Back to Journals » Neuropsychiatric Disease and Treatment » Volume 18
A Feasibility Study of Patients with Major Depression and Substance Use Disorders: Vortioxetine as Maintenance Treatment
Authors Basurte-Villamor I ![]() , Vega P
, Vega P ![]() , Roncero C
, Roncero C ![]() , Martínez-Raga J, Grau-López L, Aguilar L, Torrens M, Szerman N
, Martínez-Raga J, Grau-López L, Aguilar L, Torrens M, Szerman N ![]()
Received 17 January 2022
Accepted for publication 13 April 2022
Published 4 May 2022 Volume 2022:18 Pages 965—976
DOI https://doi.org/10.2147/NDT.S358782
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Roger Pinder
Ignacio Basurte-Villamor,1 Pablo Vega,2 Carlos Roncero,3– 5 José Martínez-Raga,6 Lara Grau-López,7– 10 Lourdes Aguilar,3– 5 Marta Torrens,11 Nestor Szerman12
1Department of Psychiatry and Behavioral Health, Clínica López Ibor, Madrid, Spain; 2Institute for Addictions, Madrid Salud, Madrid City Council, Madrid, Spain; 3Department of Psychiatry, University of Salamanca Healthcare Complex, Salamanca, Spain; 4Institute of Biomedicine of Salamanca, University of Salamanca, Salamanca, Spain; 5Psychiatric Unit, School of Medicine, University of Salamanca, Salamanca, Spain; 6Department of Psychiatry and Clinical Psychology, University Hospital Dr. Peset and University of Valencia, Valencia, Spain; 7Department of Psychiatry, Hospital Universitari Vall d’Hebron, Barcelona, Spain; 8Biomedical Network Research Centre on Mental Health, CIBERSAM, Barcelona, Spain; 9Group of Psychiatry, Mental Health and Addiction, Vall d’Hebron Research Institute, Barcelona, Spain; 10Department of Psychiatry and Forensic Medicine, Universitat Autònoma de Barcelona, Barcelona, Spain; 11Institute of Neuropsychiatry & Addictions-Hospital del Mar, Barcelona IMIM, Hospital del Mar Medical Research Institute, Barcelona University Autònoma, Barcelona, Spain; 12WADD WPA Section Dual Disorders, Mental Health and Psychiatric Institute, Gregorio Marañon University Hospital, Madrid, Spain
Correspondence: Nestor Szerman, WADD WPA Section Dual Disorders, Mental Health and Psychiatric Institute, Gregorio Marañon University Hospital, C/ Lope de Rueda 43, Madrid, 28009, Spain, Tel +34 914008690, Fax +34 915739932, Email [email protected]
Background: Limited studies have evaluated the effectiveness of vortioxetine in real-world settings, and none of them has involved patients with dual depression (major depressive disorder [MDD] and substance use disorder [SUD]). The objective of the study was to describe the effectiveness of vortioxetine in clinical practice and determine its effect on affective symptoms, cognitive function, quality of life, and substance use in patients with MDD and SUD.
Methods: Post-authorization, retrospective, multicenter, descriptive, and observational study in 80 patients with MDD and SUD receiving a maintenance treatment with vortioxetine for six months between January 2017 and April 2021.
Results: Compared with baseline, scores significantly decreased after 3 and 6 months of treatment in the Montgomery-Åsberg Depression Rating Scale total (from 28.9 to 17.7 and 12.0), and global functional impairment of the Sheehan Disability Inventory (from 26.3 to 19.1 and 16.7). The number of correct answers in the symbol digit modalities test significantly improved during vortioxetine treatment (from 40.4 to 43.8 and 48.4). Regarding the clinical global impression scale, the score for disease severity significantly decreased from 3.8 to 3.0 and 2.4. Compared with baseline, there was a significant reduction in consumption of practically all substances, especially of alcohol, cannabis, and cocaine.
Conclusion: Vortioxetine was effective in clinical practice for alleviating depressive symptoms and functional impairment, and in improving cognitive and executive functions and disease severity in patients with MDD and SUD. Moreover, the treatment with vortioxetine favored a reduction in substance use and the severity of the SUDs.
Keywords: vortioxetine, major depressive disorder, substance use disorder, dual disorder, major dual depressive disorder, real-world evidence
Introduction
Major depressive disorder (MDD) is a common illness and one of the leading causes of burden of disease and disability-adjusted life years worldwide due to its devastating impact on individuals, families, and society.1 According to the World Health Organization (WHO), depression affects more than 264 million people worldwide.2 From a clinical neuroscience and transdiagnostic perspective (beyond DSM-5), depression is considered a brain disorder affecting emotional regulation which is also involved in symptoms of substance use, eating, anxiety, and borderline personality disorders.3 Depressed patients present concurrent addictive disorders, such as substance use disorders (SUD) or behavioral addictions (like gambling disorder);4 leading to a clinical condition called as dual depression, consisting of depression with concurrent SUD.5 Indeed, approximately one third of patients with MDD have a SUD.6 A systematic review and meta-analysis with data from epidemiological surveys between 1990 and 2014 revealed significant associations between MDD and SUDs, especially with illicit drugs and alcohol.7 Patients with dual depression show unique clinical characteristics, including more cognitive symptoms, a lower treatment adherence, a higher number of suicide attempts6,8 than those with no dual disorders, in addition to being more refractory to conventional therapies. Given the phenotypic heterogeneity in MDD, supported by several genetic and neurobiological studies that state that these conditions are not discrete categories but part of a continuum or affective disorder spectrum, the treatment approach based on a single therapy is changing toward a personalized treatment.5,9 From a neuroscience perspective, it currently seems clear that there are many phenotypes of depression and many antidepressants with different mechanisms of action. When treating a patient with dual depression, knowing whether all antidepressants are equally effective is imperative. Dual depression seems to be a different phenotype needing a new approach. Antidepressant drugs, mainly selective serotonin (5-HT) reuptake inhibitors (SSRIs), are the primary psychopharmacological treatment for patients with MDD. However, several systematic reviews and meta-analyses have demonstrated that SSRIs, with a unimodal mechanism of action, are not effective for these patients.10,11 Limited response to the standard treatment for dual depression increases suffering and risk of suicide.
Thus, new psychopharmacological treatments are needed to treat dual depression.12 In this sense, the emergence of drugs with a multimodal mechanism of action should be considered as a therapeutic option.13 Vortioxetine is a multimodal antidepressant drug that received approval in 2013 for the treatment of MDD by both the US Food and Drug Administration and European Medicines Agency.14 In vitro studies have revealed that vortioxetine functions as a 5-HT1A receptor agonist, a 5-HT3, 5-HT7, and 5-HT1D receptor antagonist, a 5-HT1B receptor partial agonist, and an inhibitor of the serotonin transporter.15,16 Various short- and long-term randomized clinical trials have also evidenced the superior therapeutic benefit of vortioxetine over placebo in the treatment of depressive and cognitive symptoms in MDD patients. Moreover, vortioxetine has demonstrated efficacy in patients with inadequate response to SSRIs or serotonin-noradrenaline reuptake inhibitors (SNRI).17 To our knowledge, limited studies have evaluated the effectiveness of vortioxetine in real-world settings,18–20 and only one has involved patients with MDD and substance use disorder (SUD).21 Therefore, the objective of the present study was to describe the effectiveness of vortioxetine in routine clinical practice and determine its effect on affective symptoms, cognitive function, quality of life, and substance use in patients with MDD and SUDs.
Materials and Methods
Study Design
This post-authorization, retrospective, multicenter, descriptive, and observational study included consecutive patients with MDD and SUD receiving a maintenance treatment with vortioxetine for six months between January 2017 and April 2021. The maintenance protocol consisted of a program in which patients were evaluated on a rolling basis and based on a series of objective validated tests, all of which were part of the present study. In the day the patient was included in the study, a cross-evaluation was performed. Patients from a total of six Spanish healthcare centers were included in this study: Hospital General Universitario Gregorio Marañón, Hospital Universitario Vall d’Hebron, Hospital Universitario Dr. Peset de Valencia, CAD Instituto de Adicciones de Madrid, Institute of Neuropsychiatry & Addictions-Parc de Salut Mar de Barcelona and Complejo Asistencial Universitario de Salamanca. Although some of them are general hospitals, all patients were treated in tertiary specialist centres. Inclusion criteria were: males and females aged between 18 and 65 years; with a diagnosis of MDD, according to DMS-5 criteria;22 receiving maintenance treatment with vortioxetine in the previous six months; and patients with SUD who had complied with the clinical practice protocol for patients with MDD within six months before study inclusion. Pregnant or lactating women and patients with concomitant diseases that may interfere with the evaluation of the analyzed parameters were excluded. A total of six Spanish sites participated in the study. All procedures were in accordance with routine clinical practice and all participants provided informed consent in accordance with the Declaration of Helsinki. The study was approved by the Ethics Committee of the Gregorio Marañon University Hospital (Madrid, Spain).
Endpoints and Variables
The primary endpoint was the description of vortioxetine effectiveness at three time points (baseline and three and six months after starting vortioxetine treatment) using the Spanish version of the Montgomery-Åsberg Depression Rating Scale (MADRS), the Sheehan Disability Inventory (SDI), the symbol digit modalities test (SDMT), and the clinical global impression (CGI) scale. The MADRS is a 10-item scale used to assess symptom severity in MDD.23 Each item is rated on a Likert scale that ranges from 0 (absence of depression) to 6 (maximum depression score).24 This scale establishes the following cut-off points in a 0–60 range: absence of depression (0–6), mild depression (7–19), moderate depression (20–34) and severe depression (35–60). The SDI is a 5-item scale for assessing functional impairment in three domains, including work/school, social life, and family life, perceived stress, and social support.25 Except for social support, items are scored on a 10-point visual analogue scale arranged in the absence (0), mild (1–3), moderate (4–6), marked (7–9) and extreme (10) impairment subgroups. Social support item is represented as a percentage. The SDMT is an instrument to measure information processing speed, and to detect cognitive impairment.26 A row of nine boxes filled with different symbols was presented to the participants. Above the row, a symbol digit key, pairing the nine symbols with a number from 1 to 9, is shown. A total of 110 items were presented. By using the symbol digit key, participants were asked to match each symbol in the bottom row with a number as quick as possible. An initial practical task of ten items was performed. The obtained score, with a maximum of 110 points, corresponds to the total number of substitutions in a 90-second interval.27 The CGI scale is used to evaluate disease pattern severity, which is composed of two subscales: severity of disease, and global improvement.28 Higher scores are indicative of a higher disease severity. Secondary endpoints included the description of the sociodemographic and clinical characteristics of patients with MDD and SUD, and the changes in SUDs during vortioxetine treatment. To diagnose SUD, for each patient both past and actual history of consumption, the consumption starting age, last consumption, and an estimation of severity, if needed, were evaluated for substances such as alcohol, caffeine-related products, cannabis, hallucinogens, inhalants, opioids, sedatives, hypnotics, anxiolytics, stimulants, tobacco and other substances. Changes in the severity of SUDs were assessed using the Spanish version of the 5-item severity of dependence scale, where each item is rated on a 0–4 Likert scale.29 Higher scores are representative of greater severities. Relapsing patients were diagnosed according to the DSM-5 criteria.
Statistical Analysis
Continuous variables are expressed as mean, standard deviation (SD), 95% confidence interval (CI95%), or range (minimum and maximum values); whereas categorical ones were represented as absolute and relative frequencies. Comparisons of variables between time points (3- and 6-month of vortioxetine treatment) versus baseline were carried out using the t-test or Wilcoxon test, when appropriate. Statistical significance was established at p≤0.05. All statistical procedures were performed using SAS v14.0. Accepting an alpha risk of 0.05 and a bilateral contrast of 90%, 78 subjects were needed to detect a difference equal or higher than 10 units. A standard deviation and withdrawn rate of 2530 and 15% were assumed respectively.
Results
Study Population
A total of 80 patients were consecutively recruited for the study. None of them was excluded from analyses. Sociodemographic and clinical characteristics of patients are shown in Table 1. They were predominantly males (63.8%, n=51), with a mean age of 45.1 years (SD: 13.8). Most of them had never been married (36.3%, n=29), had primary education (40.0%, n=32), and were unemployed (40.1%, n=32). Half of the sample (51.3%, n=41) had at least one medical comorbidity, most commonly hypertension (16.3% of patients, n=13), obesity (10.0%, n=8), or human immunodeficiency virus infection (8.8%, n=7). The majority of patients experienced recurrent episodes of MDD (81.3%, n=65), mainly of moderate severity. The SUDs were mainly due to alcohol and tobacco use (66.3% [n=53] and 40.0% [n=32] of patients, respectively). The mean dose of vortioxetine was 13.8 mg/day (range: 5–20). At baseline, most of the patients (91.3%, n=73) were receiving another psychopharmacological treatment, mainly antipsychotics (37.5%, n=30), benzodiazepines (36.3%, n=29), anticonvulsants (36.3%, n=29), or other antidepressants (31.3%, n=25; Table 2). In addition, 77.5% of patients (n=62) were receiving non-pharmacological therapy, especially individual psychotherapy (58.1%, n=36). Psychopharmacological and non-pharmacological treatments remained constant at the third and sixth month of follow-up. A total of four patients at baseline (5.0%), one patient after three months (1.3%), and three patients after six months of vortioxetine treatment (3.8%) required inpatient admissions (by symptomatic decompensation, either affective or relapse of the SUD).
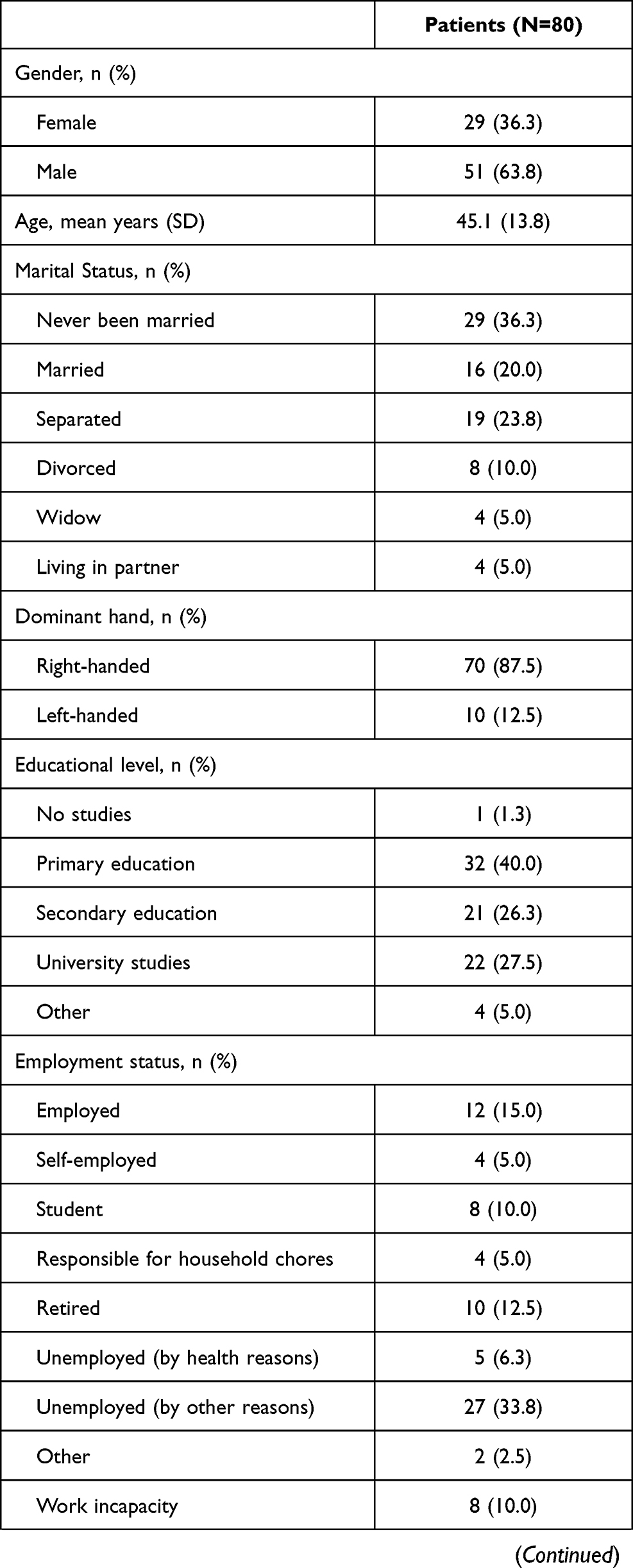 | 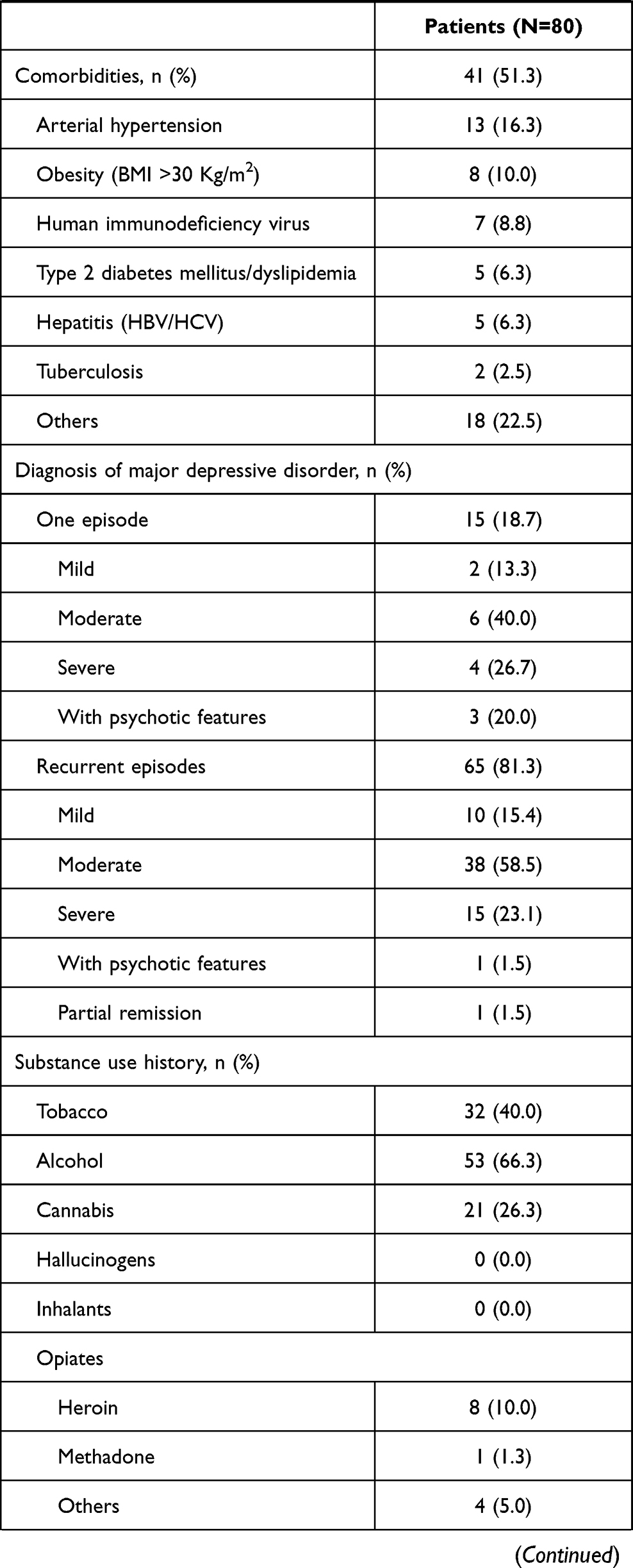 | 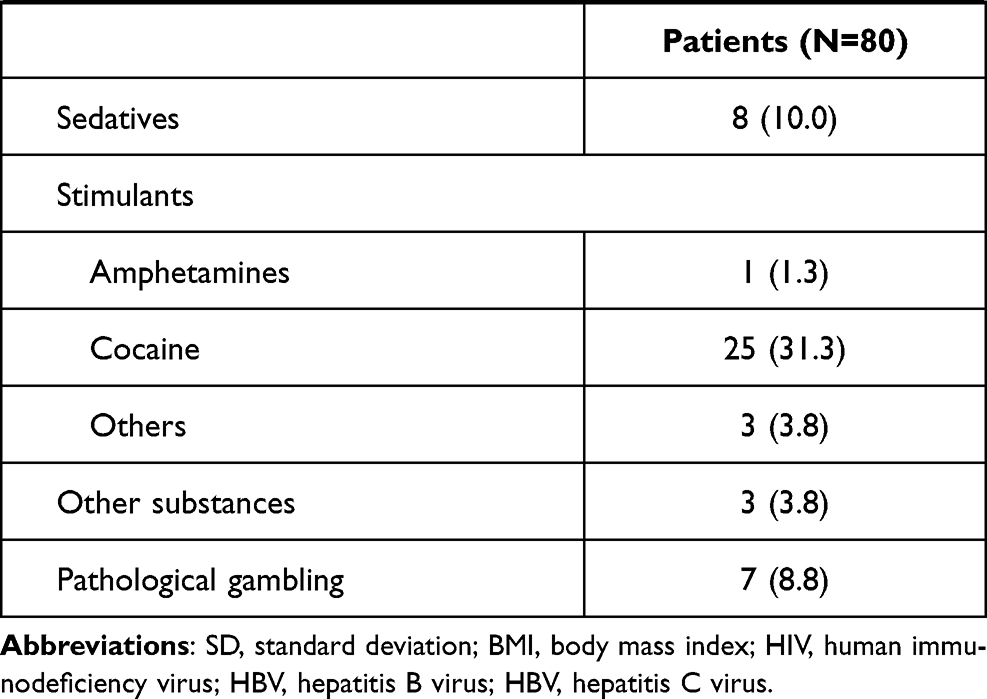 |
Table 1 Sociodemographic and Clinical Characteristics of Patients |
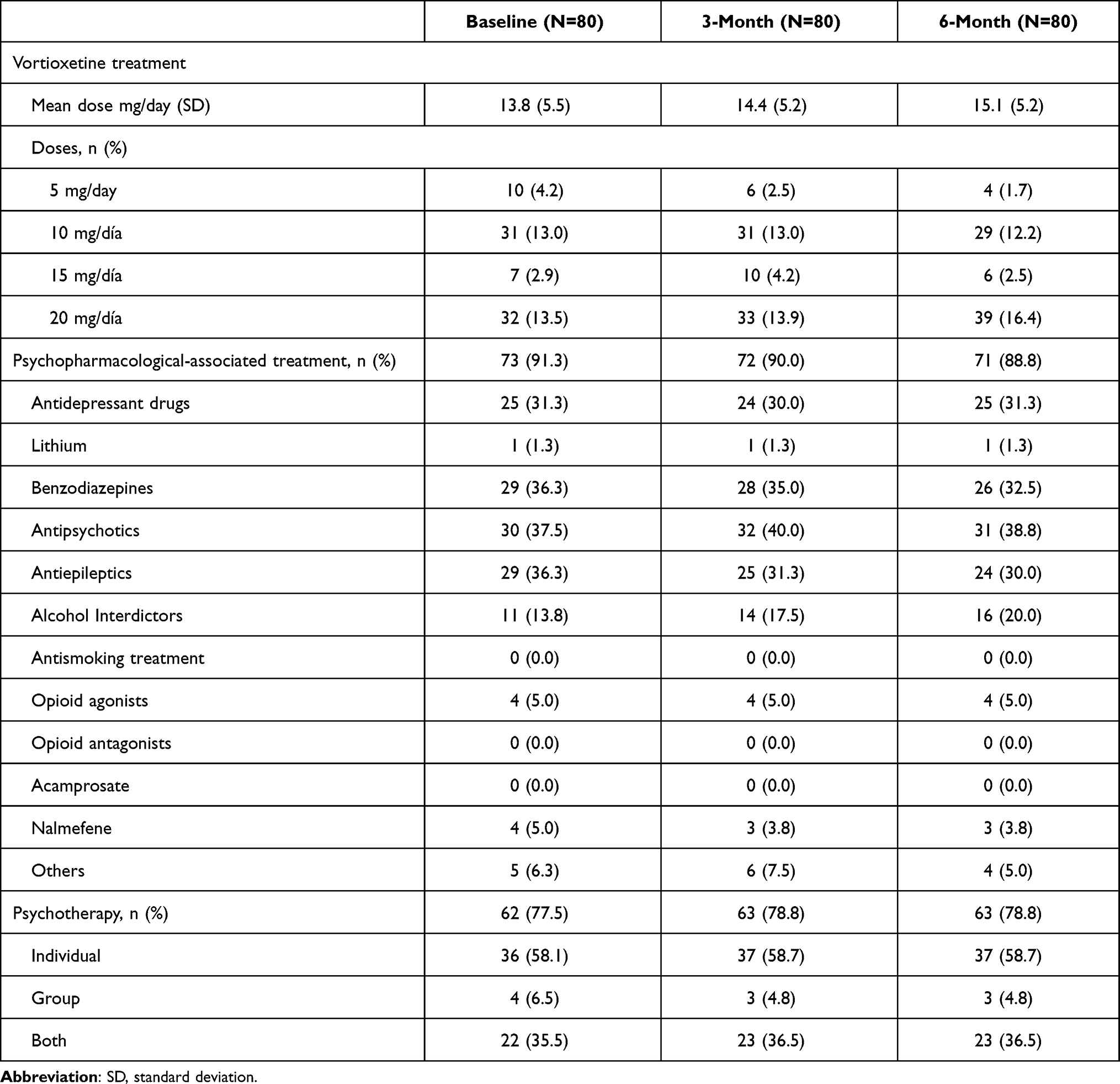 |
Table 2 Features of Treatments During Vortioxetine Treatment |
In addition, this improvement in the different scales was not dependent of the number of SUD associated to each patient, with no significant differences between patients with a single and several SUDs were observed at every time point (Supplementary Table 1). Finally, the improvement in the scores reported for every scale was also independent of the administered initial vortioxetine dose, since no differences were observed between the different doses at both three and six months. The only exception was observed in the SDMT scale for the 15 mg vortioxetine dose at six months, probably due to the lack of a higher available n (Supplementary Table 2).
Effect of the Vortioxetine Treatment
Total score in MADRS significantly decreased from baseline (mean: 28.9; 95% CI: 26.1–31.7) to the 3-month (mean: 17.7; 95% CI: 15.7–19.7; p<0.001), and the 6-month assessments (mean: 12.0; 95% CI: 10.2–13.9; p<0.001; Figure 1). Similarly, scores from all dimensions of MADRS significantly reduced after 3 and 6 months, compared with baseline (Supplementary Table 3). The score from the global functional impairment of the SDI scale also significantly declined between baseline (mean: 26.3; 95% CI: 24.2–28.5), 3-month (mean: 19.1; 95% CI: 17.0–21.1; p<0.001), and 6-month treatment (mean: 16.7; 95% CI: 14.6–18.7; p<0.001). Scores of all domains of SDI scale were significantly lower at the 3- and 6-month treatment than baseline. The number of correct answers in the SDMT significantly improved from baseline (mean: 40.4; 95% CI: 37.8–42.9) to the third (mean: 43.8; 95% CI: 41.5–46.1; p<0.001), and sixth months (mean: 48.4; 95% CI: 45.6–51.2; p<0.001; Figure 1). Regarding CGI, the score for disease severity significantly decreased from baseline (mean: 3.8; 95% CI: 3.6–4.0), to the 3-month (mean: 3.0; 95% CI: 2.8–3.2; p<0.001), and 6-month treatment (mean: 2.4; 95% CI: 2.1–2.7; p<0.001).
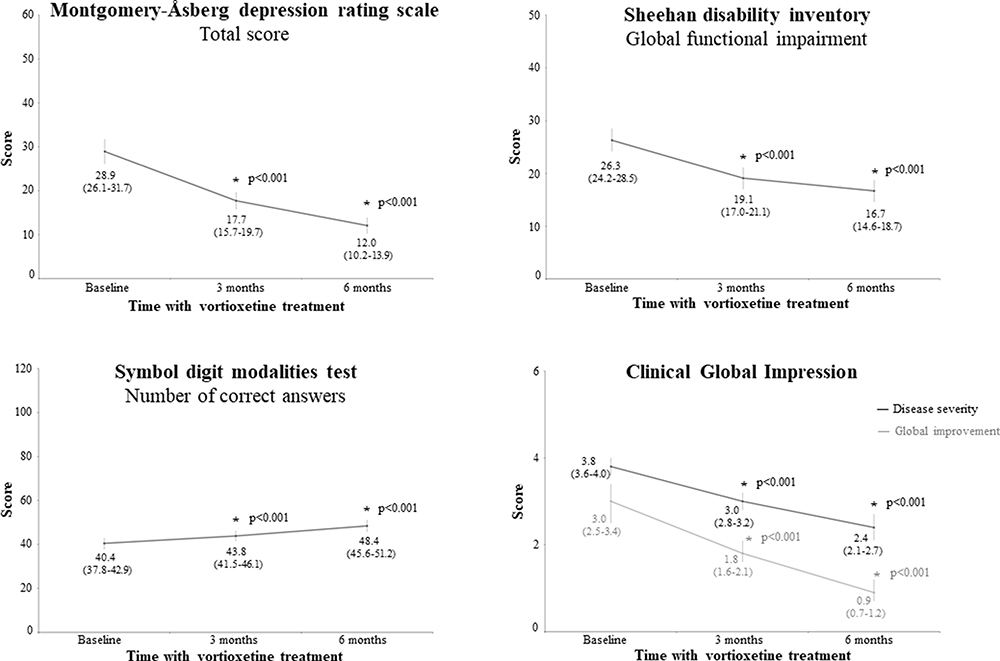 |
Figure 1 Effect of vortioxetine on evaluated tests at the three time points. Values inside the graphs are the mean and the 95% confidence interval. Asterisks (*) represent statistical significance between baseline and six months of treatment (p<0.001). |
Changes in SUDs During Vortioxetine Treatment
Compared with baseline, consumption of practically all substances decreased over the 3- and 6-month treatment, especially alcohol (from 35.0 to 23.8% and 17.5%, respectively), cannabis (from 18.8% to 13.8% and 6.3%), and cocaine (from 17.5% to 12.5% and 6.3%; Figure 2). Tobacco use remained stable at baseline and after 3 months (28.8% of patients), while it decreased after 6 months of treatment (25.0%). The severity of the alcohol addiction significantly decreased from baseline (mean: 9.1; 95% CI: 8.0–10.3) to the third month (mean: 6.6; 95% CI: 5.6–7.6; p<0.001), and the sixth month (mean: 4.7; 95% CI: 3.6–5.8; p<0.001; Table 3). Similarly, severity of cannabis addiction reduced significantly from baseline (mean: 9.7; 95% CI: 8.3–11.2) to the 3-month (mean: 7.6; 95% CI: 6.2–8.9; p=0.014), and 6-month treatment (mean: 4.1; 95% CI: 2.6–5.6; p<0.001). Decreases in severity were also significant for cocaine (mean: 5.3; 95% CI: 3.7–6.8, versus baseline, mean: 7.4; 95% CI: 5.4–9.3; p=0.022) and sedative-hypnotics (mean: 4.8; 95% CI: 1.4–8.3, versus baseline, mean: 9.2; 95% CI: 4.4–13.9; p=0.080) after 6 months, while a reduction of heroin was observed after 3 months (mean: 6.3; 95% CI: 0.1–12.6, versus baseline, mean: 12.4; 95% CI: 9.7–15.1; p=0.019).
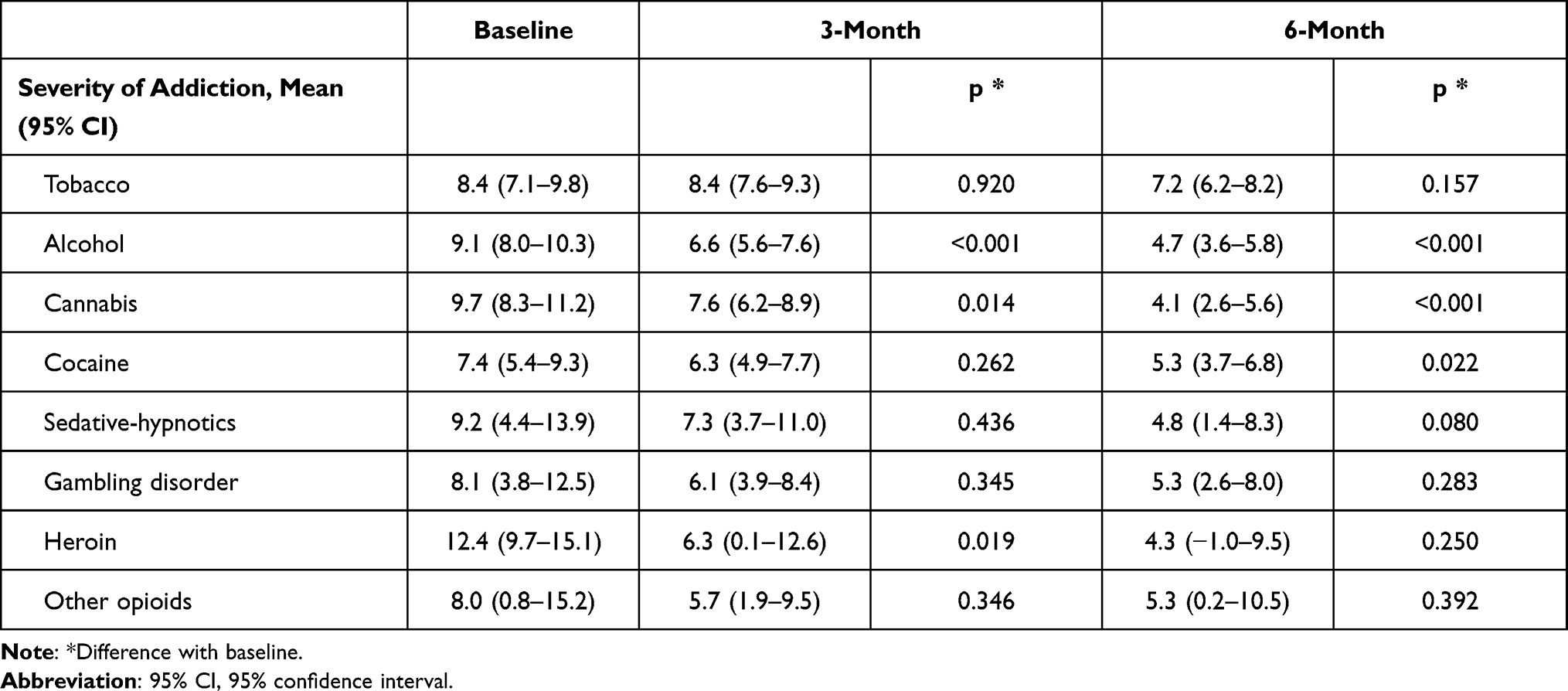 |
Table 3 Severity of the Addiction to Substances During Vortioxetine Treatment |
 |
Figure 2 Substance uses during vortioxetine treatment. Asterisks (*) represent statistical significance between baseline and six months of treatment (p<0.001). |
Discussion
We found that vortioxetine is effective in clinical practice for alleviating depressive symptoms and functional impairment, while improving cognitive and executive functions and disease severity for the management of MDD and SUD.
The treatment approach for MDD is changing to cope the heterogeneity of clinical phenotypes and endophenotypes of depression,5 especially when SUDs is also present. An adequate treatment for patients with both disorders aims at improving the depression-related symptoms (including affective, somatic, and cognitive dimensions), reducing the behaviors associated with seeking behaviors and consumption of substances. Additionally, these therapies are also directed to enhance the quality of life and life-satisfaction of patients, and achieve a higher well-being for the family and society. Vortioxetine, a novel antidepressant drug with a multimodal mechanism of action, has demonstrated its efficacy in the treatment of MDD.14,15 However, limited number of studies have explored the effectiveness of vortioxetine in real-world settings.18–20 De Carlo et al20 evaluated the efficacy, tolerability, and dropout rates of vortioxetine in 66 outpatients with major depressive episodes (45.5% with MDD diagnosis) at three time points. Authors reported significant improvements in scores of all evaluated tests (CGI efficacy index, Hamilton Anxiety Rating Scale, Hamilton Depression Rating Scale; MADRS, and Young Mania Rating Scale). Regarding MADRS, scores significantly decreased from baseline (24.5 ± 5.7) to the first (19.5 ± 6.4) and second (14.9 ± 7.6; p<0.001) time points. Responses to the treatment and remission rates were reported in 51.5% and 36.4% of patients, respectively. Similarly, Chin et al18 assessed the evolution of MDD in 138 patients receiving vortioxetine for three months in real-world settings. Significant reductions were reported during the treatment in depression severity (using the Patient Health Questionnaire-9, 18.7 ± 5.7 versus 5.0 ± 5.3), CGI-severity score (4.4 ± 0.7 versus 2.2 ± 1.1), and cognitive function (using the perceived deficit questionnaire–depression, 42.1 ± 18.8 versus 13.4 ± 13.0), in comparison to the baseline. Response to the treatment and remission rates were achieved in 80.8% and 59.0% of patients, respectively.
Despite the large proportion of patients with MDD having concurrent SUDs, yielding a higher risk of suicide, greater social and personal impairment, and other psychiatric conditions,6 only a sole study using vortioxetine has evaluated its effectiveness on these patients.21 Di Nicola et al21 described 45.6% and 22.8% of remission and response rates in patients with MDD and AUD. Moreover, 1.8% and 3.5% of patients being non-responders and experiencing a relapse, respectively. Indeed, patients with SUDs are frequently excluded from antidepressant efficacy trials for avoiding confounding results and the development of serious adverse events.29 The goal of our study was thus to provide the experience of vortioxetine in routine clinical practice on a cohort of patients with major MDD and SUD. Our results are in agreement with other real-world studies using vortioxetine.18–20 Scores for depression scale (MADRS) and functional impairment (SDI) significantly decreased during the treatment, while cognitive and executive functions (SDMT), and disease severity (CGI) significantly improved. Similar results were obtained in FOCUS,31,32 and CONNECT clinical trials.33,34 The randomized, double-blind, placebo-controlled FOCUS study analyzed the efficacy of vortioxetine (10 or 20 mg/day) in cognitive function and depressive symptoms of 602 adults.29 A post-hoc analysis of the FOCUS trial assessed changes in cognitive function of MDD working patients treated with vortioxetine. Both analyses highlighted that vortioxetine improved cognitive functions, independently of the alleviation of depressive symptoms. In the multicenter, randomized, double-blind, placebo-controlled, CONNECT study,33 vortioxetine significantly improved cognitive function and functionality, and decreased depression rates. Furthermore, in a cost-effectiveness study of vortioxetine versus duloxetine with patients from CONNECT study, authors suggested that vortioxetine may be a more adequate cost-effective alternative to duloxetine due to its superior ability to improve functional capacities.34 Therefore, both FOCUS and CONNECT trials evidenced the clinical benefit of vortioxetine on cognitive function in MDD. Moreover, Liebowitz et al,35 in a 12-week double-blind, placebo-controlled trial, evaluated the efficacy of vortioxetine in 40 patients with MDD and social anxiety disorder. Patients receiving vortioxetine showed significantly greater improvements on MADRS (effect size 0.7) and Liebowitz Social Anxiety Scale (effect size 0.7), compared to placebo. Pettinati et al,36 in a review of eight randomized, controlled trials of treatment for depression with alcohol use disorder, found that some of the antidepressants were effective in reducing depressive symptoms, however they had a mild effect in reducing alcohol use. In our study, substance use and severity of addiction was reduced significantly during vortioxetine treatment, especially for alcohol, cannabis, and cocaine.
The main limitation of the study was its retrospective nature, providing only the available information on medical charts. Additionally, it was a naturalistic study, so no comparisons were made towards a control group. Moreover, the number of patients was relatively low. In addition, while both CGI severity and improvement scales are a readily understood and practical measurement tool that can easily be administered by clinicians, among its frequently mentioned limitations the lack of well-defined behavioral anchors is included. As a result, the scoring mainly depends on the experience and judgement of the clinician, resulting in a poor inter-inter reliability. Additional criticisms include the absence of extensive psychometric validation, the inclusion of redundant information and being overly reliant on the memory of the clinician.37–40 Finally, no efforts were made to address potential sources of bias, which might represent a methodological limitation of the study. Besides this, our observations are in line with other real-world studies and clinical trials. On the other hand, main strengths of the study included that it was performed in real-world settings, and evaluated depression and SUD simultaneously. Real-world studies on vortioxetine are limited,18–20 thus the present study provides additional and positive evidence about its use, especially for MDD and SUD.
Conclusions
Vortioxetine was effective in clinical practice for reducing depression symptoms and functional impairment and improving cognitive and executive functions and disease severity in patients with MDD and SUD. Moreover, the treatment with vortioxetine favored a reduction in substance use and the severity of the SUDs. Further prospective, long-term studies, including larger cohort of patients, are required to corroborate these results.
Abbreviations
CGI, clinical global impression; CI95%, 95% confidence interval; MADRS, Montgomery-Åsberg Depression Rating Scale; MDD, major depressive disorder; SDI, Sheehan Disability Inventory; SDMT, symbol digit modalities test; SNRI, serotonin-noradrenaline reuptake inhibitors; SSRI, selective serotonin reuptake inhibitors; SUD, substance use disorder.
Ethics Approval and Informed Consent
The study was approved by the Ethics Committee of the Gregorio Marañon University Hospital (Madrid, Spain), with the reference number FPD-VOR-2019-01.
Acknowledgments
Authors also express gratitude to Meisys (Madrid, Spain) for writing assistance.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study was funded by the Fundación Patología Dual (Madrid, Spain).
Disclosure
IBV declares that he has received research grants from Lundbeck, Otsuka, and Exeltis, and educational grants from Janssen, Lundbeck, and Exeltis. CR has received fees to give lectures for Janssen-Cilag, Indivior, Servier, GSK, Gilead, MSD, Sanofi, Exceltis, AbbVie, Takeda, Rubio and Casein. He has received financial compensation for his participation as consultant or a board member of Lundbeck, Gilead, MSD, Mundipharma, INDIVIOR, Exceltis, Camurus, Gebro and Abbive board. He has carried out the PROTEUS project, which was funded by a grant from Reckitt-Benckiser/Indivior and the COSTEDOPIA project, which was funded by INDIVIOR. He received two medical education grants by Gilead and medical writing support from AbbVie. JM-R has received fees for being a speaker for Lundbeck, Janssen, and educational grants from Exeltis, and Lundbeck. LG-L has participated in symposiums for the industry during the last years, including Esteve, Lundbeck, and Janssen. MT has received fees to give lectures from Gilead, MSD, Lundbeck, Otsuka, Molteni, and Servier. She has received financial compensation for his participation as a consulting/board member of MSD, Gilead, Esteve, Servier, Lundbeck, Gebro Pharma, Molteni, and Camurus. NS has received honoraria/expenses from Janssen, Takeda, Lundbeck, Exeltis, and Rovi. He also has participated as consulting/advisory board for Lundbeck. PV and LA declare no conflicts of interest.
References
1. GBD 2017 DALYs and HALE Collaborators. Global, regional, and national disability-adjusted life-years (DALYs) for 359 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1859–1922. doi:10.1016/S0140-6736(18)32335-3
2. World Health Organization. Depression. Available from: https://www.who.int/health-topics/depression.
3. Sloan E, Hall K, Moulding R, Bryce S, Mildred H, Staiger PK. Emotion regulation as a transdiagnostic treatment construct across anxiety, depression, substance, eating and borderline personality disorders: a systematic review. Clin Psychol Rev. 2017;57:141–163. doi:10.1016/j.cpr.2017.09.002
4. Tirado Muñoz J, Farré A, Mestre-Pintó J, Szerman N, Torrens M. Dual diagnosis in Depression: treatment recommendations. Adicciones. 2018;30(1):66–76. doi:10.20882/adicciones.868
5. Szerman N, Peris L. Precision psychiatry and dual disorders. J Dual Diagn. 2018;14(4):237–246. doi:10.1080/15504263.2018.1512727
6. Davis L, Uezato A, Newell JM, Frazier E. Major depression and comorbid substance use disorders. Curr Opin Psychiatry. 2008;21(1):14–18. doi:10.1097/YCO.0b013e3282f32408
7. Lai HM, Cleary M, Sitharthan T, Hunt GE. Prevalence of comorbid substance use, anxiety and mood disorders in epidemiological surveys, 1990–2014: a systematic review and meta-analysis. Drug Alcohol Depend. 2015;154:1–13. doi:10.1016/j.drugalcdep.2015.05.031
8. Szerman N, Lopez-Castroman J, Arias F, et al. Dual diagnosis and suicide risk in a Spanish outpatient sample. Subst Use Misuse. 2012;47(4):383–389. doi:10.3109/10826084.2011.636135
9. Ng QX, Lim DY, Chee KT. Reimagining the spectrum of affective disorders. Bipolar Disord. 2020;22(6):638–639. doi:10.1111/bdi.12960
10. Torrens M, Fonseca F, Mateu G, Farré M. Efficacy of antidepressants in substance use disorders with and without comorbid depression. A systematic review and meta-analysis. Drug Alcohol Depend. 2005;78(1):1–22. doi:10.1016/j.drugalcdep.2004.09.004
11. Nunes EV, Levin FR. Treatment of depression in patients with alcohol or other drug dependence: a meta-analysis. JAMA. 2004;291(15):1887–1896. doi:10.1001/jama.291.15.1887
12. Szerman N, Arias F, Algorta J, et al. Effectiveness of tianeptine in patients with major depressive disorder and substance use disorder. Actas Esp Psiquiatr. 2021;49(4):135–144.
13. Richelson E. Multi-modality: a new approach for the treatment of major depressive disorder. Int J Neuropsychopharmacol. 2013;16(6):1433–1442. doi:10.1017/S1461145712001605
14. Gonda X, Sharma SR, Tarazi FI. Vortioxetine: a novel antidepressant for the treatment of major depressive disorder. Expert Opin Drug Discov. 2019;14(1):81–89. doi:10.1080/17460441.2019.1546691
15. Sanchez C, Asin KE, Artigas F. Vortioxetine, a novel antidepressant with multimodal activity: review of preclinical and clinical data. Pharmacol Ther. 2015;145:43–57. doi:10.1016/j.pharmthera.2014.07.001
16. Chen G, Højer AM, Areberg J, Nomikos G. Vortioxetine: clinical pharmacokinetics and drug interactions. Clin Pharmacokinet. 2018;57(6):673–686. doi:10.1007/s40262-017-0612-7
17. Montgomery SA, Nielsen RZ, Poulsen LH, Häggström L. A randomised, double-blind study in adults with major depressive disorder with an inadequate response to a single course of selective serotonin reuptake inhibitor or serotonin-noradrenaline reuptake inhibitor treatment switched to vortioxetine or agomelatine. Hum Psychopharmacol. 2014;29(5):470–482. doi:10.1002/hup.2424
18. Chin CN, Zain A, Hemrungrojn S, et al. Results of a real-world study on vortioxetine in patients with major depressive disorder in South East Asia (REVIDA). Curr Med Res Opin. 2018;34(11):1975–1984. doi:10.1080/03007995.2018.1477746
19. De Berardis D, Fornaro M, Anastasia A, et al. Adjunctive vortioxetine for SSRI-resistant major depressive disorder: a “real-world” chart review study. Braz J Psychiatry. 2020;42(3):317–321. doi:10.1590/1516-4446-2019-0690
20. De Carlo V, Vismara M, Grancini B, et al. Effectiveness, tolerability, and dropout rates of vortioxetine in comorbid depression: a naturalistic study. Hum Psychopharmacol. 2020;35(5):e2750. doi:10.1002/hup.2750
21. Di Nicola M, Pepe M, Panaccione I, et al. Effect of vortioxetine in subjects with major depressive and alcohol use disorders: a 6-month retrospective analysis. CNS Spectr. 2020;27:1–9.
22. American Psychiatric Association, American Psychiatric Association. DSM-5 Task Force. With Diagnostic and Statistical Manual of Mental Disorders: DSM-5.
23. Lobo A, Chamorro L, Luque A, Dal-Ré R, Badia X, Baró E. Validation of the Spanish versions of the Montgomery-Asberg depression and Hamilton anxiety rating scales. Med Clin. 2002;118(13):493–499. doi:10.1016/S0025-7753(02)72429-9
24. Montgomery SA, Asberg M. A new depression scale designed to be sensitive to change. Br J Psychiatry. 1979;134(4):382–389. doi:10.1192/bjp.134.4.382
25. Sheehan KH, Sheehan DV. Assessing treatment effects in clinical trials with the discan metric of the Sheehan Disability Scale. Int Clin Psychopharmacol. 2008;23(2):70–83. doi:10.1097/YIC.0b013e3282f2b4d6
26. Smith A. Symbol and Digit Modalities Test. TEA Ediciones SA; 2002.
27. Busner J, Targum SD. The clinical global impressions scale: applying a research tool in clinical practice. Psychiatry. 2007;4(7):28–37.
28. González-Saiz F, de Las Cuevas C, Barrio G, Domingo-Salvany A. Spanish version of the Severity of Dependence Scale (SDS). Med Clin (Barc). 2008;131(20):797–798. doi:10.1016/S0025-7753(08)75509-X
29. Davis LL, Wisniewski SR, Howland RH, et al. Does comorbid substance use disorder impair recovery from major depression with SSRI treatment? An analysis of the STAR*D level one treatment outcomes. Drug Alcohol Depend. 2010;107(2–3):161–170. doi:10.1016/j.drugalcdep.2009.10.003
30. Mahableshwarkar AR, Jacobsen PL, Chen Y. A randomized, double-blind trial of 2.5 mg and 5 mg vortioxetine (Lu AA21004) versus placebo for 8 weeks in adults with major depressive disorder. Curr Med Res Opin. 2013;29(3):217–226. doi:10.1185/03007995.2012.761600
31. McIntyre RS, Lophaven S, Olsen CK. A randomized, double-blind, placebo-controlled study of vortioxetine on cognitive function in depressed adults. Int J Neuropsychopharmacol. 2014;17(10):1557–1567. doi:10.1017/S1461145714000546
32. McIntyre RS, Florea I, Tonnoir B, Loft H, Lam RW, Christensen MC. Efficacy of vortioxetine on cognitive functioning in working patients with major depressive disorder. J Clin Psychiatry. 2017;78(1):115–121. doi:10.4088/JCP.16m10744
33. Mahableshwarkar AR, Zajecka J, Jacobson W, Chen Y, Keefe RS. A randomized, placebo-controlled, active-reference, double-blind, flexible-dose study of the efficacy of vortioxetine on cognitive function in major depressive disorder. Neuropsychopharmacology. 2015;40(8):2025–2037. doi:10.1038/npp.2015.52
34. Christensen MC, Munro V. Cost per successfully treated patient for vortioxetine versus duloxetine in adults with major depressive disorder: an analysis of the complete symptoms of depression and functional outcome. Curr Med Res Opin. 2018;34(4):593–600. doi:10.1080/03007995.2017.1416952
35. Liebowitz MR, Careri J, Blatt K, et al. Vortioxetine versus placebo in major depressive disorder comorbid with social anxiety disorder. Depress Anxiety. 2017;34(12):1164–1172. doi:10.1002/da.22702
36. Pettinati HM. Antidepressant treatment of co-occurring depression and alcohol dependence. Biol Psychiatry. 2004;56(10):785–792. doi:10.1016/j.biopsych.2004.07.016
37. Beneke M, Rasmus W. “Clinical Global Impressions” (ECDEU): some critical comments. Pharmacopsychiatry. 1992;25(4):171–176. doi:10.1055/s-2007-1014401
38. Rush AJ, First MB, Blacker D. Handbook of Psychiatric Measures. American Psychiatric Pub; 2008.
39. Forkmann T, Scherer A, Boecker M, Pawelzik M, Jostes R, Gauggel S. The Clinical Global Impression Scale and the influence of patient or staff perspective on outcome. BMC Psychiatry. 2011;11(1):83. doi:10.1186/1471-244X-11-83
40. Dunlop BW, Gray J, Rapaport MH. Transdiagnostic clinical global impression scoring for routine clinical settings. Behav Sci. 2017;7(3):40. doi:10.3390/bs7030040
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.