Back to Journals » OncoTargets and Therapy » Volume 15
A Durable Response of Primary Advanced Colonic Plasmacytoma Using a Combination of Surgical Resection and Adjuvant Bortezomib: A Case Report and Literature Review
Authors Alfar R, Kamal N, Abdel Razeq R, Omari Z ![]() , Bater R, Sharaf B
, Bater R, Sharaf B ![]()
Received 2 May 2022
Accepted for publication 25 September 2022
Published 7 November 2022 Volume 2022:15 Pages 1347—1354
DOI https://doi.org/10.2147/OTT.S372534
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Sanjay Singh
Rozan Alfar,1 Nazmi Kamal,2 Rashid Abdel Razeq,1 Zaid Omari,3 Rayan Bater,1 Baha’ Sharaf1
1Internal Medicine Department, King Hussein Cancer Center, Amman, Jordan; 2Pathology Department, Hematopathology Section, King Hussein Cancer Center, Amman, Jordan; 3Radiology Department, King Hussein Cancer Center, Amman, Jordan
Correspondence: Baha’ Sharaf, Internal Medicine Department, King Hussein Cancer Center, Amman, Jordan, Tel +962-6 5300460, Ext 7538, Email [email protected]
Background: Primary isolated extra-medullary plasmacytoma (EMP) is a rare entity that most commonly involves the nasopharynx or upper respiratory tract. Only 10% of cases involve the gastrointestinal tract, mainly the small intestine and the stomach. Involvement of the colon is extremely rare with less than 40 reported cases worldwide.
Case Presentation: We report a case of a 57-year-old man who was presented with a 3-week history of fresh bleeding from the rectum. Colonoscopy showed a polypoidal mass arising from the ascending colon; biopsy showed clonal plasmacytosis and a primary colonic solitary EMP diagnosis was made after exclusion of multiple myeloma (MM). Accordingly, the patient underwent a right hemicolectomy, followed by 6 cycles of bortezomib, cyclophosphamide, and dexamethasone (VCD). The patient continued to be disease-free 30 months after the completion of his chemotherapy.
Conclusion: To our knowledge, this is the first reported case of primary colonic plasmacytoma managed with surgical resection followed by an adjuvant bortezomib-based regimen with a durable response.
Keywords: primary plasmacytoma, plasmacyte dyscrasia, myeloma, colon, bortezomib
Introduction
Multiple myeloma (MM) and plasmacytoma are the two main plasma cell dyscrasias, which are characterized by monoclonal plasma cell proliferation, but while the former is systemic the latter is localized.1 Plasmacytoma may occur as a primary disorder or may occur concurrently or following the onset of MM (secondary).2 It is also classified based on the sites of involvement: osseous or extramedullary plasmacytoma (EMP), and both have different treatment outcomes and risk of progression to MM.3,4
Plasmacytoma can be diagnosed if all the following criteria are fulfilled: Biopsy-proven solitary lesion of bone or soft tissue with evidence of clonal plasma cells, no evidence of clonal plasma cell in the bone marrow, no skeletal lesions seen in computed tomography (CT), positron emission tomography (PET) scan, or magnetic resonance imaging (MRI) and no evidence of end organ damage including renal dysfunction, hypercalcemia and anemia.5 Serum protein electrophoresis (SPEP) showed a monoclonal band in up to 25% of patients with EMP. However, M band and/or Bence-Jones protein in urine does not necessarily preclude the diagnosis and this M protein usually disappears after treatment.6
Extramedullary plasmacytoma is less common than osseous plasmacytoma and constitutes less than 5% of all plasma cell neoplasms, with the aerodigestive tract being the most common site and involved in 80% of cases.6,7 Gastrointestinal tract primary plasmacytomas are a rare entity (10% of all EMP),8 and it most commonly involves stomach9 or small intestine. Given the rarity of such occurrence,10 in addition to the scarcity of data reporting similar cases worldwide,8 there is no knowledge present regarding treatment and/or prognosis of primary colon plasmacytoma.
In this paper, we report a case of colonic plasmacytoma that underwent right hemicolectomy, followed by adjuvant chemotherapy with bortezomib, cyclophosphamide and dexamethasone (VCD).
Case Presentation
A 57-year-old male was presented in July 2019 with a 3-week history of fresh bleeding via the rectum, dizziness, weight loss, and altered bowel. By physical examination, it was evident that the patient looked pale, but the abdominal and rectal examinations were unremarkable. In addition to this, basic laboratory investigations including kidney function test (KFT), liver function test (LFT), coagulation profile, and urine analysis were all within normal range. On the other hand, hemoglobin (Hb) was low at 8.5 gm/dL with low mean corpuscular volume (MCV), and blood film showed microcytic hypochromic anemia with slight neutrophilic leukocytosis and thrombocytosis.
Computed tomography scans presented soft tissue mass lesion in the lower pole of the cecum associated with multiple enlarged regional lymph nodes only, without any liver or lung lesions (Figure 1). PET scan done and showed hypermetabolic malignant cecal mass with hypermetabolic regional mesentric lymph nodes (figure 4). In addition, colonoscopy exhibited a large polypoid mass lesion arising from the cecum and extending beyond the hepatic flexure. Also, biopsy showed clonal plasmacytosis (Immunoreactive for CD138, CD56 and negative for CD3 and CD20 and lambda light chain restricted); a picture consistent with plasmacytoma (Figures 2 and 3). Bone marrow aspirate and biopsy showed no evidence of clonal plasma cell disorder. In addition to this, serum free light chain showed a kappa level of 15.5 mg/L (normal: 3.3–19.4) and lambda level of 364 mg/L (normal: 5.7–26.3); ratio 0.042 (normal: 0.26 to 1.65). Urine protein electrophoresis (UPEP) and immunofixation were normal, while a monoclonal band (IgG Lambda) in the gamma area measuring approximately 2.2 gm/dL was evident in serum protein electrophoresis (SPEP) and immunofixation. Further workup showed a β2 microglobulin 1.8 mg/L (normal 0.8–2.5), immunoglobulin-G (IgG) 2994 mg/L, IgM: 175 mg/dL and IgA: 203 mg/dL. Moreover, PET scan showed hypermetabolic malignant right colonic (cecal) mass, which is compatible with known primary tumor.
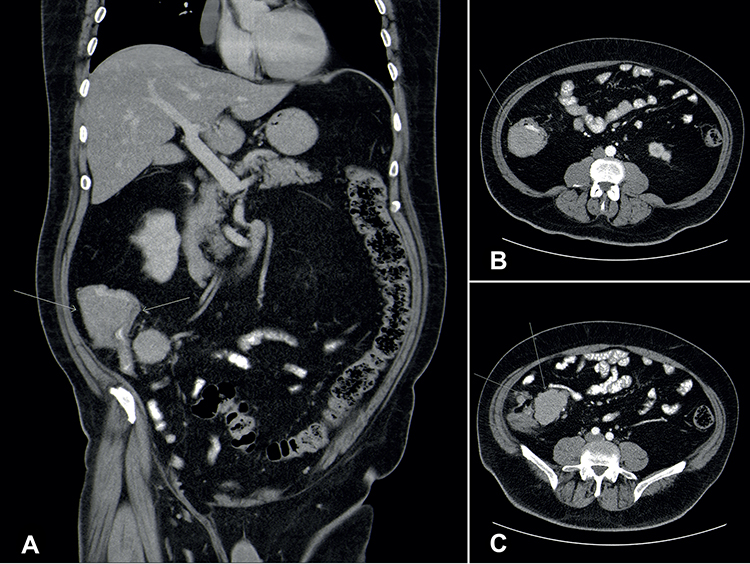 |
Figure 1 Preoperative computed tomography: (A) coronal CT scan images at presentation showing soft tissue mass in the lower pole of the caecum associated with multiple metastatic regional lymph nodes (B) Axial CT scan images at presentation showing soft tissue mass in the lower pole of the caecum (arrow) (C) Axial CT scan images at presentation showing multiple enlarged lymph nodes located along the course of the ileocolic vessels measures about 4.7*6.4 cm in axial dimension. |
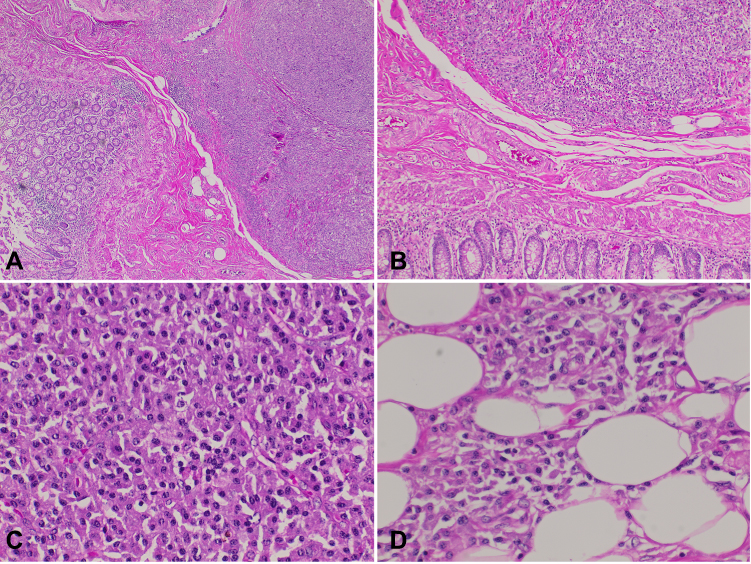 |
Figure 2 (A) 100X H&E stained section of colonic mass, (B) 200X H& E stained section of colonic mass, (C) 400X H&E stained section of colonic mass, (D) 200X H&E stained section of colonic mass. |
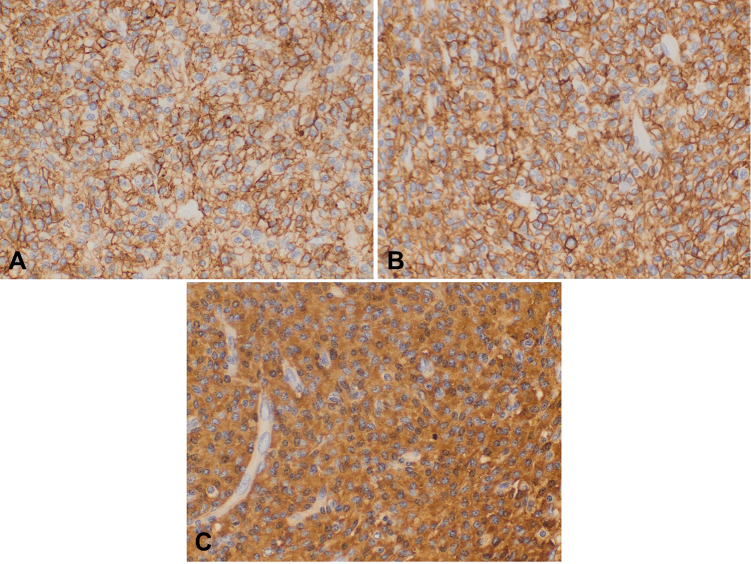 |
Figure 3 (A) CD138 immunostain (IHC400X) (B) CD56 immunostain (IHC400X) (C) Lambda light chain immunostain (IHC 400X). |
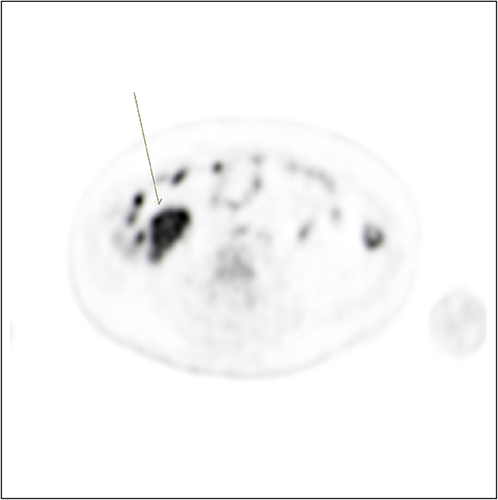 |
Figure 4 Preoperative PET scan showed: Hypermetabolic malignant right colonic (caecal) mass, which is compatible with known primary tumor and multiple hypermetabolic regional mesenteric lymph nodes metastases. |
Right hemicolectomy was performed and revealed a cecal exophytic polypoid mass measuring 5.5 cm in maximal dimension. The histopathologic study of the mass revealed a submucosal tumor composed of large oval cells consisting of a round nucleus in eccentric position with coarse chromatin and plenty of cytoplasm. The tumor infiltrates the muscular wall of the intestine and the pericolic fat (Figure 2). Eleven out of fifteen regional lymph nodes were involved, the surgical margins were free and immunohistochemical stains were performed. The tumor cells were immunoreactive for CD138+, CD56+ and showed lambda light chain restriction (Figures 2 and 3). They were negative for CD20 and synaptophysin and CD3. The overall findings are consistent with extramedullary colonic plasmacytoma.
Along with large tumor size, persistent monoclonal band, and regional lymph node involvement, radiotherapy is sought out to have minimal benefits. Moreover, data established from secondary plasmacytoma and primary plasmacytoma of sites other than colon showed favorable outcome with bortezomib adjuvant therapy. Therefore, it is worthy of investigation in primary colonic plasmacytoma.
Following surgery, the patient received adjuvant treatment with 6 cycles of VCD, which all were well tolerated. Three months after surgery, monoclonal band was reduced to 0.4 gm/dL, and after finishing all planned adjuvant VCD, no monoclonal band was seen. Currently, with 30 months after surgery, no monoclonal bands were detected and PET scan showed no evidence of disease (complete remission).
Discussion
Multiple myeloma is the most prevalent plasma cell disorder. However, in less than 5% of the cases it may present as localized clonal proliferation of clonal plasma cell called plasmacytoma, which may occur as a solitary or as multiple lesions either in the bone or soft tissue. Due to the high rate of progression to MM, prognosis of osseous extramedullary plasmacytoma is usually worse compared to the one that involves soft tissues.11,12
Extramedullary plasmacytoma of soft tissue is less common than bone EMP, and in 80% of the cases, it involves the upper aerodigestive tract.13 Primary gastrointestinal tract EMP is extremely rare and constitutes of around 10% of primary EMP. The gastrointestinal tract, stomach and small bowels14 are the most commonly involved sites. In Table 1, previously reported cases of colonic plasmacytoma are mentioned. In the literature review, 33 previous cases were reported of 9 females and 24 males. The mean age (median) was 56.8 (57), and the most commonly reported symptoms were abdominal pain, lower gastrointestinal bleeding, change in bowel habits, large bowel obstruction, and intussusception.46 Only 2 cases were presented with perforation, and surgery was the main modality of treatment; nevertheless, one reported case was treated with EMR.33,34,38
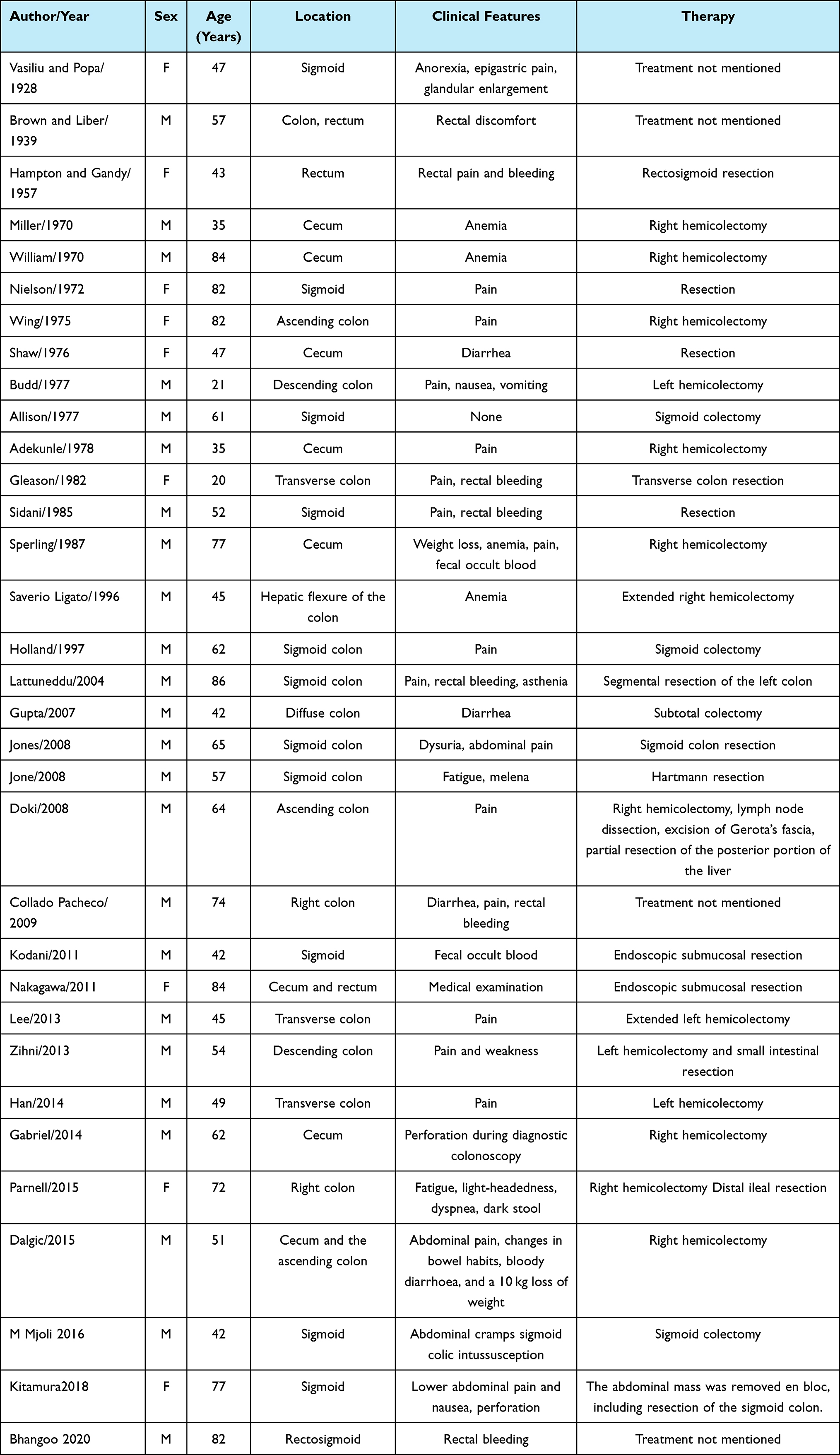 |
Table 1 Previously Reported Primary Colonic Plasmacytoma |
In general, EMPs are considered radiosensitive, with a local control rate of 90–100%,47,57 and radiotherapy is the preferred approach for those involving the head, neck, anal46 and rectal48 regions. When complete surgical resection is feasible, surgery remains the treatment of choice for colonic lesions. Alternatively, endoscopic treatments such as submucosal resection or polypectomy have proven to be sufficient in selected cases.33,34,38 In the case of a tumor size greater than 5 cm, response to radiotherapy can be poor and recurrence is potentially high.49 Nevertheless, complete resection is not feasible, or in cases of patients with positive regional lymph nodes, adjuvant radiotherapy is recommended.50
Chemotherapy has been used in the treatment of disseminated disease and preoperatively to reduce the size of the tumor. Data about using bortezomib in EMP secondary to MM showed significant efficacy in this setting. However, the number of treated patients is small in order to make a proper conclusion. In one case report, 3 out of 4 soft tissue plasmacytomas, complicating multiple myeloma, at time of relapse, had completely disappeared with bortezomib. However, other agents, like thalidomide, were not effective.51
Another case report displayed complete response of primary extramedullary gastric plasmacytoma with bortezomib and dexamethasone.52 Several other case reports illustrated similar response using bortezomib with cyclophosphamide, and dexamethasone.53–56,58
In conclusion, colonic plasmacytoma is extremely rare. Surgical resection followed by adjuvant bortezomib-based therapy may result in durable response.
Data Sharing Statement
Data will be available upon request. Please email your request to [email protected].
Ethical Statement
Written informed consent was provided by the patient to have the case published.
Acknowledgment
The authors would like to acknowledge the nursing staff for their proper follow-up with the patient.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Dores GM, Landgren O, McGlynn KA, Curtis RE, Linet MS, Devesa SS. Plasmacytoma of bone, extramedullary plasmacytoma, and multiple myeloma: incidence and survival in the United States, 1992–2004. Br J Haematol. 2009;144(1):86–94. doi:10.1111/j.1365-2141.2008.07421.x
2. Griffiths AP, Shepherd NA, Beddall A, Williams JG. Gastrointestinal tumour masses due to multiple myeloma: a pathological mimic of malignant lymphoma. Histopathology. 1997;31(4):318–323. doi:10.1046/j.1365-2559.1997.1610866.x
3. Soutar R, Lucraft H, Jackson G, et al. Guidelines on the diagnosis and management of solitary plasmacytoma of bone and solitary extramedullary plasmacytoma. Clin Oncol. 2004;16(6):405–413. doi:10.1016/j.clon.2004.02.007
4. Gerry D, Lentsch EJ. Epidemiologic evidence of superior outcomes for extramedullary plasmacytoma of the head and neck. Otolaryngol Head Neck Surg. 2013;148(6):974–981. doi:10.1177/0194599813481334
5. Dimopoulos MA, Moulopoulos LA, Maniatis A, Alexanian R. Solitary plasmacytoma of bone and asymptomatic multiple myeloma. Blood. 2000;96(6):2037–2044. doi:10.1182/blood.V96.6.2037
6. Susnerwala SS, Shanks JH, Banerjee SS, Scarffe JH, Farrington WT, Slevin NJ. Extramedullary plasmacytoma of the head and neck region: clinicopathological correlation in 25 cases. Br J Cancer. 1997;75(6):921–927. doi:10.1038/bjc.1997.162
7. Straetmans J, Stokroos R. Extramedullary plasmacytomas in the head and neck region. Eur Arch Otorhinolaryngol. 2008;265(11):1417–1423. doi:10.1007/s00405-008-0613-0
8. Gupta V, Nahak B, Sakhuja P, Agarwal AK, Kumar N, Mishra PK. Primary isolated extramedullary plasmacytoma of colon. World J Surg Oncol. 2007;5(1). doi:10.1186/1477-7819-5-47
9. Kwak H-S, Jin G-Y, Lee J-M. Radiologic findings of multiple myeloma with gastric involvement: a case report. Korean J Radiol. 2002;3(2):133. doi:10.3348/kjr.2002.3.2.133
10. Herbst A, Renner SW, Ringenberg QS, Fass R, Krouse RS. Multiple myeloma presenting with a colonic obstruction and bony lesions: a clinical dilemma. J Clin Oncol. 2008;26(34):5645–5647. doi:10.1200/JCO.2008.18.6239
11. Corwin J, Lindberg RD. Solitary plasmacytoma of bone vs. Extramedullary Plasmacytoma and Their Relationship to Multiple Myeloma Cancer. 1979;43(3):1007–1013.
12. Bolek TW, Marcus RB, Mendenhall NP. Solitary plasmacytoma of bone and soft tissue. Int J Radiat Oncol Biol Phys. 1996;36(2):329–333. doi:10.1016/S0360-3016(96)00334-3
13. Selby P, Gore M. Myeloma and other plasma cell malignancies. Oxford Textbook of Oncology. 1995;2(12):8185278.Selby P, Gore M. Myeloma and other plasma cell malignancies. Oxford Textbook of Oncology. 1995;2(12):8185278.
14. Sharma KD, Shrivastava JD. Extramedullary plasmacytoma of the gastrointestinal tract. Arch Pathol. 1961;71:22933.;71:22933.
15. Vasiliu T. ”Forme gastrointesinalis destumerurs dites plasmacytomes. Compt Rend Soc Biol. 1928;98:738–740.
16. Brown CR, Liber AF. Multiple plasmoma of the ileum and colon. Arch Pathol. 1939;28:112–113.
17. Willliam HJ, Johnson J, Taylor G. Solitary extramedullary plasmacytoma of the skin.;A review of the world literature and the report of an additional case. Cancer. 1970;26:65–68. doi:10.1002/1097-0142(197007)26:1<65::AID-CNCR2820260107>3.0.CO;2-F
18. Nielsen SM, Schenken JR, Cawley LP. Primary colonic plasmacytoma. Cancer. 1972;30:261–267. doi:10.1002/1097-0142(197207)30:1<261::AID-CNCR2820300136>3.0.CO;2-G
19. Wing EJ, Perchick J, Hubbard J. Solitary obstructing plasmacytoma of the colon. J Am Med Assoc. 1975;233(12):1298–1299. doi:10.1001/jama.1975.03260120060025
20. Shaw MI, Schweers CA, Nodquist RE, Rose DD, Kell TT. Solitary cecal plasmacytoma: electron microscopic, immunologic and cytochemical studies. Cancer. 1976;37:2220–2223. doi:10.1002/1097-0142(197605)37:5<2220::AID-CNCR2820370510>3.0.CO;2-A
21. Budd DC, Cochran RC, Metildi LA. Extramedullary plasmacytoma of the colon: a rare cause of intussusception. Am Surg. 1977;43(8):528–530.
22. Allison JG, Gétaz EP, Staples WG. Primary isolated extramedullary plasmacytoma of the colon: a case report. S Afr Med J. 1977;51(24):893–895.
23. Adekunle OO. Primary plasmacytoma of the caecum. J R Coll Surg Edinb. 1978;23:104–106.
24. Gleason TH, Hammar SP. Plasmacytoma of the colon: case report with lambda light chain, demonstrated by immunoperoxidase studies. Cancer. 1982;50(1):130–133. doi:10.1002/1097-0142(19820701)50:1<130::AID-CNCR2820500124>3.0.CO;2-O
25. Sidani MS, Campos MM, Joseph JI. Primary plasmacytomas of the colon. Dis Colon Rectum. 1983;26(3):182–187. doi:10.1007/BF02560167
26. Sperling RI, Fromowitz FB, Castellano TJ. Anaplastic solitary extramedullary plasmacytoma of the cecum. Report of a case confirmed by immunoperoxidase staining. Dis Colon Rectum. 1987;30(11):894–898. doi:10.1007/BF02555432
27. Ligato S, El-Naggar A, Cleary KR, Manning J. Extramedullary plasmacytoma mimicking primary colonic carcinoma in a patient with Crohn’s disease. Case report and literature review. Arch Pathol Lab Med. 1996;120(3):279–282.
28. Holland AJ, Kubacz GJ, Warren JR. Plasmacytoma of the sigmoid colon associated with a diverticular stricture: case report and review of the literature. J R Coll Surg Edinb. 1997;42(1):47–49.
29. Lattuneddu A, Farneti F, Lucci E, Garcea D, Ronconi S, Saragoni L. A case of primary extramedullary plasmacytoma of the colon. Int J Colorectal Dis. 2004;19(3):289–291. doi:10.1007/s00384-003-0560-6
30. Jones JE, Brand MI, Saclarides TJ, Jakate S. Primary extramedullary plasmacytomas of the colon. Am Surg. 2008;74(9):873–874. doi:10.1177/000313480807400922
31. Doki T, Takeuchi O, Kaiho T, Tsuchiya S, Matsuzaki O, Miyazaki M. Primary isolated extramedullary plasmacytoma of the colon. Int J Colorectal Dis. 2008;23(7):719–720. doi:10.1007/s00384-008-0439-7
32. Pacheco DC, de Solórzano MM, Lázaro EQ, Alvarez CI, Torre LR. Extramedullary plasmacytoma of the colon: a rare cause of gastrointestinal bleeding. Endoscopy. 2009;41(Suppl 2):E306–E307. doi:10.1055/s-0029-1215225
33. Kodani T, Osada T, Terai T, et al. Successful endoscopic mucosal resection of a solitary extramedullary plasmacytoma in the sigmoid colon. Endoscopy. 2011;43(Suppl 2):E298–E2999. doi:10.1055/s-0030-1256451
34. Nakagawa Y, Nagai T, Okawara H, et al. Minute primary extramedullary plasmacytomas of the large intestine. Endoscopy. 2011;43(S 02):E105–E106. doi:10.1055/s-0030-1256138
35. Lee SH, Ahn BK, Baek SU, Chang HK. Primary isolated extramedullary plasmacytoma in the colon. Gastroenterology Res. 2013;6(4):152–155.
36. Zihni İ, Dinç R, Canpolat S, Cengiz F, Uslu A. Extramedullary plasmacytoma of the colon: a case report. Ulus Cerrahi Derg. 2013;30(4):231–233. doi:10.5152/UCD.2013.45
37. Han YJ, Park SJ, Park MI, et al. Solitary extramedullary plasmacytoma in the gastrointestinal tract: report of two cases and review of literature. Korean J Gastroenterol. 2014;63(5):316–320. doi:10.4166/kjg.2014.63.5.316
38. Gabriel EM, Savu M. Discovery of a rare ileocecal plasmacytoma. J Surg Case Rep. 2014;2014(3):rju016. doi:10.1093/jscr/rju016
39. Parnell K, Ahmed M, Smalligan RD, Nadesan S. Extramedullary plasmacytoma mimicking colon carcinoma: an unusual presentation and review of the literature. BMJ Case Rep. 2015;2015:bcr2015210973. doi:10.1136/bcr-2015-210973
40. Dalgic T, Bostanci EB, Cakir T, et al. Solitary plasmacytoma of the cecum and the ascending colon: surgical resection as a treatment modality. Case Rep Surg. 2015;2015:126863. doi:10.1155/2015/126863
41. Hampton JM, Gandy JR. Plasmacytoma of the gastro-intestinal tract. Ann Surg. 1957;145(3):415–422. doi:10.1097/00000658-195703000-00018
42. Miller WA. Extramedullary plasmacytoma of the colon. J Can Assoc Radiol. 1970;21:33–34.
43. Mjoli M, Vorajee N, Naidoo Y, Madiba T. Solitary extramedullary plasmacytoma of the colon, rectum and anus. S Afr J Surg. 2016;54(2):45–47.
44. Kitamura F, Doi K, Ishiodori H, Ohchi T, Baba H. Primary extramedullary plasmacytoma of the sigmoid colon with perforation: a case report. Surg Case Rep. 2018;4(1):28. doi:10.1186/s40792-018-0437-0
45. Bhangoo RS, McCullough AE, Yang M. Obstructive rectosigmoid colon solitary extramedullary plasmacytoma. Dig Liver Dis. 2021;53(4):496–497. doi:10.1016/j.dld.2020.12.008
46. Antunes MI, Bujor L, Grillo IM. Anal canal- An uncommon presentation site. Rep Pract Oncol Radiother. 2011;16(1):36–39. doi:10.1016/j.rpor.2010.12.002
47. Islam SR, Attaya MN, Parupudi S, et al. Sigmoid plasmacytoma mimicking colon cancer in a patient with multiple myeloma: case report and review of literature. Gastrointest Endosc. 2010;71(3):655–657. doi:10.1016/j.gie.2009.08.003
48. Price A, Quilty PM, Ludgate SM. Extramedullary plasmacytoma of the rectum: two cases treated by radiotherapy. Clin Radiol. 1987;38(3):283–285. doi:10.1016/S0009-9260(87)80069-7
49. Tsang RW, Gospodarowicz MK, Pintilie M, et al. Solitary plasmacytoma treated with radiotherapy: impact of tumor size on outcome. Int J Radiat Oncol Biol Phys. 2001;50(1):113–120. doi:10.1016/S0360-3016(00)01572-8
50. Alexiou C, Kau RJ, Dietzfelbinger H, et al. Extramedullary plasmacytoma. Cancer. 1999;85(11):2305–2314. doi:10.1002/(SICI)1097-0142(19990601)85:11<2305::AID-CNCR2>3.0.CO;2-3
51. Laura R, Cibeira MT, Uriburu C, et al. Bortezomib: an effective agent in extramedullary disease in multiple myeloma. Eur J Haematol. 2006;76(5):405–408. doi:10.1111/j.0902-4441.2005.t01-1-EJH2462.x
52. Katodritou E, Kartsios C, Gastari V, et al. Successful treatment of extramedullary gastric plasmacytoma with the combination of bortezomib and dexamethasone: first reported case. Leuk Res. 2008;32(2):339–341. doi:10.1016/j.leukres.2007.04.016
53. Matsuda M, Sueda S, Taniguchi T. Primary cutaneous plasmacytoma. Int J Hematol. 2017;105(5):545–546. doi:10.1007/s12185-017-2203-7
54. Hughes I, Powell AG, Sarireh BA. Intraductal papillary mucinous neoplasm’s 100 most significant manuscripts: a bibliometric analysis. Int J Hepatobiliary Pancreat Dis. 2018;8:1. doi:10.5348/100076Z04DH2018BA
55. Wei JY, Tong HY, Zhu WF, Liu H, Zhang FJ, Yu WJ, et al. Bortezomib in treatment of extramedullary plasmacytoma of the pancreas. Hepatobiliary Pancreat Dis Int. 2009;8(3):32931. Available from: ;8(3):32931. Available from: https://www.ncbi.nlm.nih.gov/pubmed/19502179
56. Madiba TE, Haffajee MR. Sigmoid colon, rectum, and anus [internet]. Wiley; 2016:1308–1314. doi:10.1002/9781118430309.ch112.
57. Chang YL, Chen PY, Hung SH. Extramedullary plasmacytoma of the nasopharynx: a case report and review of the literature. Chang YL, Chen PY, Hung SH. Extramedullary plasmacytoma of the nasopharynx: a case report and review of the literature. Oncol Lett. 2013;7(2):458460. doi:;7(2):458460. doi:10.3892/ol.2013.1712.
58. Fukuhara S, Tazawa H, Okanobu H, et al. Successful treatment of primary advanced gastric plasmacytoma using a combination of surgical resection and chemotherapy with bortezomib: a case report. Int J Surg Case Rep. 2016;27:133136. doi:Fukuhara S, Tazawa H, Okanobu H, et al. Successful treatment of primary advanced gastric plasmacytoma using a combination of surgical resection and chemotherapy with bortezomib: a case report. Int J Surg Case Rep. 2016;27:133136. doi:10.1016/j.ijscr.2016.08.041.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.