Back to Journals » Open Access Rheumatology: Research and Reviews » Volume 15
A Framework to Overcome Challenges in the Management of Infections in Patients with Systemic Lupus Erythematosus
Authors Rao M ![]() , Mikdashi J
, Mikdashi J
Received 3 March 2023
Accepted for publication 18 July 2023
Published 27 July 2023 Volume 2023:15 Pages 125—137
DOI https://doi.org/10.2147/OARRR.S295036
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Chuan-Ju Liu
Madhavi Rao, Jamal Mikdashi
Department of Medicine, Division of Rheumatology and Clinical Immunology, University of Maryland School of Medicine, Baltimore, MD, USA
Correspondence: Jamal Mikdashi, Division of Rheumatology and Clinical Immunology, University of Maryland School of Medicine, 10 South Pine Street, Suite 834, Baltimore, MD, 21201, USA, Tel +1 410 706 6474, Fax +1 410 7060231, Email [email protected]
Abstract: Infections remain one of the leading causes of death in systemic lupus erythematosus (SLE), despite awareness of factors contributing to increased susceptibility to infectious diseases in SLE. Clinicians report challenges and barriers when encountering infection in SLE as certain infections may mimic a lupus flare. There are no evidence-based practice guidelines in the management of fever in SLE, with suboptimal implementations of evidence-based benefits related to infectious disease control and/or prevention strategies in SLE. Vigilance in identifying an opportunistic infection must be stressed when confronted by a diagnostic challenge during a presentation with a febrile illness in SLE. A balanced approach must focus on management of infections in SLE, and reduction in the glucocorticoids dose, given the need to control lupus disease activity to avoid lupus related organ damage and mortality. Clinical judgement and application of biomarkers of lupus flares could reduce false positives and overdiagnosis and improve differentiation of infections from lupus flares. Further precision-based risk and screening measures must identify individuals who would benefit most from low dose immunosuppressive therapy, targeted immune therapy, and vaccination programs.
Keywords: systemic lupus erythematosus, infections, challenges, management, lupus flares
Plain Language Summary
Patients with systemic lupus erythematosus (SLE) are at considerable risk of serious infections. Clinical providers report an ongoing challenge during an encounter with a febrile illness in SLE patients, by way of the varied types of infections mimicking lupus disease flare. Misdiagnosis of an infection for lupus flare will lead to complications and death if not treated. Lupus patients must seek medical attention when a febrile illness occurs. Providers should initiate prompt antibiotic treatment and reduce the dose of steroids during a febrile illness in SLE. In addition, providers should apply infectious disease controls and vaccine preventive measures during low disease activity state to prevent life-threatening conditions and death.
Introduction
Infectious diseases and their causative agents pose considerable challenges for the management of patients with systemic lupus erythematosus (SLE).1,2 Despite awareness of factors contributing to increased susceptibility to infections in SLE, and having the knowledge of vaccinations and pre-exposure prophylaxis, infections remain one of the leading causes of death in SLE across all times.3,4
The poor clinical outcome of infection in SLE reflects the complex interplay of infectious pathogens and the highly dysregulated nature of the immune system in SLE. Infections are at times coupled with lupus disease activity states where glucocorticoids and cytotoxic immune suppressive therapy may trigger infections. The major burden is that there are no evidence-based practice guidelines in the management of fever, or evidence-based benefits related to implementation of infectious disease controls and/or prevention strategies in SLE. In addition, the lack of specific biomarkers of lupus flare or lupus related infections and the near absence of clear principles on the use of preventive measures with their insufficient evidence are barriers implied in the poor outcome.
To reduce the risk of infections in SLE and their complications, providers should apply strategies of glucocorticoids dose reduction and judicious use of immunosuppressive and targeted biological therapies with treatment to target approaches.5 Novel therapeutics in SLE, though safer and efficacious in controlling disease activity and in achieving disease remission, must also prevent infections, damage accrual and death.
Importantly, providers should apply diverse therapeutic strategies including general hygienic methods, vaccinations, recognition of latent and opportunistic infections and antibiotic prophylaxis.6,7 However, implementation of these measures and their use in clinical practice is inconsistent and rarely applied.8,9
In this manuscript we analyzed the burden, the types of infection, the factors related to higher risk of infection, and highlight certain tools used in predicting infection in SLE. We propose a framework to overcome challenges in the management of infections in SLE patients and explore opportunities that can benefit the therapeutic and preventive plan of care.
Methods and Materials
We performed a semi-structured systematic review of the literature of adults (age ≥18 years) with infections in SLE between January 1985 and June 2022, using search words such as, “systemic lupus erythematosus”, “infection”, “viral syndrome”, “bacterial infections”, “fungal”, “opportunistic infections”, “parasites”, and “prevention” were reported. Sources of literature from which full-length clinical studies in humans were extracted were published in Medline, PubMed Clinical Queries and Embase, Cochrane library, and the database from CINHAL.
The Burden of Infections in SLE
Mortality and hospitalization rates related to infections in SLE have increased dramatically over the past decade compared to the general population.6 Researchers suggest a change in the trend and the pattern in SLE mortality where infection is the biggest reason for mortality compared to lupus related disease activity, lupus nephritis or cardiovascular diseases.10 Similar observations have appeared in not just the United States, but in Japan, South Korea, Canada, China, Hong Kong, Malaysia, Jamaica, Columbia, Mexico, Chile, Brazil, United Kingdom, Spain, Denmark, France, and Sweden. The impact of infection in SLE is even more pronounced in developing countries.2,11
Infections account for 20% to 55% of all deaths in SLE patients and are the leading cause of deaths within the first year after the diagnosis of SLE.12 Bacterial infections contribute to a higher relative risk of hospitalization which could be serious requiring high level care. Pulmonary infections and septicemia had the largest positive effect on increased mortality in SLE.13
Types of Infections in SLE
Bacterial Infections
Around 60% to 75% of all reported infections in SLE are common bacterial infections14 The systems of respiratory, urinary tract, skin and soft tissue are the most common sites of infection in SLE. Respiratory tract infections are common in hospitalized patients, whereas urinary system, skin and soft tissue infections are more frequent in the outpatient setting.15
Escherichia coli causing urine tract infections and streptococcal pneumonia causing bronchopneumonia, bacteremia, and sepsis represent the most frequent pathogens.16,17 Streptococcal infections are severe in SLE related to reduction in opsonization with complement factor 3b/inactive C3b (C3b/iC3b) as compared to other rheumatic syndromes and the healthy population.18
Staphylococcus aureus causes skin and soft tissue infections, bone and joint infections, as well as bacteremia. Klebsiella and pseudomonas species may cause urine tract infections related bacteremia in SLE that are associated with shortened survival rate.19
Salmonella enterica infections are more frequent among SLE subjects as compared to the general population causing a spectrum of syndromes including gall bladder infection and bacteremia.20 Atypical presentations of Salmonella species infections in SLE patients include osteomyelitis of long bones, septic arthritis, soft tissue abscess, meningitis, typhoid fever, and sepsis syndrome. Risk factors for salmonella infection in SLE are associated with splenic dysfunction and opsonization defects as well as high disease activity and use of immune suppressive therapy.21
Mycobacterial Infections
Various mycobacterial species infections are common in SLE and may disseminate leading to serious and lethal disease.22 The prevalence of Mycobacteria tuberculosis ranges from 5% to 30% depending on the specific geographic region which is higher in SLE subjects than the general population.23 Clinical presentations of mycobacteria may mimic lupus clinical syndrome, with features that involve severe extrapulmonary disease, extensive pulmonary syndromes, and high relapse rates.24 non-tuberculosis mycobacterial infections cause skin and soft tissue infections with skin nodules and skin abscesses. Higher cumulative doses of glucocorticoids and renal disease are associated with increased risk of mycobacterial species in SLE.25
Viral Infections
Herpes zoster (HZ) represents the most common viral infection in SLE patients, followed by cytomegalovirus (CMV) and human papilloma virus (HPV).26,27 Other viruses with high frequency in SLE include, parvovirus B19, hepatitis B and C, influenza, and SARS-COV-2.28,29
HZ infections occur at the age of 30 to 40 years in SLE with higher prevalence in the Asian population than in the US population.30 Risk factors include increasing age, lymphopenia, major organ disease, multi morbidities, glomerulonephritis, high dose glucocorticoids and non-glucocorticoid therapy such as mycophenolate mofetil and cyclophosphamide.31 HZ infection and reactivation occurring even during a low disease activity state is associated with serious morbidity, inferior quality of life and death. The use of high-dose glucocorticoids is associated with bacterial superinfection.
CMV infection in SLE may present as gastrointestinal bleed, colitis, hepatitis, retinitis, or encephalitis, with a high incidence of pneumonitis.32 High dose of glucocorticoids, cyclophosphamide, plasma exchange, pancytopenia and concurrent infections have been associated with serious CMV clinical syndrome. High CMV viral loads are associated with the development of CMV infection in patients with SLE.33
The rate of cervical HPV infections is higher in SLE patients than in the general population, with an increased risk for high grade squamous interepithelial lesions.34 This may be due to delayed clearance of infections or greater reactivation of latent infections, in addition to higher rates of HPV coinfection. The association between immunosuppressive medications and risk of HPV infection needs additional evaluation.
A higher proportion of hepatitis C infection is frequent in patients with SLE compared to healthy controls.35 However, there appears to be a lower risk of hepatitis B infection in patients with SLE (possible protective role of overexpressed cytokines in these patients). Nonetheless, the risk of reactivation of hepatitis B virus is higher in SLE patients receiving a daily steroid dose of >10 mg/day and patients over the age of 40. Rituximab, to treat SLE, is associated with a higher risk of reactivation of hepatitis B and patients should be screened prior to therapy.
Parvovirus B19 and SLE share certain similarities in terms of presentation, including fevers, malaise, lymphadenopathy, anemia, and rash.36 This viral infection is also able to induce the production of autoantibodies specific to SLE, like anti-dsDNA and soluble nuclear antigens. It has been proposed that parvovirus B19 can induce pathogenic autoimmunity through a variety of mechanisms, including molecular mimicry.37 However, it is difficult to estimate the prevalence of this parvovirus infection in SLE patients as immune therapy inhibits immunoglobulin (IgM and IgG) seroconversion.
The COVID-19 Global Rheumatology Alliance and OpenSAFELY databases provide data that suggest that patients with SLE are at a higher risk of severe disease, hospitalization and death from COVID-19 compared to the general population.38 The risk is highest in patients on prednisone dose >10 mg/day, and those on rituximab, as compared to those patients maintained on belimumab, hydroxychloroquine, azathioprine, methotrexate, or mycophenolate mofetil.39
Opportunistic Infections
Opportunistic infections like Listeria monocytogenes, Nocardia species, Aspergillus fumigatus, and others may present as neurologic syndromes that mimic neuropsychiatric lupus and behave more aggressively to cause severe disease leading to death.40 Cryptococcus neoformans presents in SLE as meningitis, meningoencephalitis, lung nodules and pneumonia/bronchiolitis driven by long term use of glucocorticoids and cytotoxic drugs and is associated with higher mortality rates.41
Candida albicans is a usual form of candidemia in SLE and usually involves the gastrointestinal and genitourinary system and may become invasive at times.42
Why are Lupus Patients at Substantial Risk for Infections?
Aberrant Immune Functions in SLE
The aberrant immune response in SLE, low serum complement levels, functional asplenia, and abnormal host response of neutrophils and macrophages to pathogens have contributed to the rise in infectious rates in SLE (Table 1). The impaired inflammatory response with decreased chemotaxis, membrane recognition and attachment to microorganisms, phagocytosis, oxidative metabolism could also predispose to infection.
 |
Table 1 Risk Factors for Infection in SLE |
Lymphopenia and neutropenia are common hematologic manifestations in SLE and can have poor clinical outcomes with predisposition to infection given decreased T-cell activity and dysfunctional macrophages and monocyte systems.43 Prior studies have shown that a decrease in phagocytic function and the impaired handling of immune complexes due to the presence of autoantibodies against Fc gamma receptors (FcgR) which belong to the tumor necrosis factor (TNF) alpha superfamily contribute to the risk of infections.44
Complement dysfunction is frequent in SLE, reflected by inherited complement deficiency, and hypocomplementemia during SLE disease activity. SLE patients with complement dysfunctions show an increase in risk to capsulated organisms such as Streptococcal pneumonia, Neisseria meningitis and Neisseria gonorrhea. Hypogammaglobulinemia encountered in SLE contributes to an increased risk of recurrent and severe bacterial infections, although polyclonal hypergammaglobulinemia is common in SLE. Whether immunoglobulin replacement therapy decreases the risk of infection in those patients requires further investigation.45
In addition, the risk of infection in SLE is higher in the presence of comorbidities and when using glucocorticoids, immunosuppressive and immune modulatory therapy. The incidence of kidney involvement, diabetes, and higher lupus damage index (SDI/SLE international collaborating clinic) scores were dramatically higher in SLE patients with an infection compared to SLE patients without an infection. In fact, the use of aggressive immunosuppressive therapy is a serious risk factor for the development of infections in SLE.46
Impact of Immune Therapy and Risk of Infections
The use of immunosuppressive therapy will induce difficulty in mounting an immune response to viral and bacterial infections in SLE, including the exposure to immunosuppressive agents including high-dose glucocorticoids, alkylating agents such as cyclophosphamide, in addition to mycophenolate mofetil, azathioprine, cyclosporin, and hydroxychloroquine.4,6
Importantly, glucocorticoid use is a significant risk factor for serious infections requiring hospitalization. Indeed, the risk for infection in SLE patients is a 10-fold increase in patients at a prednisone dose over 20 mg daily. Thus, the emphasis on keeping the prednisone dose below 7.5 mg daily or the use of pulses of intravenous methylprednisolone to control disease activity.47
Intravenous cyclophosphamide use has been associated with an increased risk in infection in particular HZ infections as described in SLE population studies, whereas the infection rates are similar among users of azathioprine, mycophenolate, and methotrexate.46,48 Further, mycophenolate use is associated with a lower risk of infection in non-Asian patients with lupus nephritis as compared to cyclophosphamide. However poor clinical outcomes with related deaths appeared to be more frequently observed among the Asian population.
Mycophenolate is a protective against Pneumocystis jirovecii pneumonia and Coxsackie virus infections in transplant patients; however, this protective effect in SLE patients requires confirmation. Antimalarial agents are the major anchor medication in lupus and studies have supported fewer infection rates with their exposure.49
Effective and targeted biological therapy with their steroid-sparing effects, are becoming available, yet many had adverse events, including serious infections. Infections either mild or severe do not seem to be a major concern in patients treated with belimumab as indicated in the post marketing data. On the other hand, rituximab's (an anti-CD-20 monoclonal antibody) use has been associated with severe infections, including bronchopneumonia followed by sepsis, the frequent organisms involved during rituximab therapy include S. pneumonia, followed by E. coli and S. aureus. While severe infections are associated with rituximab exposure occurring within the first 6 months of treatment, these patients have been receiving high doses of glucocorticoids.50
Like immunosuppressive therapy, biological therapy in SLE is associated with infectious comparable incidence rates including opportunistic infections. However, Janus kinase targeted therapy has a slightly higher rate of herpes zoster infections, with a dose dependent pattern of infectious risk.51
Infections May Trigger the Development of SLE
The SLE disease process is triggered by genetic, immunological, and environmental factors including the possible role of certain microbial agents (viral, bacterial, parasitic, or fungal). Through molecular mimicry, bacterial DNA can also stimulate autoreactive B cells leading to an autoimmune response.52
Viruses associated with SLE onset include, human endogenous retroviruses (HERV), Epstein-Barr virus (EBV), parvovirus B19, CMV and human immunodeficiency virus (HIV-1).53,54
The relationship between tuberculosis and SLE suggests an increased risk of SLE in patients exposed to tuberculosis based on molecular and epidemiologic data.22,55
Exposure to Helicobacter pylori has been linked to a lower risk of SLE or delay in its onset like the protective role of helminth infections in SLE, attributed to the activation of lymphocytes and secretion of interleukin 10. Toxoplasma gondii appears to protect against progression of SLE, while Leishmania infection may trigger polyclonal activation of B cells and activation of ribonucleoproteins. Controversy remains about the role of Plasmodium falciparum in reducing the risk of SLE onset.56
The onset of SLE is associated with exposure to certain vaccines including Bacillus Calmette- Guérin, and BNT162b2 mRNA, with varying degrees of severity from cutaneous lupus to lupus nephritis.57 A recent systematic review meta-analysis study has emphasized the safety of HPV vaccination in SLE, given the low-level evidence of the temporal relationship between SLE development following the exposure of HPV vaccine.58,59
Existing SLE May Undergo an Exacerbation Following an Infection
Multiple factors are known to cause SLE flares, including exposure to UV light, certain hormones, and drugs, but infections also worsen existing SLE, leading to poor outcomes.60 Infections may trigger a worsening lupus disease process leading to a feedback loop that may reinforce autoimmunity. The exposure to influenza infection is associated with lupus flares leading to hospitalization within seven days of infection, regardless of patients’ age, gender, underlying illnesses, or immunosuppressive therapies.61
Others have confirmed the association of infection and high disease activity in hospitalized lupus patients independent of prednisone dose, comorbid conditions, or disease duration.
A better understanding of the interactions between viral proteins, bacterial microbiome and lupus related nuclear autoantigens and the host immune system in SLE could help improve the therapeutic management of challenging SLE patients with infections. Thus, vigilance should be borne in mind when challenged by infection in SLE and use of clinical predictors of infection is then fundamental.
Clinical Predictors of Infections in SLE
A major challenge in the care of SLE patients is how to differentiate between a clinical presentation of an infection from a lupus flare. Investigators have suggested certain laboratory biomarkers that are indicative of infections, yet these biomarkers remain nonspecific and at times misleading. Further atypical presentation of infectious clinical syndromes in SLE may vary with the array of symptoms that mimic a lupus flare, and individual infections may present concurrently during a lupus flare. A predictor marker must then have high specificity and sensitivity for determining whether the patient is presenting an infection or a lupus flare.62
Shaking chills, leukocytosis, and neutrophilia with normal dsDNA were associated with infection in SLE.63 Yet leukopenia is common in severe sepsis, and pneumococcal pneumonia, and neutropenia in typhoid infections and brucellosis.
Certain clinical predictors of infections outlined below are applicable in clinical practice:
Serum C-Reactive Protein (CRP)
C-reactive protein (CRP) is a key acute phase protein synthesized by the liver and secreted in response to interleukin-6 stimulation. CRP has also the ability to opsonize bacteria, activate the complement pathway, and bind FcR on phagocytes, facilitating elimination of pathogens.64
CRP has been an unreliable measure for lupus disease activity (except for serositis).65
Elevated CRP (in the absence of serositis) is higher in SLE patients with bacterial infections. The cut-off value of 19.2 mg/l has a sensitivity of 81.2% and a specificity of 73.9% during an infectious event.66 However, limitations remain for the application of CRP in the diagnosis of bacterial infections in SLE and other rheumatic diseases.
Elevated Procalcitonin (PCT)
Procalcitonin (PCT) a protein consisting of 116 amino acids and the precursor of calcitonin, has a better diagnostic performance than CRP in differentiating bacterial infections from lupus flares. However, the diagnostic value of PCT and CRP in the identification of bacterial infection in SLE remains unsettled.67,68
Mannose Binding Lectin (MBL)
Mannose binding lectin (MBL) is a protein produced by the liver that activates the complement system by an associated protease, the MBL-associated serine protease. MBL polymorphisms have been associated with SLE development in multiple populations and high MBL levels are predictive of disease activity especially lupus nephritis.69
CD64
CD64 is a receptor observed on monocytes, macrophages and on neutrophils (nCD64). Peripheral nCD74 index combined with elevated CRP improves the ability to predict bacterial infections.70
High Mobility Group Box Chromosomal Protein 1 (HMGB1)
High mobility group box chromosomal protein 1 (HMGB1) is a nuclear non-histone protein and a damage associated molecular pattern protein.71 Their levels are notably higher in SLE patients, especially those with renal involvement. However, their levels are elevated after onset of sepsis and septic shock.
2′5′-Oligoadenylate Synthetase (OAS)
2′5′-oligoadenylate synthetase (OAS) is an enzyme activated by Type I IFN which leads to the degradation of RNA and is important for the protection from vital infections.72 High OASL expression levels negatively correlate with the presence of certain infections and may provide useful information in differentiating disease lupus flare.
Soluble Triggering Receptor Expressed on Myeloid Cells Type 1 (sTREM-1)
The receptor TREM-1 expressed on the surface of mature neutrophils and monocytes in response to bacterial and fungal infections lead to a higher level of the soluble form (sTREM-1) in lupus patients with flares and in those with infections, compared to quiescent disease or the general population.73
CD27
CD27 protein is a TNF receptor expressed on T- and B-lymphocytes where high expression of CD27 corresponds with high disease activity.74
Delta Neutrophil Index (DNI)
Delta neutrophil index (DNI) is a measure of immature granulocytes and is determined by subtracting the number of mature polymorphonuclear leucocytes from myeloperoxidase reactive cells. When compared to CRP, a high DNI correlates better with sepsis and aids in early diagnosis.7
Cerebrospinal Fluid (CSF) Biomarkers
Patients with neuropsychiatric lupus have elevated levels of interleukin-6 (IL-6), prostaglandin E2 (PGE2) and immunoglobulin G (IgG) in their cerebrospinal fluid (CSF).75,76 However, in central nervous system (CNS) infections, there are elevated levels of IL-6 and PGE2 but not significantly elevated CSF or IgG.
Sepsis Scores in SLE
The high mortality of SLE patients with sepsis in the intensive care units (ICU) used sepsis scores as good predictors of mortality. These include, Simplified Acute Physiology Score II (SAPS II), Sequential Organ Failure Assessment (SOFA) and Acute Physiology and Chronic Health Evaluation II (APACHE II).77
Despite the discovery of new biomarkers to verify the infections in SLE, none of these biomarkers alone confirm or exclude an infection. A mixture of these tests may be more accurate in predicting the diagnosis and monitoring of infections in SLE patients.78
Nonetheless, these biomarkers require further reliability and validity studies in different SLE populations and long-term data in SLE patients with distinct types of infections. An optimal biomarker or combination of biomarkers of infections or lupus flares should be accurate and reproducible and should enhance the approach to early diagnosis, effective treatment, and improved clinical outcome.
Proposed Steps to Take When Challenged with Infection in SLE
Assessment of SLE patients remains crucial when confronted by a major diagnostic challenge of having a presentation with a febrile illness. The need to control lupus disease activity that requires suppression of the immune system to avoid lupus related organ damage and death complicates the care of lupus patients. Yet, crucial, and appropriate evaluation of infectious etiology and prompt initiation of antibiotics will evade serious life-threatening complications.
Proposed steps to adopt when challenged by an infection in SLE are outlined and depicted in Table 2.
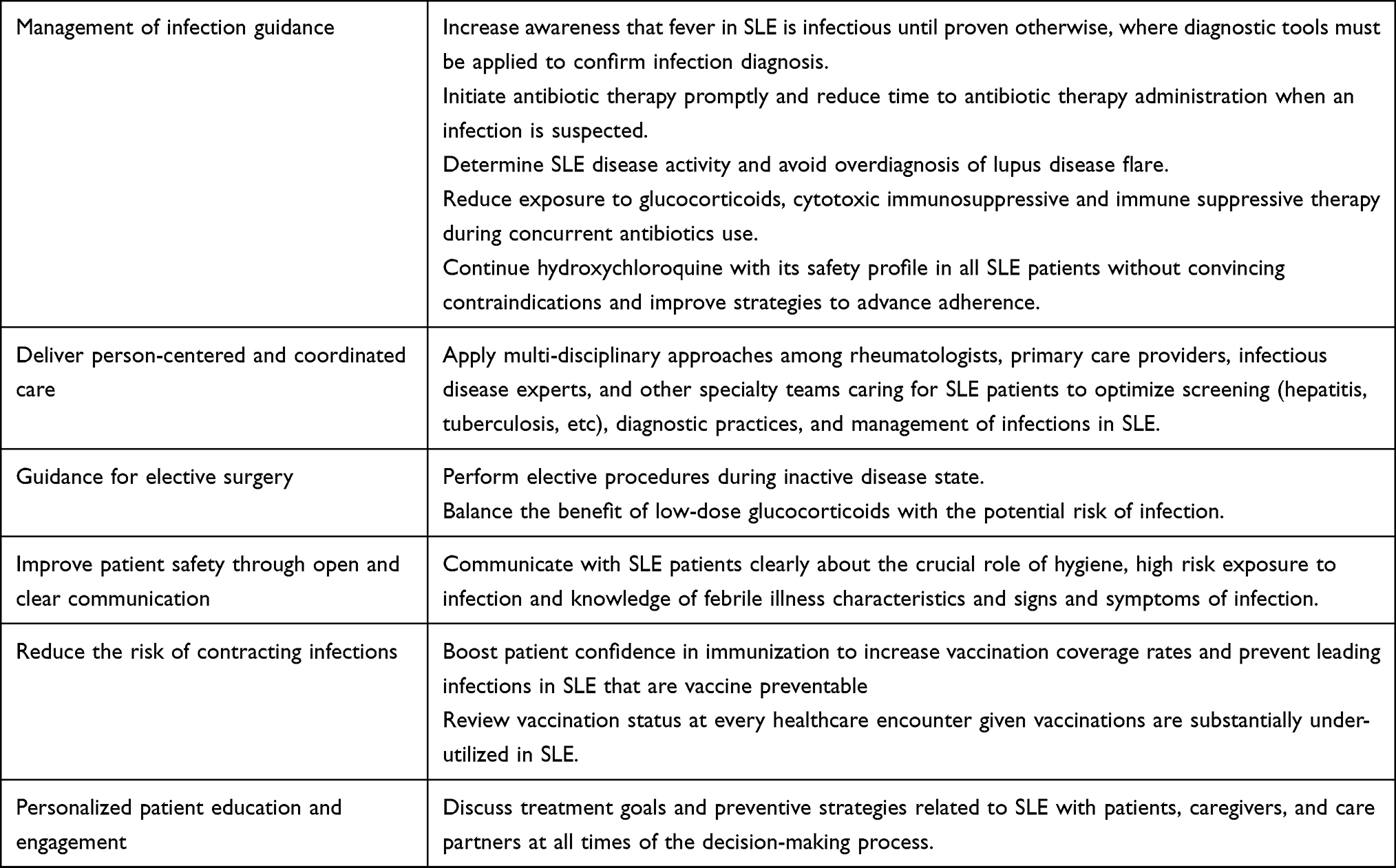 |
Table 2 Proposed Strategies to Manage an Infectious Challenge in Systemic Lupus (SLE) |
Fever in SLE is infectious until proven otherwise. While the prevalence of fever in SLE has declined over the past decades related to the intake of non-steroidal anti-inflammatory drugs, glucocorticoids and broad-spectrum antibiotics, the source of fever must be identified. Thus, vigilance warrants efforts in identifying a latent or an opportunistic infection in febrile patients with SLE.
Initial assessment should focus on risk indices based on age, multi-morbidities, use of glucocorticoids, cytotoxic immune suppressive and immune modulatory therapy. High-risk lupus patients require hospitalization. It is vital to deal with evolving sepsis and its complications in the setting of quantitative or qualitative neutropenia be it related to SLE or a complication of cytotoxic immunosuppressive therapy or immune modulatory treatment.
Frameworks in the diagnostic work up of fever emphasize ongoing evaluations guided by cultures and clinical data including awareness of antimicrobial resistant infections. Applying the abovementioned clinical predictors of infection including CRP, procalcitonin and others is helpful. Molecular diagnostic assays may be useful if available including those combined with 18F-fluorodeoxyglucose positron-emission tomography and computed tomography (FDG PET-CT) and next-generation sequencing. Nevertheless, the diagnostic yield of these tools in autoimmune disorders remains limited.79
On the other hand, fever, in systemic autoimmune disorders like SLE is linked to adaptive immunity driven by interferon response during the lupus disease activity state and must be suspected when having negative infectious work-ups or microbiological control of infections.80 It is imperative to determine disease activity in febrile illnesses in SLE and avoid possible overdiagnosis of lupus disease flare.
There are few examples of overdiagnosis of SLE and lupus flares, but it is important to approach those patients with the understanding of the risk of treatment with immune suppressive therapy and the risk of undertreatment.81
The diagnosis of SLE and lupus flare should be based on diagnostic criteria that include patients with mild disease activity. SLE disease activity must be determined clinically employing clinical questionnaires including SLE disease activity index (SLEDAI), British Isles Lupus Assessment Group disease activity index (BILAG-2004), Systemic Lupus Activity Measure (SLAM), the Systemic Lupus Activity Index (SLAI), European Consensus Lupus Activity Measurements index (ECLAM) and the Systemic Lupus Activity Questionnaire (SLAQ) for Population Studies.82
Clinical features like the presence of scleritis, cytoid bodies on eye examination, lupus dermatitis, splinter hemorrhages, cutaneous vasculitis or livedo pattern, friction rub of pericarditis and leg edema suggesting myocarditis, and pulmonary hypertension or renal disease of glomerulonephritis are clues to advocate for lupus disease activity.
Biomarkers like anti-dsDNA antibodies, complement C3 and complement C4, cardiolipin antibodies, ESR, CRP, anti-C1q antibodies, and activity on urinary sediment, added to clinical disease activity scales will help in favor of increased immune therapy treatment. However, these biomarkers are often nonspecific and lack the precision to differentiate disease activity from infection. At times serological activity may persist and not reflect adequate treatment response, though biomarker levels may decrease with immune suppression. Nonetheless, the quest for new and reliable biomarkers of lupus disease activity remains a challenge.
Determining lupus disease activity remains complicated as certain organs may respond to treatment while others get worse within the same patient. Serum cytokines, soluble cytokine receptors, markers of endothelial activation, cell markers in plasma cells, among others are informative, yet the interpretation of these markers may require long-term data at a larger scale. To be safe, caution is encouraged with careful use of immune therapy and a balanced approach to control lupus disease activity during infection events.
Reducing immune therapy during antibiotics use, in conjunction with glucocorticoid reduction plans are the primary goal for SLE treatment during an infectious event. Indeed, novel therapeutic trials have examined serious infection and hospitalization related to infection and death. In the systematic review of clinical trials in the treatment of lupus nephritis, high dose of glucocorticoids therapy was associated with increased rate of infections compared to cytotoxic and immune modulatory therapy.6,83
The use of safer immune therapy with lower infectious adverse events such as intravenous immunoglobulin must be prudent given the importance of controlling disease activity. The use of hydroxychloroquine (HCQ) must be universal in lupus patients without compelling contraindications given its association with a decrease in the incidence of infections.
Infection control strategies and prevention of infection guidelines are crucial in SLE patients receiving prednisone higher than 20 mg daily. The rheumatology and infectious disease societys' clinical practice guideline recommendations emphasize the administration of preventive vaccines during low disease activity state and prior to the initiation of cytotoxic immunosuppressive and immune modulatory therapy. Yet, preventive vaccinations are under-utilized in SLE, and improved coverage is crucial. While the importance of preventive vaccinations must be a priority, clear communication, and education of SLE patients about hygiene, substantial risk exposure to infection and awareness of febrile illness characteristics and signs and symptoms of infection are nonetheless critical for preventive approaches.
Despite the safety and efficacy of immunization against common pathogens, controversies remain regarding concerns of inadequate immune response to vaccination in SLE patients. The fear of immunization lingers with matters of de novo development of autoimmune disorder, perceived risk of autoimmune reactions and adjuvant related autoimmune syndrome, exacerbation of lupus flare triggered by the administration of vaccines.84 Educating physicians and skilled counseling of patients about the importance of immunization against pathogens in SLE will improve attitudes towards combating vaccines hesitancy.
While mortality-related infection is a major concern, most SLE patients survive their infections thanks to infection control policies and successful control strategies. Nonetheless, the spread of infectious diseases remains unpredictable, and the emergence of antibiotic-resistance and troubling new viruses are on the rise. Anticipation and measurements of risk factors involved in infectious diseases can be useful to control the exposure of infections in SLE.
The frontier infectious control measures observed during the COVID-19 pandemic have promoted high quality infectious control measures across autoimmune disorders.29,85 The timing of elective procedures vital to patient’s health must be during inactive lupus disease phases and while using low doses of glucocorticoids. To achieve high quality results, multi-disciplinary approaches among rheumatologists and infectious disease teams must optimize screening (hepatitis, tuberculosis, etc), diagnostic practices, and management of infections in lupus. Discussions with patients, caregivers, and care partners about treatment goals are fundamental.
Discussion and Conclusion
Over the last few years, substantial progress has been made with the understanding of lupus pathogenic mechanisms and novel treatment strategies in terms of control of disease activity, and prevention of damage. Yet, infection in SLE is still a major burden globally and in the United States.
Clearly SLE patients are at a substantial risk for infections given the nature of the disease and its related immune dysregulation, but most importantly the use of glucocorticoids, cytotoxic immunosuppressive and immune modulatory therapy. Providers caring for lupus patients must address the challenging task of differentiating infections from lupus flares. Fever in SLE is infectious in origin until proven otherwise, even though fever is an element in the classification criteria for SLE diagnosis.
We propose a framework to overcome challenges in the management of concurrent infections in SLE. Certain biomarkers are recognized to help distinguish infections from flares, including CRP and procalcitonin, but remain insufficient to confirm the diagnosis of infections. Clinical judgement with the use of simple scoring systems that predict infections or lupus disease activity remain useful in the decision-making of clinical care. Avoiding overdiagnosis of lupus flare and lowering the glucocorticoids dose might represent a better approach for dealing with fever in SLE. Nonetheless, research gaps remain.
Robust efforts must identify causal risk factors for infection among SLE patients including patients with low disease activity as well as high disease activity and identify effective screening programs for infections in SLE. Data from novel immune therapies in SLE about risk of infections during clinical trials remain scanty as interruption of biological therapy could be related to toxicity and not to infections. Tight control of disease activity and reduction of glucocorticoid doses must be target goals of low disease activity and clinical remission and aim at tapering or discontinuation of high-risk medications. Prophylactic therapy and screening for salient infections in SLE is a priority prior to the use of biological and immunosuppressive therapy.
From a prevention standpoint, additional research to identify potential agents can reduce infectious risk especially among non-steroid using patients. Precision-based risk and drug screening platforms for lupus patients should classify individuals who would benefit most from entering an infection screening and vaccination program. Further research on the feasibility and efficacy of providing vaccination programs in SLE is valuable.
Advancements in discovery of biomarkers of lupus flares could reduce false positives and overdiagnosis and improve differentiation of infections from lupus flares. Biomarkers that are highly predictive of negative responses to targeted immune therapies are a significant unmet clinical need. This is particularly relevant in the subsets of patients that may experience treatment resistance requiring aggressive and multiple immune suppressive therapies which can encourage exposure to infections and associated infection-related complications. Personalized treatment plans which minimize the risk of infections and ensure the safety of SLE patients must address survival rates, prevention of hospitalization, economic benefits, and enhancement of quality of life.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Arnaud L, Tektonidou MG. Long-term outcomes in systemic lupus erythematosus: trends over time and major contributors. Rheumatology. 2020;59(Suppl Supplement_5):v29–v38. PMID: 33280012; PMCID: PMC7719040. doi:10.1093/rheumatology/keaa382
2. Petri M. Infection in systemic lupus erythematosus. Rheum Dis Clin North Am. 1998;24(2):423–456. PMID: 9606766. doi:10.1016/s0889-857x(05)70016-8
3. Barber MRW, Drenkard C, Falasinnu T, et al. Global epidemiology of systemic lupus erythematosus. Nat Rev Rheumatol. 2021;17(9):515–532. PMID: 34345022; PMCID: PMC8982275. doi:10.1038/s41584-021-00668-1
4. Barber MRW, Clarke AE. Systemic lupus erythematosus and risk of infection. Expert Rev Clin Immunol. 2020;16(5):527–538. PMID: 32478627. doi:10.1080/1744666X.2020.1763793
5. Fanouriakis A, Kostopoulou M, Alunno A, et al. 2019 update of the EULAR recommendations for the management of systemic lupus erythematosus. Ann Rheum Dis. 2019;78(6):736–745. PMID: 30926722. doi:10.1136/annrheumdis-2019-215089
6. Pego-Reigosa JM, Nicholson L, Pooley N, et al. The risk of infections in adult patients with systemic lupus erythematosus: systematic review and meta-analysis. Rheumatology. 2021;60(1):60–72. PMID: 33099651; PMCID: PMC7785308. doi:10.1093/rheumatology/keaa478
7. Danza A, Ruiz-Irastorza G. Infection risk in systemic lupus erythematosus patients: susceptibility factors and preventive strategies. Lupus. 2013;22(12):1286–1294. PMID: 24098001. doi:10.1177/0961203313493032
8. Winebrake J, Khalili L, Weiner J, Gartshteyn Y, Park L, Askanase AD. Rheumatologists’ perspective on hydroxychloroquine guidelines. Lupus Sci Med. 2020;7(1):e000427. PMID: 33148665; PMCID: PMC7640534. doi:10.1136/lupus-2020-000427
9. Loza E, Carmona L, Woolf A, et al. Implementation of recommendations in rheumatic and musculoskeletal diseases: considerations for development and uptake. Ann Rheum Dis. 2022;81(10):1344.
10. Teh CL, Wan SA, Ling GR. Severe infections in systemic lupus erythematosus: disease pattern and predictors of infection-related mortality. Clin Rheumatol. 2018;37(8):2081–2086. PMID: 29667100. doi:10.1007/s10067-018-4102-6
11. Kedves M, Kósa F, Kunovszki P, et al. Large-scale mortality gap between SLE and control population is associated with increased infection-related mortality in lupus. Rheumatology. 2020;59(11):3443–3451. PMID: 32357240; PMCID: PMC7590419. doi:10.1093/rheumatology/keaa188
12. Devlin A, Shmerling RH. Systemic lupus erythematosus and infections. In: Systemic Lupus Erythematosus. Academic Press; 2021:451–459.
13. Wu X-Y, Yang M, Xie Y-S, et al. Causes of death in hospitalized patients with systemic lupus erythematosus: a 10-year multicenter nationwide Chinese cohort. Clin Rheumatol. 2019;38(1):107–115. PMID: 30123930. doi:10.1007/s10067-018-4259-z
14. Walunas TL, Jackson KL, Chung AH, et al. Disease outcomes and care fragmentation among patients with systemic lupus erythematosus. Arthritis Care Res. 2017;69(9):1369–1376. PMID: 27899012; PMCID: PMC5447502. doi:10.1002/acr.23161
15. Feldman CH, Marty FM, Winkelmayer WC, et al. Comparative rates of serious infections among patients with systemic lupus erythematosus receiving immunosuppressive medications. Arthritis Rheumatol. 2017;69(2):387–397. PMID: 27589220; PMCID: PMC5274610. doi:10.1002/art.39849
16. Yu Y, Shen H, Zhu C, Guo R, Gao Y, Lu L. Infections caused by extended-spectrum β-lactamase producing Escherichia Coli in systemic lupus erythematosus patients: prevalence, risk factors, and predictive model. Biomed Res Int. 2018;2018:8296720. PMID: 30581868; PMCID: PMC6276506. doi:10.1155/2018/8296720
17. Luijten RK, Cuppen BV, Bijlsma JW, Derksen RH. Serious infections in systemic lupus erythematosus with a focus on pneumococcal infections. Lupus. 2014;23(14):1512–1516. PMID: 25078055. doi:10.1177/0961203314543918
18. Goldblatt F, Yuste J, Isenberg DA, Rahman A, Brown J. Impaired C3b/iC3b deposition on Streptococcus pneumoniae in serum from patients with systemic lupus erythematosus. Rheumatology. 2009;48(12):1498–1501. PMID: 19797312. doi:10.1093/rheumatology/kep289
19. Kogami M, Abe Y, Shimada Y, et al. Bacteremia in systemic lupus erythematosus: risk factors, clinical and microbiological characteristics, and outcomes in the largest single-center retrospective cohort in Japan. Lupus. 2021;30(14):2292–2297. PMID: 34693822. doi:10.1177/09612033211054395
20. Kim SS, Perino G, Boettner F, Miller A, Goodman S. Salmonella septic arthritis of the knees in a patient with systemic lupus erythematosus. Lupus. 2013;22(7):740–743. PMID: 23753601. doi:10.1177/0961203313491022
21. Suárez-Avellaneda A, Quintana JH, Aragón CC, et al. Systemic lupus erythematosus in the intensive care unit: a systematic review. Lupus. 2020;29(11):1364–1376. PMID: 32723062. doi:10.1177/0961203320941941
22. Balbi GGM, Machado-Ribeiro F, Marques CDL, Signorelli F, Levy RA. The interplay between tuberculosis and systemic lupus erythematosus. Curr Opin Rheumatol. 2018;30(4):395–402. PMID: 29438163. doi:10.1097/BOR.0000000000000493
23. Chasset F, Richez C, Martin T, Belot A, Korganow AS, Arnaud L. Rare diseases that mimic Systemic lupus erythematosus (Lupus mimickers). Joint Bone Spine. 2019;86(2):165–171. PMID: 30837156. doi:10.1016/j.jbspin.2018.10.007
24. Machado Ribeiro F, Goldenberg T. Mycobacteria and autoimmunity. Lupus. 2015;24(4–5):374–381. PMID: 25801880. doi:10.1177/0961203314559634
25. Yang SC, Lai YY, Huang MC, Tsai CS, Wang JL. Corticosteroid dose and the risk of opportunistic infection in a national systemic lupus erythematosus cohort. Lupus. 2018;27(11):1819–1827. PMID: 30103646. doi:10.1177/0961203318792352
26. Quaglia M, Merlotti G, De Andrea M, Borgogna C, Cantaluppi V. Viral infections and systemic lupus erythematosus: new players in an old story. Viruses. 2021;13(2):277. PMID: 33670195; PMCID: PMC7916951. doi:10.3390/v13020277
27. Chen D, Li H, Xie J, Zhan Z, Liang L, Yang X. Herpes zoster in patients with systemic lupus erythematosus: clinical features, complications and risk factors. Exp Ther Med. 2017;14(6):6222–6228. doi:10.3892/etm.2017.5297
28. Wang S, Chen Y, Xu X, Hu W, Shen H, Chen J. Prevalence of hepatitis B virus and hepatitis C virus infection in patients with systemic lupus erythematosus: a systematic review and meta-analysis. Oncotarget. 2017;8(60):102437–102445. PMID: 29254259; PMCID: PMC5731969. doi:10.18632/oncotarget.22261
29. Fernandez-Ruiz R, Paredes JL, Niewold TB. COVID-19 in patients with systemic lupus erythematosus: lessons learned from the inflammatory disease. Transl Res. 2021;232:13–36. PMID: 33352298; PMCID: PMC7749645. doi:10.1016/j.trsl.2020.12.007
30. Kwan A, Rayes HA, Lazova T, et al. Herpes zoster in SLE: prevalence, incidence and risk factors. Lupus Sci Med. 2022;9(1):e000574. PMID: 35017186; PMCID: PMC8753438. doi:10.1136/lupus-2021-000574
31. Rondaan C, van Leer CC, Van assen S, et al. Longitudinal analysis of varicella-zoster virus-specific antibodies in systemic lupus erythematosus: no association with subclinical viral reactivations or lupus disease activity. Lupus. 2018;27(8):1271–1278. PMID: 29667858; PMCID: PMC6027773. doi:10.1177/0961203318770535
32. Bruminhent J, Autto S, Rotjanapan P, et al. A prospective study of cytomegalovirus-specific cell-mediated immune monitoring and cytomegalovirus infection in patients with active systemic lupus erythematosus receiving immunosuppressants. Open Forum Infect Dis. 2021;8(6):ofab248. PMID: 34189173; PMCID: PMC8231397. doi:10.1093/ofid/ofab248
33. Gugliesi F, Pasquero S, Griffante G, et al. Human cytomegalovirus and autoimmune diseases: where are we? Viruses. 2021;13(2):260. PMID: 33567734; PMCID: PMC7914970. doi:10.3390/v13020260
34. Méndez-Martínez S, García-Carrasco M, Jiménez-Herrera EA, et al. Factors of the epidemiological triad that influence the persistence of human papilloma virus infection in women with systemic lupus erythematosus. Lupus. 2018;27(9):1542–1546. PMID: 29732937. doi:10.1177/0961203318773176
35. Cacoub P, Comarmond C, Domont F, Savey L, Desbois AC, Saadoun D. Extrahepatic manifestations of chronic hepatitis C virus infection. Ther Adv Infect Dis. 2016;3(1):3–14. PMID: 26862398; PMCID: PMC4735500. doi:10.1177/2049936115585942
36. Illescas‐Montes R, Corona‐Castro CC, Melguizo‐Rodríguez L, Ruiz C, Costela‐Ruiz VJ. Infectious processes and systemic lupus erythematosus. Immunology. 2019;158(3):153–160.
37. James JA, Robertson JM. Lupus and epstein-barr. Curr Opin Rheumatol. 2012;24(4):383–388. PMID: 22504579; PMCID: PMC3562348. doi:10.1097/BOR.0b013e3283535801
38. Fu XL, Qian Y, Jin XH, et al. COVID-19 in patients with systemic lupus erythematosus: a systematic review. Lupus. 2022;31(6):684–696. PMID: 35382637; PMCID: PMC8990101. doi:10.1177/09612033221093502
39. Mehta P, Gasparyan AY, Zimba O, Kitas GD. Systemic lupus erythematosus in the light of the COVID-19 pandemic: infection, vaccination, and impact on disease management. Clin Rheumatol. 2022;41(9):2893–2910. PMID: 35639259; PMCID: PMC9152659. doi:10.1007/s10067-022-06227-7
40. Hsu CY, Ko CH, Wang JL, Hsu TC, Lin CY. Comparing the burdens of opportunistic infections among patients with systemic rheumatic diseases: a nationally representative cohort study. Arthritis Res Ther. 2019;21(1):211. PMID: 31604447; PMCID: PMC6790041. doi:10.1186/s13075-019-1997-5
41. Fang W, Chen M, Liu J, et al. Cryptococcal meningitis in systemic lupus erythematosus patients: pooled analysis and systematic review. Emerg Microbes Infect. 2016;5(9):e95. PMID: 27599471; PMCID: PMC5113055. doi:10.1038/emi.2016.93
42. Su CF, Lai CC, Li TH, et al. Epidemiology and risk of invasive fungal infections in systemic lupus erythematosus: a nationwide population-based cohort study. Ther Adv Musculoskelet Dis. 2021;13:1759720X211058502. PMID: 34840609; PMCID: PMC8613894. doi:10.1177/1759720X211058502
43. Carli L, Tani C, Vagnani S, Signorini V, Mosca M. Leukopenia, lymphopenia, and neutropenia in systemic lupus erythematosus: prevalence and clinical impact--A systematic literature review. Semin Arthritis Rheum. 2015;45(2):190–194. PMID: 26170228. doi:10.1016/j.semarthrit.2015.05.009
44. Singh BK, Singh S. Systemic lupus erythematosus and infections. Reumatismo. 2020;72(3):154–169. PMID: 33213128. doi:10.4081/reumatismo.2020.1303
45. Almaghlouth I, Johnson SR, Pullenayegum E, Gladman D, Urowitz M. Immunoglobulin levels in systemic lupus erythematosus: a narrative review. Lupus. 2021;30(6):867–875. PMID: 33779380. doi:10.1177/09612033211004714
46. Yuan Q, Xing X, Lu Z, Li X. Clinical characteristics and risk factors of infection in patients with systemic lupus erythematosus: a systematic review and meta-analysis of observational studies. Semin Arthritis Rheum. 2020;50(5):1022–1039. PMID: 32911280. doi:10.1016/j.semarthrit.2020.06.004
47. Pimentel-Quiroz VR, Ugarte-Gil MF, Harvey GB, et al. Factors predictive of serious infections over time in systemic lupus erythematosus patients: data from a multi-ethnic, multi-national, Latin American lupus cohort. Lupus. 2019;28(9):1101–1110. PMID: 31291843. doi:10.1177/0961203319860579
48. Mok CC. Herpes zoster vaccination in systemic lupus erythematosus: the current status. Hum Vaccin Immunother. 2019;15(1):45–48. PMID: 30130445; PMCID: PMC6363132. doi:10.1080/21645515.2018.1514228
49. Prata AR, Luís M, Assunção H, da Silva JAP. Inês LS. Antimalarial treatment and minimizing prednisolone are associated with lower risk of infection in SLE: a 24-month prospective cohort study. Clin Rheumatol. 2022;41(4):1069–1078. PMID: 34782940. doi:10.1007/s10067-021-05988-x
50. Steiger S, Ehreiser L, Anders J, Anders HJ. Biological drugs for systemic lupus erythematosus or active lupus nephritis and rates of infectious complications. Evidence from large clinical trials. Front Immunol. 2022;13:999704. PMID: 36211360; PMCID: PMC9538665. doi:10.3389/fimmu.2022.999704
51. Davis JS, Ferreira D, Paige E, Gedye C, Boyle M. Infectious complications of biological and small molecule targeted immunomodulatory therapies. Clin Microbiol Rev. 2020;33(3):e00035–19. PMID: 32522746; PMCID: PMC7289788. doi:10.1128/CMR.00035-19
52. Pan Q, Liu Z, Liao S, et al. Current mechanistic insights into the role of infection in systemic lupus erythematosus. Biomed Pharmacother. 2019;117:109122. doi:10.1016/j.biopha.2019.109122
53. Afrasiabi A, Keane JT, Ong LTC, et al. Genetic and transcriptomic analyses support a switch to lytic phase in Epstein Barr virus infection as an important driver in developing systemic lupus erythematosus. J Autoimmun. 2022;127:102781. PMID: 34952359. doi:10.1016/j.jaut.2021.102781
54. Iwata S, Tanaka Y. Association of viral infection with the development and pathogenesis of systemic lupus erythematosus. Front Med. 2022;9:849120. PMID: 35280878; PMCID: PMC8914279. doi:10.3389/fmed.2022.849120
55. Rigante D, Mazzoni MB, Esposito S. The cryptic interplay between systemic lupus erythematosus and infections. Autoimmun Rev. 2014;13(2):96–102. PMID: 24051103. doi:10.1016/j.autrev.2013.09.004
56. Dizon BLP, Pierce SK. The tangled web of autoreactive B cells in malaria immunity and autoimmune disease. Trends Parasitol. 2022;38(5):379–389. PMID: 35120815; PMCID: PMC9012675. doi:10.1016/j.pt.2022.01.005
57. Sagy I, Zeller L, Raviv Y, Porges T, Bieber A, Abu-Shakra M. New-onset systemic lupus erythematosus following BNT162b2 mRNA COVID-19 vaccine: a case series and literature review. Rheumatol Int. 2022;42(12):2261–2266. PMID: 36098769; PMCID: PMC9468534. doi:10.1007/s00296-022-05203-3
58. He N, Leng X, Zeng X. Systemic lupus erythematosus following human papillomavirus vaccination: a case-based review. Int J Rheum Dis. 2022;25(10):1208–1212. PMID: 35948863. doi:10.1111/1756-185X.14404
59. Infante V, Miyaji KT, Soarez PC, Sartori AMC. Systematic review and meta-analysis of HPV vaccination in women with systemic lupus erythematosus (SLE). Expert Rev Vaccines. 2021;20(3):309–318. PMID: 33573404. doi:10.1080/14760584.2021.1889375
60. Fernandez D, Kirou KA. What causes lupus flares? Curr Rheumatol Rep. 2016;18(3):14. PMID: 26951252. doi:10.1007/s11926-016-0562-3
61. Joo YB, Lim YH, Kim KJ, Park KS, Park YJ. Association of influenza infection with hospitalisation-related systemic lupus erythematosus flares: a time series analysis. Clin Exp Rheumatol. 2021;39(5):1056–1062. PMID: 33124567. doi:10.55563/clinexprheumatol/fmkp4b
62. Ospina FE, Echeverri A, Zambrano D, et al. Distinguishing infections vs flares in patients with systemic lupus erythematosus. Rheumatology. 2017;56(suppl_1):i46–i54. PMID: 27744359. doi:10.1093/rheumatology/kew340
63. Beça S, Rodríguez-Pintó I, Alba MA, Cervera R, Espinosa G. Development and validation of a risk calculator to differentiate flares from infections in systemic lupus erythematosus patients with fever. Autoimmun Rev. 2015;14(7):586–593. PMID: 25703012.s. doi:10.1016/j.autrev.2015.02.005
64. Singhal A, Kumar S. Neutrophil and remnant clearance in immunity and inflammation. Immunology. 2022;165(1):22–43. PMID: 34704249. doi:10.1111/imm.13423
65. Enocsson H, Gullstrand B, Eloranta ML, et al. C-reactive protein levels in systemic lupus erythematosus are modulated by the interferon gene signature and CRP gene polymorphism rs1205. Front Immunol. 2021;11:622326. PMID: 33584722; PMCID: PMC7876312. doi:10.3389/fimmu.2020.622326
66. El-Serougy E, Zayed HS, Ibrahim NM, Maged LA. Procalcitonin and C-reactive protein as markers of infection in systemic lupus erythematosus: the controversy continues. Lupus. 2019;28(11):1329–1336. PMID: 29779437. doi:10.1177/0961203318777101
67. He S, Tang C, Yu J, et al. Combining C reactive protein and serum albumin to predict 90-day mortality in systemic lupus erythematosus with serious community-acquired infections. Lupus Sci Med. 2021;8(1):e000505. PMID: 34253648; PMCID: PMC8276300. doi:10.1136/lupus-2021-000505
68. Chen Y, Shen J, Yang H, Xu S, Ma Y, Pan F. Serum procalcitonin and C-reactive protein levels as diagnostic markers for distinguishing bacterial infections from lupus flares in systemic lupus erythematosus: a systematic review and meta-analysis. Int Immunopharmacol. 2021;101(Pt B):108304. PMID: 34731783. doi:10.1016/j.intimp.2021.108304
69. Yuan ZC, Xu WD, Lan YY, et al. Association of MBL2 gene polymorphisms and systemic lupus erythematosus susceptibility: a meta-analysis. Int J Rheum Dis. 2021;24(2):147–158. PMID: 33146461. doi:10.1111/1756-185X.14017
70. Feng M, Zhang SL, Liang ZJ, et al. Peripheral neutrophil CD64 index combined with complement, CRP, WBC count and B cells improves the ability of diagnosing bacterial infection in SLE. Lupus. 2019;28(3):304–316. PMID: 30712491. doi:10.1177/0961203319827646
71. Wang H. Regulation of HMGB1 release in health and diseases. Cells. 2022;12(1):46. PMID: 36611839; PMCID: PMC9818800. doi:10.3390/cells12010046
72. Ghosh A, Shao L, Sampath P, et al. Oligoadenylate-synthetase-family protein OASL inhibits activity of the DNA sensor cGAS during DNA virus infection to limit interferon production. Immunity. 2019;50(1):51–63.e5. PMID: 30635239; PMCID: PMC6342484. doi:10.1016/j.immuni.2018.12.013
73. Ajmani S, Singh H, Chaturvedi S, et al. Utility of neutrophil CD64 and serum TREM-1 in distinguishing bacterial infection from disease flare in SLE and ANCA-associated vasculitis. Clin Rheumatol. 2019;38(4):997–1005. PMID: 30446886. doi:10.1007/s10067-018-4334-5
74. Stefanski AL, Dörner T. Immune checkpoints and the multiple faces of B cells in systemic lupus erythematosus. Curr Opin Rheumatol. 2021;33(6):592–597. PMID: 34402453. doi:10.1097/BOR.0000000000000825
75. Hirohata S, Kikuchi H. Role of serum IL-6 in neuropsychiatric systemic lupus erythematosus. ACR Open Rheumatol. 2021;3(1):42–49. PMID: 33393227; PMCID: PMC7811696. doi:10.1002/acr2.11217
76. Greenan-Barrett J, Doolan G, Shah D, et al. Biomarkers associated with organ-specific involvement in juvenile systemic lupus erythematosus. Int J Mol Sci. 2021;22(14):7619. PMID: 34299237; PMCID: PMC8306911. doi:10.3390/ijms22147619
77. Aragón CC, Ruiz-Ordoñez I, Quintana JH, et al. Clinical characterization, outcomes, and prognosis in patients with systemic lupus erythematosus admitted to the intensive care unit. Lupus. 2020;29(9):1133–1139. PMID: 32605526. doi:10.1177/0961203320935176
78. Mehta P, Singh K, Anand S, et al. Differentiating flare and infection in febrile lupus patients: derivation and validation of a calculator for resource constrained settings. Lupus. 2022;31(10):1254–1262. PMID: 35786213. doi:10.1177/09612033221112066
79. Takeuchi M, Dahabreh IJ, Nihashi T, Iwata M, Varghese GM, Terasawa T. Nuclear imaging for classic fever of unknown origin: meta-analysis. J Nucl Med. 2016;57(12):1913–1919. PMID: 27339873. doi:10.2967/jnumed.116.174391
80. Bolouri N, Akhtari M, Farhadi E, et al. Role of the innate and adaptive immune responses in the pathogenesis of systemic lupus erythematosus. Inflamm Res. 2022;71(5–6):537–554. PMID: 35298669. doi:10.1007/s00011-022-01554-6
81. Ugarte-Gil MF, González LA, Alarcón GS. Lupus: the new epidemic. Lupus. 2019;28(9):1031–1050. PMID: 31299878. doi:10.1177/0961203319860907
82. Mikdashi J, Nived O. Measuring disease activity in adults with systemic lupus erythematosus: the challenges of administrative burden and responsiveness to patient concerns in clinical research. Arthritis Res Ther. 2015;17(1):183. PMID: 26189728; PMCID: PMC4507322. doi:10.1186/s13075-015-0702-6
83. Thong KM, Chan TM. Infectious complications in lupus nephritis treatment: a systematic review and meta-analysis. Lupus. 2019;28(3):334–346. PMID: 30744523. doi:10.1177/0961203319829817
84. Zavala-Flores E, Salcedo-Matienzo J, Quiroz-Alva A, Berrocal-Kasay A. Side effects and flares risk after SARS-CoV-2 vaccination in patients with systemic lupus erythematosus. Clin Rheumatol. 2022;41(5):1349–1357. PMID: 34782941; PMCID: PMC8592807. doi:10.1007/s10067-021-05980-5
85. Aringer M, Alarcón-Riquelme ME, Clowse M, Pons-Estel GJ, Vital EM, Dall’Era M. A glimpse into the future of systemic lupus erythematosus. Ther Adv Musculoskelet Dis. 2022;14:1759720X221086719. PMID: 35368371; PMCID: PMC8972918. doi:10.1177/1759720X221086719
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.