")
Back to Journals » Infection and Drug Resistance » Volume 16
A Case of Severe Pneumocystis Pneumonia in an HIV-Negative Patient Successfully Treated with Oral Atovaquone
Authors Hirai J , Mori N , Kato H, Asai N, Hagihara M, Mikamo H
Received 2 February 2023
Accepted for publication 16 March 2023
Published 18 March 2023 Volume 2023:16 Pages 1561—1566
DOI https://doi.org/10.2147/IDR.S406904
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Jun Hirai,1,2 Nobuaki Mori,1,2 Hideo Kato,3 Nobuhiro Asai,1,2 Mao Hagihara,4 Hiroshige Mikamo1,2
1Department of Clinical Infectious Diseases, Aichi Medical University Hospital, Nagakute, Aichi, Japan; 2Department of Infection Control and Prevention, Aichi Medical University Hospital, Nagakute, Aichi, Japan; 3Department of Pharmacy, Mie University Hospital, Mie, Japan; 4Department of Molecular Epidemiology and Biomedical Sciences, Aichi Medical University, Nagakute, Aichi, Japan
Correspondence: Jun Hirai, Department of Clinical Infectious Diseases, Aichi Medical University Hospital, 1-1, Yazako-karimata, Nagakute, Aichi, 480-1195, Japan, Tel +81-561-62-3311, Fax +81-561-76-2673, Email [email protected]
Abstract: Currently, atovaquone is not recommended for treating severe Pneumocystis jirovecii pneumonia (PCP) due to insufficient evidence in clinical studies. This report describes a case of severe PCP in a human immunodeficiency virus (HIV)-negative immunosuppressed patient who was successfully treated with oral atovaquone and corticosteroids. A 63-year-old Japanese woman complained of fever and dyspnea for 3 days. She had been treated with oral prednisolone (30 mg/day) for interstitial pneumonia for 3 months without PCP prophylaxis. Although we could not confirm P. jirovecii from the respiratory specimen, a diagnosis of PCP was indicated by marked elevation of serum beta-D-glucan levels and bilateral ground-glass opacities in the lung fields. Based on the arterial blood gas test results (alveolar-arterial oxygen difference > 45 mmHg), the disease status of PCP was defined as severe. Trimethoprim-sulfamethoxazole (SXT) is the first-line drug for treating severe PCP. However, given the patient’s history of SXT-induced toxic epidermal necrolysis, she was administered atovaquone instead of SXT. Her clinical symptoms and respiratory condition gradually improved, with a 3-week treatment showing a good clinical course. Previous clinical studies on atovaquone have only been conducted in HIV-positive patients with mild or moderate PCP. Accordingly, the clinical efficacy of atovaquone for severe PCP cases or PCP in HIV-negative patients remains unclear. There is a rising incidence of PCP among HIV-negative patients, given the increasing number of patients receiving immunosuppressive medications; moreover, atovaquone has less severe side effects than SXT. Therefore, there is a need for further clinical investigation to confirm the efficacy of atovaquone in cases of severe PCP, especially among HIV-negative patients. In addition, it also remains unclear whether corticosteroids are beneficial for severe PCP in non-HIV patients. Thus, the use of corticosteroids in cases of severe PCP in non-HIV patients should also be investigated.
Keywords: Pneumocystis pneumonia, severe, atovaquone, trimethoprim-sulfamethoxazole, corticosteroid
Introduction
Pneumocystis jirovecii pneumonia (PCP), first described as a human pathogen in 1942 by van der Meer and Brug,1 is a potentially life-threatening pulmonary infectious disease that generally occurs in immunocompromised individuals.2 In individuals with human immunodeficiency virus (HIV) infection, the PCP incidence decreased from 29.9 per 1000 person-years during 1994 to 1997 to 3.9 per 1000 person-years during 2003 to 2007,3 whereas approximately 5–15% of HIV-negative immunocompromised individuals developed PCP in the absence of prophylaxis.4–7 Established risk factors for PCP include HIV infection, chemotherapy treatment for a malignant disease, and reception of hematopoietic cells or solid organ transplants.8 The incidence of PCP among patients with HIV has dramatically decreased after the introduction of antiretroviral therapy and PCP prophylaxis with trimethoprim-sulfamethoxazole (SXT). However, there is an increasing incidence of PCP among HIV-negative patients receiving immunosuppressive medications, including corticosteroids and biological products, such as tumor necrosis factor-α inhibitors and methotrexate.9,10 There remain no initiation criteria for PCP prophylaxis among HIV-negative patients receiving immunosuppressive agents.
Currently, 21-day treatment with SXT is the most common therapeutic strategy for PCP in both HIV-infected and HIV-negative patients;11,12 however, some patients cannot tolerate this treatment due to severe allergies, including Stevens–Johnson syndrome and toxic epidermal necrolysis (TEN). Atovaquone is an alternative drug for PCP treatment and is better tolerated than SXT; however, it is currently not recommended for severe PCP due to insufficient evidence.13 This report describes a case of severe PCP in an HIV-negative immunosuppressed patient with a history of SXT-induced TEN who was successfully treated with oral atovaquone alone.
Case Report
A 63-year-old Japanese woman complained of fever, dyspnea (especially on exertion), and a non-productive cough that had developed 3 days earlier. She had undergone a 3-month treatment with oral steroids for interstitial pneumonia related to mixed connective-tissue disease. She had a history of life-threatening TEN caused by SXT administered for PCP prophylaxis 2 months earlier, which was treated using two courses of steroid pulse therapy and several plasma exchanges. Subsequently, she was started on atovaquone for PCP prophylaxis; however, it was discontinued due to gastrointestinal side effects (nausea and anorexia). Therefore, she did not receive chemoprophylaxis for PCP. Moreover, she had a medical history of anaphylactic shock caused by ganciclovir treatment for cytomegalovirus (CMV) enteritis. Upon presentation to our hospital, her consciousness was clear (Glasgow Coma Scale, E4V5M6).14 Her vital signs were as follows: blood pressure, 117/78 mmHg; heart rate, 90 beats/min; body temperature, 37.8°C; respiratory rate, 26 breaths/min; and SpO2, 85% in room air. With nasal oxygen ventilation at 2 L/min, the findings of arterial blood gas analysis were as follows: pH, 7.464; pCO2, 33.4 mmHg; pO2, 94.7 mmHg; and HCO3−, 22.4 mEq/L; PaO2/FiO2 ratio, 326 mmHg, and alveolar-arterial oxygen difference (A-aDO2), 70.3 mmHg. Physical examination revealed no wheezes or crackles on chest auscultation. Blood tests revealed a normal leukocyte count of 6700 cells/µL (normal range: 3300–8600 cells/µL), an elevated C-reactive protein level of 3.75 mg/dL (normal: ≤0.04 mg/dL), lactate dehydrogenase level of 499 IU/L (normal range:124–222 IU/L), and KL-6 level of 595 IU/L (normal: ≤500 IU/L). Chest radiography revealed a bilateral, diffuse, and symmetric reticular interstitial shadow (Figure 1A). Additionally, chest computed tomography revealed a bilateral, asymmetric, and patchy mosaic appearance, as well as ground-glass opacities in the lung subpleural peripheral regions (Figure 1B and C). Based on these findings, the following differential diagnoses were considered: PCP, CMV pneumonia, and pulmonary edema due to heart failure. An additional blood test showed an increased level (155 pg/mL, normal: ≤20 pg/mL) of beta-D-glucan (a cell wall component of most fungi, including Pneumocystis jirovecii), but negative results for CMV antigenemia and IgM antibodies. The HIV antibody test results were negative, and the CD4 count was normal. Transthoracic echocardiography revealed normal cardiac function. These findings were strongly suggestive of PCP. Due to hypoxemia, she did not undergo bronchoscopy for bronchoalveolar lavage (BAL) to identify Pneumocystis jirovecii. Based on the A-aDO2 level (>45 mmHg), the disease status of PCP was considered severe. As primaquine is not registered for treating PCP in Japan, we initially recommended intravenous pentamidine, which is a recommended second-line drug for PCP treatment, given her history of SXT-induced TEN. However, she refused to receive pentamidine, given its potential side effects, including kidney damage, hypotension, and ventricular arrhythmias. This could be attributed to her previous experience with adverse reactions to various medications, which increased her anxiety regarding therapeutic agents. Given her severe respiratory status, the attending physician again persuaded the patient to receive PCP treatment. Finally, she agreed to take atovaquone, which had been previously discontinued due to nausea and anorexia; however, we explained that atovaquone is recommended as a first-line drug for mild, rather than severe, PCP. Additionally, we recommended administering methylprednisolone (mPSL) for hypoxia, which she accepted. Accordingly, atovaquone 750 mg twice a day and mPSL 80 mg/day were started. She gradually recovered and gained a stable respiratory condition (nasal oxygen was discontinued on the fifth day of treatment). There were no gastrointestinal symptoms caused by atovaquone. She received intravenous mPSL and oral atovaquone for 21 days at a therapeutic dose. At discharge, oral atovaquone was switched to a prophylactic dose (1500 mg once daily), while mPSL was switched to oral prednisolone, which was gradually tapered off (Figure 2).
 |
Figure 1 Chest X-ray image showing a bilateral diffuse symmetric reticular interstitial shadow (A). A chest computed tomography scan showing bilateral asymmetric patchy mosaic appearance and ground-glass opacities in the lung subpleural peripheral regions (B and C). |
 |
Figure 2 Clinical course of the patient in the present case. |
Discussion
We encountered a case of severe PCP successfully treated with oral atovaquone alone in an HIV-negative immunosuppressed patient. The incidence of PCP among HIV-negative patients is increasing, given the rising number of individuals receiving immunosuppressants.15 In Norway, the regional incidence rate of PCP among immunocompromised HIV-negative patients doubled from 5.0 cases per 100,000 person-years in 2007 to 10.8 in 2017.16 Moreover, from January 2010 to December 2016, >90% of patients with PCP in Japan were HIV negative (n = 4293).17 Among these patients, the most common comorbidity was hematologic malignancy (31%), followed by rheumatic/collagen diseases (26%) and solid organ tumors (18%); additionally, corticosteroids were the most commonly used drugs preceding PCP occurrence (81.2%).17 The most critical risk factor for PCP among HIV-negative patients is glucocorticoid treatment.5 We assumed that our patient developed PCP since she did not take prophylactic medication for PCP for 3 months while receiving oral glucocorticoids for treating interstitial pneumonia.
The disease status of PCP can be graded as mild, moderate, or severe based on the A-aDO2 level (mild, A-aDO2 <35 mmHg; moderate, 35 ≤ A-aDO2 ≤ 45 mmHg; and severe, A-aDO2 >45 mmHg).11 SXT is the first-line treatment of choice for PCP regardless of the disease status or HIV status; however, there remains no sufficient evidence to recommend it for HIV-negative patients.18 Selection of alternative treatment regimens for patients with PCP who cannot take SXT is partly dependent on the disease severity.19 Alternative therapeutic agents for severe PCP include intravenous pentamidine, clindamycin plus primaquine, and atovaquone.20,21 However, atovaquone is not recommended for severe PCP due to insufficient evidence. A double-blind, multicenter trial conducted in the United States found no difference in the clinical efficacy of atovaquone and SXT for PCP treatment; however, the study population only comprised patients with mild-to-moderate PCP who had acquired immunodeficiency syndrome (AIDS).22 In addition, the clinical efficacy of atovaquone and SXT is comparable (99 of 160 patients [62%] in the atovaquone cohort and 103 of 162 patients [64%] in the SXT cohort, p = 0.751). Moreover, although there were more deaths overall after 8 weeks of treatment in the atovaquone group (13 patients [8.1%] vs 4 patients [2.5%], p = 0.023), the proportion of deaths due to PCP was not different between the two groups (4 patients [2.5%] vs 1 patient [0.6%], p = 0.171). Thus, atovaquone could be the first-line drug not only in severe cases, as in the present case, but also in mild and moderate cases. Another study showed that atovaquone had a non-significantly higher successful treatment rate than intravenous pentamidine (57% vs 40%, p = 0.085); however, this study only included patients with mild-to-moderate PCP who had AIDS.23 Further studies are warranted to determine whether atovaquone can be used for patients with severe PCP, especially HIV-negative patients.
In our case, glucocorticoids were administered in addition to atovaquone for PCP treatment; however, it is still unclear whether corticosteroids are beneficial for HIV-negative patients with PCP.13 Glucocorticoids adjunctive to the anti-Pneumocystis agents are recommended for moderate or severe PCP in patients with HIV since this treatment regimen improves clinical outcomes and mortality without increasing the risk of other opportunistic infections by reducing pulmonary inflammation and preventing oxidative deterioration.24 However, the efficacy of adjunctive glucocorticoids for PCP treatment in HIV-negative patients remains unclear. Nonetheless, given the fulminant course and high mortality of PCP among HIV-negative patients, some researchers have recommended glucocorticoid therapy for patients with PaO2 <70 mmHg or A-aDO2 gradient ≥35 mmHg.24–26 A meta-analysis of 16 retrospective observational studies on PCP in HIV-negative patients found that corticosteroids in addition to anti-Pneumocystis agents were associated with decreased mortality among patients with respiratory failure (odds ratio, 0.63; 95% confidence interval, 0.41–0.95).27 Therefore, corticosteroids should be considered for severe PCP in HIV-negative patients, depending on their condition and background.
To our knowledge, only one report has described the use of oral atovaquone to treat severe PCP.28 The patient was a 64-year-old woman with glucose-6-phosphate dehydrogenase (G6PD) enzyme deficiency who complained of fever, deteriorating exertional dyspnea, and non-productive cough for 2 days. She developed PCP due to the long-term use of corticosteroids for brain tumors. She was started on atovaquone instead of SXT, given the risk of hemolytic anemia in patients with G6PD deficiency upon exposure to SXT. The patient was completely cured (Table 1). Therefore, atovaquone may be a safe alternative treatment regimen for patients with a severe allergy to SXT or G6PD deficiency. In addition, SXT often involves adverse events, such as nephrotoxicity, bone marrow depression, and skin rash, which could impede treatment completion. Compared with SXT, atovaquone has several advantages, including tolerable side effects and fewer adverse reactions, and thus clinical studies are warranted to examine the efficacy of atovaquone against severe PCP.
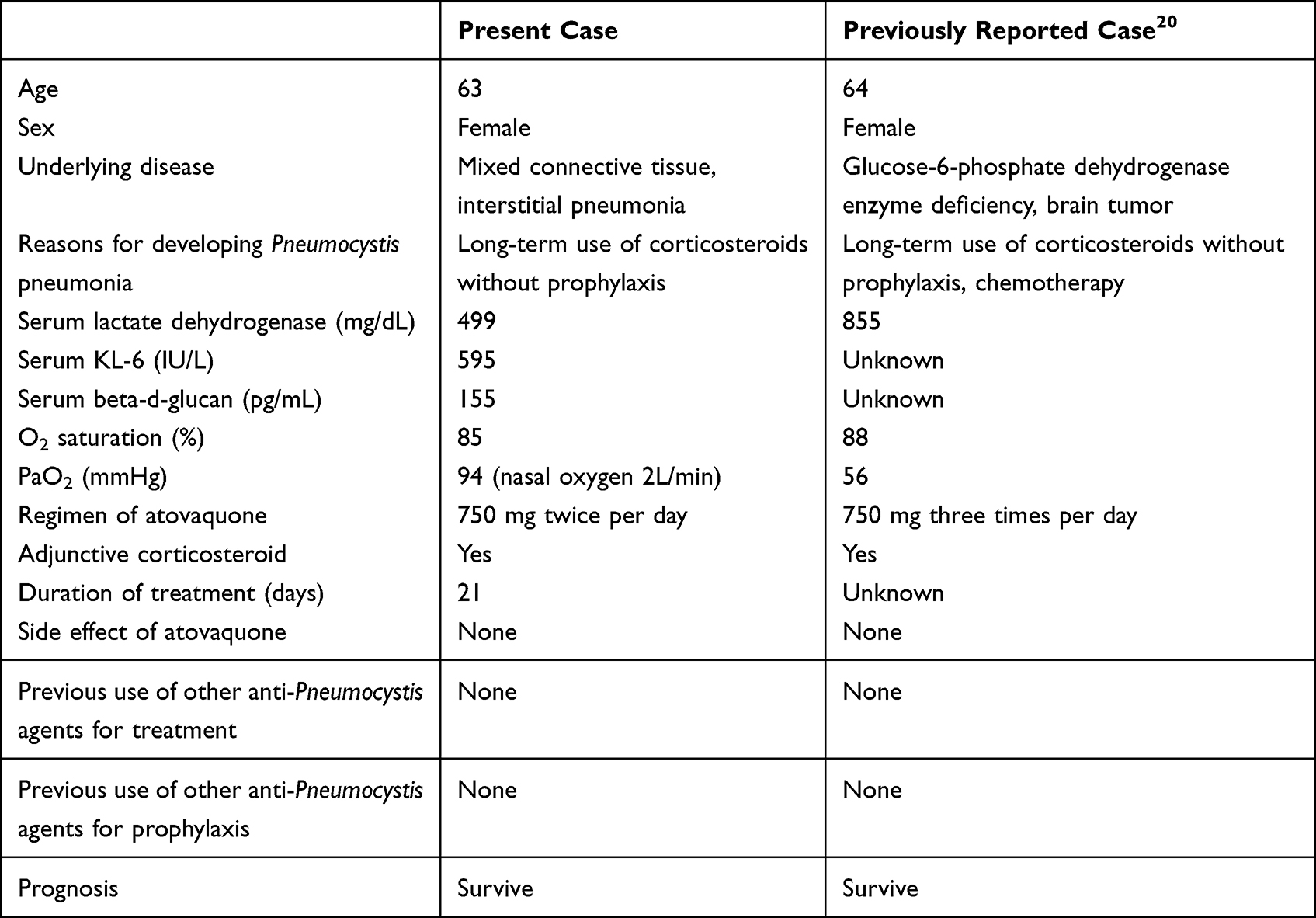 |
Table 1 Clinical Characteristics of the Present Patient and an Earlier Patient with Severe PCP |
This study had some limitations. First, this is a single case report with minimal data; nonetheless, it is important to report such cases. To our knowledge, this is the second case report describing the successful use of atovaquone as a first-line agent in an HIV-negative patient with severe PCP (A-aDO2 level >45 mmHg). Further studies are warranted to confirm the efficacy of atovaquone against severe PCP. Second, we did not perform a BAL to identify Pneumocystis jirovecii. Therefore, this was a presumptive PCP case. However, a diagnosis of PCP was strongly indicated by the long-term administration of glucocorticoids, elevation of serum beta-D-glucan, a typical computed tomography image of PCP, and an improved clinical course with atovaquone treatment.
Conclusion
We encountered a case of severe PCP in an HIV-negative patient treated with oral atovaquone alone, which yielded favorable outcomes. Since atovaquone has fewer severe side effects than SXT, further evidence is required to establish its efficacy against severe PCP, especially in HIV-negative patients. Moreover, further studies are warranted to confirm the efficacy of adjunctive corticosteroids against severe PCP in HIV-negative patients.
Abbreviations
A-aDO2, alveolar-arterial oxygen difference; AIDS, acquired immunodeficiency syndrome; CMV, cytomegalovirus; G6PD, glucose-6-phosphate dehydrogenase; HIV, human immunodeficiency virus; mPSL, methylprednisolone; PCP, Pneumocystis jirovecii pneumonia; SXT, trimethoprim-sulfamethoxazole; TEN, toxic epidermal necrolysis.
Data Sharing Statement
The data is available upon request.
Ethics and Consent
The patient was informed of the publication of this case report and signed a letter of consent. The present case did not require ethics committee approval based on the Japanese ethical guidelines for clinical research to publish case details.
Acknowledgments
We appreciate Editage for the English language editing.
Author Contributions
All authors meet the ICMJE authorship criteria. All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors and co-workers did not receive any specific funding.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Apostolopoulou A, Fishman JA. The pathogenesis and diagnosis of Pneumocystis jiroveci pneumonia. J Fungi. 2022;8(11):1167.
2. Thomas CF, Limper AH. Pneumocystis pneumonia. N Engl J Med. 2004;350(24):2487–2498. doi:10.1056/NEJMra032588
3. Buchacz K, Baker RK, Palella FJ, et al. AIDS-defining opportunistic illnesses in US patients, 1994–2007: a cohort study. AIDS. 2010;24(10):1549–1559. doi:10.1097/QAD.0b013e32833a3967
4. Sepkowitz KA. Opportunistic infections in patients with and patients without Acquired Immunodeficiency Syndrome. Clin Infect Dis. 2002;34(8):1098–1107. doi:10.1086/339548
5. Sepkowitz KA, Brown AE, Armstrong D. Pneumocystis carinii pneumonia without acquired immunodeficiency syndrome. More patients, same risk. Arch Intern Med. 1995;155(11):1125–1128. doi:10.1001/archinte.1995.00430110015002
6. Gerrard JG. Pneumocystis carinii pneumonia in HIV-negative immunocompromised adults. Med J Aust. 1995;162(5):233–235. doi:10.5694/j.1326-5377.1995.tb139873.x
7. Radisic M, Lattes R, Chapman JF, et al. Risk factors for Pneumocystis carinii pneumonia in kidney transplant recipients: a case-control study. Transpl Infect Dis. 2003;5(2):84–93. doi:10.1034/j.1399-3062.2003.00018.x
8. Catherinot E, Lanternier F, Bougnoux ME, Lecuit M, Couderc LJ, Lortholary O. Pneumocystis jirovecii Pneumonia. Infect Dis Clin North Am. 2010;24(1):107–138. doi:10.1016/j.idc.2009.10.010
9. Harigai M, Koike R, Miyasaka N; Pneumocystis Pneumonia under Anti-Tumor Necrosis Factor Therapy (PAT) Study Group. Pneumocystis pneumonia associated with infliximab in Japan. N Engl J Med. 2007;357(18):1874–1876. doi:10.1056/NEJMc070728
10. Ohmura SI, Homma Y, Masui T, Miyamoto T. Factors associated with Pneumocystis jirovecii pneumonia in patients with rheumatoid arthritis receiving methotrexate: a single-center retrospective study. Intern Med. 2022;61(7):997–1006. doi:10.2169/internalmedicine.8205-21
11. Sax PE. Treatment and prevention of Pneumocystis infection in patients with HIV. UptoDate; 2022. Available from: https://www.uptodate.com/contents/treatment-and-prevention-of-pneumocystis-pneumonia-in-patients-without-hiv?search=%E3%83%8B%E3%83%A5%E3%83%BC%E3%83%A2%E3%82%B7%E3%82%B9%E3%83%81%E3%82%B9&source=search_result&selectedTitle=2~150&usage_type=default&display_rank=2#.
12. Charles F, Thomas MHL. Treatment and prevention of Pneumocystis pneumonia in patients without HIV. UpToDate; 2022. Available from: https://www.uptodate.com/contents/treatment-and-prevention-of-pneumocystis-pneumonia-in-patients-without-hiv?search=%E3%83%8B%E3%83%A5%E3%83%BC%E3%83%A2%E3%82%B7%E3%82%B9%E3%83%81%E3%82%B9%E8%82%BA%E7%82%8E&source=search_result&selectedTitle=2~150&usage_type=default&display_rank=2.
13. Tasaka S. Recent advances in the diagnosis and management of Pneumocystis pneumonia. Tuberc Respir Dis. 2020;83(2):132–140.
14. Teasdale G, Maas A, Lecky F, Manley G, Stocchetti N, Murray G. The Glasgow Coma Scale at 40 years: standing the test of time. Lancet Neurol. 2014;13(8):844–854.
15. Matsumura Y, Shindo Y, Iinuma Y, et al. Clinical characteristics of Pneumocystis pneumonia in non-HIV patients and prognostic factors including microbiological genotypes. BMC Infect Dis. 2011;11:76.
16. Grønseth S, Rogne T, Hannula R, Åsvold BO, Afset JE, Damås JK. Epidemiological and clinical characteristics of immunocompromised patients infected with Pneumocystis jirovecii in a twelve-year retrospective study from Norway. BMC Infect Dis. 2021;21(1):659.
17. Shoji K, Michihata N, Miyairi I, Matsui H, Fushimi K, Yasunaga H. Recent epidemiology of Pneumocystis pneumonia in Japan. J Infect Chemother. 2020;26(12):1260–1264. doi:10.1016/j.jiac.2020.07.006
18. Weyant RB, Kabbani D, Doucette K, Lau C, Cervera C. Pneumocystis jirovecii: a review with a focus on prevention and treatment. Expert Opin Pharmacother. 2021;22(12):1579–1592.
19. Limper AH, Knox KS, Sarosi GA, et al. An official American Thoracic Society statement: treatment of fungal infections in adult pulmonary and critical care patients. Am J Respir Crit Care Med. 2011;183(1):96–128.
20. Masur H, Brooks JT, Benson CA, et al. Prevention and treatment of opportunistic infections in HIV-infected adults and adolescents: updated guidelines from the Centers for Disease Control and Prevention, National Institutes of Health, and HIV Medicine Association of the Infectious Diseases Society of America. Clin Infect Dis. 2014;58(9):1308–1311.
21. Ryom L, De Miguel R, Cotter AG, et al. Major revision version 11.0 of the European AIDS Clinical Society Guidelines 2021. HIV Med. 2022;23(8):849–858. doi:10.1111/hiv.13268
22. Hughes W, Leoung G, Kramer F, et al. Comparison of atovaquone (566C80) with trimethoprim-sulfamethoxazole to treat Pneumocystis carinii pneumonia in patients with AIDS. N Engl J Med. 1993;328(21):1521–1527. doi:10.1056/NEJM199305273282103
23. Dohn MN, Weinberg WG, Torres RA, et al. Oral atovaquone compared with intravenous pentamidine for Pneumocystis carinii pneumonia in patients with AIDS. Atovaquone Study Group. Ann Intern Med. 1994;121(3):174–180. doi:10.7326/0003-4819-121-3-199408010-00003
24. Ewald H, Raatz H, Boscacci R, Furrer H, Bucher HC, Briel M. Adjunctive corticosteroids for Pneumocystis jiroveci pneumonia in patients with HIV infection. Cochrane Database Syst Rev. 2015;2015(4):CD006150. doi:10.1002/14651858.CD006150.pub2
25. Moon SM, Kim T, Sung H, et al. Outcomes of moderate-to-severe Pneumocystis pneumonia treated with adjunctive steroid in non-HIV-infected patients. Antimicrob Agents Chemother. 2011;55(10):4613–4618. doi:10.1128/AAC.00669-11
26. Delclaux C, Zahar JR, Amraoui G, et al. Corticosteroids as adjunctive therapy for severe Pneumocystis carinii pneumonia in non-human immunodeficiency virus-infected patients: retrospective study of 31 patients. Clin Infect Dis. 1999;29(3):670–672. doi:10.1086/598651
27. Ding L, Huang H, Wang H, He H. Adjunctive corticosteroids may be associated with better outcome for non-HIV Pneumocystis pneumonia with respiratory failure: a systemic review and meta-analysis of observational studies. Ann Intensive Care. 2020;10(1):34. doi:10.1186/s13613-020-00649-9
28. Douzinas EE, Flevari K, Andrianakis I, Betrosian AP. Oral atovaquone for the treatment of severe Pneumocystis jirovecii pneumonia in a patient with glucose-6-phosphate dehydrogenase deficiency. Scand J Infect Dis. 2010;42(1):76–78. doi:10.3109/00365540903321606
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.