Back to Journals » Journal of Blood Medicine » Volume 17
A Delphi Consensus by Hematologists on the Burden of Treatment on Patients with Severe Hemophilia in Mexico
Authors García Chávez J, Sánchez Jara B, García Lee MT, Moreno González AM, Rodríguez Castillejos C, Villarreal Martinez L ![]() , Maldonado Silva K, Villela Peña A
, Maldonado Silva K, Villela Peña A ![]()
Received 20 February 2026
Accepted for publication 2 June 2026
Published 19 June 2026 Volume 2026:17 591589
DOI https://doi.org/10.2147/JBM.S591589
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Martin H Bluth
Jaime García Chávez,1 Berenice Sánchez Jara,2 María Teresa García Lee,3 Aída Mashenka Moreno González,4 Cecilia Rodríguez Castillejos,5 Laura Villarreal Martinez,6 Karla Maldonado Silva,7 Atenas Villela Peña8
1Servicio de Hematología, Hospital de Especialidades del Centro Médico Nacional La Raza, Ciudad de México, México; 2Servicio de Hematología Pediátrica, Hospital General del Centro Médico Nacional La Raza Instituto Mexicano del Seguro Social, Ciudad de México, México; 3Centro Integral de Hemostasia y Trombosis, Hospital General Regional No. 1 Dr. Carlos MacGregor, Instituto Mexicano del Seguro Social, Ciudad de México, México; 4Servicio de Hematología, Hospital Infantil de México Federico Gómez, SSA, Ciudad de México, México; 5Servicio de Hematología, Hospital Materno Infantil ISSEMYM, Toluca, México; 6Servicio de Hematología, Hospital Universitario, Monterrey, México; 7Subdirección de Hemato-Oncología, Instituto Nacional de Pediatría, Ciudad de México, México; 8Clínica de Hemofilia y Trombofilia, Hospital Regional Ignacio Zaragoza, ISSSTE, Ciudad de México, México
Correspondence: Jaime García Chávez, Servicio de Hematología, Hospital de Especialidades Centro Médico Nacional La Raza, Calle Seris & Zaachila s/n, Colonia La Raza, Alcaldía Azcapotzalco, Ciudad de México, 02990, México, Tel +52 5522609161, Email [email protected]; [email protected]
Purpose: Current treatment of hemophilia still represents an important burden for patients and caregivers. As a consequence, adherence can be poor, thus reducing efficiency of treatment. Then, a modified Delphi method was used to assess the burden of hemophilia treatment in Mexico.
Methods: In the first round, the experts answered online a questionnaire with 32 statements structured in eight sections: overall efficacy of recombinant coagulation factors, delivery of recombinant factors, adherence to treatment with recombinant factors, emotional burden, physical load, interference with daily life, impact of adherence on efficacy, and satisfaction with treatment. Each statement was qualified from “Totally disagree” to “Totally agree”. In the second round, those statements with less than 70% agreement between experts were discussed.
Results: Consensus was reached in more than half of the questions. There was a consensus on the limited efficacy of current treatments, the complexity of preparation and administration of the recombinant coagulation factors, and the negative effect of the emotional burden, among other statements. Answers to the section related to the impact of adherence on efficacy showed the concern of experts about this issue.
Conclusion: The burden of prophylactic hemophilia treatment on patients and caregivers in Mexico is substantial. Its negative effects on adherence and efficacy of treatment require evaluation of new approaches to hemophilia treatment.
Keywords: hemophilia, burden of treatment, adherence, efficacy, satisfaction with treatment
Introduction
Hemophilia is a hereditary hemorrhagic disorder linked to X chromosome and caused by a deficiency in coagulation factor VIII (hemophilia A, 80% of patients) or IX (hemophilia B, 20% of patients).1 It is characterized by prolonged and excessive bleeding that can be spontaneous or post-traumatic, even after minor injuries. Bleeding-derived complications include chronic pain, severe joint damage, disability, and reduced quality of life.1–3 According to the World Federation of Hemophilia, in 2024 there were globally 271,918 identified patients with hemophilia, mainly with hemophilia A (224,353 patients). They were mostly of male sex, although 10,877 (4%) were of female sex and in 16,315 patients (6%) sex was unknown.4 Also in 2024, Mexico reported 6691 patients with hemophilia from a national population of 130,861,007. Hemophilia A was diagnosed in 5491 patients and was more frequent in patients between 19 and 44 years (51%). Besides, 792 patients had hemophilia B, while in 364 patients hemophilia type was unknown.4
However, all over the world the number of identified vs. expected hemophilia patients did not match. For the Americas, there were 63,843 identified patients (37,440 excluding Canada and the United States), but the expected number was 102,271.4 Therefore, only 62% of expected patients had been diagnosed, suggesting a huge underdiagnosis of 38%.
Hemophilia management should be multidisciplinary with a team of professionals from different fields, from nurses, psychologists, dental surgeons, and orthopedists to physiotherapists, social workers, nutritionists, sport medicine specialists and genetics and laboratory specialists,5 under the coordination of a hematologist, and all of them with expertise in bleeding disorders.1,2,5 The composition of the multidisciplinary team for hemophilia management varies according to the specific healthcare facility. The involved services may differ based on the type of public health insurance and the hospital’s classification. In Mexico, facilities without specific services typically coordinate referrals to the appropriate higher-level reference center. Pharmacological treatment aims to prevent bleeding with long-term prophylaxis and to control bleeding episodes.2 The basis of traditional prophylaxis treatment is replacement therapy with the intravenous infusion of the corresponding deficient clotting factor concentrate (CFC), using recombinant or plasma-derived products.1,2 More recently, CFCs with extended half-life products are available, as well as the factor VIII mimetic agent emicizumab. This is, a bispecific monoclonal antibody, administered subcutaneously for the prophylaxis of hemophilia A, that binds to factor IXa and factor X to generate factor Xa, which translates into thrombin generation.6 Current treatments are more effective and safer than older therapies, but they still represent a significant burden for patients and caregivers. Home treatment can be beneficial, but it demands specific skills and entails an infection risk related to intravenous access.
In Mexico, the therapeutic landscape for hemophilia patients has evolved significantly over the years. Following the introduction of prophylaxis with standard half-life factor concentrates, patients required administration every 48 to 72 hours. To address the resulting treatment burden, protocols were adjusted across several hospitals to provide a one-month supply per patient; this reduced hospital visits to once monthly for medication dispensing and clinical evaluation, with medical appointments eventually extended to every two months. In recent years, the implementation of home delivery services for factor concentrates has further optimized care, allowing for medical consultations every two to three months while ensuring the continuity of treatment at home. Under current protocols for non-replacement therapies, patients are scheduled for medical evaluation and treatment provision every one to three months, depending on individual clinical judgment. Despite these improvements, with many patients receiving a one-to-two-month supply of therapy or, alternatively, benefit from home delivery programs, burden of hemophilia is still substantial, with patients requiring several visits to hospital per week and spending a great deal of time. This burden is a barrier for patients, compromising their adherence to treatment, and resulting in poor clinical evolution and greater joint damage. The burden of hemophilia treatment is a challenge for clinicians and health authorities because it can reduce adherence and, ultimately, impaired treatment outcomes.7 Despite of its consequences, the burden of treatment for patients with hemophilia and their caregivers has not been extensively studied. There are few international papers on this issue8 and almost no data from Mexico.
The main objective was to assess the burden of treatment on patients with hemophilia in Mexico by a modified Delphi panel composed of hematologists with expertise in hemophilia. Secondary objectives included to identify barriers and challenges in current treatment delivery, to determine the need for innovative therapies and enhance the access to them, to establish consensus on recommendations for managing treatment burden, and provide evidence to the country’s regulatory bodies.
Methods
Modified Delphi Method
The modified Delphi method consisted of the development of the survey questionnaire, the selection of experts, and two rounds. For both rounds, consensus was pre-defined as the coincidence of ≥70% of experts in their answer, which is the more common cut-off value for defining consensus,9 and it could be positive or negative.
Survey Questionnaire
A steering committee formed by three physicians with expertise in rare diseases and hemophilia developed a questionnaire focused on questions to understand the burden of treatment for patients with hemophilia and their caregivers. The questionnaire was composed of 32 statements structured in eight sections: overall efficacy of recombinant coagulation factors, delivery of recombinant factors, adherence to treatment with recombinant factors, emotional burden, physical load, interference with daily life, impact of adherence on efficacy, and satisfaction with treatment. Possible answers for each statement were “Totally disagree”, “Disagree”, “Nor agree or disagree”, “Agree” and “Totally agree”.
Selection of the Delphi Panel Participants
Potential participants should be physicians specialized in hematology, with expertise in hemophilia and practicing in Mexico. They were selected according to their positions, affiliations and publications in the field of hemophilia. According to these criteria, eight experts were identified and contacted with an Email describing the study and inviting them to participate in it. The experts confirmed their acceptance of the invitation to participate in the study. Their practices were mostly in Ciudad de México, whose metropolitan area has the highest population density of the country and is the main Mexican economic hub. The members of the steering committee did not take part in the panel completing the Delphi survey.
Delphi Rounds
In the first round, the questionnaire was sent by Email to the experts in July 2024. Questionnaires were anonymous and the answers were collected and analyzed with Microsoft® Forms®.
The second round was held three weeks later, in August 2024, with a hybrid meeting of the expert panel. All the statements without a consensus in the first round were discussed, with a member of the steering committee acting as an impartial moderator. The experts used their smartphones to read a QR code to access to Microsoft® Forms® and introduce anonymously their answers. Furthermore, this software created stacked bar charts based on the results of the first and second rounds.
Results
Eight experts agreed to participate in the study. They were 7 women and 1 man. The group comprised 5 pediatric hematologists and 3 adult hematologists. The experts had between 4 and 34 years of experience with patients with hemophilia, saw between 16 and 425 patients with hemophilia per year, and worked at public and/or private healthcare centers.
A consensus was achieved for 12 statements in the first round. The remaining 20 statements were discussed in the second round trying to reach a consensus for each one. Finally, a consensus was reached for 19 statements from the initially proposed 32 ones (Table 1).
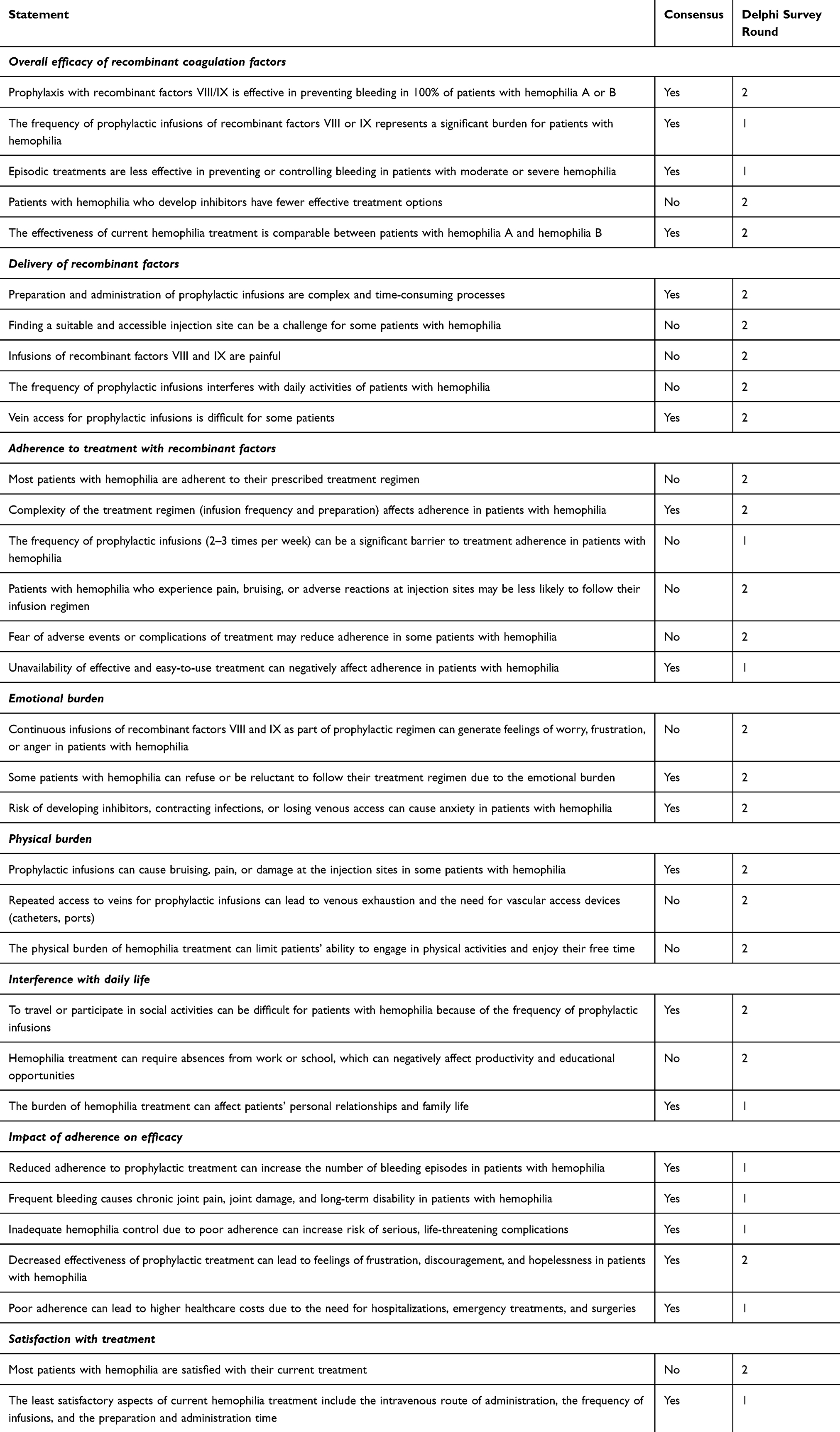 |
Table 1 Final Results of the Delphi Questionnaire |
Overall Efficacy of Recombinant Coagulation Factors
Consensus was reached for all items in this section but one (Figure 1). The expert panel considered that prophylaxis with recombinant factors VIII/IX is not effective in preventing bleeding episodes in 100% of patients with hemophilia A or B. The experts suggested several reasons for rejecting this statement. First, treatment effectiveness is not the same in all patients because of individual factors such as presence of inhibitors, disease severity and adherence to treatment. Second, a standard regimen is not universally appropriate, because some patients need dose adjustments or changes in infusion frequency. In addition, subclinical bleeding can cause joint damage and is not always prevented by prophylactic treatment. Finally, a subset of patients with hemophilia A or B without inhibitors fails to respond to replacement therapy despite receiving appropriately calculated doses. This lack of response may be attributed to multiple factors, such as increased factor clearance or other interindividual pharmacokinetic variations. The frequency of prophylactic infusions of recombinant factors VIII or IX represents a significant burden for patients with hemophilia and interferes with their daily activities, especially in children. The expert panel unanimously believed that, as it is supported by literature, episodic (on-demand) treatment is less effective in preventing or controlling bleeding in patients with moderate or severe hemophilia.10
 |
Figure 1 Overall efficacy of recombinant coagulation factor. |
There was no consensus on a reduction of effective treatment options for patients with hemophilia that develop inhibitors. However, percentages of “Agree” and “Totally agree” answers were 37.5% and 62.5%. These percentages were in line with the opinions expressed during the second round: patients with inhibitors have limited treatment options. The main choice for prophylaxis treatment in patients with hemophilia A is emicizumab using bypassing agents in bleeding events.
For patients with hemophilia B, options are even more limited, because no agent similar to emicizumab is available. Furthermore, access to these treatments can be difficult and expensive, especially within low-resource healthcare systems.
The last statement referred to effectiveness of current hemophilia treatment, which the expert panel considered as not completely comparable between patients with hemophilia A and hemophilia B. As stated above, patients with hemophilia B who develop inhibitors have fewer effective treatment options compared to patients with hemophilia A. However, gene therapy has shown more promise in hemophilia B than in hemophilia A, which could change the treatment landscape in the future. Second, there is a perception that patients with hemophilia B have a less severe bleeding phenotype than patients with hemophilia A, which may influence the intensity of treatment regimens. Lastly, there is more information on hemophilia A than on hemophilia B.
Administration of Recombinant Factors
No consensus was reached for most statements in this section (Figure 2). Preparation and administration of prophylactic infusions are complex and time-consuming processes. However, complexity can vary depending on the expertise and skill of caregivers or patients, and the same process can be more challenging for some families than for others. For caregivers, especially mothers, daily delivery of the coagulation factor can mean a huge burden that affects their daily routine and time use.
 |
Figure 2 Delivery of recombinant factors. |
In a strict manner, there was not a consensus on “Finding a suitable and accessible injection site can be a challenge for some patients with hemophilia”, but 87.5% of experts agree or totally agree with the statement. Another statement without consensus was “Infusions of recombinant factors VIII and IX are painful”, although all experts agreed or totally agreed with it. A similar result was seen for “The frequency of prophylactic infusions interferes with the daily activities of patients with hemophilia”, a statement without consensus but with all experts declaring to agree (most of them) or totally agree. Frequent infusions can interfere with daily activities of patients, with a special impact on children and adolescents that should coordinate treatment with school schedules and extracurricular activities. In addition, involvement of patients in physical and social activities can be impaired because they can feel less protected on days without infusion.
There was consensus on the difficulty for some patients in achieving vein access for prophylaxis infusions.
Adherence to Treatment with Recombinant Factors
Adherence to prescribed treatment regimen is low in most patients with hemophilia (Figure 3). It is expected that only around 50% of patients with hemophilia have good adherence to their treatment. Pediatric patients demonstrate superior adherence rates compared to adults, as caregivers ensure treatment compliance.
 |
Figure 3 Adherence to treatment with recombinant factors. |
According to the experts, the main factor impairing adherence is the complexity of treatment, including both preparation and frequency of infusions. Furthermore, pain, bruising and other adverse events at the injection site, as well as fear of adverse events, can reduce adherence. Accordingly, some patients applied less dose or change days or timing of infusions without consulting their doctors. Other reasons for poor adherence and even withdrawal are the anxiety in patients and families caused by wrong information on potential adverse events, as well as the fear of developing inhibitors against the coagulation factor.
The unavailability of effective and easy-to-use treatments of hemophilia can also reduce adherence.
Emotional Burden
Most participants considered that continuous prophylactic treatment with infusions of recombinant factors VIII and IX can generate feelings of worry, frustration, or anger in adolescents and adults with hemophilia, especially if they do not perceive an immediate improvement or did not have severe complications of hemophilia. Furthermore, the risk of developing inhibitors, contracting infections, or losing venous access, as well as a switch in therapy, can cause anxiety in patients with hemophilia. Treatment-derived emotional burden can be too hard to support for some patients and consequently, they can refuse or be reluctant to follow the prescribed therapy (Figure 4).
 |
Figure 4 Emotional burden. |
Physical Burden
Experts agreed that prophylactic infusions can cause bruising, pain, or damage at the injection sites in some patients with hemophilia (Figure 5). However, no consensus was reached on venous exhaustion and the need for vascular access devices (catheters, ports) caused by repeated venous access for prophylactic infusions. Some factors are related to venous exhaustion, including the age of patients, with higher difficult venous access in little children and obese adults, and repeated use of the same vein.
 |
Figure 5 Physical burden. |
The physical burden of hemophilia treatment could limit physical activities of patients and prevent them from enjoying their leisure time. Moreover, the frequency of infusions and treatment preparation can interfere with daily activities of patients.
Interference with Daily Life
There was a consensus on how difficult it is for patients to travel or participate in social activities because of the frequency of prophylaxis infusions. When on a trip, patients with hemophilia should have asked their doctor for a list of all items needed (vials, syringes…). They should also have a case or device at their disposal to store and maintain the treatment at cold temperature during all the required time. Furthermore, there was almost a consensus on the absences from work or school related to hemophilia treatment, which can reduce productivity and educational opportunities. Finally, the burden of hemophilia treatment can affect personal relationships and family life of patients with hemophilia (Figure 6).
 |
Figure 6 Interference with daily life. |
Impact of Adherence on Efficacy
A consensus was achieved for all the statements in this section (Figure 7), mainly in the first round. Poor therapy adherence has a negative impact on the efficacy of prophylactic treatment of hemophilia. It can increase the number of bleeding episodes and therefore morbidity in hemophilia, as frequent bleeding causes chronic joint pain, joint damage, and long-term disability. Furthermore, inadequate hemophilia control due to poor adherence can increase the risk of serious, life-threatening complications. There can also be an impact on mental health, because decreased effectiveness of prophylactic treatment can lead to feelings of frustration, discouragement, and hopelessness in patients with hemophilia. Additionally, poor adherence and the resulting decreased efficacy can lead to higher healthcare costs related to the need for hospitalization, emergency treatments, and surgeries.
 |
Figure 7 Impact of adherence on efficacy. |
Satisfaction with Treatment
Almost all the experts (87.5%) agreed or totally agreed with the idea that most patients are satisfied with their current treatment (Figure 8). The least satisfactory aspects include the intravenous route of administration, the frequency of infusions and the preparation and administration time. However, although there is always room for improvement, patients generally appreciate having access to effective treatments, especially when compared with the lack of treatment or few available options in the past.
 |
Figure 8 Satisfaction with treatment. |
Discussion
This modified Delphi survey highlights the heavy burden of current hemophilia treatment on patients and caregivers in Mexico. To our knowledge, the burden of treatment in hemophilia has not specifically been assessed by a Delphi panel. Some self-reported questionnaires on the burden of hemophilia treatment have been developed,11,12 but they are not validated for Latin America. Moreover, according to a comment from the experts in the Delphi second round, questionnaires are expensive and time-consuming processes. A modified Delphi survey with an expert panel was believed to be the best option, as the Delphi technique is useful to identify issues of interest and to reach consensus on a specific point by a group of experts.13 Results of this modified Delphi survey could be valid not only from the scientific point of view, but also to Mexican health authorities. Besides, the Delphi technique allows participation of experts from different geographical areas.13 In the present Delphi survey, differences between expert opinions can be due to the healthcare segmentation in Mexico.
Furthermore, there is limited data on hemophilia treatment burden from patient-reported experience measures. Nevertheless, studies conducted in populations of patients with hemophilia and their caregivers have also found an important treatment burden. In the explorer6 study, conducted in 33 countries all over the world and with a small Mexican participation (n = 4),14 231 patients with hemophilia answered the Hemophilia Treatment Experience Measure (Hemo-TEM) questionnaire.11 The highest treatment burden, as reflected in higher Hemo-TEM score, corresponded to patients with hemophilia A or B that had developed inhibitors or were treated episodically.14 In another international real-world study conducted in Canada, France, Germany, India, Italy, Saudi Arabia, Spain and the United States,8 495 patients with severe hemophilia answered also the Hemo-TEM questionnaire. The higher treatment burden was for patients treated with standard-release CFC compared to those treated with extended-release CFC or non-factor therapy. However, all patients experienced treatment burden in the five domains of the questionnaire (injection difficulties, physical impact, treatment bother, interference with daily life, and emotional impact). Pain during or after injection, and issues related to storing, preparing and administering treatment were the main factors in treatment burden.8 On the other hand, according to the Cost of Hemophilia in Latin America: A Socioeconomic Survey (CHESS LATAM) study, patients with severe hemophilia bear a large cost-related treatment burden.15 A Mexican study also found an important economic impact.16 Accordingly, a limitation of the present Delphi survey could be that it did not include direct opinions of patients and caregivers. However, the experts agreed that, in our country, patient treatment satisfaction is assessed through direct clinical interviews during medical consultations or via spontaneous patient reports. Patients frequently express their perceptions of therapy during visits; notably, some inquire about therapeutic alternatives upon becoming aware of emerging hemophilia treatments. Therefore, the experts considered that they were able to talk about feelings and opinions of patients and caregivers.
Treatment burden in complex regimens, including time for preparation, route of administration and frequency of infusion, could affect adherence in hemophilia.17 In addition, adherence is related to outcomes. In a systematic review, 15 studies of a total of 20 found a relationship between good adherence and better outcomes in patients with hemophilia.7 Benefits of better adherence varied between studies and included reduced bleeding risk, improvements in chronic pain and joint structure and function, and better quality of life among others. Moreover, seven studies found a relationship between low adherence and increased bleeding.7 Poor adherence not only could lead to worse outcomes, but it could also increase healthcare costs from a higher number of visits to hospital or emergency room and hospitalizations.
As treatment burden negatively impacts on adherence and hence efficacy of treatment, the experts considered essential to implement some strategies to enhance adherence. Because long-term hemophilia treatment causes physical and emotional adverse events, early education of patients and caregivers is paramount. There are two transition periods especially challenging for adherence: when adolescents begin self-treatment and when young adults initiate an independent life away from their parents.18 Other ways to enhance adherence are performing a close follow-up, achieving the involvement of a multidisciplinary team, and providing psychological support. Reducing physical and emotional burden could increase adherence. As regards to the management of hemophilia-related psychological issues in Mexico, recently there has been a concerted effort to further integrate psychological services, as achieving treatment adherence remains a significant challenge in the adolescent and young adult populations. Consequently, these patients are referred to both psychology and social work services; the latter also coordinate programs designed to foster and streamline multidisciplinary care.
Other measures to improve adherence could be using agents with extended half-life and expanding the classes of available treatments. Factor VIII-mimetic agents, such as emicizumab, have enhanced the management of hemophilia A with and without inhibitors as they can reduce treatment burden.19 Furthermore, there are promising new hemophilia treatments, such as anti-TFPI (tissue factor pathway inhibitor) monoclonal antibodies like marstacimab20 and concizumab,21 or anti-thrombin inhibitors like fitusiran, a small interfering RNA technology.22 These new agents could be useful in hemophilia A and B, even in patients with inhibitors.19 Besides, they do not require intravenous route or frequent administration and therefore they could reduce treatment burden, which could result in an enhanced adherence. An example of these new therapies is marstacimab, the first FDA-approved anti-TFPI antibody for prophylaxis in hemophilia A and B without inhibitors,23 which is administered once-weekly subcutaneously.20 These new agents could also enhance the quality of life of patients and caregivers, that is reduced in hemophilia.24,25 Furthermore, availability of new treatments could change hemophilia care by Mexican public health system, with higher availability and easier access to therapies, as well as more relaxed follow-up schedules.
Conclusions
The burden of prophylactic hemophilia treatment on patients and caregivers, perceived by hematologist in Mexico, is still substantial despite the therapeutic advances. Several factors that continue to impose a significant treatment burden on the patient have been identified, including the requirement for intravenous administration; the need for repeated venipunctures every 48 to 72 hours, depending on whether the patient has hemophilia A or B and utilizes standard half-life factors; the fear of self-infusion, and a persistent dependence on others for factor administration. The negative effects of this burden on treatment adherence require new approaches to hemophilia management.
Abbreviations
CFC, clotting factor concentrate. TFPI, tissue factor pathway inhibitor.
Ethic Statement
The study adhered to the ethical principles outlined in the Declaration of Helsinki. No patient data was collected or analyzed; therefore, no review and approval by an IRB or a research committee were needed.
Acknowledgments
The authors wish to thank Dr. Jorge García and Dr. Luis Alberto González for their collaboration in the initial phases of this project. The authors also wish to thank Content Ed Net S.L. and Carmen Acuña-Condal for their help in writing and editing the manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Pfizer financed writing and editorial support, but was not involved in any of the stages from Delphi survey design to submission of the paper for publication.
Disclosure
BSJ, CRC, LV, KMS and AVP declare no conflicts of interest.
JGCH participates as a speaker and has received honoraria advisory boards for NovoNordisk, Pfizer, Roche, Bayer and CSL.
MTGL has received honoraria for advisory boards and/or lectures and support for educational activities from Amgen, Bayer, CSL Behring, Novo Nordisk, Octapharma, Pfizer and Takeda.
AMMG has received honoraria for advisory boards and lectures from Roche, Octapharma, Novo Nordisk and Pfizer.
The authors report no other conflicts of interest in this work.
References
1. López-Arroyo JL, Pérez-Zúñiga JM, Merino-Pasaye LE, et al. Consensus on hemophilia in Mexico. Gac Med Mex. 2021;157(Suppl 1):S1–12.
2. Berro M, Aparicio R, Arbesú-Ponce MG, et al. Latin American consensus on hemophilia. Hemost y Trombos. 2025;2(1):003–013.
3. García-Chávez J, Abraham MC. Hemofilia [Hemophilia]. Gac Med Mex. 2013;149:308–321. Spanish.
4. World Federation of Hemophilia. Report on the Annual Global Survey 2024. 2025. Available from: https://www1.wfh.org/publications/files/pdf-2525.pdf.
5. Mexico General Health Council. Technical protocol for hemophilia care, 2021. Available from: https://www.gob.mx/cnts/documentos/manual-de-atencion-integral-de-hemofilia?idiom=es.
6. Coppola A, Franchini M, Pappagallo G, et al. Current choices and management of treatment in persons with severe hemophilia A without inhibitors: a mini-Delphi consensus. J Clin Med. 2022;11(3):801.
7. Khanji C, Nuabor W, Gould T, et al. Systematic literature review of outcomes associated with adherence to haemophilia drug therapy. Haemophilia. 2025;31(2):187.
8. Jiménez-Yuste V, Percier C, Shridhar N, et al. Burden of treatment on people with hemophilia: global real-world data. Blood. 2024;144(Supplement 1):5077.
9. Schifano J, Niederberger M. How Delphi studies in the health sciences find consensus: a scoping review. Syst Rev. 2025;14(1):1–21.
10. Nugent D, O’Mahony B, Dolan G. Value of prophylaxis vs on-demand treatment: application of a value framework in hemophilia. Haemophilia. 2018;24(5):755–765.
11. Brod M, Bushnell DM, Neergaard JS, Waldman LT, Busk AK. Understanding treatment burden in hemophilia: development and validation of the Hemophilia Treatment Experience Measure (Hemo-TEM). J Patient Rep Outcomes. 2023;7(1):17.
12. Brod M, Bushnell DM, Busk AK, Neergaard JS. Development and validation of the Child Hemophilia Treatment Experience Measure: a new observer-reported outcome measure. Haemophilia. 2025;31(1):48–62.
13. Shang Z. Use of Delphi in health sciences research: a narrative review. Medicine (Baltimore). 2023;102(7):E32829.
14. Windyga J, Apte S, Frei-Jones M, et al. Disease and treatment burden of patients with haemophilia entering the explorer6 non-interventional study. Eur J Haematol. 2024;113(5):631–640.
15. Evans J, Burke T, Skerritt M, et al. Impact of severe hemophilia on costs and quality of life in South American men: findings from the CHESS LATAM study. Value Heal Reg Issues. 2025:
16. Carlos-Rivera F, Gasca-Pineda R, Majluf-Cruz A, García-Chávez J. Impacto económico de la Hemofilia tipo A y B en México [Economic impact of hemophilia type A and B in Mexico]. Gac Medica Mex. 2016;152(1):19–29 Spanish.
17. Thornburg CD, Duncan NA. Treatment adherence in hemophilia. Patient Prefer Adherence. 2017;11:1677–1686.
18. Srivastava A, Santagostino E, Dougall A, et al. WFH guidelines for the management of hemophilia, 3rd edition. Haemophilia. 2020;26(Suppl 6):1–158.
19. Jimenez-Yuste V. Non-factor therapies for hemophilia: achievements and perspectives. Semin Thromb Hemost. 2025;51(1):23–27.
20. Mokresh ME, Alomari O, Mokresh S, Caliskan CS, Ilter MK. Safety and efficacy of marstacimab in patients with hemophilia A and B: a systematic review and meta-analysis. Expert Rev Hematol. 2025;18(8):649–660.
21. Hampton K, Knoebl P, Odgaard-Jensen J, et al. Treatment burden and patient preference in patients with hemophilia A or B with inhibitors on concizumab prophylaxis: results from the phase 3 EXPLORER 7 study. Hematol Transfus Cell Ther. 2023;45:S458–S459. doi:
22. Kenet G, Nolan B, Zulfikar B, et al. Fitusiran prophylaxis in people with hemophilia A or B who switched from prior BPA/CFC prophylaxis: the ATLAS-PPX trial. Blood. 2024;143(22):2256–2269.
23. FDA approves new treatment for hemophilia A or B. FDA News Press Release. 2024. Available from: https://www.fda.gov/news-events/press-announcements/fda-approves-new-treatment-hemophilia-or-b.
24. Osorio-Guzmán M, Gutiérrez-González G, Bazán-Riverón GE, Núñez-Villegas NN, Fernández-Castillo GJ. Percepción de la calidad de vida relacionada con la salud y la depresión en pacientes con hemofilia [Perception of quality of life related with health and depression in patients with hemophilia]. Rev Med Inst Mex Seguro Soc. 2017;55(4):416–422 Spanish.
25. Osorio-Guzmán M, Prado-Romero C, Parrello S. Growing up with haemophilia: quality of life and school functioning of a group of Mexican adolescents. Contin Educ. 2025;6(1):58–73.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Second-Generation Long-Acting Injectable Antipsychotics: A Comprehensive Assessment of Effectiveness, Safety, and Cost
Ifteni P, Petric PS, Popa AV, Teodorescu A, Georgescu R, Manea MC
Neuropsychiatric Disease and Treatment 2026, 22:606817
Published Date: 20 June 2026