")
Back to Journals » International Journal of Women's Health » Volume 15
A Case of Strange Arterial Embolism After Uterine Curettage
Authors Jiang W, Xiong Y, Cheng F
Received 15 July 2023
Accepted for publication 30 August 2023
Published 8 September 2023 Volume 2023:15 Pages 1417—1419
DOI https://doi.org/10.2147/IJWH.S426368
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Wenlong Jiang, Yunzhi Xiong, Fangzhou Cheng
Cardiovascular, Shenzhen Yantian District People’s Hospital, Shenzhen, People’s Republic of China
Correspondence: Wenlong Jiang, Cardiovascular, Shenzhen Yantian District People’s Hospital, Wutong Road 2010 Yantian District, Shenzhen, 518081, People’s Republic of China, Tel +86 0755-25215050, Email [email protected]
Abstract: Hysteroscopic local endometrial resection and curettage are common surgical procedures. Postoperative arterial thromboembolism is rare. However, coronary and renal embolism after the procedure has never been reported in the literature, so far. We report a 50-year-old woman who developed arterial thromboembolism 4 hours after local endometrial resection and curettage. Thrombus disappeared after anticoagulant therapy was started as soon as possible. How do strange clots form and by what route do they occur in the arterial system?
Keywords: embolism, uterine curettage, coronary artery, renal artery
Introduction
Hysteroscopy is important for patients with endometrial disease.1 Uterine curettage is also helpful in the diagnosis of endometrial cancer, especially in the case of reproductive needs, early diagnosis and treatment are very important.2,3 The safety and effectiveness of uterus curettage in clinical application have been verified. However, complications such as bleeding and thrombosis occurred in some patients after uterine curettage. Thrombus in the arterial system is rare in patients after uterus curettage, and thromboembolism in both organs is even rarer.
Case Presentation
This case involves a 50-year-old female with presenting symptom of increased menstrual volume for 9 months and irregular vaginal bleeding for 27 days. After 9 months of outpatient treatment with dydrogestrel and norethindrone, irregular vaginal bleeding continued. Transvaginal ultrasonography revealed a low echo area (about 27×16mm in size) in the left lateral wall of the uterus. Interwall myoma was considered. The endometrial line was centered and the endometrial thickness was about 9mm. Hysteroscopy was performed and endometrial polypoid hyperplasia was found in the right anterior wall and right posterior wall of the uterine cavity. The bleeding point was scattered in the local endometrium. The whole uterine cavity was scraped with a scraper, and the endometrium was thickened by unipolar electric incision. The histopathological diagnosis of excision was endometrial polyps and secreted endometrium (Figure 1). Four hours after curettage, upper abdominal pain and left lumbar distension occurred. Electrocardiogram indicated ST segment elevation of the lower wall lead, emergency coronary angiography indicated thromboembolism in the distal left posterior ventricular branch of the right coronary artery, and renal angiography indicated left renal artery branch thromboembolism. Heparin was administered with 100IU/kg anticoagulant therapy. Twenty minutes later, coronary angiography and renal angiography showed that the thrombus disappeared. Coronary and renal arteriography images are shown in Figure 1. ANA series, dsDNA, immunoglobulin and tumor index screening showed no abnormalities. Color ultrasound of lower extremity vein showed no thrombus. Rivaroxaban was subsequently given anticoagulation for 3 months and then discontinued. During 6 months of follow-up, the irregular vaginal bleeding and thromboembolism disappeared without any discomfort.
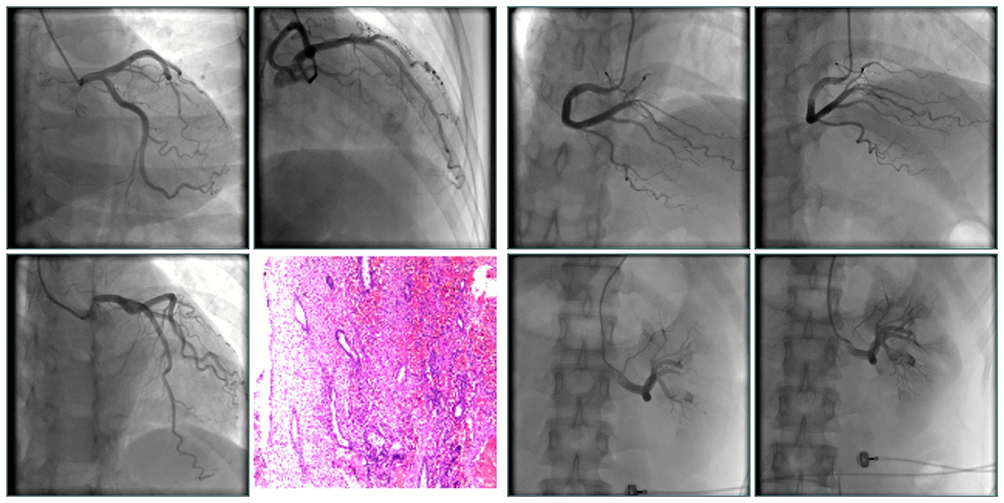 |
Figure 1 Multiposition coronary angiography revealed no stenosis of the left coronary artery. Histopathologic was performed to diagnose endometrial polyps and secretory endometrium. Coronary angiography indicated thromboembolism in the distal left posterior ventricular branch of the right coronary artery, and renal angiography indicated left renal artery branch thromboembolism. Repeat coronary angiography and renal angiography showed the disappearance of thrombus. |
Discussion
The common complications of hysteroscopic local endometrial resection and curettage include uterine perforation, massive bleeding, injury of incomplete curettage, postoperative uterine adhesion and infection, occasional venous thrombosis and a small number of reported uterine arteriovenous malformations.
A recent report has shown that acquired uterine arteriovenous malformation following dilation and curettage.4 However, arterial embolism is rare. Both coronary artery and left renal artery embolism were present in this case. Baik et al had reported that venous thrombus may enter the left atrium through patent foramen ovale and cause arterial embolism.5 Transesophageal atrial color ultrasonography did not reveal the condition of patent foramen ovale in this case. Since the thrombe disappeared immediately after heparinization, we believe that the change of coagulation function after curettage resulted in blood hypercoagulation and thrombosis of distal coronary artery and small branch of renal artery. The change of coagulation function is its pathogenesis. The coagulation function of this patient may be easily affected by surgery, and thromboembolism in similar patients should be vigilant, not only venous thromboembolism, but also the arterial system may occur, which is a rare condition.
Arterial embolism after hysteroscopic local endometrial resection and curettage is rare. This case suggests that coagulation function should be monitored after curettage, and the use of heparin should be considered in patients with hypercoagulable state and high risk of thrombosis. Arterial embolization should be ruled out for postoperative discomfort.
Data Sharing Statement
Please contact correspondence author for data requests.
Ethics Approval and Consent to Participate
Approved by Ethics Committee of Shenzhen Yantian District People’s Hospital.
Consent for Publication
Written informed consent of clinical detail and image publication was obtained from the patient.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Mutlu L, Manavella DD, Gullo G, McNamara B, Santin AD, Patrizio P. Endometrial cancer in reproductive age: fertility-sparing approach and reproductive outcomes. Cancers. 2022;14(21):5187. PMID: 36358604; PMCID: PMC9656291. doi:10.3390/cancers14215187
2. Gullo G, Etrusco A, Fabio M, Cucinella G, Rossi C, Billone V. The reproductive potential of uterus transplantation: future prospects. Acta Biomed. 2022;93(2):e2022138. PMID: 35546000; PMCID: PMC9171877. doi:10.23750/abm.v93i2.12868
3. Gullo G, Perino A, Cucinella G. Open vs. closed vitrification system: which one is safer. Eur Rev Med Pharmacol Sci. 2022;26(4):1065–1067. PMID: 35253158. doi:10.26355/eurrev_202202_28092
4. Manisha A, Tembhare A. Acquired uterine arteriovenous malformation following dilation and curettage: a case report. Pan Afr Med J. 2022;42:71. PMID: 36034014; PMCID: PMC9379433. doi:10.11604/pamj.2022.42.71.35371
5. Baik M, Shim CY, Gwak SY, et al. Patent foramen ovale and risk of recurrence in stroke of determined etiology. Ann Neurol. 2022;92(4):596–606. Epub 2022 Jul 15. PMID: 35753038. doi:10.1002/ana.26449
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.