Back to Journals » International Journal of Women's Health » Volume 18
A CFIR-Guided Qualitative Process Evaluation of a Health Insurance-Based Lifestyle Counseling Intervention During Pregnancy in Germany
Authors Litke NA, Ullrich C, Wohlhüter L, Wensing M ![]() , Bombana M
, Bombana M
Received 10 January 2026
Accepted for publication 28 March 2026
Published 22 April 2026 Volume 2026:18 595070
DOI https://doi.org/10.2147/IJWH.S595070
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 6
Editor who approved publication: Dr Matteo Frigerio
Nicola Alexandra Litke,1 Charlotte Ullrich,1 Laura Wohlhüter,2 Michel Wensing,1 Manuela Bombana1,3
1Department of General Practice and Health Services Research, Heidelberg University, Heidelberg, Germany; 2Science Management, German Cancer Research Center (DKFZ), Heidelberg, Germany; 3Department for Prevention, AOK Baden-Württemberg, Stuttgart, Germany
Correspondence: Manuela Bombana, Department of General Practice and Health Services Research, Heidelberg University, Heidelberg, Germany, Email [email protected]
Purpose: In Germany, knowledge of pregnant women as well as standards for health workers to conduct consultations on lifestyle-related risk factors (LRRFs) are suboptimal. This study aimed to identify factors influencing implementation of the “AOK Family Happiness Plus”, a counselling intervention for LRRFs during pregnancy within a health insurance setting.
Patients and Methods: This process evaluation included semi-structured interviews and a focus group with n = 16 consultants involved in delivering the intervention. Interviews lasted approximately 30– 60 minutes. Interviews were conducted in autumn 2023 during and the focus group at the end of the intervention phase, in summer 2024. Data were analysed using thematic analysis using the Consolidated Framework for Implementation Research (CFIR).
Results: Consultants highlighted the perceived benefits of the one-on-one counselling format including the four main topics of LRRF prevention during pregnancy: healthy diet, physical exercise, alcohol and tobacco use, and mental health. A strong alignment with existing prevention activities within the health insurance setting was noticed, while recruitment challenges and technical barriers in digital consultations were reported. Consultants mainly saw themselves in the role of innovation deliverers with strong self-efficacy and high capability. The involvement of gynaecologists and midwives was perceived as crucial for engaging innovation participants. Participating pregnant women were largely described as having prior knowledge of LRRF prevention. Consultants perceived that the consultation contributed to improving participants’ understanding of LRRFs during pregnancy. The intervention deliverers faced significant obstacles, including technical difficulties and recruitment issues. Suggested adaptations included the introduction of group and online formats and including postnatal follow-up.
Conclusion: The findings suggest that lifestyle counselling during pregnancy can be implemented within a health insurance setting, while highlighting important implementation challenges and contextual determinants. However, the findings reflect the perspectives of consultants delivering the intervention and should therefore be interpreted with caution. Future research should examine its effectiveness.
Keywords: risk factors, pregnancy, behaviour change, consultation, primary prevention, health literacy
Introduction
The World Health Organization (WHO) highlighted the importance of a positive pregnancy experience and the prevention of risk factors.1 For improving antenatal care, Lifestyle-Related Risk Factors (LRRFs) such as physical inactivity, poor diet and tobacco, and alcohol consumption are addressed directly. LRRFs influence not only maternal health but also the health of the (unborn) child and pregnancy outcomes: Nutrition-related risk factors contribute to a high risk for ischemic and hypertensive heart diseases and diabetes. Iron deficiency increases the risk for maternal diseases by 17%.2 Maternal smoking during pregnancy doubles the risk for sudden infant death and increases the risk of stillbirth by 23%. Even second-hand smoke increases the risk of stillbirth and having a low-birth-weight baby.3 However, according to a recent meta-analysis, 9.8% of pregnant women worldwide consume alcohol and the global prevalence of smoking during pregnancy was estimated 1.7% with the European Region as the area with the highest prevalence (8,7%).4,5 In Germany, 14% of mothers report alcohol consumption during pregnancy, whereas smoking rates among pregnant women range from 10.9% to 17–18%.6,7 Although data on alcohol and tobacco consumption were collected in the early 2000s, until then, no significant trend over time could be measured.6 This finding is supported by a recent study identifying a lack of knowledge regarding the harmful effects of alcohol and tobacco use during pregnancy among German women.8 Additionally, more than 20% of expectant mothers in Germany are classified as overweight at the beginning of pregnancy, resulting in increased birth weights of their children.6 Considering these challenges, it is crucial to promote behavioural changes and encourage a healthy lifestyle during pregnancy to improve maternal health and pregnancy outcomes.9,10 This includes fostering a balanced diet, reducing tobacco and alcohol use, and enhancing physical activity and mental well-being.
For Germany, an evidence-based guideline for preventing LRRFs during pregnancy has been published.11 Still, there is a lack of standardized protocols for care providers, such as midwives or gynaecologists, to effectively transfer this health knowledge and conduct consultations regarding LRRFs.12 Within the national prevention guide, health insurances are obligated to offer courses addressing the respective four topics of LRRFs.13 Until now, no intervention studies conducted by health insurances in Germany regarding LRRF prevention in pregnancy could be identified.
To address these issues, the public health insurance company AOK Baden-Wurttemberg (AOK BW) and the University Hospital of Heidelberg, Germany, have developed a consultation aimed at enhancing pregnancy-related health literacy and promoting healthier behaviours: the “AOK-Family Happiness Plus for Individual Prevention and Strengthening of Resources in Pregnancy and Optimization of Education in Gynaecological Care” (AOK-Family +) programme.14 The study intervention consists of a one-hour one-on-one (analogue or digital) consultation delivered by consultants who have a background as prevention experts (regarding nutrition, physical exercise, or mental health) and are located in health centres in southwestern Germany, managed by the insurance company AOK BW.14
Internationally, several antenatal lifestyle counselling programs have been implemented to address behavioural risk factors during pregnancy.15–17 However, evidence on the implementation of such interventions within statutory health insurance systems remains limited. Therefore, examining the implementation of a structured lifestyle counselling intervention within the German health insurance setting provides valuable insights into organisational and contextual determinants of preventive services in maternal health. Within the German health care system, statutory health insurance providers play an important role in delivering preventive health services under the national Prevention Act (§20 SGB V). This creates a unique opportunity to implement structured counselling programs addressing lifestyle-related risk factors during pregnancy within an established prevention infrastructure. Therefore, evaluating the implementation of such interventions in the health insurance setting is particularly relevant for understanding how prevention strategies can be integrated into routine care. The AOK-Family+ study was accompanied by evaluation research, including a process evaluation, which is reported below. Process evaluations are increasingly recommended alongside effectiveness trials to understand how complex interventions are implemented in real-world settings and which contextual factors influence their success or failure. While randomized controlled trials primarily assess intervention effectiveness, process evaluations provide insights into context and mechanisms of intervention and implementation.18 The Consolidated Framework for Implementation Research (CFIR)19,20 provides a comprehensive framework to analyse determinants of implementation across intervention characteristics, organisational contexts, individuals involved, and the implementation process.
The aim of this study was to conduct a qualitative process evaluation to identify factors influencing the implementation of the lifestyle counselling intervention during pregnancy.
Material and Methods
Study Design
For the process evaluation, a qualitative descriptive study design was applied, including semi-structured interviews and a focus group with consultants delivering the intervention. The interviews took place during the intervention, in September and October 2023. The focus group was conducted at the end of the intervention phase in June 2024. The study was conducted in accordance with the Declaration of Helsinki in its current version. The study was approved by the Ethics Committee of the Medical Faculty of Heidelberg University. All participants provided written informed consent prior to data collection, including consent for the publication of anonymized responses and direct quotations. The study was reported according to the Consolidated Criteria for Reporting Qualitative Research (COREQ) checklist (Supplementary File 1).21
Study Setting
A broad description of the intervention and its components is shown in Figure 1.
The intervention consisted of an hourlong consultation for pregnant women or preconception women who were informed about LRRFs during pregnancy. The consultation included four main topics: (a) health-promoting nutrition; (b) physical exercise; (c) mental health; and (d) the consumption of alcohol, drugs, and tobacco during pregnancy. All women received an information brochure that provided an overview and summarized the main guidelines. The consultation was performed in person or via online meetings, depending on the respective study arm via consultants in health centres of AOK BW. Within the south-western region of Baden-Wurttemberg, the AOK BW manages 46 health centres in 14 districts including prevention experts conducting courses and consultations in nutrition, physical exercise, and mental health. Prior to the intervention phase, health centres were cluster randomized in the analogue consultation, digital consultation, or control group on district level. This cluster randomization of health centres also included the respective consultants. All consultants received a digital interactive interview guideline to base the consultation on. Four short expert videos on the main topics were developed and integrated into the consultations. Furthermore, every consultant took part in on-demand training via e-learning. The consultants who conducted the digital consultations also received training and technical equipment in this regard. All consultants were employed by AOK BW, Germany, as prevention specialists situated in AOK health centres.
Participants and Recruitment
For the process evaluation, all 40 consultants who participated in the intervention study were invited. Semi-structured interviews and a focus group were conducted with consultants delivering the intervention. This included all consultants who performed digital or analogue consultations within the study. All consultants were contacted via e-mail. When they expressed their interest in their participation, a study information sheet was sent via mail. Prior to the interview and focus group, all participants were asked to fill out a short questionnaire regarding their sociodemographic background and a form of consent. For participation in the focus group specifically, consultants who had already participated in a previous interview were excluded.
Data Collection
The interview guide was developed by two female health services researchers (NL and LW) who were in close exchange within the research team (MB, CU, and MW) and additional colleagues conducting three consent meetings. The interview guideline included open questions regarding (a) the setting of the AOK BW health centres; (b) previous experiences with prevention courses and consultations; (c) aspects influencing implementation, such as training of the consultants; (d) technical implementation; (e) organizational and thematic compatibility; and (f) potential for intervention adaptation (Supplementary File 2).
The focus group guide was developed based on further research questions arising from a rapid qualitative analysis of the interview data by four researchers (NL, MW, CU, MB, and another qualitative research expert in the department). Within another expert meeting, the results of the rapid analysis were discussed, and further research questions were developed, resulting in the focus group guide. The relevant aspects and context factors influencing implementation were focused on in depth, and further aspects regarding the implementation process during the pilot study were discussed.
A short sociodemographic questionnaire was sent via mail prior to the interviews and focus group and included aspects such as sex, age group, professional background, and working experience.
Semi-structured interviews were conducted via telephone or video conference according to the preferences of the interviewees and lasted approximately 30–60 minutes. All interviews were audio-recorded and transcribed verbatim. The focus group included several consultants and was moderated by members of the research team (NL). The focus group was conducted via an online meeting program of the University of Heidelberg (heiCONF) and was protocolled by three researchers who participated in the focus group session. No interview or focus group was repeated or cancelled, and no transcript was returned to the participants for correction.
Data Analysis
The first analysis of the interviews was performed via rapid qualitative analysis (NL).22 The interviews and findings were discussed by three researchers (NL, CU, and MB). Thematic analysis according to Braun and Clarke23 was conducted, initially using an inductive approach to identify emerging themes, followed by deductive coding using the Consolidated Framework for Implementation Research (CFIR)19,20 to structure the interpretation of implementation determinants across organisational and individual levels (NL). Each CFIR category was successively examined, and codes were resorted if needed by one researcher (NL). Another researcher (CU) then reviewed all categories against the data, and after a first draft of result interpretation, plausibility between the original codes and the reported results was discussed (NL, CU).
Data analysis was performed via the qualitative data analysis program MAXQDA (Verbi GmbH) software versions 2020 and 2022. IBM SPSS Statistics Version 26 and Microsoft Excel were used for the analysis of sociodemographic data.
Results
In total, N = 16 consultants participated in interviews (n = 11), and the focus group (n = 5) resulting in an overall participation rate of 40%. All participants were employees of AOK Baden-Wurttemberg and were working in its health centres. The majority (81%) of these were female (Table 1). They had a professional background as prevention experts with a specification in either nutrition (50%), physical exercise (38%), or a combination (12%). One participant explicitly stated a professional background in mental health as well. The consultants were mostly (68%) in the range of 40–59 years of age. Three consultants were younger (25–39 years) and two were 60 years or older. Consultants reported work experience ranging from 1 to 42 years, reflecting a broad range of professional experience among participants. All consultants were conducting prevention consultations or courses on a regular basis regarding their respective professional background in addition to the study setting. When referring to these courses, the terms “general (prevention) consultations” or “general (prevention) courses” were used for better understanding and differentiation from the intervention. The citations in this manuscript were translated verbatim by the authors. Citations are formatted as follows: 1: Pseudonym; 2: sex, male (m) or female (f); 3: professional background, physical exercise (PE), nutrition (N), and/or mental health (MH); 4: position in transcript.
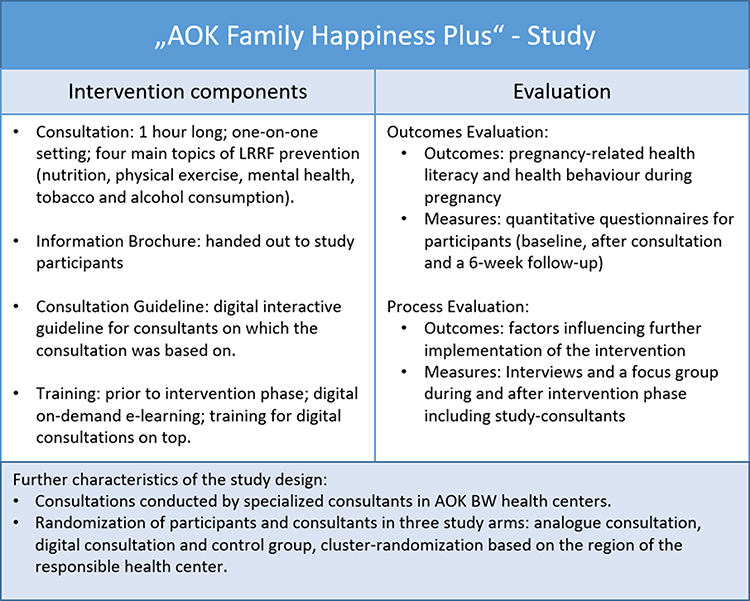 |
Figure 1 Overview of the “AOK Family Happiness Plus” study. |
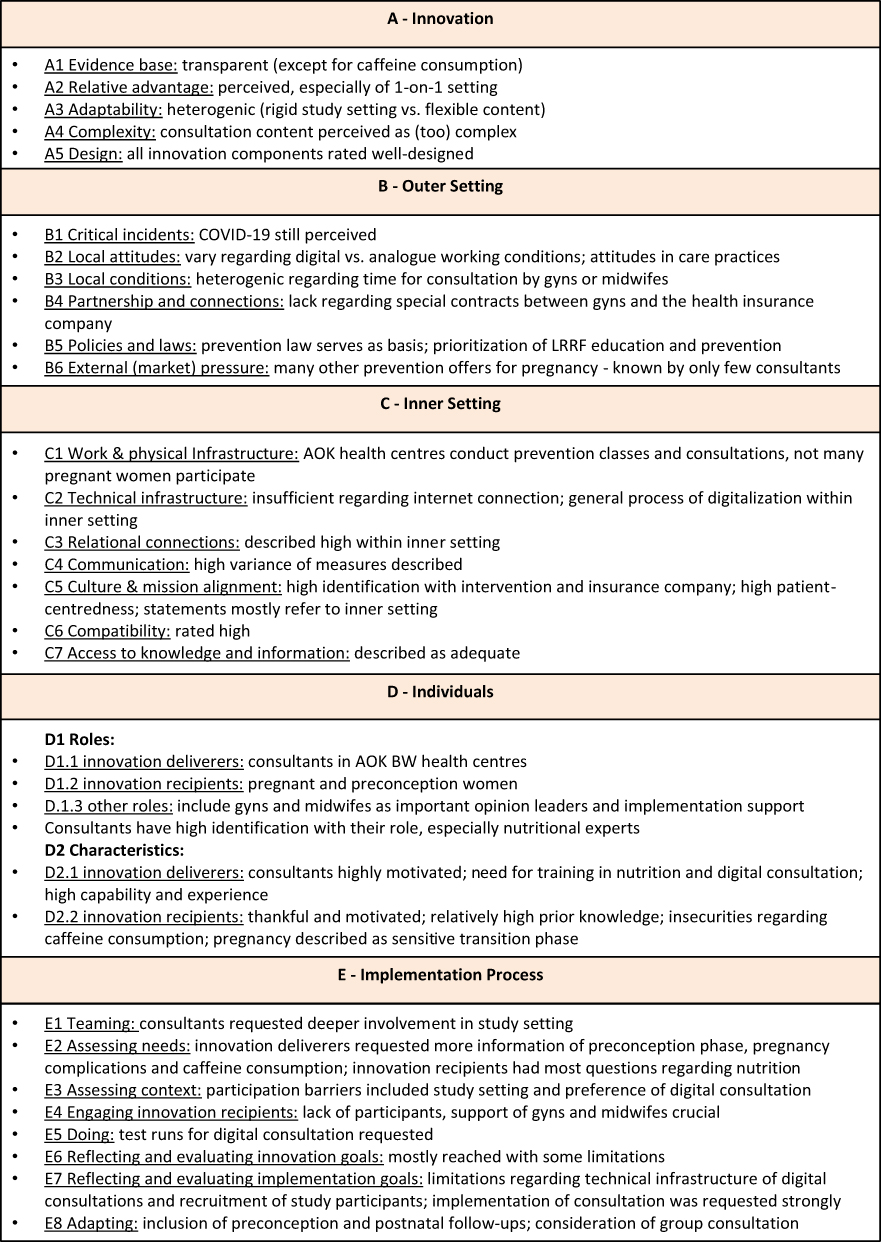 |
Figure 2 Overview of the study results according to the CFIR framework:18 (A) Innovation, (B) Outer Setting, (C) Inner Setting, (D) Individuals, and (E) Implementation Process. |
 |
Table 1 Sociodemographic Characteristics of Participating Consultants |
Results are reported according to the CFIR-framework (see Figure 2): As A. Innovation, the “AOK-Family +”-consultation and further intervention components (such as the brochure, e-learning training of the consultants, the digital or analogue setting, or the interview guideline) were defined. The AOK BW health insurance company was defined as the B. inner setting; the C. outer setting contained aspects regarding the general health system or general clients of the AOK BW prevention courses/consultations that are not part of the intervention. D. individuals included all the roles and their characteristics that are involved in the conduction or implementation of the intervention. The E. implementation process focused on aspects regarding the conduction of the “AOK-Family +”-study specifically, rather than aspects regarding the conception of the intervention.
For better clarity, categories of the CFIR are marked in italics within the text.
Innovation: Description of the Intervention and Its Components from the Consultant’s Perspective
The innovation was developed on actual evidence (A1). The information brochure, which was seen as a guideline for the consultation, contains information for consultants and for innovation recipients (study participants such as pregnant women and women in childbearing age) and citations of this evidence. For the topic of caffeine consumption, some consultants asked for further evidence, as they described that the suggestions provided in the consultation guideline and information brochure would differ from those in other guidelines.
A relative advantage (A2) is seen regarding the intervention setting. The consultation is conducted as a one-on-one consultation, which was perceived as beneficial and as an advantage over other measures in primary prevention as expressed by one consultant.
Yes, I think it’s of a high quality in comparison (to other prevention measures) because one person takes the time to have a one-to-one conversation on the topic. I don’t think that’s very common these days. (Int03/m/PE/Pos.78)
Some consultants described pregnancy-related consultation of LRRFs, such as health-promoting nutrition, as relatively similar to general consultation, as “nothing fundamental is changing in the diet” (Int02/f/N/Pos.66). The perceived relative advantage of the intervention seemed to be somewhat limited, as the consultants did not know many primary prevention measures addressing pregnancy outside of health insurance. The centralized organization of consultations and prevention courses in the AOK BW was positively highlighted by the participants compared with outsourced courses in other health insurance companies. Additionally, the combination of the four prevention themes within the information brochure was described as “great”, “summarized at a glance” and “big difference from other prevention formats” (Int01/m/PE/Pos.38) within the insurance company.
The adaptability (A3) of the intervention was heterogeneous. On the one hand, some consultants stated that they were able to individualize the consultation and its key topics to the needs and interests of the participating women. On the other hand, consultants described that they were not able to individualize the consultation, as they were strictly following the consultation guideline due to the study setting and limited time available. This resulted in little or no time for questions during the consultation. Consultants described a tension between maintaining the standardized consultation structure required by the intervention protocol and adapting counselling content to the individual needs and questions of pregnant women.
The complexity (A4) of the consultation content was perceived as rather high for the planned one-hour conversation by some consultants. Hence, others described that the topics could be addressed only superficially. Some consultants therefore perceived the intervention as adequate for “standard” (Int09/f/PE/Pos.58) pregnancies without any complications or specific questions.
In addition to these remarks, the design (A5) of the consultation, the brochure, and the preceding training for consultants were described as largely positive. The design of the consultation was perceived as informative and sufficient, with a focus on the topic of pregnancy-related nutrition. The combination of the four main topics through the consultation and the availability of a personal and a digital consultation in general were positively highlighted. In this regard, integrated videos were considered “refreshing” (Int05/f/N/Pos.28). Concerning the design of the intervention, some consultants pledged for follow-up consultations, as they would have been “surprised” (Int05/f/N/Pos.34) that there was only one appointment scheduled. One participant suggested preserving practical parts, which are not part of the intervention.
The brochure was evaluated positively in comparison with other programs of the health insurer. This was described by consultants, which also received positive feedback from the study participants, as the brochure was handed out after the consultation. In addition, the interactive digital consultation guideline handed out to the consultants was rated important for conducting the consultation.
All consultants received training in the form of on-demand e-learning which they as well edited with adequate and sufficient information. Only a few described the training as time-consuming. The preparations for the digital consultations were thoroughly described as more complex.
Outer Setting: Contextual Factors Outside the Health Insurance and the Intervention
As events or situations influencing the implementation process (B1), the COVID-19 pandemic was described by the consultants. On the one hand, personal courses within the health centres were described as having not yet reached pre-pandemic participation levels. In particular, pregnant women were perceived to be more anxious and to avoid onsite courses. On the other hand, online courses were perceived as more successful and practical. Furthermore, consultants with general prevention measures sought more onsite courses after the pandemic. As another factor influencing the implementation process, a general problem of “starting difficulties” (Int06/f/N/Pos.94) was described in the implementation of new prevention courses.
Concerning local attitudes (B2) of recipients of prevention measures in general, intrinsic motivation seemed to play a crucial role in participation. Course participants who were “sent” by a physician or their relatives were described to drop out of the course more often. Patients who have greater strain, for example, through pain, participate more regularly. These patients were described as “highly thankful for the offer” of consultations and “people say, it is great, you took the time. My doctor had told me the diagnosis, but he did not have time” (Int05/f/N/Pos.4).
With respect to digital or onsite courses, older participants and older consultants prefer courses in person. The communication of the prevention program was preferred by older patients to stay analogue, for example, via a brochure. It was described that with the additional digital marketing of prevention programs, especially younger clients were attracted. However, within their other online courses, consultants experienced the participation of highly motivated clients with less drop-out than in their onsite courses.
Concerning local conditions (B3), some participants described having experienced consultations by gynaecologists and midwifes in regular health care. Most consultants also believed gynaecologists and midwifes do not have any time for proper consultation, and some even described a lack of knowledge of LRRF prevention. Regarding partnership and connections (B4), health insurance has special agreements with local physicians, and they are asked to suggest courses or consultations provided by AOK BW to their patients.
Across interviews, consultants emphasized that recruitment and engagement of participants largely depended on referral pathways through gynaecologists and midwives that need to be strengthened.
In general, greater prioritization in political decision-making (B5) and financing was demanded for prevention measures. Consultants suggested that prevention in general and LRRFs during pregnancy specifically should be addressed in schools. In the context of external market pressure (B6), several pregnancy courses, such as yoga or gymnastics, books, WhatsApp group chats, information brochures, online articles, and various pregnancy apps, were named outside of health insurance by a few consultants. With respect to health-promoting nutrition during pregnancy, no other program was named.
Inner Setting: Health Insurance Company and Health Centres
The consultations were conducted within the health centres of AOK BW, where the consultants were employed. One participant described that there were more than 50 health centres (C1), and another mentioned that three prevention experts conducted “AOK-Family +” consultations at their health centre. Apart from the study, these experts offer courses and consultations for primary and secondary prevention, such as nutrition counselling for patients with obesity or diabetes or physical courses for patients with back pain. Pregnant women were not usually part of these courses and consultations, except for back-strengthening courses or nutritional consultation due to gestational diabetes, but this was described as very rare. By the time of data collection, the consultants mentioned that there were no courses directly addressing pregnant women. Only a few courses, such as pelvic floor exercise or yoga, were perceived as suitable for pregnant women but were not explicitly advertised as such. However, course instructors were described as having some insecurities concerning training during pregnancy.
(…) here, at AOK BW, because there isn’t really much offered. So, we have the pelvic floor course, yes, but it’s not advertised for pregnant women. I now include pregnant women because I simply know what to look out for and how to get them through it. (.) But I’ve also had colleagues who have said, yes, but is she allowed to do everything? Yes, what do I do with her if she has these and those problems? (Int09/f/PE/Pos.62)
As part of the general organizational development within AOK BW, the consultants desired the implementation of courses and consultations addressing pregnancy and maternity/young families. Information technology infrastructure (C2) was described as changing in terms of current digitalization. For example, advertisement of the course program was said to be in a change from analogue and digital publication to solely digital promotion via the internet or e-mail.
Relational connections (C3) seemed to play a crucial role within the health centres. The consultants were observed to be eager to recommend other offers within the AOK BW prevention spectrum and external experts, such as social services, psychotherapists, other internal consultations, and various courses, to their clients. As part of the culture and mission alignment (C5), the participants in this study seemed enthusiastic in increasing the company’s economy. In this regard, the “AOK-Family +” consultation was perceived as an offer that “fills the gaps” and “gains interest” (Int11/m/PE,MH/Pos.46) in an “interesting target group” (FG01/f/N/Pos.76). When asked about LRRF prevention within health care, consultants often only referred to AOK BW internal procedures and were not able to name any aspects outside of the inner setting. As another example of the inner setting culture, consultants seemed to share their employer’s cooperate values.
Since we at the AOK, or as a health insurance company, are very big on prevention, and I know how other health insurance companies deal with prevention counselling or how they deal with counselling and that everything is outsourced (…). (Int01/m/PE/Pos.40)
In general, within their statements, high client-centredness was expressed by the consultants. For example, standardized procedures were adapted to clients’ needs, and the consultants all showed high motivation to achieve successful interventions and help their clients achieve their health goals. All consultants believed that the consultation in general was important, a good and beneficial offer and that the health insurance itself was seen as suitable for conducting pregnancy-related LRRF consultations.
So, I think it’s basically a great format, I also think it’s very nice that you come before something happens, I also think it’s a very happy format, yes, it’s a nice situation, why someone comes to you, they’re not sick but they just want, well, I mean what could be nicer than having a baby? so I think it’s a really great format, a really great offer. (Int08/f/N/Pos.70)
Overall, the compatibility (C6) of the intervention with other routine tasks was rated as high. As most consultants provided courses and consultations, this new format fitted well in their routine. Some consultants described that the time for appointments was blocked in their calendars, but at the beginning of the intervention phase, no innovation recipient attended the study; hence, time for regular consultations was missing. Few consultants mentioned that the study process and preparation were time-consuming, which was regarded as extra time “on top”, for which they spent their “free time” (Int03/m/PE/Pos.52).
Individuals: Roles Involved in the Implementation Process
The main roles (D1) associated with the implementation of the intervention were the innovation deliverers (D1.1) and innovation participants (D1.2). Innovation deliverers (D1.1) included prevention experts with nutritional or physical expertise working in AOK BW health centres. In particular, nutritional experts were seen as ideal deliverers, but all health consultants in AOK BW health centres were named suitable, as “It’s all about prevention. Then that’s us.” (Int04/f/N/Pos.84).
In this context, self-efficacy of consultants was perceived as rather high. They saw themselves mainly in their role as prevention experts in health centres as innovation deliverers. Some consultants described that other care deliverers, such as midwifes and gynaecologists, should “give hints” to the intervention “but then (pregnant women) should go where there is a certain professional expertise (Int05/f/N/Pos.22).”
Innovation recipients (D1.2) include mostly pregnant women or women in family planning phase. Some partners also took part in the consultation, which was perceived as beneficial by the consultants. Some consultants wished for more partners to participate in the intervention to support their partners with the implementation of behaviour change measures before/during pregnancy.
As opinion leaders (D1.3), mostly gynaecologists and midwifes came up as a first point of contact during pregnancy and first informers about pregnancy-related LRRFs. Interchanging with peers or family was also described as opinion leading. As part of the sampling strategy within the pilot study, gynaecologists were asked to hand over and display study flyers. This measure was described as central for implementation by the consultants. However, the extent to which women were actually informed about the study by local physicians cannot be determined. In addition to other forms of implementation support (D1.3), social media or other points of contact for pregnant women were listed.
To describe the characteristics (D2) of the individuals involved, the data provide hints about consultants as innovation deliverers (D2.1) and respective women as innovation recipients (D2.2).
The consultants (D2.1) were observed to be highly motivated, open to new ideas, optimistic and ambitious. In various statements, their work in prevention courses and consultations was perceived as pleasure, and actions with high client-centredness and commitment to their work could be observed.
Innovation recipients (D2.2) were described as thankful, open to new information and motivated. For example, women were observed to have asked many (specific) questions, and some were writing notes during the consultation. Only one consultant described occasional women as less interested. Most were perceived as positive because of their pregnancy and that they “ask for help, I’ll call it, or recommendations, tips and therefore also, yes, perhaps want to change something in their lives (Int02/f/N/Pos.2).”
Most women already were described as having relatively high prior knowledge about health-promoting behaviour during pregnancy. Few consultants described a lack of knowledge, especially of the suggested avoidance of caffeine consumption and the detailed consequences of gestational alcohol consumption in some women. Their partners were generally described as having a greater need for information about health-promoting behaviour during pregnancy.
All consultants were observed to have knowledge of the topics of prevention regarding nutrition, physical exercise, and stress reduction. They were all experienced in giving courses and counselling. Mostly, throughout the training prior to study conduction, they described that they needed only “refreshment” (Int06/f/N/Pos.60) of their knowledge. Some described that they had to train more intensely, especially when they had no professional background in nutrition prior to study conduction. Others described that they had to prepare themselves more intensely for digital consultation. Many reported, they had little or no experience working with pregnant women. If they had experience, this was mostly traced back to their own or their partner’s pregnancy. Few had solid experience working with pregnant women through the courses they had given 10–15 years ago.
In general, regarding caffeine consumption, innovation recipients and innovation deliverers were described as having a lack of knowledge and uncertainty. In the “AOK-Family +” consultation, pregnant women were advised to avoid caffeine consumption of any kind. The consultants described this as new information for most of the participating women. In addition, consultants described that this guidance was new to them as well and that they were not overall sure about this regulation and even asked for further evidence to comprehend the guideline. Within the consultations, this topic was often discussed and it was described that the consultation guideline and the information brochure did not contain all the information needed for these situations.
Participating women were described as being in a phase of “transition” (Int08/f/N/Pos.24) in their lives and that they had to process much new information. Therefore, it was perceived as important to talk about intimate topics such as tobacco addiction or weight gain/loss sensitively. One consultant felt it would be too much information at once, especially for women in family planning phase, and that she would suggest informing them step by step, depending on their actual fertility state. In this statement, postnatal information was also included. Pluriparous women were observed to have more knowledge than nulliparous women. Consultants highlighted the importance of a consultation early in pregnancy or even before. Women in family planning phase were described to have a greater need for advice than pregnant women did. Consultants assumed that pregnant women in urban areas have a greater need for consultation than pregnant women in rural areas because of a larger peer network; hence, in rural areas, “the consultation is not necessary from our side” (Int10/f/PE,N/Pos.42).
Implementation Process: Further Aspects Regarding the Implementation of the Intervention
As a teaming (E1) measure, the intervention was promoted within the health insurance company and especially within the health centres. Some consultants felt that they were not engaged enough in the study organization and asked for more background information about the study and its progress. Through the intervention study, consultants identified their need (E2) for more information about preconception health, complicative pregnancies, and caffeine consumption during pregnancy which was also asked to add to the consultation guideline. One consultant described that she made many notes within the guideline and did some background research to prepare for the consultations. Participating women were described as having come up with questions addressing the postnatal phase, for example, regarding nutrition during breastfeeding. Most questions during consultations were reported regarding nutritional aspects. The topic of drug, alcohol, and tobacco consumption was described as the part with the lowest need for consultation. One woman brought her first child to the consultation, which had an influence on the consultation atmosphere and needs to be considered a possible scenario.
Some consultants described that some women randomized in the analogue study arm would have preferred a digital consultation. This was described as a possible participation barrier (E3), as within the study setting, it was not possible to switch study arms. Additionally, the study setting itself was considered to be a potential participation barrier. Possible further participation barriers included a longer timeframe between the study inscription and the actual consultation appointment, language barriers or a feeling of shame, eg. because of maternal obesity or drug consumption.
Depending on how much time passes between scheduling the appointment and the actual appointment, a few weeks may pass, during which the pregnant women may have already gained much knowledge from other sources and may think to themselves, well, now I actually know enough and may therefore cancel the consultation (Int02/f/N/Pos.48)
Consultants described that participation in the consultation was time-consuming for the women and that they might be busy otherwise during pregnancy. In general, women in early pregnancy, especially those with a greater need for primary prevention, were described as hard to reach. Here, again, the role of gynaecologists, midwives, or primary care physicians was seen as crucial and a suggestion of these, referring to the “AOK-Family +” consultation, was seen as mandatory to successfully engage (E4) potential study participants. Specifically, a personal approach by those care workers towards suitable women as well as the study team addressing the care workers in person and informing them about the intervention were described as crucial. The following communication channels were also named important for engaging innovation participants: social media (including a proper social media strategy), via mail or e-mail, via posters or flyers, within living environments (employers, stores, pharmacies, etc.), and via other courses for pregnancy and birth (eg. birth preparation courses).
Prior to intervention enrolment, consultants described conducting test runs (E5) with their peers and reported the need for a mandatory pilot consultation with the ability to practice the consultation.
Regarding the reflection and evaluation of innovation goals (E6), most consultants reported that they had positive experiences during the consultation and were able to help their study participants, for example, in answering their questions, giving them new information or specific advice, or encouraging them in their behaviour and knowledge. Although the innovation recipients were described as mostly well informed, “(…) there was always a topic that we could help with or where they had an ‘aha’ effect. Yes, that was my experience (FG02/f/PE/Pos.23).”
Other consultants highlighted AOK BW as a point of contact for pregnant and preconception women and described this as “a feeling of reliability” (FG01/f/N/Pos.99). Negative aspects that might limit the effectiveness of the intervention included the fact that the consultation contained no follow-up appointments. Furthermore, because topics were discussed only superficially and there was little time for questions, this was described as a potential limitation to the innovation goals.
A main limitation to implementation goals (E7) was technical problems within the digital consultation. Nevertheless, consultants managed to switch to another conference platform by themselves and were able to conduct the intervention as planned. The planned 1 hour could be maintained by some consultants, yet many described a longer consultation. Another major implementation goal limitation described by the consultants included recruitment difficulties, for which the consultants expressed their regret. As a consequence, study enrolment was limited, as consultants were not able to find their routine, and consultation preparations were perceived as more time-consuming.
As an overall conclusion for consultants, they pledged for the intervention to be implemented sustainably within the AOK BW range of services and described that their participating women reflected they “think it’s truly cool, the offer, and that they would also like it for others if it were a permanent part of our program. I think so too.” (FG03/f/PE/Pos.161).
Many adaptation (E8) measures were identified and allocated into two main categories: modification of the intervention and expansion potential of the intervention. As a consequence of the intervention’s complexity, consultants suggested a division into several appointments held by respective experts in each topic. For example, nutritional consultations could then be performed by nutritional experts only. This also implies follow-up appointments to accompany women during their pregnancy. A group setting was also considered for the consultation. As a possible benefit, social exchange with peers was named, which was also seen as important for women during pregnancy. Expanding the group setting as a digital information offer, such as a regular “evening information event” (Int09/f/PE/Pos.72), which was said to lower the participation threshold, was suggested. However, it was seen as important that a one-on-one consultation could always follow the group setting whenever needed. As another important aspect, turning the consultation into a “family consultation” (Int01/m/PE/Pos.34), including inviting partners or peers of the women to participate in the consultation on a regular basis, was suggested. In addition, more adequate tailoring for the preconception phase was also suggested.
Given the potential for expansion of the intervention, the phase after birth was seen as important, and a need among recent mothers was described. Potential topics included pelvic floor training, nutrition during breastfeeding, the start of complementary feeding of babies, stress management of recent mothers, efficient family organization, and fitness for new mothers. However, here again, most consultants were not able to name interventions outside of the insurance setting. Few consultants listed many offers outside of the health insurance company and stated that they saw no need for further offers.
Across domains, recruitment pathways through gynaecologists and midwives, compatibility with existing prevention activities in the health centres, and technical infrastructure for digital consultations emerged as key determinants influencing implementation.
Discussion
The present study contributes to the literature by examining the implementation of a lifestyle counselling intervention addressing multiple lifestyle-related risk factors within the organisational context of a statutory health insurance system. To summarize the results, the intervention and its components were seen as well composed and focused on an important topic by the intervention delivers. In particular, the combination of the four main topics and the one-on-one setting were positively highlighted. The consultants highly identified themselves with the intervention, and their compatibility with work routines was described as high. The consultants mainly saw themselves in the role of innovation deliverers with strong self-efficacy and high capability. Stronger involvement of gynaecologists or midwifes was seen as crucial for opinion leading and communicating the intervention to potential innovation participants. Consultants and participating women were described as highly motivated. Pregnant women were mostly perceived to have knowledge about LRRFs prior to the intervention. Consultants perceived that the consultation contributed to improving participants’ understanding of LRRFs, although behavioural outcomes were not assessed in this process evaluation. Implementation goals were subjectively achieved with some major limitations, such as technical difficulties and recruiting problems. Adaptation of the intervention was suggested for group and online settings as well as regarding the potential for expansion for the phase after birth. The study was guided by a conceptual framework but did not involve in-depth theorizing. Across interviews, the impression arose that the perspective of most consultants focused mainly on the inner setting of AOK health centres. The health care system, the regular health care providers of pregnant women, and even other health insurances were often not considered in their statements. As the intervention study aimed to implement the intervention as part of regular care, embedding of consultants and the intervention further in regular care procedures is necessary but within the present study limited due to the insurance company setting. Here, it also remains unclear, how other health insurances manage the implementation of the prevention law (§20 section 4, Nr.1 and section 5, SGB V) which obligates health insurances to offer certain prevention programs. Some consultants also framed pregnant women as an “interesting target group” for prevention activities. This reflects the institutional context of health insurance–based prevention and highlights the need to critically consider how public health objectives and economic incentives intersect in such programs. Consultants stated that other health insurances would outsource their courses which was devaluated by them. Due to lack of evidence, this cannot be assessed properly and it cannot be stated if insurance courses have a better quality than outsourced courses conducted by local course instructors. In a conclusion, transferability of results might be limited. At this time, it seems like the intervention is the first one that combines the obligated four topics within a consultation addressing pregnancy.
Beyond organisational factors, the findings also point to the importance of maternal motivation and engagement in shaping participation in the intervention. Consultants described varying levels of interest and readiness among pregnant women, which may influence both recruitment and uptake of counselling services.
In addition, digital delivery formats were perceived as both a facilitator and a barrier, suggesting that differences in access to and familiarity with digital technologies may affect participation and implementation reach.
Integrating lifestyle counselling into routine antenatal care pathways, such as existing consultations with gynaecologists or midwives, was identified as a key opportunity to enhance accessibility and sustainability of the intervention.
Furthermore, consultants highlighted the importance of training and preparation for delivering the intervention, indicating that structured training formats may support implementation quality and consistency.
From an implementation perspective, these findings suggest that scaling and long-term integration of such interventions will depend on the alignment with routine care structures, availability of resources, and the ability to adapt delivery formats to different population needs.
Discussion of Research Design
Qualitative analysis requires careful interpretation of participants’ perspectives and contextual factors, and the thematic analysis applied in this study involved iterative coding, discussion among researchers, and interpretation of themes within the CFIR framework. There were no CFIR categories that inductively emerged from the interview data. Several categories did not yield codes, such as innovation – cost; implementation process – tailoring strategies and planning; roles – high and mid-level leaders, implementation leads and implementation team members; inner setting – incentive systems and relative priority. However, including consultants in the process evaluation meets the intention of the CFIR, which is used to collect data from individuals who have power and/or influence over implementation outcomes.19 In some cases, categories from the original CFIR20 version appeared more suitable. For example, “beliefs about the innovation” was prominent in the data but is no longer an explicit category in the updated CFIR
Across CFIR domains, several determinants appeared to interact and influence implementation outcomes. For example, recruitment challenges described in the outer setting were closely linked to engagement mechanisms involving gynaecologists and midwives as referral partners. Similarly, technical barriers affecting digital consultations reflected organisational infrastructure conditions within the inner setting. These findings illustrate how implementation success depended not only on the intervention design itself but also on interactions between organisational structures, professional networks, and available resources.
The innovation deliverers strongly perceived the intervention’s relative advantage and effectiveness, which is considered crucial for successful implementation.20
As all consultants were employed within the same health insurance organisation, organisational perspectives may have influenced some interpretations of the intervention. This process evaluation primarily reflects the perspectives of consultants delivering the intervention. While this approach provides important insights into implementation processes and organisational determinants, it does not capture the perspectives of pregnant women participating in the intervention. As a result, interpretations regarding participants’ knowledge, motivation, or perceived benefits should be considered indirect observations. Future research including participants’ perspectives would provide a more comprehensive understanding of the intervention’s implementation and reception.
The present process evaluation therefore focuses on implementation from the perspective of intervention deliverers, complementing other evaluation components examining participant outcomes. Some consultants had not yet conducted intervention consultations at the time of the interviews; therefore, their perspectives primarily reflect expectations and early implementation experiences.
Within the interviews and focus group, consultants listed important strategies in this regard. However, most of them were included in the sampling strategy of the main study, eg., a large social media campaign and the engagement of gynaecologists, as well as a personal approach towards primary care physicians.14 Gynaecologists and midwifes were only approached via mail and were asked to hand out information flyers. It is not possible to estimate how many care workers passed those flyers on to possible innovation recipients. The recruitment challenges observed in this study suggest that outreach strategies based solely on health insurance communication channels may be insufficient, highlighting the importance of stronger integration with routine antenatal care providers. In addition, recruitment challenges may have influenced the reach of the intervention, while uncertainties regarding specific counselling recommendations highlight the importance of maintaining fidelity through clear and consistent evidence-based guidance.
As participation in the process evaluation was voluntary, it is possible that consultants who chose to participate differed in their perspectives or experiences from those who did not participate.
For future implementation of the consultation, the recruitment strategy was analysed and as a result, it was seen as crucial to involve care workers as major implementation support and as gatekeepers to reach pregnant women and women who express their desire to have children.24 In Germany, women aged 20–34 years are eligible for cervical cancer screening once a year. Routine screening appointments may also provide opportunities to integrate preventive counselling, including discussions of LRRFs.25 However, reaching all women in Germany remains challenging. Studies show large variation in cervical cancer screening utilisation, ranging from 3% to 88%.25 A previous study revealed that women with a lower socioeconomic status were observed to have lower health knowledge about LRRFs during pregnancy and therefore should be reached by the intervention.8 The utilization of care during pregnancy, and therefore the potential for study engagement of these women, is highly heterogeneous and depends on many different factors besides the socioeconomic status.26 In Germany, women with a higher socioeconomic status were low-utilizers of mammography screenings in regular care.27 Hence, it is difficult to engage all women by including gynaecologists as main gatekeepers and providing implementation support, but this should be seen as one of the most important points of contact to engage women.
Discussion of Intervention Components and Implementation
The present study contributes to the literature by providing insights into organisational and contextual determinants influencing the implementation of pregnancy-related lifestyle counselling within a statutory health insurance setting. In this study, the combination of the four main topics of LRRFs was highlighted. The topics of the consultation meet with the guidelines of “healthy start–young family” and follow the guidelines for prevention courses in health insurers within the national prevention law (§20 section 4, Nr.1 and section 5, SGB V).11 However, some differences were identified. For example, dental care and vaccination during pregnancy play a role in German guidelines but are not included in the “AOK-Family +”.11 Within this study, the abstention of caffeine consumption was recommended to the women within the consultations. Consultants reported uncertainty regarding recommendations on caffeine consumption during pregnancy. International guidelines differ in their communication of caffeine recommendations; for example, the European Food Safety Authority considers caffeine intake of up to approximately 200 mg per day during pregnancy to be safe.11,28 Such inconsistencies highlight the importance of providing clear and consistent evidence-based guidance within counselling interventions to avoid confusion among both consultants and pregnant women. Recent studies have shown that low caffeine intake can also be associated with certain risks, and reliable data for low doses of caffeine intake during pregnancy are needed to define a safe dose.29 Uncertainty among consultants regarding the recommendation to completely avoid caffeine during pregnancy also highlights the importance of providing clear and consistent evidence-based guidance to ensure intervention credibility and fidelity.
Furthermore, it was described by the consultants that German midwifes and gynaecologists did not have time or adequate competence to conduct a profound consultation regarding LRRF within regular care. A previous study supported this finding and revealed a lack of time and guidelines for LRRF consultation as well as unfavourable regulations and undefined responsibilities.12 In Germany, the “healthy start–young family” network has published guidelines and further information media for reducing LRRF during pregnancy.11,30 However, standardized guidelines for care workers on how this recommended behaviour change can be achieved are lacking.31 The “AOK-Family +” consultation could therefore be one starting point and an evidence-based approach to address aimed behaviour change. However, these findings reflect the perceptions of consultants delivering the intervention and should not be interpreted as evidence of behavioural change among participants.
Using the CFIR framework, several determinants influencing implementation became apparent. These included the perceived relative advantage of the one-on-one consultation format, strong compatibility with existing prevention activities within the health centres, a supportive implementation climate within the organisation, the importance of engagement through referral networks involving gynaecologists and midwives, and the role of available organisational resources in enabling delivery of the counselling intervention.
Conclusion
This study provides insights into the implementation of lifestyle counselling during pregnancy within a health insurance setting and highlights key contextual determinants and implementation challenges. The intervention includes well-designed components with a complex consultation that combines four main topics for LRRF prevention during pregnancy: health-promoting nutrition, physical exercise, mental health, and the absence of tobacco and alcohol consumption. Innovation goals were subjectively achieved from the perspective of innovation deliverers. Still, the intervention is seen as an evidence-based approach to address behaviour changes prior to and during pregnancy. Consultation programs within public health insurances therefore might contribute to enhance knowledge of LRRF prevention in pregnancy. While the intervention demonstrates potential to strengthen preventive counselling during pregnancy within the health insurance setting, challenges such as recruitment pathways and organisational integration need to be addressed for broader implementation. Future implementation of lifestyle counselling interventions during pregnancy should strengthen recruitment pathways, particularly through stronger collaboration with gynaecologists and midwives and integration into routine antenatal care structures. In addition, further research should evaluate the effectiveness of such interventions in improving health behaviours among pregnant women. These findings should also be interpreted in light of the contextual constraints identified in this study, including recruitment challenges, technical barriers in digital delivery, and organisational conditions within the health insurance setting.
Trial Registration
The German Clinical Trials Register DRKS00027804. Registered on 2022/01/12.
Ethics Approval and Consent to Participate
The study was conducted in accordance with the Declaration of Helsinki in its current version. The study was approved by the ethics committee of the Medical Faculty of the University of Heidelberg, Germany, (S-419/2021) on 28.05.2021 and 15.08.2023 (process evaluation amendment). All participants gave written informed consent prior to data collection.
Acknowledgments
We thank all project participants, especially all consultants of the “AOK-Family +” consultation, for their participation in this study and for their commitment to the study. We like to thank Christoph Hepe, Dr. Lina Hermeling, Fiona Rohr, Jessica Vogel, and Alexa Wohnhas of the AOK BW for their support in the study, recruitment of study participants and writing protocols. We thank Dr. Regina Poß-Doering, University Hospital Heidelberg, for her support in the development of interview and focus group guidelines.
Funding
This study is funded by the German health insurer AOK Baden-Baden-Württemberg.
Disclosure
MB is employed by the health insurance company AOK Baden-Württemberg that funded the study. Although MB is employed by AOK Baden-Württemberg, the funding organisation had no role in the qualitative data analysis, interpretation of findings, or preparation of the manuscript. The other authors state that they have no competing interests for this work.
References
1. World Health Organization. WHO Recommendations on Antenatal Care for a Positive Pregnancy Experience. Geneva: World Health Organization; 2016.
2. Institute for Health Metrics and Evaluation. GBD Compare: Germany, Females, All Ages, Risk Factors 2021–2024. Seattle, WA: IHME; 2024. Available from: https://vizhub.healthdata.org/gbd-compare/.
3. World Health Organization. Tobacco Control to Improve Child Health and Development: Thematic Brief. Geneva: World Health Organization; 2021.
4. Popova S, Lange S, Probst C, et al. Estimation of national, regional, and global prevalence of alcohol use during pregnancy and fetal alcohol syndrome: a systematic review and meta-analysis. Lancet Glob Health. 2017;5(3):e290–17. doi:10.1016/S2214-109X(17)30021-9
5. Lange S, Probst C, Rehm J, et al. National, regional, and global prevalence of smoking during pregnancy in the general population: a systematic review and meta-analysis. Lancet Glob Health. 2018;6(7):e769–e776. doi:10.1016/S2214-109X(18)30223-7
6. Bergmann KE, Bergmann RL, Ellert U, et al. Perinatal risk factors for long-term health. Results of the German Health Interview and Examination Survey for Children and Adolescents (KiGGS). Bundesgesundheitsbl. 2007;50(5–6):670–676. doi:10.1007/s00103-007-0228-4
7. Kuntz B, Zeiher J, Starker A, et al. Rauchen in der Schwangerschaft – querschnittergebnisse aus KiGGS Welle 2 und Trends. In: Epidemiologie und Gesundheitsberichterstattung. Berlin: Robert Koch-Institut; 2018.
8. Oechsle A, Wensing M, Ullrich C, et al. Health knowledge of lifestyle-related risks during pregnancy: a cross-sectional study of pregnant women in Germany. Int J Environ Res Public Health. 2020;17(22):8483. doi:10.3390/ijerph17228626
9. Navarro P, Mehegan J, Murrin CM, et al. Associations between a maternal healthy lifestyle score and adverse offspring birth outcomes and childhood obesity in the Lifeways Cross-Generation Cohort Study. Int J Obes Lond. 2020;44(11):2213–2224. doi:10.1038/s41366-020-00652-x
10. Saur AM, Dos Santos MA. Risk factors associated with stress symptoms during pregnancy and postpartum: integrative literature review. Women Health. 2021;61(7):651–667. doi:10.1080/03630242.2021.1954132
11. Koletzko B, Cremer M, Flothkötter M, et al. Diet and lifestyle before and during pregnancy: practical recommendations of the Germany-wide Healthy Start – young Family Network. Geburtshilfe Frauenheilkd. 2018;78(12):1262–1282. doi:10.1055/a-0713-1058
12. Bombana M, Wensing M, Wittenborn L, et al. Health education about lifestyle-related risk factors in gynecological and obstetric care: a qualitative study of healthcare providers’ views in Germany. Int J Environ Res Public Health. 2022;19(18):11384. doi:10.3390/ijerph191811674
13. GKV Spitzenverband. Leitfaden Prävention. Berlin: GKV-Spitzenverband; 2023. Available from: https://www.gkv-spitzenverband.de/krankenversicherung/praevention_selbsthilfe_beratung/praevention_und_bgf/leitfaden_praevention/leitfaden_praevention.jsp.
14. Krämer M, Wohlhüter L, Hermeling L, et al. A counselling intervention for individual strategies to prevent complications and strengthen resources during pregnancy in gynaecological care (AOK-Family+): study protocol for a cluster-randomised controlled trial. Trials. 2024;25(1):393. doi:10.1186/s13063-024-08215-5
15. North S, Crofts C, Thoma C, Zinn C. The role of maternal diet on offspring hyperinsulinaemia and adiposity after birth: a systematic review of randomised controlled trials. J Dev Orig Health Dis. 2022;13(5):527–540. doi:10.1017/S2040174421000623. Epub 2021 Nov 2. PMID: 34725018.
16. Killeen SL, Phillips CM, Delahunt A, et al. Effect of an Antenatal Lifestyle Intervention on Dietary Inflammatory Index and Its Associations with Maternal and Fetal Outcomes: a Secondary Analysis of the PEARS Trial. Nutrients. 2021;13(8):2798. doi:10.3390/nu13082798. PMID: 34444958; PMCID: PMC8399423.
17. Dodd JM, Deussen AR, Louise J. A Randomised Trial to Optimise Gestational Weight Gain and Improve Maternal and Infant Health Outcomes through Antenatal Dietary, Lifestyle and Exercise Advice: the OPTIMISE Randomised Trial. Nutrients. 2019;11(12):2911. doi:10.3390/nu11122911. PMID: 31810217; PMCID: PMC6949931.
18. Wensing M, Poß-Doering R. Process Evaluation in Health Services Research. In: Wensing M, Ullrich C, editors. Foundations of Health Services Research. Cham: Springer; 2023. doi:10.1007/978-3-031-29998-8_13.
19. Damschroder LJ, Reardon CM, Widerquist MAO, et al. The updated Consolidated Framework for Implementation Research based on user feedback. Implement Sci. 2022;17(1):75. doi:10.1186/s13012-022-01245-0
20. Damschroder LJ, Aron DC, Keith RE, et al. Fostering implementation of health services research findings into practice: a consolidated framework for advancing implementation science. Implement Sci. 2009;4(1):50. doi:10.1186/1748-5908-4-50
21. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
22. Nevedal AL, Reardon CM, Opra Widerquist MA, et al. Rapid versus traditional qualitative analysis using the Consolidated Framework for Implementation Research (CFIR). Implement Sci. 2021;16(1):67. doi:10.1186/s13012-021-01111-5
23. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
24. Litke N, Wensing M, Hermeling L, Bombana M. Quantitative evaluation of recruitment strategies in a cluster-randomized trial: segmented regression and cost analysis from the AOK-Family + study. BMC Med Res Methodol. 2025;25(1):269. doi:10.1186/s12874-025-02734-8. PMID: 41315936; PMCID: PMC12670862.
25. Bujan Rivera J, Klug SJ. Gebärmutterhalskrebsscreening in Deutschland. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. 2018;61(12):1528–1535. doi:10.1007/s00103-018-2835-7
26. Mehta PK, Carter T, Vinoya C, et al. Understanding high utilization of unscheduled care in pregnant women of low socioeconomic status. Womens Health Issues. 2017;27(4):441–448. doi:10.1016/j.whi.2017.01.007
27. Dreier M, Borutta B, Töppich J, et al. Mammography and cervical cancer screening: a systematic review about women’s knowledge, attitudes and participation in Germany. Gesundheitswesen. 2012;74(11):722–735. doi:10.1055/s-0031-1286271
28. EFSA Panel on Dietetic Products. Nutrition and Allergies. Scientific opinion on the safety of caffeine. EFSA J. 2015;13(5):4102.
29. Rohweder R, de Oliveira Schmalfuss T, Dos Santos Borniger D, et al. Caffeine intake during pregnancy and adverse outcomes: an integrative review. Reprod Toxicol. 2024;123:108518. doi:10.1016/j.reprotox.2023.108518
30. Koletzko B, Bauer CP, Bung P, et al. Nutrition in pregnancy: practice recommendations of the “Healthy Start – young Family Network”. Dtsch Med Wochenschr. 2012;137(24):1309–1314. doi:10.1055/s-0032-1305074
31. Rockliffe L, Peters S, Heazell AEP, et al. Factors influencing health behaviour change during pregnancy: a systematic review and meta-synthesis. Health Psychol Rev. 2021;15(4):613–632. doi:10.1080/17437199.2021.1938632
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Prevention of Melasma During Pregnancy: Risk Factors and Photoprotection-Focused Strategies
Zhao L, Fu X, Cheng H
Clinical, Cosmetic and Investigational Dermatology 2024, 17:2301-2310
Published Date: 15 October 2024
Study of Radioclinical and Risk Factors of Cerebral Venous Thrombosis: A Retrospective Analysis of Patients Presenting to a Tertiary Hospital in Mogadishu, Somalia
Adam BA, Osman AA, Sheikh Hassan M, Sidow NO, Osman Hidig MF, Mohamed AA, Ibrahim AA, Mohamed SA, Mohamed YG, Ahmed SA, Jeele MOO, Hassan MO
International Journal of General Medicine 2025, 18:371-378
Published Date: 23 January 2025