Back to Journals » Cancer Management and Research » Volume 14
A Dosimetric Study Comparing Different Radiotherapy Planning Techniques With and Without Deep Inspiratory Breath Hold for Breast Cancer
Authors S Nair S ![]() , Devi VNM, Sharan K, Nagesh J
, Devi VNM, Sharan K, Nagesh J ![]() , Nallapati B, Kotian S
, Nallapati B, Kotian S ![]()
Received 21 July 2022
Accepted for publication 24 November 2022
Published 29 December 2022 Volume 2022:14 Pages 3581—3587
DOI https://doi.org/10.2147/CMAR.S381316
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Harikrishna Nakshatri
Sarath S Nair,1,2 V N Meena Devi,1 Krishna Sharan,2 Jyothi Nagesh,2 Brahmaiah Nallapati,2 Shambhavi Kotian3
1Department of Physics, Noorul Islam Centre for Higher Education Kumaracoil, Tamilnadu, India; 2Department of Radiotherapy & Oncology, Kasturba Medical College Manipal, Manipal Academy of Higher Education, Manipal, India; 3Department of Medical Physics, Manipal College of Health Professions, Manipal Academy of Higher Education, Manipal, India
Correspondence: Sarath S Nair, Email [email protected]
Objective: To analyze whether deep inspiratory breath hold (DIBH) would be dosimetrically beneficial irrespective of radiotherapy planning techniques for patients with left breast cancers requiring adjuvant radiotherapy.
Methods: Planning CT scans were taken in free-breathing (FB) as well as deep-inspiration breath hold (DIBH) for patients requiring adjuvant radiotherapy for left breast cancers. After registration, three radiotherapy plans – 3D-conformal radiotherapy (3DCRT), intensity modulated RT (IMRT), and volumetric modulated arc-therapy (VMAT) – were generated for both FB and DIBH scans for each patient. The dose-volume parameters were collected from the dose-volume histogram and analyzed. A paired t-test is used for statistical analysis of the parameters.
Findings: The study was conducted on thirteen patients. The mean dose of the left lung was reduced with DIBH by 32%, 24%, and 6% (8.6 Gy, 6.6 Gy, and 6.4 Gy) with 3DCRT, IMRT, and VMAT, respectively. The mean heart dose was reduced by 3.3 Gy (2.2 vs 5.5 Gy), 2.2 Gy (7.5 vs 9.7 Gy), and 1.2 Gy (5.8 vs 7 Gy) with 3DCRT, IMRT, and VMAT with DIBH. Similarly, the left anterior descending artery (LAD) mean dose was relatively reduced by 80%, 34%, and 20% when compared with the FB scans for 3DCRT, IMRT, and VMAT respectively, with max dose in the 3DCRT plan.
Novelty/Applications: DIBH appears to have maximum benefit in achieving a better sparing of organs-at-risk for patients being considered for 3DCRT, and to a lesser extent with even IMRT and VMAT techniques.
Keywords: deep inspiration breath hold, DIBH, active breath coordinator, ABC, volumetric modulated arc therapy, VMAT, intensity modulated radiation therapy, IMRT, left anterior descending coronary artery, LAD
Introduction
Breast cancer is an important cause of cancer morbidity and mortality in women worldwide. It is a well-known fact that adjuvant radiation therapy is an integral component of therapy in the management of non-metastatic early as well as locally advanced breast cancer.1 3D-Conformal radiotherapy (3DCRT) is the most common technique of adjuvant RT by virtue of its simplicity, but more recent treatment techniques such as intensity modulated radiotherapy (IMRT), volumetric modulated arc therapy (VMAT), tomotherapy, etc offer the potential to reduce volumes of organs-at-risk (OARs) exposed to high doses.2,3 These techniques are more likely to be considered in more complex cases such as patients requiring internal mammary node radiation. Cardiotoxicity resulting from radiotherapy for breast cancers has been associated with morbidity and mortality.4,5 The most common cause of cardiac mortality is ischemic cardiac disease, believed to be the result of radiation exposure to the anterior heart, predominantly the left anterior descending artery (LAD). This makes it pertinent to maximally reduce the radiation dose exposure to organs-at-risk (OARs). However, optimum dose reduction of the heart cannot be always achieved with these new techniques. Advanced techniques can arguably reduce the volume of heart and lung exposed to high radiation doses. Nevertheless, there are several unanswered questions with these treatment techniques, the most important concern being a higher integral dose. Even though offering higher conformity and superior target coverage, advanced techniques such as IMRT and VMAT are invariably associated with increased low-dose exposure to OARs.3 In this particular scenario, respiratory immobilization plays a vital role in reducing the heart as well as the lung dose to a lesser extent. This can be achieved using gating, tracking, and optimized free breathing modules. Out of these, DIBH breathing gating is the most common module used. There are multiple methods present now to achieve the gating technique, out of which the two most widely used are ABC and RPM. An Active Breathing Coordinator (ABC; Elekta Oncology Systems, Stockholm, Sweden) respiratory gating device allows the patient to breathe in a controlled manner, so that the heart, as well as lung volume dose, can be reduced.6,7 This is usually executed with the deep inspiration breath-hold (DIBH) technique. During both simulation and treatment delivery, the patient takes a deep breath and holds it in for some time to negate respiratory movement, expand the lung, and push the heart away from the chest wall. Some studies have reported that prone breast irradiation could be an alternative for DIBH.8 But prone position immobilization has its own limitations. The second method is by using the Real-Time Position Management (RPM) system (Varian Medical Systems, Palo Alto, CA, USA), where the patient’s breath cycles are tracked using an infrared tracker placed on the patient monitored by a dedicated camera.9 Besides these gating systems, manual gating in DIBH and voluntary breath hold were also commonly used by many departments.
The purpose of this study was to dosimetrically evaluate the additional benefit of different planning techniques such as 3DCRT, IMRT, and VMAT in left breast cancer when used with DIBH, in order to identify if DIBH continued to offer superior OAR dosimetry despite the technique of RT.
Materials and Methods
The study was conducted on patients with left-sided breast cancer reporting for adjuvant radiotherapy to our department after obtaining institutional ethics committee approval. Patients with a history of lung and/or heart diseases and those who could not execute DIBH were excluded. Informed consent was taken from all patients prior to recruitment. The eligibility criteria are given in Table 1. Patients with left sided-breast cancers who were able to comprehend the breath-hold procedure, and were able to hold breath for at least 20 seconds at a stretch, were included. The desired breath-hold threshold was 1.25 liters. Edentulous patients who could not hold the mouthpiece, those with respiratory comorbidities which precluded the required breath-hold duration, and patients planned for simultaneous integrated boost techniques were excluded. Patients were immobilized either by using a vacuum cushion or by breast board, in a supine position with both hands above the head. All patients were trained to execute breath-hold through the mouthpiece attached to the spirometer with a filter kit, which is of single use (shown in Figure 1A).
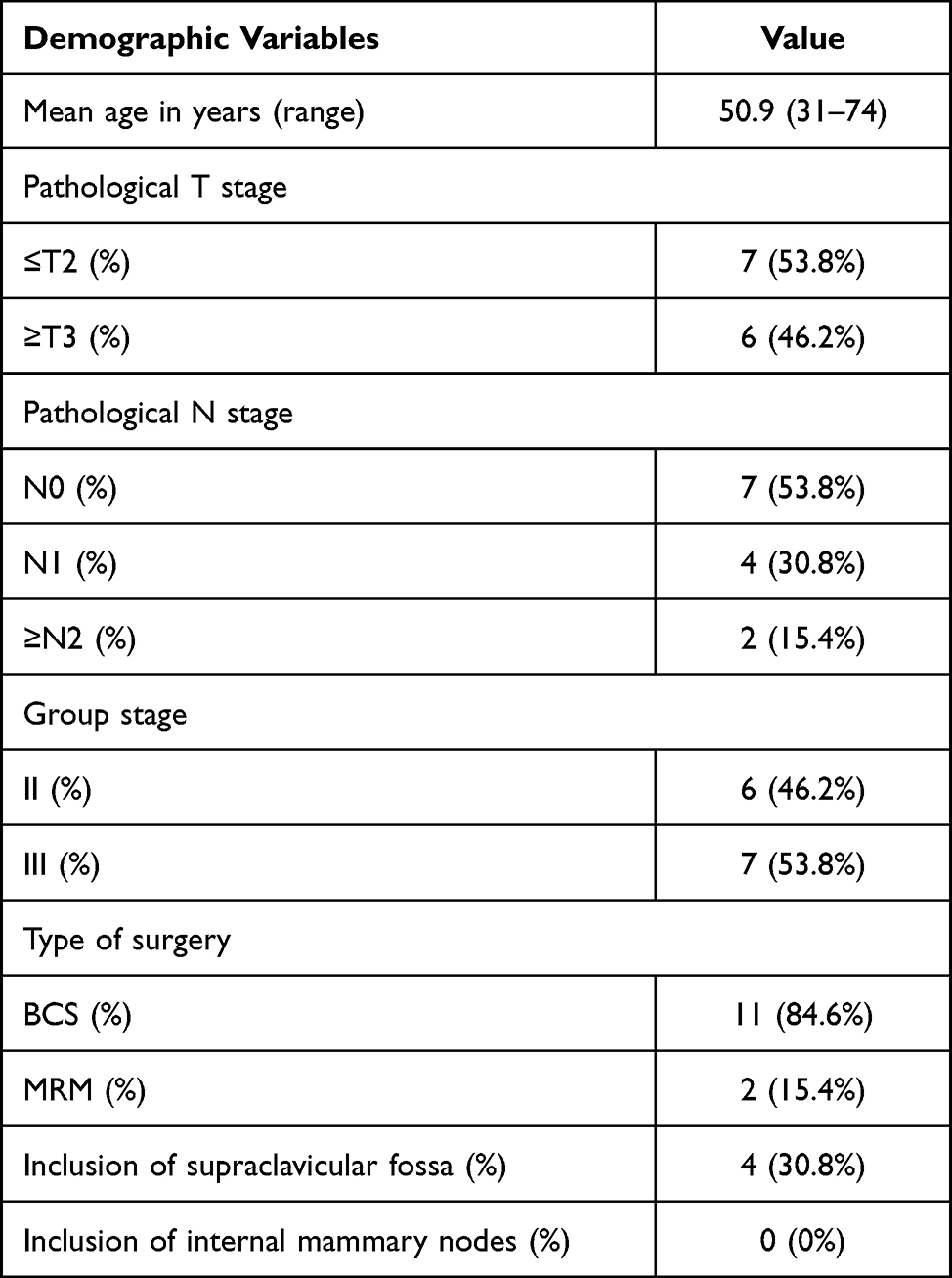 |
Table 1 Patient Inclusion Criteria for the Study |
 |
Figure 1 Main parts of ABC gating (Elekta): (A) spirometer, (B) ABC gating monitor. |
Breath taken through the mouthpiece is monitored by a spirometer, an integral part of the Active Breath Coordinator (ABC) device (Elekta, Stockholm, Sweden), that monitors the airflow in a controlled threshold volume and time to maintain a predefined lung volume and breath-hold time for each patient. A screen attached to the gating device monitors the respiratory cycle of the patients (Figure 1B).
Once the patient was able to adequately execute DIBH, planning computed tomography images were taken with 3 mm slice thickness for free-breathing (FB) and DIBH in a Philips brilliance 16 big bore CT machine. Free-breathing images were taken for reference as well as comparison purposes only, and patient treatment was executed with DIBH only. Volume delineation of the target and OAR in each image set was done as per standard RTOG contouring protocol in the Monaco contouring station. For each patient image set, 3DCRT, IMRT, and VMAT plans were generated. The Monaco 5.11 Treatment Planning System with collapsed cone and Monte Carlo algorithm was used for planning. All patients were planned for hypofractionated whole-breast/chest-wall RT of 42.5 Gy in 16 fractions using 6 or 10 MV photon beams. All patients were contoured and plans were generated by the same oncologist and physicist in order to reduce inter-personal errors.
For 3DCRT, two oblique-opposed tangential beams were used, and an anterior–posterior beam was placed for the supraclavicular field. For IMRT, five beams (330°, 10°, 50°, 100°, 150°) were used and for VMAT a double arc of 200° arc was used. Dose-constraint parameters and identical beam parameters were used for FB and DIBH image sets for planning purposes. Once the treatment plan achieved the prescribed constraints, it was reviewed by the treating oncologist for approval and execution. The dose distribution of the 3DCRT planning technique in DIBH and FB is given in Figure 2A and B with IMRT and VMAT planning in ABC gating in Figure 3A and 7B.
 |
Figure 2 3DCRT planning in both modules: (A) 3DCRT planning in DIBH ABC gating, (B) with free breathing module. |
 |
Figure 3 Planning in DIBH gating module: (A) IMRT plan in DIBH ABC gating module, (B) VMAT plan in DIBH ABC gating. |
The dose-volume parameters for each OAR such as the left and right lung, heart, LAD, and target volumes were recorded for each patient. Once the plan was verified and approved, a dose-volume histogram was generated, and parameters such as mean dose, V10, and V20 for the heart, mean dose, V20, and V30 for the lung, and mean and maximum doses for LAD were recorded. The heterogeneity index and conformity index for the target were directly calculated from the Treatment Planning System, wherein the heterogeneity index describes the uniformity of dose within a target volume, calculated as ratio of dose received by 5% volume divided by the dose received by 95% target volume and the conformity index describes the degree to which the prescribed dose confirms the target volume, derived from the prescription isodose volume divided by the PTV volume with both an ideal value of one.10 For statistical analyzing, paired t-test was used to compare and was considered significant if the P‐value was <0.05.
Results and Discussion
A total of thirteen patients' (six patients with stage IIA, four with stage IIIB, and three with stage IIIA) data were taken up for comparison of FB and DIBH dosimetry. While target and other OAR volumes were found to be similar between FB and DIBH scans, as expected, the lung volume increased with DIBH by an average of 39% and 28% on the left and right sides respectively when compared with FB. The change in contour volumes in both methods with its statistical significance is given in Table 2.
 |
Table 2 Organ-at-Risk and Target Volumes in DIBH and Free Breathing Method with Its Statistical Significance |
The dose-volume parameters for the heart, right and left lung, left anterior descending artery (LAD), and PTV of individual patients were collected and compared for different planning technique with DIBH and FB using the cumulative dose-volume histogram (DVH) shown in Table 3. While all plans had an improvement in terms of OAR sparing when DIBH was used, the 3DCRT technique best benefitted the most from it. Moreover, the volume of OARs irradiated, especially volumes exposed to low doses, had substantially reduced with the combination of 3DCRT and DIBH.
 |
Table 3 Comparison of Dose Exposure in Free-Breathing (FB) and Deep-Inspiratory Breath-Hold (DIBH) with the Three Treatment Techniques |
Also, while maintaining the predefined adequacy of target coverage of V95 >95%, 3DCRT was found to consistently provide the lowest dose exposure to all OARs. The only exception was maximum dose to the LAD which was slightly lower with VMAT (25 Gy vs 31 Gy), though the difference in mean dose was more striking in favor of 3DCRT (5 Gy vs 15 Gy), suggesting that the overall dose exposure to LAD is least with it. In contrast, the maximum dose to LAD was highest with free-breathing 3DCRT plans. Similarly, a reduction in mean heart dose was noted in all three planning techniques when DIBH was implemented, with both the lowest absolute doses and relative dose reduction being best-achieved with 3DCRT. The relative dose difference was reduced with more advanced treatment techniques such as IMRT and VMAT. Cardiac morbidity due to ischemic disease in breast cancer, especially in left side carcinoma, in radiotherapy is a major long-term toxicity of concern.11,12 Any gating, whether voluntary, moderate, or abdominal breathing maneuvered DIBH, could dramatically reduce the dose exposure, thereby potentially reduce cardiac morbidity. A study done by Hong et al found that patients treated with DIBH had heart doses less than those with FB.13 DIBH has also been reported to greatly benefit in decreasing dose exposure to the lungs.14–16 A review study comparing FB and DIBH gating during tangential field irradiation found that the mean heart dose was 3.8 Gy with FB compared to 1.59 Gy with ABC, and the mean dose to the LAD was reduced by more than 50% while retaining an equivalent target coverage.17 Other similar studies comparing DIBH and FB have generally focused on either 3DCRT or VMAT. A study done by Heiddi Stranz and Brigittie Zurl to evaluate the impact on heart dose using a 3DCRT plan in free breathing and DIBH found that irradiated cardiac volume can be significantly reduced by the DIBH technique.18 Borst et al state that, using a DIBH protocol in treatment will help in small setup variability with significance heart and LAD dose reduction.19 However, studies on the relative benefit of DIBH with different radiotherapy planning techniques have been limited, and our study suggests the continued benefit of DIBH in reducing OAR doses irrespective of treatment technique used. This makes an important implication on the benefit of DIBH in all patients with left-sided breast cancer requiring radiotherapy.
Regarding the contoured volume, a small decrease in volume of PTV and heart, and a negligible reduction in LAD volume was observed with gating compared to FB. While this variation could be possibly attributed to increased intrathoracic pressure induced by lung inflation, it is also at least partly the result of minor variations in contouring. The variation in volume was not statistically significant, except for the lungs, where there was an expected increase in the average volume by more than a third with DIBH. With regard to the target volume, coverage, 3DCRT provided a marginally lower coverage that was statistically non-significant. However, conformity and heterogeneity indices were best with VMAT, while 3DCRT provided acceptable results. FB and gating appeared to have no impact on conformity and homogeneity indices with specific planning technique.
Our study has several limitations. It was conducted on a small sample size, and none of the patients received treatment to the internal mammary nodes, which pose an even greater challenge in RT planning for breast cancers. Moreover, it does not address the question of patient selection for DIBH. The major drawback with gating is its difficulty in implementing it for all patients. DIBH gating necessitates patient training, and only cooperative patients who can hold breath for a reasonable duration can be selected. Further, another significant problem noticed is in patient setup verification using volumetric cone beam CT acquisition. Adequate time was spent for this, due to the shorten breath hold time (average of 20 sec) a patient can hold, as a result, an average of 3–4 breath breaks were needed to complete one full image acquisition. Not all left breast patients benefit equally from DIBH technique. Therefore, such a technique may be unjustifiably labor intensive in nature and time-consuming as well as unnecessarily expensive.20,21 A study by Ferini et al suggests the possibility of predicting the benefit of DIBH-RT using anatomical patterns.22 Moreover which patients will benefit most from the DIBH technique other than the left breast is also debatable.
Conclusion
DIBH was found to reduce unwanted dose exposure to all the relevant organs-at-risk in radiotherapy for breast cancer. This benefit persisted despite the technique of treatment used for radiotherapy delivery. In our study, a combination of DIBH and 3DCRT planning was found to provide the best plans in terms of reducing OAR dose, while retaining a similar coverage. Despite the benefit being lesser with more advanced radiotherapy planning techniques, namely IMRT and VMAT, DIBH was nevertheless contributing to a potentially clinically relevant relative dose reduction. We conclude that respiratory management using DIBH is a beneficial tool for adjuvant radiotherapy for all patients with left breast cancers, and should be considered especially when 3DCRT planning is used. The results of this study firmly depend on the choice of the beam, its parameters, and optimization time spent for each plan in the treatment planning station.
Ethics Approval and Consent to Participate
Kasturba hospital institutional ethics committee of Manipal, Manipal Academy of Higher Education approved the study (Approval number is −186/2019) and informed written consent was obtained from all subjects. The study was performed following the approved guidelines and complies with the Declaration of Helsinki.
Funding
There is no funding to report.
Disclosure
The authors have no relevant conflict of interest to disclose for the present study.
References
1. Fadavi P, Nafissi N, Mahdavi SR, Jafarnejadi B, Javadinia SA. Outcome of hypofractionated breast irradiation and intraoperative electron boost in early breast cancer: a randomized non-inferiority clinical trial. Cancer Rep. 2021;4(5):e1376. doi:10.1002/cnr2.1376
2. Teoh M, Clark CH, Wood K, Whitaker S, Nisbet A. Volumetric modulated arc therapy: a review of current literature and clinical use in practice. Br J Radiol. 2011;84(1007):967–996. PMID: 22011829; PMCID: PMC3473700. doi:10.1259/bjr/22373346
3. Das Majumdar SK, Amritt A, Dhar SS, et al. A dosimetric study comparing 3D-CRT vs. IMRT vs. VMAT in left-sided breast cancer patients after mastectomy at a tertiary care centre in Eastern India. Cureus. 2022;14(3):e23568. PMID: 35494897; PMCID: PMC9045011. doi:10.7759/cureus.23568
4. Hufnagle JJ, Andersen SN, Maani EV. Radiation therapy induced cardiac toxicity. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022. Available from https://www.ncbi.nlm.nih.gov/books/NBK554453/.
5. Banfill K, Giuliani M, Aznar M, et al; IASLC Advanced Radiation Technology committee. Cardiac toxicity of thoracic radiotherapy: existing evidence and future directions. J Thorac Oncol. 2021;16(2):216–227. PMID: 33278607; PMCID: PMC7870458. doi:10.1016/j.jtho.2020.11.002
6. Desai N, Currey A, Kelly T, Bergom C. Nationwide trends in heart-sparing techniques utilized in radiation therapy for breast cancer. Adv Radiat Oncol. 2019;4(2):246–252. PMID: 31011669; PMCID: PMC6460327. doi:10.1016/j.adro.2019.01.001
7. Lin CH, Lin LC, Que J, Ho CH. A seven-year experience of using moderate deep inspiration breath-hold for patients with early-stage breast cancer and dosimetric comparison. Medicine. 2019;98(19):e15510. PMID: 31083193; PMCID: PMC6531160. doi:10.1097/MD.0000000000015510
8. Verhoeven K, Sweldens C, Petillion S, et al. Breathing adapted radiation therapy in comparison with prone position to reduce the doses to the heart, left anterior descending coronary artery, and contralateral breast in whole breast radiation therapy. Pract Radiat Oncol. 2014;4(2):123–129. PMID: 24890353. doi:10.1016/j.prro.2013.07.005
9. Oh SA, Yea JW, Kim SK, et al. Optimal gating window for respiratory-gated radiotherapy with real-time position management and respiration guiding system for liver cancer treatment. Sci Rep. 2019;9(1):4384. doi:10.1038/s41598-019-40858-2
10. Petrova D, Smickovska S, Lazarevska E. Conformity index and homogeneity index of the postoperative whole breast radiotherapy. Open Access Maced J Med Sci. 2017;5(6):736–739. PMID: 29123573; PMCID: PMC5672112. doi:10.3889/oamjms.2017.161
11. Wennstig AK, Wadsten C, Garmo H, et al. Long-term risk of ischemic heart disease after adjuvant radiotherapy in breast cancer: results from a large population-based cohort. Breast Cancer Res. 2020;22:10. doi:10.1186/s13058-020-1249-2
12. Lim YJ, Koh J. Heart-related mortality after postoperative breast irradiation in patients with ductal carcinoma in situ in the contemporary radiotherapy era. Sci Rep. 2021;11:2790. doi:10.1038/s41598-021-82263-8
13. Hong JC, Rahimy E, Gross CP, et al. Radiation dose and cardiac risk in breast cancer treatment: an analysis of modern radiation therapy including community settings. Pract Radiat Oncol. 2018;8(3):e79–e86. PMID: 28888675. doi:10.1016/j.prro.2017.07.005
14. Bergom C, Currey A, Desai N, Tai A, Strauss JB. Deep inspiration breath hold: techniques and advantages for cardiac sparing during breast cancer irradiation. Front Oncol. 2018;8:87. doi:10.3389/fonc.2018.00087
15. Estolin A, Ciccarelli S, Vidano G, Avitabile R, Dusi F, Alongi F. Deep inspiration breath-hold intensity modulated radiation therapy in a large clinical series of 239 left-sided breast cancer patients: a dosimetric analysis of organs at risk doses and clinical feasibility from a single center experience. Br J Radiol. 2019;92(1101):20190150. PMID: 31265316; PMCID: PMC6732919. doi:10.1259/bjr.20190150
16. Ferdinand S, Mondal M, Mallik S, et al. Dosimetric analysis of DIBH in left-sided breast cancer radiotherapy and evaluation of pre-treatment predictors of cardiac doses for guiding patient selection for DIBH. Tech Innov Patient Support Radiat Oncol. 2021;17:25–31. PMID: 33681484; PMCID: PMC7930610. doi:10.1016/j.tipsro.2021.02.006
17. Kunheri B, Kotne S, Nair SS, Makuny D. A dosimetric analysis of cardiac dose with or without active breath coordinator moderate deep inspiratory breath hold in left sided breast cancer radiotherapy. J Cancer Res Ther. 2017;13(1):56–61. PMID: 28508834. doi:10.4103/jcrt.JCRT_1414_16
18. Stranzl H, Zurl B. Postoperative irradiation of left-sided breast cancer patients and cardiac toxicity. Dose deep inspiration breath-hold (DIBH) technique protect the heart? Strahlenther Onkol. 2008;184:354–358. doi:10.1007/s00066-008-1852-0
19. Borst GR, Sonke JJ, den Hollander S, et al. Clinical results of image-guided deep inspiration breath hold breast irradiation. Int J Radiat Oncol Biol Phys. 2010;78:1345–1351. doi:10.1016/j.ijrobp.2009.10.006
20. Ferini G, Valenti V, Viola A, Umana GE, Martorana E. A critical overview of predictors of heart sparing by deep-inspiration-breath-hold irradiation in left-sided breast cancer patients. Cancers. 2022;14(14):3477. PMID: 35884538; PMCID: PMC9319386. doi:10.3390/cancers14143477
21. Latty D, Stuart KE, Wang W, Ahern V. Review of deep inspiration breath-hold techniques for the treatment of breast cancer. J Med Radiat Sci. 2015;62(1):74–81. PMID: 26229670; PMCID: PMC4364809. doi:10.1002/jmrs.96
22. Ferini G, Molino L, Tripoli A, et al. Anatomical predictors of dosimetric advantages for deep-inspiration-breath-hold 3D-conformal radiotherapy among women with left breast cancer. Anticancer Res. 2021;41(3):1529–1538. PMID: 33788746. doi:10.21873/anticanres.14912
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.