Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
A Data-Driven Paradigm for a Resilient and Sustainable Integrated Health Information Systems for Health Care Applications
Authors Epizitone A ![]() , Moyane SP, Agbehadji IE
, Moyane SP, Agbehadji IE
Received 1 August 2023
Accepted for publication 2 November 2023
Published 12 December 2023 Volume 2023:16 Pages 4015—4025
DOI https://doi.org/10.2147/JMDH.S433299
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Ayogeboh Epizitone,1 Smangele Pretty Moyane,2 Israel Edem Agbehadji3
1ICT and Society Research Group, Department of Information and Corporate Management, Durban University of Technology, Durban, South Africa; 2Department of Information and Corporate Management, Durban University of Technology, Durban, South Africa; 3Centre for Transformative Agricultural and Food Systems, School of Agricultural, Earth and Environmental Sciences, University of KwaZulu-Natal, Pietermaritzburg, South Africa
Correspondence: Ayogeboh Epizitone, Tel +27 73-310-9150, Email [email protected]
Introduction: Many transformations and uncertainties, such as the fourth industrial revolution and pandemics, have propelled healthcare acceptance and deployment of health information systems (HIS). External and internal determinants aligning with the global course influence their deployments. At the epic is digitalization, which generates endless data that has permeated healthcare. The continuous proliferation of complex and dynamic healthcare data is the digitalization frontier in healthcare that necessitates attention.
Objective: This study explores the existing body of information on HIS for healthcare through the data lens to present a data-driven paradigm for healthcare augmentation paramount to attaining a sustainable and resilient HIS.
Method: Preferred Reporting Items for Systematic Reviews and Meta-Analyses: PRISMA-compliant in-depth literature review was conducted systematically to synthesize and analyze the literature content to ascertain the value disposition of HIS data in healthcare delivery.
Results: This study details the aspects of a data-driven paradigm for robust and sustainable HIS for health care applications. Data source, data action and decisions, data sciences techniques, serialization of data sciences techniques in the HIS, and data insight implementation and application are data-driven features expounded. These are essential data-driven paradigm building blocks that need iteration to succeed.
Discussions: Existing literature considers insurgent data in healthcare challenging, disruptive, and potentially revolutionary. This view echoes the current healthcare quandary of good and bad data availability. Thus, data-driven insights are essential for building a resilient and sustainable HIS. People, technology, and tasks dominated prior HIS frameworks, with few data-centric facets. Improving healthcare and the HIS requires identifying and integrating crucial data elements.
Conclusion: The paper presented a data-driven paradigm for a resilient and sustainable HIS. The findings show that data-driven track and components are essential to improve healthcare using data analytics insights. It provides an integrated footing for data analytics to support and effectively assist health care delivery.
Keywords: health information system, HIS, data, healthcare, analytics
Introduction
The hallmark digitalised transformation within the healthcare arena has been characterised by the continuous growth of healthcare data, which has been considered complex and dynamic.1 Over time, the global data influx has resulted in many blessings and challenges in several industries, especially healthcare.2,3 Among the blessings is the availability of intelligent decisions and actions to enhance competitive advantage. Many other profitable undertakings that shape organisations, such as data-driven strategies and planning, have been realised in many industries. Concomitantly, there were also many dares in the data. In many areas, issues such as violation of privacy, data structure, and social stratification are some of the known challenges posed by the influx of data, particularly in healthcare.1,4,5 Nevertheless, data within the healthcare sector are highly relevant, and at the same time, data can enhance or sabotage healthcare.
Within healthcare, HIS is a key handler of health-related data. Its deployment has imparted healthcare in many ways in which traditional healthcare systems have been failed. Information and data exchange is one of the main tasks of the HIS, which has been the focus of its offerings within the healthcare industry.1,6 Many processes and healthcare applications have been advanced by HIS.5,7 However, their deployment is not flawless but entrenched with enough dare, which warrants the need for their augmentation.8 Along with this demand for a resilient and sustainable HIS for healthcare is the need for quality data. The need for quality data is one of the reported dares associated with HIS adoption.1,8
Data quality in HIS is fundamental in the execution of knowledge to specialists who rely on it for many processes, such as planning, decision-making and precision healthcare.3,9 The mediating role of HIS within healthcare enables the exchange of data and information that contributes significantly to health.3,10 Despite this, health data within the HIS are considered to be complex and require computational processes that are regarded as challenging.11 Regardless of this premise, the reliance of specialists on health data remains constant due to the fact that many decision-making and planning processes emanate from HIS data. However, many data science applications have been employed to highlight the contributions and potential of data insights in augmenting healthcare.
Extant literature reveals insurgent data within healthcare to be problematic and disruptive and, at the same time, embedded with the potential to revolutionise healthcare.1,3 Several issues, such as data quality, security, and governance, are some of the prominent challenges constantly foreshowed in the healthcare context.12,13 Thus, studies that explore the existing body of research on HIS for healthcare through data lenses are crucial. Therefore, the objective of this paper is to explore the existing body of research on HIS for healthcare through the data lens to present a data-driven paradigm for healthcare augmentation that is paramount to the attainment of sustainable and resilient HIS for healthcare. This study highlights previous data science techniques employed in healthcare. It builds on these prior work to present a data impetus underpinning a resilient and sustainable HIS for healthcare applications, capitalising on the data-driven track to enable sustainable and resilient HIS for healthcare that harnesses data-generated insights to render quality health services.14
This paper is organised into sections that begin with the introduction (1) and an overview of the existing HIS frameworks for healthcare (2). Data-driven paradigm for resilient and sustainable HIS in healthcare (3). Data sources (4). Data actions and decisions (5). Data science techniques (6). Data technique serialisation in HIS (7). The data insights implementation and applications (8). The conclusion (9) that finalizes the paper.
Methods
The methodology adopted in this study was a systematic, comprehensive literature review. This study is conducted systematically to synthesise the extant literature within the context and analyse the content to ascertain the value disposition of data in the HIS in relation to healthcare delivery. Several search engines were used to retrieve related research publications that fit the scope and context of this study. The main database used was the Web of Science. Other databases, such as SCOPUS and Google Scholar, were used to obtain additional relevant work associated with the context. Only articles containing references to the keywords HIS, information, healthcare, health data, and related healthcare systems were analysed scrupulously for inclusion criteria. Publications that were not within the scope or context of the study were excluded. The main exclusion criteria were based on publications that did not constitute a journal or conference proceedings and were not written in English. Articles that did not have the keywords such as health information systems, healthcare and data were also excluded as they did not align with the scope of inquiry. The research materials were aggregated for synthesis following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) framework. This methodology was preferred over others, such as scoping and content review, because it allowed for more in-depth inquest. Figure 1, the PRISMA flow statement, demonstrates the methodological phases of this research, along with the exclusion and inclusion criteria implemented for the study synthesis.
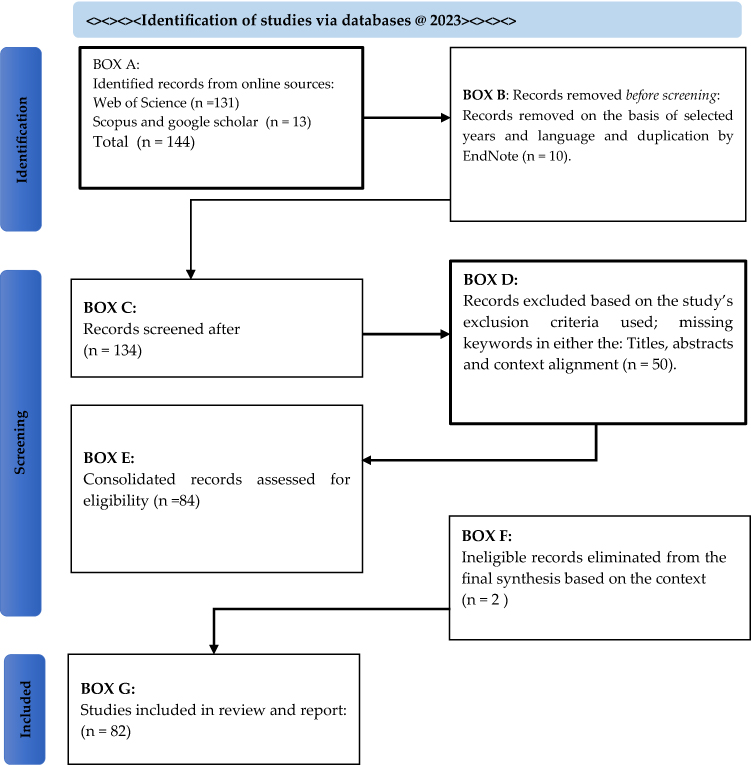 |
Figure 1 Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow statement for the study. |
Related Work and Discussion
His Implemented Frameworks for Health Care Applications
A critical review of the extant literature reveals that many benefits of HIS for healthcare applications are compromised by determinants such as inadequate resources, incompetent staff, data dissemination issues, and investment concerns.9,10,15 Therefore, to harness HIS potential, many authors have presented frameworks for its enactment in healthcare.16–19 However, extant literature has identified the initial design of the information framework as one of the dares for HIS implementation, revealing the fault line revolving around the ease of access and utilisation of the relevant stakeholders.20 Several frameworks have been developed and reported in the discourse on HIS for healthcare applications, many of which have been technologically and socially driven.21,22 A popular framework is the Technological Acceptance Model (TAM) employed in HIS to ascertain the perceptions that drive its adoption.19,23,24 The “Human, Organization, Process and Technology-fit” (HO(P)T-Fit) framework is another that builds on the foundational “Human, Organization, Process and Technology-fit” (HOT-Fit) framework, designed to decrease HIS-induced medical errors and enhance health safety.25 Other frameworks include the information success system model (ISSM),26 task-technology fit – TTF,27 Extended Technology Acceptance model – TAM2,28 Fit between individuals, tasks, and technology (FITT), and unified theory of acceptance and use of technology – UTAUT.29–32 These have been collectively employed in the health arena to drive the enhancement and adoption of HIS for health care applications.19,26
Conceptual and research frameworks were developed along the same line.17,20,33–35 Helwig, Bishop-Williams, Berrang-Ford, Lwasa, Namanya and Grp36 accentuate the importance of HIS evaluation using an eco-health framework that highlights stakeholders’ worth. However, despite the development and implementation of these frameworks, HIS enactment still suffers from major drawbacks that limit its potential in health care applications. As a result, there is evidence of a hiatus that needs to be filled to maximise the potential of HIS in the enhancement of health care applications. Furthermore, while there have been many technological focus frameworks in the current knowledge of HIS, there are limited data-centric frameworks. Consequently, most HIS frameworks are utterly bereft from the perspective of data sciences, which has enormous potential to leverage the contribution of modern-day data analytics. Furthermore, they fail to provide cutting-edge solutions for many problems associated with HIS and healthcare applications. Thus, this study sought to develop a data-driven framework for a resilient and sustainable HIS for healthcare applications to curb some of the HIS dares within the healthcare arena.
A Data-Driven Paradigm for Resilient and Sustainable HIS for Health Care Applications
The impetus for a data-driven paradigm for resilient and sustainable HIS for health care applications is grounded in its evolutionary capabilities, which afford many promising features, such as ease of access, intelligent decision-making, and seamless processes. Mohd Nor, Taib, Saad, Zaini, Ahmad, Ahmad and Dhillon37 asserted the future inference of data mining to healthcare development as a source of opportunities for enhancing healthcare applications. Several applications of data sciences in the healthcare arena have been alluded to provide insight from clinical narratives and unstructured data. Data science techniques such as dimensionality reduction, rule-based mining, natural language processing, machine learning, and deep learning have been employed in many healthcare areas to enhance health care applications.38–41 Computational enhancement applications, such as machine learning, deep learning, and artificial intelligence, have been deployed in many sectors, where their input has afforded quality service delivery. In the healthcare arena, related work such as “natural language processing”, “machine learning”, and “deep learning” has been done.11,42–49 However, there are challenges associated with healthcare data that have led to many shortcomings in computational applications. A study by Flora, Margaret and Dan50 identifies the incapability of qualifying, scrutinising, and using data to plan and manage service delivery. Negro-Calduch, Azzopardi-Muscat, Krishnamurthy and Novillo-Ortiz1 state that the nature of healthcare datasets and its associated nature poses various dares allied with their processing, privacy, security, storage, analysis, data exchange, and usability.
Notwithstanding, Chen, Yu, Hailey and Cui51 theorise that empirical testing and contextual analysis are essential components associated with data collection processes that can be used to develop frameworks for HIS.52 Thus, this study aimed to create a resilient and sustainable HIS for health care applications using a data-driven paradigm. An overview of the data-driven paradigm for resilient and sustainable HIS for health care applications is shown in Figure 2. The figure shows the healthcare environment in which the HIS is deployed.
 |
Figure 2 Data-driven paradigm for a resilient and sustainable HIS for health care applications; Source: Author. |
The deployed HIS is intended to serve healthcare stakeholders at different levels of care and management functions. These modules independently handle functions associated with care and management such as diagnostics, admission, treatment, discharge, and resources allocation. Both Modules directly interact with the health care application processes. These processes in the healthcare environment iterate across four principal functions: planning, engineering, transition, and operations. Every health care application provided by healthcare providers is first and foremost planned, engineered, transitioned, and operated. In the planning phase, what needs to be done is defined. The process is modelled in the engineering phase before it reaches the transition stage, where it is deployed into a practical enactment. The next step is the operation stage in which the actions are executed. Across the environment, data that required analysis are generated. From the data analysed, insights are generated that, when applied, will transform and aid healthcare services. A post-enactment action serves as a surveyor of the entire framework. This captures the sociotechnical premise that posits that technology and human intervention are equally valuable in providing efficient and effective healthcare. This flow demonstrates how data transverses across the environment, indicating the actions to be implemented to attain a resilient and sustainable HIS for healthcare applications.
Data Sources
Contingent to the type of HIS instance, health data output emerges from the health care applications.53–56 These data frequently have been regarded with contentions around many data-associated issues such as the size, access and exchanges.57,58 Azzopardi-Muscat, Kluge, Asma and Novillo-Ortiz59 accentuated the need to strengthen data and information systems for unobstructed interchanges. These needs are anchored in the inability to leverage the vast availability of various health data emerging from the HIS. The extant literature identifies the lack of health data standardisation as a major barrier and the basis of an unprecedented global crisis affecting many nations.57,59 Several reasons for the lack of data definition, calculation, and formats have been associated with the delay in data relay between the HIS and different instances generating data. Coupled with the dearth of integration, interoperability, and trained personnel to manage and utilise these data within the health system have necessitated the need for a data-driven paradigm for resilient and sustainable HIS for health care applications within the healthcare arena.58,60 Thus, case study data revolves around health care applications directly linked to HIS and healthcare stakeholders.
Data Action and Decisions
Data generated from health care applications within the healthcare arena are required to be timely, credible, reliable and actionable to enable decisions that are data-driven as well as to enable considerate monitoring and forecasting within the healthcare setting.50,59–62 Decision-making occurs in different sectors within the healthcare space. For these decisions to be made, data from different modules were targeted in the HIS environment. However, the absence of insight from the data generated within this environment can hinder the effectiveness of decisionmaking and their precision.63 Gesicho and Babic61 reported that data underuse in decision-making at various health system levels is prevalent. Thus, data-driven actions are essential for critical decision-making associated with health care applications and future health challenges.9,35,57,59,64 The extant literature reveals that the foremost action for a data-driven decision is dependent on the mechanism established.51,57,59,63 According to Azzopardi-Muscat, Kluge, Asma and Novillo-Ortiz,59 the impetus of this mechanism is to facilitate data coordination, use, and comparison in both national and international settings to foster effective coordination and centralisation of diverse data sources. Thus, decision-making employed this contraption to assimilate and dissimilate consistent and complete data.43
Furthermore, extant literature posits that data needs and related processes associated with their flow must be defined to enforce the rapid intervention needed for health care enhancement.42,43 Figure 3 illustrates the pathway of effectors’ decision-making supported by the HIS emerging from the data provided. The decision pathway espoused by Panerai65 demonstrates that the foremost data tract influences the healthcare sector. This track stems from the data generated primarily from the determinants of health and flows through the HIS environment, necessitating an action that requires decision-making. However, it identified political, environmental, social, technological, economic, and legal (PESTEL) constraints that affect decision-making in the healthcare system. Health policy, resource allocation, and health services are effectors determined by decisions emanating from environmental data. The overall impact depends on the population, including health levels, equity, and satisfaction. The data inference maintains a stronghold for effectors and the people in the HIS environment.
 |
Figure 3 Effectors decision making pathway supported by HIS (Source; Panerai 2014). |
Data Science Techniques
The emergence of data sciences, in conjunction with statistics and science, has been subsidised to deal with the plethora of data surges. Extant literature has heralded it as a multimodal paradigm that incorporates knowledge production and scientific discovery.12,66,67 It is also considered to have evolved as a function to curb many ill-defined qualms associated with data, regardless of the discipline. Priestley and McGrath66 posited these applications to be the catalysts emerging from the fusion of statistics and computer science at their peripheries, fashioning an academic “heterosis” that retort to the emergence of a novel problem set, for which the different silo discipline was ill-equipped to tackle. Thus, data science is an umbrella of computerised applications that provide analytical insights when deployed.68 It is posited to provide descriptive, predictive, and prescriptive analytics that deliver outcomes for precise and imprecise problems and challenges.69–72 Specifically, it provides insights into happenings to ascertain a well-defined outcome, predict future outcomes accurately, and enable the best possible decisions and actions.73–75 Thus, within the healthcare arena, the employment of data science affords health analytics that entail a vast majority of applications that enhance health care applications through prevention, diagnosis, and streamlining operations.66,73,76 However, despite these impactful offerings and promises of data science capabilities, “datafication” within the healthcare setting is considered a source of data-centric dares and prospects.66 Jeffery, Pagano, Hemingway and Valadez77 associate meagre outcomes and verdicts with data impediments such as quality.
Nevertheless, powerful applications of data science techniques in healthcare have revolutionised healthcare applications.76 These techniques, spanning the pre-processing of data and exploratory data analysis to modelling data, have proven indispensable for healthcare analytics that enhance health care applications. In a data-driven paradigm, these techniques are proposed for incorporation into the HIS to render it sustainable and resilient in pursuing quality health care. Table 1 presents some instances of different data science techniques employed in the healthcare arena for health care applications.
 |
Table 1 Data Sciences Techniques Deployed in the Health Arena for Health Care Applications |
The Serialization of Data Science Techniques within the Health Information System
There have been many applications of data science techniques within the healthcare arena to provide insights needed to transform health care delivery. Many of these applications have been applied to data emerging from the HIS and experimented with outside its milieu. The need to incorporate serialisation of data science techniques within the HIS provides a direct stream to implement insights from data and support intelligent decisions. Implementing this will address many of the existing challenges in the healthcare arena. Benefits, such as reduced time and intelligent decision support, will be enacted within the healthcare arena for HIS and health care applications. These will subsequently afford and enable ubiquitous HIS support for health care and health management modules as well as health care applications. Across the different nodes within the HIS, the data analytics serialisation converts the insights generated from the data analysis and channels to the appropriate area where they can be utilised to enhance health care applications.
Data Insights Implementation and Applications
The contribution of HIS data is paramount to delivering efficient and quality health care applications, and it has been alluded to as substantial in development within the healthcare arena.78 The integration of data science techniques, such as machine learning modelling and artificial intelligence that focuses on data, is also considered paramount to the attainment of resilient and sustainable HIS for health care applications. Many insights generated from application data science techniques have been successfully portrayed and deployed to address health care application challenges. Although many computational system designs are emerging with a keen anchor in data sciences, a lack of incorporation of the generated insight into the computational pipeline is evident within the healthcare space. This phenomenon is apparent in HIS, where data heterogeneity is a practical challenge hindering integration.79 Thus, a resilient and sustainable HIS for health care applications is envisioned to incorporate intensive data analysis and modelling for intelligent and ambient healthcare. Combining these capabilities afforded by health technologies to leverage the potential of data analytics to provide practical evidence that can be used to initiate health care applications such as diagnosis and treatment, as well as to prevent and detect occurrences of health care events is indespensable.80 Therefore, the insights emerging from analysed health data can be deployed in all areas associated with and influenced by the data, facilitating health care applications using a data-driven paradigm.3 The enactment of a data-driven paradigm for resilient and sustainable HIS for health care applications is unparalleled in this digitalisation era.81 It serves as a mechanism to uplift current healthcare systems.82
Conclusions
Several applications of data sciences in the healthcare arena have been alluded to provide insight from clinical narratives and unstructured data. Data science techniques that provide descriptive, predictive, and prescriptive capabilities are highly significant for revolutionising healthcare applications. Although HIS have been transforming healthcare practices over the years, there have been significant concerns about their forte and aptitude to be harnessed. Implementing a data-driven strategy is an important step in the realisation of sustainable healthcare, as it provides an integrated footing for data analytics to support and assist effective and efficient health care delivery.
The aim of this study was to explore the existing body of research on HIS for healthcare through the data lens to present a data-driven paradigm for healthcare augmentation that is paramount to the attainment of sustainable and resilient HIS for healthcare. A novel data-driven paradigm for resilient and sustainable HIS in health care applications is recommended to satisfy this aim. The outline of the data-driven paradigm serves as a robust and reproducible pipeline that can be employed to enhance health care applications in the HIS environment. Thus, the data-driven paradigm for a resilient and sustainable HIS converges the collaboration and support of technological advancement to leverage its abilities and potential to employ data insights for health care applications. Future research is required to implement and benefit from data-driven paradigms.
Consent for publication
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Negro-Calduch E, Azzopardi-Muscat N, Krishnamurthy RS, Novillo-Ortiz D. Technological progress in electronic health record system optimization: systematic review of systematic literature reviews. Int J Med Inf. 2021;152:
2. Epizitone A. The Simulation of Big Data to Revolutionize the Effectiveness of Corporate Policy. Interdiscipl J Econ Bus Law. 2022;11:86.
3. El Khatib M, Hamidi S, Al Ameeri I, Al Zaabi H, Al Marqab R. Digital Disruption and Big Data in Healthcare- Opportunities and Challenges. Clinicoecon Outcomes Res. 2022;14:563–574. doi:10.2147/ceor.S369553
4. Prasser F, Kohlbacher O, Mansmann U, Bauer B, Kuhn KA, Consortium D. Data Integration for Future Medicine (DIFUTURE) An Architectural and Methodological Overview. Methods Inf Med. 2018;57(S 01):E57–E65. doi:10.3414/me17-02-0022
5. Abedjan Z, Boujemaa N, Campbell S, et al. Data science in healthcare: benefits, challenges and opportunities. Data Sci Healthcare. 2019;3–38.
6. Isleyen F, Ulgu MM. Data Transfer Model for HIS and Developers Opinions in Turkey. Stud Health Technol Inform. 2020;270:557–561. doi:10.3233/shti200222
7. Epizitone A, Moyane SP, Agbehadji IE. Health Information System and Health Care Applications Performance in the Healthcare Arena: a Bibliometric Analysis. Healthcare. 2022;10(11):2273. doi:10.3390/healthcare10112273
8. Epizitone A. Framework to Develop a Resilient and Sustainable Integrated Information System for Health Care Applications: a Review. Int J Adv Comput Sci Appl. 2022;13(7):477–481.
9. Ahmadi M. Dimensions and Assessment Methods of Data Quality in Health Information Systems. Acta Med Mediterranea. 2017;33(2):313–320. doi:10.19193/0393-6384_2017_2_047
10. Kpobi L, Swartz L, Ofori-Atta AL. Challenges in the use of the mental health information system in a resource-limited setting: lessons from Ghana. Article. Bmc Health Serv Res. 2018;18(1):
11. Digan W, Neveol A, Neuraz A, et al. Can reproducibility be improved in clinical natural language processing? A study of 7 clinical NLP suites. Article. J Am Med Inf Assoc. 2021;28(3):504–515. doi:10.1093/jamia/ocaa261
12. Abu-Salih B, Al-Qurishi M, Alweshah M, Al-Smadi M, Alfayez R, Saadeh H. Healthcare knowledge graph construction: a systematic review of the state-of-The-art, open issues, and opportunities. Review. J Big Data. 2023;10(1):81. doi:10.1186/s40537-023-00774-9
13. Pal SK, Mukherjee S, Baral MM, Aggarwal S. Problems of Big Data Adoption in the healthcare Industries. Asia Pac J Health Manag. 2021;16(4):282–287.
14. Anwar J, Torvaldsen S, Sheikh M, Taylor R. Under-estimation of maternal and perinatal mortality revealed by an enhanced surveillance system: enumerating all births and deaths in Pakistan. BMC Public Health. 2018;18(1):428. doi:10.1186/s12889-018-5363-3
15. Samra H, Li A, Soh B. G3DMS: design and Implementation of a Data Management System for the Diagnosis of Genetic Disorders. Article. Healthcare. 2020;8(3):
16. Braithwaite J, Churruca K, Ellis LA, et al.. Complexity science in healthcare. Sydney: Australian Institute of Health Innovation, Macquarie University; 2017.
17. Dudley L, Mamdoo P, Naidoo S, Muzigaba M. Towards a harmonised framework for developing quality of care indicators for global health: a scoping review of existing conceptual and methodological practices. Review. Bmj Health Care Inf. 2022;29(1):e100469. doi:10.1136/bmjhci-2021-100469
18. Chaney SC, Mechael P, Thu NM, Diallo MS, Gachen C. Every Child on the Map: a Theory of Change Framework for Improving Childhood Immunization Coverage and Equity Using Geospatial Data and Technologies. Article. J Med Internet Res. 2021;23(8):e29759. doi:10.2196/29759
19. Alsharo M, Alnsour Y, Alabdallah M. How habit affects continuous use: evidence from Jordan’s national health information system. Inf Health Social Care. 2020;45(1):43–56. doi:10.1080/17538157.2018.1540423
20. Mezarina LR, Silva-Valencia J, Escobar-Agreda S, et al. Need for the Development of a Specific Regulatory Framework for Evaluation of Mobile Health Apps in Peru: systematic Search on App Stores and Content Analysis. Jmir Mhealth Uhealth. 2020;8(7):e16753. doi:10.2196/16753
21. Kalong NA, Yusof M. Waste in health information systems: a systematic review. Int J Health Care Qual Assur. 2017;30(4):341–357. doi:10.1108/ijhcqa-06-2016-0082
22. Joseph AL, Stringer E, Borycki EM, Kushniruk AW. Evaluative Frameworks and Models for Health Information Systems (HIS) and Health Information Technologies (HIT). Stud Health Technol Inform. 2022;289:280–285. doi:10.3233/shti210914
23. Hoque MR. An empirical study of mHealth adoption in a developing country: the moderating effect of gender concern. BMC Med Inf Decis Making. 2016:1651. doi:10.1186/s12911-016-0289-0
24. Hung MC, Jen WY. The Adoption of Mobile Health Management Services: an Empirical Study. J Med Syst. 2012;36(3):1381–1388. doi:10.1007/s10916-010-9600-2
25. Yusof MM. A Socio-Technical and Lean Approach Towards a Framework for Health Information Systems-Induced Error. IOS Press; 2019:30741248. https://www.scopus.com/inward/record.uri?eid=2-s2.0-85061236878&doi=10.3233%2f978-1-61499-951-5-508&partnerID=40&md5=7e20e2e6cc3ba1efedad66a3283af06f.
26. Ebnehoseini Z, Tabesh H, Deghatipour A, Tara M. Development an extended-information success system model (ISSM) based on nurses’ point of view for hospital EHRs: a combined framework and questionnaire. BMC Med Inf Decis Making. 2022;22(1):71. doi:10.1186/s12911-022-01800-1
27. O’Connor Y, Andreev P, O’Reilly P. MHealth and perceived quality of care delivery: a conceptual model and validation. BMC Med Inf Decis Making. 2020;20(1):41. doi:10.1186/s12911-020-1049-8
28. Omar A, Ellenius J, Lindemalm S. Evaluation of Electronic Prescribing Decision Support System at a Tertiary Care Pediatric Hospital: the User Acceptance Perspective. Stud Health Technol Inf. 2017;234:256–261.
29. van Bussel MJP, Odekerken-Schröder GJ, Ou C, Swart RR, Jacobs MJG. Analyzing the determinants to accept a virtual assistant and use cases among cancer patients: a mixed methods study. BMC Health Serv Res. 2022;22(1):890. doi:10.1186/s12913-022-08189-7
30. Bawack RE, Kamdjoug JRK. Adequacy of UTAUT in clinician adoption of health information systems in developing countries: the case of Cameroon. Int J Med Inf. 2018;109:15–22. doi:10.1016/j.ijmedinf.2017.10.016
31. Ammenwerth E, Iller C, Mahler C. IT-adoption and the interaction of task, technology and individuals: a fit framework and a case study. BMC Med Inf Decis Making. 2006;6(1):1–13. doi:10.1186/1472-6947-6-3
32. Kujala S, Ammenwerth E, Kolanen H, Ervast M. Applying and extending the FITT framework to identify the challenges and opportunities of successful eHealth services for patient self-management: qualitative interview study. J Med Internet Res. 2020;22(8):e17696. doi:10.2196/17696
33. Mohamadali NA, Aziz NFA, Zahari NAM A novel conceptual framework of Health information systems (HIS) sustainability.
34. Andargoli AE, Scheepers H, Rajendran D, Sohal A. Health information systems evaluation frameworks: a systematic review. Int J Med Inf. 2017;97:195–209. doi:10.1016/j.ijmedinf.2016.10.008
35. Ng’etich AKS, Voyi K, Mutero CM, Munoz-Zanzi C. Development and validation of a framework to improve neglected tropical diseases surveillance and response at sub-national levels in Kenya. PLoS Negl Trop Dis. 2021;15(10):e0009920. doi:10.1371/journal.pntd.0009920
36. Helwig JE, Bishop-Williams KE, Berrang-Ford L, Lwasa S, Namanya DB, Grp IR. Doing More Than Asking for Opinions: a Framework for Participation and Ecohealth in Health Information System Evaluations. Int J Healthcare Inf Syst Inf. 2020;15(3):22–46. doi:10.4018/ijhisi.2020070102
37. Mohd Nor NA, Taib NA, Saad M, et al. Development of electronic medical records for clinical and research purposes: the breast cancer module using an implementation framework in a middle income country- Malaysia. BMC Bioinf. 2019;19(Suppl S13):402. doi:10.1186/s12859-018-2406-9
38. Tenali N, Babu GRM. A Systematic Literature Review and Future Perspectives for Handling Big Data Analytics in COVID-19 Diagnosis. Review. New Gen Comput. 2023;41(2):243–280. doi:10.1007/s00354-023-00211-8
39. Sharif MI, Li JP, Khan MA, Kadry S, Tariq U. M(3)BTCNet: multi model brain tumor classification using metaheuristic deep neural network features optimization. Article; Early Access. Neural Comput Appl. 2022;2022. doi:10.1007/s00521-022-07204-6
40. Sin P, Hokynkova A, Marie N, Andrea P, Krc R, Podrouzek J. Machine Learning-Based Pressure Ulcer Prediction in Modular Critical Care Data. Article. Diagnostics. 2022;12(4):850. doi:10.3390/diagnostics12040850
41. Velpula P, Pamula R. CEECP: CT-based enhanced e-clinical pathways in terms of processing time to enable big data analytics in healthcare along with cloud computing. Article. Comput Ind Eng. 2022;168108037. doi:10.1016/j.cie.2022.108037
42. Jauk S, Kramer D, Avian A, Berghold A, Leodolter W, Schulz S. Technology Acceptance of a Machine Learning Algorithm Predicting Delirium in a Clinical Setting: a Mixed-Methods Study. J Med Syst. 2021;45(4):48. doi:10.1007/s10916-021-01727-6
43. Yang S, Wei R, Guo J, Xu L. Semantic Inference on Clinical Documents: combining Machine Learning Algorithms with an Inference Engine for Effective Clinical Diagnosis and Treatment. IEEE Access. 2017;5:7865914. doi:10.1109/ACCESS.2017.2672975
44. Kasthurirathne SN, Biondich PG, Grannis SJ, Purkayastha S, Vest JR, Jones JF. Identification of Patients in Need of Advanced Care for Depression Using Data Extracted From a Statewide Health Information Exchange: a Machine Learning Approach. J Med Internet Res. 2019;21(7):e13809. doi:10.2196/13809
45. You Y, Doubova SV, Pinto-Masis D, Pérez-Cuevas R, Borja-Aburto VH, Hubbard A. Application of machine learning methodology to assess the performance of DIABETIMSS program for patients with type 2 diabetes in family medicine clinics in Mexico. BMC Med Inf Decis Making. 2019;19(1):221. doi:10.1186/s12911-019-0950-5
46. Chen JIZ, Hengjinda P. Early prediction of coronary artery disease (CAD) by machine learning method-A comparative study. J Artif Intell. 2021;3(01):17–33.
47. Masood S, Khan R, El-Latif AA A, Ahmad M. An FCN-LSTM model for neurological status detection from non-invasive multivariate sensor data. Article; Early Access. Neural Comput Appl. 2022;2022. doi:10.1007/s00521-022-07117-4
48. Razzak I, Naz S, Ashraf A, Khalifa F, Bouadjenek MR, Mumtaz S. Mutliresolutional ensemble PartialNet for Alzheimer detection using magnetic resonance imaging data. Article. Int J Intell Syst. 2022;37(10):6613–6630. doi:10.1002/int.22856
49. Azad C, Bhushan B, Sharma R, Shankar A, Singh KK, Khamparia A. Prediction model using SMOTE, genetic algorithm and decision tree (PMSGD) for classification of diabetes mellitus. Multimedia Syst. 2022;28(4):1289–1307. doi:10.1007/s00530-021-00817-2
50. Flora OC, Margaret K, Dan K. Perspectives on utilization of community based health information systems in Western Kenya. Pan Afr Med J. 2017;272017. doi:10.11604/pamj.2017.27.180.6419
51. Chen H, Yu P, Hailey D, Cui TR. Identification of the essential components of quality in the data collection process for public health information systems. Health Inf J. 2020;26(1):664–682. doi:10.1177/1460458219848622
52. Chen H, Yu P, Hailey D, Cui TR. Validation of 4D Components for Measuring Quality of the Public Health Data Collection Process: elicitation Study. J Med Internet Res. 2021;23(5):e17240. doi:10.2196/17240
53. Aziz HA. A review of the role of public health informatics in healthcare. J Taibah Univ Med Sci. 2017;12(1):78–81. doi:10.1016/j.jtumed.2016.08.011
54. Orellana A, Estrada V, Alfonso D. MVD: a Model for the Detection of Variability in Hospital Processes Using Process Mining. IEEE Latin Am Trans. 2018;16(3):966–974. doi:10.1109/tla.2018.8358680
55. Qayyum A, Mazher M, Nuhu A, Benzinou A, Malik AS, Razzak I. Assessment of physiological states from contactless face video: a sparse representation approach. Article. Computing. 2023;105(4):761–781. doi:10.1007/s00607-021-01028-3
56. Rehman A, Khan A, Fatima G, Naz S, Razzak I. Review on chest pathogies detection systems using deep learning techniques. Artif Intell Rev. 2023. 2023. doi:10.1007/s10462-023-10457-9
57. Braunack-Mayer A, Fabrianesi B, Street J, et al. Sharing Government Health Data With the Private Sector: community Attitudes Survey. J Med Internet Res. 2021;23(10):e24200. doi:10.2196/24200
58. Moloczij N, Gough K, Solomon B, et al. Development of a hospital-based patient-reported outcome framework for lung cancer patients: a study protocol. Article. Health Quality Life Outcomes. 2018;16(1):10. doi:10.1186/s12955-017-0837-z
59. Azzopardi-Muscat N, Kluge HHP, Asma S, Novillo-Ortiz D. A call to strengthen data in response to COVID-19 and beyond. Article. J Am Med Inf Assoc. 2021;28(3):638–639. doi:10.1093/jamia/ocaa308
60. Gäbler G, Lycett D, Gall W. Integrating a New Dietetic Care Process in a Health Information System: a System and Process Analysis and Assessment. Int J Environ Res Public Health. 2022;19(5):2491. doi:10.3390/ijerph19052491
61. Gesicho MB, Babic A. Using Innovation-Decision Model to Describe the Adoption to Utilization of HIV-Data for Decision-Making in LMICs. Stud Health Technol Inform. 2018;251:117–120.
62. Gamal A, Barakat S, Rezk A. Letter to Editor (Response from author): toward a universal electronic health record system. J Biomed Infor. 2021;117:103770. doi:10.1016/j.jbi.2021.103770
63. Hyppönen H, Lumme S, Reponen J, et al. Health information exchange in Finland: usage of different access types and predictors of paper use. Int J Med Inform. 2019;122:1–6. doi:10.1016/j.ijmedinf.2018.11.005
64. Delnord M, Abboud LA, Costa C, Van Oyen H. Developing a tool to monitor knowledge translation in the health system: results from an international Delphi study. Eur J Public Health. 2021;31(4):695–702. doi:10.1093/eurpub/ckab117
65. Panerai R. Health information systems. Global perspectives in health: Health information systems; 2014:1–6.
66. Priestley JL, McGrath RJ. The evolution of data science: a new mode of knowledge production. Int J Knowledge Manag. 2019;15(2):97–109.
67. Li W, Chai Y, Khan F, et al. A comprehensive survey on machine learning-based big data analytics for IoT-enabled smart healthcare system. Mobile Netw Appl. 2021;26(1):234–252. doi:10.1007/s11036-020-01700-6
68. Benjelloun S, El Aissi ME, Lakhrissi Y, Ben Ali SE. Data Lake Architecture for Smart Fish Farming Data-Driven Strategy. Appl Syst Innov. 2023;6(1):8. doi:10.3390/asi6010008
69. Feldman J, Thomas-Bachli A, Forsyth J, Patel ZH, Khan K. Development of a global infectious disease activity database using natural language processing, machine learning, and human expertise. J Am Med Inf Assoc. 2019;26(11):1355–1359. doi:10.1093/jamia/ocz112
70. Medic G, Kosaner KlieSs M, Atallah L, et al. Evidence-based Clinical Decision Support Systems for the prediction and detection of three disease states in critical care: a systematic literature review. F1000Res. 2019;8:1728. doi:10.12688/f1000research.20498.1
71. Benis A, Harel N, Barak Barkan R, Srulovici E, Key C. Patterns of Patients’ Interactions With a Health Care Organization and Their Impacts on Health Quality Measurements: protocol for a Retrospective Cohort Study. JMIR Res Protoc. 2018;7(11):e10734. doi:10.2196/10734
72. Shimpi N, McRoy S, Zhao HM, Wu M, Acharya A. Development of a periodontitis risk assessment model for primary care providers in an interdisciplinary setting. Article. Technol Health Care. 2020;28(2):143–154. doi:10.3233/thc-191642
73. Martins B, Ferreira D, Neto C, Abelha A, Machado J. Data Mining for Cardiovascular Disease Prediction. Article. J Med Syst. 2021;45(1):6. doi:10.1007/s10916-020-01682-8
74. Neto C, Senra F, Leite J, et al. Different Scenarios for the Prediction of Hospital Readmission of Diabetic Patients. J Med Syst. 2021;45(1):11. doi:10.1007/s10916-020-01686-4
75. Bozorgmehr K, Goosen S, Mohsenpour A, Kuehne A, Razum O, Kunst AE. How Do Countries’ Health Information Systems Perform in Assessing Asylum Seekers’ Health Situation? Developing a Health Information Assessment Tool on Asylum Seekers (HIATUS) and Piloting It in Two European Countries. Int J Environ Res Public Health. 2017;14(8):894. doi:10.3390/ijerph14080894
76. Tyagi A, Singh P. Health information system. In: Healthcare Policy and Reform: concepts, Methodologies, Tools, and Applications. IGI Global; 2018:1554–1564.
77. Jeffery C, Pagano M, Hemingway J, Valadez JJ. Hybrid prevalence estimation: method to improve intervention coverage estimations. Proc Natl Acad Sci U S A. 2018;115(51):13063–13068. doi:10.1073/pnas.1810287115
78. Tamm A, Jones HJS, Perry W, et al. Establishing a colorectal cancer research database from routinely collected health data: the process and potential from a pilot study. Bmj Health Care Inf. 2022;29(1):e100535. doi:10.1136/bmjhci-2021-100535
79. Mlakar I, Safran V, Hari D, et al. Multilingual Conversational Systems to Drive the Collection of Patient-Reported Outcomes and Integration into Clinical Workflows. Symmetry-Basel. 2021;13(7):1187. doi:10.3390/sym13071187
80. Shaik K, Ramesh JVN, Mahdal M, Rahman MZU, Khasim S, Kalita K. Big Data Analytics Framework Using Squirrel Search Optimized Gradient Boosted Decision Tree for Heart Disease Diagnosis. Article. Appli Sci. 2023;13(9):5236. doi:10.3390/app13095236
81. Mardani A, Saraji MK, Mishra AR, Rani P. A novel extended approach under hesitant fuzzy sets to design a framework for assessing the key challenges of digital health interventions adoption during the COVID-19 outbreak. Appl Soft Comput. 2020;96:106613. doi:10.1016/j.asoc.2020.106613
82. Epizitone A, Moyane SP, Agbehadji IE. A Systematic Literature Review of Health Information Systems for Healthcare. MDPI. 2023;11:959.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.