")
Back to Journals » International Journal of General Medicine » Volume 16
A Cross-Sectional Survey of Physicians’ Knowledge and Awareness of Chronic Pain Associated with Rheumatoid Arthritis in Rheumatology Departments in Zhejiang Province, China
Received 25 July 2023
Accepted for publication 22 September 2023
Published 14 November 2023 Volume 2023:16 Pages 5281—5288
DOI https://doi.org/10.2147/IJGM.S432366
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Luca Testarelli
Meiju Zhou,1 Ci Lu,2 Fang Yuan1
1Department of Rheumatology and Immunology, Zhejiang Hospital, Hangzhou, Zhejiang Province, People’s Republic of China; 2Department of Rheumatology and Immunology, Run Run Shaw Hospital, Zhejiang University School of Medicine, Hangzhou, Zhejiang Province, People’s Republic of China
Correspondence: Fang Yuan, Department of Rheumatology and Immunology, Zhejiang Hospital, No. 1299 Gudun Road, Hangzhou, Zhejiang Province, 310012, People’s Republic of China, Tel +86-18072963566, Email [email protected]
Objective: To assess physicians’ knowledge and awareness of chronic pain associated with rheumatoid arthritis (RA) in Rheumatology departments throughout Zhejiang province to improve chronic pain relief in RA patients.
Methods: A cross-sectional questionnaire survey was conducted onsite and online among rheumatologists in tertiary and secondary hospitals across Zhejiang province, China. The questionnaire inquired about rheumatoid arthritis-related pain cognition, pain assessment, pain management protocols, and medication choice.
Results: Among the 150 questionnaires included, 98 were from tertiary hospitals, and 52 were from secondary hospitals. There was no difference in rheumatologists’ perceptions of chronic pain in RA patients between tertiary and secondary hospitals. About 55.1% of rheumatologists from tertiary hospitals and 44.2% of rheumatologists from secondary hospitals utilized unstandardized pain assessment scales. About 46.9% of rheumatologists in tertiary hospitals and 36.5% of rheumatologists in secondary hospitals favored the numerical rating scale (NRS). About 87.8% of rheumatologists in tertiary hospitals and 71.7% of rheumatologists in secondary hospitals conducted pain assessment within 4 hours of admission. About 66.3% of rheumatologists working in tertiary hospitals and 32.7% of rheumatologists practicing in secondary hospitals believed their hospitals had pain departments. For RA patients who complained of pain for the first time, secondarily, or repeatedly, 48%, 26%, and 36.7% of rheumatologists preferred nonsteroidal anti-inflammatory drugs (NSAIDs), glucocorticoids, and opioid analgesics, respectively. For RA patients with mild, moderate, or severe pain, 74%, 6%, and 16% of rheumatologists preferred NSAIDs, glucocorticoids, and opioid analgesics, respectively.
Conclusion: The assessment and treatment of chronic pain associated with RA are not standardized. For management, more rheumatologists preferred NSAIDs and glucocorticoids.
Keywords: rheumatoid arthritis, chronic pain, survey and questionnaire
Introduction
Rheumatoid arthritis (RA) is a chronic autoimmune inflammatory disease of the synovial tissues. The most prevalent form of autoimmune arthritis results in joint discomfort, stiffness, swelling, and limited joint movement, ultimately resulting in structural damage, deformity, and disability.1 The most prevalent symptom of rheumatoid arthritis is pain, which impairs functional ability and quality of life.2 Ninety-seven percent of early rheumatoid arthritis patients experience pain, which is also the primary reason for seeking medical attention, and 90.4% of these RA patients are already experiencing intense pain on consultation.3
Chronic pain is a typical symptom of RA, and the features of peripheral and central pain processing may be exacerbated by inflammation, and disturbed pain processing may be a feature contributing to widespread pain.4 Notably, some RA patients experience non-inflammatory pain.5 Numerous studies revealed that pain and joint inflammation could be uncoupled over the illness course and that pain could persist despite inflammatory remission.6,7 These findings suggest that anti-rheumatic medications may be insufficiently effective in controlling pain that is not directly linked to inflammation.8 Thus, physicians might face a dilemma when dealing with rheumatoid arthritis patients who exhibit no signs of inflammation.
As a result, pain remains a key complaint in rheumatoid arthritis patients, warranting urgent improvement. Nonsteroidal anti-inflammatory drugs (NSAIDs) and disease-modifying anti-rheumatic drugs (DMARDs) can help to modify autoimmune inflammation and improve symptoms of RA.7,8 A previous study found that about 90% of rheumatoid arthritis patients prioritized pain relief over other symptoms and that around 80% of rheumatoid arthritis patients with negative joint symptoms (no joint swelling or tenderness) continued to experience mild to severe pain after treatment initiation.9
However, many rheumatologists focus on treating the underlying inflammation in RA but pain control is often reported as the main concern for patients, particularly in the early disease stage.10 In fact, even with effective control of inflammation of RA, the pain in some RA patients is persist, but the mechanisms and the dysregulation of pain pathways remains unknown, maybe peripheral and central sensitization.11 Combined our clinical experience, the chronic pain of RA did not get enough recognition. So, we performed a questionnaire survey of 150 rheumatologists in Zhejiang province to ascertain their level of knowledge and awareness of chronic pain associated with rheumatoid arthritis.
Method
Study Design
Our cross-sectional study recruited 150 rheumatologists from departments of Rheumatology across the Zhejiang province. The survey was conducted using onsite and online delivered questionnaires. The Zhejiang hospital ethics committee approved this study (2021124k). Informed consent was implied by completing and returning their questionnaires.
Given the paucity of rheumatologists in Zhejiang province, the sample size for this study was not estimated. Inclusion criteria: rheumatologists working in the Zhejiang province, including doctors from other internal medicine departments who are engaged in rheumatology. Exclusion criteria: incomplete questionnaires were excluded. If the responses were identical, a single questionnaire was chosen.
Distribution and Collection
The questionnaires (Appendix 1) were distributed onsite and via online WeChat groups at the Zhejiang Conference of Rheumatology. One medical staff member distributed questionnaires and gathered data over a one-week period. Data were obtained by means of an anonymous, self-reporting survey.
Questionnaires Setting
The survey was divided into five parts: (1) Cognition of chronic pain associated with RA in rheumatologists; (2) Pain assessment scales; (3) Timing of pain assessment; (4); pain management protocols; (5) Clinical management of pain associated with RA.
Statistical Analysis
All data were analyzed using SPSS Version 23 statistical software. Descriptive data were presented as n (%). Statistical analysis was performed using the chi-square test (Fisher’s exact test). A P-value <0.05 was considered statistically significant.
Results
Baseline Characteristics
From the 22nd to the 29th of September, 2022, a total of 180 questionnaires were distributed. Of those, 150 were considered valid, with an effective recovery rate of 83.3%. Of the invalid 30, 29 were incomplete, and 2 were identical (we chose one). Of the 150 questionnaires distributed to rheumatologists, 98 came from tertiary hospitals and 52 from secondary hospitals.
Cognition of Chronic Pain Associated with RA
Table 1 shows the cognition of chronic pain associated with RA among rheumatologists in Zhejiang province. The objective of the questionnaire survey was to assess whether rheumatologists in Zhejiang province have a robust understanding of chronic pain linked with RA. The 6 following items were queried: (1) Whether physicians are aware of chronic pain associated with RA; (2) whether chronic pain associated with RA is an important issue; (3) whether chronic pain associated with RA is controllable; (4) whether your pain management is outdated; (5) whether RA patients’ pain is relieved promptly; and (6) whether chronic pain associated with RA is refractory. About 33.3% of rheumatologists believed chronic pain associated with RA was refractory, but 100% of rheumatologists thought chronic pain associated with RA was treatable. Statistical analysis revealed no significant difference between rheumatologists in tertiary and secondary hospitals concerning the awareness of chronic pain associated with RA.
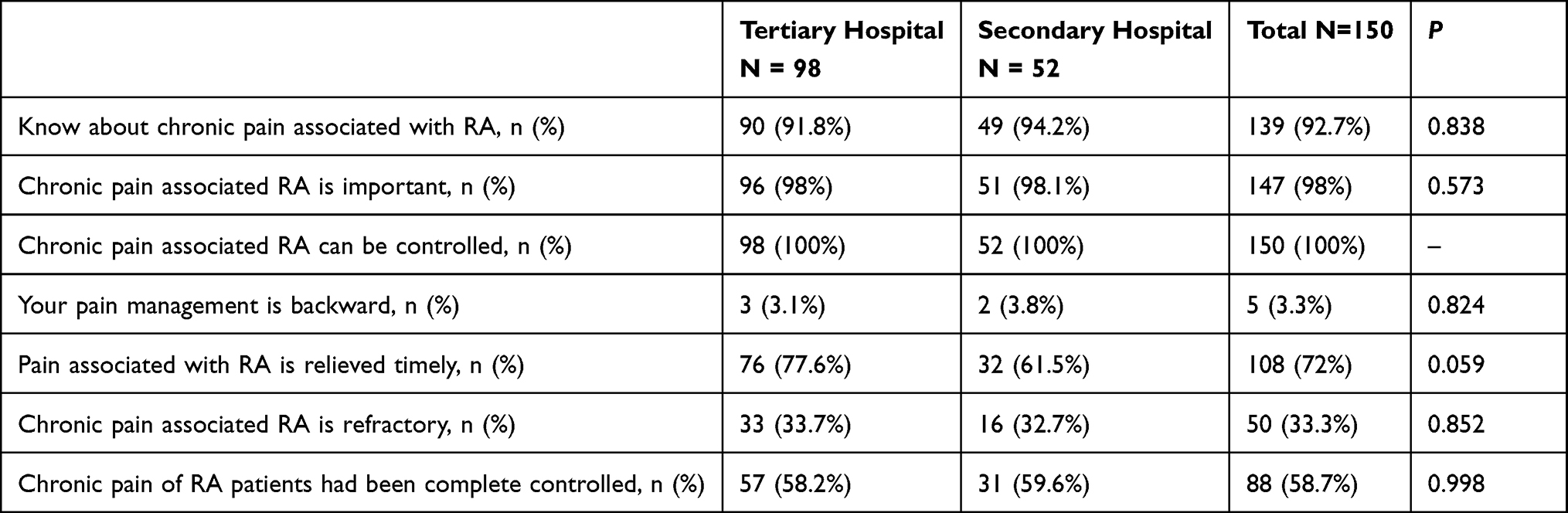 |
Table 1 Cognition of Chronic Pain Associated with RA of Rheumatologists |
Assessment Scales of Chronic Pain Associated with RA
Among the 150 questionnaires, 40% (n = 60) rheumatologists used the numerical rating scale (NRS), 18% (n = 27) used visual analog scale (VAS), 25.3% (n = 38) used verbal rating scale (VRS) to assess chronic pain associated with RA. While 4.7% (n = 7) chose other assessment tools, including the Wong-Baker face pain revision (FPS-R) and brief pain inventory (BPI). Twelve percent (n = 18) of rheumatologists did not conduct pain assessments of patients. Compared with secondary hospitals, rheumatologists in tertiary hospitals were more likely to use the NRS (46.9% vs 26.9%, P = 0.027), while rheumatologists in secondary hospitals preferred the VRS (36.5% vs 19.4%, P = 0.036) (Figure 1).
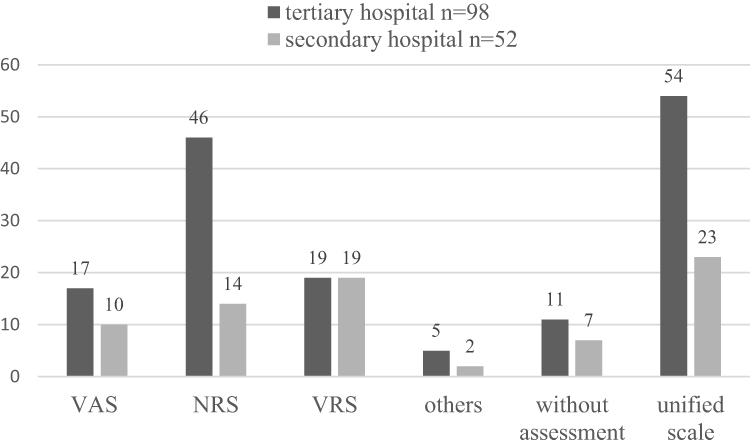 |
Figure 1 Assessment of chronic pain associated with RA. |
Assessment Frequency of Chronic Pain Associated with RA
Eighty-two percent (n = 123) of rheumatologists assessed rheumatologists assessed the pain associated with RA within 4 hours of admission, and 91.3% (n = 137) conducted daily assessments. In comparison, 2% (n = 3) of rheumatologists assessed pain weekly, and 94.6% (n = 142) evaluated subject to condition changes. Compared with rheumatologists in secondary hospitals, rheumatologists in tertiary hospitals were more inclined to assess pain within 4 hours of admission (87.5% vs 71.1%, P = 0.022) (Figure 2).
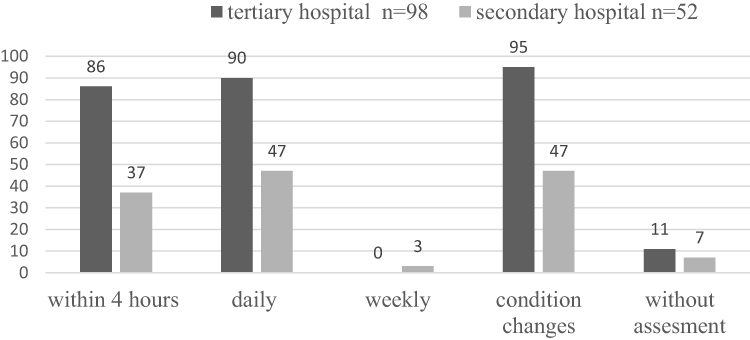 |
Figure 2 Pain assessment frequencies in Rheumatology department of Zhejiang province. |
Pain Management Protocols
The pain management protocols were established in 26% of Rheumatology departments, and multidisciplinary panel of pain were performed in 22.7% of Rheumatology departments. The prevalence of pain monitor setups was low, with 21.4% (n = 21) in tertiary hospitals and 15.4% (n = 8) in secondary hospitals, respectively. Similarly, pain education on the patients was poor, with 19.4% (n = 19) in tertiary hospitals and 21.1% (n = 11) in secondary hospitals, respectively. Compared with secondary hospitals, more tertiary hospitals established pain departments (66.3% vs 32.7%, P = 0.005) (Table 2).
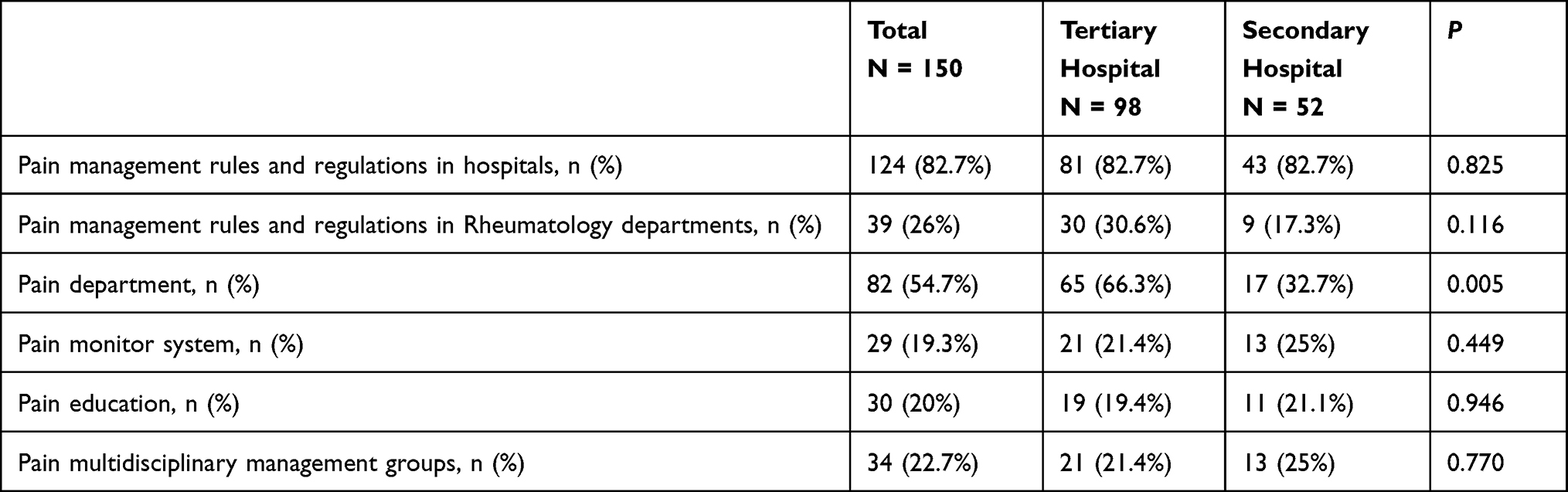 |
Table 2 Pain Management Rules and Regulations Systems |
Management of RA Patients According to the Number of Pain Complaints
NSAIDs were recommended by 48% (n = 72) of rheumatologists when RA patients initially complained of pain. Glucocorticoids were favored by 26% (n = 39) and 36.7% (n = 55) of rheumatologists for RA patients with secondary or repeated complaints of pain, respectively. Only a limited percentage of rheumatologists used physiotherapy as a treatment method (Table 3).
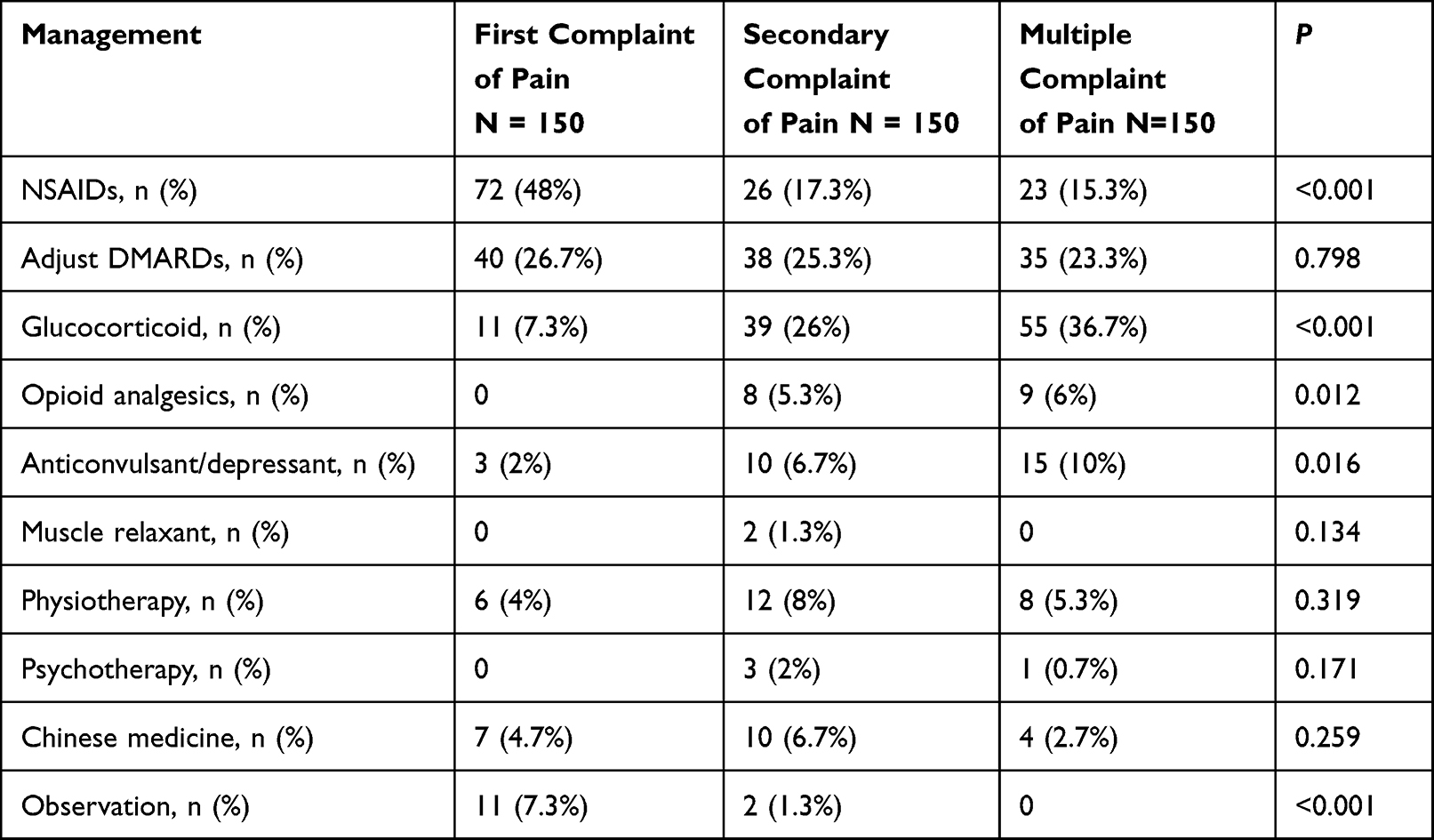 |
Table 3 Preferred Management of Rheumatologists of RA Patients with Different Times of Complaint |
Management of RA Patients with Different Degrees of Pain
The preferred clinical management of RA patients with varying degrees of pain is shown in Table 4. When treating RA patients with minor discomfort, 74% (n = 111) of rheumatologists favored NSAIDs. Rheumatologists adjusted DMARDs and glucocorticoid doses in 35.3% (n = 53) and 34% (n = 51) of cases, respectively. Forty-six percent (n = 69) of rheumatologists chose glucocorticoids to treat RA patients with significant pain. A few doctors chose physiotherapy, psychotherapy, Chinese medicine, anticonvulsant/depressant, and muscle relaxant.
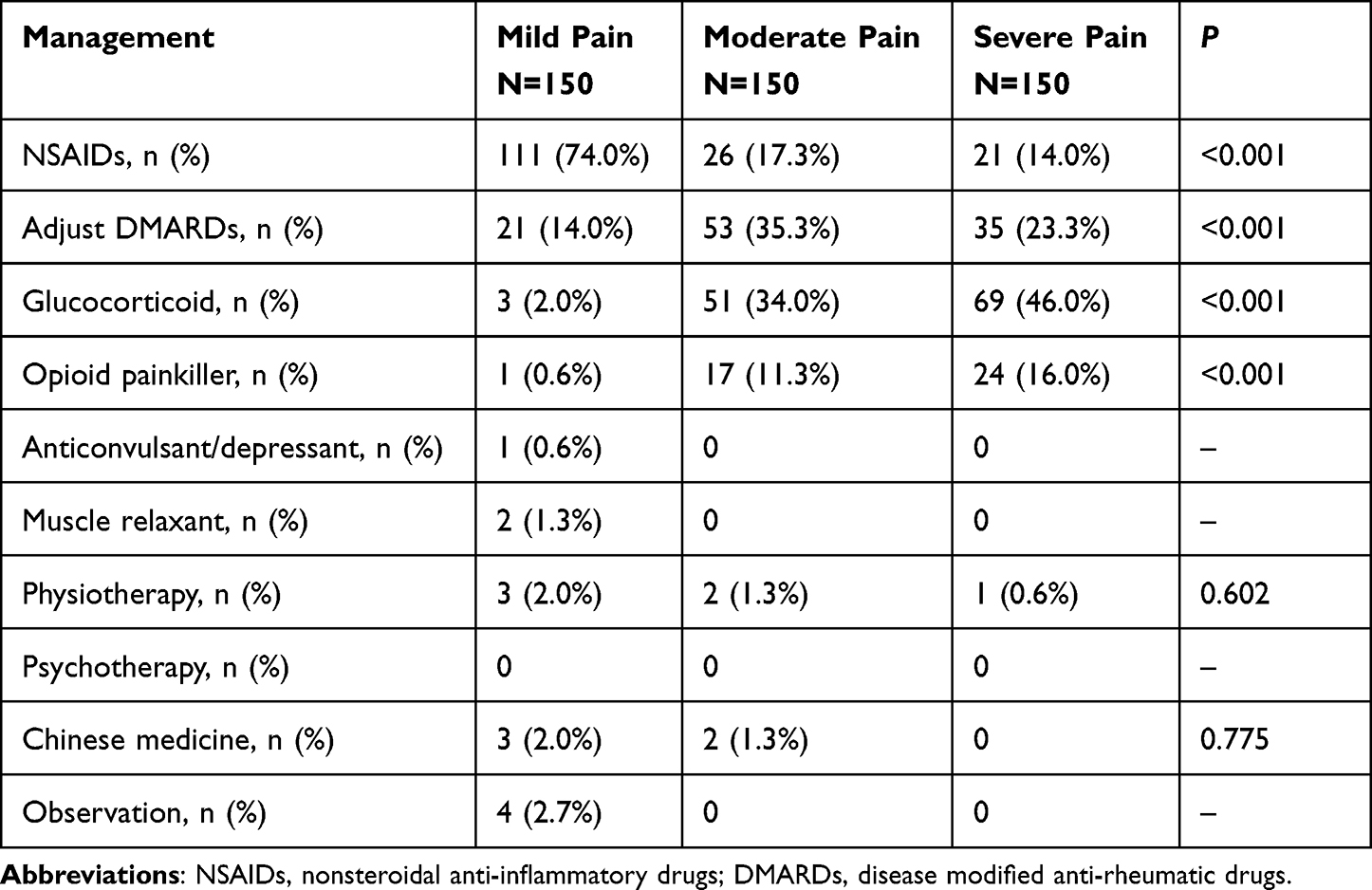 |
Table 4 Preferred Management of Rheumatologists of RA Patients with Different Pain Degree |
Discussion
RA is an inflammatory illness that induces severe discomfort, including joint degeneration, functional impairment, and chronic pain.12 NSAIDs and DMARDs are usually beneficial in relieving inflammation-related pain symptoms in people with RA.13 However, rheumatologists may still face a challenge since debilitating pain can persist even after inflammation has subsided.6
Taylor et al14 conducted an observational study that included 2795 patients with RA (756 from Europe and 2039 from the USA) to assess patients’ perceptions regarding pain management in RA, although the majority of patients indicated that their RA was under control, 75% of Europeans and 82% of Americans said their pain was moderate to severe, and the majority of Europeans (60%) and Americans (65%) said they were dissatisfied with their arthritic pain management. In our study, 33.3% of rheumatologists believed pain associated with RA was refractory, and only 58.7% of rheumatologists believed pain associated with RA patients had been completely controlled. Moreover, there was no significant difference between rheumatologists in tertiary and secondary hospitals regarding cognition of chronic pain associated with RA.
However, there was a significant difference in terms of the assessment scale preferred for pain assessment. Rheumatologists in tertiary hospitals preferred the NRS scale, while rheumatologists in secondary hospitals preferred the VRS scale. Interestingly, 82% of rheumatologists assessed the degree of pain experienced by RA patients within 4 hours of admission. More rheumatologists in tertiary hospitals assessed pain within 4 hours compared with secondary hospitals. Karcioglu et al15 systematically reviewed 872 potentially relevant studies, and ultimately analyzed 19 full-text articles, and found that VAS, VRS, and NRS scales were valid, reliable, and appropriate for use in clinical practice, although the VRS scale was harder to implement than the others, generally, the NRS had good sensitivity and generates data that could be analyzed for audit purposes. Nevertheless, the scores of these scales could be influenced by factors other than pain intensity. Thong et al16 administered measures of pain intensity, pain unpleasantness, catastrophizing, depressive symptoms, and pain interference to 101 individuals with chronic lower back or knee pain, and found the NRS, VAS, and VRS scales were strongly associated with one another, validating their usefulness as pain intensity measures. Notably, they further found that VAS appeared most similar to NRS and less influenced by non-pain intensity factors. Nonetheless, there is currently no recommended scale for assessing pain associated with RA.
Comorbid fibromyalgia in inflammatory rheumatic conditions appears to affect assessment of disease severity, particularly patient-reported outcome measures, and may influence response to treatment.17 Disease activity measures with subjective elements are conflated in patients with fibromyalgia and do not reliably assess true inflammatory disease. This needs to be taken into account when evaluating the severity and therapy of RA patients.18,19
Only 54.7% and 25% of rheumatologists believed there were pain departments and multidisciplinary panel of pain in hospitals, respectively. The biopsychosocial model of pain has sparked the development of more therapeutically effective and cost-efficient interdisciplinary chronic pain management programs over the last few years.20 Multidisciplinary programs involve several healthcare providers from different departments (physicians, psychologists, physical therapists, occupational therapists).21 Once established, these multidisciplinary programs greatly enhance the effectiveness of treatment for the chronic pain sufferers and create a rewarding experience for the treatment providers.22,23
Observational studies revealed that despite successful immune-suppressive therapy such as DMARDs (which include biological agents), many RA patients continued to have significant pain, which is proven to impact both quality of life and working ability.13 Other pain management alternatives include education complemented by physical activities and exercises, orthotics, psychological and social interventions, sleep hygiene, weight management, pharmacological and joint-specific treatment options, and multidisciplinary pain management programs.24–26 Educational intervention, orthotics, weight management, and multidisciplinary treatment programs have also shown effectiveness in chronic pain management in Europe and the United States, but there are few representative studies in China.8,26
Herein, 74% of rheumatologists chose NSAIDs for RA patients with mild pain, while 46% of rheumatologists preferred glucocorticoids to treat RA patients with severe pain. As the frequency and intensity of pain increase, more rheumatologists preferred glucocorticoids as the treatment of choice. Glucocorticoids are linked to a dose-dependent increase in the risk of severe infection in RA patients on stable DMARDs therapy, with small but substantial risks even at dosages of 5 mg or less per day.26,27 As a result, rheumatologists must weigh the benefits of low-dose glucocorticoids against the possibility of side effects.28
Chronic pain caused by RA is a significant and costly issue in China, as well as the rest of the world. Epidemiological research on RA-related chronic pain was primarily conducted in Europe and North America, with only scarce reports from China.9,29,30 Traditional medical approaches have been questioned, implying the necessity for alternate chronic pain treatment strategies.
We first launched the study. So far, there were no similar studies. We believed the study improved a certain degree of advances in the chronic pain of RA field. In this study, significant differences were found regarding the pain cognition, pain management protocols, and management choice at different levels of hospitals. The awareness of chronic pain associated with RA must be addressed in order to improve the quality of life of RA patients.
Our study has several limitations: (1) Zhejiang Province is a developed Chinese province with a small population. (2) The samplings were not conducted randomly; thus, sample collections might be biased. (3) The questionnaires lacked standardization, and the questionnaires’ reliability and validity were not rigorously assessed.
Conclusion
The chronic pain associated with RA is poorly recognized by the rheumatologists. The assessment and treatment of chronic pain associated with RA are not standardized. For management, more rheumatologists preferred NSAIDs and glucocorticoids.
Statement of Ethics
This study was approved by the Ethics Committee of Zhejiang hospital (No. 2021124k). The study protocol complied with the Declaration of Helsinki guidelines and was approved by the ethics committee of Zhejiang Hospital. All Rheumatologists provided informed consent.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Emery P, Breedveld FC, Dougados M, et al. Early referral recommendation for newly diagnosed rheumatoid arthritis: evidence based development of a clinical guide. Ann Rheum Dis. 2002;61(4):290–297. doi:10.1136/ard.61.4.290
2. Hootman JM, Helmick CG, Brady TJ. A public health approach to addressing arthritis in older adults: the most common cause of disability. Am J Public Health. 2012;102(3):426–433. doi:10.2105/AJPH.2011.300423
3. De Cock D, Van der Elst K, Stouten V, et al. The perspective of patients with early rheumatoid arthritis on the journey from symptom onset until referral to a rheumatologist. Rheumatol Adv Pract. 2019;3(2):rkz035. doi:10.1093/rap/rkz035
4. Cao Y, Fan D, Yin Y. Pain mechanism in rheumatoid arthritis: from cytokines to central sensitization. Mediators Inflamm. 2020;2020:2076328. doi:10.1155/2020/2076328
5. Lampa J. Pain without inflammation in rheumatic diseases. Best Pract Res Clin Rheumatol. 2019;33(3):101439. doi:10.1016/j.berh.2019.101439
6. Lee YC, Cui J, Lu B, et al. Pain persists in DAS28 rheumatoid arthritis remission but not in ACR/EULAR remission: a longitudinal observational study. Arthritis Res Ther. 2011;13(3):R83. doi:10.1186/ar3353
7. Lee YC. Effect and treatment of chronic pain in inflammatory arthritis. Curr Rheumatol Rep. 2013;15(1):300. doi:10.1007/s11926-012-0300-4
8. Altawil R, Saevarsdottir S, Wedrã©n S, Alfredsson L, Klareskog L, Lampa J. Remaining pain in early rheumatoid arthritis patients treated with methotrexate. Arthritis Care Res. 2016;68(8):1061–1068. doi:10.1002/acr.22790
9. Hendricks O, Andersen TE, Christiansen AA, et al. Efficacy and safety of cannabidiol followed by an open label add-on of tetrahydrocannabinol for the treatment of chronic pain in patients with rheumatoid arthritis or ankylosing spondylitis: protocol for a multicentre, randomised, placebo-controlled study. BMJ Open. 2019;9(6):e028197. doi:10.1136/bmjopen-2018-028197
10. van der Elst K, Meyfroidt S, De Cock D, et al. Unraveling patient-preferred health and treatment outcomes in early rheumatoid arthritis: a longitudinal qualitative study. Arthritis Care Res. 2016;68(9):1278–1287. doi:10.1002/acr.22824
11. Zhang A, Lee YC. Mechanisms for Joint Pain in Rheumatoid Arthritis (RA): from cytokines to central sensitization. Curr Osteoporos Rep. 2018;16(5):603–610. doi:10.1007/s11914-018-0473-5
12. Firestein GS. Evolving concepts of rheumatoid arthritis. Nature. 2003;423(6937):356–361. doi:10.1038/nature01661
13. Walker N, Michaud K, Wolfe F. Work limitations among working persons with rheumatoid arthritis: results, reliability, and validity of the work limitations questionnaire in 836 patients. J Rheumatol. 2005;32(6):1006–1012.
14. Taylor P, Manger B, Alvaro-Gracia J, et al. Patient perceptions concerning pain management in the treatment of rheumatoid arthritis. J Int Med Res. 2010;38(4):1213–1224. doi:10.1177/147323001003800402
15. Karcioglu O, Topacoglu H, Dikme O, Dikme O. A systematic review of the pain scales in adults: which to use? Am J Emerg Med. 2018;36(4):707–714. doi:10.1016/j.ajem.2018.01.008
16. Thong ISK, Jensen MP, Miró J, Tan G. The validity of pain intensity measures: what do the NRS, VAS, VRS, and FPS-R measure? Scand J Pain. 2018;18(1):99–107. doi:10.1515/sjpain-2018-0012
17. Zhao SS, Duffield SJ, Goodson NJ. The prevalence and impact of comorbid fibromyalgia in inflammatory arthritis. Best Pract Res Clin Rheumatol. 2019;33(3):101423. doi:10.1016/j.berh.2019.06.005
18. Coskun Benlidayi I. Fibromyalgia interferes with disease activity and biological therapy response in inflammatory rheumatic diseases. Rheumatol Int. 2020;40(6):849–858. doi:10.1007/s00296-019-04506-2
19. Mease PJ. Fibromyalgia, a missed comorbidity in spondyloarthritis: prevalence and impact on assessment and treatment. Curr Opin Rheumatol. 2017;29(4):304–310. doi:10.1097/BOR.0000000000000388
20. Gatchel RJ, McGeary DD, McGeary CA, Lippe B. Interdisciplinary chronic pain management: past, present, and future. Am Psychol. 2014;69(2):119–130. doi:10.1037/a0035514
21. Yang B, Cui Z, Zhu X, et al. Clinical pain management by a multidisciplinary palliative care team: experience from a tertiary cancer center in China. Medicine. 2020;99(48):e23312. doi:10.1097/MD.0000000000023312
22. Cohen SP, Bhaskar A, Bhatia A, et al. Consensus practice guidelines on interventions for lumbar facet joint pain from a multispecialty, international working group. Reg Anesth Pain Med. 2020;45(6):424–467. doi:10.1136/rapm-2019-101243
23. Danilov A, Danilov A, Barulin A, Kurushina O, Latysheva N. Interdisciplinary approach to chronic pain management. Postgrad Med. 2020;132(sup3):5–9. doi:10.1080/00325481
24. Zdziarski LA, Wasser JG, Vincent HK. Chronic pain management in the obese patient: a focused review of key challenges and potential exercise solutions. J Pain Res. 2015;8:63–77. doi:10.2147/JPR.S55360
25. Lo J, Chan L, Flynn S. A systematic review of the incidence, prevalence, costs, and activity and work limitations of amputation, osteoarthritis, rheumatoid arthritis, back pain, multiple sclerosis, spinal cord injury, stroke, and traumatic brain injury in the United States: a 2019 update. Arch Phys Med Rehabil. 2021;102(1):115–131. doi:10.1016/j.apmr.2020.04.001
26. Geenen R, Overman CL, Christensen R, et al. EULAR recommendations for the health professional’s approach to pain management in inflammatory arthritis and osteoarthritis. Ann Rheum Dis. 2018;77(6):797–807. doi:10.1136/annrheumdis-2017-212662
27. George MD, Baker JF, Winthrop K, et al. Risk for serious infection with low-dose glucocorticoids in patients with rheumatoid arthritis: a cohort study. Ann Intern Med. 2020;173(11):870–878. doi:10.7326/M20-1594
28. Kerschbaumer A, Sepriano A, Smolen JS, et al. Efficacy of pharmacological treatment in rheumatoid arthritis: a systematic literature research informing the 2019 update of the EULAR recommendations for management of rheumatoid arthritis. Ann Rheum Dis. 2020;79(6):744–759. doi:10.1136/annrheumdis-2019-216656
29. Yu C, Li M, Duan X, et al. Chinese registry of rheumatoid arthritis (CREDIT): i. Introduction and prevalence of remission in Chinese patients with rheumatoid arthritis. Clin Exp Rheumatol. 2018;36(5):836–840.
30. Jin S, Li M, Fang Y, et al. Chinese Registry of rheumatoid arthritis (CREDIT): II. Â prevalence and risk factors of major comorbidities in Chinese patients with rheumatoid arthritis. Arthritis Res Ther. 2017;19(1):251. doi:10.1186/s13075-017-1457-z
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.