Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 18
A Cross-Sectional Study of the Association Between Uric Acid-to-High-Density Lipoprotein Cholesterol Ratio and Carotid Atherosclerosis in Patients with Type 2 Diabetes Mellitus
Authors Huang C ![]() , Luo Y, Huang J, Qiu X, Tu M
, Luo Y, Huang J, Qiu X, Tu M ![]()
Received 9 March 2025
Accepted for publication 28 July 2025
Published 14 August 2025 Volume 2025:18 Pages 2873—2883
DOI https://doi.org/10.2147/DMSO.S527130
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Pablo Corral
Cuihua Huang,1 Yan Luo,2 Jianqing Huang,1 Xiuping Qiu,1 Mei Tu1
1Longyan First Affiliated Hospital of Fujian Medical University, Longyan, Fujian, 364000, People’s Republic of China; 2State Grid Longyan Electric Power Supply Company, Longyan, Fujian, 364031, People’s Republic of China
Correspondence: Xiuping Qiu, Email [email protected] Mei Tu, Email [email protected]
Background: Carotid atherosclerosis (CAS) is a key diabetic complication needing predictive biomarkers. The serum uric acid-to-high-density lipoprotein cholesterol ratio (UHR), linked to metabolic dysfunction, may serve this role. Therefore, this cross-sectional study examines UHR-CAS association in type 2 diabetes.
Methods: This study included 615 type 2 diabetes patients, collecting demographic, biochemical, and carotid ultrasound data. Spearman correlation analyzed UHR’s relationship with cardiovascular risk factors. Multivariate logistic regression combined with stratified regression modeling assessed UHR’s independent link with CAS, while receiver operating characteristic (ROC) analysis evaluated its predictive value.
Results: CAS patients showed elevated UHR and cardiovascular risk markers (age, body mass index [BMI], homeostatic model assessment of insulin resistance [HOMA-IR], systolic blood pressure, low-density lipoprotein cholesterol [LDL-c], triglycerides, smoking) compared to controls (P < 0.05). UHR tertiles demonstrated dose–response associations with carotid intima-media thickness (cIMT) ≥ 1.0 mm, plaque formation, and CAS (P < 0.05). UHR exhibited positively with BMI, HOMA-IR, systolic blood pressure, triglycerides, uric acid (UA), and cIMT (P < 0.05), but inversely with total cholesterol, high-density lipoprotein cholesterol (HDL-c), and LDL-c (P < 0.05). UHR independently predicted carotid plaques (OR: 1.086, 95% CI: 1.033– 1.142, P = 0.001) and CAS (OR: 1.097, 95% CI: 1.035– 1.162, P = 0.002). Stronger associations occurred in BMI ≥ 25 kg/m² (OR: 1.210, 95% CI: 1.089– 1.345, P < 0.001) and hypertension subgroups (OR: 1.136, 95% CI: 1.033– 1.248, P = 0.008). ROC analysis demonstrated UHR’s superior CAS prediction (AUC = 0.656, 95% CI: 0.611– 0.701, P < 0.01) over triglyceride-to-HDL-c ratio, triglyceride-glucose index, HDL-c, and UA (P < 0.05).
Conclusion: UHR is an independent CAS risk factor in type 2 diabetes, outperforming traditional biomarkers for cardiovascular risk assessment.
Keywords: carotid atherosclerosis, type 2 diabetes mellitus, uric acid-to-high-density lipoprotein cholesterol ratio
Introduction
Cardiovascular disease (CVD) represented a significant burden in diabetic populations. Epidemiological studies demonstrated that CVD was the leading cause of mortality among individuals with diabetes, accounting for approximately 50% of deaths.1 Atherosclerosis, characterized by arterial wall thickening and plaque formation, served as the primary pathological basis for CVD due to its association with vascular stenosis and impaired blood flow.2 Previous research indicated that carotid atherosclerosis (CAS) in patients with type 2 diabetes mellitus strongly correlated with the occurrence of cardiovascular events, including myocardial infarction and stroke.3,4 These findings highlighted the importance of investigating CAS risk factors to improve CVD prevention and management in diabetic patients.
Uric acid (UA) and high-density lipoprotein cholesterol (HDL-c) were well-established biomarkers of cardiovascular health.5–8 Elevated UA levels were associated with lipid metabolism disorders, inflammation, and endothelial dysfunction, all of which contributed to atherosclerosis pathogenesis.9 In contrast, HDL-c played a protective role by improving lipid metabolism, exerting anti-inflammatory effects, and maintaining vascular endothelial function.10 Patients with type 2 diabetes mellitus commonly exhibited elevated UA levels and reduced HDL-c levels, both of which were associated with increased CVD risk.11,12 Recently, the serum uric acid-to-high-density lipoprotein cholesterol ratio (UHR) emerged as a novel composite biomarker for cardiovascular risk assessment, integrating both UA and HDL-c measurements. Studies demonstrated that UHR was strongly correlated with the occurrence of metabolic syndrome and adverse cardiovascular prognosis.13–16 Emerging clinical evidence has further substantiated the strong correlations between UHR and extra-cardiac complications in type 2 diabetes mellitus cohorts, with particularly compelling links observed for kidney injury and non-alcoholic fatty liver disease progression.17,18 However, research investigating the potential correlation between UHR and CAS in this specific population remained notably scarce, warranting further comprehensive investigation.
Therefore, this study attempted to investigate the association between UHR and CAS in patients with type 2 diabetes mellitus through a cross-sectional analysis. By identifying UHR as a potential biomarker, this research provided evidence for developing precise CVD prevention strategies in type 2 diabetes mellitus cohorts.
Materials and Methods
Study Population
This study consecutively enrolled adults with type 2 diabetes mellitus admitted to the metabolic management center at Longyan First Affiliated Hospital of Fujian Medical University from June 2023 to March 2024. Inclusion criteria were: (1) age ≥18 years; and (2) T2DM diagnosis confirmed per American Diabetes Association (ADA) guidelines.19 Exclusion criteria included: (1) acute diabetic complications (eg, diabetic ketoacidosis or hyperosmolar hyperglycemic syndrome); (2) severe renal/hepatic impairment (eg, end-stage renal disease or hepatic cirrhosis); (3) active infections, malignancies, or autoimmune disorders; (4) incomplete carotid ultrasound data; and (5) current use of UA modifying agents (eg, febuxostat, thiazide diuretics). After screening, 615 eligible participants were included in the final analysis.
General Condition and Biochemical Index Collection
Demographic characteristics (gender, age), clinical parameters (duration of diabetes mellitus, height, weight, blood pressure), and behavioral factors (smoking history defined as ≥1 cigarette/day or ≥7 cigarettes/week for six consecutive months) were documented using standardized questionnaires. Anthropometric measurements (height and weight) were obtained with calibrated instruments; blood pressure measurements were performed in triplicate following standardized protocols. Fasting venous blood samples were analyzed using a Cobas 8000 automated biochemical analyzer (Roche Diagnostics), with hemoglobin A1c (HbA1c) quantified via high-performance liquid chromatography (Bio-Rad D10 system). Biochemical parameters included: Fasting blood glucose (FBG), total cholesterol (TC), triglycerides (TG), low-density lipoprotein cholesterol (LDL-c), HDL-c, UA, creatinine (Cr), blood urea nitrogen (BUN), alanine aminotransferase (ALT), and albumin.
Derived indices comprised: (1) body mass index (BMI) = weight (kg)/height² (m²); (2) homeostatic model assessment of insulin resistance (HOMA-IR) = [fasting glucose (mmol/L) × fasting insulin (μU/mL)]/22.5; (3) uric acid-to-HDL-C ratio (UHR) = [UA (mg/dL)/HDL-C (mg/dL)] ×100; (4) triglyceride-to-HDL-C ratio (THR) = [TG (mg/dL)/HDL-C (mg/dL)]; and (5) triglyceride-glucose index (TyG) = ln[fasting TG (mg/dL) × fasting glucose (mg/dL)/2].
CAS Definition
Carotid ultrasound examinations were performed using a high-resolution B-mode ultrasound system (Philips EPIQ 5, L12-5 MHz linear array transducer). All scans were conducted by a certified vascular sonographer following standardized positioning protocols with participants positioned supine and the neck slightly extended. Carotid intima-media thickness (cIMT) was measured at 1 cm proximal to the carotid bifurcation, and the mean value of bilateral measurements was recorded as the final cIMT (unit: mm). Carotid intimal thickening was defined as cIMT ≥1.0 mm, while carotid plaque was identified as either focal protrusion exceeding 50% of adjacent vessel wall thickness or cIMT ≥1.5 mm. CAS required documented carotid intimal thickening or plaque presence.20
Statistical Analysis
SPSS 24.0 statistical software was utilized for data analysis in this study. Based on distribution characteristics, measurement data with normal distribution were expressed as mean ± standard deviation (x±s), while non-normally distributed data were presented as median (interquartile range) [M (IQR)]. Categorical data were described as number of cases (percentage) [n (%)]. For inter-group comparisons, normally distributed continuous variables were analyzed using independent-samples t-test or one-way analysis of variance, while non-normally distributed variables were compared via Mann–Whitney U-test or Kruskal–Wallis test; categorical variables were assessed by chi-square test or Fisher’s exact test. Spearman correlation analysis evaluated correlations between UHR and indicators including BMI, blood pressure, blood lipids, and insulin resistance. Multivariate logistic regression analyzed the independent association between UHR and CAS, while hierarchical logistic regression explored influencing factors. Receiver operating characteristic (ROC) curves evaluated the predictive performance of metabolic indicators (UHR, THR, TyG, HDL, UA) for CAS. A two-tailed test was conducted with α=0.05, and P<0.05 was deemed statistically significant.
Results
Basic Characteristics of the Study Population
The study included 615 patients with type 2 diabetes mellitus after excluding 45 patients based on predefined criteria (as shown in Figure 1), with 220 patients in the non-CAS group and 395 patients in the CAS group. Baseline characteristics are summarized in Table 1. The table clearly illustrated whether the study groups were well-balanced in baseline characteristics or exhibited clinically relevant differences in demographic and clinical parameters. The mean age of patients was 60.02 ± 11.54 years, with 55.45% being male. The CAS group exhibited significantly higher age, greater male proportion, longer diabetes duration, and increased cIMT compared with the non-CAS group (P < 0.05) . In addition, the CAS group demonstrated higher cardiovascular risk markers including BMI, HOMR-IR, SBP, TC, LDL-c, TG, UA, UHR, THR, and TyG levels, alongside reduced HDL-c (P < 0.05) . Additionally, creatinine, BUN, smoking prevalence, hypertension rates, and use of anti-arteriosclerotic medications were significantly higher in the CAS group (P < 0.05).
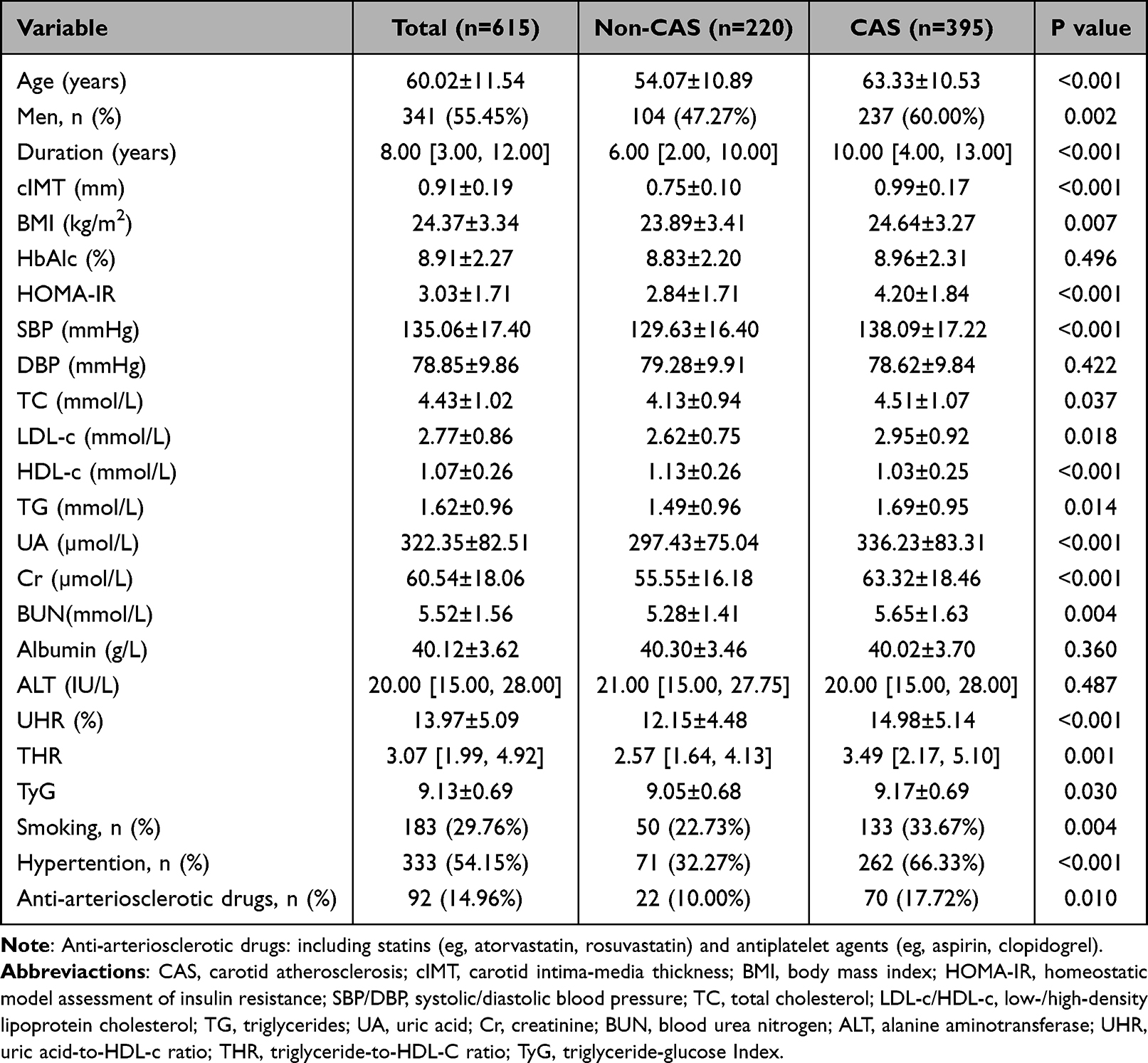 |
Table 1 Comparison of Baseline Data Between Non-CAS and Comorbid CAS Patients |
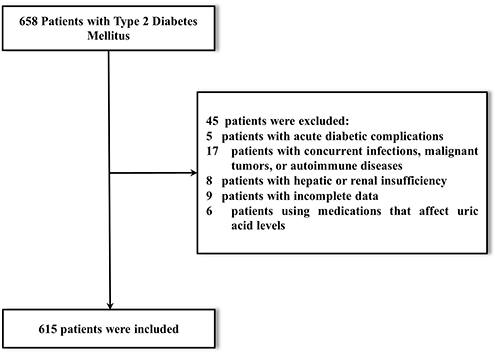 |
Figure 1 Participant flow diagram: inclusion and exclusion process. |
Differences in the Incidence of cIMT ≥ 1mm, Carotid Plaque Formation, and CAS According to UHR Tertiles
When patients were stratified into tertiles based on UHR, the incidence of cIMT ≥1.0 mm, carotid plaque formation, and CAS showed a significant increase across ascending UHR tertiles, indicating a dose–response relationship between elevated UHR and these CAS outcomes (as shown in Figure 2, P <0.05).
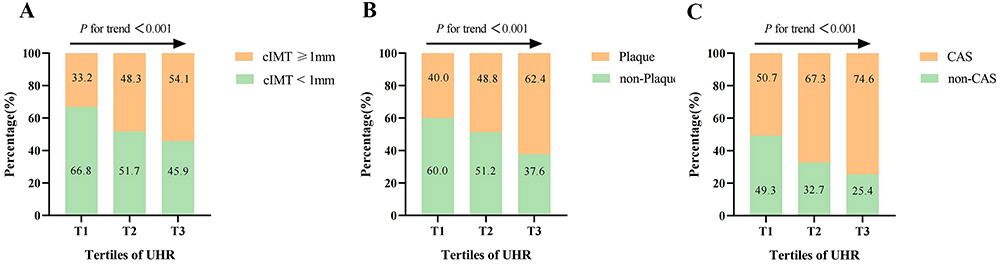 |
Figure 2 Comparison of incidence rates of cIMT≥1 mm (A), carotid plaque formation (B), and CAS (C) across UHR tertiles. Abbreviactions: cIMT, carotid intima-media thickness; CAS, carotid atherosclerosis; UHR, uric acid-to-HDL-c ratio. |
Correlation Analysis Between UHR and Cardiovascular Risk Factors as Well as cIMT
Correlation analysis in Table 2 demonstrated significant associations between UHR and key cardiometabolic parameters. Specifically, UHR demonstrated positive correlations with BMI, HOMA-IR, SBP, TG, and UA; negative correlations with TC, LDL-c, and HDL-c (all P < 0.05). These results suggest that UHR is associated with multiple cardiovascular risk factors. Notably, as shown in Figure 3, UHR displayed a particularly strong positive correlation with cIMT (r = 0.181, P < 0.001), suggesting its potential clinical relevance in CAS assessment.
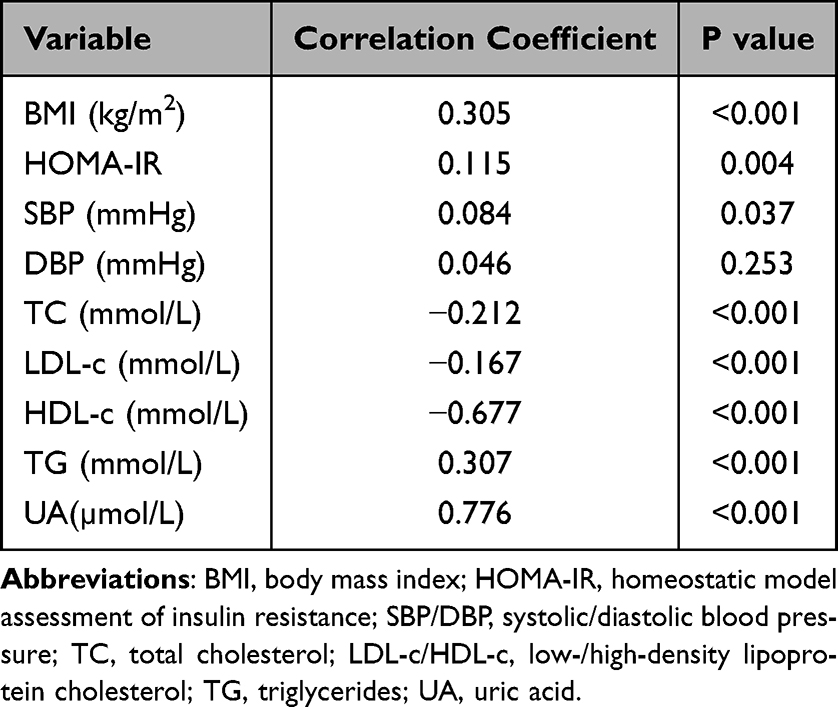 |
Table 2 Correlation Analysis Between UHR and Other Metabolic Indicators |
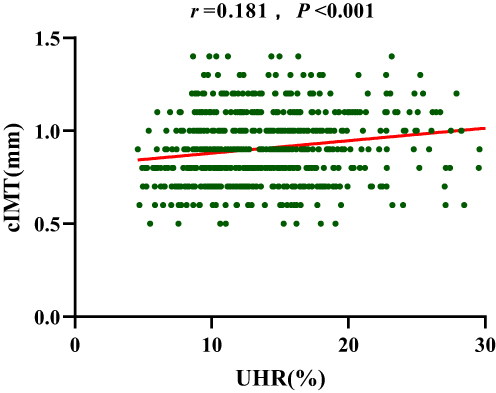 |
Figure 3 Correlation analysis between UHR and cIMT. Abbreviactions: cIMT, carotid intima-media thickness; UHR, uric acid-to-HDL-c ratio. |
Multivariate Logistic Regression Analysis of UHR with cIMT≥1mm, Carotid Plaque, and CAS
As shown in Figure 4, multivariate logistic regression analysis showed that after adjusting for potential confounding factors, UHR did not significantly increase the risk of cIMT ≥1 mm (OR: 1.048, 95% CI: 0.999–1.100, P = 0.056). However, UHR was independently associated with an increased risk of carotid plaque formation (OR: 1.086, 95% CI: 1.033–1.142, P = 0.001) and CAS (OR: 1.097, 95% CI: 1.035–1.162, P = 0.002).
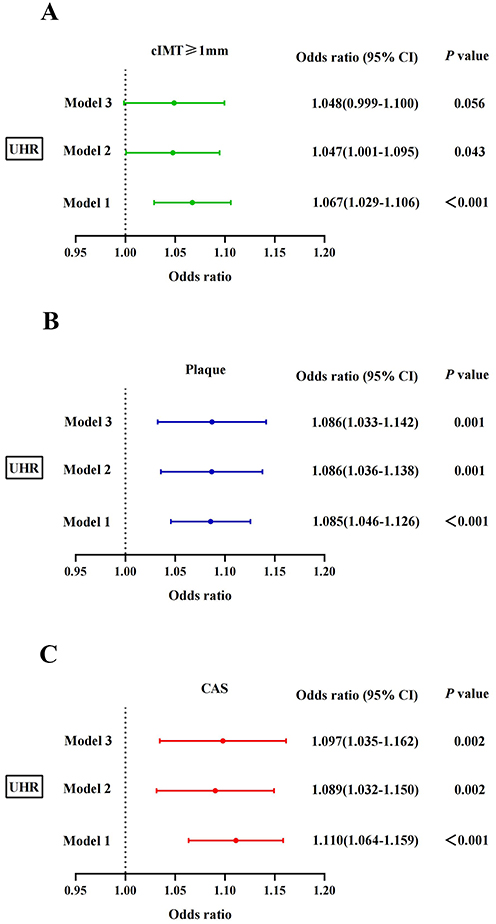 |
Figure 4 Logistic regression analysis of the association between UHR and cIMT ≥1 mm (A), carotid plaque formation (B), and CAS (C). Model 1: adjusted for sex and age. Model 2: further adjusted for duration of diabetes mellitus, body mass index, homeostatic model assessment of insulin resistance, systolic blood pressure, diastolic blood pressure, total cholesterol, triglycerides, and low-density lipoprotein cholesterol based on Model 1. Model 3: additionally adjusted for creatinine, blood urea nitrogen, alanine aminotransferase, smoking status, and anti-arteriosclerotic medications based on Model 2. Abbreviactions: cIMT, carotid intima-media thickness; CAS, carotid atherosclerosis; UHR, uric acid-to-HDL-c ratio. |
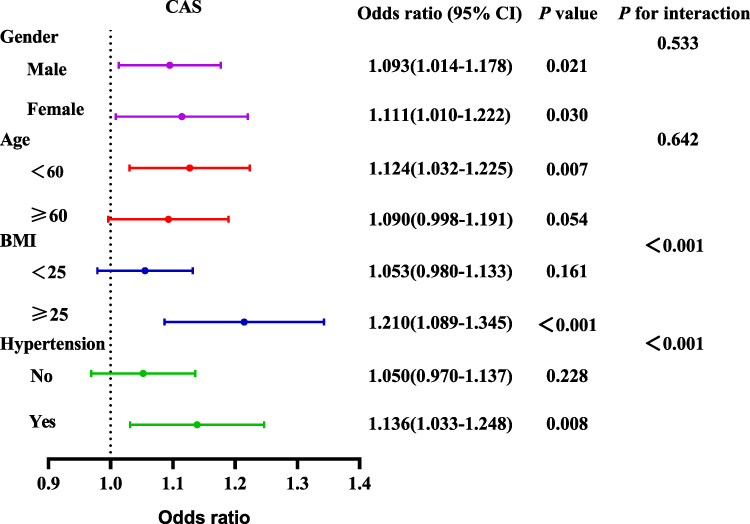 |
Figure 5 Stratified regression analysis of UHR and carotid atherosclerosis stratified by sex, age, BMI, and hypertension. Abbreviations: BMI, body mass index; CAS, carotid atherosclerosis. |
Hierarchical Logistic Regression Analysis of the Association Between UHR and CAS
The relationship between UHR and CAS was further assessed in as shown in Figure 5 after stratification by sex, age, BMI, and hypertension status. The results demonstrated that this relationship was modified by BMI and hypertension, with the independent association primarily observed in individuals with BMI ≥ 25 kg/m² (OR: 1.210, 95% CI: 1.089–1.345, P < 0.001), and hypertension (OR: 1.136, 95% CI: 1.033–1.248, P = 0.008), regardless of age or gender (P for interaction>0.05).
ROC Curve Analysis for Evaluating the Predictive Performance of UHR
As shown in Figure 6 and Table 3, ROC curve analysis was performed to evaluate the predictive performance of UHR for CAS. The area under the curve (AUC) for UHR was 0.656 (95% CI: 0.611–0.701, P < 0.001), with an optimal cutoff value of 13.070. At this threshold, UHR exhibited a sensitivity of 60.3% and a specificity of 63.6% for predicting CAS. Additionally, the AUCs of THR, TyG, 1/HDL-c, and UA were calculated for comparison. UHR demonstrated a significantly higher AUC value compared with THR (P = 0.035), TyG (P = 0.001), 1/HDL-c (P = 0.047), and UA (P = 0.041).
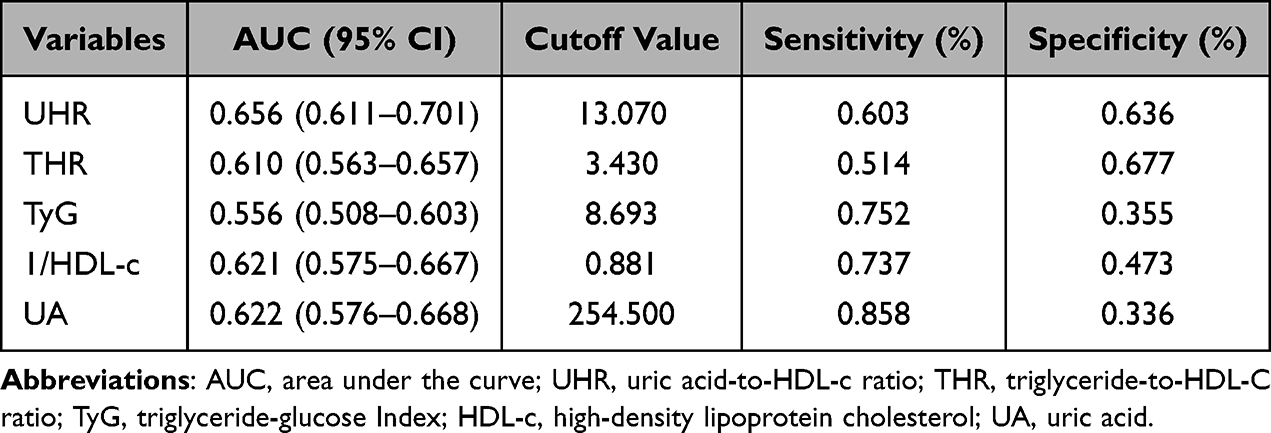 |
Table 3 ROC Analysis of UHR, THR, TyG, HDL-c, and UA in Identifying CAS |
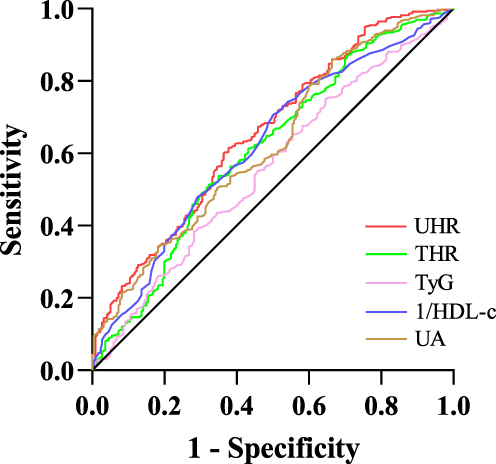 |
Figure 6 ROC analysis of UHR, THR, TyG, HDL-c, and UA for predicting CAS. Abbreviations: TyG, triglyceride-glucose Index; HDL-c, high-density lipoprotein cholesterol; UA, uric acid; UHR, uric acid-to-HDL-c ratio; THR, triglyceride-to-HDL-C ratio. |
Discussion
Diabetic patients bear a heavy burden of cardiovascular diseases, with cardiovascular and cerebrovascular events constituting the leading causes of mortality.21 CAS, a validated early marker of systemic atherosclerosis, is strongly associated with cardiovascular risk in this population.22 Therefore, this study investigated the relationship between UHR and CAS in diabetic patients, thereby providing novel insights for early cardiovascular risk stratification. Consistent with our hypothesis, we observed elevated UHR levels in the CAS group compared to the non-CAS cohort (P < 0.05). Correlation analysis revealed significant positive associations between UHR and cardiovascular risk factors, including BMI, HOMA-IR, SBP, and TG. After adjusting for confounders, UHR independently correlated with plaque formation and CAS in diabetic patients. Furthermore, stratified analysis demonstrated that the association between UHR and CAS was primarily manifested in overweight individuals (BMI ≥ 25 kg/m²) and hypertensive subgroups, whereas no significant gender- or age-related differences were observed. Clinically, UHR outperformed traditional markers (THR, TyG, HDL-c, and UA) in predicting CAS risk, as evidenced by ROC curve analysis (AUC: 0.656 vs 0.556–0.622, P < 0.05).
Mounting clinical evidence has firmly established hyperuricemia as an independent risk factor for CAS.23–25 In this context, the UHR has gained prominence as a novel integrated biomarker that simultaneously reflects purine metabolism and lipid homeostasis in cardiovascular pathophysiology.26,27 A cohort study involving 48,054 participants showed 16% and 20% increased risks for all-cause and cardiovascular mortality, respectively, in the highest UHR quintile.28 Relevant investigations further demonstrated UHR’s predictive value for coronary hemodynamic abnormalities29 and its association with vulnerable plaque characteristics including rupture, erosion, and thrombosis formation.30 Critically, accumulating clinical evidence had established that the UHR independently predicted multiple diabetes-associated complications in patients with type 2 diabetes mellitus, particularly lower extremity arterial disease, chronic kidney disease, and steatotic liver disease.31–33 Our findings corroborated and extended these observations through multivariate analysis that showed each 1% UHR increment conferred 8.6% and 9.7% increased risks for carotid plaque and CAS, respectively, in type 2 diabetes patients. This risk amplification was particularly pronounced in subjects with BMI ≥25 kg/m² or hypertension, suggesting synergistic vascular injury from metabolic derangements. Notably, in head-to-head comparisons with established metabolic markers (THR, TyG, UA, and HDL-c),34,35 UHR demonstrated superior predictive performance for CAS risk assessment.
Our study provided mechanistic insights into UHR’s role in cardiovascular risk among type 2 diabetes patients. Blood pressure, insulin resistance, and dyslipidemia were established as major cardiovascular risk factors that significantly elevated risks of both atherosclerosis development and subsequent cardiovascular events.36–38 The positive correlation between UHR and SBP observed in this study aligns with prior research findings.39 However, no significant association was observed between UHR and DBP in the current cohort. This discrepancy may reflect hyperuricemia’s specific effects on vascular tension and hemodynamics, which predominantly influencing SBP rather than DBP.40 Recent large-scale clinical evidence has established that elevated UHR levels independently predict worsened insulin resistance and impaired glycemic control.41 Our investigation in a type 2 diabetes cohort further substantiated these findings, demonstrating a significant positive association between UHR and HOMA-IR. At the molecular level, we propose that hyperuricemia-induced oxidative stress in adipocytes may serve as a key pathological mechanism, driving both ectopic lipid deposition and the development of insulin resistance.42 Lipid profile analysis further demonstrated a significant positive association between UHR and TG levels, implying that elevated UHR might contribute to atherogenesis through dysregulated lipid metabolism. Interestingly, UHR demonstrated a consistent inverse association with TC, LDL-c, and HDL-c. Although HDL-c was conventionally considered cardioprotective, its levels might be modulated by TC and LDL-c concentrations. These apparently contradictory associations could be explained by common underlying metabolic mechanisms, with cholesterol ester transfer protein activity representing a plausible mediator of these complex interactions.43
The pathophysiological mechanism between UHR and CAS in type 2 diabetes remains unclear, but it may involve synergistic interactions among inflammation, oxidative stress, endothelial dysfunction, and metabolic disorders. Previous investigation demonstrated that hyperuricemia activated the NLRP3 inflammasome pathway, which promoted inflammatory cytokine release (eg, interleukin-1β and interleukin-18) and triggered chronic vascular inflammation, ultimately accelerating atherogenesis.44 Concurrently, hyperuricemia exacerbated oxidative stress through increased production of reactive oxygen species, which damaged vascular endothelial cells and facilitated LDL-c oxidation.45 Notably, multiple clinical studies consistently reported that reduced HDL-c levels impaired its anti-inflammatory and antioxidant functions, including impaired inhibition of inflammatory factor release, reduced free radical scavenging and defective reverse cholesterol transport mechanisms.7,46 These findings confirmed that such dysfunctions directly contributed to amplified lipid deposition in arterial walls. Furthermore, the imbalance between UA and HDL-c synergistically induced endothelial dysfunction, characterized by reduced nitric oxide (NO) production, impaired vasodilation, and increased release of vasoconstrictors such as endothelin-1, collectively exacerbating vascular damage.47–49
In conclusion, our multivariate regression analysis demonstrates that UHR serves as a significant independent predictor of CAS in patients with type 2 diabetes mellitus, exhibiting superior discriminative capability compared to traditional biomarkers. These findings underscore UHR’s potential clinical value for CAS risk assessment in patients with type 2 diabetes mellitus. While this study provides the first evidence of an association between UHR and CAS in type 2 diabetes populations, several methodological limitations warrant careful interpretation. First, the predominantly cross-sectional design precluded definitive conclusions regarding causal relationships between the UHR and CAS. Second, substantial heterogeneity in genetic profiles, lifestyle factors, and metabolic characteristics across populations constrained the generalizability of the findings. Additionally, while the study included patients from real-world clinical settings where comorbidities were common, this aspect introduced potential confounding effects. Consequently, large-scale, multicenter studies are imperative to validate the clinical significance of UHR and its potential for guiding CAS management in type 2 diabetes mellitus patients.
Data Sharing Statement
The datasets will be made available from the corresponding author upon reasonable request.
Ethical Statement
The study protocol adhered to the Declaration of Helsinki and received ethical approval from the Institutional Ethics Committee of Longyan First Affiliated Hospital of Fujian Medical University (Approval No. IC-2022-009). All participants provided written informed consent forms prior to enrollment.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study did not receive any financial support from funding agencies.
Disclosure
The authors declare that there are no competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. An Y, Zhang P, Wang J, et al. Cardiovascular and all-cause mortality over a 23-year period among Chinese with newly diagnosed diabetes in the da qing IGT and diabetes study. Diabetes Care. 2015;38(7):1365–1371. doi:10.2337/dc14-2498
2. Madaudo C, Coppola G, PARLATI ALM, et al. Discovering inflammation in atherosclerosis: insights from pathogenic pathways to clinical practice. Int J Mol Sci. 2024;25(11):6016. doi:10.3390/ijms25116016
3. Brohall G, Odén A, Fagerberg B. Carotid artery intima‐media thickness in patients with Type 2 diabetes mellitus and impaired glucose tolerance: a systematic review. Diabetic Med. 2005;23(6):609–616. doi:10.1111/j.1464-5491.2005.01725.x
4. Wong ND, Sattar N. Cardiovascular risk in diabetes mellitus: epidemiology, assessment and prevention. Nat Rev Cardiol. 2023;20(10):685–695. doi:10.1038/s41569-023-00877-z
5. Du L, Zong Y, LI H, et al. Hyperuricemia and its related diseases: mechanisms and advances in therapy. Signal Transduction Targeted Ther. 2024;9(1).
6. Zheng Y, Chen Z, Yang J, et al. The role of hyperuricemia in cardiac diseases: evidence, controversies, and therapeutic strategies. Biomolecules. 2024;14(7):753. doi:10.3390/biom14070753
7. Diaz L, Bielczyk-Maczynska E. High-density lipoprotein cholesterol: how studying the ‘good cholesterol’ could improve cardiovascular health. Open Biology. 2025;15(2). doi:10.1098/rsob.240372
8. Benkhoff M, Polzin A. Lipoprotection in cardiovascular diseases. Pharmacol Ther. 2024;264.
9. Wojtasińska A, Frąk W, Lisińska W, et al. Novel insights into the molecular mechanisms of atherosclerosis. Int J Mol Sci. 2023;24(17):13434. doi:10.3390/ijms241713434
10. Madaudo C, Bono G, Ortello A, et al. Dysfunctional high-density lipoprotein cholesterol and coronary artery disease: a narrative review. J Personalized Med. 2024;14(9):996. doi:10.3390/jpm14090996
11. Won K-B, Choi S-Y, Chun EJ, et al. Sex difference in the risk of coronary artery calcification progression related to hyperuricemia among asymptomatic 12,316 Korean adults. Sci Rep. 2024;14(1). doi:10.1038/s41598-024-80324-2.
12. Wan H, Wu H, Wei Y, et al. Novel lipid profiles and atherosclerotic cardiovascular disease risk: insights from a latent profile analysis. Lipids Health Dis. 2025;24(1). doi:10.1186/s12944-025-02471-3.
13. Kolahi Ahari R, Mansoori A, Sahranavard T, et al. Serum uric acid to high‐density lipoprotein ratio as a novel indicator of inflammation is correlated with the presence and severity of metabolic syndrome: a large‐scale study. Endocrinol Diabetes Metabol. 2023;6(6).
14. Yin J, Zheng C, Li Z, et al. Gender differences in the association between the uric acid to high-density lipoprotein cholesterol ratio and diabetes risk: a mediation analysis of c-reactive protein, triglycerides, and insulin resistance. Lipids Health Dis. 2024;23(1). doi:10.1186/s12944-024-02404-6.
15. Yang F, Wang J, Wu S, et al. Effect of cumulative uric acid to high-density lipoprotein cholesterol ratio on myocardial infarction in prospective cohorts. Curr Prob Cardiol. 2025;50(1):102889. doi:10.1016/j.cpcardiol.2024.102889
16. Lai X, Chen T. Association of serum uric acid to high-density lipoprotein cholesterol ratio with all-cause and cardiovascular mortality in patients with diabetes or prediabetes: a prospective cohort study. Front Endocrinol. 2024;15.
17. Aktas G, Yilmaz S, Kantarci DB, et al. Is serum uric acid-to-HDL cholesterol ratio elevation associated with diabetic kidney injury? Postgraduate Med. 2023;135(5):519–523. doi:10.1080/00325481.2023.2214058
18. Cui Y, Qu Z, Hu W, et al. Relationship between uric acid to high density lipoprotein cholesterol ratio and nonalcoholic fatty liver disease in nonoverweight/obese patients with type 2 diabetes. Int J Endocrinol. 2023;2023:1–7. doi:10.1155/2023/2513175
19. Elsayed NA, Aleppo G, Bannuru RR, et al. 2. diagnosis and classification of diabetes:standards of care in diabetes—2024. Diabetes Care. 2024;47(Supplement_1):S20–S42. doi:10.2337/dc24-S002
20. Piepoli MF, Hoes AW, Agewall S, et al. European Guidelines on cardiovascular disease prevention in clinical practice. Eur Heart J. 2016;37(29):2315–2381. doi:10.1093/eurheartj/ehw106
21. Low Wang CC, Hess CN, Hiatt WR, et al. Clinical update: cardiovascular disease in diabetes mellitus. Circulation. 2016;133(24):2459–2502. doi:10.1161/CIRCULATIONAHA.116.022194
22. Willeit P, Tschiderer L, Allara E, et al. Carotid intima-media thickness progression as surrogate marker for cardiovascular risk. Circulation. 2020;142(7):621–642. doi:10.1161/CIRCULATIONAHA.120.046361
23. Liu C, Sun X, Lin H, et al. Association between hyperhomocysteinemia and metabolic syndrome with early carotid artery atherosclerosis: a cross-sectional study in middle-aged Chinese population. Nutrition. 2018;53:115–119. doi:10.1016/j.nut.2018.02.014
24. Novo G, Ma M, Wang L, et al. Meta-analysis of the correlation between serum uric acid level and carotid intima-media thickness. PLoS One. 2021;16(2).
25. Mello FM, Bensenor IM, Santos IS, et al. Serum uric acid levels and subclinical atherosclerosis: results from the Brazilian Longitudinal study of adult health (ELSA-Brasil). Curr Prob Cardiol. 2023;48(3):101525. doi:10.1016/j.cpcardiol.2022.101525
26. Li S, Zhang Y, Luo D, et al. Correlation between serum uric acid to high-density lipoprotein cholesterol ratio and cardiometabolic multimorbidity in China: a nationwide longitudinal cohort study. Nutr Metab Cardiovasc Dis;2025. 104210. doi:10.1016/j.numecd.2025.104210
27. Ding L, Guo H, Zhang C, et al. Serum uric acid to high-density lipoprotein cholesterol ratio is a predictor for all-cause and cardiovascular disease mortality in patients with diabetes: evidence from NHANES 2005–2018. Nutr Metab Cardiovasc Dis. 2024;34(11):2480–2488. doi:10.1016/j.numecd.2024.07.001
28. Li Z, Liu Q, Yao Z. The serum uric acid-to-high-density lipoprotein cholesterol ratio is a predictor for all-cause and cardiovascular disease mortality: a cross-sectional study. Front Endocrinol. 2024;15.
29. Li F, Zhao D, Li Q, et al. Uric acid to high-density lipoprotein cholesterol ratio is a novel marker to predict functionally significant coronary artery stenosis. J Int Cardiol. 2022;2022:1–8. doi:10.1155/2022/4797529
30. Deng F, Jia F, Sun Y, et al. Predictive value of the serum uric acid to high-density lipoprotein cholesterol ratio for culprit plaques in patients with acute coronary syndrome. BMC Cardiovascular Dis. 2024;24(1). doi:10.1186/s12872-024-03824-z.
31. Shao C, Fei C, Gu M, et al. Comparative predictive value of the tyg index and UHR for lower extremity artery disease in type 2 diabetes: a retrospective analysis. Diabetes Metabolic Syndrome Obesity. 2025;18:1341–1351. doi:10.2147/DMSO.S496727
32. Chen X, Zhang J, Lu F, et al. Association between uric acid to high-density lipoprotein cholesterol ratio and chronic kidney disease in Chinese patients with type 2 diabetes mellitus: a cross-sectional study. Front Nutrition. 2025;12.
33. Zhu X, Yin H, Han J, et al. association between uric acid to HDL-C ratio and metabolic dysfunction-associated steatotic liver disease in type 2 diabetes mellitus: a cross-sectional study. Diabetes Metabolic Syndrome Obesity. 2025;18:1459–1466. doi:10.2147/DMSO.S520688
34. Urbina EM, Khoury PR, Mccoy CE, et al. Triglyceride to HDL-C ratio and increased arterial stiffness in children, adolescents, and young adults. Pediatrics. 2013;131(4):e1082–e90. doi:10.1542/peds.2012-1726
35. Jiang Z-Z, Zhu J-B, Shen H-L, et al. A high triglyceride-glucose index value is associated with an increased risk of carotid plaque burden in subjects with prediabetes and new-onset type 2 diabetes: a real-world study. Front Cardiovascular Med. 2022;9.
36. Rahimi K, Bidel Z, Nazarzadeh M, et al. Pharmacological blood pressure lowering for primary and secondary prevention of cardiovascular disease across different levels of blood pressure: an individual participant-level data meta-analysis. Lancet. 2021;397(10285):1625–1636. doi:10.1016/S0140-6736(21)00590-0
37. Kosmas CE, Bousvarou MD, Kostara CE, et al. Insulin resistance and cardiovascular disease. J Int Med Res. 2023;51(3). doi:10.1177/03000605231164548.
38. Mach F, Baigent C, Catapano AL, et al. ESC/EAS guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk. Atherosclerosis. 2019;290:140–205.
39. Yin J, Zheng C, Lin X, et al. The potential of the serum uric acid to high-density lipoprotein cholesterol ratio as a predictive biomarker of diabetes risk: a study based on NHANES 2005–2018. Front Endocrinol. 2025;15.
40. Chaudhary K, Malhotra K, Sowers J, et al. Uric acid - key ingredient in the recipe for cardiorenal metabolic syndrome. Cardiorenal Medicine. 2013;3(3):208–220. doi:10.1159/000355405
41. Zhou X, Xu J. Association between serum uric acid‐to‐high‐density lipoprotein cholesterol ratio and insulin resistance in an American population: a population‐based analysis. J Diabetes Invest. 2024;15(6):762–771. doi:10.1111/jdi.14170
42. Johnson RJ, Lanaspa MA, Gaucher EA. Uric acid: a danger signal from the RNA world that may have a role in the epidemic of obesity, metabolic syndrome, and cardiorenal disease: evolutionary considerations. Semin Nephrol. 2011;31(5):394–399. doi:10.1016/j.semnephrol.2011.08.002
43. Tall AR, Rader D J. Trials and Tribulations of CETP Inhibitors. Circulation Research. 2018;122(1):106–112. doi:10.1161/CIRCRESAHA.117.311978
44. Li H, Qian F, Liu H, et al. Elevated uric acid levels promote Vascular Smooth Muscle Cells (VSMC) proliferation via an nod-like receptor protein 3 (NLRP3)-inflammasome-dependent mechanism. Med Sci Monit. 2019;25:8457–8464. doi:10.12659/MSM.916667
45. Dai Y, Cao Y, Zhang Z, et al. Xanthine oxidase induces foam cell formation through LOX-1 and NLRP3 activation. Cardiovasc Drugs Ther. 2017;31(1):19–27. doi:10.1007/s10557-016-6706-x
46. Soppert J, Lehrke M, Marx N, et al. Lipoproteins and lipids in cardiovascular disease: from mechanistic insights to therapeutic targeting. Adv Drug Delivery Rev. 2020;159:4–33. doi:10.1016/j.addr.2020.07.019
47. Dogru S, Yasar E, Yesilkaya A. Effects of uric acid on oxidative stress in vascular smooth muscle cells. Biomed Rep. 2024;21(6). doi:10.3892/br.2024.1859
48. Moriarty PM, Gibson CA. Association between hematological parameters and high-density lipoprotein cholesterol. Curr Opinion Cardiol. 2005;20(4):318–323. doi:10.1097/01.hco.0000167722.22453.47
49. Chao H-H, Liu J-C, Lin J-W, et al. Uric acid stimulates endothelin-1 gene expression associated with NADPH oxidase in human aortic smooth muscle cells. Acta Pharmacol Sin. 2008;29(11):1301–1312. doi:10.1111/j.1745-7254.2008.00877.x
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Association Between Triglyceride-Glucose Index and Serum Uric Acid Levels: A Biochemical Study on Anthropometry in Non-Obese Type 2 Diabetes Mellitus Patients
Luo Y, Hao J, He X, Wang C, Zhao H, Zhang Z, Yang L, Ren L
Diabetes, Metabolic Syndrome and Obesity 2022, 15:3447-3458
Published Date: 3 November 2022
Association of Uric Acid to Creatinine Ratio with Metabolic Dysfunction-Associated Fatty Liver in Non-Obese Individuals Without Type 2 Diabetes Mellitus

Liu J, Wang C, Wang Y, Yao S
Diabetes, Metabolic Syndrome and Obesity 2024, 17:131-142
Published Date: 8 January 2024
White Blood Cell Count Is Associated with Hyperuricemia in Patients with Type 2 Diabetes Mellitus
Peng YF, Yin H, Hu L, Fang L, Jia DR, Li L
Journal of Inflammation Research 2025, 18:3993-3999
Published Date: 17 March 2025
Development and Validation of a Nomogram for Predicting Carotid Atherosclerosis in Non-Obese Patients with Type 2 Diabetes
Cui Y, Li L, Li Y, Yu P
Diabetes, Metabolic Syndrome and Obesity 2025, 18:4547-4557
Published Date: 16 December 2025