")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 18
A Bibliometric Analysis of Comorbidity of COPD and Lung Cancer: Research Status and Future Directions
Authors Fang H , Dong T , Li S , Zhang Y, Han Z , Liu M, Dong W, Hong Z, Fu M, Zhang H
Received 8 October 2023
Accepted for publication 15 December 2023
Published 22 December 2023 Volume 2023:18 Pages 3049—3065
DOI https://doi.org/10.2147/COPD.S425735
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Russell
Hanyu Fang,1,2 Tairan Dong,1 Shanlin Li,1 Yihan Zhang,1 Zhuojun Han,1 Mingfei Liu,1,2 Wenjun Dong,1,2 Zheng Hong,1,2 Min Fu,3 Hongchun Zhang1,2
1Graduate School, Beijing University of Chinese Medicine, Beijing, People’s Republic of China, 100029; 2Department of Traditional Chinese Medicine for Pulmonary Diseases, Center of Respiratory Medicine, China-Japan Friendship Hospital, Beijing, 100029, People’s Republic of China; 3Department of Infectious Diseases, Xiyuan Hospital, China Academy of Chinese Medical Sciences, Beijing, 100029, People’s Republic of China
Correspondence: Hongchun Zhang, Department of Traditional Chinese Medicine for Pulmonary Diseases, Center of Respiratory Medicine, China-Japan Friendship Hospital, Beijing, 100029, People’s Republic of China, Tel +86 13701226664, Email [email protected] Min Fu, Department of Infectious Diseases, Xiyuan Hospital, China Academy of Chinese Medical Sciences, Beijing, 100029, People’s Republic of China, Tel +86 13366093706, Email [email protected]
Objective: Although studies on the association between COPD and lung cancer are of great significance, no bibliometric analysis has been conducted in the field of their comorbidity. This bibliometric analysis explores the current situation and frontier trends in the field of COPD and lung cancer comorbidity, and to lay a new direction for subsequent research.
Methods: Articles in the field of COPD and cancer comorbidity were retrieved from Web of Science Core Collections (WoSCC) from 2004 to 2023, and analyzed by VOSviewer, CiteSpace, Biblimatrix and WPS Office.
Results: In total, 3330 publications were included. The USA was the leading country with the most publications and great influence. The University of Groningen was the most productive institution. Edwin Kepner Silverman was the most influential scholar in this field. PLOS One was found to be the most prolific journal. Mechanisms and risk factors were of vital importance in this research field. Environmental pollution and pulmonary fibrosis may be future research prospects.
Conclusion: This bibliometric analysis provided new guidance for the development of the field of COPD and lung cancer comorbidity by visualizing current research hotspots, and predicting possible hot research directions in the future.
Keywords: COPD, lung cancer, bibliometric analysis, VOSviewer, CiteSpace
Introduction
Chronic obstructive pulmonary disease (COPD) and lung cancer are two significant lung diseases with high incidence and mortality rates worldwide, posing a considerable threat to people’s health and lives. Lung cancer incidence has been on the rise in recent years, with the latest GLOBOCAN data from the International Agency for Research on Cancer indicating an incidence rate of 11.4% and a death rate of 18% among all malignancies worldwide in 2020.1–4 The current prevalence of COPD is estimated to be 5% to 15%.5 In addition to their impact on health, both COPD and lung cancer also result in significant economic costs, imposing a substantial burden on patients, families, and society as a whole. Therefore, promoting research on COPD, lung cancer, and their comorbidities is critical to optimize lung function screening, enhance the diagnosis and treatment of lung diseases, safeguard life and health, and alleviate the economic pressure on families and society. In recent years, there has been an increasing recognition of the similarities between COPD and lung cancer in terms of their etiology, pathogenesis, clinical presentation, and treatment.6
Bibliometrics is a scientific method that uses mathematical, statistical, and other measurement methods to analyze the distribution structure, quantitative relationships, and change patterns of literature within a specific field.7 By utilizing bibliometric features, visual analysis can be conducted to identify research directions, hot areas, and frontier directions. There are already scholars performing bibliometric analysis in many medical fields of research, such as cancer,8 osteoarthritis,9 COVID-19,10 etc. However, no bibliometric study has been conducted in the field of Comorbidity of Chronic Obstructive Pulmonary Disease and Lung Cancer. Therefore, this study aims to provide new guidance for the development of this field by analyzing relevant research from 2004 to 2023 using bibliometric methods, visualizing current research hotspots, and predicting possible hot research directions in the future.
Methods
Paper Retrieval and Data Extraction
In this study, we conducted a systematic literature search and data extraction by searching the Web of Science Core Collection (WoSCC) for published articles from 2004 to 2023. We used the search strategy TS=(“COPD” OR “chronic obstructive pulmonary disease*”) AND TS=(“lung cancer*” OR “lung carcinoma*” OR “lung neoplasm*”) to retrieve articles and reviews related to comorbidity of chronic obstructive pulmonary disease and lung cancer. All publications were retrieved as of March 29, 2023. Only English articles and reviews were included in the analysis, while other forms of publications, such as reprints, book chapters, conference abstracts, news items, letters, editorial material, corrections, data files, early access, bibliographies, and biographical entries were excluded. Duplicate publications were identified and removed using Citespace. A total of 2634 articles and 666 reviews were collected and analyzed (Figure 1).
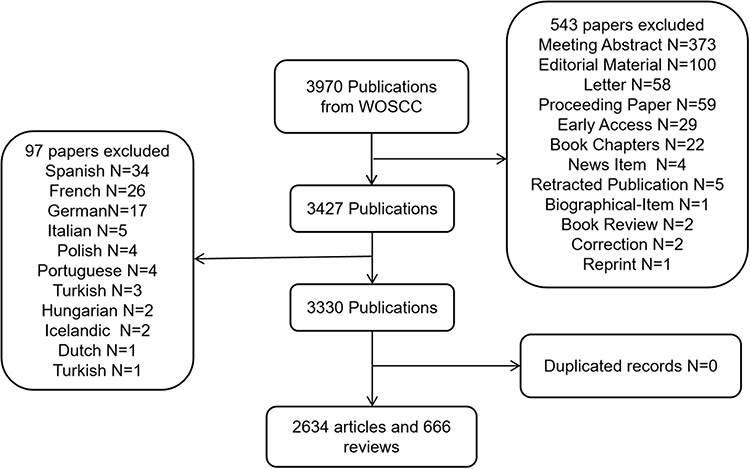 |
Figure 1 Flowchart of the literature screening process. |
Bibliometric Analysis
We analyzed the bibliometric indicators, including the number of publications (NP) and total citations (TC), obtained from the WoSCC database to evaluate the quality of the publications. The H-index was used in some cases to assess the scholarly achievements of regions or countries, journals, institutions, and individuals, which is an index to quantify an individual’s scientific research output.11 We employed statistical computing, graphics, and data visualization tools such as VOSviewer, CiteSpace, Biblimatrix, and WPS Office. We used VOSviewer and CiteSpace to extract and analyze potential information from the collected data and optimized visual graphs using Scimago Graphica. To plot statistical data, we utilized Biblimatrix, which is based on R, and WPS Office.
Results
Annual Publication Trends
Using our search strategy, we identified a total of 3,300 papers and reviews published between 2004 and 2023, containing 86,612 total citations (Figure 2). The annual publication rate fluctuated, reflecting the pace and progress of research in this field, as well as the level of interest it has generated. The overall publication count can be accurately modeled by a quadratic function (R2=0.9976), indicating a consistent upward trend (Figure 2). We anticipate that this trend will continue to accelerate in the future.
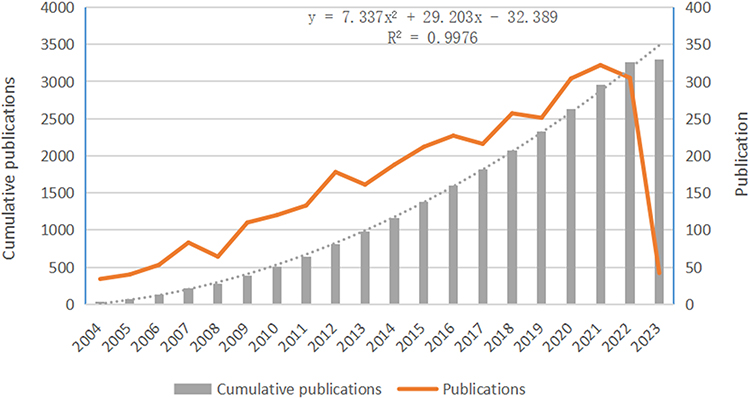 |
Figure 2 Trend of publications related to comorbidity of chronic obstructive pulmonary disease and lung cancer (2004–2023). |
Country Analysis
The analysis of publications from different countries provides valuable insights into the importance placed on a research area by a country and the degree of influence it holds in that area. Table 1 displays the top ten countries receiving the most total citations (TC). The United States obtained the most citations (40,760), followed by the United Kingdom and China with 12,174 and 9956 total citations, respectively. However, the number of citations does not always reflect the quality of publications. The United States, the United Kingdom, and China produced high-quality publications with average article citations of 55.20, 54.23, and 23.12, respectively. Canada, the United Kingdom, and the Netherlands also had high-quality publications, with an average of over 50 article citations, indicating that authors from these countries focused on the hot topics of this area and produced quality papers. Conversely, China ranked third in TC, but its average article citations were the lowest among the top 10 TC countries, suggesting a need to improve the quality of papers produced. A similar situation was observed in Japan and Spain, indicating the need for these countries to focus more on the quality of their papers.
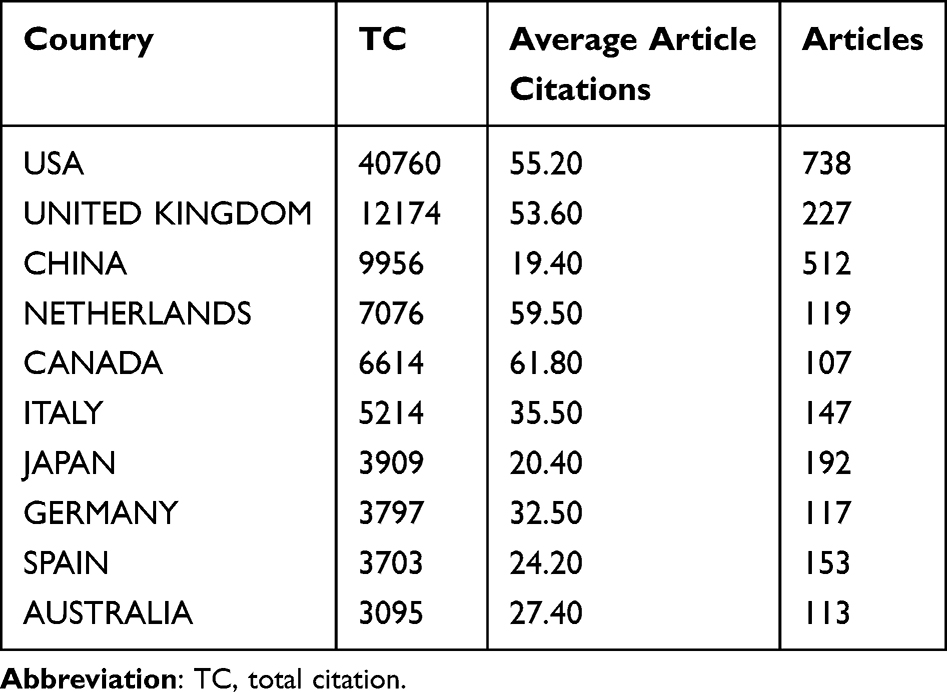 |
Table 1 Top 10 Productive Countries/Regions Related to Chronic Obstructive Pulmonary Disease and Lung Cancer Research |
We utilized Vosviewer to generate cooperation and clusters between countries of all authors, and Scimago Graphica to create a geographical map (Figure 3A). Among the different cooperative network clusters, inter-country cooperation was generally low, with only the United States exhibiting adequate inter-country cooperation in this area. This finding suggests that countries should further deepen their cooperation to promote the development of the discipline. The trends in the number of publications from each country over time are displayed in Figure 3B. The United States’ publication rate has stabilized after peaking in 2012, while China’s publication rate has been consistently rising. The publication rates of other countries have either remained stable or have shown an upward trend.
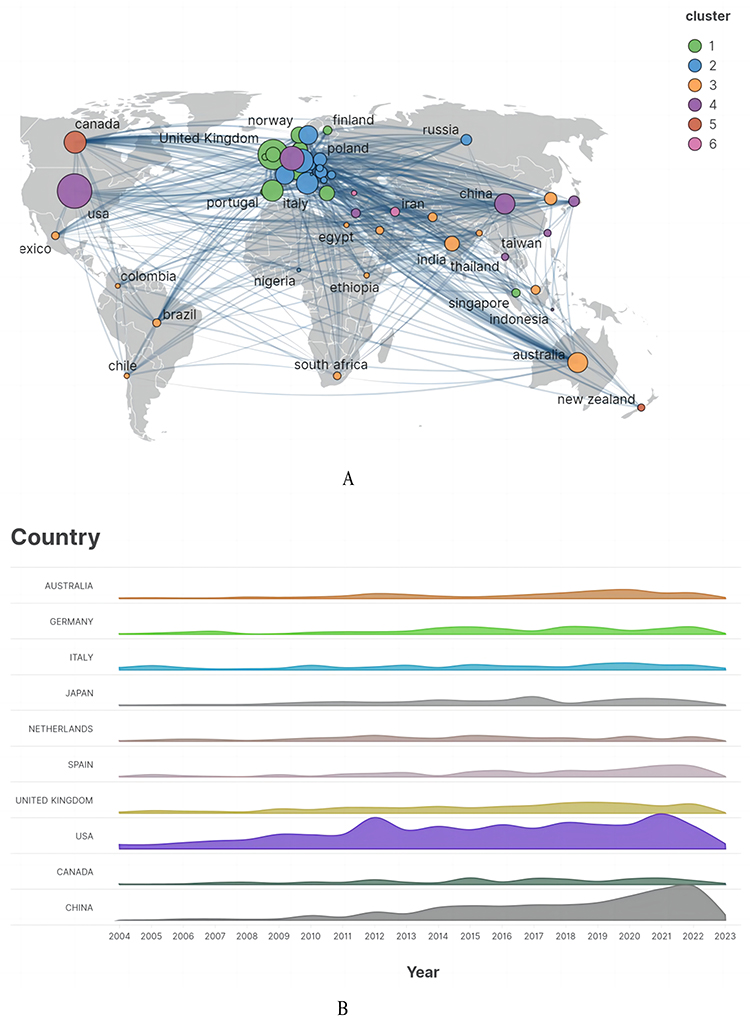 |
Figure 3 (A) The cooperation and clusters between countries of all authors. (B) The annual trends in the number of publications from each country over time. |
Author and Institution Analysis
H-index reflects the comprehensive influence and contribution of an author to a field.11 The top 10 authors with the highest H-index in comorbidity of chronic obstructive pulmonary disease and lung cancer are listed in Table 2. Edwin Kepner Silverman from Harvard Medical School got the first place with 17 publications in this area, followed by Higginson IJ and Yong RP. The authors’ co-occurrence network and burst chart were explored by Citespace, respectively (Figure 4A and B). Authors with more citations and publications tend to collaborate more. Figure 4C shows the visualization of the earliest publication time and publication volume of institution generated by Scimago Graphica. Top 10 institutions with the largest number of publications are listed in Table 3.
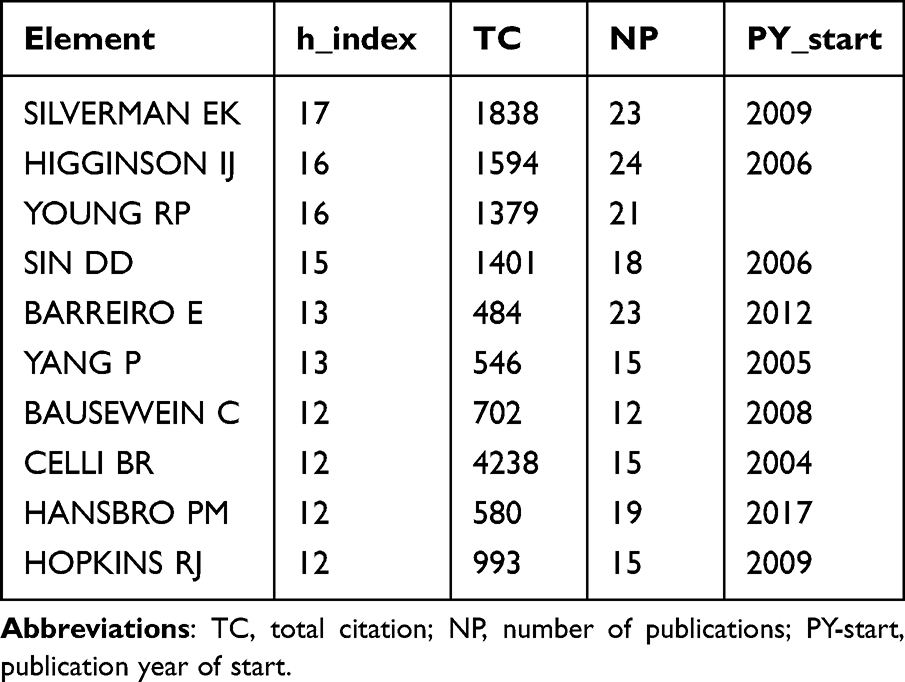 |
Table 2 The Top 10 Authors with the Highest H-Index |
 |
Table 3 The Top 10 Institutions with the Largest Number of Publications |
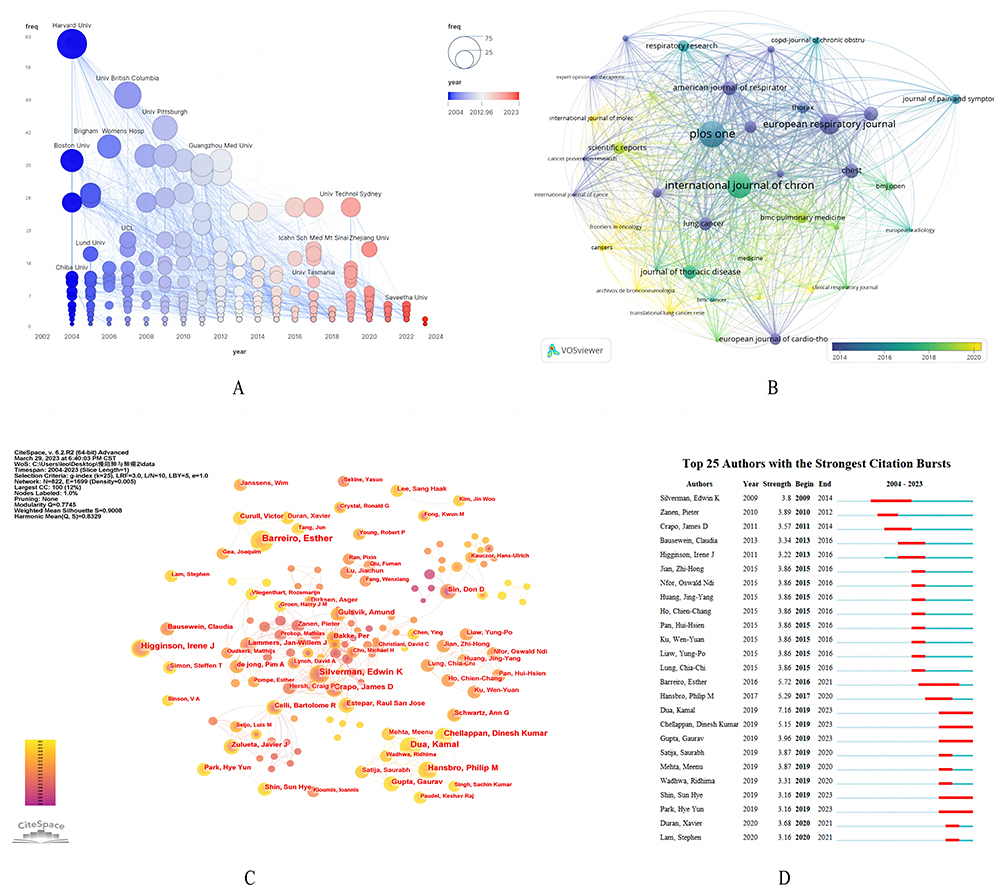 |
Figure 4 (A) The exploration of the authors’ co-occurrence network. (B) The top 25 authors with the strongest citation bursts. (C) The visualization of the earliest publication time and publication volume of institution generated. (D) The journal co-occurrence map. |
Bibliometric Analysis of Journal
The VOSviewer software was used to identify the most prominent and productive journals related to circadian rhythms in respiratory disease. In total, 3,300 publications were found in 943 academic journals (Table 4). PLOS One, with an impact factor (IF) of 3.752 according to Clarivate’s Journal Citation Reports, published the most papers with a total of 94. The International Journal of Chronic Obstructive Pulmonary Disease, with an IF of 2.893, ranked second, publishing 88 papers. Lung Cancer was found to be the most cited journal in the top 10 journals. The journal co-occurrence map (Figure 4D) indicates that PLOS One and the International Journal of Chronic Obstructive Pulmonary Disease are the two largest nodes. From Figure 4D, we can see that in the early stages of this field, there were more publications in well-established respiratory journals. Subsequently, comprehensive open-access journals gradually gained an advantage in publishing. Recently, publications in tumor-related journals have become more prominent.
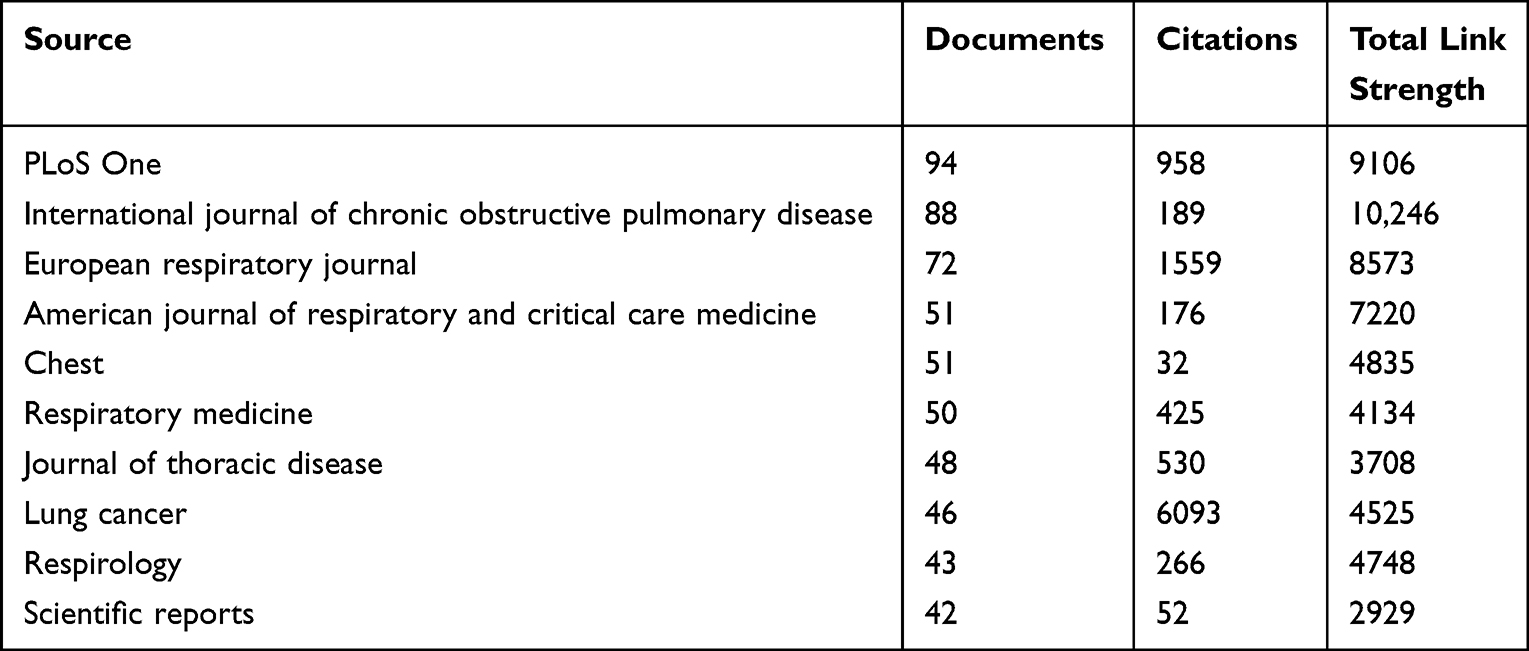 |
Table 4 The Most Prominent and Productive Journals Related to Circadian Rhythms in Respiratory Disease |
Reference Analysis
The reference co-citation analysis is a core function of CiteSpace, which can extract cluster labels based on cited documents.12 The cited and citing documents represent the research frontier and knowledge base.13 In our study on the comorbidity of chronic obstructive pulmonary disease and lung cancer, we set a scaling factor of k = 25 and used the g-index to identify homogenized groups of highly cited documents related to the field. We also checked and explained the co-citation of references. Cluster analysis can be used to study the structure of knowledge and the boundaries of research interests. By conducting cluster analysis on co-cited documents, we summarized the research areas of this field and explored hotspots and research directions.14 From the 135 clusters extracted from a total of 120,260 references cited in the articles, we identified the top 18 clusters based on cluster labels extracted from the title of cited articles using the Log-likelihood ratio (LLR) algorithm, such as #0 nonsteroidal anti-inflammatory drug, #1 lung cancer, #2 PD-1 blockade, #3 gut microbiota, #4 epithelial-mesenchymal transition, #5 nicotine dependence, #6 fine particulate matter, #7 small-cell lung cancer, #8 palliative care, #9 expression profiling, #10 white paper, #11 non-coding RNA, #12 multicenter study, #13 STROBE-compliant article, #16 relationship, #18 HIV, #20 varenicline, and #24 women (Figure 5A). The modularity Q value was 0.7745, and the weighted mean silhouette of each cluster was 0.9011, indicating reasonable cluster quality. Purple contours represent early clusters, such as #12 and #16, while yellow contours represent recent cluster labels, such as #11 and #3 (Figure 5B). Node size in the network is proportional to the betweenness centrality, which measures the probability that a node lies on the shortest path between any two nodes in the network. Nodes with high betweenness centrality may act as mediators between different clusters or within clusters, facilitating the transformation of research topics and paradigms. Table 5 lists the top ten ranked items by centrality.15 The most centrally located item is Adcock IM (2011) in Cluster #1, with a centrality of 0.16. The second is McGarvey LP (2007) in Cluster #0, with a centrality of 0.13. The third is de Torres JP (2011) in Cluster #1, with a centrality of 0.12. The fourth is Henschke CI (2015) in Cluster #1, with a centrality of 0.11. The fifth is Chang SH (2014) in Cluster #2, with a centrality of 0.10. Notably, four of the top ten central nodes belong to Cluster #1, while three belong to Cluster #0. The comorbidity of chronic obstructive pulmonary disease and lung cancer, which is the main focus of the #0 nonsteroidal anti-inflammatory drug and #1 lung cancer clusters, is the core mechanism of various research directions in this field.
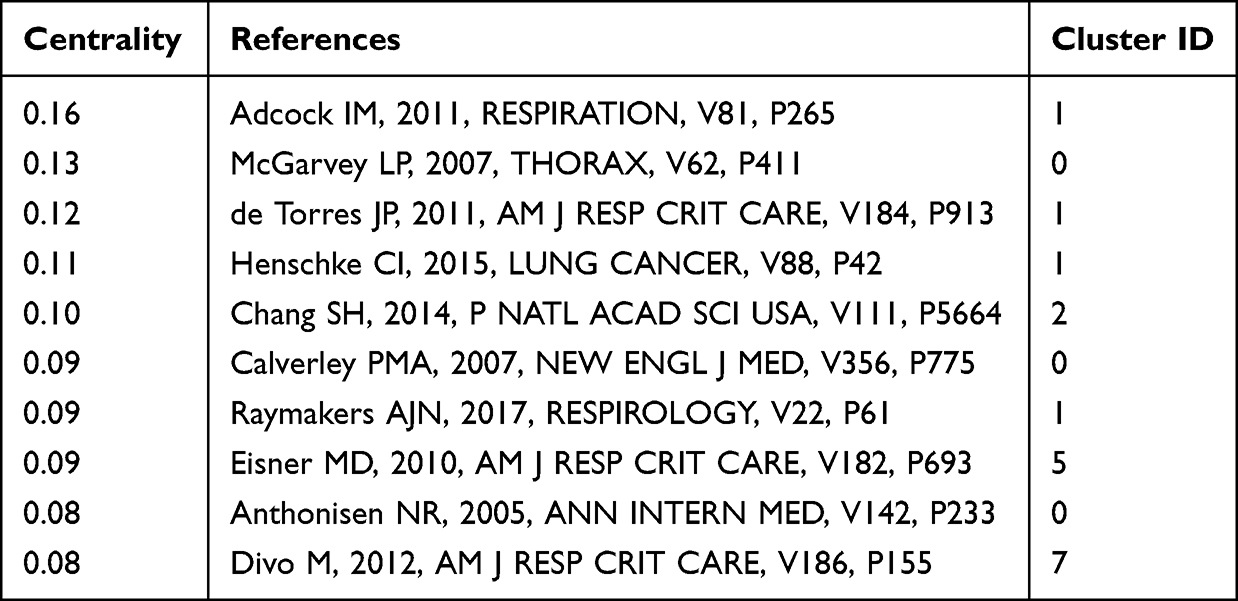 |
Table 5 The Top Ten Ranked Items by Centrality |
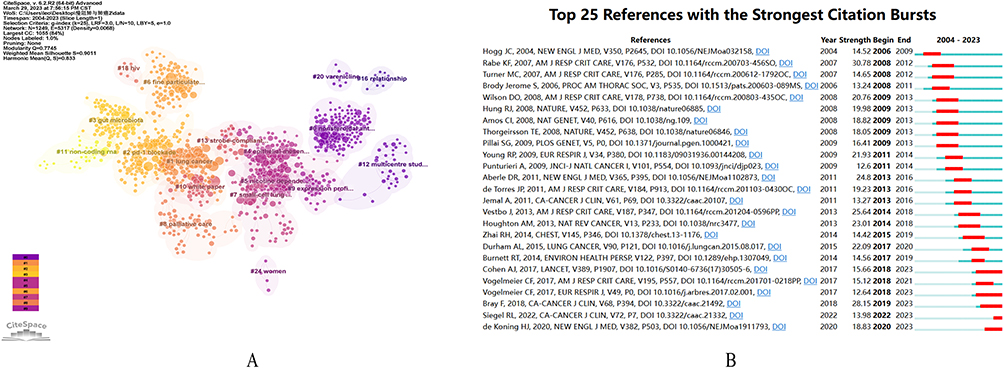 |
Figure 5 (A) The top 18 clusters from the 135 clusters. (B) Top 25 references with the strongest citation bursts. |
Key Words
VOSviewer was utilized for keyword co-occurrence and clustering analysis (Figure 6A and B). A total of 10,471 keywords were extracted, with 16 appearing over 200 times and 35 over 100 times. The keyword density plot identified high-frequency co-occurring words, revealing research hotspots (Figure 6C). Excluding search terms, the most significant terms were risk, morbidity, and inflammation. Clustering analysis was used to reveal the knowledge structure of the research area.16 Based on the strength of the links between the co-occurring keywords, the network was divided into five clusters with clear homogeneity among terms within each cluster. Cluster 1 (red) was the most important, containing 55 projects related to inflammation, asthma, gene expression, oxidative stress, and biomarkers. The second group (green) comprised 40 projects related to smoking, including risk, emphysema, and prevalence. Cluster 3 (blue) focused on symptom management and quality of life, with 35 projects, including management, acute exacerbation, dyspnea, palliative care, and exercise. Cluster 4 (yellow) mainly described the diagnosis and treatment of comorbidities of chronic obstructive pulmonary disease and lung cancer, with 30 projects, including survival, impact, diagnosis, surgery, therapy, prognosis, and non-small cell cancer. Cluster 5 (purple) mainly described the mortality and risk factors associated with the comorbidities of chronic obstructive pulmonary disease and lung cancer, with 15 projects, including mortality, risk factors, tobacco exposure, air pollution, and PM 2.5.
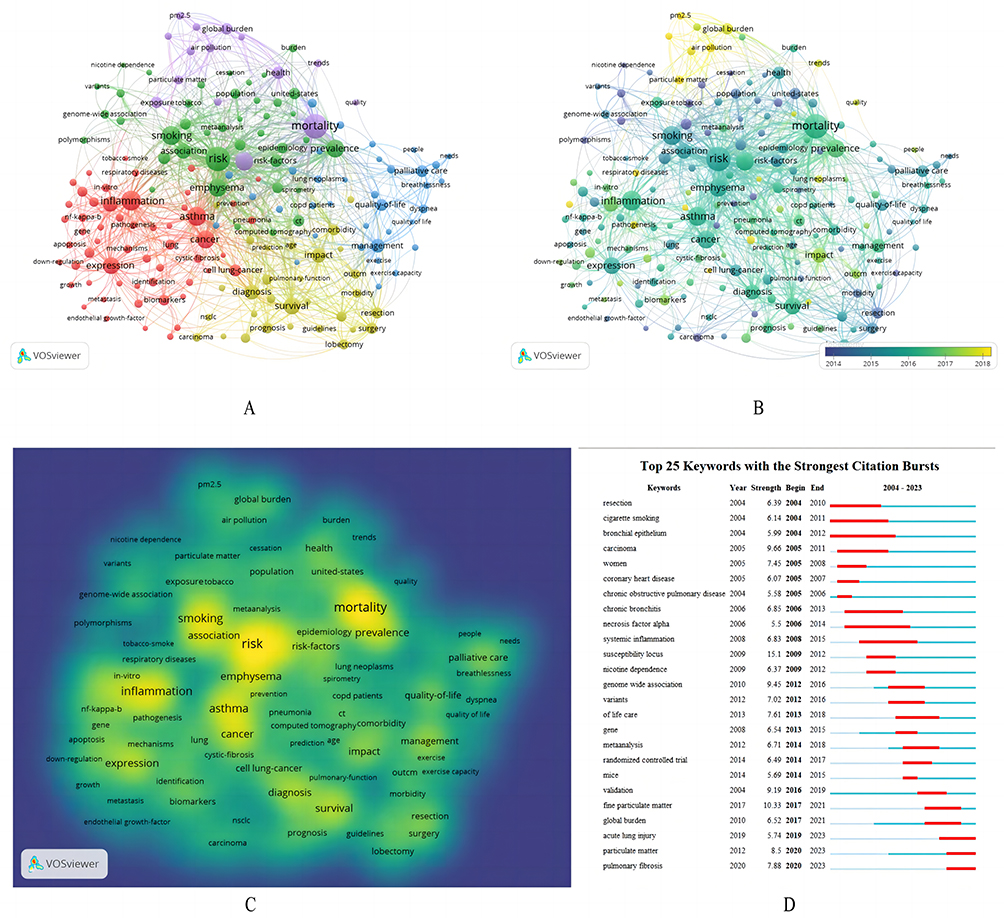 |
Figure 6 (A) Co-occurrence network analysis and clustering analysis of keywords. (B) Co-occurrence network analysis with time. (C) High-frequency co-occurring words. (D) The top 25 keywords with the strongest citation bursts. |
The timeline map of high-frequency keywords was generated using CiteSpace to display the evolutionary process in different clusters.17 Each keyword was plotted according to the year it first appeared, with the color of the link indicating the year in which the two keywords first appeared simultaneously. Keyword bursts were utilized to detect the frequency and magnitude of keyword occurrences, which described the relationship between clusters from a temporal perspective. The keyword timeline map and burst analysis provided a depiction of the temporal characteristics of clustering, and explored the hotspots and frontiers of this research area. We identified 25 keywords that represented the research field appropriately in terms of burst intensity, duration, and timing through CiteSpace for burst analysis of keywords and timeline analysis (Figures 6D and 7A). Trend topic is also generated by Biblimatrix (Figure 7B).
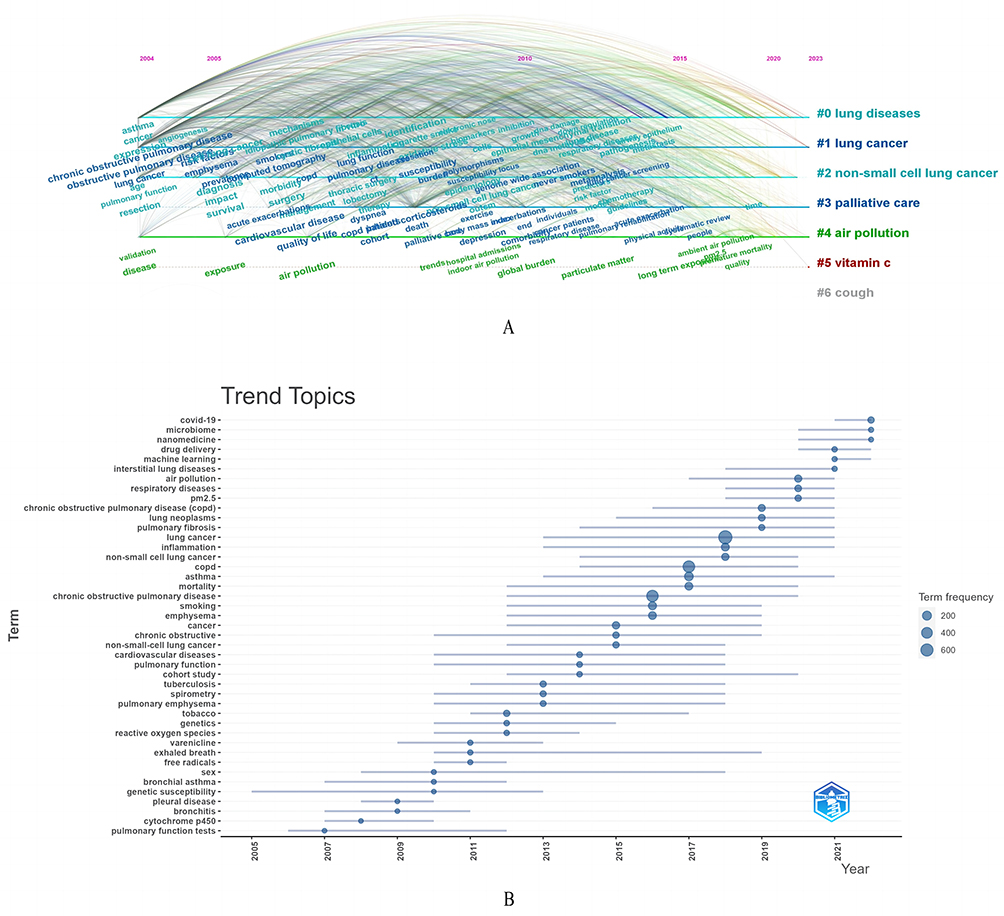 |
Figure 7 (A) Timeline of keywords with different clusters. (B) Trend topics generated by bibliometrix in R. |
Discussion
The comorbidity of COPD and lung cancer is highly prevalent, and both diseases are related in terms of etiology and pathogenesis, and can cause or affect each other (Table 6).6 Investigations have demonstrated that the amount of active or passive smoking, duration of smoking, and mortality rate of lung cancer and COPD in smokers are more than 10 times higher than those in non-smokers, indicating a strong correlation between smoking and the development of these diseases.18,19 Smoking causes stromal destruction, epithelial cell death, and inadequate blood supply, leading to impaired lung barrier function and inflammation. In this process, the lung may undergo abnormal tissue repair, and these autonomic adjustments are important causes of COPD and lung cancer.6 In addition to smoking, environmental pollution, occupational exposure, and gender are common risk factors for the development of both diseases (Table 6). Inflammation and oxidative stress are important pathogeneses of lung cancer comorbid with COPD.10–15,17–26 Inflammatory cell infiltration is common in both diseases, and neutrophils, macrophages, CD4+ and CD8+ lymphocytes are involved in their pathogenesis.27 In the course of COPD emphysema, lung damage caused by inflammation is repaired and remodeled by continuous cell proliferation in lung tissue, leading to lung carcinogenesis comorbid with COPD.28 During oxidative stress, the increase of reactive oxygen species (ROS) may induce lung inflammation, mucus hypersecretion, and anti-protease inactivation, which promote the occurrence and development of COPD. Furthermore, oxidative stress can damage cell structures, causing DNA damage, inducing cell carcinogenesis, and leading to the occurrence of lung cancer. Bronchoalveolar lavage fluid analysis of patients with COPD and lung cancer comorbidity found that 15 proteins involved in ROS metabolism were differentially expressed, indicating that oxidative stress is an important pathogenesis common to both diseases.29
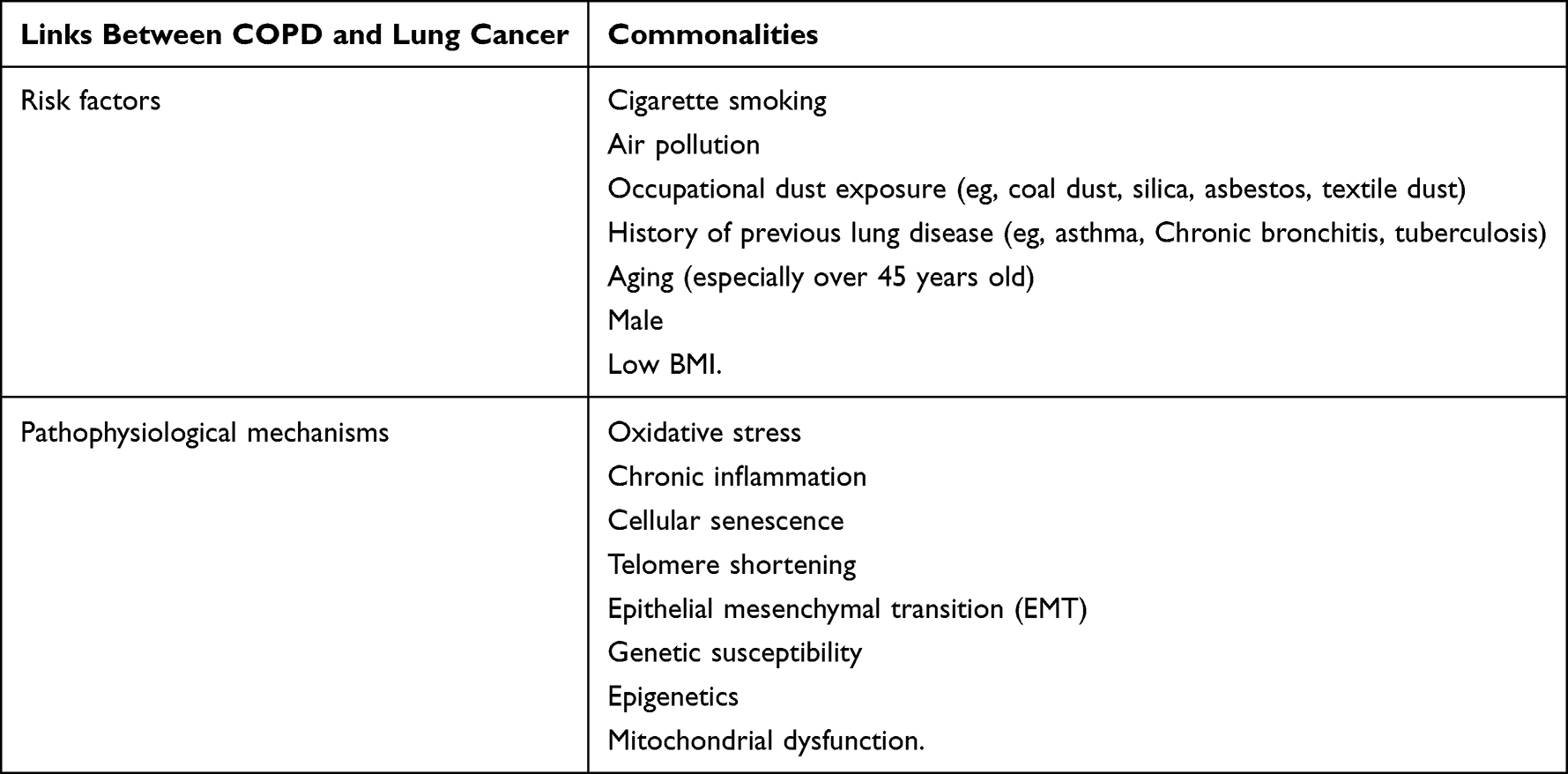 |
Table 6 Relationship of Risk Factors and Pathogenesis in COPD and Lung Cancer |
Both inflammation and oxidative stress are closely related and promote the development of chronic obstructive pulmonary disease (COPD) and comorbid lung cancer. Additionally, lung aging is also an important pathogenesis of the comorbidity between COPD and lung cancer. Studies have demonstrated that patients with comorbid COPD and lung cancer commonly have decreased lung function due to aging of lung tissues which leads to lower lung immune function, making them more susceptible to external infections and diseases. Furthermore, the mucous membrane of COPD patients is significantly weaker than normal in removing foreign substances such as carcinogens. As a result, the decline of lung function is accelerated, which can easily cause premature lung failure and increase the incidence of lung cancer.30 Genetic susceptibility is also an important pathogenesis for both diseases. Studies have shown that 80% to 90% of COPD and lung cancer patients have a history of tobacco smoke exposure. However, only 20% to 30% of smokers have COPD, and 10% to 15% have lung cancer.31 Therefore, there is a certain genetic susceptibility to the development of these two diseases. It has also been suggested that the comorbidity of COPD and lung cancer is a genetic disorder associated with genetic polymorphisms and multiple genes including susceptibility and protection genes.32,33 To effectively treat the comorbidity of COPD and lung cancer, we need to improve the level of diagnosis by screening COPD patients for lung cancer and detecting the occurrence of comorbidity early through early diagnosis. This will enable us to take effective interventions to reduce the burden on individuals, families and society. In the future, basic research on comorbidity of COPD and lung cancer needs to be further strengthened, especially more detailed research on the pathogenesis and the effectiveness of treatment options based on it.
For the first time ever, we analyzed the current status and trends in the development of comorbidity of COPD and lung cancer using bibliometric analysis. Our search of the WoSCC database yielded 3,330 papers and reviews published between 2004 and 2021, as of March 29, 2023. To assess the spatial and temporal distribution, author contributions, and journal quality of these articles, we used CiteSpace and VOSviewer. Furthermore, we conducted burst hotspot analysis, cluster analysis, and keyword analysis to identify the current areas of research focus and frontiers in comorbidity of COPD and lung cancer.
The change in annual trends based on published publications indicates a dynamic change from 34 annual publications in 2004 to 322 publications in 2022. Although the annual number of publications decreased in 2008, 2017, 2019 and 2023, studies on comorbidity of COPD and lung cancer have increased year by year. By analyzing countries and institutions, the top 5 countries in terms of citations were the United States, the United Kingdom, China, Netherlands, and Canada, indicating their significant influence in the field. However, among these top 5 countries, China ranks last in terms of average article citations among the top 10 TC countries, highlighting the need for improvement in the quality of Chinese publications. On the other hand, the other four countries produced high-quality publications with an average of over 50 article citations, showcasing the high quality of publications published in these countries. It is worth noting that the top 10 countries are mostly concentrated in European and American regions, with only the United States carrying out adequate inter-country cooperation, indicating the need for deeper cooperation to promote the development of the discipline. Regarding trends in the number of publications, China’s publication rate has been steadily increasing, while that of the United States has stabilized after peaking in 2012. This suggests that China is becoming more productive in this field, while the United States has already reached a certain level.
In the analysis of the institution, it was found that the University of Groningen was the most productive with 117 articles, followed by Harvard University with 102 articles and the University of British Columbia with 89 articles. The University of Groningen mainly focuses on studying the molecular mechanisms that determine malignant transformation in a broad spectrum of tumors and translating these fundamental insights into improved early detection and treatment of cancer, ultimately leading to personalized cancer therapy. Harvard University is involved in researching the tumor microenvironment, mechanisms of cancer development and treatment, and systematic reviews of COPD. In addition, Harvard University, the University of British Columbia, and the University of Pittsburgh have played important roles with a high frequency of publications before 2010. However, new institutions with increasing publication frequencies have emerged, such as the University of Technology Sydney, the Icahn School of Medicine at Mount Sinai, and Zhejiang University, although their publication frequencies are still far from those of established institutions in the early years.
The analysis of the top 10 authors of H-index showed that Edwin Kepner Silverman from Harvard Medical School ranked first with the H-index of 17, whose studies focused mainly on alpha 1-antitrypsin deficiency, chronic obstructive pulmonary disease, emphysema, pulmonary fibrosis. Higginson IJ, from King’s College London and Young RP, from University of Auckland both got the second place with the H-index of 16. Higginson IJ’s research mainly discussed palliative care for advanced illness. Young RP mainly studied lung cancer screening and treatments of lung cancer and COPD. In terms of the strongest citation bursts, Edwin Kepner Silverman’s burst moment occurred earliest (2009), while Dua, Kamal’s burst was the strongest and last to the present day. The co-occurrence network among authors was also analyzed, which found that authors with more citations and publications were more likely to actively collaborate. Edwin Kepner Silverman was one of the centers of the network. High H-index, high TC, strong citation bursts and more collaboration might help him win the first place of authors in this field. Univ Groningen is the affiliation with the largest number of published articles (117), followed by Harvard Univ with 102 articles, indicating their significant influence in this research area.
According to the analysis of journals, PLOS One (IF=3.752) was found to be the most prolific journal with a total of 94 publications, indicating its significant role in this field. The International Journal of Chronic Obstructive Pulmonary Disease (IF=2.893) ranked second with 88 published papers, followed by the European Respiratory Journal (IF=33.795) with 72 published papers. Moreover, Lancet was the most cited journal, indicating that the papers it published were of high quality. In terms of the visual analysis of journal co-occurrence, PLOS One, The International Journal of Chronic Obstructive Pulmonary Disease, and European Respiratory Journal had the highest centrality. Over time, well-established respiratory journals published more papers in the early stage, while more comprehensive open-access journals have gradually gained an edge in recent years. Additionally, it is worth mentioning that tumor-related journals have become more prominent.
The co-citations of references were also illustrated. Among the top 10 cited references, the most cited paper is Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary published by Vestbo J. et al from American Journal of Respiratory and Critical Care Medicine in 2013, with citation counts of 74. The highest citation of this article may due to its executive summary of GLOD, which facilitates other studies in this field. On the basis of the burst detection analysis of citation, Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary published by Rabe KF et al from American Journal of Respiratory and Critical Care Medicine in 2007 ranked first with bursts of 30.78. The second one is Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries published by Bray F. et al from CA-Cancer J Clin in 2018 with bursts of 28.15. As two breaking hotspots, they reflected the rapidly growing interest in this research field and led to research directions focused on COPD and lung cancer respectively.
According to the clusters analysis, 135 clusters were extracted from a total of 120,260 references cited in the articles, and the top 18 clusters were identified based on cluster label extracted from the title of cited articles using the Log-likelihood ratio (LLR) algorithm, such as #0 nonsteroidal anti-inflammatory drug, #1 lung cancer, #2 pd-1 blockade, #3 gut microbiota, #4 epithelial-mesenchymal transition, #5 nicotine dependence, #6 fine particulate matter, #7 small-cell lung cancer, #8 palliative care, #9 expression profiling, #10 white paper, #11 non-coding rna, #12 multicentre study, #13 strobe-compliant article, #16 relationship, #18 hiv, #20 varenicline, #24 women.
A majority of the clusters focused on the relationship between COPD and lung cancer, their common risk factors, pathological mechanism, and related treatments. However, they laid particular stress on different items. Cluster #0 (nonsteroidal anti-inflammatory drug) explored etiopathogenesis of COPD and lung cancer, including the evolution of the pathological effects of airway obstruction in patients with COPD and the potential pathogenic molecular links between tobacco smoking-related COPD and squamous cell carcinoma.34,35 It is of great significance for the early diagnosis, treatment and even prevention of COPD and lung cancer. Moreover, cluster#11 (non-coding rna) explored common pathways for pathogenesis to COPD and lung cancer, and indicated the role of immune dysfunction, the lung microbiome, extracellular vesicles, underlying genetic susceptibility and epigenetic factors in the development of COPD and lung cancer.27 Cluster#5 (nicotine dependence) focused on gene locus associated with lung cancer and COPD, and their results provide compelling evidence of a locus at 15q25 predisposing to lung cancer and a locus at CHRNA3/5 contributing to COPD.36–38 Additionally, the literature in cluster #16 (relationship) focused on the role of polymorphisms of alleles in the pathogenesis of COPD and lung cancer.39,40 Articles in cluster#9 (expression profiling) discovered the injury caused by cigarette smoke throughout the airway and explored the gene expression in lung. The result indicated that gene expression in normal large-airway epithelial cells can be used as a lung cancer biomarker, and S1RT1 plays a pivotal role in regulation of NF-kappaB-dependent proinflammatory mediators in lung of smokers and patients with COPD.41–44 These researches may contribute to the development of new diagnostic methods and therapies. Cluster#20 (varenicline) mainly involved assessment and verification efficacy and safety of varenicline as a therapy for smoking cessation,45–47 which is able to effectively control the important risk factor of smoking. Papers in cluster#1 (lung cancer) mainly discussed the common mechanisms to lung cancer and COPD, showing that lung cancer and COPD are with the same underlying genetic predisposition, telomere shortening, mitochondrial dysfunction and premature aging. Additionally, COPD may induce lung cancer by increasing oxidative stress and the resulting DNA damage, chronic exposure to pro-inflammatory cytokines, repression of the DNA repair mechanisms and increased cellular proliferation.28,48,49 And articles in cluster#4 (epithelial-mesenchymal transition) concluded that COPD and emphysema are both independent risk factors for lung cancer, which are not related to smoking.50–52 Cluster#2 (pd-1 blockade) and cluster#3 (gut microbiota) tended to explore therapies on the basis of studying the pathogenesis of COPD and lung cancer.53–56 According to the analysis of cluster#6 (fine particulate matter), cluster#13 (strobe-compliant article) and cluster#18 (hiv), exposure to ozone and fine particulate matter in ambient air, previous lung diseases and HIV infection are associated with an increased risk of COPD and lung cancer, which has impactions for prophylaxis and treatment of COPD and lung cancer.57–64 Studies in cluster#8 (palliative care) paid attention to the effectiveness of early palliative care and end-of-life-care for patients with COPD and lung cancer and provided robust evidence to support the early integration of palliative care for patients with COPD and lung cancer.65,66 These researches have promoted the future research progress and clinical application of palliative care and end-of-life-care. Cluster#7 (small-cell lung cancer) was more concentrated on COPD comorbidities, and indicated that COPD is a complex disease involving more than airflow obstruction, which has profound effects on cardiac function and gas exchange with systemic consequences. In addition, the inflammation in COPD may result in important systemic manifestations, so that treatment of COPD inflammation may concomitantly treat systemic inflammation and associated comorbidities.67,68 Cluster #12 (multicentre study) made clear that COPD and lung cancer are diseases leading to high mortality and high burden worldwide,69,70 which called for more attention from academic community. From the analysis of cluster#10 (white paper), low-dose computed tomography played a vital role in lung cancer screening, which can reduce mortality.71,72 Differences in COPD between the sexes were discussed in cluster #24 women, indicating the morbidity of lung disease in women has increased over years. It could be due to the increasing prevalence of tobacco use in women and their susceptibility to psychological impairment.73–75
The analysis of keyword co-occurrence, clustering, burst intensity and timeline map can be utilized to explore the research direction, hotspots and development thread of this field. In terms of keyword co-occurrence, “risk” was keyword with the highest frequency in this field, reflecting the fact that “risk” was a hotspot in this field in 2010s. The network between co-occurrence was divided into five main clusters based on the strength of the links, which were particular to #0 lung diseases, #1 lung cancer, #2 non-small cell lung cancer, #3 palliative care, #4 air pollution, which represented the main research hotspots and trends in this field.
From the analysis of the keyword timeline map, the hotspots and trends at different time points can be objectively tracked. Before 2010, the researches were focused on pathological mechanisms and therapies of lung diseases. During 2010 to 2015, studies included bronchial symptoms and mechanisms and gene susceptibility. Between 2015 and 2020, in addition to cancer and smoking, COPD, lung cancer and risk turned out to be widely concerned with high frequencies. Besides, researches focused on several risk factors, complications and epidemiology of lung diseases as well. Topics related to air pollution still played important roles in recent studies after 2020, while pembrolizumab, impacts and covid-19 are the cutting-edge topics at present. By analyzing the keyword burst intensity at different time points, carcinoma was a vital keyword in the early stage. Along with the development of research in this field, chronic bronchitis, systemic inflammation and susceptibility locus have become hotspots in this field, from which susceptibility locus had the highest bursts intensity. Subsequently, genome wide association, life care, fine particulate matter and global burden gained popular attention. Up to now, acute lung injury, particulate matter and pulmonary fibrosis have been the leading-edge keywords in this field. Throughout the developing progress, it can be found that previous studies focused on the pathogenesis and had been progressing continuously, from histological level to the genetic level. Subsequently, standardized diagnosis and treatment guidelines have also become the research priority in this area. For lung cancer patients with COPD, if COPD is not treated during anti-tumor treatment, they will face more surgical complications, shorter OS and FPS.76,77 However, as long as COPD receives routine treatment according to guidelines, the survival time of lung cancer patients with COPD is similar to that without COPD.78 Studies have shown that the prevalence of COPD in lung cancer patients is about 28.4%-39.8%, but 72%-92.9% of COPD were undiagnosed in lung cancer patients, and only 27.1% of patients received treatment consistent with the GOLD guidelines.79,80 Encouragingly, patients with lung cancer combined with COPD seem to benefit more from immunotherapy compared to those without COPD,81 which may be related to their shared pathological and physiological bases (Table 6).82,83 In the future, it is highly necessary to explore and develop more reasonable treatment regimens targeting the common pathogenesis of the two diseases.And in past few years, new research directions including multiple types of environmental exposures and global burden have emerged. It is worth noting that different risk factors have been focused in all periods. It is reasonable to speculate that more researches will be concerned about prevention and treatment of COPD and lung cancer from fine particulate matter, the role of pulmonary fibrosis in COPD and lung cancer and relevant new therapeutic directions.
Conclusion
After conducting a bibliometric analysis using CiteSpace and VOSviewer, we gained a deeper understanding of the research development, hotspots, and future trends in comorbidity of COPD and lung cancer over the past 19 years. The USA is the leading country in this field, and better collaboration and communication among countries, institutions, and authors is needed. This objective and quantitative method provides important clues for researchers to understand the structural and temporal dynamics of the field. Based on the analysis, hot spot changes in the field have been identified and future research prospects may mainly focus on environmental pollution and pulmonary fibrosis.
Funding
This study is supported by National Natural Science Foundation of China Project: Research on the Repair Mechanism of Respiratory Injury in COPD Mice by Traditional Chinese Medicine for Strengthening the Body, Strengthening the Health, and Regulating the Skin and Hair of the Lung (82074367); National Natural Science Foundation Project: Effect of Bufei Granule on Improving the Condition of Airway Inflammation-Mucous Hyperplasia in COPD by Controlling miRNA-TLR4 Signaling Network (81703858).
Disclosure
The authors declare that there is no conflicts of interest.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clinicians. 2021;71(3):209–249. doi:10.3322/caac.21660
2. Vestbo J, Hurd SS, Agustí AG, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med. 2013;187(4):347–365. doi:10.1164/rccm.201204-0596PP
3. Lozano R, Naghavi M, Foreman K, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet (London, England). 2012;380(9859):2095–2128. doi:10.1016/S0140-6736(12)61728-0
4. Zhong N, Wang C, Yao W, et al. Prevalence of chronic obstructive pulmonary disease in China: a large, population-based survey. Am J Respir Crit Care Med. 2007;176(8):753–760. doi:10.1164/rccm.200612-1749OC
5. Global Initiative for Chronic Obstructive Lung Disease. 2020 Global strategy for prevention, diagnosis and management of COPD[EB/OL]; January 10, 2021. Available from: https://gold-copd.org/gold-report.
6. Qi C, Sun, SW, Xiong, XZ . From COPD to lung cancer: mechanisms linking, diagnosis, treatment, and prognosis. Int J Chronic Obstr. 2022;17:2603–2621. doi:10.2147/COPD.S380732
7. Kim Y-M, Delen D. Medical informatics research trend analysis: a text mining approach. Health Inf J. 2018;24(4):432–452. doi:10.1177/1460458216678443
8. Zhou F, Liu Y, Liu C, et al. Knowledge landscape of tumor-associated macrophage research: a bibliometric and visual analysis. Front Immunol. 2023;14:1078705. doi:10.3389/fimmu.2023.1078705
9. Liao J, Yu X, Chen J, et al. Knowledge mapping of autophagy in osteoarthritis from 2004 to 2022: a bibliometric analysis. Front Immunol. 2023;14:1063018. doi:10.3389/fimmu.2023.1063018
10. Meng L, Wen KH. An overview and trend analysis of research on the relationship between urban streets and residents’ health in China pre- and post COVID-19 pandemic. Front Public Health. 2023;11:1126656. doi:10.3389/fpubh.2023.1126656
11. Hirsch JE. An index to quantify an individual’s scientific research output. Proc Natl Acad Sci U S A. 2005;102(46):16569–16572. doi:10.1073/pnas.0507655102
12. Synnestvedt MB, Chen C, Holmes JH. Citespace II: visualization and knowledge discovery in bibliographic databases. AMIA Annu Symp Proc. 2005;2005:724–728. doi:10.1002/asi.20317
13. Chen CM, Ibekwe-SanJuan F, Hou JH. The structure and dynamics of cocitation clusters: a multiple-perspective cocitation analysis. J Am Soc Inf SciTechnol. 2010;61(7):1386–1409. doi:10.1002/asi.21309
14. Qin Y, Zhang Q, Liu Y. Analysis of knowledge bases and research focuses of cerebral ischemia-reperfusion from the perspective of mapping knowledge domain. Brain Res Bull. 2020;156:15–24. doi:10.1016/j.brainresbull.2019.12.004
15. Freeman LC. Centrality in social networks: conceptual clarification. SocNetw. 1979;1(3):215–239. doi:10.1016/0378-8733(78)90021-728
16. Brandes U. A faster algorithm for betweenness centrality. J Math Sociol. 2001;25(2):163–177. doi:10.1080/0022250X.2001.9990249
17. Chen CM. Science mapping: a systematic review of the literature. J of Data Inf Sci. 2017;2(2):1–40. doi:10.1515/jdis-2017-0006
18. Taylor R, Najafi F, Dobson A, et al. Meta-analysis of studies of passive smoking and lung cancer: effects of study type and continent. Int J Epidemiol. 2007;36(5):1048–1059. doi:10.1093/ije/dym158
19. Mortaz E, Folkerts G, Nijkamp FP, et al. ATP and the pathogenesis of COPD. Eur J Pharmacol. 2010;638(1–3):1–4. doi:10.1016/j.ejphar.2010.04.019
20. Matakidou A, Eisen T, Houlston RS, et al. Systematic review of the relationship between family history and lung cancer risk. Br J Cancer. 2005;93(7):825–833. doi:10.1038/sj.bjc.6602769
21. Jin YT, Xu YC, Yang RD, et al. Familial aggregation of lung cancer in a high incidence area in China. Br J Cancer. 2005;92(7):1321–1325. doi:10.1038/sj.bjc.6602465
22. Raaschou-Nielsen O, Bak H, Sørensen M, et al. Air pollution from traffic and risk for lung cancer in three Danish cohorts. Cancer Epidemiol Biomarkers Prev. 2010;19(5):1284–1291. doi:10.1158/1055-9965.EPI-10-0036
23. De Matteis S, Consonni D, Bertazzi PA, et al. Exposure to occupational carcinogens and lung cancer risk. Evolution of epidemiological estimates of attributable fraction. Acta Biomed. 2008;79(Suppl 1):34–42.
24. Suzuki R, Miyazaki Y, Takagi K, et al. Matrix metalloproteinases in the pathogenesis of asthma and COPD: implications for therapy. Treat Respir Med. 2004;3(1):17–27. doi:10.2165/00151829-200403010-00003
25. Bozinovski S, Vlahos R, Hansen M, et al. Akt in the pathogenesis of COPD. Int J Chronic Obstr. 2006;1(1):31–38. doi:10.2147/copd.2006.1.1.31
26. Reid PT, Sallenave J-M. Cytokines in the pathogenesis of chronic obstructive pulmonary disease. Curr Pharm Des. 2003;9(1):25–38. doi:10.2174/1381612033392440
27. Parris BA, O’Farrell HE, Fong KM, et al. Chronic obstructive pulmonary disease (COPD) and lung cancer: common pathways for pathogenesis. J Thoracic Dis. 2019;11(Suppl 17):S2155–S2172. doi:10.21037/jtd.2019.10.54
28. Houghton AM. Mechanistic links between COPD and lung cancer. Nat Rev Cancer. 2013;13(4):233–245. PMID: 23467302. doi:10.1038/nrc3477
29. Pastor MD, Nogal A, Molina-Pinelo S, et al. Identification of proteomic signatures associated with lung cancer and COPD. J Proteom. 2013;89:227–237. doi:10.1016/j.jprot.2013.04.037
30. Binkley MS, King MT, Shrager JB, et al. Pulmonary function after lung tumor stereotactic ablative radiotherapy depends on regional ventilation within irradiated lung. Radiother Oncol. 2017;123(2):270–275. PMID: 28460826. doi:10.1016/j.radonc.2017.03.021
31. Young RP, Hopkins RJ, Gamble GD, et al. Genetic evidence linking lung cancer and COPD: a new perspective. Appl Clin Gen. 2011;4:99–111. doi:10.2147/TACG.S20083
32. Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A. Global cancer statistics, 2012. CA Cancer J Clin. 2015;65(2):87–108. PMID: 25651787. doi:10.3322/caac.21262
33. Sinden NJ, Baker MJ, Smith DJ, Kreft JU, Dafforn TR, Stockley RA. α-1-antitrypsin variants and the proteinase/antiproteinase imbalance in chronic obstructive pulmonary disease. Am J Physiol Lung Cell Mol Physiol. 2015;308(2):L179–90. PMID: 25416382; PMCID: PMC4338942. doi:10.1152/ajplung.00179.2014
34. Hogg JC, Chu F, Utokaparch S, et al. The nature of small-airway obstruction in chronic obstructive pulmonary disease. N Engl J Med. 2004;350(26):2645–2653. PMID: 15215480. doi:10.1056/NEJMoa032158
35. Caramori G, Casolari P, Cavallesco GN, Giuffrè S, Adcock I, Papi A. Mechanisms involved in lung cancer development in COPD. Int J Biochem Cell Biol. 2011;43(7):1030–1044. PMID: 20951226. doi:10.1016/j.biocel.2010.08.022
36. Hung RJ, McKay JD, Gaborieau V, et al. A susceptibility locus for lung cancer maps to nicotinic acetylcholine receptor subunit genes on 15q25. Nature. 2008;452(7187):633–637. PMID: 18385738. doi:10.1038/nature06885
37. Pillai SG, Ge D, Zhu G, et al.; ICGN Investigators. A genome-wide association study in chronic obstructive pulmonary disease (COPD): identification of two major susceptibility loci. PLoS Genet. 2009;5(3):e1000421. PMID: 19300482; PMCID: PMC2650282. doi:10.1371/journal.pgen.1000421
38. Amos CI, Wu X, Broderick P, et al. Genome-wide association scan of tag SNPs identifies a susceptibility locus for lung cancer at 15q25.1. Nat Genet. 2008;40(5):616–622. PMID: 18385676; PMCID: PMC2713680. doi:10.1038/ng.109
39. Park JY, Chen L, Elahi A, Lazarus P, Tockman MS. Genetic analysis of microsomal epoxide hydrolase gene and its association with lung cancer risk. Eur J Cancer Prev. 2005;14(3):223–230. PMID: 15901990; PMCID: PMC3715303. doi:10.1097/00008469-200506000-00005
40. Stemmler S, Arinir U, Klein W, et al. Association of interleukin-8 receptor alpha polymorphisms with chronic obstructive pulmonary disease and asthma. Genes Immun. 2005;6(3):225–230. PMID: 15772681. doi:10.1038/sj.gene.6364181
41. Adcock IM, Caramori G, Barnes PJ. Chronic obstructive pulmonary disease and lung cancer: new molecular insights. Respiration. 2011;81(4):265–284. PMID: 21430413. doi:10.1159/000324601
42. Pierrou S, Broberg P, O’Donnell RA, et al. Expression of genes involved in oxidative stress responses in airway epithelial cells of smokers with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2007;175(6):577–586. PMID: 17158281. doi:10.1164/rccm.200607-931OC
43. Spira A, Beane JE, Shah V, et al. Airway epithelial gene expression in the diagnostic evaluation of smokers with suspect lung cancer. Nat Med. 2007;13(3):361–366. PMID: 17334370. doi:10.1038/nm1556
44. Rajendrasozhan S, Yang SR, Kinnula VL, Rahman I. SIRT1, an antiinflammatory and antiaging protein, is decreased in lungs of patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2008;177(8):861–870. PMID: 18174544; PMCID: PMC2292827. doi:10.1164/rccm.200708-1269OC
45. Howard P, Knight C, Boler A, Baker C. Cost-utility analysis of varenicline versus existing smoking cessation strategies using the BENESCO Simulation model: application to a population of US adult smokers. Pharmacoeconomics. 2008;26(6):497–511. PMID: 18489200. doi:10.2165/00019053-200826060-00004
46. Gonzales D, Rennard SI, Nides M, et al.; Varenicline Phase 3 Study Group. Varenicline, an alpha4beta2 nicotinic acetylcholine receptor partial agonist, vs sustained-release bupropion and placebo for smoking cessation: a randomized controlled trial. JAMA. 2006;296(1):47–55. PMID: 16820546. doi:10.1001/jama.296.1.47
47. Stead LF, Perera R, Bullen C, Mant D, Lancaster T. Nicotine replacement therapy for smoking cessation. Cochrane Database Syst Rev. 2008;1:CD000146. Update in: Cochrane Database Syst Rev. 2012;11:CD000146. PMID: 18253970. doi:10.1002/14651858.CD000146.pub3
48. Yang IA, Relan V, Wright CM, et al. Common pathogenic mechanisms and pathways in the development of COPD and lung cancer. Expert Opin Ther Targets. 2011;15(4):439–456. PMID: 21284573. doi:10.1517/14728222.2011.555400
49. Durham AL, Adcock IM. The relationship between COPD and lung cancer. Lung Cancer. 2015;90(2):121–127. PMID: 26363803; PMCID: PMC4718929. doi:10.1016/j.lungcan.2015.08.017
50. Wilson DO, Weissfeld JL, Balkan A, et al. Association of radiographic emphysema and airflow obstruction with lung cancer. Am J Respir Crit Care Med. 2008;178(7):738–744. PMID: 18565949; PMCID: PMC2556456. doi:10.1164/rccm.200803-435OC
51. Young RP, Hopkins RJ, Christmas T, Black PN, Metcalf P, Gamble GD. COPD prevalence is increased in lung cancer, independent of age, sex and smoking history. Eur Respir J. 2009;34(2):380–386. PMID: 19196816. doi:10.1183/09031936.00144208
52. Turner MC, Chen Y, Krewski D, Calle EE, Thun MJ. Chronic obstructive pulmonary disease is associated with lung cancer mortality in a prospective study of never smokers. Am J Respir Crit Care Med. 2007;176(3):285–290. PMID: 17478615. doi:10.1164/rccm.200612-1792OC
53. Perrotta F, D’Agnano V, Scialò F, et al. Evolving concepts in COPD and lung cancer: a narrative review. Minerva Med. 2022;113(3):436–448. PMID: 35156786. doi:10.23736/S0026-4806.22.07962-9
54. Mark NM, Kargl J, Busch SE, et al. Chronic obstructive pulmonary disease alters immune cell composition and immune checkpoint inhibitor efficacy in non-small cell lung cancer. Am J Respir Crit Care Med. 2018;197(3):325–336. PMID: 28934595; PMCID: PMC5803651. doi:10.1164/rccm.201704-0795OC
55. Trappe A, Donnelly SC, McNally P, Coppinger JA. Role of extracellular vesicles in chronic lung disease. Thorax. 2021;76(10):1047–1056. PMID: 33712504; PMCID: PMC8461402. doi:10.1136/thoraxjnl-2020-216370
56. Eapen MS, Hansbro PM, Larsson-Callerfelt AK, et al. Chronic obstructive pulmonary disease and lung cancer: underlying pathophysiology and new therapeutic modalities. Drugs. 2018;78(16):1717–1740. PMID: 30392114. doi:10.1007/s40265-018-1001-8
57. Burnett RT, Pope CA 3rd, Ezzati M, et al. An integrated risk function for estimating the global burden of disease attributable to ambient fine particulate matter exposure. Environ Health Perspect. 2014;122(4):397–403. Erratum in: Environ Health Perspect. 2014 Sep;122(9):A235. PMID: 24518036; PMCID: PMC3984213. doi:10.1289/ehp.1307049
58. Cohen AJ, Brauer M, Burnett R, et al. Estimates and 25-year trends of the global burden of disease attributable to ambient air pollution: an analysis of data from the Global Burden of Diseases Study 2015. Lancet. 2017;389(10082):1907–1918. Erratum in: Lancet. 2017 Jun 17;389(10087):e15. Erratum in: Lancet. 2018 Apr 21;391(10130):1576. PMID: 28408086;PMCID: PMC5439030. doi:10.1016/S0140-6736(17)30505-6
59. Maji KJ, Dikshit AK, Arora M, Deshpande A. Estimating premature mortality attributable to PM2.5 exposure and benefit of air pollution control policies in China for 2020. Sci Total Environ. 2018;612:683–693. PMID: 28866396. doi:10.1016/j.scitotenv.2017.08.254
60. Huang JY, Jian ZH, Ndi Nfor O, et al. The impact of coexisting asthma, chronic obstructive pulmonary disease and tuberculosis on survival in patients with lung squamous cell carcinoma. PLoS One. 2015;10(7):e0133367. PMID: 26196516; PMCID: PMC4510446. doi:10.1371/journal.pone.0133367
61. Brenner DR, McLaughlin JR, Hung RJ. Previous lung diseases and lung cancer risk: a systematic review and meta-analysis. PLoS One. 2011;6(3):e17479. PMID: 21483846; PMCID: PMC3069026. doi:10.1371/journal.pone.0017479
62. Triplette M, Crothers K, Attia EF. Non-infectious pulmonary diseases and HIV. Curr HIV/AIDS Rep. 2016;13(3):140–148. PMID: 27121734. doi:10.1007/s11904-016-0313-0
63. Lambert AA, Kirk GD, Astemborski J, Mehta SH, Wise RA, Drummond MB. HIV infection is associated with increased risk for acute exacerbation of COPD. J Acquir Immune Defic Syndr. 2015;69(1):68–74. PMID: 25942460; PMCID: PMC4422097. doi:10.1097/QAI.0000000000000552
64. Gingo MR, Balasubramani GK, Kingsley L, et al. The impact of HAART on the respiratory complications of HIV infection: longitudinal trends in the MACS and WIHS cohorts. PLoS One. 2013;8(3):e58812. PMID: 23554932; PMCID: PMC3595204. doi:10.1371/journal.pone.0058812
65. Higginson IJ, Bausewein C, Reilly CC, et al. An integrated palliative and respiratory care service for patients with advanced disease and refractory breathlessness: a randomized controlled trial. Lancet Respir Med. 2014;2(12):979–987. PMID: 25465642. doi:10.1016/S2213-2600(14)70226-7
66. Curtis JR. Palliative and end-of-life care for patients with severe COPD. Eur Respir J. 2008;32(3):796–803. PMID: 17989116. doi:10.1183/09031936.00126107
67. Divo M, Cote C, de Torres JP, et al.; BODE Collaborative Group. Comorbidities and risk of mortality in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2012;186(2):155–161. PMID: 22561964. doi:10.1164/rccm.201201-0034OC
68. Barnes PJ, Celli BR. Systemic manifestations and comorbidities of COPD. Eur Respir J. 2009;33(5):1165–1185. PMID: 19407051. doi:10.1183/09031936.00128008
69. Mathers CD, Loncar D. Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med. 2006;3(11):e442. PMID: 17132052; PMCID: PMC1664601. doi:10.1371/journal.pmed.0030442
70. Jemal A, Ward E, Hao Y, Thun M. Trends in the leading causes of death in the United States, 1970–2002. JAMA. 2005;294(10):1255–1259. PMID: 16160134. doi:10.1001/jama.294.10.1255
71. Kauczor HU, Bonomo L, Gaga M, et al. European Society of Radiology (ESR); European Respiratory Society (ERS). ESR/ERS white paper on lung cancer screening. Eur Radiol. 2015;25(9):2519–2531. PMID: 25929939; PMCID: PMC4529446. doi:10.1007/s00330-015-3697-0
72. Moyer VA; U.S. Preventive Services Task Force. Screening for lung cancer: u.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2014;160(5):330–338. PMID: 24378917. doi:10.7326/M13-2771
73. Rahmanian SD, Diaz PT, Wewers ME. Tobacco use and cessation among women: research and treatment-related issues. J Womens Health (Larchmt). 2011;20(3):349–357. PMID: 21375414; PMCID: PMC3058892. doi:10.1089/jwh.2010.2173
74. Gan WQ, Man SF, Postma DS, Camp P, Sin DD. Female smokers beyond the perimenopausal period are at increased risk of chronic obstructive pulmonary disease: a systematic review and meta-analysis. Respir Res. 2006;7(1):52. PMID: 16571126; PMCID: PMC1435894. doi:10.1186/1465-9921-7-52
75. Di Marco F, Verga M, Reggente M, et al. Anxiety and depression in COPD patients: the roles of gender and disease severity. Respir Med. 2006;100(10):1767–1774. PMID: 16531031. doi:10.1016/j.rmed.2006.01.026
76. Shin SH, Shin S, Im Y, et al. Effect of perioperative bronchodilator therapy on postoperative pulmonary function among lung cancer patients with COPD. Sci Rep. 2021;11:8359. doi:10.1038/s41598-021-86791-1
77. Wang F, Xie XH, Lin XQ, et al. Exploration of the treatment model for patients with advanced non-small cell lung cancer complicated with chronic obstructive pulmonary disease based on real-world data. Zhonghua Jie He He Hu Xi Za Zhi. 2020;43:450–454.
78. Ajimizu H, Ozasa H, Sato S, et al. Survival impact of treatment for chronic obstructive pulmonary disease in patients with advanced non-small-cell lung cancer. Sci Rep. 2021;11:23677. doi:10.1038/s41598-021-03139-5
79. Mouronte-Roibás C, Leiro-Fernández V, Fernández-Villar A, Botana-Rial M, Ramos-Hernández C, Ruano-Ravina A. COPD, emphysema and the onset of lung cancer. A systematic review. Cancer Lett. 2016;382(2):240–244. doi:10.1016/j.canlet.2016.09.002
80. Zhang J, Zhou JB, Lin XF, Wang Q, Bai CX, Hong QY. Prevalence of undiagnosed and undertreated chronic obstructive pulmonary disease in lung cancer population. Respirology. 2013;18(2):297–302. doi:10.1111/j.1440-1843.2012.02282.x
81. Lin M, Huang Z, Chen Y, et al. Lung cancer patients with chronic obstructive pulmonary disease benefit from anti-PD-1/PD-L1 therapy. Front Immunol. 2022;13:1038715. doi:10.3389/fimmu.2022.1038715
82. Nucera F, Mumby S, Paudel KR, et al. Role of oxidative stress in the pathogenesis of COPD. Minerva Med. 2022;113(3):370–404. doi:10.23736/S0026-4806.22.07972-1
83. Caramori G, Ruggeri P, Mumby S, et al. Molecular links between COPD and lung cancer: new targets for drug discovery? Expert Opin Ther Targets. 2019;23(6):539–553. doi:10.1080/14728222.2019.1615884
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.