Back to Journals » Drug Design, Development and Therapy » Volume 19
A Comparative Study of Sugammadex and Neostigmine: A Bibliometric Analysis of the Past 15 Years
Authors Yin D, Tang B, Hu X, Hu H ![]()
Received 10 February 2025
Accepted for publication 16 July 2025
Published 29 July 2025 Volume 2025:19 Pages 6357—6377
DOI https://doi.org/10.2147/DDDT.S519235
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Qiongyu Guo
Dawei Yin,1,* Bin Tang,1,* Xiaoyan Hu,2,* Huan Hu1,*
1Department of Anesthesiology, Huangshi Maternity and Children’s Health Hospital, Affiliated Maternity and Children’s Health Hospital of Hubei Polytechnic University, Huangshi Key Laboratory of Birth Defects Prevention, Huangshi, Hubei, People’s Republic of China; 2Department of Radiation and Medical Oncology, Zhongnan Hospital of Wuhan University, Wuhan, Hubei, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Huan Hu, Department of Anesthesiology, Huangshi Maternity and Children’s Health Hospital, 9 Guilin South Road, Huangshi, Hubei, 435000, People’s Republic of China, Email [email protected] Xiaoyan Hu, Department of Radiation and Medical Oncology, Zhongnan Hospital of Wuhan University, 169 Donghu Road, Wuhan, Hubei, 430071, People’s Republic of China, Email [email protected]
Purpose: Sugammadex is a novel selective relaxant binding agent for aminosteroid neuromuscular blocking agents (NMBAs). However, existing literature reveals major knowledge gaps regarding its current applications and emerging research trends. Therefore, this study employed bibliometric analysis to map the evolutionary trajectory and research frontiers in sugammadex studies over the past 15 years.
Methods: Publications on sugammadex (2009– 2024) along with neostigmine studies (1993– 2008) were retrieved from the Web of Science Core Collection. Data aggregation was performed using Microsoft Excel, while bibliometric visualizations were generated through the Bibliometrix package in R software. Additional network analyses were conducted using VOSviewer and CiteSpace.
Results: The analysis encompassed 765 articles. Sugammadex-related research exhibited a notable upward trend, particularly from 2017 to 2021. The United States of America (USA) emerged as the most productive country in publication output (186 articles) and demonstrated superior quality (h-index: 16). Among institutions, Merck & Co. contributed the highest number of publications (74). Similar to neostigmine, key research areas for sugammadex have included: pharmacokinetics and pharmacodynamics, adverse reactions, clinical applications, and specific patient populations. This focus is evidenced by substantial common references and keywords.
Conclusion: Sugammadex surpasses neostigmine in rapidly, effectively, and safely reversing NMB induced by rocuronium/vecuronium across all depths. Its use expands to reversing residual NMB from NMBAs in various patient groups (hepatic/renal impairment, obese, neuromuscular disease, elderly, pediatric) and scenarios like difficult airways. Future research will focus on adverse reactions, effects in special populations, establishing quantitative NMB monitoring standards, and understanding NMBA antagonism failure mechanisms.
Keywords: Sugammadex, org25969, bibliometric analysis, neuromuscular blockade, specific populations, research trends
Introduction
In surgeries under general anesthesia, neuromuscular blocking agents (NMBAs) optimize tracheal intubation and surgical exposure. However, undetected residual neuromuscular blockade (NMB) carries perioperative mortality risks.1 Preventing residual NMB requires: precise NMBA dosing, intraoperative monitoring, and postoperative antagonism.2 Neostigmine (a cholinesterase inhibitor) and sugammadex are common antagonists. Table 1 compares their profiles.1–3 Neostigmine, a common neuromuscular blockade antagonist and cholinesterase inhibitor, has been widely used in clinical settings since the 1950s to reverse postoperative residual neuromuscular blockade.4 Nonetheless, the incidence of residual neuromuscular blockade remains significantly elevated.5 In July 2008, the European Medicines Agency (EMA) approved sugammadex. Sugammadex, a novel altered γ-cyclodextrin, is utilized to antagonize the steroid non-depolarizing neuromuscular blockers, specifically rocuronium and vecuronium. Unlike conventional antagonists such as neostigmine, sugammadex reduces the concentration of non-depolarizing neuromuscular blockade in the bloodstream by encapsulating them and forming complexes, thereby reversing NMB induced by rocuronium or vecuronium. In comparison to neostigmine, sugammadex presents several significant clinical advantages, including swift and reliable reversal of NMB at any depth, improved patient safety and decreased occurrence of residual NMB during recovery and more efficient utilization of healthcare resources.6 Bibliometrics involves the application of mathematical and statistical techniques to analyze publications across various fields, enabling the evaluation of contributions and collaborations among various countries/regions, institutions, journals, and authors. This approach encompasses clustering and burst detection of keywords and references, which aid in identifying research focal points, assessing academic productivity, and determining trends in clinical research.7,8 While sugammadex is broadly acknowledged as an innovative neuromuscular blocking agent, there is a scarcity of information in the literature concerning present and future trends. Since the approval of sugammadex in 2008, we identified and analyzed studies conducted over the subsequent 15 years (from 2009 onward) and compared these findings with those from neostigmine-related studies published between 1993 and 2008. Therefore, the aim of this study was to explore future research trends and significant issues related to sugammadex by performing a bibliometric analysis and comparing it with the keyword co-occurrence analysis of neostigmine.
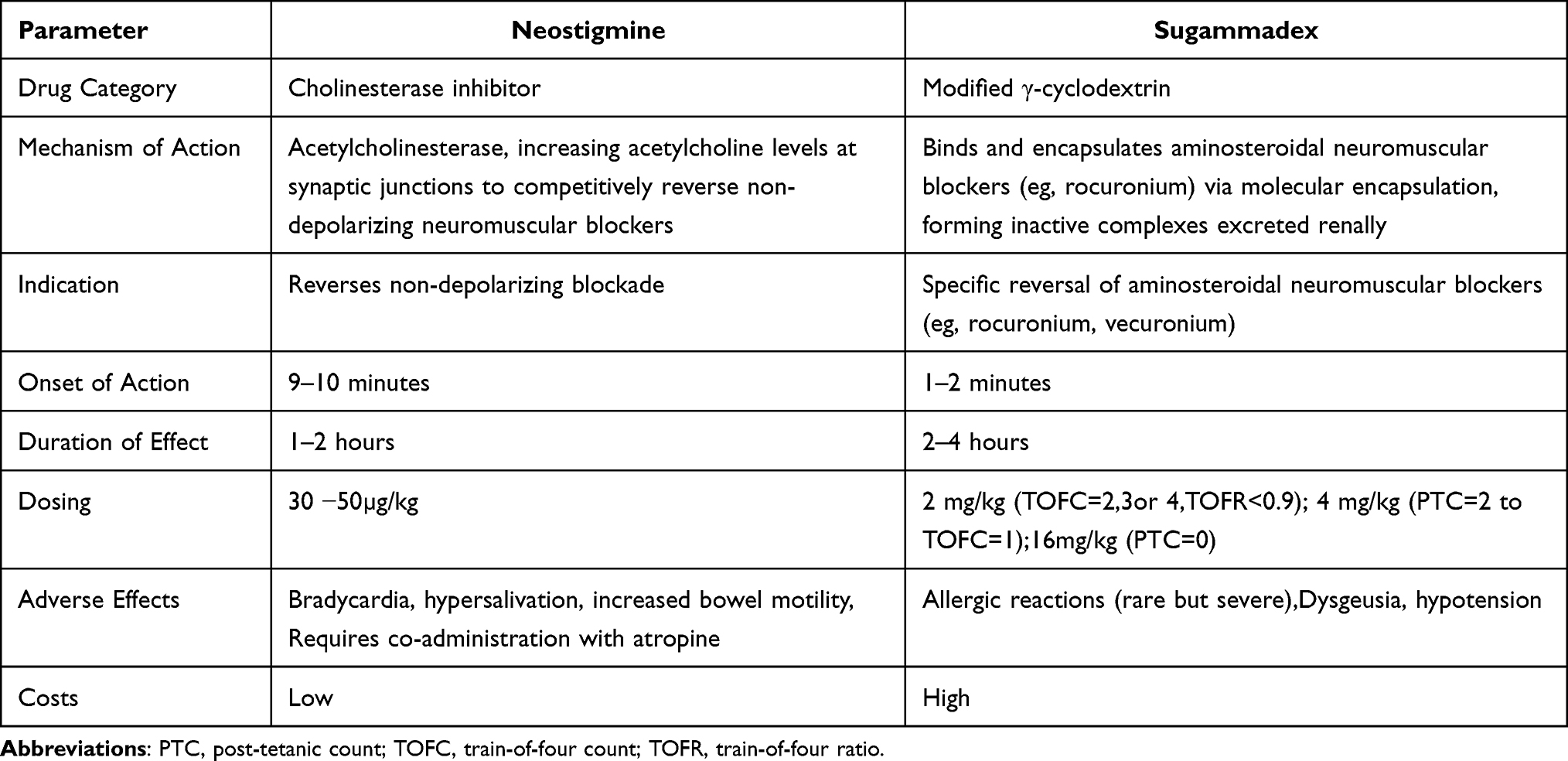 |
Table 1 A Comparative Analysis of Neostigmine and Sugammadex |
Methods
Data Sources and Search Strategies
This research utilized the Web of Science Core Collection (WoSCC) as its main database. WoSCC is widely acknowledged as a leading literary resource and is considered the most appropriate choice for performing bibliometric analyses.9,10
The employed search strategy encompassed the following terms: (TS=sugammadex) OR (TS=org25969), spanning publications from 2009 to 2024.
Inclusion and Exclusion Criteria
The criteria for inclusion were established as follows: (1) Original research articles, (2) Publications in English language, (3) Research articles published between January 1, 2009 and November 11, 2024.
Exclusion criteria included: (1) Studies unrelated to sugammadex; (2) articles where sugammadex was not the primary focus; (3) abstracts, editorials, conference proceedings, meeting summaries, letters, book chapters, retracted publications, or notices of concern; (4) articles lacking an abstract or a digital object identifier (DOI); (5) articles that are not available in their entirety. All literature compilation and data gathering were finalized by November 11, 2024.
Statistical Analysis and Visualization
Data pertaining to sugammadex were transformed into txt format and exported for bibliometric analysis using CiteSpace (6.3.R3), R 4.3.3 “bibliometrix” (https://www.bibliometrix.org), and VOSviewer. CiteSpace, a visualization tool created by Professor Chaomei Chen and built on Java, proficiently highlights significant scientific institutions, key authors, and essential keywords, while also mapping out research trends and trajectories.11,12 In the visual maps produced by CiteSpace, each node represents a country, institution, author, journal, or keyword. Node dimensions represent the frequency of occurrence or citation, while color indicates the year. In the visualization map, the outermost purple ring represents the centrality of each node, where a thicker ring signifies a greater degree of centrality. Nodes exhibiting high centrality (> 0.1) generally regarded as pivotal or critical points in a field.13 The evaluation of the network’s overall structural properties through cluster analysis employed both modularity (Q value) and mean silhouette scores (S value). A cluster quality was considered acceptable when the conditions Q > 0.3 and S > 0.5 were met. The “Bibliometrix package”, a tool designed for bibliometric analysis in R, provides a range of functions and visualization tools that facilitate the monitoring of research themes across different time periods and the evaluation of journals.13 The tools VOSviewer (version 1.6.20) and an online bibliometric platform (accessible at https://bibliometric.com) were employed to produce a visual network analysis illustrating the collaborative interactions among various countries, as well as to create a density visualization map of the keywords.
Results
From January 1, 2009 to November 11, 2024, 1,518 publications on sugammadex were identified. Upon the removal of conference abstracts, editorials, publications in languages other than English, as well as other categories of documents deemed irrelevant, 765 articles remained for further evaluation. These articles were then carefully reviewed by two research teams, who examined the titles and abstracts to eliminate any studies irrelevant to sugammadex. Ultimately,765 articles satisfied the eligibility criteria and were incorporated into in the final analysis (Figure 1).
 |
Figure 1 PRISMA flowchart of the study. |
Annual Publications and Annual Citations
This bibliometric analysis encompasses a total of 765 publications that have garnered a cumulative total of 13,492 citations, resulting in an average of 16.45 citations per individual publication, and the analysis indicates an h-index of 55 as of the year 2024. As illustrated in Figure 2, during the first two years, no research results were published. Subsequently, the number of publications gradually grew each year, but it was not until 2019 that the annual publication counts surpassed 50. In parallel, annual citations steadily increased from 2011 to 2024, peaking in 2023 with a total of 1,795 citations.
 |
Figure 2 Trend Analysis of Sugammadex-related Publications and Citations: 2009–2024. |
Publications by Countries/Regions
The number of sugammadex-related publications by countries/regions from 2009 to 2024 is illustrated in Figure 3A. Over this period, the United States of America (USA) generated the largest quantity of publications (n=186, 24.31%), followed by South Korea (n=98,12.81%) and China (n=84,10.98%). The USA has maintained a significant lead since 2020, while the number of China annual publications overtook that of South Korea by 2021. Figure 3B illustrates the 10 leading countries/regions with the highest total number of publications (Np), total citations (Tc), and total link strength (TLS), with the USA leading in both academic output and scholarly contributions to sugammadex research. Figure 3C distinguishes between Single Country Publications (SCP), characterized by authors hailing from a single nation, and Multiple Country Publications (MCP), which involve contributions from authors across various countries. Notably, the Netherlands and France have the largest number of international co-authors in sugammadex research, while the USA has shown a stronger tendency toward internal collaborations.
 |
Figure 3 Visualization Map of Countries/Regions. (A) Sugammadex-related articles published from 2009 to 2024 by countries/regions. (B) The top 10 countries with the most Sugammadex-related articles published from 2009 to 2024. (C)The top 10 countries with the most corresponding authors. |
Publications by Institutions
To evaluate the academic impact of institutions, we identified the top 10 based on publication counts. The leading institutions ranked by the quantity of their publications were Merck & Co. (USA, n = 49), Seoul National University (South Korea, n = 27), Harvard University (USA, n = 23) and Massachusetts General Hospital (USA, n = 15) (Figure 4A). Merck & Co. achieved the highest centrality score of 0.39 among international institutions, underscoring its prominent role in global sugammadex research, as shown in Figure 4B and C. Meanwhile, Merck & Co. has been instrumental in pioneering research and fostering collaborations that have significantly boosted overall research productivity. Researchers from institutions in the USA and South Korea have also made substantial contributions, particularly in advancing key areas of sugammadex research.
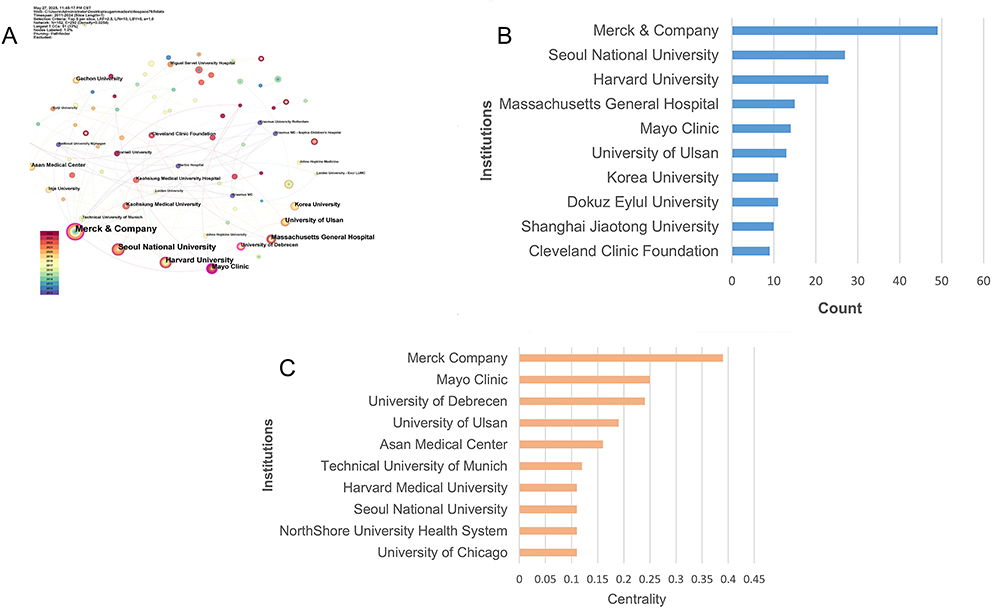 |
Figure 4 Cooperation Between Institutions on Sugammadex. (A) Cooperation networks between different institutions; (B) The top 10 institutions in count; (C) The top 10 institutions in centrality. |
Analysis of Authors and Cited Authors
The analysis of 765 screened publications revealed that 200 authors contributed to sugammadex-related research. Table 2 presents the top 10 cited authors according to their total citations and publications, while Figure 5A shows annual variations in their research output. In this figure, authors’ names are plotted on the vertical axis and publication years are shown on the horizontal axis. The dimensions of the circles denote the volume of publications, with larger circles indicating higher output, while the color intensity reflects the average annual citation count, with darker colors signifying greater citations. Manfred Blobner from University of Ulm leads both in publication counts (12 articles) and citation counts (178 citations), as shown in Figure 5B. Professor Suzuki Takahiro has contributed to sugammadex research since 2011, continuing through 2022.
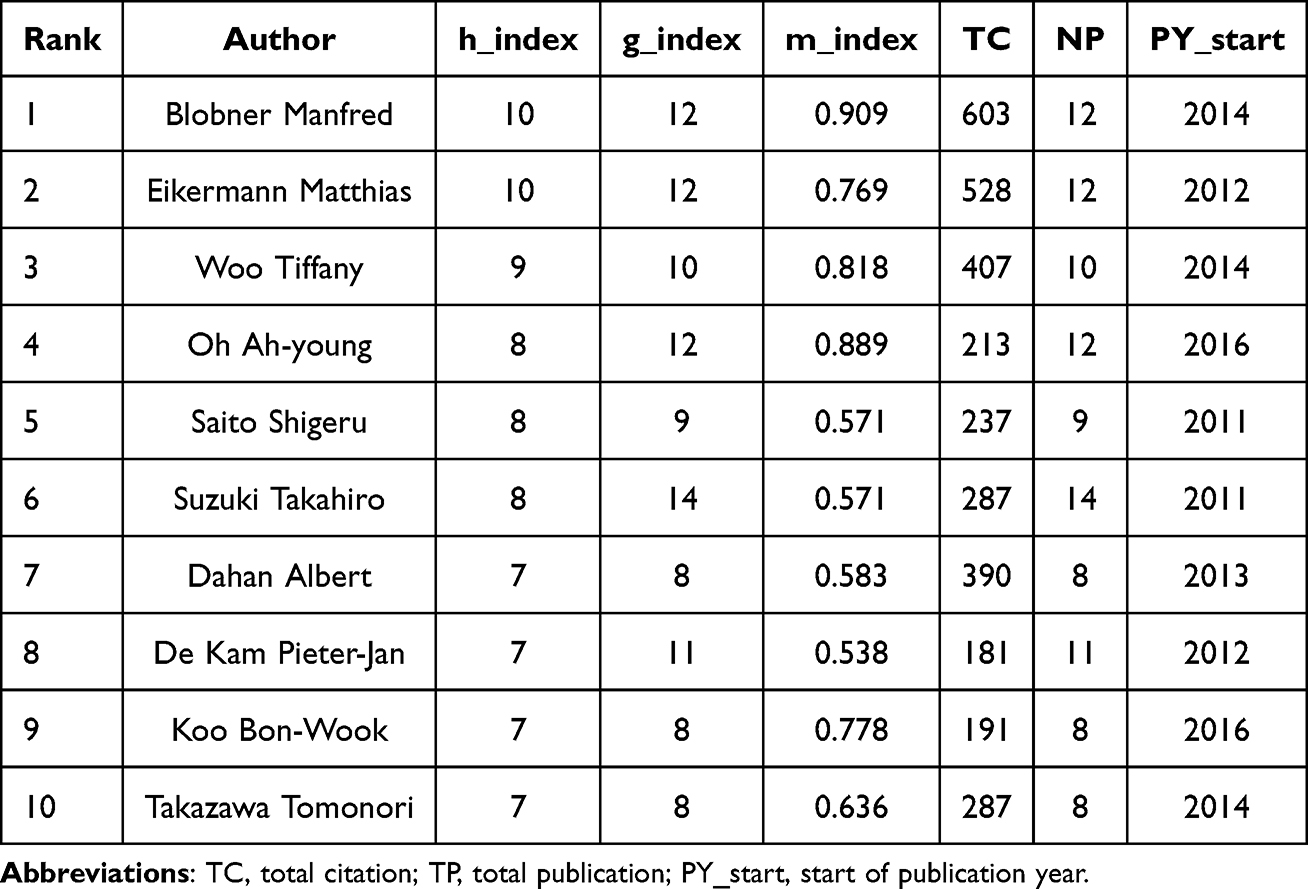 |
Table 2 The Top 10 Most-Cited Authors in Sugammadex |
 |
Figure 5 Authors Analysis on Sugammadex. (A) Authors’ productions over time; (B) Most local cited authors. |
Analysis of Journals
The authority and influence of journals are mainly measured by its citation count. Table 3 presents the 10 most active journals, ranked according to various metrics, including Journal Citation Reports (JCR) quartile, impact factor (IF), h-index, g-index, m-index, total number of citations (Tc), total number of publications (Np), and the year of publication start (PY_start). The British Journal of Anaesthesia, with 43 publications, ranks first, receiving a total of 1,998 citations. The journals with the highest impact factors were the British Journal of Anaesthesia (9.1) and Anesthesiology (9.1), followed by Anaesthesia (7.5) and Anesthesia and Analgesia (4.6). According to Bradford’s law, nine core source journals are categorized in Zone 1 (Figure 6A). Regarding centrality, Acta Anaesthesiologica Scandinavica achieved the highest score (0.18) among all journals (Figure 6B). These journals are widely regarded within the anesthesia field, known for their significant impact and esteemed reputation.
 |
Table 3 The Top 10 Journals with the Most Sugammadex-Related Articles |
 |
Figure 6 Journals Analysis on Sugammadex. (A) Core Journals by Bradford’s law. (B) The top 10 cited journals in centrality. |
Analysis of References
- Analyzing cited references is a key method for identifying emerging trends and uncovering research opportunities in any academic field. The co-citation graph of references (Figure 7A) includes 106 nodes and 177 edges. The nodes are color-coded by publication date, while the dimensions of each node correspond to frequency with which a reference is cited. A purple circle surrounding a node indicates its centrality, highlighting its importance within the network of references. The most cited reference is “Post-Anesthesia Pulmonary Complications After Use of Muscle Relaxants (POPULAR): A Multicenter, Prospective Observational Study” by Eva Kirmeier, which has a centrality score of 0.30 and 238 citations. The reference with the highest centrality, “Retrospective Investigation of Postoperative Outcome After Reversal of Residual NMBAs (Neuromuscular Blockades): Sugammadex, Neostigmine, or No Reversa” by Thomas Ledowski (centrality = 0.60), is recognized as a critical node in the co-citation network, marking it as a pivotal work in the field.
 |
Figure 7 Cited References Analysis on Sugammadex. (A)The network map of cited references; (B) The clustering of cited references; (C) The top 20 cited references with the strongest citation bursts. |
Cluster analysis of cited references identified eleven key research clusters (Q value = 0.6548, S value = 0.8634), which are as follows: #0 postoperative pulmonary complications, #1 rocuronium-induced neuromuscular blockade, #2 surgical condition, #3 a critical appraisal, #4 real problem, #5 neuromuscular blockade and #6 current practice (Figure 7B). These clusters represent the primary areas of focus within sugammadex research.
References exhibiting high “burst intensity” have a greater impact on shaping future research directions. Burst intensity is a measure of how frequently a reference is cited in a short time, reflecting its sudden influence. The two references with the highest burst strength were “Sugammadex versus Neostigmine for Reversal of Neuromuscular Blockade and Postoperative Pulmonary Complications (STRONGER): A Multicenter Matched Cohort” (burst strength=28.35) and “Efficacy and safety of sugammadex versus neostigmine in reversing neuromuscular blockade in adults” (burst strength = 19.79) (Figure 7C).
Keywords Analysis
Table 4 presents the top 20 keywords pertaining to sugammadex research, ranked by total link strength (TLS), a measure of their impact. Among these, sugammadex appears most frequently, with 360 occurrences, followed by NMBAs (143), rocuronium (136), and neostigmine (90).
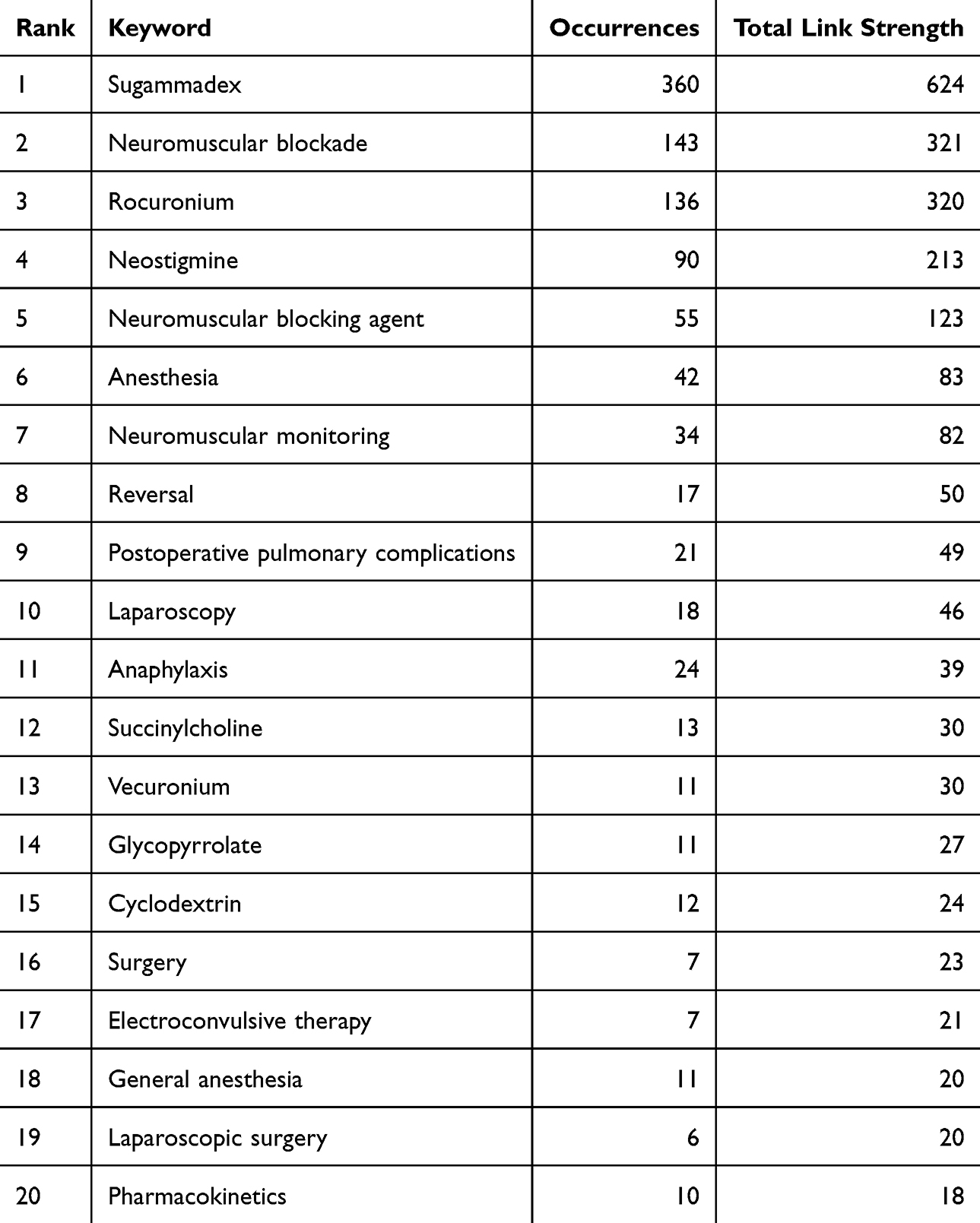 |
Table 4 The Top 20 Keywords Related to Sugammadex |
Keywords serve as the central themes of research articles. To identify the current research hotspots, we conducted a co-occurrence analysis of keywords that appeared more than eight times using VOSviewer. This analysis produced a keyword co-occurrence network (Figure 8A), which were classified into 9 clusters. The main cluster are cluster 1 (red, n = 28) primarily focuses on comparisons between sugammadex and neostigmine in reversing NMBAs after general anesthesia. Cluster 2 (green, n = 20) examines postoperative pulmonary complications caused by residual NMB. Cluster 3 (blue, n = 18) focuses on reversing the residual NMBAs following general anesthesia. Cluster 4 (yellow, n = 12) focuses on using NMBAs during thyroid surgery under general anesthesia. Cluster 5 (purple, n = 11) focuses on the anaphylaxis or hypersensitive reactions while applying sugammadex or NMBAs. Cluster 6 (light blue, n = 6) focuses on study on the pharmacokinetics of cyclodextrins. In Figure 8B, the keywords are color-coded based on their average occurrence time. Specifically, words highlighted in blue denote an earlier appearance, whereas those represented in yellow signify a more recent occurrence. The average publication year (APY) indicated that the most recent keywords were postoperative pulmonary complications (Cluster 2, APY: 2021.7), postoperative nausea and vomiting (Cluster 9, APY: 2021.12), and “glycopyrrolate” (Cluster 1, APY: 2022.6). These topics are closely associated with the investigation of sugammadex effects on residual neuromuscular blockades and its clinical applications in special populations. Figure 8C displays the frequency of keywords within each cluster, with red indicating high frequency and blue indicating lower frequency.
 |
Figure 8 Keywords Analysis on Sugammadex. (A) The network visualization of keywords analysis; (B) The overlay visualization of keywords analysis; (C) The density visualization of keywords analysis. (D) The top 20 keywords with the strongest citation bursts. |
Utilizing the citation burst detection feature in CiteSpace, we uncovered emerging trends through keyword analysis. Over the past 15 years, the relaxant binding agent exhibited the strongest citation burst (burst strength = 7.61), reflecting a sustained and intensified research focus in this domain. Keywords such as pulmonary complications, residual neuromuscular blockade, and postoperative pulmonary complications have recently garnered significant attention, establishing themselves as key areas of research (Figure 8D).
Finally, Tables 4 and 5 present the top 20 keywords for sugammadex and neostigmine research, respectively. Sugammadex remains the most frequent keyword in both groups, as it is a key antagonist of neuromuscular blockers.
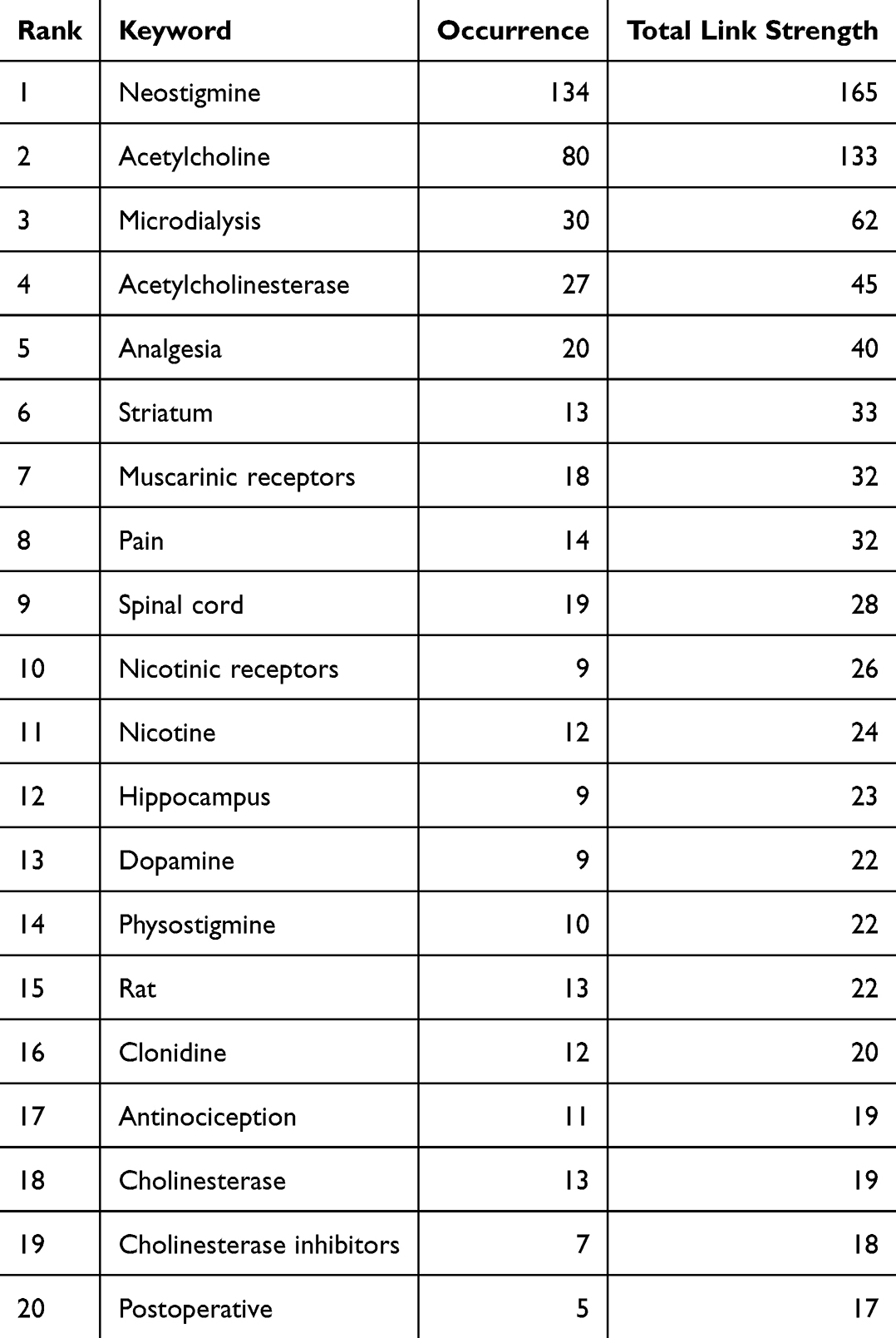 |
Table 5 The Top 20 Keywords Related to Neostigmine |
In neostigmine-related research, the most frequent keywords include neostigmine (134 occurrences), acetylcholine (80), microdialysis (30), and acetylcholinesterase (27).
Funding Analysis
A total of 765 publications (97.4% of all analyzed studies) received funding from 200 distinct agencies. As shown in Table 6, Merck & Co. (USA) was the leading funder, supporting 48 publications. Geographically, seven of the top 10 funding agencies were based in the United States, three in China and Japan collectively, and one in the Netherlands. The concentration of research funding in the United States mirrors its leading role in sugammadex studies, a position bolstered by substantial investments in biopharmaceutical innovation.
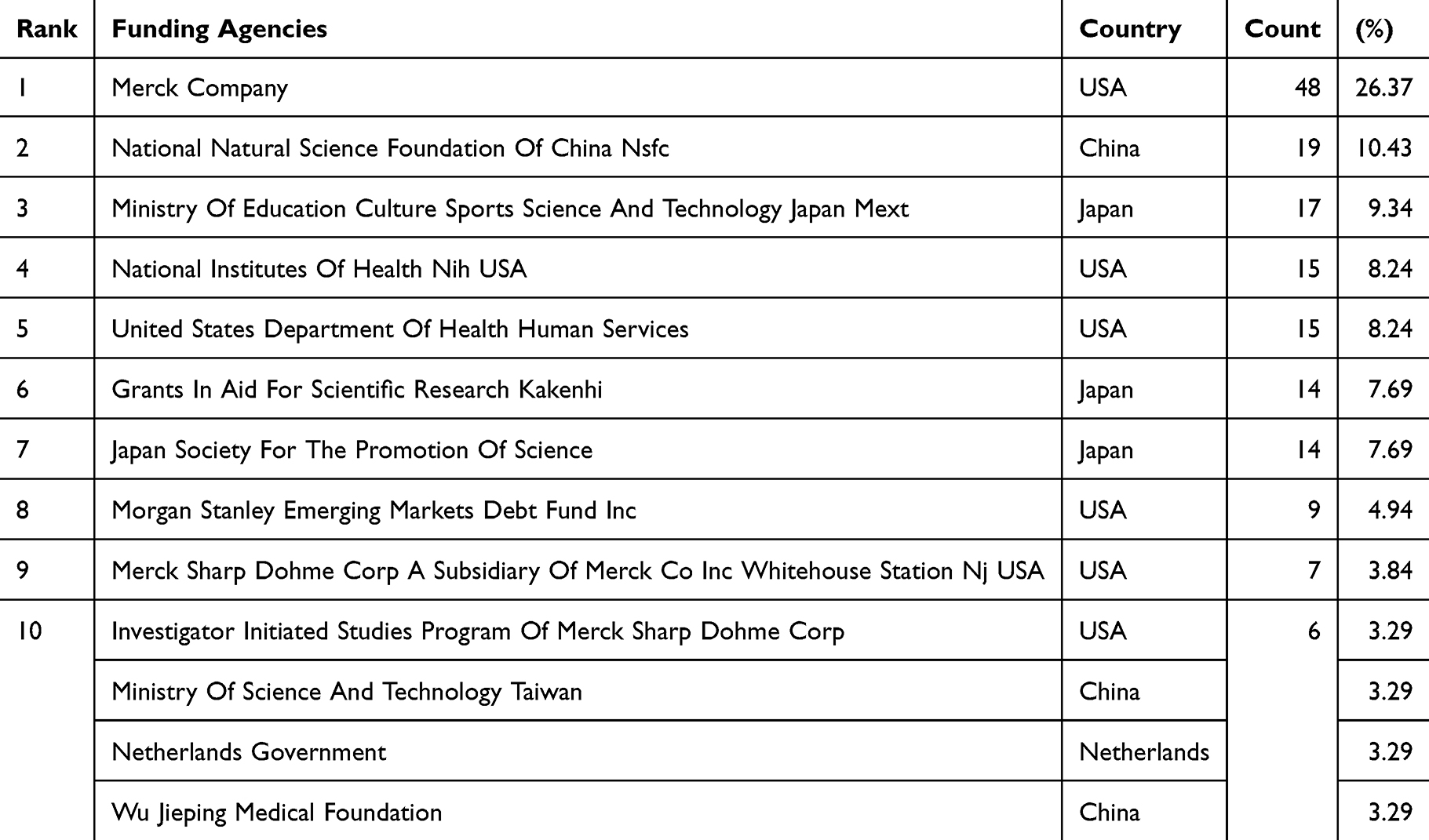 |
Table 6 The Top 10 Funding Agencies for Sugammadex Researches |
Discussion
This bibliometric analysis systematically assessed 765 articles on sugammadex published over the past 15 years. Using CiteSpace and VOSviewer, we mapped and analyzed prevailing research trends, examined their evolution, and identified potential avenues for future exploration in sugammadex research.
Basic Information Analysis
Based on the CiteSpace bibliometric analysis, the number of publications on sugammadex has consistently risen over the last 15 years, with a notable surge around 2019, which followed the approval of sugammadex in China in 2017. In terms of global contributions, the USA and its institutions maintain a dominant position, reflected in their high centrality, which underscores their pivotal role in sugammadex research and international collaboration. This preeminence is probably due to the USA’s advanced research infrastructure, significant investment in scientific innovation, and a setting that fosters groundbreaking discoveries. Manfred Blobner from Ulm University is the most prolific and most referenced author in this domain. His extensive body of work has significantly shaped our understanding of sugammadex, particularly through studies addressing its optimal dosage for reversing the neuromuscular blockade effects of rocuronium and vecuronium, comparisons with neostigmine, postoperative pulmonary complications, and its application in specific populations, as well as in perioperative neuromuscular monitoring.14–18 The British Journal of Anaesthesia was the most cited journal in the field, followed by Anaesthesia and Anesthesia & Analgesia. These journals are highly influential within anesthesiology. Additionally, the most cited reference was “post-anesthesia pulmonary complications after use of muscle relaxants (POPULAR): a multicenter, prospective observational study”, authored by Eva Kirmeier. This study provided critical insights into the recommended dosing of sugammadex for reversing moderate and deep muscle relaxation caused by rocuronium and vecuronium.
Comparative Analyses of Sugammadex and Neostigmine Based on Keywords
Neostigmine, commonly used to reverse NMBAs, is linked to various adverse effects. When administered with anticholinergic drugs, adverse effects including tachycardia, postoperative urinary retention, blurred vision, and sedation. While sugammadex does not require the use of anticholinergics, it is also linked to several potential complications, including postoperative residual NMB, allergic reactions, coagulopathy, cardiovascular effects, bronchospasm, laryngospasm, nausea, vomiting, prolonged renal excretion, mitochondrial neural cell apoptosis, and a metallic taste. In clinical practice, neostigmine is typically administered when a Train of Four (TOF) T2 response is observed upon completion of the surgery. The recovery time from NMBAs with neostigmine varies depending on the dosage and combination of anticholinergic agents. The recovery time from muscle relaxation following an injection of neostigmine at 0.02 mg/kg and atropine at 0.01 mg/kg, or neostigmine at 40 μg/kg and atropine at 0.02 mg/kg, or neostigmine at 70 μg/kg and glycopyrrolate at 14 mg/kg, ranges from 35.7 to 65.6 minutes. In comparison, sugammadex offers a faster and more reliable reversal of NMBAs. For moderate block (with at least one twitch after TOF), a dose of 2 mg/kg of sugammadex is recommended, achieving a TOF ratio of 0.9 within approximately 2 minutes. For deep block (no twitch after TOF but at least one twitch after tetanic stimulation), the recommended dose is 4 mg/kg, which restores a TOF ratio of 0.9 within 1.6 to 3.3 minutes. In emergency situations requiring immediate return to spontaneous ventilation, a higher dose of 16 mg/kg is recommended. Although sugammadex offers a quicker and more efficient reversal of NMB, particularly in complex airway management scenarios, it is important to note that further clinical evidence is needed to fully confirm its efficacy. There have been instances where sugammadex has failed to reverse NMB effectively, underscoring the need for more extensive studies to establish its reliability and broaden its clinical applications.
Advantages of Sugammadex for Specific Populations
The Elderly
In older adults aged 65 years and above, the administration of sugammadex to reverse NMBAs induced by rocuronium typically results in a delayed recovery to a Train of Four (TOF) ratio of 0.9, with the process taking approximately 1–2 minutes longer compared to younger populations.19 In a study by Dr. McDonagh and his team, patients were categorized into three age groups: adults (18–64 years), younger elderly (65–74 years), and older elderly (75 years and above). While sugammadex (2 mg/kg) effectively reversed the blockade in all age groups, elderly patients required more time to recover to TOF 0.9. Importantly, this delay did not notably impact the effectiveness of sugammadex or result in an increased incidence of adverse effects.20 Dosing considerations for elderly patients are further supported by the findings of Shin et al, who observed that the effective dose of sugammadex to rapidly reverse deep NMB (within 2 minutes) was slightly higher in elderly individuals compared to younger patients (5.4 mg/kg versus 4.4 mg/kg, respectively). This suggests that increasing the dose of sugammadex in elderly patients may be necessary for achieving a faster reversal of the blockade.21 Further investigation by Muramatsu et al indicated that elderly patients, particularly those with renal impairment, are more susceptible to residual NMB when administered lower doses of sugammadex. Therefore, it is critical to adjust the dose based on neuromuscular monitoring, ensuring that elderly patients receive an adequate dose to fully reverse the blockade.22 A study by Williams III et al also highlighted that a 4 mg/kg dose of sugammadex for deep NMB may not fully eliminate the risk of residual blockade, further emphasizing the need for individualized dosing. In summary, while sugammadex is generally effective for elderly patients, careful consideration of patient age, renal function, and the degree of NMB is essential. Adjusting the dose based on clinical monitoring can aid in reducing the risk of residual blockade and ensure a more complete reversal of NMB in this population.23
In Child
Residual NMB after extubation in pediatric anesthesia are a significant concern, with studies showing a prevalence of up to 48.2%.24 This underscores the necessity for vigilant monitoring and the appropriate use of NMBAs antagonists following general anesthesia in children. Currently, sugammadex is approved by the European Medicines Agency for use in children aged 2 to 17 years, with the Cochrane Collaboration recommending a dose range of 2–4 mg/kg for reversing moderate NMB induced by rocuronium in pediatric patients aged 2 to 18. However, the US Food and Drug Administration (FDA) has yet to grant approval for its use in children.25 In a retrospective study involving over 200 pediatric patients, sugammadex (2–4 mg/kg) was found to be more rapid and effective than neostigmine in reversing moderate NMB caused by rocuronium.26 Additionally, sugammadex is favored in pediatric populations due to its lower incidence of postoperative nausea and vomiting, which are common side effects of other NMBAs antagonists. Despite these benefits, the administration of sugammadex in children younger than 2 years old has been largely confined to case reports, particularly involving neonates and infants. In these cases, the typical dosages for reversing moderate to deep muscle relaxation range from 2 to 4 mg/kg, while higher doses of 16 mg/kg are recommended in emergency situations, such as “can’t intubate, can’t ventilate” (CICV) scenarios.27,28 However, some studies have reported instances of recurrent NMBAs following sugammadex administration in children. Jean-Philippe’s research suggests that these issues may be linked to factors such as excessive use of rocuronium, inadequate neuromuscular monitoring, or incorrect dosing of sugammadex.29 Given these considerations, further clinical investigation is essential. Multicenter, large-scale trials involving children, particularly those under 2 years old, are essential to verify the safety and effectiveness of sugammadex in this patient group. At present, the lack of comprehensive pediatric studies limits the widespread endorsement of sugammadex for children, necessitating further research before it can be universally recommended.
In Obesity
Obese patients tend to have an increased apparent volume of distribution, higher cardiac output, greater blood volume, and altered local blood flow, all of which can affect the peak plasma concentration, clearance rate, and elimination half-life of various anesthetics.30–32 Additionally, obesity is associated with reduced lung function and diminished functional residual capacity, increasing the risk of pulmonary complications postoperatively.33 As a result, the residual effects of anesthetic agents, particularly muscle relaxants, can significantly heighten the risk of perioperative complications such as upper airway obstruction, aspiration, and pneumonia.34 Numerous studies have highlighted the potential benefits of sugammadex in improving both safety and recovery in obese surgical patients. Sugammadex has demonstrated a faster reversal of NMBAs compared to neostigmine, leading to shorter extubation times,35 reduced postoperative hospital stays, and overall faster recovery. Furthermore, when combined with other rapid recovery strategies—such as preoperative nutritional support, intraoperative warming, and early postoperative feeding and mobilization—its use can further expedite recovery, enhance early postoperative physical and mental well-being, and reduce the incidence of complications, thereby improving overall surgical outcomes.36 One critical area of investigation in sugammadex use in obese patients revolves around the optimal dosing strategy, particularly whether the dose should be based on total body weight (TBW) or ideal body weight (IBW). Early clinical trials during the development of sugammadex suggested that dosing based on TBW provides a constant molar ratio between the drug and neuromuscular blocking agents, thereby effectively minimizing residual blockades.37,38 Inadequate dosing, on the other hand, may lead to extended recovery durations and a heightened risk of residual NMB or recurarization.39,40 A study by Van Lancker et al compared the extubation times of sugammadex dosed according to TBW, IBW, IBW+20%, and IBW+40% in patients with morbid obesity. Their findings indicated that a dose of 2 mg/kg based on IBW+40% was optimal for ensuring safe and effective recovery from NMB.41 In contrast, Llauradó et al reported that IBW-based dosing was insufficient to reverse deep or moderate NMB in patients with morbid obesity.42 Badaoui et al further suggested that the required dose for reversing deep NMB in obese patients should be between 130–150% of the weight-based dose (4 mg/kg of IBW).43 Sanfilippo et al, for instance, concluded that IBW-based sugammadex dosing alone is both safe and effective for the rapid reversal of NMBAs.44 More recent studies have corroborated this, showing that 1.5 mg/kg of IBW-based sugammadex can successfully reverse moderate NMB in obese patients.45 Duarte et al also reported that IBW-based dosing is effective for reversing moderate NMB in patients with morbid obesity.46 A meta-analysis conducted by Lu confirmed that, in obese patients, the reversal of muscle relaxation using IBW-based dosing of sugammadex took approximately 56 seconds longer than when based on TBW. However, no significant difference in reversal times was found when comparing IBW, TBW, or corrected body weight (CBW) dosing. These findings suggest that a lower-dose regimen based on CBW may be more suitable for morbidly obese patients.47 Considering the current body of evidence, the recommended dosing for sugammadex in obese patients is 1.5–2 mg/kg based on IBW (or IBW+40%) for the reversal of moderate NMB, and 4 mg/kg of IBW+30%-50% for the reversal of deep NMB.
In Patient with Brugada Syndrome
Brugada syndrome (BrS) is an inherited cardiac disorder that renders individuals susceptible to ventricular arrhythmias and abrupt cardiac arrest. The principal interventions include implantable cardioverter-defibrillators (ICDs) and quinidine.48 When administering general anesthesia to patients with Brugada Syndrome, some scholars avoid using neostigmine due to concerns about its cardiovascular adverse reactions when reversing NMB.49 Although some cases have not shown adverse reactions when using neostigmine,50 it still needs to be used cautiously. Ebru Biricik and Rita Conde discovered that 2 mg/kg of sugammadex can be administered safely and effectively to reverse NMB in patients with Brugada Syndrome, and no adverse reactions were observed during postoperative monitoring and follow-up.51,52 Junpei Konishi et al reported that 10mg/kg of sugammadex was used to reverse the deep muscle relaxation induced by 1.2mg/kg of rocuronium in patients with Brugada Syndrome.53
In Patients with Myasthenia Gravis (MG)
Myasthenia gravis (MG) is a disorder affecting the transmission of signals at the neuromuscular junction. It is caused by autoantibodies that target important proteins on the muscle cell’s membrane, specifically the acetylcholine receptor and muscle-specific kinase. This targeting disrupts normal communication between nerves and muscles, resulting in impaired neuromuscular signal transmission.54,55 MG can impact all skeletal muscles, manifesting as variable muscle weakness and abnormal fatigue, with symptoms typically milder in the morning and intensifying throughout the evening. Frequently affected regions include the extraocular muscles, medullary muscles, limb muscles, and respiratory muscles. The involvement of respiratory muscles may result in a myasthenic crisis (acute respiratory failure), representing the most serious complication of MG, with a mortality rate ranging from 10% to 20%.56 Patients with myasthenia gravis are particularly vulnerable to postoperative residual NMB and respiratory complications due to their heightened sensitivity to non-depolarizing muscle relaxants.57 A study by Tomas Vymazal involving 117 MG patients demonstrated that a 2–4 mg/kg dose of sugammadex effectively reversed NMB rapidly in all patients, with no significant adverse events documented.58 Additionally, a substantial cohort study involving 506 patients in Japan undergoing thymoma resection indicated that the use of sugammadex was linked to notable decreases in postoperative myasthenic crises and overall hospitalization expenses in comparison to the control group.59 A retrospective analysis by Hyun-Joung No et al also found that MG patients treated with sugammadex had shorter postoperative hospital stays compared to those treated with neostigmine.60 Furthermore, several case reports have highlighted the successful use of sugammadex in MG patients, with rapid reversal of rocuronium-induced muscle relaxation observed, and minimal postoperative complications.61–70 Notably, one case involved a 3-week-old infant diagnosed with transient MG, who underwent laparoscopic pyloromyotomy for pyloric stenosis.61 In addition, two parturients undergoing cesarean sections under general anesthesia also experienced successful reversal of NMB with sugammadex.67,68 Despite these promising results, there have been reports of incomplete reversal in some cases. For instance, in one MG patient, the administration of 200 mg of sugammadex in four divided doses resulted in a TOFR of only 60%. Full recovery (TOFR = 100%) was ultimately achieved after administering 2 mg of neostigmine and 0.5 mg of atropine 10 minutes later.71 A similar failure of reversal was documented in another MG patient, indicating the need for caution in these cases.72
It is important to note that both the US FDA and the Korean Ministry of Food and Drug Safety caution against the use of sugammadex in patients with severe renal impairment (creatinine clearance <30 mL/min) or those undergoing dialysis. L. M. Staals’ pharmacokinetic study demonstrated that sugammadex clearance is significantly slower in patients with renal failure, leading to prolonged plasma concentrations compared to healthy individuals.73 A number of studies have investigated the use of sugammadex in patients with end-stage renal disease (ESRD) or those who have received kidney transplants.73–83 These studies, including case-control and retrospective analyses, have shown that doses of 2.0 mg/kg and 4.0 mg/kg of sugammadex are effective in reversing both moderate and deep NMBAs induced by rocuronium in these patients. However, recovery times may be longer than in healthy individuals due to the reduced plasma clearance of sugammadex in patients with ESRD. Therefore, careful monitoring of neuromuscular recovery is critical to avoid residual blockade. In patients who have undergone kidney transplantation, sugammadex has been shown to reverse NMB safely and effectively, with no adverse effects on kidney function.
Further Research
The study of residual neuromuscular blockade and postoperative pulmonary complications continues to be a vital area of focus in modern clinical research. A substantial prospective observational study carried out in 28 European nations, including 22,803 patients undergoing general anesthesia, failed to identify a significant association between the reversal of NMBAs and improved clinical outcomes.84 In a similar vein, a randomized controlled trial led by Brandon M. Togioka and colleagues, which assessed older adults undergoing prolonged surgeries, did not demonstrate a significant reduction in in-hospital pulmonary complications with sugammadex as compared to neostigmine.85 These findings are consistent with other studies,86,87 such as those by Leslie et al, who questioned the efficacy of sugammadex in reducing perioperative pulmonary complications and emphasized the need for higher-quality observational trials to substantiate these effects.88 However, despite these mixed findings, a body of large-scale clinical trials has consistently supported sugammadex’s role in reducing perioperative pulmonary complications, suggesting that it may be beneficial in certain patient populations.89
One major challenge in interpreting these studies is the variability in the observation criteria for perioperative pulmonary complications. Furthermore, elements such as age, body mass index (BMI), smoking habits, and pain management approaches may significantly influence the recovery of pulmonary function and hypoxemia during the postoperative period.90 Future clinical trials should control for these confounding variables. Nearly all studies conducted thus far have employed neuromuscular monitoring, with the train-of-four (TOF) ratio of 0.9 being the preferred threshold for monitoring neuromuscular recovery. However, there is still no consensus on the ideal neuromuscular monitoring threshold. Notably, extubation at a TOF ratio of 0.9 has not consistently been linked to a reduction in postoperative pulmonary complications.84 Although a TOF ratio of less than 0.9 is generally recognized as a reliable marker for residual NMB, emerging research suggests that a higher threshold of 0.95 may be more effective in reducing the incidence of postoperative pulmonary complications.91 This highlights the necessity for further studies to investigate the efficacy of recovery to a TOF ratio greater than 0.9. The absence of uniformity in neuromuscular monitoring protocols emphasizes the need for standardized methodologies in future trials. Additionally, while there have been reported cases of sugammadex failure to reverse NMBAs, the underlying causes of these failures and the mechanisms behind sugammadex-induced allergic reactions remain poorly understood. These gaps in knowledge represent critical areas for further investigation to elucidate the complexities surrounding sugammadex’s clinical use and improve patient safety.
Limitations
This study has several important limitations that must be considered. First, the analysis was conducted solely using the WoSCC database, thereby excluding potentially relevant research from other comprehensive academic databases. This limitation could have led to the omission of pertinent studies that may contribute valuable insights to the field. Second, the growing body of sugammadex-related research in anesthesiology presents another challenge. As the volume of publications in this area continues to increase rapidly, it is possible that some relevant studies were overlooked during the data collection process. Consequently, this may have resulted in an incomplete overview of the current landscape of sugammadex research. Third, while bibliometric analysis offers valuable quantitative insights into publication trends, it does not inherently assess the quality of the studies it reviews. Unlike qualitative evaluation methods, such as the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) system, which appraises the strength of evidence, bibliometric analysis primarily focuses on publication volume, citation frequency, and other bibliometric indicators. Therefore, this method does not account for crucial factors such as the rigor of research design or the validity of experimental methodologies, both of which play a significant role in the reliability and impact of research findings. Additionally, bibliometric analysis is prone to the “rich-get-richer” phenomenon. This could potentially bias the representation of emerging or less-prominent research topics, thereby skewing the overall findings of the analysis.
Conclusion
In conclusion, this research employed sophisticated bibliometric tools, such as CiteSpace, VOSviewer, and the Bibliometrix package in R, to perform a thorough and impartial analysis of the research landscape related to sugammadex. Sugammadex, an innovative selective relaxant binding agent in modern anesthesiology, exhibits significantly enhanced reversal efficacy for NMB relative to conventional anticholinesterase agents such as neostigmine, while demonstrating accelerated recovery profiles and reduced incidence of parasympathetic activation-related adverse effects. Over the past decade, the volume of publications on sugammadex has nearly tripled, underscoring its growing significance and laying a robust theoretical foundation for ongoing and future research. Recent studies mainly concentrate on investigating sugammadex’s ability to decrease the occurrence of residual NMBAs and postoperative pulmonary complications across a variety of patient populations. Furthermore, its use in specific demographic groups is an area of active investigation. Moving forward, the frontier of research will likely concentrate on a more granular understanding of sugammadex, including its safety and efficacy in special populations, its integration with neuromuscular monitoring, and the underlying mechanisms of allergic reactions and antagonism failure. Additionally, future studies should aim to elucidate the association between sugammadex use and postoperative complications.
Abbreviations
APY, average publication year; BMI, body mass index; CBW, Corrected Body Weight; CICV, cannot intubate cannot ventilate; DOI, digital object identifier; ED95, Effective Dose 95%; EMA, European Medicines Agency; ESRD, end-stage renal disease; FDA, Food and Drug Administration; IBW, ideal body weight; ICDs, implantable cardioverter-defibrillators; TBW, total body weight; GRADE, Grading of Recommendations Assessment Development and Evaluation; TLS, total link strength; NMBAs, neuromuscular blocking agents; NMB, neuromuscular block; USA, United States of America; WoSCC, Web of Science Core Collection.
Author Contributions
All authors made substantial and integral contributions to the work presented in this manuscript, including the conceptualization, study design, data acquisition, analysis, and interpretation of the results. They were all actively involved in drafting, revising, and critically reviewing the manuscript. Moreover, each author has given their final approval for the version intended for publication.The authors also reached a consensus on the choice of journal for submission and collectively accepted responsibility for all aspects of the work.
Disclosure
Dawei Yin and Bin Tang are co-first authors for this study. Xiaoyan Hu and Huan Hu are co-correspondence authors for this study. The authors state that they have no conflicts of interest to report concerning this work.
References
1. Frenkel M, Lien CA. Eliminating residual neuromuscular blockade: a literature review. Ann Transl Med. 2024;12(4):65. doi:10.21037/atm-23-1743
2. Thilen SR, Weigel WA, Todd MM, et al. American society of anesthesiologists practice guidelines for monitoring and antagonism of neuromuscular blockade: a report by the American society of anesthesiologists task force on neuromuscular blockade. Anesthesiology. 2023;138(1):13–41. doi:10.1097/aln.0000000000004379
3. Fuchs-Buder T, Meistelman C, Raft J. Sugammadex: clinical development and practical use. Korean J Anesthesiol. 2013;65(6):495–500. doi:10.4097/kjae.2013.65.6.495
4. Bridenbaugh PO, Churchll-Davidson HC. Response to tubocurarine chloride and its reversal by neostigmine methylsulfate in man. JAMA. 1968;203(8):541–544. doi:10.1001/jama.1968.03140080001001
5. Murphy GS, Brull SJ. Residual neuromuscular block: lessons unlearned. Part I: definitions, incidence, and adverse physiologic effects of residual neuromuscular block. Anesth Analg. 2010;111(1):120–128. doi:10.1213/ANE.0b013e3181da832d
6. Hristovska A-M, Duch P, Allingstrup M, Afshari A. Efficacy and safety of sugammadex versus neostigmine in reversing neuromuscular blockade in adults. Cochrane Database Syst Rev. 2017;2017(9). doi:10.1002/14651858.Cd012763
7. Chen Y, Jin Q, Fang H, et al. Analytic network process: academic insights and perspectives analysis. J Cleaner Prod. 2019;235:1276–1294. doi:10.1016/j.jclepro.2019.07.016
8. Ninkov A, Frank JR, Maggio LA. Bibliometrics: methods for studying academic publishing. Perspect Med Edu. 2021;11(3):173–176. doi:10.1007/s40037-021-00695-4
9. Peng C, Kuang L, Zhao J, Ross AE, Wang Z, Ciolino JB. Bibliometric and visualized analysis of ocular drug delivery from 2001 to 2020. J Control Release. 2022;345:625–645. doi:10.1016/j.jconrel.2022.03.031
10. Ye L, Liang R, Liu X, Li J, Yue J, Zhang X. Frailty and sarcopenia: a bibliometric analysis of their association and potential targets for intervention. Ageing Res Rev. 2023;92. 10.1016/j.arr.2023.102111.
11. Glanzel W, Chen C, Song M. Visualizing a field of research: a methodology of systematic scientometric reviews. PLoS One. 2019;14(10). doi:10.1371/journal.pone.0223994
12. Chen C. Searching for intellectual turning points: progressive knowledge domain visualization. Proc Natl Acad Sci USA. 2004;101(Suppl 1):5303–5310. doi:10.1073/pnas.0307513100
13. Wang W, Wang H, Yao T, et al. The top 100 most cited articles on COVID-19 vaccine: a bibliometric analysis. Clin Exp Med. 2023;23(6):2287–2299. doi:10.1007/s10238-023-01046-9
14. Blobner M, Hunter JM, Ulm K. How robust are the stronger and stil-stronger studies? Br J Anaesth. 2023;130(1):e41–e44. doi:10.1016/j.bja.2022.08.021
15. Dubois BFH, Fraessdorf J, Blobner M, Hollmann MW, Mouws EMJP. Muscle weakness after sugammadex: incomplete reversal of neuromuscular blockade or delayed postoperative recurarisation? Br J Anaesth. 2023;130(3):e409–e412. doi:10.1016/j.bja.2022.11.016
16. Kaufhold N, Schaller SJ, Stäuble CG, et al. Sugammadex and neostigmine dose-finding study for reversal of residual neuromuscular block at a train-of-four ratio of 0.2 (SUNDRO20). Br J Anaesth. 2016;116(2):233–240. doi:10.1093/bja/aev437
17. Baumüller E, Schaller SJ, Chiquito Lama Y, et al. Postoperative impairment of motor function at train-of-four ratio ≥0.9 cannot be improved by sugammadex (1 mg kg−1). Br J Anaesth. 2015;114(5):785–793. doi:10.1093/bja/aeu453
18. Herring WJ, Mukai Y, Wang A, et al. A randomized trial evaluating the safety profile of sugammadex in high surgical risk ASA physical class 3 or 4 participants. BMC Anesthesiol. 2021;21(1). doi:10.1186/s12871-021-01477-5
19. Carron M, Bertoncello F, Ieppariello G. Profile of sugammadex for reversal of neuromuscular blockade in the elderly: current perspectives. Clin Interv Aging. 2018;13:13–24. doi:10.2147/cia.S134108
20. Pearce B, Holtham A. An unusual cause of dural puncture. Anaesthesia. 2010;65(6):652–653. doi:10.1111/j.1365-2044.2010.06359.x
21. Shin S, Han DW, Lee HS, Song MK, Jun EK, Kim SY. Elderly patients require higher doses of sugammadex for rapid recovery from deep neuromuscular block. Basic Clin Physiol Pharmacol. 2015;118(6):462–467. doi:10.1111/bcpt.12507
22. Muramatsu T, Isono S, Ishikawa T, et al. Differences of recovery from rocuronium-induced deep paralysis in response to small doses of sugammadex between elderly and nonelderly patients. Anesthesiology. 2018;129(5):901–911. doi:10.1097/aln.0000000000002412
23. Williams WH, Cata JP, Lasala JD, Navai N, Feng L, Gottumukkala V. Effect of reversal of deep neuromuscular block with sugammadex or moderate block by neostigmine on shoulder pain in elderly patients undergoing robotic prostatectomy. Br J Anaesth. 2020;124(2):164–172. doi:10.1016/j.bja.2019.09.043
24. Klucka J, Kosinova M, Krikava I, Stoudek R, Toukalkova M, Stourac P. Residual neuromuscular block in paediatric anaesthesia. Br J Anaesth. 2019;122(1):e1–e2. doi:10.1016/j.bja.2018.10.001
25. Won YJ, Lim BG, Lee DK, Kim H, Kong MH, Lee IO. Sugammadex for reversal of rocuronium-induced neuromuscular blockade in pediatric patients: a systematic review and meta-analysis. Medicine. 2016;95(34):e4678. doi:10.1097/md.0000000000004678
26. Tobias JD. Current evidence for the use of sugammadex in children. Paediatr Anaesth. 2017;27(2):118–125. doi:10.1111/pan.13050
27. Efune PN, Alex G, Mehta SD. Emergency sugammadex reversal in an 850-G premature infant: a case report. J Pediatr Pharmacol Ther. 2021;26(1):107–110. doi:10.5863/1551-6776-26.1.107
28. Carlos RV, Torres ML, de Boer HD. Rocuronium and sugammadex in a 3 days old neonate for draining an ovarian cyst. neuromuscular management and review of the literature. Braz J Anesthesiol. 2016;66(4):430–432. doi:10.1016/j.bjane.2015.01.004
29. Salaün JP, Décary E, Veyckemans F. Recurarisation after sugammadex in children: review of case reports and recommendations. Br J Anaesth. 2024;132(2):410–414. doi:10.1016/j.bja.2023.09.028
30. Cheymol G. Effects of obesity on pharmacokinetics implications for drug therapy. Clin Pharmacokinet. 2000;39(3):215–231. doi:10.2165/00003088-200039030-00004
31. Adams JP, Murphy PG. Obesity in anaesthesia and intensive care. Br J Anaesth. 2000;85(1):91–108. doi:10.1093/bja/85.1.91
32. Leykin Y, Pellis T, Lucca M, Lomangino G, Marzano B, Gullo A. The pharmacodynamic effects of rocuronium when dosed according to real body weight or ideal body weight in morbidly obese patients. Anesth Analg. 2004;99(4):1086–1089. doi:10.1213/01.Ane.0000120081.99080.C2
33. Shashaty MGS, Stapleton RD. Physiological and management implications of obesity in critical illness. Ann Am Thoracic Soc. 2014;11(8):1286–1297. doi:10.1513/AnnalsATS.201404-159FR
34. Plaud B, Debaene B, Donati F, Marty J. Residual paralysis after emergence from anesthesia. Anesthesiology. 2010;112(4):1013–1022. doi:10.1097/ALN.0b013e3181cded07
35. Wang S, Dong Y, Wang S, Han Y, Li Q. The efficacy and adverse effects of sugammadex and neostigmine in reversing neuromuscular blockade inpatients with obesity undergoing metabolic and bariatric surgery: a systematic review with meta-analysis and trial sequential analysis. Medicina. 2024;60(11). doi:10.3390/medicina60111842
36. Claroni C, Covotta M, Torregiani G, et al. Recovery from anesthesia after robotic-assisted radical cystectomy: two different reversals of neuromuscular blockade. J Clin Med. 2019;8(11):1774. doi:10.3390/jcm8111774
37. Bom A, Bradley M, Cameron K, et al. A novel concept of reversing neuromuscular block: chemical encapsulation of rocuronium bromide by a cyclodextrin-based synthetic host. Angew Chem Int Ed Engl. 2002;41(2):266–270. doi:10.1002/1521-3773(20020118)41:2<265::aid-anie265>3.0.co;2-q
38. Naguib M. Sugammadex: another milestone in clinical neuromuscular pharmacology. Anesth Analg. 2007;104(3):575–581. doi:10.1213/01.ane.0000244594.63318.fc
39. Brueckmann B, Sasaki N, Grobara P, et al. Effects of sugammadex on incidence of postoperative residual neuromuscular blockade: a randomized, controlled study. Br J Anaesth. 2015;115(5):743–751. doi:10.1093/bja/aev104
40. Asztalos L, Szabó-Maák Z, Gajdos A, et al. Reversal of vecuronium-induced neuromuscular blockade with low-dose sugammadex at train-of-four count of four: a randomized controlled trial. Anesthesiology. 2017;127(3):441–449. doi:10.1097/aln.0000000000001744
41. Van Lancker P, Dillemans B, Bogaert T, Mulier JP, De Kock M, Haspeslagh M. Ideal versus corrected body weight for dosage of sugammadex in morbidly obese patients. Anaesthesia. 2011;66(8):721–725. doi:10.1111/j.1365-2044.2011.06782.x
42. Llauradó S, Sabaté A, Ferreres E, Camprubí I, Cabrera A. Sugammadex ideal body weight dose adjusted by level of neuromuscular blockade in laparoscopic bariatric surgery. Anesthesiology. 2012;117(1):93–98. doi:10.1097/ALN.0b013e3182580409
43. Badaoui R, Cabaret A, Alami Y, et al. Reversal of neuromuscular blockade by sugammadex in laparoscopic bariatric surgery: in support of dose reduction. Anaesth Crit Care Pain Med. 2016;35(1):25–29. doi:10.1016/j.accpm.2015.09.003
44. Sanfilippo M, Alessandri F, Wefki Abdelgawwad Shousha AA, Sabba A, Cutolo A. Sugammadex and ideal body weight in bariatric surgery. Anesthesiol Res Pract. 2013;2013:389782. doi:10.1155/2013/389782
45. Abd El-Rahman AM, Othman AH, El Sherif FA, Mostafa MF, Taha O. Comparison of three different doses sugammadex based on ideal body weight for reversal of moderate rocuronium-induced neuromuscular blockade in laparoscopic bariatric surgery. Minerva Anestesiol. 2017;83(2):138–144. doi:10.23736/s0375-9393.16.11349-5
46. Duarte N, Caetano AMM, Neto S, Filho GRO, Arouca GO, Campos JM. Sugammadex by ideal body weight versus 20% and 40% corrected weight in bariatric surgery - double-blind randomized clinical trial. Braz J Anesthesiol. 2018;68(3):219–224. Uso de sugamadex pelo peso corporal ideal versus corrigido em 20% e 40% em cirurgia bariátrica – ensaio clínico randômico e duplo‐cego. doi:10.1016/j.bjan.2017.10.010
47. Liao JQ, Shih D, Lin TY, Lee M, Lu CW. Appropriate dosing of sugammadex for reversal of rocuronium-/vecuronium-induced muscle relaxation in morbidly obese patients: a meta-analysis of randomized controlled trials. J Int Med Res. 2022;50(8):3000605221116760. doi:10.1177/03000605221116760
48. Karlinski Vizentin V, Ferreira Felix I, da Fonseca R P, et al. Epicardial substrate ablation in patients with symptomatic Brugada syndrome: an updated systematic review and single-arm meta-analysis. Heart Rhythm. 2025. doi:10.1016/j.hrthm.2025.01.006
49. Cordery R, Lambiase P, Lowe M, Ashley E. Brugada syndrome and anesthetic management. J Cardiothorac Vasc Anesth. 2006;20(3):407–413. doi:10.1053/j.jvca.2006.02.005
50. Edge CJ, Blackman DJ, Gupta K, Sainsbury M. General anaesthesia in a patient with Brugada syndrome. Br J Anaesth. 2002;89(5):788–791. doi:10.1093/bja/89.5.788
51. Biricik E, Hatipoglu Z, Kucukbingoz C. Sugammadex in a patient with Brugada syndrome. urk J Anaesthesiol Reanim. 2016;44(2):99–101. doi:10.5152/tjar.2016.60973
52. Conde R, Pereira M. Anesthetic management of a patient with Brugada syndrome - the use of sugammadex in major abdominal surgery. Braz J Anesthesiol. 2013;63(1):159–160. doi:10.1016/S0034-7094(13)70207-1
53. Konishi J, Suzuki T, Kondo Y, Baba M, Ogawa S. Rocuronium and sugammadex used effectively for electroconvulsive therapy in a patient with Brugada syndrome. J ect. 2012;28(2):e21–22. doi:10.1097/YCT.0b013e31824b74f5
54. Phillips WD, Vincent A. Pathogenesis of myasthenia gravis: update on disease types, models, and mechanisms. F1000Res. 2016;5. 10.12688/f1000research.8206.1.
55. Koneczny I, Herbst R. Myasthenia gravis: pathogenic effects of autoantibodies on neuromuscular architecture. Cells. 2019;8(7). doi:10.3390/cells8070671
56. Dresser L, Wlodarski R, Rezania K, Soliven B. Myasthenia gravis: epidemiology, pathophysiology and clinical manifestations. J Clin Med. 2021;10(11):2235. doi:10.3390/jcm10112235
57. Drachman DB. Myasthenia gravis and other diseases of the neuromuscular junction. In: Harrison’s Principles of Internal Medicine. McGraw-Hill Companies, Inc; 2008.
58. Vymazal T, Krecmerova M, Bicek V, Lischke R. Feasibility of full and rapid neuromuscular blockade recovery with sugammadex in myasthenia gravis patients undergoing surgery - a series of 117 cases. Ther Clin Risk Manag. 2015;11:1593–1596. doi:10.2147/tcrm.S93009
59. Mouri H, Jo T, Matsui H, Fushimi K, Yasunaga H. Effect of sugammadex on postoperative myasthenic crisis in myasthenia gravis patients: propensity score analysis of a Japanese nationwide database. Anesth Analg. 2020;130(2):367–373. doi:10.1213/ane.0000000000004239
60. No HJ, Yoo YC, Oh YJ, et al. Comparison between sugammadex and neostigmine after video-assisted thoracoscopic surgery-thymectomy in patients with myasthenia gravis: a single-center retrospective exploratory analysis. J Pers Med. 2023;13(9):1380. doi:10.3390/jpm13091380
61. Rubin JE, Ramamurthi RJ. The role of sugammadex in symptomatic transient neonatal myasthenia gravis: a case report. A a Case Rep. 2017;9(9):271–273. doi:10.1213/xaa.0000000000000590
62. Unterbuchner C, Fink H, Blobner M. The use of sugammadex in a patient with myasthenia gravis. Anaesthesia. 2010;65(3):302–305. doi:10.1111/j.1365-2044.2009.06236.x
63. Kuo KC, Wong CS, Wu TJ. Case report: successful reversal of residual block with sugammadex in a patient not known to have myasthenia gravis. Am J Case Rep. 2022;
64. Dontukurthy S, Wisler C, Raman V, Tobias JD. Myasthenia gravis and sugammadex: a case report and review of the literature. Saudi J Anaesth. 2020;14(2):244–248. doi:10.4103/sja.SJA_721_19
65. Sungur Ulke Z, Yavru A, Camci E, Ozkan B, Toker A, Senturk M. Rocuronium and sugammadex in patients with myasthenia gravis undergoing thymectomy. Acta Anaesthesiol Scand. 2013;57(6):745–748. doi:10.1111/aas.12123
66. De Boer HD, Van Egmond J, Driessen JJ, Booij L. Sugammadex in patients with myasthenia gravis. Anaesthesia. 2010;65(6):653. doi:10.1111/j.1365-2044.2010.06360.x
67. Garcia V, Diemunsch P, Boet S. Use of rocuronium and sugammadex for caesarean delivery in a patient with myasthenia gravis. Int J Obstet Anesth. 2012;21(3):286–287. doi:10.1016/j.ijoa.2012.02.006
68. Soyoral L, Goktas U, Cegin MB, Baydi V. Successful use of sugammadex for caesarean section in a patient with myasthenia gravis. Braz J Anesthesiol. 2017;67(2):221–222. doi:10.1016/j.bjane.2014.08.008
69. Rudzka-Nowak A, Piechota M. Anaesthetic management of a patient with myasthenia gravis for abdominal surgery using sugammadex. Arch Med Sci. 2011;7(2):361–364. doi:10.5114/aoms.2011.22094
70. Song S, Cho HB, Park SY, et al. Postoperative mortality in patients with end-stage renal disease according to the use of sugammadex: a single-center retrospective propensity score matched study. Anesth Pain Med. 2022;17(4):371–380. doi:10.17085/apm.22189
71. Fernandes HDS, Ximenes JLS, Nunes DI, Ashmawi HA, Vieira JE. Failure of reversion of neuromuscular block with sugammadex in patient with myasthenia gravis: case report and brief review of literature. BMC Anesthesiol. 2019;19(1):160. doi:10.1186/s12871-019-0829-0
72. Sugi Y, Nitahara K, Shiroshita T, Higa K. Restoration of train-of-four ratio with neostigmine after insufficient recovery with sugammadex in a patient with myasthenia gravis. A a Case Rep. 2013;1(3):43–45. doi:10.1097/ACC.0b013e3182953053
73. Staals LM, Snoeck MM, Driessen JJ, Flockton EA, Heeringa M, Hunter JM. Multicentre, parallel-group, comparative trial evaluating the efficacy and safety of sugammadex in patients with end-stage renal failure or normal renal function. Br J Anaesth. 2008;101(4):492–497. doi:10.1093/bja/aen216
74. Staals LM, Snoeck MM, Driessen JJ, et al. Reduced clearance of rocuronium and sugammadex in patients with severe to end-stage renal failure: a pharmacokinetic study. Br J Anaesth. 2010;104(1):31–39. doi:10.1093/bja/aep340
75. Min KC, Lasseter KC, Marbury TC, et al. Pharmacokinetics of sugammadex in subjects with moderate and severe renal impairment. Int J Clin Pharmacol Ther. 2017;55(9):746–752. doi:10.5414/cp203025
76. Adams DR, Tollinche LE, Yeoh CB, et al. Short-term safety and effectiveness of sugammadex for surgical patients with end-stage renal disease: a two-centre retrospective study. Anaesthesia. 2020;75(3):348–352. doi:10.1111/anae.14914
77. Ono Y, Fujita Y, Kajiura T, et al. Efficacy and safety of sugammadex in patients undergoing renal transplantation. JA Clin Rep. 2018;4(1):56. doi:10.1186/s40981-018-0192-z
78. Paredes S, Porter SB, Porter IE, Renew JR. Sugammadex use in patients with end-stage renal disease: a historical cohort study. Can J Anaesth. 2020;67(12):1789–1797. Utilisation de sugammadex chez les patients atteints d’insuffisance rénale terminale: une étude de cohorte historique. doi:10.1007/s12630-020-01812-3
79. de Souza CM, Tardelli MA, Tedesco H, et al. Efficacy and safety of sugammadex in the reversal of deep neuromuscular blockade induced by rocuronium in patients with end-stage renal disease: a comparative prospective clinical trial. Eur J Anaesthesiol. 2015;32(10):681–686. doi:10.1097/eja.0000000000000312
80. Valente A. High need for sugammadex for rocuronium reversal with acute renal failure and normal need in the same patient with no renal impairment. J Clin Anesth. 2020;67:109981. doi:10.1016/j.jclinane.2020.109981
81. Arslantas R, Cevik BE. Retrospective investigation of grafted kidney function after reversal of neuromuscular blockade using neostigmine or sugammadex. Transplant Proc. 2019;51(7):2265–2267. doi:10.1016/j.transproceed.2019.03.051
82. Vargas M, Buonanno P, Sica A, et al. Effects of sugammadex plus rocuronium vs neostigmine plus cisatracurium during renal transplantation on graft function: a retrospective, case-control study. Transplant Proc. 2021;53(3):818–824. doi:10.1016/j.transproceed.2020.09.012
83. Carron M, Andreatta G, Pesenti E, et al. Impact on grafted kidney function of rocuronium-sugammadex vs cisatracurium-neostigmine strategy for neuromuscular block management. An Italian single-center, 2014-2017 retrospective cohort case-control study. Perioper Med. 2022;11(1):3. doi:10.1186/s13741-021-00231-2
84. Kirmeier E, Eriksson LI, Lewald H, et al. Post-anaesthesia pulmonary complications after use of muscle relaxants (POPULAR): a multicentre, prospective observational study. Lancet Respir Med. 2019;7(2):129–140. doi:10.1016/s2213-2600(18)30294-7
85. Togioka BM, Yanez D, Aziz MF, Higgins JR, Tekkali P, Treggiari MM. Randomised controlled trial of sugammadex or neostigmine for reversal of neuromuscular block on the incidence of pulmonary complications in older adults undergoing prolonged surgery. Br J Anaesth. 2020;124(5):553–561. doi:10.1016/j.bja.2020.01.016
86. Martinez-Ubieto J, Ortega-Lucea S, Pascual-Bellosta A, et al. Prospective study of residual neuromuscular block and postoperative respiratory complications in patients reversed with neostigmine versus sugammadex. Minerva Anestesiol. 2016;82(7):735–742.
87. Alday E, Muñoz M, Planas A, Mata E, Alvarez C. Effets du renversement du bloc neuromusculaire à l’aide de sugammadex vs de la néostigmine sur l’évolution respiratoire postopératoire après une chirurgie abdominale majeure: une étude randomisée contrôlée. [Effects of neuromuscular block reversal with sugammadex versus neostigmine on postoperative respiratory outcomes after major abdominal surgery: a randomized-controlled trial]. Can J Anaesth. 2019;66(11):1328–1337. doi:10.1007/s12630-019-01419-3
88. Leslie K. Sugammadex and postoperative pulmonary complications: is stronger evidence required? Anesthesiology. 2020;132(6):1299–1300. doi:10.1097/aln.0000000000003282
89. Kheterpal S, Vaughn MT, Dubovoy TZ, et al. Sugammadex versus neostigmine for reversal of neuromuscular blockade and postoperative pulmonary complications (STRONGER): a multicenter matched cohort analysis. Anesthesiology. 2020;132(6):1371–1381. doi:10.1097/aln.0000000000003256
90. Wang X, Guo K, Sun J, et al. Semirecumbent positioning during anesthesia recovery and postoperative hypoxemia: a randomized clinical trial. JAMA Network Open. 2024;7(6):e2416797. doi:10.1001/jamanetworkopen.2024.16797
91. Blobner M, Hunter JM, Meistelman C, et al. Use of a train-of-four ratio of 0.95 versus 0.9 for tracheal extubation: an exploratory analysis of POPULAR data. Br J Anaesth. 2020;124(1):63–72. doi:10.1016/j.bja.2019.08.023
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Worldwide Bibliometric Analysis of Published Literature on Osteoporosis Vertebral Compression Fracture
Li Y, Tian J, Ge M, Ji L, Kang Y, Xia C, Zhang J, Huang Y, Feng F, Zhao T, Shao H
Journal of Pain Research 2022, 15:2373-2392
Published Date: 18 August 2022
Scientific Knowledge of Rheumatoid Arthritis: A Bibliometric Analysis from 2011 to 2020
Xu J, Yu J, Jiao W, Chen G, Liu L, Zhang M, Wu D
Journal of Pain Research 2022, 15:2761-2772
Published Date: 8 September 2022
A Bibliometric Analysis of Acupuncture Treatment of Tension-Type Headache from 2003 to 2022
Zhu D, Xu W, Mao Q, Zhong G, Chen R, Jiao L
Journal of Pain Research 2023, 16:1647-1662
Published Date: 18 May 2023
Bibliometric and Visual Analysis in the Field of Dry Needling for Myofascial Pain Syndrome from 2000 to 2022
Luo N, Li R, Fu B, Zeng Y, Fang J
Journal of Pain Research 2023, 16:2461-2475
Published Date: 18 July 2023
Bibliometric Analysis of Global Trends in Remimazolam-Related Research Over the Past 15 Years: Compared with Propofol
Hu X, Wang B, Hu L, Han D, Wu J
Drug Design, Development and Therapy 2023, 17:2119-2135
Published Date: 20 July 2023