")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
A Cross-Sectional Survey of Pulmonologists Working at Non-ILD Centers in the United States
Authors Biehl R , Jeganathan N, Imperio M, Becerra BJ, López D, Alismail A
Received 12 May 2023
Accepted for publication 11 July 2023
Published 14 July 2023 Volume 2023:16 Pages 1939—1942
DOI https://doi.org/10.2147/JMDH.S421089
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Rodney Biehl,1 Niranjan Jeganathan,1,2 Michelle Imperio,2,3 Benjamin J Becerra,1,4 David López,1 Abdullah Alismail1,3
1Department of Cardiopulmonary Sciences, School of Allied Health Professions, Loma Linda University, Loma Linda, CA, USA; 2Department of Pulmonary and Critical Care Medicine, Loma Linda University Health, Loma Linda, CA, USA; 3Department of Medicine, School of Medicine, Loma Linda University, Loma Linda, CA, USA; 4Department of Information and Decision Sciences, California State University of San Bernardino, San Bernardino, CA, USA
Correspondence: Abdullah Alismail, Department of Cardiopulmonary Sciences, Department of Medicine, Loma Linda University Health, Loma Linda, CA, USA, Email [email protected]
Abstract: The purpose of this cross-sectional short report study was to evaluate the perception of pulmonologist working in noninterstitial lung disease centers on challenges (COE) encountered in daily practice. Results of this survey revealed that only 40% of their patients are referred to an ILD COE, out of 69% who have access to an ILDCOE. Of these patients who were referred, the perceived benefits were rated high when it comes to having an accurate diagnosis.
Keywords: ILD, interstitial lung disease, idiopathic pulmonary fibrosis, multidisciplinary discussion
Introduction
Idiopathic pulmonary fibrosis (IPF) is a chronic, progressive, interstitial lung disease (ILD) and the most common of the numerous ILDs.1,2 Although heterogeneity exists in the natural history of IPF, the overall prognosis is poor, with a median survival of 3–4 years.3
Early and accurate diagnosis of IPF is challenging, and delays in both diagnosis and treatment initiation are associated with worse survival.4–6 Unfortunately, many patients experience a significant delay in diagnosis and multiple misdiagnoses prior to the actual diagnosis of IPF.7 Studies show improved accuracy of diagnosis and earlier initiation of treatment in patients treated at specialized ILD centers.4,8–10 Additionally, the use of multidisciplinary discussion (MDD) among specialists from different disciplines such as radiology, pathology, and rheumatology has been shown to improve diagnostic confidence and may produce better prognostic separation in diagnosis.8,11,12 Clinical guidelines currently recommend the use of MDD in the diagnosis of IPF.3,13,14
However, data on the availability and utilization of important resources in the diagnosis of IPF by pulmonologists working at non-ILD centers is scarce. Currently, there are 81 ILD Care Centers in the United States (https://www.pulmonaryfibrosis.org/docs/default-source/media/ccn-fact-sheet-2022.pdf?Status=Master&sfvrsn=942f276d_3/%20CCN-Fact-Sheet-2022%20.pdf). We conducted a social and behavioral survey to gain insight into the challenges encountered by non-ILD center pulmonologists in establishing a diagnosis of IPF and assess their referral patterns to ILD centers. In this short report, we report our findings of this cross-sectional study of physicians within the United Stated of America.
Methods
The Loma Linda University Institutional Review Board examined the study and exempted it from full review since it is an anonymous survey. The survey included background questions (ie, primary work setting, experience/training in ILD) and questions related to survey participants’ perceptions with the level of difficulty with components of IPF diagnosis and the benefits of referral to an ILD center.
The survey was emailed to pulmonologists throughout the United States as an anonymous questionnaire using a proprietary medical database. Data collection began in March 2020 and ended in May 2020. The target participants were pulmonary physicians working at a non-ILD center. We excluded those self-identifying as working in an ILD center. The survey content was validated by pulmonologists specializing in IPF, respiratory therapists, and statisticians. Once the respondents opened the survey, the first question was the consent to participate. If they select “yes, I am interested to participate”, survey started; when selecting “No, I do not want to participate”, survey ended.
We reported descriptive statistics in numbers and percentages, and continuous variables in medians and interquartile ranges (IQR, 25–75th percentiles).
Results
A total of N=65 pulmonologists working at non-ILD centers have responded to the survey. The number of years in practice varied widely (the median was 25 (IQR 5–42)). Only 30.8% reported having any recent training in ILD (conference/CME 18.5%, fellowship 6.2%, other 6.1%). The average number of patients diagnosed with IPF also varied (median of 5 (IQR 1–75) in the past year and 20 (IQR 3–250) in the past three years). The majority (81%) agreed on the importance of early diagnosis of IPF.
Next, we evaluated the perceived level of difficulty with components of IPF diagnosis on a scale of 1–5 (least to most difficult) (Figure 1a). The median difficulty score for access to MDD was 3.00 (IQR 1–4), access to High resolution computed tomography (HRCT) of the chest was 1.00 (IQR 1.0–2.5), patient compliance was 2.0 (IQR 1.0–3.0), and disease/guidelines familiarity was 2.0 (IQR 1.0–3.0). The median percent of the time respondents indicated utilizing MDD was 45% (IQR 0–100).
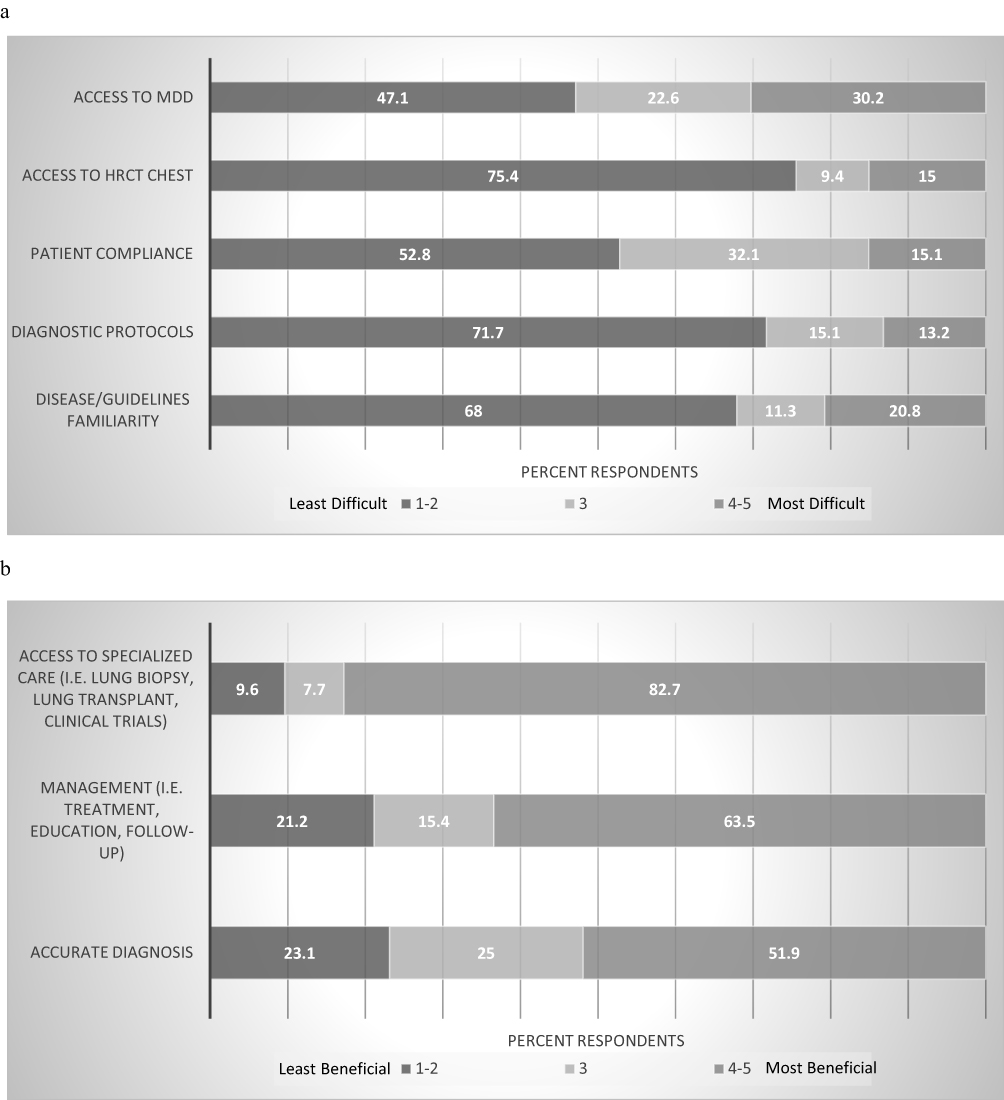 |
Figure 1 (a) Difficulty level with diagnostic components of IPF. Each bar represents the percentage of non-ILD center pulmonologists responses based on a Likert scale: 1 to 5 (least difficult to most difficult). (b) Benefits of Referral to an ILD Center. Each bar represents the percentage of non-ILD center pulmonologists responses based on a Likert scale: 1 to 5 (least beneficial to most beneficial). Abbreviations: HRCT, High resolution computed tomography; MDD, multidisciplinary discussion. |
Only 69.2% of the respondents reported having access to an ILD center. The median for the percentage of time the respondents referred suspected IPF patients to an ILD center was 40.5% (IQR 20–67.5) for those with access to an ILD center. For the group with access, there was no difference in baseline factors (recent ILD training, number of years in practice, number of ILD patients seen) between those more likely to refer (median and above, ≥ 40.5% of the time) to an ILD center and those less likely to refer to an ILD center (below median, <40.5% of the time).
Next, we evaluated the perceived benefits of referral to an ILD center on a scale of 1–5 (least beneficial to most beneficial) (Figure 1b). The median for access to specialized care was 5.0 (IQR 4.0–5.0), an accurate diagnosis was 4.0 (IQR 3.0–4.75), and management was 4.0 (IQR 3.0–4.75). Supplementary Table 1 shows a list of the total survey questions and response count and % of each question.
Discussion
A significant percentage of patients do not have access to an ILD center and are cared for by pulmonologists at non-ILD centers. In this pilot study, we examined the non-ILD center pulmonologists perspective on the challenges with IPF diagnosis and perceived benefits of referring patients to an ILD center. The median number of patients diagnosed with IPF by non-ILD center pulmonologists was only 5 per year. Similarly, prior studies have shown that most pulmonologists treat only a small number of IPF patients per year.
We examined the difficulty level with the important components in IPF diagnosis. The percentage of pulmonologists rating the difficulty level as high (4 or 5 on a scale of 1 to 5) was 30.2% for access to MDD, 15% for HRCT access, 15.1% for patient compliance and 20.8% for disease familiarity. Although the majority stated that access to MDD was not difficult, the utilization was low (used in less than half of the IPF cases). ILD centers have shown to be beneficial for IPF patients as they are equipped and designed to manage a large volume of these patients. The percentage of pulmonologists rating the benefits of referring to an ILD center as high (4 or 5) was 83% for access to specialized care, 63.5% for management and 51.9% for accurate diagnosis. However, even for those with access to an ILD center, utilization was much lower than expected (median percent was 41% for suspected IPF patients).
There are likely various reasons for the underutilization of MDD and referral to an ILD center. Most physicians in this study had not recently received any formalized training in ILD, perhaps indicating a knowledge gap in both the importance of early diagnosis and best practices in making the diagnosis. Additionally, a significant percentage did report having difficulties with access to MDD and access to an ILD center, highlighting the need for improvement in the availability of these resources and infrastructure. We strongly recommend providers to have enhance MDD access as it will improve IPF related outcomes. Furthermore, utilizing uptodate methods such as online conferences, networking with IPF specialists at ILD centers would improve the diagnosis as well as access, especially for general physicians working at Non-ILD centers.
This study has several limitations. First, the sample size is small. The reason for the low sample size and response is most likely the timeframe of the data collection, as it took place at the beginning of the COVID-19 pandemic. The self-reported design of this survey may also limit the conclusions that can be drawn from the results, as answers are subject to various forms of bias, including desirability and recall biases. Additional studies using objectively collected data on the frequency of ILD center referral and MDD usage would be useful. Further research is needed to expand our understanding of the reasons for underutilization of ILD centers and MDD by non-ILD center pulmonologists. In addition, we believe that future studies should focus on addressing ways to utilize MDD in terms access to improve IPF related outcomes.
Funding
There is no funding to report.
Disclosure
All authors report no conflict of interest.
References
1. Travis WD, Costabel U, Hansell DM, et al. An official American Thoracic Society/European Respiratory Society statement: update of the international multidisciplinary classification of the idiopathic interstitial pneumonias. Am J Respir Crit Care Med. 2013;188(6):733–748. doi:10.1164/rccm.201308-1483ST
2. Oliveira DS, de Araújo Filho JA, Paiva AFL, Ikari ES, Chate RC, Nomura CH. Idiopathic interstitial pneumonias: review of the latest American Thoracic Society/European Respiratory Society classification. Radiol Bras. 2018;51(5):321–327. doi:10.1590/0100-3984.2016.0134
3. Raghu G, Collard HR, Egan JJ, et al. An official ATS/ERS/JRS/ALAT statement: idiopathic pulmonary fibrosis: evidence-based guidelines for diagnosis and management. Am J Respir Crit Care Med. 2023. doi:10.1164/rccm.2009-040GL
4. Lamas DJ, Kawut SM, Bagiella E, et al. Delayed access and survival in idiopathic pulmonary fibrosis | a cohort study. Am J Respir Crit Care Med. 2023. doi:10.1164/rccm.201104-0668OC
5. Hoyer N, Prior TS, Bendstrup E, Shaker SB. Diagnostic delay in IPF impacts progression-free survival, quality of life and hospitalisation rates. BMJ Open Respir Res. 2022;9(1):e001276. doi:10.1136/bmjresp-2022-001276
6. Kolb M, Richeldi L, Behr J, et al. Nintedanib in patients with idiopathic pulmonary fibrosis and preserved lung volume. Thorax. 2017;72(4):340–346. doi:10.1136/thoraxjnl-2016-208710
7. Cosgrove GP, Bianchi P, Danese S, Lederer DJ. Barriers to timely diagnosis of interstitial lung disease in the real world: the INTENSITY survey. BMC Pulm Med. 2018;18(1):9. doi:10.1186/s12890-017-0560-x
8. Flaherty KR, Andrei AC, King TE, et al. Idiopathic interstitial pneumonia: do community and academic physicians agree on diagnosis? Am J Respir Crit Care Med. 2007;175(10):1054–1060. doi:10.1164/rccm.200606-833OC
9. Maher TM, Swigris JJ, Kreuter M, et al. Identifying barriers to idiopathic pulmonary fibrosis treatment: a survey of patient and physician views. Respiration; International Review of Thoracic Diseases. 2018;96(6):514–524. doi:10.1159/000490667
10. Marijic P, Schwarzkopf L, Maier W, Trudzinski F, Kreuter M, Schwettmann L. Comparing outcomes of ILD patients managed in specialised versus non-specialised centres. Respir Res. 2023. doi:10.1186/s12931-022-02143-1
11. Flaherty KR, King TE, Raghu G, et al. Idiopathic interstitial pneumonia: what is the effect of a multidisciplinary approach to diagnosis? Am J Respir Crit Care Med. 2004;170(8):904–910. doi:10.1164/rccm.200402-147OC
12. Fujisawa T, Mori K, Mikamo M, et al. Nationwide cloud-based integrated database of idiopathic interstitial pneumonias for multidisciplinary discussion. Eur Respir J. 2019;53(5):1802243. doi:10.1183/13993003.02243-2018
13. Raghu G, Remy-Jardin M, Myers JL, et al. Diagnosis of idiopathic pulmonary fibrosis. An official ATS/ERS/JRS/ALAT clinical practice guideline. Am J Respir Crit Care Med. 2018;198(5):e44–68. doi:10.1164/rccm.201807-1255ST
14. Raghu G, Remy-Jardin M, Richeldi L, et al. Idiopathic pulmonary fibrosis (an update) and progressive pulmonary fibrosis in adults: an official ATS/ERS/JRS/ALAT clinical practice guideline. Am J Respir Crit Care Med. 2022;205(9):e18–47. doi:10.1164/rccm.202202-0399ST
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.