")
Back to Journals » Infection and Drug Resistance » Volume 16
A Case of Multidrug-Resistant Klebsiella pneumoniae Treated with Carrimycin
Authors Zhu W, Tian Y, Xiang L, Cao L, He L
Received 3 February 2023
Accepted for publication 12 April 2023
Published 20 April 2023 Volume 2023:16 Pages 2365—2369
DOI https://doi.org/10.2147/IDR.S407076
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Wenjun Zhu,* Yaping Tian,* Lin Xiang, Linna Cao, Lirong He
Department of Respiratory and Critical Care Medicine, The Second Affiliated Hospital of Nanchang University, Nanchang, Jiangxi, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Lirong He, Department of Respiratory and Critical Care Medicine, The Second Affiliated Hospital of Nanchang University, Nanchang, Jiangxi, 330006, People’s Republic of China, Tel +86 18170905103, Fax +86 0791 86311242, Email [email protected]
Abstract: One of the most pressing emerging issues in bacterial resistance is multidrug-resistant Klebsiella pneumoniae. The treatment of K. pneumoniae infections is often problematic because of the lack of available therapeutic options, leading to negative effects on morbidity, mortality, and healthcare-associated costs. Carrimycin is a macrolide antibiotic with good antibacterial effects. In this study, we report a patient diagnosed with multidrug-resistant K. pneumoniae infection who was treated with carrimycin. The patient presented with cough, expectoration, dyspnea, and severe hypoxemia requiring noninvasive ventilation. We successively used a variety of antibiotics, including meropenem, tigecycline, and polymyxin, with unsatisfactory results. Finally, we used carrimycin, and the patient’s condition improved, resulting in hospital discharge. Therefore, for patients with multidrug-resistant K. pneumoniae infection that does not respond to conventional anti-infective treatments, carrimycin can be considered a treatment option.
Keywords: carrimycin, Klebsiella pneumoniae, multidrug-resistant
Introduction
Klebsiella pneumoniae is one of the most common pathogens causing infections, including urinary tract infections, pneumonia and bacteremia.1 The global prevalence of multidrug-resistant K. pneumoniae (MDR-KP) colonization is 0.13% to 22%, with a combined prevalence of 5.43% (3.73–7.42%).2 Meanwhile, infection caused by MDR-KP has a high mortality rate, and it is often associated with an increased risk of inadequate antibiotic treatment.3 In recent years, combination therapy including colistin, fosfomycin, high-dose meropenem, tigecycline, and aminoglycosides has been the most widely used strategy, but the efficacy is not ideal. In recent decades, new antimicrobials against MDR-KP have been developed, and they are currently in various stages of clinical research.4
Carrimycin, also known as bitespiramycin, is a new genetically engineered macrolide. It is mainly composed of isovalerylspiramycin I–III, and it contains a small amount of other 4″-acylspiramycin components.5,6 It has an antibacterial spectrum similar to spiramycin but better pharmacokinetic characteristics.7 First, carrimycin is a macrolide antibacterial drug, that can inhibit bacterial protein synthesis by blocking the activity of peptidyl transferase in the 50s ribosome, thus achieving bacterial inhibition. Meanwhile, compared with other macrolide antibiotics, carrimycin and its metabolites exhibit stronger lipid solubility and a longer half-life after isovaleryl modification, which contribute to their penetration and persistence in tissues. This property gives carrimycin stronger antibacterial activity than other macrolide antibiotics.8 Second, macrolides have dual antibacterial and immunomodulatory properties.9,10 Carrimycin promotes neutrophil migration to sites of inflammation and enhances macrophage phagocytosis to regulate host immunity. Based on these potential antimicrobial properties, carrimycin has been approved by the China Food and Drug Administration (H20190029) for the treatment of acute tracheal bronchitis.
In this study, we describe a case of MDR-KP infection treated with carrimycin. To the best of our knowledge, there are few reports on the treatment of MDR-KP infection with this drug.
Case Presentation
An 82-year-old man who had been diagnosed with MDR-KP infection presented to our hospital with complaints of repeated coughing and expectoration for more than 20 years and a current recurrence of more than 20 days. His past medical history included chronic obstructive pulmonary disease and Parkinson’s disease. Rales could be heard in his lungs. Chest high-resolution computed tomography revealed a patchy high-density shadow with an unclear boundary and infectious disease in the right lung (Figure 1). He was transferred to our hospital for further treatment. Laboratory examination detected an elevated white blood cell count and C-reactive protein level. MDR-KP was detected repeatedly in sputum culture. Based on the presence of inflammation, the imaging findings, and sputum culture, we made a diagnosis of MDR-KP infection.
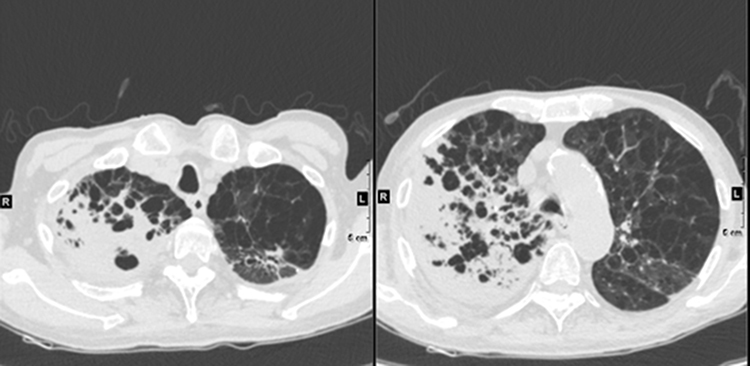 |
Figure 1 Chest high-resolution computed tomography revealed a patchy high-density shadow with an unclear boundary and infectious disease in the right lung. |
Because the principal treatment for K. pneumoniae pneumonia is anti-infective treatment and sputum drainage, we empirically treated him with meropenem 1 g every 8 h and tigecycline 50 mg every 12 h. Three days after admission, MDR-KP grew in the patient’s sputum cultures. Despite treatment with antibiotics, cough, yellow purulent sputum, and appetite reduction persisted, and the organism continued to grow in sputum cultures. The bacterium was susceptible to tigecycline, amikacin, and polymyxin. We switched the treatment to tigecycline and amikacin based on drug sensitivity testing because of clinical deterioration (Table 1). On day 10, chest X-ray revealed further aggravation of the pulmonary exudative lesions. We changed the antibiotics to tigecycline and polymyxin. After 1 week of tigecycline and polymyxin treatment, the patient’s cough and yellow purulent sputum persisted, and chest X-ray disclosed no reduction of the lesions (Figure 2A). According to the consultation opinion of the Clinical Drug Department, we adjusted the anti-infective regimen to meropenem and carrimycin. We administered meropenem and carrimycin for 10 days, followed by 10 days of carrimycin monotherapy. After 4 weeks of antibiotic therapy, the patient was discharged after his condition improved.
 |
Table 1 Drug Resistance of Multidrug-Resistant Klebsiella pneumoniae |
 |
Figure 2 Chest X-ray. (A) Before treatment with carrimycin. (B) After 4 weeks of treatment with carrimycin. |
Over the course of carrimycin treatment, the patient experienced improvement of his cough, expectoration, chest congestion, and appetite. After 4 weeks of carrimycin treatment, repeated chest computed tomography demonstrated that the lesion had shrank (Figure 2B). After carrimycin therapy, the patient reported an ability to resume his daily routine, which was not possible prior to this treatment. He was followed up for 8 weeks after the completion of therapy without incident and with apparent symptom resolution. Inflammatory markers (C-reactive protein) decreased over the treatment course, whereas this white blood cell count rose slightly, which could have been related to the acute exacerbation of chronic obstructive pulmonary disease during glucocorticoid therapy. His clinical course is presented in Figure 3.
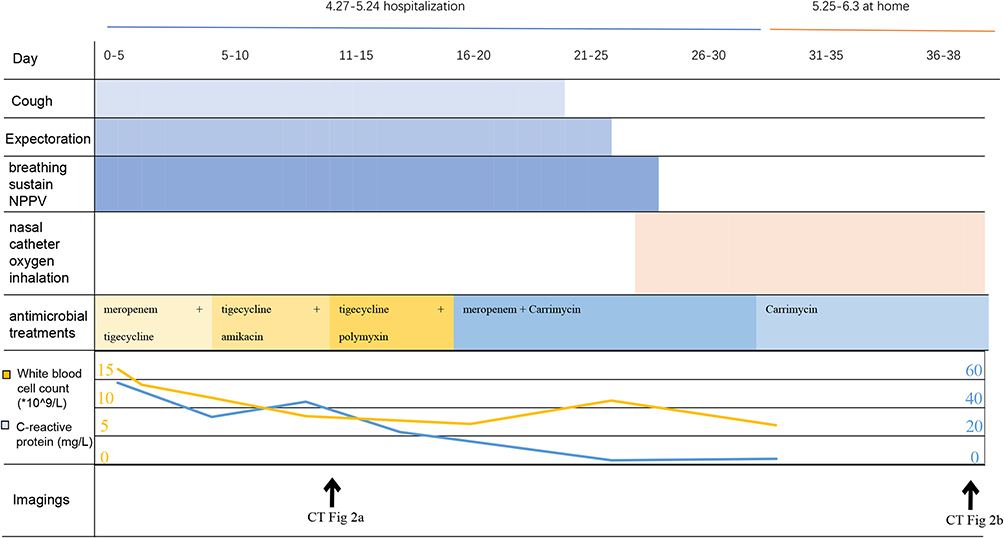 |
Figure 3 Clinical course. Abbreviation: CT, computed tomography. |
Discussion
We presented a rare case of MDR-KP infection treated with carrimycin. Most previously reported cases required combination therapies. Combination therapies including high-dose meropenem, colistin, fosfomycin, tigecycline, and aminoglycosides are widely used. However, because of various drug resistance mechanisms, the therapeutic effect is not satisfactory. Our case was successfully treated with carrimycin, which might be an alternative therapy in patients who are not candidates for conventional treatment because of suboptimal efficacy.
An analysis of the patient’s treatment revealed several interesting issues. First, the mechanism of carrimycin, a novel macrolide antibiotic, for the treatment of MDR-KP is unclear. The possible mechanisms for the effectiveness of carrimycin can be described from the following two aspects. First, carrimycin has a similar mechanism of bacterial inhibition as macrolide antibiotics while benefiting from its superior structure; therefore, it has stronger antibacterial activity than other macrolide antibiotics. Second, macrolide antibiotics have immunomodulatory effects,11 which can enhance the host immune response and thus increase its bactericidal effect. Critical illness is related to immune dysregulation, which is characterized by concurrent hyperinflammation and immune suppression. Pathogen-associated molecular patterns and damage-associated molecular patterns expressed by microorganisms are released from injured tissues, and they bind to pattern recognition receptors such as Toll-like receptors (TLRs) and Nod-like receptors to initiate intense inflammatory responses, leading to organ failure.12,13 Conversely, macrolides reduce TLR expression on the surface of dendritic cells and macrophages to exert their immunomodulatory effects.14 In addition, macrolides dampen hyperinflammation by reducing pro-inflammatory cytokine release and limiting immune cell migration.15 Carrimycin, as a novel macrolide derivative, might have immunomodulatory effects, which could be one of its potential antibacterial mechanisms. Another concern is whether there carrimycin has synergistic effects on antibiotics to which K. pneumoniae is resistant and the potential mechanisms of action. Some scholars have started to examine this issue and have already conducted relevant studies, and we can expect to obtain the results of such studies in the future. Finally, recent studies have revealed that carrimycin is also affective against COVID-19 and tumors.16–18 We believe that with the extensive clinical use and study of carrimycin, the clinical indications of carrimycin will be further expanded.
This case report had some limitations. First, bacterial molecular genotypic and virulence typing of this strain was not performed. Second, multicenter, large-sample studies are needed to further confirm the efficacy and safety of carrimycin alone or in combination for the treatment of MDR-KP.
Conclusion
The treatment of MDR-KP infection has emerged as a new challenge. This case report emphasized that when conventional treatment is not effective, carrimycin could represent an alternative treatment.
Compliance with Ethics Guidelines
Informed consent was obtained from the patient for publication of all related materials. This study was approved by the Medical Research Ethics Committee of the Second Affiliated Hospital of Nanchang University (ethical approval no. 2023-001).
Acknowledgment
We thank Joe Barber Jr., PhD, from Liwen Bianji (Edanz) (www.liwenbianji.cn) for editing the English text of a draft of this manuscript. Wenjun Zhu and Yaping Tian are co-first authors.
Disclosure
All authors declare that we have no conflict of interest.
References
1. Stojowska-Swedrzynska K, Lupkowska A, Kuczynska-Wisnik D, Laskowska E. Antibiotic heteroresistance in Klebsiella pneumoniae. Int J Mol Sci. 2022;23(1):449.
2. Tesfa T, Mitiku H, Edae M, Assefa N. Prevalence and incidence of carbapenem-resistant K. pneumoniae colonization: systematic review and meta-analysis. Syst Rev. 2022;11(1). doi:10.1186/s13643-022-02110-3
3. Bassetti M, Righi E, Carnelutti A, Graziano E, Russo A. Multidrug-resistant Klebsiella pneumoniae: challenges for treatment, prevention and infection control. Expert Rev Anti Infect Ther. 2018;16(10):749–761. doi:10.1080/14787210.2018.1522249
4. Galani I, Karaiskos I, Giamarellou H. Multidrug-resistant Klebsiella pneumoniae: mechanisms of resistance including updated data for novel beta-lactam-beta-lactamase inhibitor combinations. Expert Rev Anti Infect Ther. 2021;19(11):1457–1468. doi:10.1080/14787210.2021.1924674
5. He W, Yang C, Zhao X, Wang Y. Antimicrobial activity of bitespiramycin, a new genetically engineered macrolide. Bioorg Med Chem Lett. 2017;27(19):4576–4577. doi:10.1016/j.bmcl.2017.08.046
6. Wang MJ, Xue J, Zou WB, et al. Identification of the components of bitespiramycin by liquid chromatography-mass spectrometry. J Pharm Biomed Anal. 2012;66:402–410. doi:10.1016/j.jpba.2012.03.013
7. Ma C, Zhou H, Li J, et al. Construction of 4-isovalerylspiramycin-I-producing strain by in-frame partial deletion of 3-O-acyltransferase gene in Streptomyces spiramyceticus WSJ-1, the bitespiramycin producer. Curr Microbiol. 2011;62(1):16–20. doi:10.1007/s00284-010-9664-8
8. Shi XG, Sun YM, Zhang YF, Zhong DF. Tissue distribution of bitespiramycin and spiramycin in rats. Acta Pharmacol Sin. 2004;25(11):1396–1401.
9. Wong EHC, Porter JD, Edwards MR, Johnston SL. The role of macrolides in asthma: current evidence and future directions. Lancet Respir Med. 2014;2(8):657–670. doi:10.1016/S2213-2600(14)70107-9
10. Kanoh S, Rubin BK. Mechanisms of action and clinical application of macrolides as immunomodulatory medications. Clin Microbiol Rev. 2010;23(3):590–+. doi:10.1128/CMR.00078-09
11. Zimmermann P, Ziesenitz VC, Curtis N, Ritz N. The immunomodulatory effects of macrolides-a systematic review of the underlying mechanisms. Front Immunol. 2018;9. doi:10.3389/fimmu.2018.00302
12. Reijnders TDY, Saris A, Schultz MJ, van der Poll T. Immunomodulation by macrolides: therapeutic potential for critical care. Lancet Respir Med. 2020;8(6):619–630. doi:10.1016/S2213-2600(20)30080-1
13. Pollock J, Chalmers JD. The immunomodulatory effects of macrolide antibiotics in respiratory disease. Pulm Pharmacol Ther. 2021;71:102095.
14. Lin SJ, Kuo ML, Hsiao HS, Lee PT. Azithromycin modulates immune response of human monocyte-derived dendritic cells and CD4(+) T cells. Int Immunopharmacol. 2016;40:318–326. doi:10.1016/j.intimp.2016.09.012
15. Polancec DS, Kos VM, Banjanac M, et al. Azithromycin drives in vitro GM-CSF/IL-4-induced differentiation of human blood monocytes toward dendritic-like cells with regulatory properties. J Leukoc Biol. 2012;91(2):229–243. doi:10.1189/jlb.1210655
16. Liang SY, Zhao TC, Zhou ZH, et al. Anti-tumor effect of carrimycin on oral squamous cell carcinoma cells in vitro and in vivo. Transl Oncol. 2021;14(6):101074. doi:10.1016/j.tranon.2021.101074
17. Cui J, Zhou JC, He WQ, et al. Targeting selenoprotein H in the nucleolus suppresses tumors and metastases by Isovalerylspiramycin I. J Exp Clin Cancer Res. 2022;41(1). doi:10.1186/s13046-022-02350-0
18. Yan HY, Sun J, Wang K, et al. Repurposing carrimycin as an antiviral agent against human coronaviruses, including the currently pandemic SARS-CoV-2. Acta Pharmaceutica Sinica B. 2021;11(9):2850–2858. doi:10.1016/j.apsb.2021.02.024
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.