Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
A Cross-Sectional Study on the Knowledge and Awareness of Lung Cancer and Screening in Jazan Region, Saudi Arabia
Authors Madkhali MA ![]() , Alhazmi E, Hakami F, Darraj H
, Alhazmi E, Hakami F, Darraj H ![]() , Hamdi S, Hakami KM
, Hamdi S, Hakami KM ![]() , Gadi WH
, Gadi WH ![]() , Sharahily RM, Hufaysi AH, Alhazmi L, Oraibi O
, Sharahily RM, Hufaysi AH, Alhazmi L, Oraibi O ![]() , Alqassimi S
, Alqassimi S ![]() , Mohrag M, Elmakki E
, Mohrag M, Elmakki E
Received 12 August 2023
Accepted for publication 28 November 2023
Published 5 December 2023 Volume 2023:16 Pages 3857—3870
DOI https://doi.org/10.2147/JMDH.S435129
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Mohammed Ali Madkhali,1 Essam Alhazmi,2 Faisal Hakami,2 Hussam Darraj,2 Sulaiman Hamdi,2 Khalid M Hakami,2 Wala H Gadi,2 Raghad Mohammed Sharahily,2 Anwar Hassan Hufaysi,2 Luai Alhazmi,3 Omar Oraibi,3 Sameer Alqassimi,3 Mostafa Mohrag,3 Erwa Elmakki3
1Department of Internal Medicine, Division of Hematology and Oncology, Faculty of Medicine, Jazan University, Jazan, Saudi Arabia; 2Faculty of Medicine, Jazan University, Jazan, Saudi Arabia; 3Internal Medicine Department, Faculty of Medicine, Jazan University, Jazan, Saudi Arabia
Correspondence: Mohammed Ali Madkhali, Department of Internal Medicine, Division of Hematology and Oncology, Faculty of Medicine, Jazan University, Jazan, Saudi Arabia, Tel +966-501450951, Email [email protected]
Background: Lung cancer (LC) is the most common cause of cancer-related deaths worldwide. With lung cancer often diagnosed at advanced stages, understanding the local population’s awareness levels is crucial for designing effective preventive strategies. By identifying gaps in knowledge, the research aims to inform targeted health education efforts, optimize resource allocation, influence policy development, and contribute to the limited body of research on lung cancer awareness in the region, ultimately fostering improved public health outcomes.
Methods: This was a cross-sectional observational study conducted in Jazan region, Saudi Arabia, from July 2022 to June 2023, 671 participants over 18 years old, encompassing both genders, were gsurveyed. Data was collected through a questionnaire covering sociodemographic characteristics and LC-related awareness. SPSS 23 was used for analysis. Factors associated with knowledge scores were explored using independent t-tests and ANOVA, with the Tukey post-hoc test identifying specific group differences.
Results: The study included 671 participants, most participants were between 18 and 35 years (73.5%), with 38.5% males and 61.5% females. Lung cancer (LC) awareness was high (95.1%), with 4.9% reporting a family history. Knowledge assessment revealed a mean score of 14.66, with 41.6% having low, 49.5% moderate, and 8.9% high knowledge levels. Correct responses were notable for recognizing LC as a common cancer, a leading cause of death, and associating smoking and shisha with risk. Symptoms were well identified. Screening awareness was at 63.5%, with 78.8% willing to undergo tests if at risk. Age, marital status, and occupation were associated with knowledge, while factors like gender, nationality, residency, education, income, and smoking status showed no significant associations.
Conclusion: The findings indicate that there are knowledge gaps related to LC and its screening in Jazan region in Saudi Arabia. Effective awareness programs targeting specific sociodemographic groups are needed to improve the early detection and outcomes.
Keywords: lung neoplasms, awareness, knowledge, smoking, health education, public health, risk factors, health literacy, preventive medicine, student health, shisha
A Letter to the Editor has been published for this article.
Introduction
Lung cancer (LC), a significant global health concern, ranks among the most common malignancies worldwide.1,2 In 2018, it accounted for over 1.7 million deaths, solidifying its position as the leading cause of cancer-related mortality.2 Saudi Arabia is no exception, with LC ranking as the 5th most diagnosed cancer and the 3rd most common cause of cancer death.3,4 The incidence of LC in Saudi Arabia has seen a significant rise, with cases increasing roughly 3.5 times from 350 to 1200 between 1990 and 2016.3 Despite this increase, a systematic approach for LC prevention in the primary care setting is currently lacking. Consequently, LC diagnoses often occur in advanced stages.4
Globally, only 15% of LC cases are detected at an early stage; Saudi Arabia’s statistics align with this trend, with just 14% of cases diagnosed early with localized tumors.4 However, early detection via LC screening programs can reduce LC mortality by up to 20%.5,6 Risk factors for LC are numerous and varied, with smoking topping the list. Other risk factors include secondhand smoke, exposure to radon, asbestos, arsenic, diesel exhaust, and certain forms of silica and chromium. Additionally, a personal or family history of lung cancer, radiation therapy to the chest, and dietary factors like beta-carotene supplements have been linked to an increased LC risk.7,8
Symptoms associated with LC include cough, dyspnea (shortness of breath), hemoptysis (coughing up blood), chest pain, and clubbing of the fingers.9 Most LC cases, about 53%, occur in men and women between the ages of 55 and 74.10 Despite increased survival rates for most malignancies, LC is often detected at an advanced stage, resulting in a five-year survival rate of only 5%.1 This late presentation is partially attributed to poor awareness of LC symptoms.11
Improvement in LC outcomes may hinge upon enhancing LC awareness, symptom recognition, early diagnosis, and access to appropriate treatment.12 A Malaysian study revealed that both smokers and non-smokers were willing to undergo LC screening once they were informed of their risk.13 In contrast, 92.8% of USA veterans were willing to screen for LC regardless of their smoking habits.14 Interestingly, most USA veterans in a smoking cessation study viewed LC screening as a stimulating and reflective exercise, despite some feeling anxious during the process.15
In Jazan region in the southwest of Saudi Arabia, there is a high prevalence of LC risk factors such as smoking, respiratory illnesses, and exposure to environmental toxins.4,16 Despite LC is the 3rd leading cause of cancer-related death in Saudi Arabia, there is a lack of a systematic approach to LC prevention, resulting in late-stage diagnoses. The increasing incidence of LC, particularly in the Jazan Region, necessitates a comprehensive assessment of current knowledge, awareness, and screening utilization. With risk factors such as high rates of smoking and exposure to environmental toxins prevalent in the region, understanding the local context becomes crucial. This study aims to uncover specific deficiencies in awareness and screening practices, particularly among various demographic groups, to inform targeted interventions. By addressing these gaps, the research endeavors to contribute valuable insights for the development of effective public health strategies, ultimately enhancing LC awareness, early detection, and improving health outcomes in the Jazan Region.
Methods and Materials
Study Design, Setting and Participants
This was cross-sectional observational study conducted in Jazan region, Saudi Arabia, from July 2022 to June 2023. Jazan region is located in the southwest of Saudi Arabia, north of Yemen, and has a population of around 1.6 million people. The study population included all adults (male and female) over the age of 18 years. The exclusion criteria were being less than 18 years old, refusal to participate in the study, people from outside Jazan province.
Sample Size and Sampling Method
The sample size for this study was determined using the Raosoft sample size calculator and found that 385 participants are required to achieve a 95% confidence interval and a 5% margin of error. A simple random sampling technique used to select participants from the Jazan population.
Data Collection and Study Tool
The data were collected through a self-administered questionnaire, which was developed following a comprehensive review of related articles and consultation with an expert in the field. The questionnaire was crafted in the Arabic language and administered online, with the questionnaire link distributed to the targeted population. It is structured into three sections: the socio-demographic characteristics of participants, general questions regarding lung cancer knowledge and awareness, and inquiries about lung cancer screening procedures. Prior to the main study, a pilot study was conducted involving a group of 20 participants to test the data collection tool. The reliability of the questionnaire was assessed using Cronbach’s alpha test (0.87). Subsequent to the pilot study, certain enhancements, and reorganization of select questions were implemented, leading to necessary changes in the data collection instrument to improve its usability.
Statistical Analysis
Statistical analysis was conducted using the Statistical Package for the Social Sciences, SPSS v.23. Categorical variables were presented using frequencies and percentages, while numerical variables were described with minimum, maximum, mean, and standard deviation. The assessment of factors associated with knowledge scores utilized both independent t-tests and ANOVA tests. Following the ANOVA test, a Tukey post-hoc test was employed to identify specific group differences. The level of significance for all analyses was set at 0.05.
Ethical Consideration
Our study received approval from the Scientific Research Ethics Committee (REC) at Jazan University in Saudi Arabia (reference number: REC-44/02/317; date: September 26, 2022) in accordance with the 1964 Helsinki Declaration and its subsequent amendments. Informed consent was obtained from all participants, and their information is maintained confidentially, with the data solely utilized for scientific purposes.
Results
A total of 671 participants were included in the study, 493 (73.5%) participants fell within the 18–35 years category, 101 (15.1%) were aged 36–45 years, 66 (9.8%) were between 46 and 60 years, and 11 (1.6%) were 61 years and older. In terms of gender, 258 (38.5%) were males, while 413 (61.5%) were females. The majority of 427 (63.6%) were single, 229 (34.1%) married. Most of participants 393 (58.6%) lived in urban areas, while 278 (41.4%) resided in rural areas. Educational levels indicated that 206 (30.7%) were uneducated, 436 (65%) had high school education, a diploma, or less education, and 29 (4.3%) held a bachelor’s degree. Monthly income distribution revealed that most participants earned less than 5000 SR, with 118 (17.6%) falling into the 5000–10,000 SR income bracket, 84 (12.5%) earning between 10,000 and 15,000 SR, and a minority having an income exceeding this range. Table 1
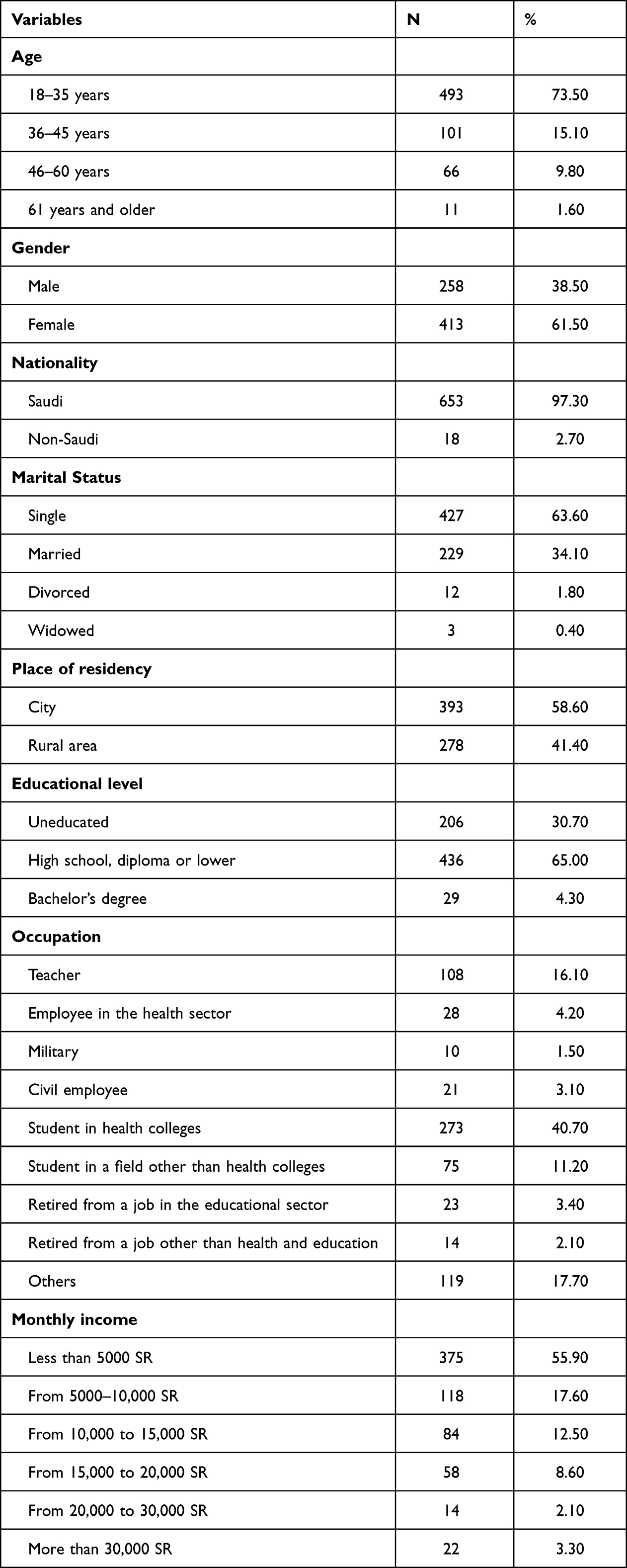 |
Table 1 Socio-Demographic Profile of the Participants (n = 671) |
Table 2 provides the smoking profile of the participants. Out of the total, 66 (9.8%) were smokers, 582 (86.7%) reported that they were not, and 23 (3.4%) indicated they had previously been smokers. Among the current smokers, 44 (66.7%) expressed intentions to quit, 8 (12.1%) stated they were not planning to quit, and 14 (21.2%) were uncertain about their desire to quit. Regarding the presence of family members or friends who smoke, 473 (70.5%) confirmed having a family member or friend who smokes, 179 (26.7%) reported they did not, and 19 (2.8%) were unsure. Of the 473 participants with smoking family members or friends, 408 (86.3%) reported advising their family or friends to quit, while 65 (13.7%) disclosed that they did not provide such advice.
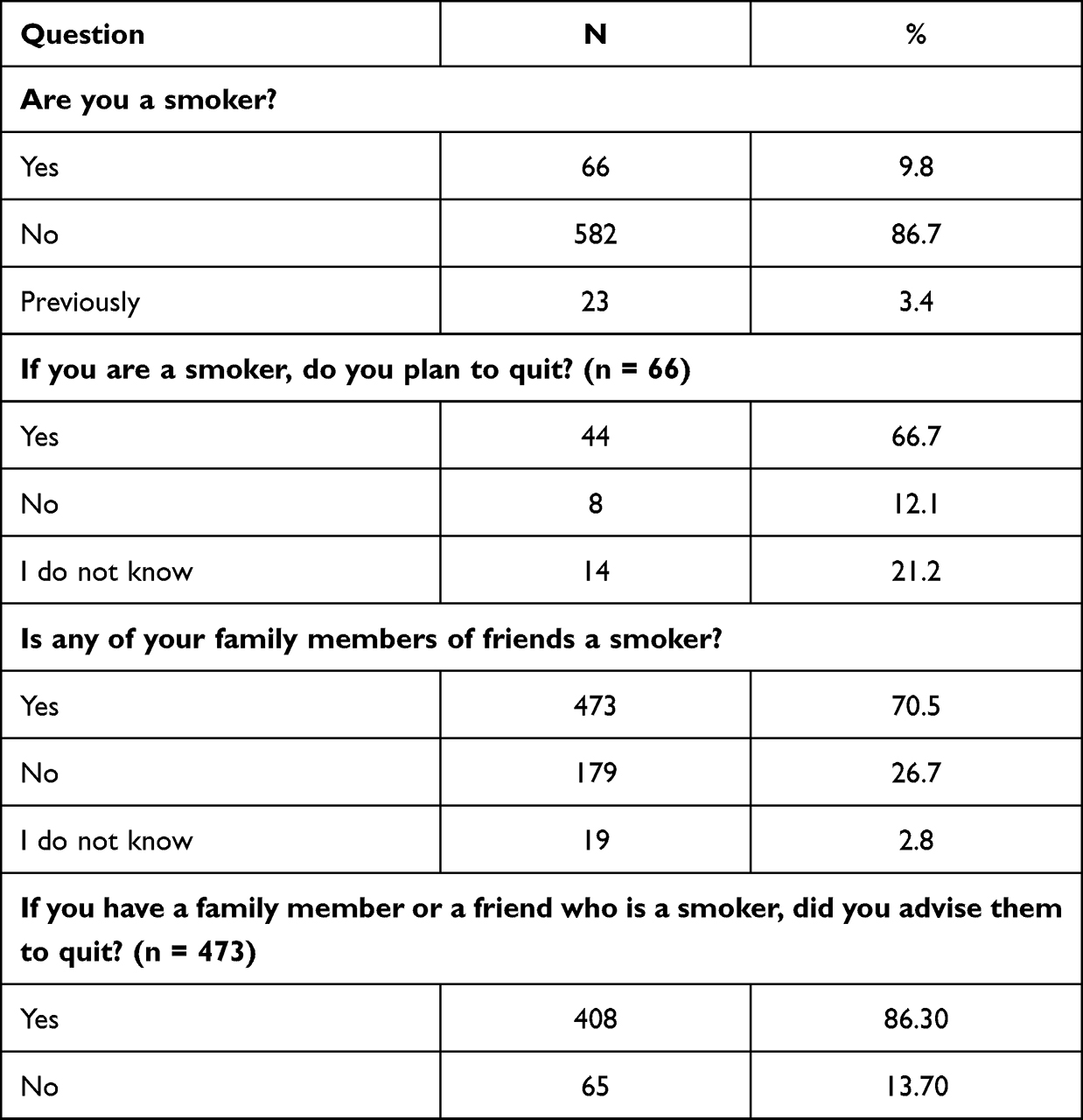 |
Table 2 Smoking Profile of Participants (n = 671) |
When asked if they had ever heard about lung cancer, 416 (95.1%) participants affirmed their prior knowledge, while 33 (4.9%) reported being unaware of lung cancer. When questioned about whether a member of their family had ever had lung cancer, among participants who were already familiar with lung cancer, 31 (4.9%) acknowledged having a family history of lung cancer, 576 (90.3%) denied such a family history, and 31 (4.9%) reported uncertainty about whether they had a family history of lung cancer.
Table 3 presents the participants’ knowledge assessment of lung cancer, indicating a minimum knowledge score of 2, a maximum of 25, and a mean score of 14.66 ± 4.45. 66.6% of participants correctly recognized lung cancer as one of the most common cancers. Additionally, 74.9% of participants provided the accurate response that lung cancer is one of the leading causes of death. Regarding the awareness of risk factors for lung cancer, the majority of participants correctly identified smoking (97.6%) and shisha (93.6%) as risk factors for lung cancer. However, only 16.6% of participants accurately identified that lung cancer is a genetic disease. When questioned about symptoms associated with an increased likelihood of developing lung cancer, the majority of participants concurred that shortness of breath (75.86%), coughing with blood (75.39%), and persistent chest pain (72.10%) are indicative risk factors. The mean knowledge score for participants was 14.66 (SD = 4.45), ranging from a minimum score of 2 to a maximum of 25 out of a possible 27. This suggests an overall moderate level of knowledge among participants regarding lung cancer.
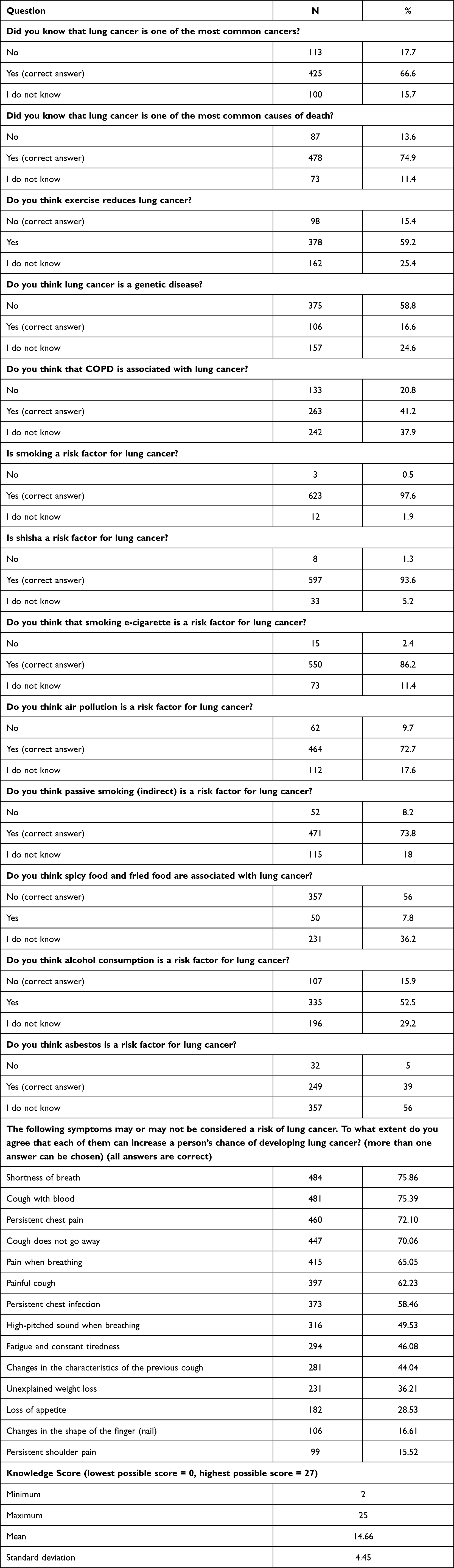 |
Table 3 Participants Knowledge Assessment Toward Lung Cancer (n = 638) |
In Figure 1, the distribution of participants’ knowledge levels toward lung cancer is depicted. Specifically, 279 (41.6%) participants demonstrated a low knowledge level (less than 50% of the total score, ie, a score of 13 or less), 332 (49.5%) exhibited a moderate knowledge level (between 50% and 75% of the total score, ie, a score between 14 and 20), and 60 (8.9%) displayed a high knowledge level (more than 75% of the total score, ie, a score of 21 and above).
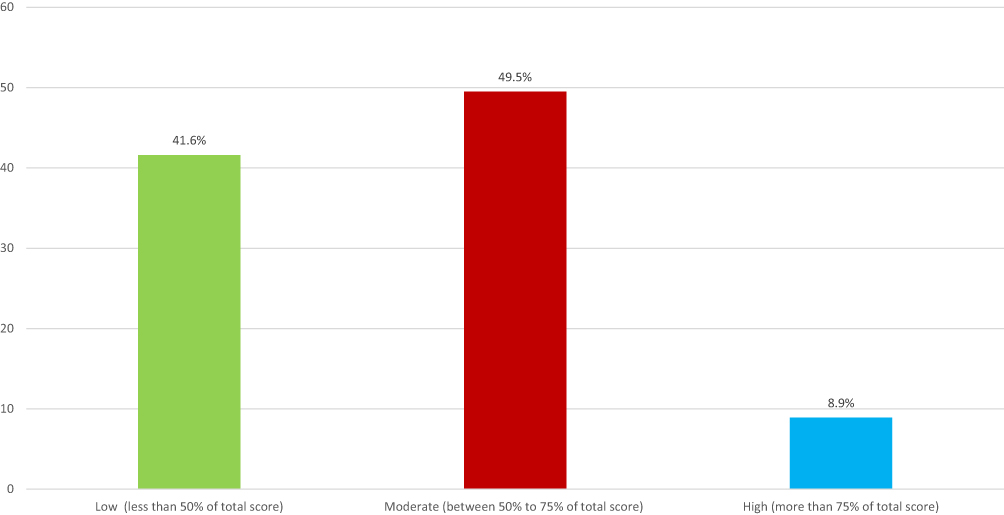 |
Figure 1 Participants Knowledge Levels Toward Lung Cancer. |
Table 4 outlines the screening profile of the participants. A substantial majority, 612 (95.9%) participants, expressed the belief that early detection of lung cancer contributes to preventing death or advanced stages, while 11 (1.7%) reported not holding this belief, and 15 (2.4%) were uncertain. Among the participants, 405 (63.5%) reported awareness of the existence of screening for early detection of lung cancer, with 232 (36.4%) indicating a lack of knowledge about this screening. Among the subset of 405 participants familiar with the screening, 396 (97.8%) believed in the benefits of these tests, 4 (1%) believed there was no benefit, and 5 (1.2%) were uncertain about the benefits. Furthermore, 503 (78.8%) participants expressed willingness to undergo a screening test if they had a risk factor for lung cancer, while 72 (11.3%) reported being unwilling to undergo screening, and 63 (9.9%) were unsure about their willingness.
 |
Table 4 Lung Cancer Screening Profile (n = 638) |
Table 5 presents the factors associated with knowledge of lung cancer. Age exhibited a significant association with knowledge of lung cancer (p < 0.001), indicating that older age groups had lower knowledge levels about lung cancer. The Tukey post-hoc test disclosed that participants aged 18–38 years old had significantly higher knowledge scores compared to every other age group, respectively (p < 0.05). Marital status also demonstrated a significant association with knowledge of lung cancer (p < 0.001), revealing that single participants had the highest knowledge mean score compared to other groups. The Tukey post-hoc test indicated that single participants had a significantly higher knowledge score compared to married participants (p < 0.05). Occupation showed a significant association with knowledge of lung cancer (p < 0.001), with students in health colleges exhibiting the highest knowledge mean score. The Tukey post-hoc test further revealed that students in health colleges had a significantly higher knowledge score (p < 0.05) compared to each of the following groups: teachers, students in fields other than health colleges, and participants retired from a job in the education sector. However, gender, nationality, place of residency, educational level, monthly income, smoking status, intention to quit smoking, having a family member or friend who smokes, and providing advice to family members or friends to quit smoking did not exhibit a significant association with the knowledge score toward lung cancer.
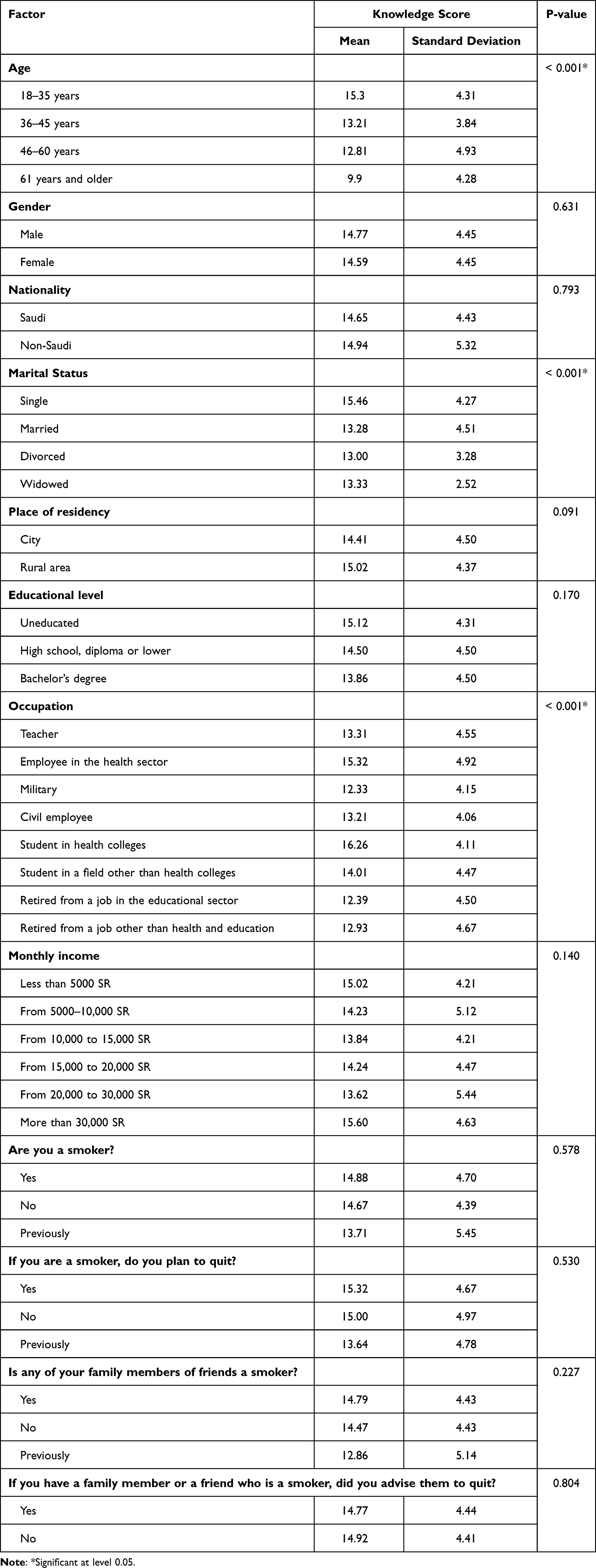 |
Table 5 Factors Associated with Knowledge Toward Lung Cancer |
Discussion
This study offers valuable insights into the sociodemographic characteristics, smoking profile, knowledge, and screening behaviors related to lung cancer (LC) among residents of Jazan, Saudi Arabia. The demographic profile of the participants predominantly consisted of young, female, single individuals residing in cities, with a high school education or less. The majority were Saudi nationals, and the most common occupation was a student at a health college. The mean knowledge score for LC slightly exceeded the midpoint at 14.66 out of 25, but a considerable proportion of participants demonstrated low knowledge levels, with less than 10% classified as having high knowledge. This aligns with findings from other studies in Saudi Arabia and other countries that highlight suboptimal cancer awareness among the general population.17,18 In the current study, most participants had heard of LC before, though a minority reported a family history of the disease, consistent with previous studies.18 The incidence and mortality of LC have significantly increased among the Saudi population in recent decades.4,8 Notably, LC is often diagnosed in the late stages due to few or no symptoms in the early stages.19 Therefore, raising awareness about the risks and promoting early detection can significantly impact a person’s outcome.
The findings reveal a significant association between age, marital status, and occupation with knowledge about lung cancer. Interestingly, no significant association was found between other sociodemographic factors, such as gender, nationality, place of residence, education level, and monthly income, with knowledge about lung cancer. These results are consistent with previous studies that have reported sociodemographic factors influencing health knowledge and behaviors.20,21 The age group 18–35 years exhibited a higher level of knowledge about LC compared to older age groups, possibly due to greater exposure to health information through modern media platforms, which are more frequently used by younger generations.22 Therefore, awareness campaigns should especially target older, married individuals without a healthcare background.
Marital status also exerted a significant impact on knowledge levels, with single individuals displaying higher knowledge scores compared to their married counterparts. This finding contrasts with some previous studies that suggest married individuals often have better health knowledge and behaviors due to the supportive role of spouses.23 However, considering the young age of the majority of our participants, it could be that many of the single individuals are students currently exposed to health education, thereby increasing their knowledge levels. An Asian cohort study indicated that unmarried individuals had a higher risk of total mortality, including cancer.24 Occupation emerged as another significant factor associated with knowledge of lung cancer. Health college students exhibited significantly higher knowledge scores compared to individuals in other occupations. This finding is anticipated due to the nature of their curriculum, which includes learning about diseases such as lung cancer. Our findings align with a study of students at a Malaysian tertiary institution that discovered more than half of those students were knowledgeable about.25 This suggests that health education could be an effective strategy for improving knowledge about LC among the general population.26
In this study, 9.8% of the participants reported being current smokers, a prevalence lower than the global prevalence of tobacco smoking (20.2%).27 This discrepancy may be attributed to the younger age demographic, cultural factors, or potential underreporting of smoking status. Moreover, it is concerning that over 70% of participants reported having family or friends who smoke, yet only 13.7% advised them to quit. Given that second-hand smoke exposure is a well-established risk factor for LC,28 encouraging smoking cessation through public health strategies becomes crucial for mitigating the substantial burden of LC in Saudi Arabia.29 A London study revealed that former (14.5%) and never smokers (13%) believed LC screening was pointless if a person was still smoking.30
Despite the high level of awareness about lung cancer, approximately 41.6% of the participants demonstrated a low level of knowledge about the disease. Similar knowledge gaps have been reported in previous studies from Saudi Arabia and other countries.31–33 Furthermore, about 63.5% of the participants were aware of the existence of LC screening, and a significant majority (78.8%) expressed willingness to undergo screening if they had risk factors for lung cancer. This indicates a positive attitude towards prevention and early detection, suggesting that educational interventions promoting screening could be well received in this population. This finding aligns with previous research highlighting the critical role of early detection in reducing LC mortality.5,6 The study findings underscore the need for comprehensive nationwide LC awareness programs focusing on at-risk groups. Communication campaigns through the media, schools, mosques, and healthcare facilities can help educate the public about LC risk factors, signs and symptoms, and the importance of early detection. Healthcare providers also need training to adhere to standard guidelines for screening high-risk patients, enabling early diagnosis and improved outcomes for lung cancer.
This study’s limitations underscore the need for cautious interpretation of its findings. The cross-sectional design, while adept at capturing a momentary snapshot, precludes establishing causal relationships, limiting insights into the temporal dynamics of lung cancer knowledge and behaviors. The sample’s regional specificity, drawn from Jazan, raises concerns about generalizability to the broader Saudi population, given potential cultural and socioeconomic variations. The skewed age distribution towards younger individuals may not fully represent the nuanced perspectives of older age groups, impacting the broader applicability of the study’s outcomes. Furthermore, reliance on self-reported data introduces the risk of recall and social desirability biases, influencing the accuracy of participants’ responses. While the study illuminates critical aspects of lung cancer awareness in Jazan, these limitations emphasize the importance of considering context and population characteristics when extrapolating the findings to inform broader public health strategies. Addressing these limitations in future research endeavors could refine our understanding of lung cancer awareness and screening practices in Saudi Arabia.
Conclusions
In this study, the findings indicate knowledge gaps related to LC and screening in Jazan region of Saudi Arabia. Effective awareness programs targeting specific sociodemographic groups are needed to improve the early detection and outcomes. Future research should employ a more diverse sample and consider longitudinal designs to enhance the study’s external validity. Incorporating qualitative research methods could also help explore the underlying factors influencing LC knowledge and awareness in more depth. Health education campaigns should be tailored to target older, married individuals, particularly those not in the healthcare field. Greater efforts should be made to raise awareness about the dangers of second-hand smoke and the importance of advising family and friends to quit smoking. Lastly, comprehensive nationwide LC awareness programs are needed, particularly focusing on high-risk groups.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424. doi:10.3322/caac.21492
2. Barta JA, Powell CA, Wisnivesky JP. Global epidemiology of lung cancer. Ann Glob Heal. 2019;85. doi:10.5334/aogh.2419
3. Althubiti MA, Eldein MMN. Trends in the incidence and mortality of cancer in Saudi Arabia. Saudi Med J. 2018;39:1259–1262. doi:10.15537/smj.2018.12.23348
4. Almatroudi A. A retrospective cohort study of lung cancer incidences and epidemiological analysis in Saudi Arabian population from 2006–2016. Int J Environ Res Public Health. 2021;18:11827. doi:10.3390/ijerph182211827
5. Oudkerk M, Liu S, Heuvelmans MA, Walter JE, Field JK. Lung cancer LDCT screening and mortality reduction — evidence, pitfalls and future perspectives. Nat Rev Clin Oncol. 2021;18:135–151. doi:10.1038/s41571-020-00432-6
6. Field JK, Vulkan D, Davies MPA, et al. Lung cancer mortality reduction by LDCT screening: UKLS randomised trial results and international meta-analysis. Lancet Reg Heal Eur. 2021;10:100179. doi:10.1016/j.lanepe.2021.100179
7. Al-Hamdan N, Ravichandran K, Al-Sayyad J, et al. Incidence of cancer in gulf cooperation council Countries, 1998–2001. East Mediterr Health J. 2009;15:600.
8. Jazieh AR, Algwaiz G, Alshehri SM, Alkattan K. Lung Cancer in Saudi Arabia. J Thorac Oncol. 2019;14:957–962. doi:10.1016/j.jtho.2019.01.023
9. Beckles MA, Spiro SG, Colice GL, Rudd RM. Initial evaluation of the patient with lung cancer*. Chest. 2003;123:97S–104S. doi:10.1378/chest.123.1_suppl.97S
10. Torre LA, Siegel RL, Ward EM, Jemal A. Global cancer incidence and mortality rates and trends—an update. Cancer Epidemiol Biomarkers Prev. 2016;25:16–27. doi:10.1158/1055-9965.EPI-15-0578
11. Simon AE, Juszczyk D, Smyth N, et al. Knowledge of lung cancer symptoms and risk factors in the UK: development of a measure and results from a population-based survey. Thorax. 2012;67:426–432. doi:10.1136/thoraxjnl-2011-200898
12. Smith P, Smits S, Owen S, et al. Feasibility and acceptability of a cancer symptom awareness intervention for adults living in socioeconomically deprived communities. BMC Public Health. 2018;18:695. doi:10.1186/s12889-018-5606-3
13. Loh JF, Tan SL. Lung cancer knowledge and screening in the context of the Malaysian population. J Pharm Pract Res. 2018;48:56–64. doi:10.1002/jppr.1341
14. Schluger NW, Koppaka R. Lung disease in a global context. A call for public health action. Ann Am Thorac Soc. 2014;11:407–416. doi:10.1513/AnnalsATS.201312-420PS
15. Zeliadt SB, Heffner JL, Sayre G, et al. Attitudes and perceptions about smoking cessation in the context of lung cancer screening. JAMA Intern Med. 2015;175:1530. doi:10.1001/jamainternmed.2015.3558
16. Al-Ahmadi K, Al-Zahrani A. NO2 and Cancer Incidence in Saudi Arabia. Int J Environ Res Public Health. 2013;10:5844–5862. doi:10.3390/ijerph10115844
17. Ravichandran K, Al-Hamdan N, Mohamed G. Knowledge, attitude, and behavior among Saudis toward cancer preventive practice. J Fam Community Med. 2011;18:135.
18. Dlamini SB, Sartorius B, Ginindza TG. Knowledge, attitudes and practices towards lung cancer among adults in KwaZulu-Natal, South Africa: a cross-sectional survey. J Public Health Africa. 2022;13. doi:10.4081/jphia.2022.2111
19. Ellis PM, Vandermeer R. Delays in the diagnosis of lung cancer. J Thorac Dis. 2011;3:183–188. doi:10.3978/j.issn.2072-1439.2011.01.01
20. Viswanath K, Finnegan JR. The knowledge gap hypothesis: twenty-five years later. Ann Int Commun Assoc. 1996;19:187–228. doi:10.1080/23808985.1996.11678931
21. Chen LS, Kaphingst KA. Risk perceptions and family history of lung cancer: differences by smoking status. Public Health Genomics. 2011;14:26–34. doi:10.1159/000294151
22. Percheski C, Hargittai E. Health information-seeking in the digital age. J Am Coll Heal. 2011;59:379–386. doi:10.1080/07448481.2010.513406
23. Umberson D. Gender, marital status and the social control of health behavior. Soc Sci Med. 1992;34:907–917. doi:10.1016/0277-9536(92)90259-S
24. Leung CY, Huang H-L, Abe SK, et al. Association of marital status with total and cause-specific mortality in Asia. JAMA Netw Open. 2022;5:e2214181. doi:10.1001/jamanetworkopen.2022.14181
25. Thabit H, Zainuddin N. Knowledge and perception on lung cancer and its screening: a study among undergraduate students of the International Islamic University Malaysia, Kuantan Campus. J Biomed Clin Sci. 2017;2:61–66.
26. Czaja R, Manfredi C, Price J. The determinants and consequences of information seeking among cancer patients. J Health Commun. 2003;8:529–562. doi:10.1080/716100418
27. Alison Commar (WHO Jenewa), Vinayak Prasad (WHO Jenewa) ET d’Espaignet (Universitas N, Australia). WHO global report on trends in prevalence of tobacco use; 2000:26.
28. Couraud S, Labonne S, Missy P, et al. BioCAST: le Bio-observatoire national du cancer bronchiques chez les patients non fumeurs (IFCT1002). Rev Mal Respir. 2013;30:576–583. doi:10.1016/j.rmr.2013.03.006
29. Moradi-Lakeh M, El Bcheraoui C, Tuffaha M, et al. Tobacco consumption in the Kingdom of Saudi Arabia, 2013: findings from a national survey. BMC Public Health. 2015;15:611. doi:10.1186/s12889-015-1902-3
30. Quaife SL, McEwen A, Janes SM, Wardle J. Attitudes towards lung cancer screening in socioeconomically deprived and heavy smoking communities: informing screening communication. Heal Expect. 2017;20:563–573. doi:10.1111/hex.12481
31. Rutten LJF, Arora NK, Bakos AD, Aziz N, Rowland J. Information needs and sources of information among cancer patients: a systematic review of research (1980–2003). Patient Educ Couns. 2005;57:250–261. doi:10.1016/j.pec.2004.06.006
32. Shankar A, Roy S, Bhandari R, et al. Level of awareness of lung cancer risk factors, signs, symptoms and safe practices among college teachers of different states in India: do awareness programmes have an impact on adoption of safe practices? Gulf J Oncolog. 2015;1:57–62.
33. Hanson HM, Raag M, Adrat M, Laisaar T. Awareness of lung cancer symptoms and risk factors in general population. Open J Respir Dis. 2017;07:1–11. doi:10.4236/ojrd.2017.71001
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.