Back to Journals » Advances in Medical Education and Practice » Volume 17
A Comparative Educational Intervention Study of Peer Teaching and Flipped Classroom Models in Pediatric Intensive Care Rotation
Authors Wu S, Ma J, Zhou L, Huang S, Dong X, Li Y, Huang J, Bai Z
Received 15 February 2026
Accepted for publication 21 May 2026
Published 29 May 2026 Volume 2026:17 603790
DOI https://doi.org/10.2147/AMEP.S603790
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sateesh Arja
Shuiyan Wu,1 Jiajun Ma,1 Libing Zhou,1 Saihu Huang,1 Xingqiang Dong,1 Ying Li,1 Jie Huang,2 Zhenjiang Bai1
1Pediatric Intensive Care Unit, Children’s Hospital of Soochow University, Suzhou, Jiangsu, 215025, People’s Republic of China; 2Department of Clinical Pediatrics, Children’s Hospital of Soochow University, Suzhou, Jiangsu, 215025, People’s Republic of China
Correspondence: Zhenjiang Bai
Pediatric Intensive Care Unit, Children’s Hospital of Soochow University, Suzhou, Jiangsu, People’s Republic of China
, Tel +86-0512-80692300, Email [email protected]
Background: Providing effective pediatric critical care education during short pediatric intensive care unit (PICU) rotations remains challenging due to high patient acuity, time-sensitive decision-making, and limited reflection time. This study aimed to compare the impact of peer teaching and flipped classroom models on educational outcomes for residents during PICU rotations.
Methods: This single-center, non-randomized comparative educational intervention study included 76 residents rotating in the PICU at the Children’s Hospital of Soochow University between January 2022 and October 2023. Residents participated in either peer teaching (Group A, n = 38) or flipped classroom teaching (Group B, n = 38). Outcomes were evaluated using theoretical examinations, Mini-Clinical Evaluation Exercise (mini-CEX) scores, and post-intervention questionnaires assessing self-perceived skill improvement and engagement.
Results: There were no significant differences in theoretical examination scores (80.77 ± 6.29 vs 80.08 ± 7.29, p = 0.526) or mini-CEX performance (7.92 ± 0.82 vs 7.90 ± 0.73, p = 0.837) between the two groups. Residents in the peer teaching group reported greater improvements in communication skills, confidence, and problem-solving ability. In contrast, residents in the flipped classroom group perceived greater gains in conceptual understanding and teamwork. Most participants (92.1%) regularly accessed online lectures, and content relevance to clinical practice was rated highly (8.44 ± 1.85).
Conclusion: Both peer teaching and flipped classroom approaches were effective in PICU resident education, each demonstrating distinct strengths in fostering different competencies. A blended educational strategy may further optimize learning outcomes during short-term critical care rotations.
Keywords: peer teaching, flipped classroom, pediatric intensive care, resident education, medical education
Introduction
Pediatric critical care medicine is a core component of standardized residency training. The pediatric intensive care unit (PICU) environment is characterized by complex pathophysiology, multi-organ dysfunction, and the need for rapid clinical decision-making. This high-stakes setting presents unique educational challenges: short rotation durations limit deep immersion, patient acuity demands immediate application of knowledge, and time constraints restrict opportunities for structured reflection.1–3 Residents rotating through the PICU must therefore integrate theoretical knowledge with real-time clinical reasoning under significant pressure. Traditional lecture-based teaching, which primarily relies on passive knowledge transmission, may be insufficient to address these cognitive and practical demands. As a result, learner-centered educational strategies have increasingly been introduced in medical education to promote active engagement, knowledge consolidation, and clinical reasoning.
The flipped classroom model is one such strategy that has gained widespread attention. In this model, learners acquire foundational knowledge prior to class through pre-recorded lectures or digital materials and then apply this knowledge during interactive clinical discussions. By shifting lower-order cognitive tasks outside the classroom, flipped teaching allows in-class time to focus on higher-order thinking activities such as problem-solving and case analysis.4,5 While this model can enhance active learning and conceptual understanding,6–8 its success in high-intensity settings like the PICU hinges on learner self-regulation and consistent pre-class preparation, which may be variable under time constraints.
Peer teaching represents another learner-centered strategy that has been increasingly adopted in medical education. In peer teaching models, learners assume instructional roles and teach content to their colleagues. This process requires knowledge organization, reflection, and articulation, which may promote deeper cognitive processing and reinforce understanding.9–11 Peer teaching has been shown to enhance communication skills, confidence, and engagement, particularly in clinical skill training. However, its effectiveness can be influenced by variability in peer teaching quality and the cognitive load of simultaneously learning and teaching in a demanding rotation. Nevertheless, few studies have directly compared peer teaching and flipped classroom models within high-intensity clinical environments such as the PICU.
Although both approaches emphasize active learning, they may foster different dimensions of competency development. Specifically, peer teaching may excel in developing procedural confidence and communication, while the flipped classroom might better support structured knowledge acquisition and conceptual integration. There remains limited evidence regarding their relative effectiveness and potential complementary roles in short-term pediatric critical care rotations. In our PICU, both peer teaching and flipped classroom models have been implemented over the past two years. The present study aimed to compare these two models across multiple educational outcome domains—including knowledge acquisition, clinical skill performance, and self-perceived competencies in communication, problem-solving, and teamwork, and to explore their respective strengths in supporting resident learning during short-term PICU training.
Methods
Study Design
This was a single-center, non-randomized comparative educational intervention study conducted at the Children’s Hospital of Soochow University between January 2022 and October 2023. The study employed a sequential, cohort-based design. To minimize temporal confounding and ensure comparable exposure for all participants, the two teaching models were implemented in alternating 2-month blocks over the study period. Each resident participated in only one teaching model during their two-month PICU rotation. Thus, participants were allocated to either the peer teaching or flipped classroom group based on the rotation period in which they were enrolled. This study received ethics approval from the Institutional Review Board of Children’s Hospital of Soochow University (Approval Number: 2024CS196). All participants provided written informed consent. Participation was voluntary, and residents were informed that their decision would not affect their academic evaluation or rotation grading.
Participants
Eligible participants were all residents undertaking their mandatory two-month PICU rotation within the study period. Residents were excluded if their rotation duration was longer than two months, or if they had participated in both teaching models due to schedule adjustments. All 76 eligible residents consented to participate and were enrolled consecutively, resulting in a total sample size of 76. Thirty-eight residents participated during a period where the peer teaching model was active and were assigned to the peer teaching group (Group A), and thirty-eight residents participated during a subsequent period where the flipped classroom model was active and were assigned to the flipped classroom group (Group B). All residents completed the full rotation. Baseline characteristics of the participants, including age, gender, training year, and prior PICU experience, are presented in Table 1.
 |
Table 1 Comparison of Clinical Ability Assessment Between Peer Teaching and Flipped Teaching Groups |
Educational Interventions
Peer Teaching (Group A)
Residents selected topics from ten core PICU subjects, including sepsis, pediatric advanced life support, diabetic ketoacidosis, acute respiratory distress syndrome, oxygen therapy, multiple organ dysfunction syndrome, intracranial hypertension, and electrolyte imbalance.
Residents prepared 10–15-minute lectures and presented them to peers using blackboard-based instruction. Faculty members provided commentary and facilitated discussion. Each session included 5–6 interactive questions. See Figure S1 for details of the post-session questions.
Flipped Classroom (Group B)
Critical care physicians recorded ten core topic lectures (10–15 minutes each), which were professionally edited and uploaded to the WeChat learning platform. Residents were required to complete viewing one week before rotation.
Each topic included five structured questions. During ward rounds, faculty facilitated case-based discussions to reinforce theoretical knowledge and clinical application.
Outcome Measures
Primary Outcomes
Theoretical Examination
An end-of-rotation examination was developed specifically for this study. The multiple-choice test was blueprint-aligned to cover all ten core PICU topics. It was reviewed for content validity by three independent PICU faculty members. The examination was administered electronically at the end of the rotation under standardized conditions.
Mini-Clinical Evaluation Exercise (Mini-CEX)
A structured mini-CEX assessment was conducted by supervising faculty during real patient encounters. Each resident was assessed once during the rotation across six domains: medical interviewing, physical examination, clinical judgment, professionalism, counseling skills, and overall clinical competence, using a 9-point rating scale (1–9). All assessors received a standardized briefing on the scoring criteria prior to the study. The internal consistency (Cronbach’s alpha) of the mini-CEX tool in our context was 0.88.
Secondary Outcomes
Self-Reported Improvements
To assess perceived learning gains in a comparable manner across groups, we administered a standardized post-intervention questionnaire in Figure S2. This questionnaire assessed residents’ self-perceived improvements in communication skills, confidence, problem-solving ability, conceptual understanding, and teamwork. All items used a uniform 10-point Likert scale (1 = no improvement, 10 = exceptional improvement). The questionnaire was piloted for clarity and relevance with a small group of residents not involved in the study.
Data Collection
All outcome data were collected at the end of the two-month rotation period, immediately prior to the resident’s departure from the PICU. Data collection was overseen by a research assistant who was not involved in the teaching or clinical assessment of the residents.
Statistical Analysis
Statistical analyses were performed using SPSS version 22.0. Continuous variables were expressed as mean ± standard deviation and compared using independent-sample t-tests. Categorical variables were analyzed using chi-square tests or Fisher’s exact test as appropriate. To describe the magnitude of differences between groups, effect sizes were calculated. For between-group comparisons of continuous outcomes, Cohen’s d was reported with 95% confidence intervals (CIs). For comparisons of proportions, the absolute difference with 95% CIs was reported. A p-value <0.05 was considered statistically significant.
Results
Baseline Characteristics
A total of 76 residents completed the PICU rotation and were included in the final analysis, with 38 residents assigned to the peer teaching group (Group A) and 38 to the flipped classroom group (Group B) (Figure 1). Baseline characteristics were comparable between the two groups. The mean age was 29 years in Group A and 26 years in Group B, with no statistically significant difference (p = 0.073). Residents’ training level (post-graduate year), prior PICU experience, and prior exposure to similar active learning methods were also similar between groups (Table 1). The proportion of male residents was also similar between groups (26.3% vs 23.7%, p = 1.000), indicating balanced demographic characteristics at baseline.
 |
Figure 1 The flow chart of this study. |
Outcomes in Knowledge Acquisition and Clinical Performance
In line with the study aim of comparing educational outcomes, we first evaluated objective measures of knowledge and clinical skill. At the end of the rotation, no statistically significant differences were observed between the two groups in objective academic performance. The mean theoretical examination score was 80.77 ± 6.29 in the peer teaching group and 80.08 ± 7.29 in the flipped classroom group (t = 0.442, p = 0.526, Cohen’s d = 0.101, 95% CI [–0.349, 0.551]). Similarly, mini-CEX scores were comparable between groups (7.92 ± 0.82 vs 7.90 ± 0.73, t = 0.106, p = 0.837, Cohen’s d = 0.024, 95% CI [–0.425, 0.474]) (Table 1). These findings suggest that both educational strategies achieved similar outcomes in knowledge acquisition and clinical performance.
Self-Reported Competency Development
Although objective examination results were similar, differences emerged in residents’ self-perceived development across specific competency domains. Residents in the peer teaching group reported significantly greater mean improvements in communication skills (89.5% vs 42.1%, χ2=15.529, p < 0.001), and problem-solving ability (92.1% vs 81.6%, χ2=1.058, p = 0.304). In contrast, residents in the flipped classroom group reported greater gains in conceptual understanding (60.5% vs 71.1%, χ2=0.901, p = 0.343) and teamwork and cooperation skills (5.3% vs 31.6%, χ2=7.924, p = 0.005) (Figure 2). These results indicate that the two teaching approaches were associated with distinct patterns of perceived competency development.
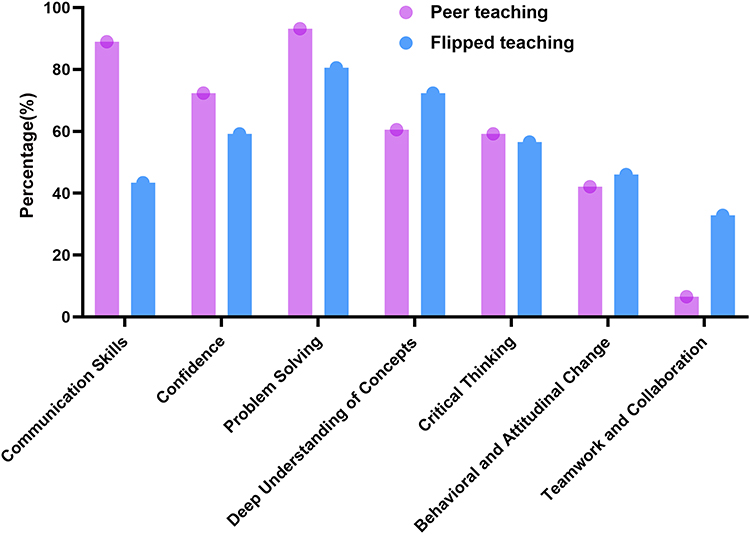 |
Figure 2 Analysis of lecture effects on residents participating in peer and flipped teaching groups. X axis, residents’ self-reported competency development, Y axis, the percentage (%). |
Engagement and Perceptions of the Flipped Classroom Model
Engagement with the flipped classroom model was high. In Group B, 92.1% (35/38) of residents completed the pre-recorded lectures via the WeChat platform before the end of rotation. The average self-reported familiarity with lecture content prior to viewing was 4.91 ± 2.16 on a 10-point scale. After completing the online modules, residents rated the ease of understanding as 7.78 ± 1.70 and the practicality of the lecture content for clinical work as 8.44 ± 1.85, suggesting high perceived educational value.
Topic Selection and Preparation Characteristics in Peer Teaching
In the peer teaching group, residents selected topics from ten predefined PICU subjects. Most participants chose topics inspired by patients under their care (71.1%) or based on personal interest (57.9%). Additional factors influencing topic selection included practicality (76.3%), common diseases (55.3%), novelty (42.1%), and simplicity (7.9%) (Figure 3).
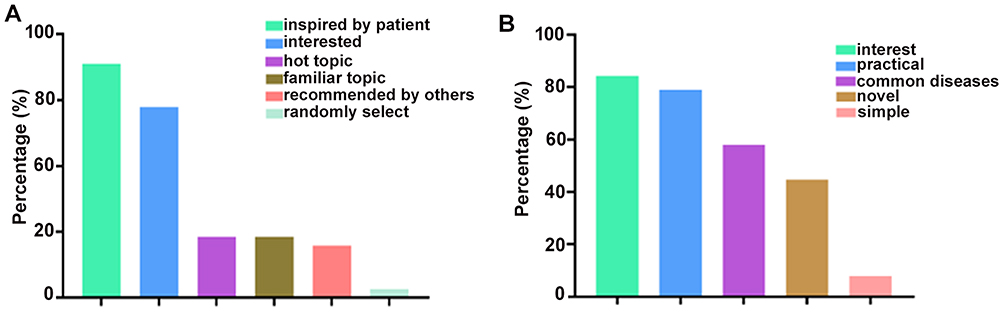 |
Figure 3 A: Survey of topic content among residents in peer teaching group. (B) Perspectives of students on lecture content in peer teaching group. |
Residents were further categorized according to preparation time (<7 days vs ≥7 days). Those in the <7-day group were significantly younger (25.50 ± 4.68 vs 29.82 ± 6.04 years, p = 0.022) and reported lower stress levels (p = 0.033). However, self-evaluation scores did not differ significantly between the two preparation groups (6.69 ± 1.45 vs 6.36 ± 1.50, p = 0.509) (Table 2).
 |
Table 2 Relationship Between Preparation Time and Self-Evaluation of Residents in Peer Lectures |
Discussion
Pediatric critical care training presents unique educational challenges. Compared with other specialties, the PICU environment requires rapid decision-making, integration of multi-organ pathophysiology, and proficiency in invasive procedures. Residents rotating through the PICU must therefore acquire substantial theoretical knowledge while simultaneously developing clinical reasoning within a limited timeframe. Traditional lecture-based instruction alone may be insufficient to meet these complex educational demands, as it often emphasizes passive knowledge transmission rather than active cognitive engagement.12,13 Our study was designed to evaluate how two active learning models—peer teaching and the flipped classroom—might address these challenges in a short PICU rotation. The core finding of our study is that both interventions were similarly effective in promoting knowledge acquisition (theoretical examination) and clinical performance (mini-CEX).
In the present study, both peer teaching and flipped classroom approaches achieved comparable objective outcomes in theoretical examination scores and mini-CEX performance. These findings are consistent with previous studies demonstrating that innovative learner-centered strategies do not necessarily produce superior short-term examination results but may enhance engagement and perceived learning effectiveness.4,5,8,14 It reinforces the notion that within a compressed timeframe, providing structured, focused educational content—whether through peer-led synthesis or faculty-curated pre-learning—is key to achieving baseline competency, and that one model is not objectively superior to the other in this regard.
However, a deeper, more nuanced picture emerged from the analysis of residents’ self-perceived competency development, which directly addressed our aim of exploring the “respective strengths” of each model. We found distinct, statistically significant patterns with moderate to large effect sizes. Residents in the peer teaching group reported substantially greater improvements in communication skills, confidence, and problem-solving ability. This can be theoretically explained by the “learning-by-teaching” effect.15,16
Furthermore, preparation and presentation may enhance metacognitive awareness and self-efficacy, explaining the observed increase in confidence. Although residents who prepared for longer periods reported higher stress levels, their self-evaluation scores were not significantly different, suggesting that moderate cognitive load may not adversely affect perceived learning outcomes.17,18
In contrast, residents in the flipped classroom group more frequently reported improvements in conceptual understanding and teamwork. The structured, pre-class acquisition of knowledge likely served to “front-load” foundational concepts, freeing up cognitive resources during in-person sessions for higher-order activities like synthesis, application, and collaborative problem-solving.6,7,19 This model effectively created a shared baseline of knowledge among the group, facilitating more sophisticated and equitable case discussions during ward rounds, which in turn fostered teamwork. The high engagement rate (92.1%) and positive ratings for content clarity and clinical relevance confirm that this model was both feasible and valued by learners in the high-pressure PICU context, though its success is contingent on the quality of digital resources and learner self-regulation.20,21
An important implication of our findings is that reliance solely on traditional objective metrics (exam scores, checklist-based assessments) may obscure important educational benefits. Although examination scores were similar, residents perceived meaningful and distinct skill development aligned with the inherent pedagogical structure of each model. This suggests that the choice of teaching model should be guided not by a quest for superior test scores, but by the specific competency domains one aims to emphasize. Peer teaching appears particularly suited to cultivating procedural confidence, communication clarity, and knowledge synthesis—skills critical for independent practice and handovers. Flipped teaching may be more effective at building a robust, shared conceptual framework and fostering collaborative clinical reasoning.
Therefore, rather than viewing these as competing strategies, our data support their complementary nature. A blended educational model that strategically integrates both approaches could leverage their respective strengths: using flipped classroom elements to ensure efficient and consistent knowledge transfer, and incorporating peer teaching sessions to solidify that knowledge through explanation and to hone communication and teaching skills. Such a model may offer a more holistic and optimized learning experience for residents navigating the intense, time-limited PICU environment.10,11
Limitations
This study has several limitations that temper the generalizability of our conclusions and should be considered when interpreting the results. First, it was conducted at a single center with a relatively small sample size. Second, the non-randomized, sequential cohort design, while pragmatic, introduces the possibility of selection bias and unmeasured temporal confounding. Third, outcomes were assessed immediately post-intervention without long-term follow-up to determine skill retention. Finally, while we standardized and validated our self-report measures in revision, they remain subject to recall and social desirability biases. Most critically, the significant differences were observed in self-perceived, rather than objectively measured, competencies. While these perceptions are educationally important, they require validation through longitudinal observation or behavioral assessment. Future multi-center studies with randomized designs, objective longitudinal assessments (eg., direct observation of communication, structured clinical reasoning tests), and economic analyses of implementation effort are warranted.
Conclusions
Within the context of a short-term PICU rotation, both peer teaching and flipped classroom models are feasible and effective educational strategies for achieving baseline knowledge and clinical performance objectives. More importantly, this comparative study reveals that each approach fosters a distinct profile of perceived competency development: peer teaching strongly enhances communication and confidence, while the flipped classroom robustly supports conceptual understanding and teamwork. These complementary profiles suggest that an integrated, blended educational approach, rather than a single model, may be optimal for addressing the multifaceted competency requirements of pediatric critical care training within time-constrained rotations.
Data Sharing Statement
The datasets generated during the current study are available from the corresponding author (Zhenjiang Bai) upon reasonable request.
Ethics Statement
Ethical approval was obtained from the Institutional Review Board of the Children’s Hospital of Soochow University (No. 2024CS196). The study was conducted in accordance with the Declaration of Helsinki. Participation was voluntary, and informed consent was obtained from all participants.
Funding
Design of the study and collection, analysis and interpretation of data by fund from Suzhou Science and Technology Development Project (SKY2023011, SYW2025015, SZXK202509). Writing the manuscript was supported by the Natural Science Foundation of Jiangsu Province (BK20251795,K2024061).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Chudgar SM, Cox CE, Que LG, et al. Current teaching and evaluation methods in critical care medicine: has the accreditation council for graduate medical education affected how we practice and teach in the intensive care unit? Crit Care Med. 2009;37:49–8. doi:10.1097/CCM.0b013e31819265c8
2. Servotte J-C, Bragard I, Szyld D, et al. Efficacy of a short role-play training on breaking bad news in the emergency department. West J Emerg Med. 2019;20:893–902. doi:10.5811//westjem.2019.8.43441
3. Van Keer R-L, Deschepper R, Huyghens L, Bilsen J. Challenges in delivering bad news in a multi-ethnic intensive care unit: an ethnographic study. Patient Educ Counseling. 2019;102(12):2199–2207. doi:10.1016/j.pec.2019.06.017
4. Smith KM, Geletta S, Duelfer K. Flipped classroom in podiatric medical education. J Ame Podiatric Med Assoc. 2020;110(5):
5. Chen F, Lui AM, Martinelli SM. A systematic review of the effectiveness of flipped classrooms in medical education. Med Educ. 2017;51(6):585–597. doi:10.1111/medu.13272
6. Li Y, Tang X-F, Cheng H. Application of a flipped classroom teaching model based on micro-videos in the standardized training of dermatological residents in China. Front Med. 2023;10:1250168. doi:10.3389/fmed.2023.1250168
7. Wu -Y-Y, Liu S, Man Q, et al. Application and evaluation of the flipped classroom based on micro-video class in pharmacology teaching. Front Public Health. 2022;10:838900. doi:10.3389/fpubh.2022.838900
8. Rose E, Claudius I, Tabatabai R, et al. The flipped classroom in emergency medicine using online videos with interpolated questions. J Emerg Med. 2016;51:284–291.e1. doi:10.1016/j.jemermed.2016.05.033
9. Choong R, Macauslan F. How to be involved in peer teaching. BMJ. 2020;368:l6897. doi:10.1136/bmj.l6897
10. Benè KL, Bergus G. When learners become teachers: a review of peer teaching in medical student education. Family Med. 2014;46(10):783–787.
11. Afshar M, Zarei A, Moghaddam MR, Shoorei H. Flipped and peer-assisted teaching: a new model in virtual anatomy education. BMC Med Educ. 2024;24(1):722. doi:10.1186/s12909-024-05697-4
12. Tonglin S, Yanqing W. Standardized training for resident doctors in China. J Biomed Res. 2014;28(3):155–156. doi:10.7555/JBR.28.20130181
13. CoBaTrICE Collaboration. The educational environment for training in intensive care medicine: structures, processes, outcomes and challenges in the European region. Intensive Care Med. 2009;35(9):1575–1583. doi:10.1007/s00134-009-1514-4
14. Blair RA, Caton JB, Hamnvik O-PR. A flipped classroom in graduate medical education. Clin Teacher. 2020;17(2):195–199. doi:10.1111/tct.13091
15. Barrios-Anderson A, Wu E, Liu DD, et al. A survey study examining the motivations, concerns, and perspectives of medical students engaging in neurosurgical research. Surg Neurol Int. 2021;12:490. doi:10.25259/SNI_742_2021
16. Salmi L-R, Côté P, Cedraschi C. Covering patient’s perspective in case-based critical review articles to improve shared decision making in complex cases. Health Expect Int J Public Particip Health Care Health Policy. 2020;23:1037–1044.
17. McEwen BS, Nasca C, Gray JD. Stress effects on neuronal structure: hippocampus, Amygdala, and prefrontal cortex. Neuropsychopharmacology. 2016;41(1):3–23. doi:10.1038/npp.2015.171
18. Cohen S, Alper CM, Doyle WJ, Treanor JJ, Turner RB. Positive emotional style predicts resistance to illness after experimental exposure to rhinovirus or influenza a virus. Psychosomatic Med. 2006;68(6):809–815. doi:10.1097/01.psy.0000245867.92364.3c
19. Chen Y-L, Chiu Y-W, Yu C-H, Chang Y-C, Chen Y-T. Flipped classroom teaching model with video instruction improves skills in local anesthesia training. Journal of Dental Sciences. 2024;19(2):1070–1074. doi:10.1016/j.jds.2024.02.001
20. Othman SA, Kamarudin Y, Sivarajan S, et al. Students’ perception on flipped classroom with formative assessment: a focus group study. Eur J Dent Educ off J Assoc Dent Educ Eur. 2023;27:419–427. doi:10.1111/eje.12823
21. Chan E, Botelho MG, Wong GTC, Sattar K. A flipped classroom, same-level peer-assisted learning approach to clinical skill teaching for medical students. PLoS One. 2021;16(10):e0258926. doi:10.1371/journal.pone.0258926
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Eyes for Ears: Usage and Efficacy of a Podcast for Ophthalmic Education
Pouw AE, Cai F, Redfern AJ, Chow J, Young BK
Clinical Ophthalmology 2023, 17:2163-2170
Published Date: 28 July 2023
Student Perceptions and Effectiveness of Video-Based Flipped Classroom for Improving Medical Physiology Teaching at AUSOM
Kottath Veetil P, Kollukkad Mani M, Arja SB, Paramban S, Kattambally PA, Fatteh R, Arja SB
Advances in Medical Education and Practice 2025, 16:1159-1167
Published Date: 3 July 2025
Integrating an Undergraduate Longitudinal POCUS Curriculum to Enhance Anatomy Learning: A Short Report
Goulet G, Dallaire G, Hadj-Mimoune S, Trépanier G
Advances in Medical Education and Practice 2026, 17:610429
Published Date: 29 May 2026