Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 16
A Cohort Study to Evaluate the Risk of Hospitalisation for Congestive Heart Failure Associated with the Use of Aclidinium and Other Chronic Obstructive Pulmonary Disease Medications in the UK Clinical Practice Research Datalink
Authors Rebordosa C, Plana E ![]() , Rubino A, Aguado J
, Rubino A, Aguado J ![]() , Lei A, Daoud S, Saigi-Morgui N
, Lei A, Daoud S, Saigi-Morgui N ![]() , Perez-Gutthann S
, Perez-Gutthann S ![]() , Rivero-Ferrer E
, Rivero-Ferrer E ![]()
Received 20 January 2021
Accepted for publication 9 May 2021
Published 31 May 2021 Volume 2021:16 Pages 1461—1475
DOI https://doi.org/10.2147/COPD.S301624
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Richard Russell
Cristina Rebordosa, 1 Estel Plana, 1 Annalisa Rubino, 2 Jaume Aguado, 1 Alejhandra Lei, 3 Sami Daoud, 4 Nuria Saigi-Morgui, 1 Susana Perez-Gutthann, 1 Elena Rivero-Ferrer 1
1RTI Health Solutions, Barcelona, Spain; 2Epidemiology, Respiratory and Immunology, AstraZeneca, Cambridge, UK; 3Patient Safety Biopharma, AstraZeneca, Barcelona, Spain; 4BioPharmaceuticals Research and Development, Late-Stage Development Research and Innovation, AstraZeneca, Gaithersburg, MD, USA
Correspondence: Cristina Rebordosa
RTI Health Solutions, Av. Diagonal, 605, 9-1, Barcelona, 08028, Spain
Tel +34 93 241 7766
Fax +34 93 760 8507
Email [email protected]
Background: The long-acting anticholinergic (LAMA) aclidinium was approved in Europe in 2012 to relieve symptoms in adults with chronic obstructive pulmonary disease (COPD). A Post-Authorisation Safety Study (PASS) was initiated to assess potential cardiovascular safety concerns for aclidinium.
Objective: To estimate the adjusted incidence rate ratio (IRR) for hospitalisation for heart failure in patients with COPD who were new users of aclidinium, tiotropium, other LAMA, long-acting beta-agonists/inhaled corticosteroids (LABA/ICS), and LAMA/LABA were compared with initiators of LABA.
Methods: This population-based cohort study included patients with COPD aged ≥ 40 years initiating COPD medications in the Clinical Practice Research Datalink (CPRD) GOLD in the United Kingdom from 2012 to 2017. Medications were identified via general practice prescriptions. The first-ever hospitalisations for heart failure were identified in the Hospital Episode Statistics, and general practitioner records from the CPRD. Poisson regression models were used to estimate the IRR for hospitalisation for heart failure in users of COPD medications versus LABA, adjusting for clinically relevant covariates.
Results: The study included 4350 new users of aclidinium, 23,405 of tiotropium, 6977 of other LAMAs, 3122 of LAMA/LABA, 26,093 of LABA/ICS, and 5678 of LABA. Mean age was 69– 70 years across medication groups. Aclidinium users had the highest proportion of severe COPD, and LABA users had the lowest (35% vs 19%, respectively). Crude incidence rates per 1000 person-years for the first-ever hospitalisation for heart failure ranged from 6.9 in LABA to 9.5 in aclidinium. Using LABA as reference, adjusted IRRs (95% confidence interval) for first-ever hospitalisation for heart failure were 0.90 (0.53– 1.53) for aclidinium, 1.02 (0.69– 1.51) for tiotropium, 0.86 (0.50– 1.47) for other LAMAs, 1.09 (0.41– 2.92) for LAMA/LABA, and 1.01 (0.69, 1.48) for LABA/ICS.
Conclusion: The study did not find increased risks of hospitalisations for heart failure in new users of aclidinium, tiotropium, other LAMAs, LAMA/LABA, and LABA/ICS compared with LABA.
Keywords: aclidinium, LAMA, heart failure, United Kingdom
Introduction
In July 2012, the inhaled long-acting anticholinergic (LAMA) Eklira/Bretaris Genuair (aclidinium bromide 322 µg twice daily; marketing authorisation holder: AstraZeneca AB, Södertälje, Sweden) was approved in the European Union for maintenance bronchodilator treatment to relieve symptoms in adult patients with chronic obstructive pulmonary disease (COPD).1 Long-acting anticholinergics are considered both effective and safe for the management of COPD and are recommended treatment in international clinical guidelines.2 Some studies have raised concerns about the cardiovascular safety of the LAMA treatments tiotropium and ipratropium bromide, although at the time of regulatory approval of aclidinium bromide in the European Union, this evidence was inconsistent.3–8
To further understand the safety of two LAMA treatments, Eklira (aclidinium bromide) and Duaklir (aclidinium bromide/formoterol fumarate dihydrate; marketing authorisation holder: AstraZeneca AB, Södertälje, Sweden), we initiated a Post-Authorisation Safety Study (PASS) using data from the Clinical Practice Research Datalink (CPRD) in the United Kingdom (UK) to assess the following cardiovascular safety concerns: all-cause mortality,9 heart failure, myocardial infarction, stroke, and arrhythmias. The PASS was registered at the EU PAS Register on 27 May 2016 with the registry identification number EUPAS13616 (http://www.encepp.eu/encepp/viewResource.htm?id=18823). Here, we report the results of a cohort study of patients with COPD in which we evaluated whether the use of aclidinium bromide is associated with an increased risk of hospitalisation for congestive heart failure.
The primary objective of this study was to compare the risk of first-ever hospitalisation for heart failure (ie, among patients without prior hospitalisation for heart failure) in patients with COPD initiating treatment with aclidinium bromide and other selected COPD medications with the risk of first-ever hospitalisation in patients with COPD initiating treatment with long-acting beta2-agonists (LABA) (primary endpoint). Additional analyses evaluated the risk of a first hospitalisation for heart failure during the study period among patients with or without prior hospitalisation for heart failure (secondary endpoint) and also the effect of duration of use on the risk of the primary endpoint.
Materials and Methods
Study Design Overview
This was a noninterventional, population-based cohort study of patients aged 40 years or older with a recorded diagnosis of COPD initiating treatment with aclidinium bromide monotherapy (Anatomical Therapeutic Chemical [ATC] code R03BB05) or other selected COPD medications identified in CPRD General Practitioner Online Database (CPRD GOLD), in the UK. Figure 1 depicts the study design and eligibility criteria for the study cohorts.
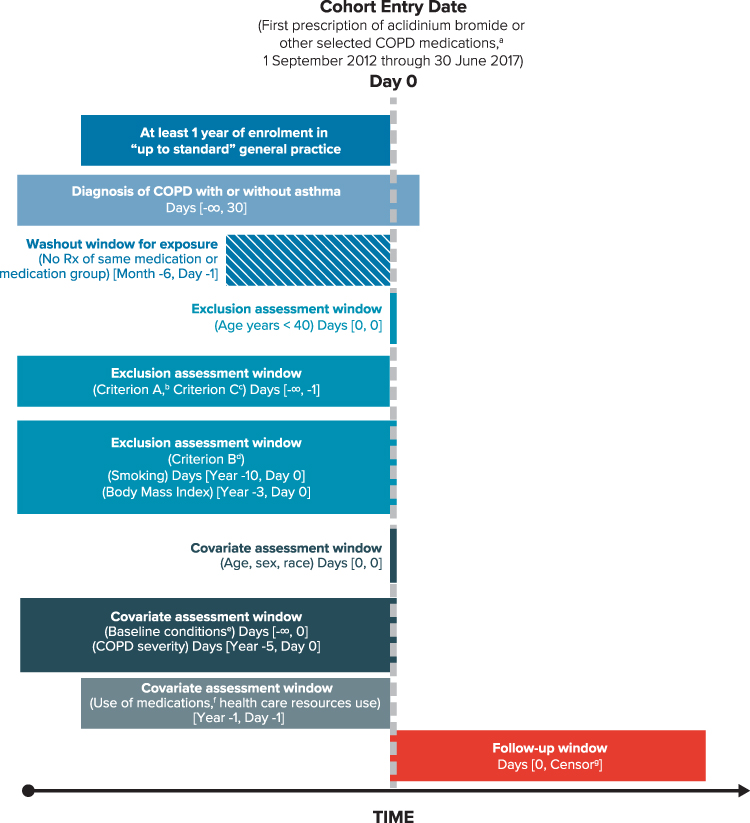 |
Figure 1 Overview of Study Design and Eligibility Criteria for the Study Cohorts. aOther COPD medications: tiotropium, other LAMA (glycopyrronium bromide, umeclidinium), LAMA/LABA (glycopyrronium/indacaterol, umeclidinium/vilanterol, and tiotropium/olodaterol), LABA (formoterol, salmeterol, indacaterol, olodaterol), and LABA/ICS (formoterol/budesonide, formoterol/beclometasone, formoterol/fluticasone, salmeterol/fluticasone propionate, vilanterol/fluticasone). bCriterion A: patients with any of the following non-cardiovascular, life-threatening conditions recorded in the database at any time before the start date: cancer, HIV (human immunodeficiency virus), respiratory failure, end-stage renal disease, organ transplant, drug or alcohol abuse, coma, or congenital anomalies. cCriterion C: prior history of hospitalisation for heart failure. dCriterion B: patients with missing information on smoking or body mass index. eChronic heart failure, causes of heart failure (ischaemic heart disease, cardiac valve disease, diseases of the myocardium, hypertension, other causes), diabetes, pulmonary embolism, asthma, hyperlipidaemia, anaemia, peripheral vascular disease, cerebrovascular diseases, stroke, transient ischaemic attack, renal disease, liver disorders. fRespiratory (SABA, oral glucocorticosteroids, mucolytics, antihistamines, ICS, SAMA, cough and cold preparations) and non-respiratory medications (antibiotics, cardiovascular medications, lipid-lowering drugs, antihypertensive medications, antiarrhythmics, nitrates, antidiabetics, and vaccines). gEarliest of outcome of interest (hospitalisation for heart failure), death, disenrollment from the practice, or end of the study period. Source: Original design diagram template can be found at www.repeatinitiative.org/projects.html. Abbreviations: COPD, chronic obstructive pulmonary disease; ICS, inhaled corticosteroid; LABA, long-acting beta2-agonist; LAMA, long-acting anticholinergic; Rx, prescription; SABA, short-acting beta2-agonist; SAMA, short-acting muscarinic antagonist. |
Setting
The study was conducted in the UK with data extracted from the CPRD GOLD, which includes patient-level medical records collected within the primary care setting. CPRD contains diagnostic and prescribing information recorded by general practitioners as part of routine clinical practice in the UK. The data source covers approximately 5 million individuals in the UK population, who are representative of the overall UK population in terms of age and sex. A large proportion of the CPRD practices are linkable with other health care data sets (eg, hospitalisation records and national mortality data) via the patient’s National Health Service number, sex, date of birth, and postal code. In the current study, information from the Hospital Episode Statistics (HES) database was used, as available, for a subset of practices where linkage was available. The validity of CPRD as a reliable data source for drug safety studies in numerous therapeutic areas is well established.10–13 The Independent Scientific Advisory Committee (ISAC) approved the protocol 17_070R on 28 June 2017.
Cohort Selection
Patients included in the study were new users of aclidinium bromide (monotherapy or in non–fixed-dose combination with formoterol or other medications) and new users of one of the following COPD medications: tiotropium, another LAMA (glycopyrronium bromide, umeclidinium), a LAMA/LABA combination (glycopyrronium/indacaterol, umeclidinium/vilanterol, and tiotropium/olodaterol), a LABA (formoterol, salmeterol, indacaterol, olodaterol), or a LABA/ICS combination (formoterol/budesonide, formoterol/beclometasone, formoterol/fluticasone, salmeterol/fluticasone propionate, and vilanterol/fluticasone). The start date was the date of the first prescription when all other eligibility criteria were met between 1 September 2012 and 30 June 2017 (inclusive).
Patients were included in the study if they met all the following criteria: (1) had been prescribed a study medication of interest during the study period, with no prescription of the same medication or medication group during the 6 months before the start date (new user); (2) had at least 1 year of enrolment in CPRD GOLD prior to the start date (only patients with permanent registration status in “up to standard” participating general practices were included in the cohort); (3) were aged 40 years or older at the start date; and (4) had a recorded diagnosis of COPD, with or without asthma, at any time before or up to 30 days after the start date. Diagnoses of COPD were identified through outpatient diagnoses recorded in CPRD GOLD (Read codes) or HES (International Classification of Diseases, Tenth Revision [ICD-10] codes J40-J44).
Patients were excluded if they had any of the following non-cardiovascular life-threatening conditions recorded in the database at any time before the start date: cancer, HIV (human immunodeficiency virus), dependence on a respirator, end-stage renal disease, organ transplant, drug or alcohol abuse, coma, or congenital anomalies. In addition, patients with missing information on smoking history or body mass index (BMI) before the start date were excluded.
Variables
Exposure, Time at Risk, and Ascertainment of Duration
Exposure to the study medications was ascertained using CPRD prescription records. Days’ supply was calculated from information on the prescription instructions and the quantity prescribed. For patients with missing information, imputation was conducted using the mode of days’ supply for each drug substance, strength, and quantity prescribed, when available.
Time at risk for the effects of each study medication was ascertained according to the days’ supply of each prescription plus a 7-day extension period. Episodes of continuous use were defined by consecutive prescriptions with a maximum gap of 7 days between the end of the days’ supply of one prescription and the start of the next prescription. An episode of continuous use ended at the end of follow-up or 7 days after the end of days’ supply of the earlier prescription when there was a gap of more than 7 days between prescriptions. The first episode of continuous use started at the start date. Current use, the main exposure of interest, was defined as the sum of all episodes of continuous use (and further classified into single or multiple study medication use).
Duration of use of each study medication was calculated as the total time of continuous use of that medication and was categorised as short duration (< 6 months) and long duration (≥ 6 months). Time at risk for long-duration use started after 6 months of use.
Congestive Heart Failure Endpoint
Congestive heart failure was defined as the first-ever hospitalisation for heart failure among patients without prior hospitalisation for heart failure (primary endpoint) and as the first hospitalisation for heart failure during the study period among patients with or without prior hospitalisation for heart failure (secondary endpoint). Although ascertainment of congestive heart failure can include both hospitalisations and outpatient diagnoses, it was anticipated that differential clinical diagnoses in patients with COPD might be an issue, especially for outpatient diagnoses. Therefore, we selected as a primary endpoint the most severe events requiring first-time hospitalisation, including patients with either a first-time diagnosis of congestive heart failure or a previous outpatient diagnosis of congestive heart failure who progressed to a more severe functional class requiring hospitalisation. Prior outpatient diagnoses of heart failure were taken into account in the analysis as a potential confounder and an analysis stratified by prior outpatient diagnoses of heart failure.
As a first step, hospitalisation for heart failure and dates of hospitalisation were identified and ascertained through adaptations of previously used electronic algorithms to detect heart failure.14 The following algorithm was used to ascertain potential cases according to availability of information: (1) for patients in practices linkable to the HES, (a) through HES primary discharge diagnosis code for acute heart failure or (b) through HES secondary discharge diagnosis code for acute heart failure; and (2) for patients in practices not linkable to HES, through CPRD GOLD Read codes plus hospitalisation, where hospitalisation or emergency department visit for heart failure were ascertained in the CPRD GOLD through outpatient codes (Read codes) for hospitalisation or emergency department visit within 30 days before or after the heart failure Read code date. Validation of the electronic algorithms to identify hospitalisation for heart failure was performed in two steps, as described in Supplemental Appendix A (see Figure A-1 and Tables A-1through A-4).
Covariates
Confounding factors were defined by diagnoses, procedures, and medication prescriptions recorded in either CPRD GOLD or HES data, measured before the start date (except concurrent use of medications). Confounding factors included age, sex, race/ethnicity, BMI, smoking history, socioeconomic status, health care utilisation, comorbidities, comedications, and severity of COPD (Figure 1). As in most studies using health data, we assumed that absence of a code for conditions or drug exposure was due to the absence of that condition or exposure. Classification of COPD severity was determined by using the GOLD 2016 definition15 (Table B-1, Supplemental Appendix B).
Statistical Analyses
Cohort attrition and patient characteristics were summarised descriptively. The number and percentage of cases of hospitalisation for heart failure (primary and secondary endpoints) identified and validated were calculated. Crude incidence rates and 95% confidence intervals (CIs) were estimated using the Poisson distribution. Crude and adjusted incidence rate ratios (IRRs) for hospitalisations of heart failure and 95% CIs for the effect of each study medication compared with LABA were estimated using Poisson regression models for overall, single, and multiple use of each study medication, as well as by duration of use. The confounders included in the final regression model were those considered clinically relevant or those that produced a change of 10% or more in the magnitude of the exposure coefficient estimated from the model comparing use of aclidinium versus use of LABA: age, sex, COPD severity, prior history of outpatient diagnosis of congestive heart failure, calendar period of the start date, asthma, ICS use, and diuretics use.
Crude and adjusted IRRs and 95% CIs for first-ever hospitalisation for heart failure were calculated for each study medication versus LABA and were stratified by the following patient characteristics of interest: COPD severity, age, history of asthma, history of an outpatient diagnosis of congestive heart failure, and histories of potential etiologies of heart failure. In addition, sensitivity analyses were conducted to explore the impact of the following: 1) extending the time window for definition of use from 7 days to 30 days; 2) restricting to patients eligible for linkage to HES; 3) restricting to cases confirmed after validation; and 4) adjusting by propensity score of aclidinium versus LABA deciles (before and after trimming at first percentile of aclidinium and 99th percentile of LABA).
Results
Cohort Characteristics
The primary endpoint cohort (without prior hospitalisation for heart failure) included a total of 4350 new users of aclidinium, 23,405 of tiotropium, 6977 of other LAMAs, 3132 of LAMA/LABA, 5678 of LABA, and 26,093 of LABA/ICS (Figure 2).
 |
Figure 2 Cohort Attrition for New Users of Aclidinium Bromide and Other Study Medications. aPercentages are row percentages. The rest of the percentages in figure are based on the total number of all users in each column. bEligibility criteria were assessed at each prescription recorded within the study period for each user of a study medication. A patient became eligible at the date of the first prescription of the study medication that fulfilled the eligibility criteria. For those patients not included in the cohort, the eligibility criteria were assessed through their last prescription within the study period. The most restrictive criterion was a 6-month prescription-free period prior to the start date; hence, the number of eligible patients is the same in both columns. cExclusion criterion A comprises cancer or other serious, non-cardiovascular life-threatening conditions or indicators of severe comorbidity recorded in the database at any time before the start date. Exclusion criterion B comprises missing data on smoking and body mass index (2.7% of the patient-cohort users).dExclusion criterion C is prior hospitalisation for heart failure recorded in the databases any time before the start date. Abbreviations: COPD, chronic obstructive pulmonary disease; ICS, inhaled corticosteroid; LABA, long-acting beta2-agonist; LAMA, long-acting anticholinergic. |
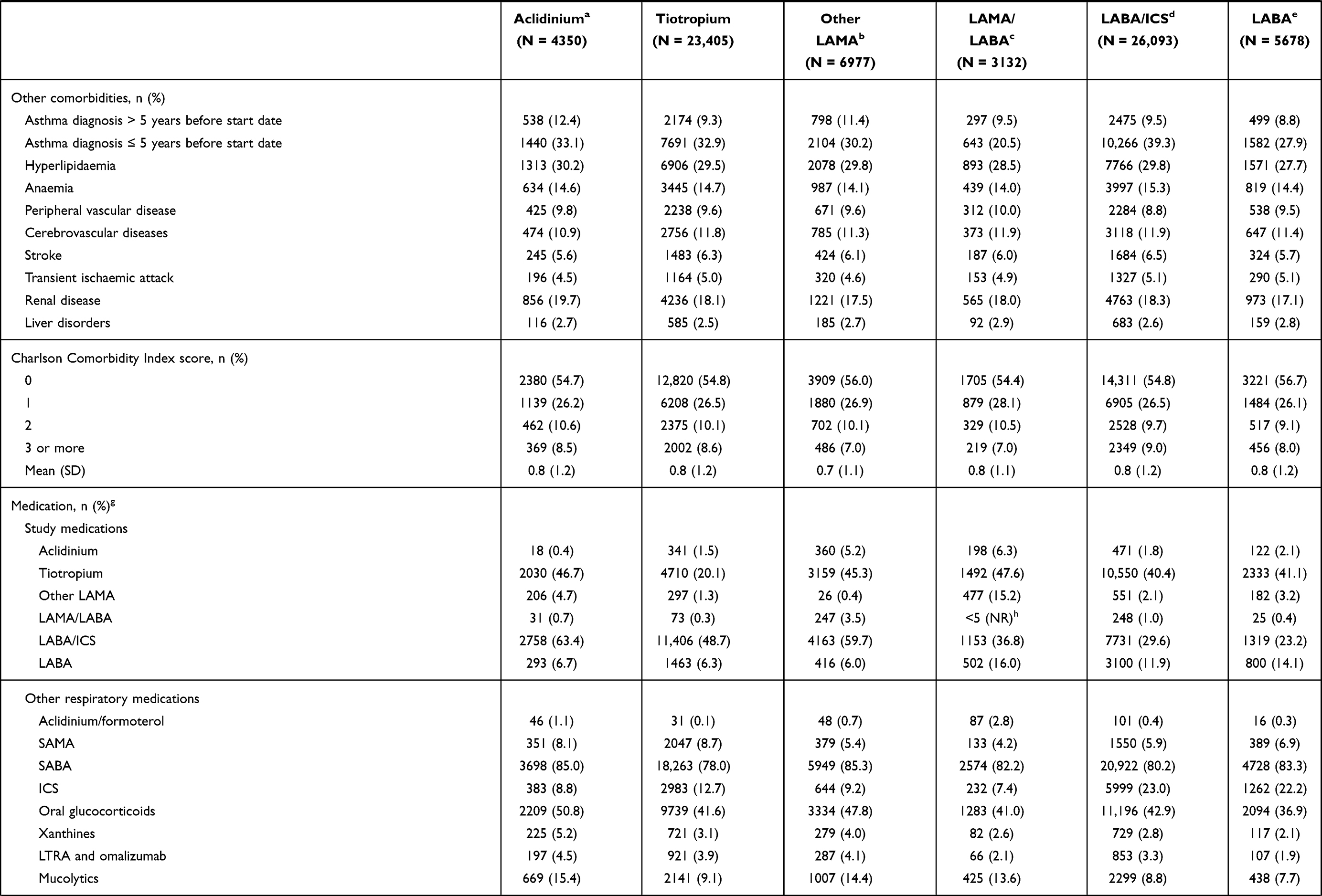
At baseline, mean age was 69 years for users of most study medication groups, except LAMA/LABA, where it was 70 years. Approximately half of the users were women, between 36% and 40% were current smokers, and one-third were obese (Table 1). Users of aclidinium had the highest frequency of more severe COPD (35.4% with GOLD D severity), followed by users of other LAMA (30.9%), while users of LABA had the highest frequency of less severe (GOLD A) COPD (38.8%), followed by users of LABA/ICS (35.0%). The proportion of patients with prior history of outpatient diagnosis of congestive heart failure was similar across study cohorts (range, 3.2–4.1%). Users of LABA/ICS had the highest frequency of a recorded diagnosis of asthma, while users of LAMA/LABA had the lowest frequency. The distribution of the Charlson Comorbidity Index score was similar across the study medication groups. Users of aclidinium, other LAMA, and LAMA/LABA had the highest frequency of previous use of all study medications and other respiratory medications, except ICS, the use of which was highest among users of LABA and of LABA/ICS. Users of aclidinium, other LAMA, and LAMA/LABA also had the highest frequency of referrals to a respiratory specialist.
 |
 |
 |
Table 1 Characteristics at the Start Date, by Study Medication, Among Patients Without Prior Hospitalisation for Heart Failure |
Congestive Heart Failure Endpoint
The number of hospitalisations for heart failure identified, validated, and confirmed is presented in Figure A-1 of Supplemental Appendix A.16 The electronic algorithm initially identified 2283 potential cases of heart failure during the study period.
Supplemental Appendix A presents the results of the validation in detail. Briefly, for the primary endpoint of first-ever hospitalisation for heart failure among patients without prior hospitalisation for heart failure, the positive predictive values (PPVs) were between 93.9% and 98.5% for cases identified through the HES primary diagnosis, 50.2% for cases identified through the HES secondary diagnosis, and 83.6% for cases identified through the CPRD GOLD Read code plus hospitalisation. Based on these PPVs, the main analysis included all cases identified through the HES primary diagnosis and CPRD GOLD Read code plus hospitalisation and only confirmed cases from those identified through an HES secondary diagnosis. A sensitivity analysis considering as cases only those that were confirmed after validation was conducted.
Incidence Rates and Incidence Rate Ratios of First Hospitalisation for Heart Failure
The highest crude incidence rates per 1000 person-years of first-ever hospitalisation for congestive heart failure (primary endpoint) were for new users of aclidinium (9.52; 95% CI, 6.66–13.17) and new users of LAMA/LABA (8.27; 95% CI, 4.41–14.15). New users of LABA had the lowest incidence rate per 1000 person-years (6.91; 95% CI, 4.66–9.87).
The adjusted IRRs for the first-ever hospitalisation of heart failure for use of each study medication versus the use of LABA are presented in Table 2. Use of aclidinium and other study medications showed no increased risk of first-ever hospitalisation for heart failure compared with use of LABA. Similarly, no increased risk was observed when comparing all study medications with aclidinium (Table C-1, Supplemental Appendix C). Incidence rate ratios for the secondary endpoint (first hospitalisation for heart failure during the study period) were similar to the IRRs for the primary endpoint (Table C-2, Supplemental Appendix C).
 |
Table 2 Crude Incidence Rate and Crude and Adjusted Incidence Rate Ratio for First-Ever Hospitalisation for Heart Failure Comparing Overall, Single, and Multiple Use of Each Study Medication with Use of Long-Acting Beta-Agonists Among Patients Without Prior Hospitalisation for Heart Failure |
Similarly, the risk of first-ever hospitalisation for heart failure for single use or multiple use of any of the study medications did not differ with the risk for single use of LABA. The adjusted IRRs (95% CI) for first-ever hospitalisation of heart failure for both single and multiple use of study medications versus single use of LABA were, in general, lower than the IRRs for overall use (Table 2), ranging from 0.21 (0.02, 1.93) for multiple use of LAMA/LABA to 0.90 (0.54, 1.47) for multiple use of LABA/ICS. The number of events among single users was low for all study medications except for tiotropium and LABA/ICS.
After adjustment, no increased risk of first-ever hospitalisation for heart failure was observed for short duration of use of any of the study medications compared with the short duration of use of LABA. A decreased risk of first-ever hospitalisation for heart failure was observed for a short duration of use of other LAMAs compared with a short duration of use of LABA (IRR, 0.39; 95% CI, 0.17–0.88), although this finding was based on only 14 cases. Long duration use of the study medications compared with long duration of use of LABA showed higher risks of first-ever hospitalisation for heart failure (Table C-3, Supplemental Appendix C). Incidence rates for short and long duration use of the study medications ranged from 4.64 per 1000 person-years for long-duration use of LABA to 10.40 per 1000 person-years for short-duration use of aclidinium. Except for long-duration use of other LAMAs, incidence rates were higher for short duration of use than for use overall and long duration of use.
Subgroup and Sensitivity Analyses
Incidence rate ratios of first-ever hospitalisation for heart failure (primary endpoint) for each study medication versus use of LABA were estimated by categories of COPD severity, age, history of asthma, history of outpatient diagnosis of heart failure, and history of potential aetiologies of heart failure. Additionally, IRRs were also estimated (1) among patients with available linkage to HES and (2) including only cases that were confirmed. In general, IRRs were similar across subgroups, with some variations (Figure 3). No association between use of any study medication and first-ever hospitalisation for heart failure compared with use of LABA was observed for any of the subgroups. For use of all the study medications compared with use of LABA, the magnitude of the estimates was generally higher among patients in GOLD 2016 COPD severity categories A and B, younger patients, patients without asthma, patients without prior history of outpatient heart failure, and patients with valvular disease. In the complementary subgroups, ie, patients with COPD GOLD C or D severity categories, older patients, patients with asthma, patients with prior history of outpatient heart failure, and patients with other causes of heart failure, the risk estimates were lower when compared with LABA users. For several subgroups, the precision of effect estimates was low due to the low number of cases.
 |
Figure 3 Subgroup and Sensitivity Analysis: Use of Study Medications Versus Use of LABA. aAll the models were adjusted by age, sex, COPD severity, prior outpatient diagnosis of congestive heart failure, diuretic use, ICS use, asthma, and calendar year at start date, unless one of these variables was used for stratification. bAs measured through GOLD 2016 severity categories at the start date. cWith current asthma (ie, at least one asthma diagnosis recorded within 5 years before the start date). Abbreviations: CI, confidence interval; COPD, chronic obstructive pulmonary disease; GOLD, Global Initiative for Chronic Obstructive Lung Disease; HES, Hospital Episode Statistics; ICS, inhaled corticosteroid; IRR, incidence rate ratio; LABA, long-acting beta2-agonist; LAMA, long-acting anticholinergic. |
The results were also consistent across sensitivity analyses (Figure 3). In the analysis extending the duration of exposure to 30 days, for all the study medications, IRRs for first-ever hospitalisation for heart failure were similar to those obtained in the main analysis. The sensitivity analysis that was based on only confirmed cases after validation resulted in IRRs for the first-ever hospitalisation for heart failure similar to the IRRs obtained in the main analysis for all the study medications (ie, no association was found for any of the study medications), although the magnitude of the point estimates was slightly higher and the 95% CIs wider. Finally, in the sensitivity analysis adjusted for the propensity score deciles, the IRR for first-ever hospitalisation for heart failure for users of aclidinium compared with users of LABA (IRR, 0.86; 95% CI, 0.50–1.48) was similar to the risk estimate and 95% CI observed for the main analysis. After trimming, the propensity score adjusted IRR was closer to the null (IRR, 1.04; 95% CI, 0.58–1.85).
Discussion
This is an observational study on hospitalisation for congestive heart failure risk among patients representative of the real-world population of COPD patients initiating COPD maintenance medications. In this study conducted in patients with COPD aged 40 years or older in general practices in the UK, no increased risk of hospitalisation for heart failure was observed for use of aclidinium, tiotropium, other LAMAs, LAMA/LABA, or LABA/ICS compared with use of LABA. Although many patients were concomitant users of more than one of the study medications, no increased risk of hospitalisation for heart failure was observed when restricting the analysis to single users of the study medications. In general, results were similar across categories of COPD severity, age, history of asthma, history of outpatient congestive heart failure, and across potential aetiologies of heart failure.
New users of LABA had the lowest incidence rates of first-ever hospitalisation for heart failure. The higher incidence rates observed among short duration of use of LABA suggest that confounding by indication, whereby the indication for an exposure has an impact on the outcome of interest, could have a role in the reduced relative risk estimates of hospitalisation for heart failure observed for use of aclidinium and the other study medications compared with use of LABA. Alternative definitions of duration of exposure and restriction of analysis to confirmed cases or to patients with linkage to HES did not affect the study results. In the sensitivity analysis by duration of use, long duration (6 months or more) of use of all the study medications showed an increased risk of first-ever hospitalisation for heart failure compared with long duration of use of LABA, while short-term duration of use of all study medications showed a decreased risk of first-ever hospitalisation for heart failure compared with short duration of use of LABA. The reason for these findings may be reduced comparability of the cohorts when stratifying by duration of use, as shown in a post hoc descriptive review of long- and short-term users of aclidinium and LABA (Table C-4, Supplemental Appendix C). This evaluation showed that long-term users of aclidinium were sicker patients, with a higher Charlson Comorbidity Index score, a higher proportion of patients with prior chronic congestive heart failure, more severe COPD, more prior use of oral corticosteroids, and less prior use of beta-blockers than long-term users of LABA.
Taken together, results from this study do not support an increased risk of hospitalisation for congestive heart failure among patients with COPD treated with aclidinium, tiotropium, other LAMAs, LAMA/LABA, or LABA/ICS when compared with patients with COPD treated with LABA. There were no differences between the primary and secondary endpoints analyses, possibly because of the low number of patients that differed between these two groups. Overall, the study results were consistent across subgroups and sensitivity analyses. The small differences in the risks observed in the analysis stratified by subgroups of patients may be explained by random variability from the low number of events and unmeasured confounding.
Results of this non-interventional study are consistent with previous studies performed among users of tiotropium. In a study conducted in the Netherlands using data from the Integrated Primary Care Information database, the IRR for heart failure for tiotropium versus LABA was 1.06 (95% CI, 0.53–2.10).8 A similar IRR (0.85; 95% CI, 0.63–1.14) was observed in a study conducted by The Health Improvement Network in the UK.5
Use of bronchodilators (LABA or LAMA) has been shown to be a predictor of worsening of heart failure in a broad spectrum of patients with heart failure.17–19 However, it is not clear if this association could be attributed to confounding by indication and the severity of the underlying lung disease. While a study evaluating whether the risk of heart failure after adding one bronchodilator (LAMA or LABA) to patients on monotherapy (LABA or LAMA) led to a mild increase in the risk of heart failure, the authors noted that this was not due to events occurring soon after the addition of the second bronchodilator and that the increased risk could have been due to potential protopathic bias from a recent prescription for a bronchodilator given for dyspnoea related to early stages of myocardial dysfunction rather than a worsening of COPD.20 On the other hand, studies evaluating intense ICS-containing therapy, particularly triple combination therapy, showed a reduction in the risk of all-cause mortality. Although there are studies showing a relationship between exacerbations and coronary events,21,22 reduction in all-cause mortality could not be completely attributed to a reduced risk of exacerbations, and when deaths were adjudicated, these were most frequently due to cardiovascular causes.23–26 These findings suggest that the increased risk of worsening of heart failure observed among users of bronchodilators compared with non-users is more likely to be related to the underlying pulmonary disease than to an effect of the medications. This is further supported by the results from the current study where, despite users of LABA having less severe COPD and having the lowest incidence rate of hospitalisations for heart failure than aclidinium users, users of other study medications did not have an increased risk of hospitalisations for heart failure when compared with LABA and after the analysis was adjusted for COPD severity.
The results of this study should be considered in view of several limitations. Although the precision of the study was sufficient to assess the risk of hospitalisation for heart failure associated with use of the study medications, the precision of the IRRs for several of the subgroup analyses was low and based on a low number of events. Moreover, as mentioned previously, confounding by indication could have driven reduced risk estimates of hospitalisation for heart failure among users of aclidinium and other study medications compared with LABA users. Analyses before and after trimming the patients in the extreme percentiles of the distribution of the propensity score showed that the adjusted IRRs before trimming did not differ from those in the main analysis, suggesting that the relevant variables were included in the Poisson regression model. After trimming, the results were closer to the null, suggesting that the trimmed population may be driving differences in the IRRs for study medications when compared with LABA in some subanalyses. It should be noted that COPD severity may change over time, as prognosis of COPD depends on the complex interaction between genetic and environmental risk factors.2 Also, newly approved drugs for COPD may be more frequently prescribed to patients with more severe COPD or comorbidity or to patients not adequately controlled with available medications, as found for LAMAs in this study. There is evidence that selective prescribing of newly marketed drugs may attenuate over time. In a study conducted in the UK, COPD severity was higher among patients prescribed tiotropium soon after approval than 10 to 15 months later.4 Finally, this study was conducted using health information recorded in automated, population-based databases. An advantage of these data sources is that the data are collected from routine health care without interfering with regular clinical practice. However, there are some limitations, including the potential for misclassification of exposure and outcome, which were minimal in this study (except for cases identified by the HES secondary algorithm).
Conclusions
Results from this observational study conducted in patients with COPD in the UK indicate that the use of aclidinium, tiotropium, other LAMAs, LAMA/LABA, and LABA/ICS compared with the use of LABA is not associated with an increased risk of hospitalisation for heart failure. The ongoing cardiovascular PASS programme, with the next substudies evaluating stroke, myocardial infarction, and arrhythmias, will provide further insight into the cardiovascular safety of aclidinium and other COPD medications.
Abbreviations
BMI, body mass index; CI, confidence interval; COPD, chronic obstructive pulmonary disease; CPRD, Clinical Practice Research Datalink; EU, European Union; HES, Hospital Episode Statistics; HIV, human immunodeficiency virus; ICD-10, International Classification of Diseases, Tenth Revision; ICS, inhaled corticosteroid; IRR, incidence rate ratio; ISAC, Independent Scientific Advisory Committee; LABA, long-acting beta-agonists; LAMA, long-acting anticholinergic; MHRA, Medicines and Healthcare products Regulatory Agency; PASS, Post-Authorisation Safety Study; PPV, positive predictive value; UK, United Kingdom.
Data Sharing Statement
This study is based on data from the Clinical Practice Research Datalink obtained under licence from the UK Medicines and Healthcare products Regulatory Agency. The data are provided by patients and collected by the NHS as part of their care and support. The interpretation and conclusions contained in this study are those of the author/s alone. Copyright © (2018), re-used with the permission of The Health & Social Care Information Centre. All rights are reserved.
Data access is available and subject to a license agreement that contains terms and conditions of use set forth by the United Kingdom Medicines & Healthcare Products Regulatory Agency. Clinical Practice Research Datalink´s website: https://www.cprd.com/home/. Enquiries about data access can be directed to: [email protected], or +44 (0)20 3080 6383.
Ethics Approval and Informed Consent
The study was approved by the Independent Scientific Advisory Committee (ISAC) for the Medicines and Healthcare products Regulatory Agency (MHRA) 28 June 2017 (protocol 17_070RA). All data accessed comply with relevant data protection and privacy regulations.
Acknowledgments
Bettina T Blak (AZ) for data extraction; Esther García Gil (AZ) for protocol design; Javier Nuevo (AZ) for operational oversight; Jordi Castellsague (RTI-HS) and Cristina Varas (RTI-HS) for scientific and clinical contributions; Christine Bui for project management and outcome validation support; Kate Lothman and John Forbes (RTI-HS) for manuscript editing; and Emily Gill (RTI-HS) for graphic design. The abstract of this paper was presented, in part, at the 35th ICPE International Conference on Pharmacoepidemiology & Therapeutic Risk Management; August 28, 2019; Philadelphia, Pennsylvania. The poster’s abstract was published, as follows: Plana E, Rivero-Ferrer E, Aguado J, Saigi-Morgui N, Nuevo J, Daoud SZ, Lei A, Perez-Gutthann S, Rebordosa C. Hospitalization for heart failure among patients using aclidinium bromide and other COPD medications: a post-authorisation safety study in the CPRD. Poster presented at the 35th ICPE International Conference on Pharmacoepidemiology & Therapeutic Risk Management; August 28, 2019; Philadelphia, Pennsylvania. [abstract] Pharmacoepidemiol Drug Saf. 2019 Aug 20; 28(S2):1153.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval for the version to be published; have agreed on the journal to which the article has been submitted; and agreed to be accountable for the content of the article.
Funding
This study was performed under a research contract between RTI Health Solutions (RTI-HS) and AstraZeneca and was funded by AstraZeneca. The contracts provide the research team independent publication rights. The sponsors had no role in the data collection or analysis; however, in line with the Guideline on Good Pharmacovigilance Practices: Module VIII: Post-authorisation Safety Studies of the European Medicines Agency, the sponsors had the opportunity to view the results and interpretations included in the manuscript and provide comments before submission of the manuscript for publication.
Disclosure
CR, EP, JA, NSM, SPG, and ERF are salaried employees of RTI Health Solutions, a nonprofit research organisation that conducts research with multiple pharmaceutical companies and has an independent right to publish the results of this study. AR is an employee of BioPharmaceuticals R&D, AstraZeneca, Cambridge, United Kingdom. AL is an employee of BioPharmaceuticals R&D, AstraZeneca, Barcelona, Spain. SD is an employee of BioPharmaceuticals R&D, AstraZeneca, Gaithersburg, Maryland, United States. The authors report no other conflicts of interest in this work.
References
1. EMA. Summary of opinion (initial authorisation). Eklira Genuair: aclidinium bromide. European Medicines Agency, Committee for Medicinal Products for Human Use; May 24, 2012. Available from: http://www.ema.europa.eu/docs/en_GB/document_library/Summary_of_opinion_-_Initial_authorisation/human/002211/WC500127779.pdf.
2. GOLD. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease (2020 report). Global Initiative for Chronic Obstructive Lung Disease; 2020. Available from: http://goldcopd.org/gold-reports/.
3. de Luise C, Lanes SF, Jacobsen J, Pedersen L, Sørensen HT. Cardiovascular and respiratory hospitalizations and mortality among users of tiotropium in Denmark. Eur J Epidemiol. 2007;22(4):267–272. doi:10.1007/s10654-007-9106-5
4. Jara M, Lanes SF, Wentworth C
5. Jara M, Wentworth C
6. Macie C, Wooldrage K, Manfreda J, Anthonisen N. Cardiovascular morbidity and the use of inhaled bronchodilators. Int J Chron Obstruct Pulmon Dis. 2008;3(1):163–169. doi:10.2147/COPD.S1516
7. Ogale SS, Lee TA, Au DH, Boudreau DM, Sullivan SD. Cardiovascular events associated with ipratropium bromide in COPD. Chest. 2010;137(1):13–19. doi:10.1378/chest.08-2367
8. Verhamme KM, Afonso AS, van Noord C, et al. Tiotropium Handihaler and the risk of cardio- or cerebrovascular events and mortality in patients with COPD. Pulm Pharmacol Ther. 2012;25(1):19–26. doi:10.1016/j.pupt.2011.10.004
9. Rebordosa C, Aguado J, Plana E, et al. Use of aclidinium did not increase the risk of death in a noninterventional cohort study in the Clinical Practice Research Datalink (CPRD), United Kingdom. Respir Med. 2019;152:37–43. doi:10.1016/j.rmed.2019.04.018
10. Jick H, Jick SS, Derby LE. Validation of information recorded on general practitioner based computerised data resource in the United Kingdom. BMJ. 1991;302(6779):766–768.
11. Jick SS, Kaye JA, Vasilakis-Scaramozza C, et al. Validity of the General Practice Research Database. Pharmacotherapy. 2003;23(5):686–689. doi:10.1592/phco.23.5.686.32205
12. Herrett E, Thomas SL, Schoonen WM, Smeeth L, Hall AJ. Validation and validity of diagnoses in the General Practice Research Database: a systematic review. Br J Clin Pharmacol. 2010;69(1):4–14. doi:10.1111/j.1365-2125.2009.03537.x
13. Herrett E, Gallagher AM, Bhaskaran K, et al. Data resource profile: clinical Practice Research Datalink (CPRD). Int J Epidemiol. 2015;44(3):827–836. doi:10.1093/ije/dyv098
14. Saczynski J, Andrade S, Harrold L, et al. Mini-sentinel systematic evaluation of health outcome of interest definitions for studies using administrative and claims data. Pharmacoepidemiol Drug Saf. 2012;21(S1):129–140. doi:10.1002/pds.2313
15. Rebordosa C, Plana E, Aguado J, et al. GOLD assessment of COPD severity in the Clinical Practice Research Datalink (CPRD). Pharmacoepidemiol Drug Saf. 2019;28(2):126–133
16. Saigi N, Rebordosa C, Bui C, et al. A validation exercise: identifying hospitalizations for heart failure among patients with COPD in the CPRD. Poster presented at the 35th ICPE International Conference on Pharmacoepidemiology & Therapeutic Risk Management; August 26, 2019. Philadelphia, PA [abstract]. Pharmacoepidemiol Drug Saf. 2019;28(S2):334.
17. Au DH, Udris EM, Fan VS, Curtis JR, McDonell MB, Fihn SD. Risk of mortality and heart failure exacerbations associated with inhaled beta-adrenoceptor agonists among patients with known left ventricular systolic dysfunction. Chest. 2003;123:1964–1969. doi:10.1378/chest.123.6.1964
18. Au DH, Udris EM, Curtis JR, McDonell MB, Fihn SD. Association between chronic heart failure and inhaled beta-2-adrenoceptor agonists. Am Heart J. 2004;148:915–920. doi:10.1016/j.ahj.2004.03.048
19. Hawkins NM, Wang D, Petrie MC, et al. Baseline characteristics and outcomes of patients with heart failure receiving bronchodilators in the CHARM programme. Eur J Heart Fail. 2010;12(6):557–565. doi:10.1093/eurjhf/hfq040
20. Suissa S, Dell’Aniello S, Ernst P. Concurrent use of long-acting bronchodilators in COPD and the risk of adverse cardiovascular events. Eur Respir J. 2017;49(5):1602245. doi:10.1183/13993003.02245-2016
21. Donaldson GC, Hurst JR, Smith CJ, Hubbard RB, Wedzicha JA. Increased risk of myocardial infarction and stroke following exacerbation of COPD. Chest. 2010;137(5):1091–1097. doi:10.1378/chest.09-2029
22. Kunisaki KM, Dransfield MT, Anderson JA, et al. Exacerbations of chronic obstructive pulmonary disease and cardiac events: a cohort analysis. Am J Respir Crit Care Med. 2018;198(1):51–57. doi:10.1164/rccm.201711-2239OC
23. Martinez FJ, Rabe KF, Ferguson GT, et al. Reduced all-cause mortality in the ETHOS trial of budesonide/glycopyrrolate/formoterol for chronic obstructive pulmonary disease. a randomized, double-blind, multicenter, parallel-group study. Am J Respir Crit Care Med. 2021;203(5):553–564. doi:10.1164/rccm.202006-2618OC
24. Lipson DA, Crim C, Criner GJ, et al. Reduction in all-cause mortality with fluticasone furoate/umeclidinium/vilanterol in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2020;201(12):1508–1516. doi:10.1164/rccm.201911-2207OC
25. Andreas S, Taube C. Inhaled therapy reduces COPD mortality. ERJ Open Res. 2020;6(4):00634–2020. doi:10.1183/23120541.00634-2020
26. Vestbo J, Fabbri L, Papi A, et al. Inhaled corticosteroid containing combinations and mortality in COPD. Eur Respir J. 2018;52(6):1801230. doi:10.1183/13993003.01230-2018
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.