haemocoagulase and vitamin K have a higher V4 than those using tranexamic acid.
Effect of V2 on V4 at a significance level (t = 8.73, P < 0.001). This study shows that the coefficient of effect of V2 on V4 was 0.662 > 0. This indicates a significant positive effect of V2 on V4. In other words, the larger V2, the larger V4.
Effects of V3 on V4 at a significance level (t = 5.968, P < 0.001). The coefficient of effect of V3 onV4 was 0.559, indicating that a larger V3 associated with a larger V4.
The remaining factors did not have a significant impact on V4, as indicated by a P-value > 0.05.
Regression Equations for Predicting Residual Volume One Week One Day After Surgery
Through multiple linear regression analysis, we have obtained the following optimal regression equations for predicting the residual volume 1 week 1 day after surgery:
Residual volume 1 week 1 day after surgery (V4) = 0.375 × Age +28.876 × Aspirin* + 9.196 × Absence of hemostatic agents* + 14.731 × Hemocoagulase* + 15.388 × vitamin K* + 0.154 × Kaempferol sodium* + 0.662 × V2 + 0.559 × V3* - 31.117.
*aspirin and hemostatic agent are classified as having=1 and not having=0.
All factors with a significance level of P < 0.05 indicate that the regression equation is significant, as shown in Table 2.
 |
Table 2 Univariate Linear Regression Analysis |
After conducting a multivariate linear regression analysis (Table 2), it can be concluded that the fit of the equation is good as the fit R-square has reached 65.2% > 50%. This indicates that the multiple linear regression model utilized in this study accurately reflects the influence of independent variables on the dependent variable. Additionally, the regression equation was found to be significant (F = 15.31, P < 0.05), suggesting that at least one of the independent variables considered in the study has a significant impact on V4.
Discussion
The primary risk factor for CSDH is an underlying traumatic brain injury.12 A systematic review and meta-analysis focusing on radiological prognostic factor CSDH found a recurrence rate of 14.4%.1 Various factors have been implicated in recurrence after hematoma evacuation, including diabetes, liver dysfunction, hemodialysis, and antiplatelet agents.13,14 High recurrence rates are associated with lower quality of life and increased reoperation for CSDH.15 It is important to consider all of these potential contributors to the pathogenesis of CSDH.12
The course of CSDH can last for 3 weeks or more, and its symptoms are typically mild.16 This suggests that both resorptive and collection process involved in hematoma formation.16 As blood products accumulate at a faster rate than they can be resorbed physiologically, the hematoma gradually enlarges.17 Whereas within a week postoperatively, the increase in effusion was, generally, the most rapid due to drain removal. In some cases, patients may require a second surgery within a week after the initial surgery, which is defined as recurrence. It is important to distinguish risk factors for recurrence at this time from those evident during long-term follow-up. Consequently, this study used the residual cavity volume 1 week after surgery as a baseline prognostic indicator for predicting the surgical efficacy of CSDH.
An increasing number of studies have demonstrated the significant role of local inflammatory response in the formation and development of CSDH. On adventitia, various inflammatory cells, including neutrophils, lymphocytes, monocytes, and eosinophils were observed. High concentrations of inflammatory and proangiogenic cytokines were found in the hematoma compared with the serum of patients with CSDH, which were associated with recurrence, suggesting the presence of local inflammation in the hematoma.18,19 In the study of Fan et al, all inflammatory indices on routine examination of peripheral blood in patients with CSDH were found to be within the normal range.16 However, white blood cell count, neutrophil count, and percentage of neutrophils were higher in CSDH patients than in controls.16 This finding implies that CSDH causes a mild systemic inflammatory response in peripheral blood.16 In this study, low lymphocytes and low monocytes were positively correlated with V4.
The neutrophil count ratio and PLR are crucial markers of inflammatory responses. Many inflammatory responses and immune diseases incorporate these two markers into their diagnostic criteria.20–23 Mohammad et al24 investigated the predictive value of NLR for early postoperative adverse outcomes in elderly patients with hip fractures and proposed that NLR, along with other risk factors, can be considered a risk factor for hospitalization for postoperative complications. Previous studies have been conducted by research institutes on acute intracerebral hematoma and NLR, proposing that high NLR predicts worse outcome within 3 months.25 Zhang et al26 compared CSDH patients with a healthy control group and found that the former had a higher neutrophil count and higher NLR. This may be the first study to demonstrate changes in the levels of inflammatory markers in the peripheral blood of CSDH patients compared to healthy individuals. Adilson et al27 found that postoperative neutrophil count and NLR were higher in patients with recurrence, and the postoperative NLR ratio was independently associated with recurrence. Adilson et al27 suggested that inflammatory response may be a part of the recurrence mechanism. Like other inflammatory diseases, inflammatory cells are initially part of the healing process, but exacerbation and/or perpetuation turn it into a pathologic process, turning it into pathological processes.27
The study by Fan et al found that CSDH only caused a mild inflammatory response, suggesting that not all components of the hematoma flowed into the peripheral blood.16 In the study of an acute subdural hemorrhage (SDH) model, Fan et al demonstrated that hematomas in the subdural space drain extracranially through the meningeal and cervical lymphatics.28 This suggests that patients with CSDH also have their hematomas absorbed through the meningeal and cervical lymphatics.28 This absorption process may be the reason why CSDH does not produce a strong systemic inflammatory response in peripheral blood.28
In addition to peripheral blood, validation indicators in hematoma fluid also have significant research significance. In Teodor et al’s study,29 GDNF, NT-3, and IL-8 showed significant differences in different classifications, with higher values in the trabecular type.29 In addition, patients with mediastinum in the CSDH lesion area had higher levels of GDNF, MCP-3, NT-3, CXCL1, CXCL5, IL8, and OSM.29 There is no correlation between Markwalder grading and inflammatory biomarkers.29
A systematic review and meta-analysis conducted by Huang et al revealed that burr hole craniostomy (BHC) had higher efficacy compared to minicraniotomy (MC) in reducing the rate of recurrence, the rate of reoperation, and the duration of surgery.12 The duration of surgery was significantly shorter in the BHC group compared with the MC group.30,31 However, in this study, operative time was not significantly associated with the prognosis of CSDH.
Overactivation of the coagulation and fibrinolytic systems in CSDH and high expression of tissue-type fibrinogen activator in the hematoma are considered possible causes of an inability to coagulate.32 Additionally, contribution of comorbidities (hypertension and diabetes) to the recurrence of CSDH is similar to the use of anticoagulants and antiplatelet agents.33,34 Patients with hypertension and diabetes commonly take these medications to prevent or treat cardio-cerebrovascular events.33,34 However, findings of previous retrospective studies have been inconsistent.33,34 Tranexamic acid, an antifibrinolytic medication that inhibits tissue plasminogen activator and plasmin, has been shown to counterbalance fibrin breakdown and reduce kallikrein-induced inflammation within the CSDH area.35,36 In this study, we observed that V4 was significantly larger in patients using hemocoagulase and vitamin K compared to those using tranexamic acid.
In the literature, multiple retrospective studies have suggested an association between postoperative subdural air and recurrence.37–39 Univariate analysis has identified a volume of subdural air greater than 10 mL,37 the presence of subdural air on the seventh postoperative day,38 and a percentage of subdural air occupying the lungs subdural space39 as risk factors for recurrence. Therefore, Kuroki et al40 proposed the implementation of a strict closed-system drainage to prevent subdural air and, subsequently, recurrence of CSDH. Furthermore, Nakaguchi et al39 reported that significant postoperative accumulation of subdural air is a major contributor to the CSDH intimal pressure differential. The mechanism responsible for this pressure imbalance is thought to be high pressure in the haematoma cavity after surgery, while low pressure in the subarachnoid space.39 In this study, both pneumatosis and effusion on the postoperative day affect the residual cavity 1 week after surgery, which is consistent with the results of previous studies.
Currently, there exist a large number of predictive models for CSDH. In an effort to evaluate the efficacy of published prognostic models for predicting patient outcome with unilateral CSDH, Holl et al conducted a retrospective analysis of a database from three regions in the Netherlands.2,4–6 However, none of the models demonstrated significant discriminative ability or calibration.4–6 In particular, Alford and Jack’s model dichotomized continuous predictors, which can lead to information loss and limited information applicability to future studies.2,4–6 To avoid such shortcomings, this study opted to utilize linear regression analysis to establish the relationship between continuous and inverse variables and weeks of residual cavity after surgery, without grouping them together.
Holl et al have suggested that the size of a CSDH does not necessarily correlate with a greater midline shift or more severe clinical symptoms.2 Additionally, smaller CSDHs do not always recover quickly without recurrence.2 The use of anticoagulants is also not necessarily associated with a larger volume of CSDH nor are more severe symptoms at admission indicative of worse functional outcomes.2 This heterogeneity of the data for patients with CSDH makes accurate prediction challenging.2 Previous studies have had varying follow-up times, resulting in differing prognostic indicators. In this study, the follow-up time was set at 1 week after surgery. In future studies, we will further subdivide the follow-up time to investigate factors influencing recurrence during different periods and identify the most appropriate prognostic indicators.
Conclusion
Age, aspirin, hemostatic agents, V2, and V3 are significantly associated with V4. We established a regression equation that can predict this volume with CSDH. The model fit is robust with an R-squared value of 65.2% > 50%. We expect that in future studies more sample sizes can be included and further subgrouping of studies will be performed according to follow-up time. Most importantly, at least we cannot conflate the prognosis in a week with the prognosis in three months. We also anticipate that this study will provide innovative insights for future researchers.
Ethics Statement
This study has been approved by the Ethics Committee of the Sixth Affiliated Hospital of Wenzhou Medical University and has obtained informed consent from all study participants, following the guidelines outlined in the Helsinki Declaration.
Funding
This work was supported by grants funded by the Medical and Health Research Project of Zhejiang province [Grant No. 2023XY260], the City-level public welfare technology application research project of Lishui [Grant No. 2021SJZC086], and the City-level public welfare technology application research project of Lishui [Grant No. 2021SJZC080].
Disclosure
The authors declared that they have no conflicts of interest to this work.
References
1. Miah IP, Tank Y, Rosendaal FR, et al. Radiological prognostic factors of chronic subdural hematoma recurrence: a systematic review and meta-analysis. Neuroradiology. 2021;63(1):27–40. doi:10.1007/s00234-020-02558-x
2. Holl DC, Mikolic A, Blaauw J, et al. External validation of prognostic models predicting outcome after chronic subdural hematoma. Acta Neurochir. 2022;164(10):2719–2730. doi:10.1007/s00701-022-05216-8
3. Edlmann E, Holl DC, Lingsma HF, et al. Systematic review of current randomised control trials in chronic subdural haematoma and proposal for an international collaborative approach. Acta Neurochir. 2020;162(4):763–776. doi:10.1007/s00701-020-04218-8
4. Jack A, O’Kelly C, McDougall C, et al. Predicting recurrence after chronic subdural haematoma drainage. Can J Neurol Sci. 2015;42(1):34–39. doi:10.1017/cjn.2014.122
5. Andersen-Ranberg NC, Debrabant B, Poulsen FR, et al. The Danish chronic subdural hematoma study-predicting recurrence of chronic subdural hematoma. Acta Neurochir. 2019;161(5):885–894. doi:10.1007/s00701-019-03858-9
6. Alford EN, Rotman LE, Erwood MS, et al. Development of the Subdural Hematoma in the Elderly (SHE) score to predict mortality. J Neurosurg. 2019;132(5):1616–1622. doi:10.3171/2019.1.Jns182895
7. Yan C, Yang MF, Huang YW. A Reliable Nomogram Model to Predict the Recurrence of Chronic Subdural Hematoma After Burr Hole Surgery. World Neurosurg. 2018;118:e356–e66. doi:10.1016/j.wneu.2018.06.191
8. Turgut M, Akhaddar A, Hall W, et al. Subdural Hematoma. Past to Present to Future Management. 2021.
9. Turgut M, Akhaddar A, Turgut AT. Calcified or Ossified Chronic Subdural Hematoma: a Systematic Review of 114 Cases Reported During Last Century with a Demonstrative Case Report. World Neurosurg. 2020;134:240–263. doi:10.1016/j.wneu.2019.10.153
10. Turgut M, Yay M. A Rare Case of Ossified Chronic Subdural Hematoma Complicated with Tension Pneumocephalus. J Neurol Surg Rep. 2019;80(4):e44–e45. doi:10.1055/s-0039-1694738
11. Nakaguchi H, Tanishima T, Yoshimasu N. Factors in the natural history of chronic subdural hematomas that influence their postoperative recurrence. J Neurosurg. 2001;95(2):256–262. doi:10.3171/jns.2001.95.2.0256
12. Huang YW, Yin XS, Li ZP. Burr hole craniostomy vs. minicraniotomy of chronic subdural hematoma: a systematic review and meta-analysis. Eur Rev Med Pharmacol Sci. 2022;26(14):4983–4990. doi:10.26355/eurrev_202207_29284
13. Han MH, Ryu JI, Kim CH, et al. Predictive factors for recurrence and clinical outcomes in patients with chronic subdural hematoma. J Neurosurg. 2017;127(5):1117–1125. doi:10.3171/2016.8.Jns16867
14. Kim JH, Kang DS, Kim JH, et al. Chronic subdural hematoma treated by small or large craniotomy with membranectomy as the initial treatment. J Korean Neurosurg Soc. 2011;50(2):103–108. doi:10.3340/jkns.2011.50.2.103
15. Forster MT, Mathé AK, Senft C, et al. The influence of preoperative anticoagulation on outcome and quality of life after surgical treatment of chronic subdural hematoma. J Clin Neurosci. 2010;17(8):975–979. doi:10.1016/j.jocn.2009.11.023
16. Fan Y, Wu D, Zhang X, et al. The inflammatory cellular feature in the peripheral blood of chronic subdural hematoma patients. J Clin Lab Anal. 2022;36(10):e24706. doi:10.1002/jcla.24706
17. Fiorella D, Arthur AS. Middle meningeal artery embolization for the management of chronic subdural hematoma. J Neurointerv Surg. 2019;11(9):912–915. doi:10.1136/neurintsurg-2019-014730
18. Hua C, Zhao G, Feng Y, et al. Role of Matrix Metalloproteinase-2, Matrix Metalloproteinase-9, and Vascular Endothelial Growth Factor in the Development of Chronic Subdural Hematoma. J Neurotrauma. 2016;33(1):65–70. doi:10.1089/neu.2014.3724
19. Stanisic M, Aasen AO, Pripp AH, et al. Local and systemic pro-inflammatory and anti-inflammatory cytokine patterns in patients with chronic subdural hematoma: a prospective study. Inflamm Res. 2012;61(8):845–852. doi:10.1007/s00011-012-0476-0
20. Ahsen A, Ulu MS, Yuksel S, et al. As a new inflammatory marker for familial Mediterranean fever: neutrophil-to-lymphocyte ratio. Inflammation. 2013;36(6):1357–1362. doi:10.1007/s10753-013-9675-2
21. Feng JF, Huang Y, Chen QX. Preoperative platelet lymphocyte ratio (PLR) is superior to neutrophil lymphocyte ratio (NLR) as a predictive factor in patients with esophageal squamous cell carcinoma. World J Surg Oncol. 2014;12:58. doi:10.1186/1477-7819-12-58
22. Hu ZD, Sun Y, Guo J, et al. Red blood cell distribution width and neutrophil/lymphocyte ratio are positively correlated with disease activity in primary Sjögren’s syndrome. Clin Biochem. 2014;47(18):287–290. doi:10.1016/j.clinbiochem.2014.08.022
23. Tamhane UU, Aneja S, Montgomery D, et al. Association between admission neutrophil to lymphocyte ratio and outcomes in patients with acute coronary syndrome. Am J Cardiol. 2008;102(6):653–657. doi:10.1016/j.amjcard.2008.05.006
24. Golsorkhtabaramiri M, McKenzie J, Potter J. Predictability of Neutrophil to Lymphocyte Ratio in preoperative elderly Hip fracture patients for post-operative short-term complications: a retrospective study. BMC Musculoskelet Disord. 2023;24(1):227. doi:10.1186/s12891-023-06211-5
25. Lattanzi S, Cagnetti C, Provinciali L, et al. Neutrophil-to-Lymphocyte Ratio Predicts the Outcome of Acute Intracerebral Hemorrhage. Stroke. 2016;47(6):1654–1657. doi:10.1161/strokeaha.116.013627
26. Zhang Y, Yang Y, Long S, et al. Assessment of peripheral blood cell inflammatory markers in patients with chronic subdural hematoma. Clin Neurol Neurosurg. 2020;191:105738. doi:10.1016/j.clineuro.2020.105738
27. de Oliveira AJM, Solla DJF, de Oliveira KF, et al. Postoperative neutrophil-to-lymphocyte ratio variation is associated with chronic subdural hematoma recurrence. Neurol Sci. 2022;43(1):427–434. doi:10.1007/s10072-021-05241-y
28. Liu X, Gao C, Yuan J, et al. Subdural haematomas drain into the extracranial lymphatic system through the meningeal lymphatic vessels. Acta Neuropathol Commun. 2020;8(1):16. doi:10.1186/s40478-020-0888-y
29. Svedung Wettervik T, Sundblom J, Ronne-Engström E. Inflammatory biomarkers differentiate the stage of maturation in chronic subdural hematomas. J Neuroimmunol. 2023;381:578127. doi:10.1016/j.jneuroim.2023.578127
30. Lee JK, Choi JH, Kim CH, et al. Chronic subdural hematomas: a comparative study of three types of operative procedures. J Korean Neurosurg Soc. 2009;46(3):210–214. doi:10.3340/jkns.2009.46.3.210
31. Duerinck J, Van Der Veken J, Schuind S, et al. Randomized Trial Comparing Burr Hole Craniostomy, Minicraniotomy, and Twist Drill Craniostomy for Treatment of Chronic Subdural Hematoma. Neurosurgery. 2022;91(2):304–311. doi:10.1227/neu.0000000000001997
32. Edlmann E, Giorgi-Coll S, Whitfield PC, et al. Pathophysiology of chronic subdural haematoma: inflammation, angiogenesis and implications for pharmacotherapy. J Neuroinflammation. 2017;14(1):108. doi:10.1186/s12974-017-0881-y
33. Torihashi K, Sadamasa N, Yoshida K, et al. Independent predictors for recurrence of chronic subdural hematoma: a review of 343 consecutive surgical cases. Neurosurgery. 2008;63(6):1125–1129. doi:10.1227/01.Neu.0000335782.60059.17
34. Tugcu B, Tanriverdi O, Baydin S, et al. Can recurrence of chronic subdural hematoma be predicted? A retrospective analysis of 292 cases. J Neurol Surg a Cent Eur Neurosurg. 2014;75(1):37–41. doi:10.1055/s-0032-1330961
35. Soleman J, Nocera F, Mariani L. The conservative and pharmacological management of chronic subdural haematoma. Swiss Med Wkly. 2017;147:w14398. doi:10.57187/smw.2017.14398
36. Kageyama H, Toyooka T, Tsuzuki N, et al. Nonsurgical treatment of chronic subdural hematoma with tranexamic acid. J Neurosurg. 2013;119(2):332–337. doi:10.3171/2013.3.Jns122162
37. Kanazawa T, Takahashi S, Minami Y, et al. Prediction of postoperative recurrence of chronic subdural hematoma using quantitative volumetric analysis in conjunction with computed tomography texture analysis. J Clin Neurosci. 2020;72:270–276. doi:10.1016/j.jocn.2019.11.019
38. Amirjamshidi A, Abouzari M, Eftekhar B, et al. Outcomes and recurrence rates in chronic subdural haematoma. Br J Neurosurg. 2007;21(3):272–275. doi:10.1080/02688690701272232
39. Nakaguchi H, Tanishima T, Yoshimasu N. Relationship between drainage catheter location and postoperative recurrence of chronic subdural hematoma after burr-hole irrigation and closed-system drainage. J Neurosurg. 2000;93(5):791–795. doi:10.3171/jns.2000.93.5.0791
40. Kuroki T, Katsume M, Harada N, et al. Strict closed-system drainage for treating chronic subdural haematoma. Acta Neurochir. 2001;143(10):1041–1044. doi:10.1007/s007010170010
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.