")
Back to Journals » Nature and Science of Sleep » Volume 12
A Further Introduction to Dental Sleep Medicine
Authors Lobbezoo F , de Vries N, de Lange J, Aarab G
Received 10 August 2020
Accepted for publication 28 September 2020
Published 14 December 2020 Volume 2020:12 Pages 1173—1179
DOI https://doi.org/10.2147/NSS.S276425
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sarah L Appleton
Frank Lobbezoo,1 Nico de Vries,1– 3 Jan de Lange,4 Ghizlane Aarab1
1Department of Orofacial Pain and Dysfunction, Academic Centre for Dentistry Amsterdam (ACTA), University of Amsterdam and Vrije Universiteit Amsterdam, Amsterdam, the Netherlands; 2Department of Otorhinolaryngology, Onze Lieve Vrouwe Gasthuis (OLVG) West, Amsterdam, the Netherlands; 3Department of Pulmonary Medicine and Multidisciplinary Sleep Disorders Centre, Antwerp University Hospital, University of Antwerp, Edegem, Belgium; 4Department of Oral and Maxillofacial Surgery, Amsterdam University Medical Centre and Academic Centre for Dentistry Amsterdam (ACTA), Amsterdam, the Netherlands
Correspondence: Frank Lobbezoo
Department of Orofacial Pain and Dysfunction, Academic Centre for Dentistry Amsterdam (ACTA), Gustav Mahlerlaan 3004, Amsterdam 1081 LA, the Netherlands
Tel +31-20-5980412
Fax +31-20-5980333
Email [email protected]
Abstract: Dental sleep medicine traditionally focuses on sleep-related breathing disorders, such as snoring and obstructive sleep apnea. However, everyday practice shows that also other sleep disorders touch on dentistry, including sleep-related orofacial pain, xerostomia, hypersalivation, gastroesophageal reflux disease and bruxism. A new definition, which covers all the diagnostic and treatment aspects of these disorders, has therefore been formulated for dental sleep medicine. This article describes why this development started and sketches the current state of affairs regarding the discipline of dental sleep medicine. The different dental sleep disorders are also described briefly, with special focus on the more remarkable associations between them.
Keywords: dentistry, sleep medicine, sleep disorders, comorbidities
Introduction
The dental discipline “dental sleep medicine” is highly multidisciplinary and demands a great deal of specialist medical know-how of those who work in it, for example, in the fields of ear, nose and throat specialization, neurology, pulmonary diseases, internal medicine and psychiatry. This challenging area is of particular interest to oral and maxillofacial (OMF) surgeons, orthodontists, oral medicine and oral pathology specialists, orofacial pain specialists and dentists specializing in dental sleep medicine, while medical doctors also need a broader knowledge of dental sleep medicine in the interest of providing the best possible patient care in interdisciplinary settings.1,2
Although the diagnosis and treatment of sleep-related disorders fall under medicine, some sleep disorders touch on dentistry. Especially in countries where individuals visit their dentist on a regular (eg yearly) basis, the dentist may be able, for example, to identify risk factors or consequences of certain sleep disorders in the mouth or masticatory system or to carry out screening with the help of questionnaires and thus contribute to the diagnostic process. The importance of this contribution is illustrated by the fact that more than 80% of individuals with OSA are not diagnosed,3 which has enormous implications for the patient, those in his/her environment and society as a whole. The dentist can also play a role in the treatment of certain sleep disorders, whether or not the patient is referred by a general practitioner or medical specialist. Finally, some sleep disorder treatments have consequences for the mouth and masticatory system. There are, therefore, plenty of reasons for categorizing sleep disorders with dental causes and/or consequences as ‘dental sleep disorders’.
It is this article’s aim to further introduce the emerging discipline of dental sleep medicine to all professionals working in sleep medicine, including medical doctors and dentists specializing in dental sleep medicine.
Dental Sleep Medicine
The discipline of dental sleep medicine entails the diagnosis and treatment of dental sleep disorders. In 2008, the American Academy of Dental Sleep Medicine formulated the following definition for this discipline:52
Dental sleep medicine is an area of dental practice that focuses on the use of oral appliance therapy to treat sleep-disordered breathing, including snoring and obstructive sleep apnea (OSA)
However, since dental sleep medicine involves more than sleep-related breathing disorders, in 2016, the following alternative definition was proposed:4
“Dental Sleep Medicine is the discipline concerned with the study of the oral and maxillofacial causes and consequences of sleep-related problems.”
This definition makes clear that the area focuses on a range of problems in which dentistry can (or must) play a role. But the ultimate credit goes to Lavigne et al5 who, already more than two decades ago, wrote a publication on this discipline entitled “Sleep disorders and the dental patient”. They counted the following as forms of dental sleep disorders: snoring and OSA, orofacial pain in relation to sleep problems, sleep-related xerostomia and hypersalivation, sleep-related gastroesophageal reflux disease (GERD), and sleep-related bruxism. The authors describe the way in which the dentist can identify each complaint and the role he/she can play in its treatment. They also discuss the division of roles between general practitioner/medical specialists. The conclusion of this “landmark” publication is that the role of dentists is highly relevant in the diagnosis and treatment of these sleep disorders. The authors do, however, qualify this by adding that many aspects of these dental sleep disorders are still unknown and that the relationship between them requires investigation in the future.
In 2016, Lobbezoo et al4 elaborated on the publication by Lavigne et al,5 formulating a new definition of dental sleep medicine and giving an update on the most recent insights on the various aspects of dental sleep disorders and their mutual relationships.4 Table 1 lists the dental sleep disorders in question. They are described briefly below, thereby summarizing and further elaborating on the previous publication by Lobbezoo et al.4 Given that the disorders listed in Table 1 can be accompanied by other sleep disorders that touch on dentistry, we will also discuss a few of the more striking associations between the dental sleep disorders. Finally, the role of the dentist in the assessment and management of dental sleep disorders is described, which is also important information for medical doctors specializing in sleep medicine.
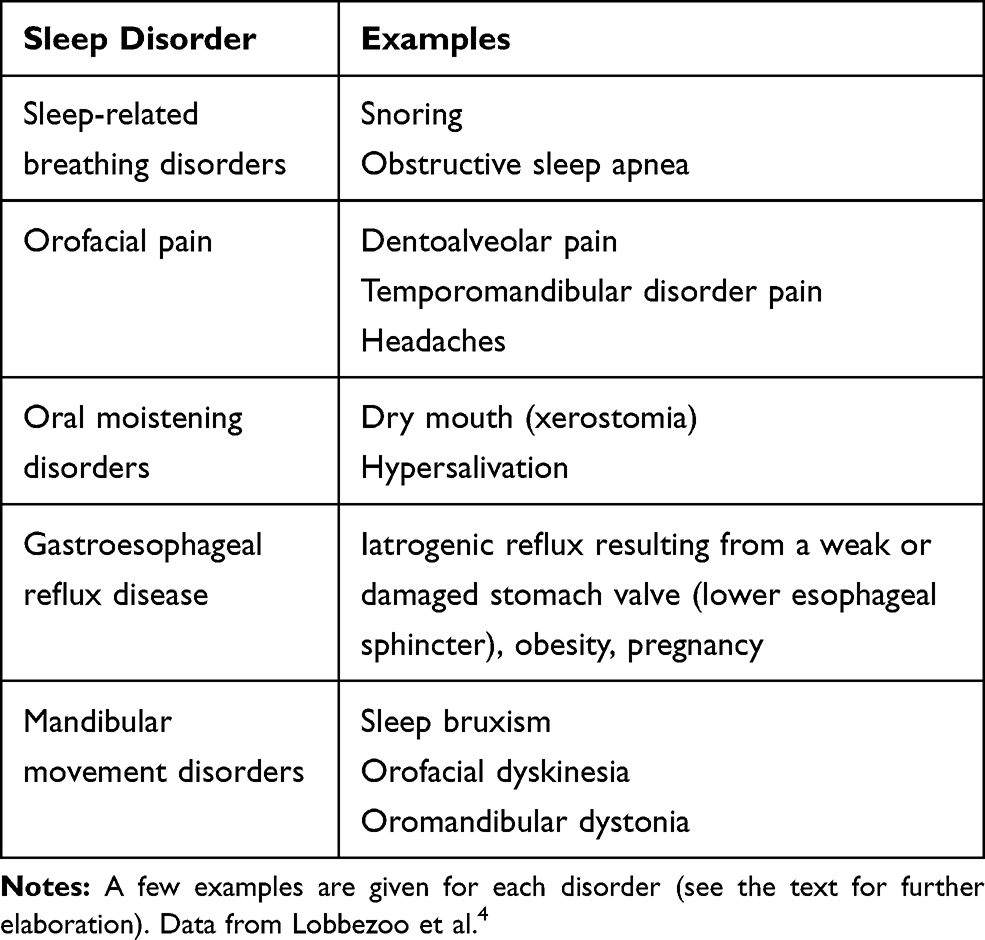 |
Table 1 Summary of Sleep Disorders That Can Be Qualified as Dental Sleep Disorders |
Sleep-Related Breathing Disorders
This category includes snoring and OSA.
Snoring
This all too well-known condition is characterized by audible vibrations of the upper airway during respiration in sleep.6 It is a common problem amongst both men and women and it increases with age: around a half of middle-aged men and a quarter of middle-aged women snore regularly.7 Depending on various factors, such as age, gender and the way in which the snoring is determined, its prevalence in the general population varies from 2% to 85%.8 Assuming that the individual in question does not have OSA, the consequences are primarily of a social nature: bed partners, in particular, sometimes experience very disturbed nights.9 The consequences can therefore be considerable.
Obstructive Sleep Apnea (OSA)
OSA is characterized by repeated obstruction of the collapsible part of the upper airway. This is accompanied by oxygen desaturation and the patient sleeps less deeply and/or wakes up regularly. Between 9% and 38% of the general adult population has OSA.10 The etiology of OSA is multifactorial: associations with various demographic, anatomical, biological and behavioral factors have been described. Its consequences are considerable: OSA can cause the patient to wake up feeling unrested, excessive fatigue/daytime sleepiness, cardiovascular diseases (including hypertension, stroke, heart failure, coronary artery disease and atrial fibrillation), cognitive deterioration, a reduction in libido and a range of other health problems, some of which are serious.11–13 Associations with multiple dental sleep disorders have been found, notably with sleep-related orofacial pain, xerostomia, hypersalivation, GERD, and bruxism (for details, see these disorders’ respective paragraphs below).
The role of the dentist (or dental specialist) is not limited simply to the fabrication of a mandibular advancement appliance on the indication of a medical specialist; he/she can also identify the complaints, symptoms, and risk factors of OSA, such as very loud snoring, excessive fatigue/daytime sleepiness and headaches on waking up. In addition, the dentist/dental specialist can assess the patency of the intraoral airway by identifying a large tongue, enlarged tonsils and a retrognathic mandible. Further, by being alert to specific combinations of complaints and symptoms, such as high blood pressure, obesity and excessive fat storage in the neck region, he/she can also contribute to the diagnostic process. It is important to note that despite the fact that several tools have been introduced for the establishment of possible OSA (eg the Berlin questionnaire, the STOP-BANG questionnaire14,15) there are still no valid instruments available in oral health care practice that provide irrefutable, definite evidence of the presence of OSA. More research is therefore necessary.
Orofacial Pain
Orofacial pain is very common; Lipton et al16 reported that approximately 22% of the general adult population of the United States of America reported having one or more forms of orofacial pain during the previous six months. Orofacial pain comes in many guises. The pain can, for example, be dentoalveolar in nature (and thus originate from the dental elements and the supporting tissues around them), musculoskeletal (pain that originates from muscles or joints), neuropathic (pain that originates from the nervous tissue) or vascular (pain that originates from the vascular or perivascular tissues). Headaches are also deemed orofacial pains. The dentist’s role in the diagnosis and treatment of these conditions is that he/she refers patients with complicated dentoalveolar complaints to an endodontist or an OMF surgeon, and patients with complex musculoskeletal pain, neuropathic pain and/or headaches to an orofacial pain specialist, an OMF surgeon or a general practitioner/medical specialist.
All forms of orofacial pain can affect the patient’s sleep because, for instance, they make it difficult for him/her to drop off or wake him/her up during the night. To illustrate this, 36% of patients with a painful temporomandibular disorders (TMD) experience insomnia.17 This can lead to patients not feeling rested when they get up, reduced levels of energy and resistance, fatigue, irritable bowels and even feelings of depression.17 It should be noted that orofacial pain is not necessarily the cause of sleep problems. The reverse is also possible: ie poor sleep quality can cause orofacial pain. The precise relationship between the two phenomena differs from person to person.18
In addition to the reciprocal relationship between orofacial pain and sleep quality sketched above, there is also increasing evidence of an association between orofacial pain and sleep disorders: for example, 28% of patients with TMD pain also have OSA.17 There are, furthermore, indications that patients with OSA experience more TMD pain than otherwise healthy individuals: figures of 52% and 10% were given by Cunali et al19 and LeResche20 respectively. Sanders et al21 suggest that OSA symptoms precede first-onset TMD-pain complaints via central sensitization. Precise details of the association between OSA and TMD pain are, however, still largely unknown and more research is therefore necessary. The same applies to the much-researched association between TMD pain and sleep bruxism. It is commonly assumed that sleep bruxism overloads the masticatory system, thereby causing pain and dysfunction of the constituent musculoskeletal structures. So far, however, the literature on this topic has only yielded contradictory findings, a striking point being that the more accurately the two conditions are analyzed, the weaker the association is found to be.22
It is very important for the dentist to have insight into the reciprocal relationship between orofacial pain and sleep quality and also in the associations that orofacial pain can have with OSA, sleep bruxism and general sleep disorders, such as insomnia, in order to be able to start the correct course of treatment. Interdisciplinary collaboration, both inside and outside dentistry, will often be necessary here.18
Oral Moistening Disorders
This category includes xerostomia and hypersalivation.
Xerostomia
This condition is defined as “having a dry mouth”.23,24 The patient is bothered by a feeling of dryness in the oral cavity and throat. The prevalence is considerable and, depending on the population examined, varies from 10% to 80%.25 The following are often suggested as potential causes: mouth breathing when waking up; sleeping with an open mouth and snoring; medical conditions such as diabetes, Sjögren’s syndrome, OSA and GERD; and the use of medication, which often has the side effect of a dry mouth.25,26 The treatment of OSA is also associated with a dry mouth: both mandibular advancement appliances and continuous positive airway pressure (CPAP) are linked to complaints of a dry mouth,27 although it should be pointed out that CPAP devices with air humidification contribute to partially solve this problem.28 Xerostomia can wake patients up repeatedly at night, and once awake, they make use of the interruption to go and get something to drink. All in all, xerostomia can therefore disturb one’s sleep pattern greatly.
Dentists play a crucial role in identifying the symptoms of a dry mouth as well as the prevention of its potentially negative consequences. Causal treatment is usually carried out under the supervision of general practitioners/medical specialists or, in the case of mouth breathing, of speech therapists.
Hypersalivation
Hypersalivation entails the production of too much saliva. This means that the balance between saliva production and the frequency of swallowing is disturbed. The frequency of swallowing is lower during sleeping than waking hours: when asleep, on average people swallow about three times an hour whereas, when awake, they swallow at least once every two minutes.29,30 Patients with hypersalivation often complain of a wet pillow or even wet bed linen. The prevalence of hypersalivation is considerable, ie 8%,31 although it is lower than that of xerostomia (see above). Possible causes are conditions such as Parkinson’s disease;32 periodontal problems; poorly-fitting/loose prosthetics; irritated soft tissues in the oropharynx resulting from GERD; and, again, a whole range of medicines.25 Along with xerostomia, hypersalivation is also listed as one of the possible side effects of the mandibular advancement appliances used to treat OSA.27 Hypersalivation also wakens the individual repeatedly, with all the detrimental effects of drowsiness and suchlike during the day. Hypersalivation can, furthermore, cause aspiration, resulting in coughing or even suffocation.
Based on the above description, it is clear that the dentist can make a significant contribution to the identification of hypersalivation and, more particularly, in the causal treatment of cases of hypersalivation originating from dental conditions. If hypersalivation is caused by non-dental factors, a multidisciplinary approach, in collaboration with general practitioners/medical specialists, is indicated.
Gastroesophageal Reflux Disease (GERD)
GERD is defined as a retrograde flow of stomach acid into the distal oesophagus and even into the oral cavity.33 The patient reports having “heartburn”, which disturbs his/her sleep, and may also complain of a sour taste in his/her mouth. Epidemiological research shows that around 20% of the general population experiences GERD once a week, making it a big problem for society as a whole.34,35 Factors that can cause GERD are a weak or damaged stomach valve (lower esophageal sphincter), a diaphragmatic hernia, obesity and pregnancy.36 GERD has considerable consequences for the individual: it can cause wear of the teeth in the form of intrinsic chemical wear (erosion) and sensitive dental elements as a consequence.37 It can also exacerbate xerostomia and hypersalivation, choking being a possible consequence of the latter.25 GERD is, furthermore, associated with causing or aggravating snoring and OSA, although evidence of a causal connection has yet to be found.38 There is, moreover, strong evidence that GERD and sleep bruxism are related to one another, with GERD events preceding bruxism events.39,40 As such, the masticatory muscle activity is thought to help stimulate the secretion of saliva and the resulting increase in pH.39,40
The dentist plays a crucial role in identifying reflux based on its consequences for both the soft tissues of the oropharynx (redness, swelling) and for the teeth (erosion). In addition, he/she can remedy the latter by building up the worn and sensitive teeth with composite material.
Mandibular Movement Disorders
This category includes, amongst other conditions, sleep bruxism, dyskinesia and dystonia.
Sleep Bruxism
Bruxism was recently defined as a repetitive masticatory muscle activity that is characterized by clenching or grinding of the teeth and/or bracing or thrusting of the lower jaw.41 Although bruxism can occur during the day (awake bruxism, ie, a masticatory muscle activity during wakefulness that is characterized by repetitive or sustained tooth contact and/or by bracing or thrusting of the mandible and is not a movement disorder in otherwise healthy individuals42), sleep bruxism (ie, a masticatory muscle activity during sleep that is characterized as rhythmic (phasic) or non-rhythmic (tonic) and is not a movement disorder or a sleep disorder in otherwise healthy individuals42) will be discussed briefly below, with reference to the review article by Lobbezoo et al.43 Sleep bruxism has a prevalence of 12.8 ± 3.1% in the general population.44 Various psychosocial (stress and anxiety), biological (sleep arousals, disturbed neurotransmitter balance and genetics) and exogenous (medicine use, smoking and alcohol) factors play a role in the multifactorial etiology of this disorder.43 The following are listed as possible consequences of the condition: breaking or losing teeth, fillings or implants; intrinsic mechanical wear of the teeth (attrition); masticatory muscle hypertrophy; musculoskeletal pain (TMD pain; see above); and mandibular dysfunction complaints.43 It must be emphasized that some patients with bruxism do not experience these detrimental consequences. Indeed, sleep bruxism is increasingly being associated with potentially positive health outcomes, such as the reduction of the possible detrimental consequences of GERD for the soft tissues of the oropharynx and for the teeth and the strengthening of the upper airway; the latter helps prevent the occurrence of hypopneas or even apneas.45 Interestingly, sleep bruxism is also associated with other sleep-related disorders that are in most cases associated with sleep arousals, such as insomnia,46 Periodic Leg Movements in Sleep,47 and REM sleep Behavior Disorder.48
The dentist is the appropriate professional to diagnose and treat bruxism but he/she should only treat the disorder if it results in serious negative consequences for the patient (eg severe attrition or TMD pain). In the case of severe bruxism, the diagnosis and treatment can be carried out together with general practitioners/medical specialists, preferably after consultation with an orofacial pain specialist.
Orofacial Dyskinesia
This group of movement disorders is characterized by involuntary, predominantly choreatic (dance-like) movements of face, lips, tongue and jaw. If the condition is limited to the jaw, it is important that the dental or medical professional distinguishes between this and the bruxism-related grinding of teeth.49 There are no prevalence figures for the general population available but the condition is rare. Underlying psychiatric conditions and the long-term use of certain medicines (eg neuroleptics and dopamine-related medicines) are thought to be possible causes.49 The impact of orofacial dyskinesia on the daily lives of patients is enormous although little is known about the local consequences. The sleep of patients that experience this debilitating condition may also be disturbed. A good medical history that focuses on the possible causes of the condition, can point the dentist in the direction of an orofacial dyskinesia but its diagnosis and treatment require specialist medical treatment.
Oromandibular Dystonia
If these excessive, involuntary and persistent muscular contractions of lips, tongue and jaw are limited to the jaw, oromandibular dystonia can be confused with bruxism-related clenching.49 Nevertheless, this is a real and potentially debilitating movement disorder, with the same possible causes and consequences as the orofacial dyskinesia described above; it can have enormous social consequences for individuals experiencing it. Unfortunately, prevalence figures for the general population are not available for this condition, which is equally rare, either. The diagnosis and treatment of oromandibular dystonia should, again, be carried out by medical specialists but the dentist can establish its possible presence based on a good medical history that focuses on the possible causes of the condition.
Concluding Remarks
The everyday practice of dental sleep medicine shows that the various dental sleep disorders regularly occur as comorbidities and that they are rarely found in isolation in any one individual patient. Dental sleep disorders therefore jointly form a complex comorbidity network. It is crucial that we unravel this network if we are to provide patients with the best possible care, following personalized management strategies. More research, with appropriate designs to serve the studies’ aims, is therefore necessary. An equally important point for patients is that it is essential that dental sleep medicine education around the world is developed at both undergraduate and postgraduate levels.50 The dentists of the future will have to be fast-tracked to enable them to make their unique contribution to the diagnosis and treatment of this intriguing group of patients as soon as possible. It is the firm belief of the authors of this present article that dental sleep medicine will become increasingly important in the future: this discipline is not simply a passing fashion − it is here to stay!
Abbreviations
CPAP, continuous positive airway pressure; GERD, gastroesophageal reflux disease; OMF, oral and maxillofacial; OSA, obstructive sleep apnea; SBD, sleep-related breathing disorders; TMD, temporomandibular disorders.
Acknowledgments
This paper is created from two previously published articles. It is a modified and elaborated version of an article that was previously published in the Journal of Oral Rehabilitation, Lobbezoo F, Aarab G, Wetselaar P, Hoekema A, Lange J de, Vries N de. A new definition of dental sleep medicine. J Oral Rehabil. 2016;43(10):786–790, with permission from John Wiley and Sons, Hoboken, NJ, USA; © 2016 John Wiley & Sons Ltd.4 It is also an abbreviated and translated version of a Dutch article published in Nederlands Tijdschrift voor Tandheelkunde, Lobbezoo F, Aarab G. Tandheelkundige slaapgeneeskunde: nadere kennismaking met een jong vakgebied [Dental sleep medicine: A further introduction to an emerging dental discipline]. Ned Tijdschr Tandheelkd. 2020;127(4):222–230, with permission from the Nederlands Tijdschrift voor Tandheelkunde B.V., Amsterdam, The Netherlands.51
Funding
No funding was received for this work.
Disclosure
Frank Lobbezoo is a member of the Academic Advisory Boards for GrindCare and Oral Function of Sunstar Suisse S.A., receives research grants from Sunstar Suisse S.A., SomnoMed-Goedegebuure, Health Holland, and Airway Management. Nico de Vries is consultant for Philips Health Care, member of the Medical Advisory Board of NightBalance, and researcher for Inspire and Nyxoa. Jan de Lange declares that he has no conflicts of interest. Ghizlane Aarab is a member of the Academic Advisory Board for Oral Function of Sunstar Suisse S.A. and receives research grants from Sunstar Suisse S.A., SomnoMed-Goedegebuure, and Health Holland. The authors report no other potential conflicts of interest for this work.
References
1. Aarab G, Lobbezoo F. Dental sleep medicine redefined. Sleep Breath. 2018;22:1233. doi:10.1007/s11325-018-1697-4
2. Lobbezoo F, Aarab G. Increasing the visibility of dental sleep disorders. J Clin Sleep Med. 2018;14:1827. doi:10.5664/jcsm.7424
3. Simpson L, Hillman DR, Cooper MN, et al. High prevalence of undiagnosed obstructive sleep apnoea in the general population and methods for screening for representative controls. Sleep Breath. 2013;17:967–973. doi:10.1007/s11325-012-0785-0
4. Lobbezoo F, Aarab G, Wetselaar P, Hoekema A, de Lange J, de Vries N. A new definition of dental sleep medicine. J Oral Rehabil. 2016;43:786–790. doi:10.1111/joor.12421
5. Lavigne GJ, Goulet JP, Zuconni M, Morisson F, Lobbezoo F. Sleep disorders and the dental patient: a review of diagnosis, pathophysiology and management. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1999;88:257–272. doi:10.1016/S1079-2104(99)70025-9
6. American Academy of Sleep Medicine. International Classification of Sleep Disorders.
7. Young T, Palta M, Dempsey J, Skatrud J, Weber S, Badr S. The occurrence of sleep-disordered breathing among middle-aged adults. New Engl J Med. 1993;328:1230–1235. doi:10.1056/NEJM199304293281704
8. Deary V, Ellis JG, Wilson JA, Coulter C, Barclay NL. Simple snoring: not quite so simple after all? Sleep Med Rev. 2014;18:453–462. doi:10.1016/j.smrv.2014.04.006
9. Endeshaw Y, Rice TB, Schwartz AV, et al. Health ABC Study. Snoring, daytime sleepiness, and incident cardiovascular disease in the health, aging, and body composition study. Sleep. 2013;36:1737–1745. doi:10.5665/sleep.3140
10. Senaratna CV, Perret JL, Lodge CJ, et al. Prevalence of obstructive sleep apnea in the general population: a systematic review. Sleep Med Rev. 2017;34:70–81. doi:10.1016/j.smrv.2016.07.002
11. Yaggi HK, Concato J, Kernan WN, Lichtman JH, Brass LM, Mohsenin V. Obstructive sleep apnea as a risk factor for stroke and death. N Engl J Med. 2005;353:2034–2041. doi:10.1056/NEJMoa043104
12. McNicholas WT, Bonsigore MR. Management Committee of EU COST ACTION B26. Sleep apnoea as an independent risk factor for cardiovascular disease: current evidence, basic mechanisms and research priorities. Eur Respir J. 2007;29:156–178. doi:10.1183/09031936.00027406
13. O’Connor GT, Caffo B, Newman AB, et al. Prospective study of sleep-disordered breathing and hypertension: the Sleep Heart Health Study. Am J Respir Crit Care Med. 2009;179:1159–1164. doi:10.1164/rccm.200712-1809OC
14. Chiu HY, Chen PY, Chuang LP, et al. Diagnostic accuracy of the Berlin questionnaire, STOP-BANG, STOP, and Epworth sleepiness scale in detecting obstructive sleep apnea: a bivariate meta-analysis. Sleep Med Rev. 2017;36:57–70. doi:10.1016/j.smrv.2016.10.004
15. Reuter H, Herkenrath S, Treml M, et al. Sleep-disordered breathing in patients with cardiovascular diseases cannot be detected by ESS, STOP-BANG, and Berlin questionnaires. Clin Res Cardiol. 2018;107:1071–1078. doi:10.1007/s00392-018-1282-7
16. Lipton JA, Ship JA, Larach-Robinson D. Estimated prevalence and distribution of reported orofacial pain in the United States. J Am Dent Assoc. 1993;124:115–121. doi:10.14219/jada.archive.1993.0200
17. Smith MT, Wickwire EM, Grace EG, et al. Sleep disorders and their association with laboratory pain sensitivity in temporomandibular joint disorder. Sleep. 2009;32:779–790. doi:10.1093/sleep/32.6.779
18. de Leeuw R, Klasser GD, eds. Orofacial Pain: Guidelines for Assessment, Diagnosis, and Management. Chicago, IL: Quintessence Publishing Co, Inc; 2008.
19. Cunali PA, Almeida FR, Santos CD, et al. Prevalence of temporomandibular disorders in obstructive sleep apnea patients referred for oral appliance therapy. J Orofac Pain. 2009;23:339–344.
20. LeResche L. Epidemiology of temporomandibular disorders: implications for the investigation of etiologic factors. Crit Rev Oral Biol Med. 1997;8:291–305. doi:10.1177/10454411970080030401
21. Sanders AE, Essick GK, Fillingim R, et al. Sleep apnea symptoms and risk of temporomandibular disorder: OPPERA cohort. J Dent Res. 2013;92(7 Suppl):70S–7S. doi:10.1177/0022034513488140
22. Manfredini D, Lobbezoo F. Relationship between bruxism and temporomandibular disorders: a systematic review of literature from 1998 to 2008. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010;109:e26–e50. doi:10.1016/j.tripleo.2010.02.013
23. Nederfors T. Xerostomia and hyposalivation. Adv Dent Res. 2000;14:48–56. doi:10.1177/08959374000140010701
24. Löfgren CD, Wickström C, Sonesson M, Lagunas PT, Christersson C. A systematic review of methods to diagnose oral dryness and salivary gland function. BMC Oral Health. 2012;12:29. doi:10.1186/1472-6831-12-29
25. Llena-Puy C. The role of saliva in maintaining oral health and as an aid to diagnosis. Med Oral Patol Oral Cir Bucal. 2006;11:E449–E455.
26. Scully C. Drug effects on salivary glands: dry mouth. Oral Dis. 2003;9:165–176. doi:10.1034/j.1601-0825.2003.03967.x
27. Jonas DE, Amick HR, Feltner C, et al. Screening for obstructive sleep apnea in adults: an evidence review for the U.S. preventive services task force [Internet]. Rockville (MD): Agency for Healthcare Research and Quality (US); 2017. Available from http://www.ncbi.nlm.nih.gov/books/NBK424160.
28. Kennedy B, Lasserson TJ, Wozniak DR, Smith I. Pressure modification or humidification for improving usage of continuous positive airway pressure machines in adults with obstructive sleep apnoea. Cochrane Database Syst Rev. 2019;12(12):CD003531.
29. Sato K, Nakashima T. Human adult deglutition during sleep. Ann Otol Rhinol Laryngol. 2006;115:334–339. doi:10.1177/000348940611500503
30. de Vries N, van de HP, Leemans CR, Eds. Leerboek KNO En Hoofd-Halschirurgie. Houten: Springer; 2019:433.
31. Lalonde B, Lavigne GJ, Goulet J-P, Barbeau J. Prevalence of reported salivary dysfunction symptoms in an adult Northern population. J Dent Res. 1997;76:99.
32. Kalf JG, de Swart BJ, Borm GF, Bloem BR, Munneke M. Prevalence and definition of drooling in Parkinson’s disease: a systematic review. J Neurol. 2009;256:1391–1396. doi:10.1007/s00415-009-5098-2
33. Vakil N, van Zanten SV, Kahrilas P, Dent J, Jones R. The Montreal definition and classification of gastroesophageal reflux disease: a global evidence-based consensus. Am J Gastroenterol. 2006;101:1900–1920. doi:10.1111/j.1572-0241.2006.00630.x
34. Dent J, El-Serag HB, Wallander MA, Johansson S. Epidemiology of gastro-oesophageal reflux disease: a systematic review. Gut. 2005;54:710–717. doi:10.1136/gut.2004.051821
35. Djärv T, Wikman A, Nordenstedt H, Johar A, Lagergren J, Lagergren P. Physical activity, obesity and gastroesophageal reflux disease in the general population. World J Gastroenterol. 2012;18:3710–3714. doi:10.3748/wjg.v18.i28.3710
36. Zachariah RA, Goo T, Lee RH. Mechanism and pathophysiology of gastroesophageal reflux disease. Gastrointest Endosc Clin N Am. 2020;30:209–226. doi:10.1016/j.giec.2019.12.001
37. Wetselaar P, Manfredini D, Ahlberg J, et al. Associations between tooth wear and dental sleep disorders, a narrative overview. J Oral Rehabil. 2019;46:765–775.
38. Lim KG, Morgenthaler TI, Katzka DA. Sleep and nocturnal gastroesophageal reflux: an update. Chest. 2018;154:963–971. doi:10.1016/j.chest.2018.05.030
39. Miyawaki S, Tanimoto Y, Araki Y, Katayama A, Fujii A, Takano-Yamamoto T. Association between nocturnal bruxism and gastroesophageal reflux. Sleep. 2003;26:888–892. doi:10.1093/sleep/26.7.888
40. Ohmure H, Oikawa K, Kanematsu K, et al. Influence of experimental esophageal acidification on sleep bruxism: a randomized trial. J Dent Res. 2011;90:665–671. doi:10.1177/0022034510393516
41. Lobbezoo F, Ahlberg J, Glaros AG, et al. Bruxism defined and graded: an international consensus. J Oral Rehabil. 2013;40:2–4. doi:10.1111/joor.12011
42. Lobbezoo F, Ahlberg J, Raphael KG, et al. International consensus on the assessment of bruxism: report of a work in progress. J Oral Rehabil. 2018;45:837–844. doi:10.1111/joor.12663
43. Lobbezoo F, Ahlberg J, Manfredini D, Winocur E. Are bruxism and the bite causally related? J Oral Rehabil. 2012;39:489–501. doi:10.1111/j.1365-2842.2012.02298.x
44. Manfredini D, Winocur E, Guarda-Nardini L, Paesani D, Lobbezoo F. Epidemiology of bruxism in Adults. A systematic review of the literature. J Orofacial Pain. 2013;27:99–110. doi:10.11607/jop.921
45. Lavigne GJ, Kato T, Kolta A, et al. Neurobiological mechanisms involved in sleep bruxism. Crit Rev Oral Biol Med. 2003;14:30–46. doi:10.1177/154411130301400104
46. Maluly M, Andersen ML, Dal-Fabbro C, et al. Polysomnographic study of the prevalence of sleep bruxism in a population sample. J Dent Res. 2013;92(7_suppl):S97–S103. doi:10.1177/0022034513484328
47. Van der Zaag J, Naeije M, Wicks DJ, Hamburger HL, Lobbezoo F. Time-linked concurrence of sleep bruxism, periodic limb movements, and EEG arousals in sleep bruxers and healthy controls. Clin Oral Investig. 2014;18:507–513. doi:10.1007/s00784-013-0994-3
48. Abe S, Gagnon JF, Montplaisir JY, et al. Sleep bruxism and oromandibular myoclonus in rapid eye movement sleep behavior disorder: a preliminary report. Sleep Med. 2013;14:1024–1030. doi:10.1016/j.sleep.2013.04.021
49. Lobbezoo F, Naeije M. Dental implications of some common movement disorders: a concise review. Archs Oral Biol. 2007;52:395–398. doi:10.1016/j.archoralbio.2006.09.005
50. Lobbezoo F, Aarab G. Dental sleep medicine in the dental curriculum: what should be the dot on the horizon? Sleep Breath. 2020. doi:10.1007/s11325-020-02133-x
51. Lobbezoo F, Aarab G. Tandheelkundige slaapgeneeskunde: nadere kennismaking met een jong vakgebied [Dental sleep medicine: a further introduction to an emerging dental discipline]. Ned Tijdschr Tandheelkd. 2020;127(4):222–230. doi:10.5177/ntvt.2020.04.20006
52. aadsm.org [homepage on the Internet]. About dental sleep medicine. Available from: https://www.aadsm.org/. Accessed December 2, 2020
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.