Back to Journals » Infection and Drug Resistance » Volume 16
A Case Report of Streptococcus Dysgalactiae Toxic Shock Syndrome Complicated with Symmetric Peripheral Gangrene
Authors Shen X ![]() , Liang H, Wu G, Chen M, Li J
, Liang H, Wu G, Chen M, Li J
Received 21 June 2023
Accepted for publication 5 September 2023
Published 8 September 2023 Volume 2023:16 Pages 5977—5983
DOI https://doi.org/10.2147/IDR.S426930
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Xiaoqing Shen,* Hongkai Liang,* Guishen Wu, Miaolian Chen, Jianwei Li
Department of Critical Care Medicine, Zhongshan People’s Hospital, Zhongshan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jianwei Li, Department of Critical Care Medicine, Zhongshan People’s Hospital, Zhongshan, 528400, People’s Republic of China, Email [email protected]
Abstract: Streptococcus dysgalactiae subspecies equlsimilis (SDSE) is considered an important bacterial pathogen, and attention has also increased with the increasing number of invasive SDSE infections. Here, we report a patient with S. dysgalactiae toxic shock syndrome complicated by symmetrical peripheral gangrene (SPG). Despite surviving active treatment, amputation severely impacts the quality of life of patients. Therefore, we should pay attention to the early treatment of SDSE infection and the prevention and treatment of related complications.
Keywords: Streptococcus dysgalactiae subspecies equlsimilis, streptococcal poisoning shock syndrome, symmetric peripheral gangrene
Introduction
Streptococcus dysgalactiae subspecies equlsimilis (SDSE) belongs to a group of β-hemolytic streptococci, and is a common symbiont of humans. It is often colonizes in the human throat, skin, gastrointestinal tract, and the vagina.1 The incidence of bacteremia caused by SDSE is increasing worldwide, and streptococcal toxic shock syndrome (STSS) is of particular concern.
Symmetric peripheral gangrene (SPG) is a rare and serious complication of septic shock associated with a high amputation rate and mortality. It is a symmetrical, distal ischemic injury in the absence of major vascular occlusive diseases.2 Herein, we report a case of STSS caused by a SDSE infection that was complicated by rapidly progressive SPG that involved the toes and fingers.
Case Report
A 69-year-old woman was diagnosed as having right breast cancer in 2015 and underwent radical surgery. In 16 August 2022, she developed high fever, pain and swelling in her right upper limb. After 4 days of treatment in Zhongshan Huangpu Hospital her symptoms became worse and she was transferred to the intensive care unit (ICU) of Zhongshan People’s Hospital due to septic shock. She was confused on admission, The examination showed a blood pressure of 80/40 mmHg (100–140/60–90mmHg), a heart rate of 105 beats/min (60–100 beats/min), a breathing frequency of 25 breaths/min (12–20 breaths/min), an armpit temperature of 39°C (36–37°C), and a peripheral oxygen saturation of 94% (95–100%). Laboratory studies revealed white blood cell (WBC) count was 1.17×109/L), platelet count was 70×109/L, hemoglobin was 94 g/L (all decreased), and 85.5% neutrophils, interleukin-6 (IL-6) > 5000 pg/mL, C-reactive protein (CRP) was 164.0 mg/L. Serum creatinine was elevated at 158 µmol/L (Table 1). Enhanced spiral Computed tomography (CT) of the right upper limb showed mild edema of the upper arm and forearm (Figure 1). Vascular color ultrasound of extremities normal.
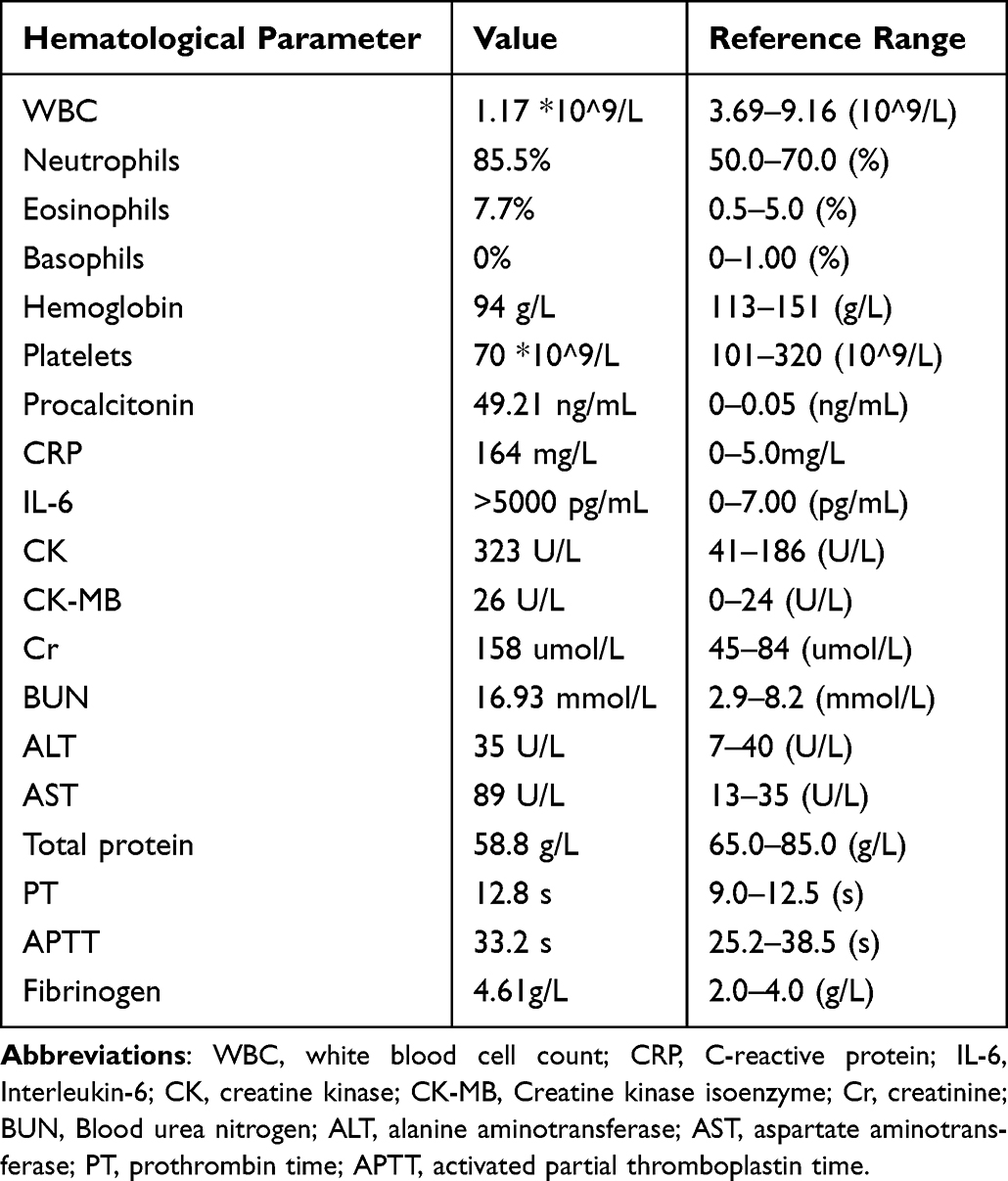 |
Table 1 Laboratory Data at Hospital Admission |
 |
Figure 1 Spiral enhanced computer scan of right arm showed mild edema. |
Considering the soft tissue infection of the right upper limb complicated with septic shock, empirical meropenem (1g, q8h) combined with vancomycin (1g, q12h) via intravenous drip for anti-infection, and norepinephrine was given to maintain an average arterial blood pressure of > 65 mmHg. In order to obtain relevant results as soon as possible, blood samples were submitted for metagenomic next-generation sequencing (mNGS) testing before starting antibiotic use, while traditional blood cultures, sputum cultures, and urine cultures were perfected. Other treatments included rehydration, low-molecular-weight heparin for anticoagulation, drugs for raising platelets and topical magnesium sulfate on the right upper limb. On the second day of treatment, the patient’s procalcitonin decreased to 9.47 pg/mL (Figure 2). The mNGS results indicated the presence of SDSE. However, the patient developed cyanosis of her fingers and toes, large purpura on the skin, and some large blisters (Figure 3a–c). Liver function tests on day 3 showed a steep rise in transaminases (Figure 4) and progression of limb end ischemia was observed (Figures 5a–c), while blood cultures also showed SDSE. Streptococcus was isolated from blood, combined with hypotension, multiple organ dysfunction (including coagulation, liver function, renal function), blister formation, and limb gangrene, and in summary, the patient ‘s symptoms and laboratory data met the criteria for STSS. The results of drug sensitivity showed that the patient was sensitive to penicillin, ceftriaxone, linezolid and vancomycin, and intermediate to clindamycin. However, because the patient had a history of allergy to penicillin he also had renal impairment and thrombocytopenia. In order to avoid further aggravation of renal insufficiency and thrombocytopenia, we chose intravenous drip of ceftriaxone (2g qd) for anti-infection, and anisodamine was added to improve microcirculation in an attempt to reduce acral ischemia. After 10 days of treatment, the patient was transferred from the ICU to the general ward. However, the ischemia at the extremities gradually worsened and amputation was performed after eventually developed SPG (Figure 6a–c).
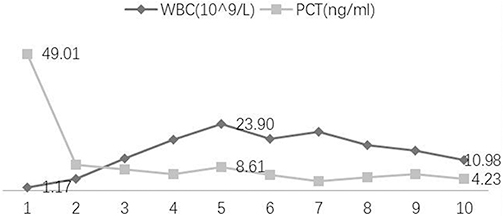 |
Figure 2 Changes of white blood cell (WBC) count and procalcitonin (PCT) indicators in intensive care unit. |
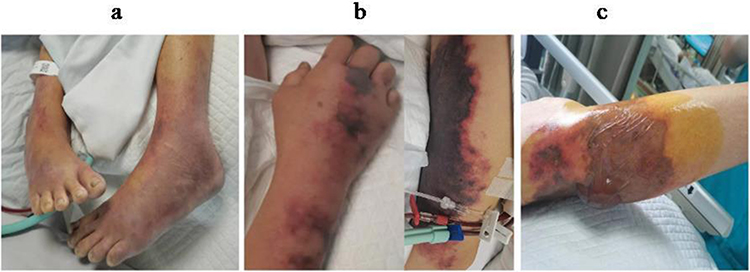 |
Figure 3 Characteristic features of Streptococcal Infected Limbs. Notes: (a) Limb ischemia. (b) Subcutaneous haemorrhage. (c) Giant blisters. |
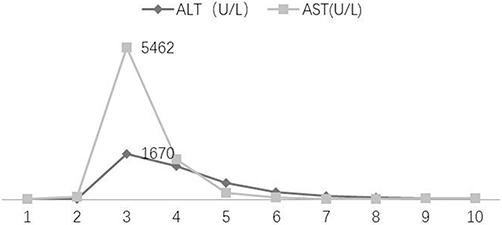 |
Figure 4 Changes in transaminase parameters in the intensive care unit. Abbreviations: ALT, Alanine Aminotransferase; AST, Aspartate Aminotransferase. |
 |
Figure 5 Limb ischemia following SDSE infection. Notes: (a) Lower limb ischemia. (b) Upper limb ischemia. (c) Symmetrical limb ischemia. |
 |
Figure 6 Manifestations of SPG Following SDSE Infection. Notes: (a). Gangrene plantar. (b) Gangrene dorsalis pedis. (c). Upper limb gangrene. |
Discussion
SDSE (group C or G Streptococcus) belongs to the hemolytic Streptococcus type B family. Group C and group G Streptococci are also commonly called pyogenic Streptococci because they are genetically close to pyogenic Streptococci.3 Because SDSE was recognized as a part of the normal flora of the human pharynx, skin, gastrointestinal tract, and vagina,4,5 the colonization of these bacteria has been considered harmless. However, the pathogenicity of SDSE is currently well recognized, and an increasing number of epidemiological studies have indicated that it can cause a variety of diseases similar to those caused by Streptococcus pyogenes. Notably, the number of invasive SDSE infections is reported to be increasing world-wide,6–9 and STSS and bacteremia are of particular concern.10–14 It has also been noted that the incidence of bacteremia is gradually increasing.15,16 However, no large-scale epidemiological studies in China have provided data on SDSE infection. Many studies have found that invasive SDSE infection is more commonly seen as a community-acquired disease in elderly patients with comorbidities.17–19 As the number of elderly people in China is increasing, infection with the invasive Streptococcus dysgalactiae subsp. equisimilis is also likely increase and should attract the attention of clinicians.
The patient reported herein was an elderly woman with a history of breast cancer. Thus, she was at high-risk for invasive SDSE infection, and eventually developed SDSE-induced STSS, and most previous STSS cases were caused by GAS and progressed rapidly with a mortality rate of more than 50%, while in recent years, GCS has also been shown to be one of the main pathogens causing various infectious diseases, and most STSS patients associated with GCS and GGS have underlying diseases such as cardiopulmonary disease, diabetes, malignancy, and renal or hepatic failure.20 In particular, in GGS, SDSE is considered to be the organism causing non-GAS type STSS, and in patients with systemic infections caused by GAS, the incidence of STSS is about 7%, which is higher than that of STSS caused by GGS.21 Antibiotic treatment is necessary for SDSE. SDSE and other large colony C and G Streptococci are usually sensitive to penicillin, which is considered the first choice for the treatment of infections caused by these microorganisms. In our patient, because the patient was allergic to penicillin, we chose ceftriaxone for anti-infection, along with appropriate supportive measures (including fluid resuscitation, administration of vasopressors, and mechanical ventilation), and the patient eventually obtained a favorable outcome, Most cases of STSS are caused by GAS. Among patients with STSS, those with group A Streptococci infection who receive intravenous immunoglobulin (IVIG) have improved outcomes.22 However, there is still a lack of research regarding SDSE infection.
Notably, our patient rapidly developed SPG during the disease progression. SPG can be secondary to many conditions such as sepsis and heart failure, and it typically involves the distal limbs but can also involve the nose, lips, ears, scalp, and genitals. It is often aggravated by factors including warfarin treatment, deep vein thrombosis, hypotension, pressor drug treatment, and anticoagulation system failure.23–27 Recently, acute ischemic hepatitis has been identified as a potential risk factor for symmetric peripheral gangrene,28,29 and may be related to impairment of protein C synthesis caused by acute liver dysfunction. About a quarter of patients with SPG will require amputation, and the condition is associated with a mortality rate of over 50%. Only a few cases of SPG have been reported, and little is known about its epidemiology. Our patient received anticoagulation treatment after diagnosis, but cyanosis appeared at the distal limbs on the second day and progressed despite the anticoagulation treatment. During her hospital course, hypotension, use of vasoactive drugs, and liver dysfunction may have aggravated the ischemia, eventually leading to the development of SPG. This kind of ischemic limb injury can occur rapidly, and even if anticoagulant therapy is begun immediately after the ischemia is recognized it may have not effect.
Conclusion
We reported a case of SDSE-induced STSS complicated with symmetric peripheral gangrene. This case highlights that more attention should be given to pathogenic SDSE infections, and the potential for progression to SPG.
Ethics Approval and Consent
The design and methods of the research are in accordance with the requirements of related regulations and procedures as well as the ethical principles. The study approved by the Ethical Committee of Zhongshan People’s Hospital (Medical Ethics 2023-009). The patient information in this article is anonymous and written informed consent was obtained from the patient’s immediate family for the publication of this case report and accompanying images.
Consent for Publication
Written informed consent was obtained from the patient’s immediate family for the publication of this case report and accompanying images. A copy of the written consent form is available for review by the Editor-in-Chief of this journal. All authors read and approved the final manuscript.
Acknowledgments
We would like to thank the members of our department for their insight and support. Xiaoqing Shen and Hongkai Liang are co-first authors for this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or Critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work. All authors have read and approved the manuscript.
Funding
No funding was received for this study.
Disclosure
The authors declare that they have no conflicts of interests.
References
1. Baracco GJ, Fischetti VA, Novick RP, Ferretti JJ, Portnoy DA, Rood JI.; Infections Caused by Group C and G Streptococcus (Streptococcus dysgalactiae subsp. equisimilis and others): epidemiological and clinical aspects. Microbiol Spectr. 2019;7(2). doi:10.1128/microbiolspec.GPP3-0016-2018
2. Sharma BD, Kabra SR, Gupta B. Symmetrical peripheral gangrene. Trop Doct. 2016;34(1):2–4. doi:10.1177/004947550403400102
3. Jensen A, Kilian M. Delineation of Streptococcus dysgalactiae, its subspecies, and its clinical and phylogenetic relationship to Streptococcus pyogenes. J Clin Microbiol. 2012;50(1):113–126. doi:10.1128/JCM.05900-11
4. Auckenthaler R, Hermans P, Washington J. Group G streptococcal bacteremia: clinical study and review of the literature. Rev Infect Dis. 1983;5(2):196–204. doi:10.1093/clinids/5.2.196
5. Liao C-H, Liu L-C, Huang Y-T, Teng L-J, Hsueh P-R. Bacteremia caused by group G streptococci, Taiwan. Emerg Infect Dis. 2008;14(5):837. doi:10.3201/eid1405.070130
6. Hughes JM, Wilson ME, Brandt CM, Spellerberg B. Human infections due to Streptococcus dysgalactiae subspecies equisimilis. Clin Infect Dis. 2009;49(5):766–772. doi:10.1086/605085
7. Barnham M, Kerby J, Chandler R, Millar M. Group C streptococci in human infection: a study of 308 isolates with clinical correlations. Epidemiol Infect. 1989;102(3):379–390. doi:10.1017/S0950268800030090
8. Gustafson LW, Blaakær J, Helmig RB; Group A streptococci infection. A systematic clinical review exemplified by cases from an obstetric department. Eur J Obstet Gynecol Reprod Biol. 2017;215:33–40. doi:10.1016/j.ejogrb.2017.05.020
9. Broyles LN, Van Beneden C, Beall B, et al. Population-based study of invasive disease due to β-hemolytic streptococci of groups other than A and B. Clin Infect Dis. 2009;48(6):706–712. doi:10.1086/597035
10. Efstratiou A. Pyogenic streptococci of Lancefield groups C and G as pathogens in man. J Appl Microbiol. 1997;83(S1):72S–79S. doi:10.1046/j.1365-2672.83.s1.8.x
11. Loubinoux J, Plainvert C, Collobert G, Touak G, Bouvet A, Poyart C. Adult invasive and noninvasive infections due to Streptococcus dysgalactiae subsp. equisimilis in France from 2006 to 2010. J Clin Microbiol. 2013;51(8):2724–2727. doi:10.1128/JCM.01262-13
12. Kittang B, Bruun T, Langeland N, Mylvaganam H, Glambek M, Skrede S. Invasive group A, C and G streptococcal disease in western Norway: virulence gene profiles, clinical features and outcomes. Clin Microbiol Infect. 2011;17(3):358–364. doi:10.1111/j.1469-0691.2010.03253.x
13. Oppegaard O, Mylvaganam H, Skrede S, Langeland N, Kittang B. Sequence diversity of sicG among group C and G Streptococcus dysgalactiae subspecies equisimilis isolates associated with human infections in western Norway. Eur J Clin Microbiol Infect Dis. 2014;33:273–277. doi:10.1007/s10096-013-1955-0
14. Rantala S. Streptococcus dysgalactiae subsp. equisimilis bacteremia: an emerging infection. Eur J Clin Microbiol Infect Dis. 2014;33:1303–1310. doi:10.1007/s10096-014-2092-0
15. Pérez-Ayala A, Pérez-Molina J, Norman F, et al. Chagas disease in Latin American migrants: a Spanish challenge. Clin Microbiol Infect. 2011;17(7):1108–1113. doi:10.1111/j.1469-0691.2010.03423.x
16. Oppegaard O, Mylvaganam H, Kittang B. Beta-haemolytic group A, C and G streptococcal infections in Western Norway: a 15-year retrospective survey. Clin Microbiol Infect. 2015;21(2):171–178. doi:10.1016/j.cmi.2014.08.019
17. Ekelund K, Skinhøj P, Madsen J, Konradsen H. Invasive group A, B, C and G streptococcal infections in Denmark 1999–2002: epidemiological and clinical aspects. Clin Microbiol Infect. 2005;11(7):569–576. doi:10.1111/j.1469-0691.2005.01169.x
18. Takahashi T, Sunaoshi K, Sunakawa K, et al. Clinical aspects of invasive infections with Streptococcus dysgalactiae ssp. equisimilis in Japan: differences with respect to Streptococcus pyogenes and Streptococcus agalactiae infections. Clin Microbiol Infect. 2010;16(8):1097–1103. doi:10.1111/j.1469-0691.2009.03047.x
19. Takahashi T, Asami R, Tanabe K, et al. Clinical aspects of invasive infection with Streptococcus dysgalactiae subsp. equisimilis in elderly patients. J Infect Chemother. 2010;16(1):68–71. doi:10.1007/s10156-009-0016-1
20. Hashikawa S, Iinuma Y, Furushita M, et al. Characterization of group C and G streptococcal strains that cause streptococcal toxic shock syndrome. J Clin Microbiol. 2004;42(1):186–192. doi:10.1128/JCM.42.1.186-192.2004
21. Takahashi T, Ubukata K, Watanabe H. Invasive infection caused by Streptococcus dysgalactiae subsp. equisimilis: characteristics of strains and clinical features. J Infect Chemother. 2011;17(1):1–10. doi:10.1007/s10156-010-0084-2
22. Kaul R, McGeer A, Norrby-Teglund A, et al. Intravenous immunoglobulin therapy for streptococcal toxic shock syndrome—a comparative observational study. Clin Infect Dis. 1999;28(4):800–807. doi:10.1086/515199
23. Warkentin TE, Cook RJ, Sarode R, Sloane DA, Crowther MA. Warfarin-induced venous limb ischemia/gangrene complicating cancer: a novel and clinically distinct syndrome. Blood J Am Soc Hematol. 2015;126(4):486–493.
24. Warkentin TE, Elavathil LJ, Hayward CP, Johnston MA, Russett JI, Kelton JG. The pathogenesis of venous limb gangrene associated with heparin-induced thrombocytopenia. Ann Intern Med. 1997;127(9):804–812. doi:10.7326/0003-4819-127-9-199711010-00005
25. Molos MA, Hall JC. Symmetrical peripheral gangrene and disseminated intravascular coagulation. Arch Dermatol. 1985;121(8):1057–1061. doi:10.1001/archderm.1985.01660080111027
26. Ghosh S, Bandyopadhyay D, Ghosh A. Symmetrical peripheral gangrene: a prospective study of 14 consecutive cases in a tertiary‐care hospital in eastern India. J Eur Acad Dermatol Venereol. 2010;24(2):214–218. doi:10.1111/j.1468-3083.2009.03329.x
27. Warkentin TE. Ischemic limb gangrene with pulses. N Engl J Med. 2015;373(7):642–655. doi:10.1056/NEJMra1316259
28. Warkentin TE. Anticoagulant failure in coagulopathic patients: PTT confounding and other pitfalls. Expert Opin Drug Saf. 2014;13(1):25–43. doi:10.1517/14740338.2013.823946
29. Warkentin TE. Heparin-induced thrombocytopenia in critically ill patients. In: Seminars in Thrombosis and Hemostasis. Thieme Medical Publishers; 2015:049–060.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.