Back to Journals » Infection and Drug Resistance » Volume 16
A Candidemia Case Caused by a Novel Drug-Resistant Candida auris with the Y132F Mutation in Erg11 in Mainland China
Authors Xu Z, Zhang L, Han R, Ding C ![]() , Shou H, Duan X, Zhang S
, Shou H, Duan X, Zhang S
Received 10 March 2023
Accepted for publication 10 May 2023
Published 18 May 2023 Volume 2023:16 Pages 3065—3072
DOI https://doi.org/10.2147/IDR.S409708
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Zhaoxia Xu,1,* Lei Zhang,2,* Ran Han,1 Chengwei Ding,1 Haochang Shou,1 Xueguang Duan,1 Shengwei Zhang1
1Department of Clinical Laboratory, Dongfang Hospital, Beijing University of Chinese Medicine, Beijing, People’s Republic of China; 2State Key Laboratory of Pathogen and Biosecurity, Beijing Institute of Microbiology and Epidemiology, Academy of Military Medical Sciences, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xueguang Duan; Shengwei Zhang, Department of Clinical Laboratory, Dongfang Hospital, Beijing University of Chinese Medicine, Beijing, People’s Republic of China, Tel +86 13911179092 ; +86 13124780206, Email [email protected]; [email protected]
Background: Candida auris is a pathogen first found in external ear canal, becoming a major threat to global health. Here, we describe a candidemia case caused by a novel drug-resistant Candida auris strain.
Case Presentation: An 80-year-old patient, with multiple serious medical conditions, was suffered from candidemia caused by Candida auris, died 9 days after admission in our hospital. Phylogenetic analysis indicates that this C. auris isolate (designated BJCA003) belongs to the South Asian clade, carries the Y132F mutation in the protein Erg11. And antibiotic susceptibility test indicated that BJCA003 is resistant to fluconazole and amphotericin B, not susceptible to caspofungin. In addition, this strain has multiple colony and cellular morphologies under different culture conditions.
Conclusion: Strain BJCA003 is a novel drug resistant C. auris strain in mainland China, the Y132F mutation in Erg11 may attribute to fluconazole-resistance, alarming that we still face more challenges about C. auris.
Keywords: Candida auris, candidemia, drug-resistant, mutation, morphologies
Introduction
Candida auris is a human fungal pathogen, first isolated in Japan in 2009.1 Since then, many C. auris isolates have been reported worldwide.2–4 This pathogen can contaminate the environment around the patients who were colonized by the fungus, and can survive for long periods in major outbreaks.5
Recent studies of C. auris highlight its threatening properties of multidrug resistance and high mortality.6–8 It is more likely to infect critically ill and long-term hospitalized patients with severe comorbidities, such as pneumonia, chronic kidney disease, and cardiovascular diseases. C. auris has now become a major cause of candidemia,9 an ongoing challenge for accurate identification of this organism, often misidentified as other Candida species, has complicated clinical management.10 Five distinct clades of C. auris have been identified to date,11 and many isolates are resistant to fluconazole, often caused by hotspot gene mutations in ERG11.5
Since the first case in China was identified in 2018,12 more than 60 C. auris clinical cases have been reported. The first reported isolate was susceptible to all tested antifungal drugs, but several since then have displayed a high minimum inhibitory concentration (MIC) for amphotericin B and echinocandins, many isolates were resistant to fluconazole.13 We report here a new strain of C. auris isolated from patient’s blood in Beijing, which belongs to the South Asian clade, carries the Y132F mutation in the protein Erg11 and is co-resistant to fluconazole and amphotericin B, differ from all the strains identified in past in mainland China. We designated it as BJCA003 and further explore its phylogeny, antifungal susceptibility, and morphological characteristics.
Materials and Methods
General Indicators Detection
The level of hemoglobin (HGB), platelet (PLT) and white cell count was tested by XT- 4000i (Sysmex Inc, Kobe, Japan), C-reactive protein (CRP) was tested by BC-5310 (Mindray Medical International Limited, Shenzhen, China). Procalcitonin (PCT) was tested by Cobas e801 (Roche Diagnostics, Mannheim, Germany). Plasma (1–3)-beta-D-glucan (BDG) and serum galactomannan antigen levels were quantified with a commercial test kit (Dynamiker Biotechnology Co., Ltd. (Tianjin, China)).
Microbiological Identification, Morphological and MIC Analyses
Blood samples were collected directly into both aerobic and anaerobic bottles (Bio Mérieux, Lyon, France) and transferred to our microbiology laboratory for analysis. Microbe detection and identification were performed with a Vitek-2 MS (database VITEK MS IVD KB V3.2) and a Vitek-2 Compact, version 8.01 (Bio Mérieux, Lyon, France). Sequencing of the internal transcribed spacer (ITS) was accomplished by RuiBio Bio Tech (Beijing, China), the sequence data were determined by Basic Local Alignment Search Tool (BLAST) analysis.
To observe morphological characteristics, approximately 2×103CFU/mL of the strain was plated onto different media of blood agar, China blue agar, Sabouraud dextrose agar (Thermo Fisher, MA, USA), and CHROMagar Candida medium (Autobio, Zhengzhou, China). After culturing for 36h at 35°C, a single colony was picked to smear for Gram staining (Baso Diagnostics, Inc., Zhuhai, China).
Antifungal susceptibility testing was accomplished by using the YeastOne Plate (Thermo Fisher Scientific, MA, USA), colorimetric microdilution method was used based on the CLSI to determine the MIC value of eight antifungal drugs (fluconazole, itraconazole, voriconazole, caspofungin, anidulafungin, micafungin, amphotericin B, and 5-flucytosine).
Genetic and Phylogenetic Analysis of the Isolate BJCA003 of C. auris
C. auris genomic DNA was extracted using an enzymatic lysis method as previously described.14 Whole-genome sequencing was conducted using both the Illumina and Nanopore platforms as described in the Supplementary Methods. The ITS and D1/D2 (region of the large subunit (28S) of the ribosomal DNA) sequences of C. auris and previous reported isolates were aligned using ClustalW2 and a maximum likelihood phylogenetic tree was generated using IQ-TREE with 1000 bootstrap repeats. Schizosaccharomyces pombe strain ATCC 38366 was used for outgroup, ITS and D1/D2 sequences of the reported strains were acquired from the GenBank (https://www.ncbi.nlm.nih.gov/) database directly or extracted from the genome sequences. The hotspot gene mutations of ERG11 in the isolate BJCA003 were compared to the reference ERG11 sequence of C. auris (GenBank accession MK059959) using blastn (version 2.10.1).
Results
Case Presentation
An 80-year-old male patient was admitted to our hospital on Jan.5, 2022 with multiple medical conditions for several years. He has been diagnosed with chronic renal insufficiency (elevated serum creatinine) ten years ago and renal anemia seven years ago. He was intermittently treated with human erythropoietin. Two weeks before transferring to our hospital, the patient was administered continuous renal replacement therapy because serum creatinine rising to a level of 400 µmol/L and oliguria. His past medical history included hypertension, coronary heart disease, plasmacytoma, fungal pneumonia, bacterial pneumonia, hepatic insufficiency, and hyperhomocysteinemia. The patient presented asthenia, anuria, without fever and had no cough or sputum. He also had petechiae on the forearm and a 5×5 cm ecchymosis on the chest. Auscultation detected bilateral coarse breathing. He had a CRP plasma level of 59.7mg/L, a procalcitonin level of 0.931ng/mL, and a serum creatinine level of 467μmol/L. His erythrocyte and platelet counts were 1.87×1012/L and 42×109/L, respectively. His hemoglobin level was 68g/L, and his white blood cell count was normal. A chest CT scan revealed a dense opacity in the middle of the right lung, lung nodules, mild interstitial changes, and pleural effusion.
Before transferring to our hospital, the patient’s blood culture was negative for Aspergillus spp. or Mucorales and positive for Candida, while the exact type of Candida had not been identified at that time, an intravenous infusion of 800mg fluconazole on the first day, followed by 400mg per day for several days, as an treatment strategy for this condition in another hospital. Because this was ineffective, he was treated empirically with piperacillin sodium tazobactam sodium at 2.25g three times a day in our hospital. His treatment history for plasmacytoma was unknown because of hospitalization in another hospital before. Leucogen was used to treat for his hypocytosis, Other treatment strategies included platelet transfusion, hemodialysis, antihypertensive therapy, acid inhibitory, liver protection therapy and treatment of anemia.
The patient’s condition did not improve during the treatment course. His inflammatory blood markers of CRP and procalcitonin remained high (Table 1), indicating a persistent infection. Although the patient had a normal body temperature when he was admitted to our hospital, it increased to 38.2°C on the fourth day, and fluctuated somewhat up and down, reaching 39°C only once briefly. Unfortunately, the patient died nine days after admission to our hospital (Figure 1).
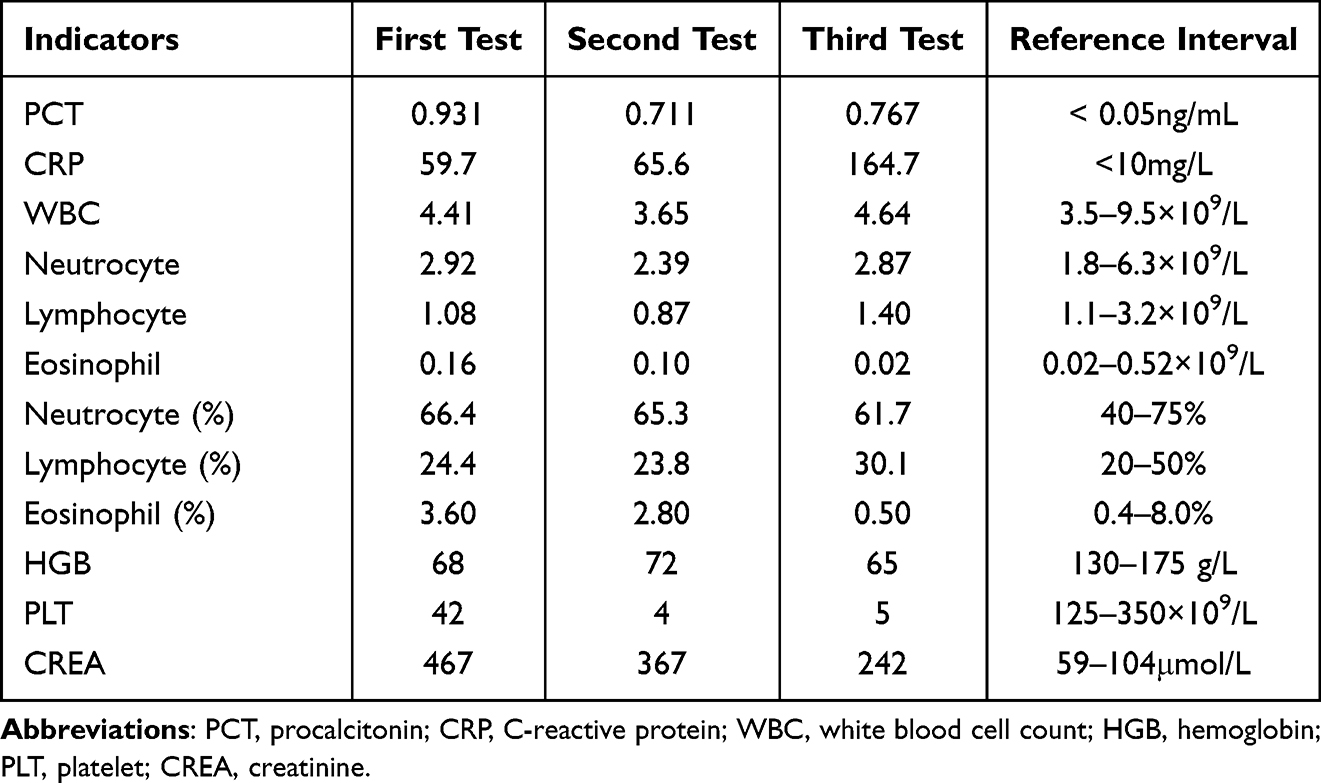 |
Table 1 General Indicators of the Examination |
 |
Figure 1 The course of disease progression and C. auris identification. Gray solid line shows the period of the patient’s hospital stay; gray-dashed line represents the period between the death of the patient and the confirmation of the strain; periods of fluconazole or piperacillin sodium tazobactam sodium treatments are marked by black arrows. |
Identification and Phylogenetic Analysis
First, we performed both 1, 3-β-D glucan detection and Galactomannan antigen test on January 7, which were surprisingly both negative. Later on Jan.10, a blood sample was sent to our clinic laboratory for blood culture analysis. After approximately 35 hours, an aerobic blood culture tested positive. A Gram stain revealed that it appeared to be an unevenly colored, elongated fungal spore. It was subsequently identified as C. auris by Vitek-2 MS (99%) and Vitek-2 Compact (98%), and was confirmed by ITS sequencing. A blast comparison indicated a 98.3% identity to C. auris (NR_154998.1) and 96.7% identity to Candida suratensis (NR_155008.1).
Phylogenetic analysis based on ITS and the D1/D2 regions sequences showed that the isolate of C. auris BJCA003 belongs to the South Asian clade. Additionally, Y132F mutation in Erg11 and a-type mating type locus (MTLa) were observed by WGS analysis (Figure 2).
 |
Figure 2 Phylogenetic analysis of C. auris (BJCA003) compared with reference strains. The isolates from mainland China are highlighted in red and the isolate of BJCA003 is highlighted in red color and bold font, the strains isolated from Hong Kong and Taiwan are highlighted in blue. The percentages of replicate trees in which the associated taxa clustered together in the bootstrap test (1000 replicates) are indicated in black dots at the branches. |
Antifungal Susceptibility
MICs of eight antifungal drugs were determined by susceptibility testing. The result indicates this strain was susceptible to itraconazole, voriconazole, anidulafungin, micafungin and 5-flucytosine. The MICs of these drugs are 0.12μg/mL, 0.5μg/mL, 0.5μg/mL, 0.25μg/mL and 0.12μg/mL respectively. However, fluconazole MICs was ≥128μg/mL and amphotericin B MICs was 2μg/mL, which means this pathogen was resistant to fluconazole and amphotericin B. Additionally, the MIC value of caspofungin was 8μg/mL, meaning the strain was not susceptible to caspofungin, according to the explanation of the instructions of YeastOne Plate (Table 2).
 |
Table 2 MICs of Antifungal Drugs |
Morphological Analysis
C. auris exhibits different morphologies on different media.12,15 To investigate morphological characteristics of this strain, we spotted it onto plates of blood, China blue, Sabouraud and CHROM agars, and cultured for 36 hours at 35°C. The strain appeared as creamy smooth colonies on blood, China blue, and Sabouraud agar plates, while it appeared as pink colored colonies on the CHROMagar Candida medium. After Gram staining, we observed morphological characteristics under a 100× microscopy. On Sabouraud and blood agar, oval-shaped, yeast morphology, as well as budding cells was observed. Cells on Sabouraud agar were more oval and bigger than cells on blood agar. On China blue and CHROMagar Candida, cells were relatively round, additionally, cells grown on China blue agar were rounder and smaller than cells from other three media. We did not see any hyphal or pseudohyphal cells on these media (Figure 3).
 |
Figure 3 Morphologies of C. auris grown on Sabouraud (SDA), blood (BA), China blue (CBA) and CHROMagar Candida plates. The image on the right side shows a magnification of the image marked by a black rectangle. |
Discussion
Since C. auris came to light in 2009, this organism has often exhibited multidrug-resistance and a high mortality rate, presenting a serious global health threat.6,16,17 Until our case, all infections reported in mainland China have been cured. Unfortunately, the patient in our study with the pathogen in his blood, died from fungemia combined with other medical complications nine days after admission to our hospital. C. auris primarily infects individuals with compromising immune defenses conditions,18 and our patient suffered from multiple serious conditions for years.
Detection of 1, 3-β-D glucan most often indicates fungal infections,19 but this patient, unexpectedly, tested negative. However, matrix-assisted laser desorption ionization-time of flight mass spectrometry and a rapid microbial identification system revealed C. auris in his blood.
To date, at least 60 known clinical C. auris strains have been isolated in China, with 39 from Shenyang, 15 from Hong Kong, three from Beijing, two from Xiamen and one from Tainan.13,20 In mainland China, greater than 90% of these C. auris strains had a single-resistance to fluconazole, minority of them exhibited high MICs for echinocandins and amphotericin B. Except for BJCA001 belonging to South Asian clade, all the other C. auris strains belong to South African clade. Like BJCA001, the isolate BJCA003 also belongs to South Asian clade, however, it exhibited drug resistance to fluconazole and amphotericin B. In addition, we can see a high MIC value for caspofungin in C. auris BJCA003, which is very different from BJCA001. Strain BJCA001 was susceptible to all tested antifungals, while C. auris BJCA003 was resistant to at least two kinds of antifungals. Nearly all fluconazole-resistant isolates of C. auris have one of three specific mutations (VF125AL, Y132F, or K143R) in ERG11,21 the gene encoding the target enzyme of the triazoles. The Y132F mutation was observed in strain of BJCA0003, unlike strains found in Beijing previously: strains BJCA002 and C1921 carried the VF125AL mutation, and strain BJCA001 had no mutations in Erg11, indicating the import of strain BJCA003 from out of Beijing. Importantly, these differences of mutation in Erg11 potentially provide an explanation for the notable variations in drug-resistance of C. auris.
The patient was initially treated with fluconazole because of Candida infection. This medication was given up as soon as the patient was admitted to our hospital due to a lack of response. C. auris BJCA003 was shown to be resistant to fluconazole after patient’s death. Therefore, an early identification of the specific C. auris variant, and administration of an affective antifungal agent(s) is essential. Unfortunately, accurate identification of C. auris infection in the clinical laboratory is still difficult due to misidentification as other fungal species.22 Thus, there is a pressing need for rapid and accurate identification devices and methods for C. auris.
Candida species have multiple cellular morphologies.23,24 Reversible morphological changes of Candida albicans are associated with virulence.25,26 Similarly, C. auris also have multiple colony and cellular morphologies including the yeast, filamentous, aggregated, and elongated forms.27 In our case, the strain exhibits different cellular morphologies when grown on different media. It was oval on Sabouraud and blood agar, while it was round on China blue agar and CHROMagar Candida. This strain may also undergo reversible transitions when culture conditions changed. Taken together, more attention should be paid on C. auris in Chinese hospitals.
Conclusion
The novel C. auris (strain BJCA003) is very different from other strains reported in mainland China. First, it belongs to the South Asian clade and carries the Y132F mutation in Erg11; moreover, it is resistant to antifungal drugs of fluconazole and amphotericin B, making it more difficult for accurate identification and effective treatment. Therefore, Chinese hospitals have encountered more challenges in the prevention and treatment of C. auris infection.
Abbreviations
C. auris, Candida auris; HGB, hemoglobin; PLT, platelet; CRP, C-reactive protein; PCT, procalcitonin; BDG, (1–3)-beta-D-glucan.
Data Sharing Statement
The raw sequencing data and the assembled genome can be accessed in the NCBI Sequence Read Archives (SRA) and GenBank under BioProject accession number PRJNA867138.
Ethics Approval and Consent to Participate
This study has been approved by IRB of Dongfang Hospital Beijing University of Chinese Medicine with the reference number of JDF-IRB-2022000101.
Consent for Publication
Written informed consent to the patient to this study was provided by the patient next of kin.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding was obtained for this study.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Satoh K, Makimura K, Hasumi Y, Nishiyama Y, Uchida K, Yamaguchi H. Candida auris sp. nov., a novel ascomycetous yeast isolated from the external ear canal of an inpatient in a Japanese hospital. Microbiol Immunol. 2009;53(1):41–44. doi:10.1111/j.1348-0421.2008.00083.x
2. Spivak ES, Hanson KE. Candida auris: an emerging fungal pathogen. J Clin Microbiol. 2018;56(2). doi:10.1128/jcm.01588-17
3. Du H, Bing J, Hu T, Ennis CL, Nobile CJ, Huang G. Candida auris: epidemiology, biology, antifungal resistance, and virulence. PLoS Pathog. 2020;16(10):e1008921. doi:10.1371/journal.ppat.1008921
4. Forsberg K, Woodworth K, Walters M, et al. Candida auris: the recent emergence of a multidrug-resistant fungal pathogen. Med Mycol. 2019;57(1):1–12. doi:10.1093/mmy/myy054
5. Ahmad S, Alfouzan W. Candida auris: epidemiology, diagnosis, pathogenesis, antifungal susceptibility, and infection control measures to combat the spread of infections in healthcare facilities. Microorganisms. 2021;9(4). doi:10.3390/microorganisms9040807
6. Tsay S, Kallen A, Jackson BR, Chiller TM, Vallabhaneni S. Approach to the investigation and management of patients with candida auris, an emerging multidrug-resistant yeast. Clin Infect Dis. 2018;66(2):306–311. doi:10.1093/cid/cix744
7. Rudramurthy SM, Chakrabarti A, Paul RA, et al. Candida auris candidaemia in Indian ICUs: analysis of risk factors. J Antimicrob Chemother. 2017;72(6):1794–1801. doi:10.1093/jac/dkx034
8. de Jong AW, Hagen F. Attack, defend and persist: how the fungal pathogen Candida auris was able to emerge globally in healthcare environments. Mycopathologia. 2019;184(3):353–365. doi:10.1007/s11046-019-00351-w
9. Al-Obaid I, Asadzadeh M, Ahmad S, et al. Fatal breakthrough candidemia in an immunocompromised patient in Kuwait Due to Candida auris exhibiting reduced susceptibility to echinocandins and carrying a novel mutation in hotspot-1 of FKS1. J Fungi. 2022;8(3). doi:10.3390/jof8030267
10. Saris K, Meis JF, Voss A. Candida auris. Curr Opin Infect Dis. 2018;31(4):334–340. doi:10.1097/qco.0000000000000469
11. Chow NA, de Groot T, Badali H, Abastabar M, Chiller TM, Meis JF. Potential fifth clade of Candida auris, Iran, 2018. Emerg Infect Dis. 2019;25(9):1780–1781. doi:10.3201/eid2509.190686
12. Wang X, Bing J, Zheng Q, et al. The first isolate of Candida auris in China: clinical and biological aspects. Emerg Microbes Infect. 2018;7(1):93. doi:10.1038/s41426-018-0095-0
13. Du H, Bing J, Nobile CJ, Huang G. Candida auris infections in China. Virulence. 2022;13(1):589–591. doi:10.1080/21505594.2022.2054120
14. Zhang L, Chen T, Wang Y, et al. Comparison analysis of different DNA Extraction methods on suitability for long-read metagenomic nanopore sequencing. Front Cell Infect Microbiol. 2022;12:919903. doi:10.3389/fcimb.2022.919903
15. Fan S, Zhan P, Bing J, et al. A biological and genomic comparison of a drug-resistant and a drug-susceptible strain of Candida auris isolated from Beijing, China. Virulence. 2021;12(1):1388–1399. doi:10.1080/21505594.2021.1928410
16. Lone SA, Ahmad A. Candida auris-The growing menace to global health. Mycoses. 2019;62(8):620–637. doi:10.1111/myc.12904
17. Wickes BL. Analysis of a Candida auris outbreak provides new insights into an emerging pathogen. J Clin Microbiol. 2020;58(4). doi:10.1128/jcm.02083-19
18. Bandara N, Samaranayake L. Emerging and future strategies in the management of recalcitrant Candida auris. Med Mycol. 2022;60(4). doi:10.1093/mmy/myac008
19. Sunamura EI, Iwasaki M, Shiina S, et al. A novel enzyme immunoassay for the measurement of plasma (1 → 3)-β-D-glucan levels. J Immunol Methods. 2020;487:112872. doi:10.1016/j.jim.2020.112872
20. Bing J, Wang S, Xu H, et al. A case of Candida auris candidemia in Xiamen, China, and a comparative analysis of clinical isolates in China. Mycology. 2022;13(1):68–75. doi:10.1080/21501203.2021.1994479
21. Rybak JM, Sharma C, Doorley LA, Barker KS, Palmer GE, Rogers PD. Delineation of the direct contribution of Candida auris ERG11 mutations to clinical triazole resistance. Microbiol Spectr. 2021;9(3):e0158521. doi:10.1128/Spectrum.01585-21
22. Chen Y, Zhao J, Han L, et al. Emergency of fungemia cases caused by fluconazole-resistant Candida auris in Beijing, China. J Infect. 2018;77(6):561–571. doi:10.1016/j.jinf.2018.09.002
23. Huang G. Regulation of phenotypic transitions in the fungal pathogen Candida albicans. Virulence. 2012;3(3):251–261. doi:10.4161/viru.20010
24. Whiteway M, Bachewich C. Morphogenesis in Candida albicans. Annu Rev Microbiol. 2007;61:529–553. doi:10.1146/annurev.micro.61.080706.093341
25. Thompson DS, Carlisle PL, Kadosh D. Coevolution of morphology and virulence in Candida species. Eukaryotic Cell. 2011;10(9):1173–1182. doi:10.1128/ec.05085-11
26. Biswas S, Van Dijck P, Datta A. Environmental sensing and signal transduction pathways regulating morphopathogenic determinants of Candida albicans. MMBR. 2007;71(2):348–376. doi:10.1128/mmbr.00009-06
27. Fan S, Yue H, Zheng Q, et al. Filamentous growth is a general feature of Candida auris clinical isolates. Med Mycol. 2021;59(7):734–740. doi:10.1093/mmy/myaa116
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Epidemiological Trends and Antimicrobial Resistance of Candida auris: A Focus on 7 Cases in a Single Medical Institution of Southern China
Wang Y, Lin L, Li J, Wang X, Zhang J, Xi L, Cai W, Lu S
Infection and Drug Resistance 2025, 18:2557-2568
Published Date: 16 May 2025