Back to Journals » Lung Cancer: Targets and Therapy » Volume 8
65Plus: open-label study of bevacizumab in combination with pemetrexed or pemetrexed/carboplatin as first-line treatment of patients with advanced or recurrent nonsquamous non-small-cell lung cancer
Authors Schuette W, Schneider CP, Engel-Riedel W, Schumann C ![]() , Kohlhaeufl M, Serke MHU, Hoeffken G
, Kohlhaeufl M, Serke MHU, Hoeffken G ![]() , Kortsik C, Reck M
, Kortsik C, Reck M
Received 31 May 2017
Accepted for publication 5 September 2017
Published 6 November 2017 Volume 2017:8 Pages 217—229
DOI https://doi.org/10.2147/LCTT.S142972
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Pan-Chyr Yang
Wolfgang Schuette,1 Claus-Peter Schneider,2,3 Walburga Engel-Riedel,4 Christian Schumann,5,6 Martin Kohlhaeufl,7 Monika Heidi Ursel Serke,8 Gert Hoeffken,9 Cornelius Kortsik,10 Martin Reck11
1Department of Internal Medicine II, Hospital Martha-Maria Halle-Doelau, Halle, 2Department of Pneumonology, Central Hospital, Bad Berka, 3Department of Internal Medicine, DRK Manniske Hospital, Bad Frankenhausen, 4Cologne Clinics, Merheim Lung Hospital, Cologne, 5Pneumonology, Department of Internal Medicine II, University Hospital Ulm, 6Clinic for Pneumology, Thoracic Oncology, Sleep, and Respiratory Critical Care, Kempten-Oberallgäu, 7Center of Pneumonology and Chest Surgery, Hospital Schillerhoehe, Gerlingen, 8Pneumonology, Lung Clinics, Hemer, 9Center of Pneumonology, Chest and Vascular Surgery, Specialty Hospital Coswig, Coswig, 10Department of Pneumonology, Catholic Hospital, Mainz, 11Department of Thoracic Oncology, Lung Clinic, Grosshansdorf, Germany
Background: The aim of the study was to investigate in terms of noninferiority the efficacy and safety of a monochemotherapy regimen of pemetrexed plus bevacizumab (BevPem) versus carboplatin/pemetrexed plus bevacizumab (BevCPem) in elderly patients as first-line treatment for advanced metastatic or recurrent nonsquamous non-small-cell lung cancer (NSCLC).
Materials and methods: 65Plus was a Phase III, randomized, open-label study. In total, 253 patients received BevPem (n=119) or BevCPem (n=134). The primary outcome measure was progression-free survival. Secondary end points were overall survival, tumor response, and safety outcomes. Evaluations were performed for the whole study population and stratified according to Eastern Cooperative Oncology Group (ECOG) performance status (PS).
Results: Noninferiority of BevPem in comparison to BevCPem could not be demonstrated for the overall population (P=0.7864). Significant superiority of the combined treatment BevCPem was seen in patients of ECOG PS 0–1 (median PFS 5.1 vs 6.9 months, HR 1.353, 95% CI 1.03–1.777), while the opposite tendency was observed in patients with ECOG PS 2 (median PFS 2.9 vs 1.5 months, HR 0.628, 95% CI 0.195–2.025). Overall, better tolerability was found for the BevPem group, irrespective of ECOG PS.
Conclusion: Results from the 65plus study give evidence that BevPem and BevCPem treatments may exert differential effects on PFS, depending on the patients ECOG PS. It appears that patients with better ECOG PS (0–1) benefited more from the combined treatment with carboplatin, while the group comprising more severely impaired patients (ECOG PS 2) benefited more from the monochemotherapy.
Keywords: bevacizumab, pemetrexed, carboplatin, NSCLC, elderly patients
Introduction
Platinum-based chemotherapy is the standard treatment for advanced-stage (IV) nonsquamous non-small-cell lung cancer (NSCLC). It significantly improves survival and achieves better symptom control than best-supportive care.1,2 In Phase III trials, doublet combinations of cisplatin with taxanes (paclitaxel or docetaxel), gemcitabine, vinorelbine, irinotecan, or pemetrexed (Pem) have produced superior therapeutic results compared with cisplatin alone, but no particular two-drug, platinum-based combination has been identified as superior to the others with respect to its efficacy.3–7 However, some of these combinations appear to have a better tolerability and safety profile than others. For instance, this has been demonstrated for the combination of cisplatin with Pem when compared to a doublet combination of cisplatin with gemcitabine.8 Furthermore, combination with bevacizumab (Bev), a recombinant, humanized monoclonal antibody targeting VEGF essential for tumor-associated angiogenesis, led to an improved outcome and acceptable safety risk, especially for patients with nonsquamous NSCLC.9 Therefore, it was hypothesized that the combination of carboplatin, Pem, and Bev (BevCPem) may have improved efficacy, especially in a patient population of this particular histological type. In fact, this has been proven in a Phase II study, where BevCPem was shown to be efficacious and of acceptable toxicity.10 The treatment regimen of this study included induction therapy with BevCPem followed by maintenance BevPem. On the other hand, the PointBreak study did not show superiority of this special combination with respect to most of the outcome parameters, although progression-free survival (PFS) was significantly improved compared to treatment with paclitaxel/carboplatin plus Bev.11 Nevertheless, by the time of the start of the 65plus study, the BevCPem combination was assumed to be very efficacious and tolerable. The study was based on the hypothesis that BevPem might be potent enough, especially in elderly patients with nonsquamous NSCLC, to enable the omission of carboplatin, which would result in a combination treatment that shows comparable efficacy on one hand and exhibits a significantly better tolerability profile on the other. Non-platinum-containing regimens are increasingly being accepted, and may be used as alternatives to platinum-based regimens in the first-line setting. For elderly patients or patients with available Eastern Cooperative Oncology Group (ECOG) performance status (PS) 2 data support the use of single-agent chemotherapy.12 Therefore, the population selected for the 65plus study included only elderly patients (≥65 years), as it was deemed to be mandatory to obtain full efficacy for younger patients, whereas the improved toxicity profile without carboplatin might be of higher importance for the elderly.
Materials and methods
Eligibility
Patients were eligible for the study if they were aged at least 65 years, had histologically or cytologically documented inoperable, locally advanced (stage IIIB with supraclavicular lymph-node metastases or malignant pleural or pericardial effusion), metastatic (stage IV) or recurrent NSCLC other than squamous NSCLC, at least one measurable lesion according to Response Evaluation Criteria in Solid Tumors (RECIST),13 ECOG PS of 2 or less,14 and life expectancy of at least 12 weeks. Patients were also required to have adequate hematological, blood-clotting, hepatic, and renal function.
Patients with mixed non-small cell and small cell tumors or mixed adenosquamous carcinomas with a predominantly squamous component and those who had received prior platinum-based or other chemotherapy regimens for advanced disease were ineligible for the study. However, prior chemotherapy given as neoadjuvant or adjuvant therapy for early-stage disease and completed at least 6 months prior to diagnosis of advanced-stage disease was not counted as a prior regimen. Major exclusion criteria further encompassed history of hemoptysis, tumors invading major blood vessels, radiotherapy, major surgery, significant traumatic injury within 28 days prior to enrolment, anticipation of the need for major surgery during study treatment, minor surgery within 24 hours prior to the first Bev infusion, history of inherited bleeding diathesis or coagulopathy with the risk of bleeding, use of full-dose anticoagulants or thrombolytic agents for therapeutic purposes, inability to interrupt salicylates or other nonsteroidal anti-inflammatory drugs (with the exception of low-dose aspirin), uncontrolled hypertension or clinically significant cardiovascular disease, nonhealing wounds, active peptic ulcers or bone fractures, history of abdominal fistulae, gastrointestinal perforation or intra-abdominal abscess within 6 months of enrolment, presence of clinically significant third-space fluid collections that could not be controlled by drainage or other procedures, history of diverticulitis, and yellow-fever vaccination within 30 days of enrolment. The protocol was conducted in accordance with the Declaration of Helsinki and Good Clinical Practice guidelines15 and was approved by each center’s ethics committee (Table S1). All patients signed written informed consent before treatment.
Treatment schedule
This trial was registered under the ClinicalTrials.gov identifier NCT00976456. The study was conducted as a randomized, open-label, multicenter, comparative Phase III study. Eligible patients were randomly assigned to one of two parallel-treatment arms. Patients in arm A received Bev 7.5 mg/kg plus Pem 500 mg/m2 as a 10-minute intravenous (IV) infusion on day 1 of each 3-week cycle. Patients in arm B were treated with Bev 7.5 mg/kg plus combination chemotherapy consisting of Pem 500 mg/m2 as a 10-minute IV infusion and carboplatin AUC 5 as a 30- to 60-minute IV infusion. The first Bev treatment was administered as an IV infusion over 90 minutes after chemotherapy. If the first infusion was well tolerated, the second infusion was given over 60 minutes and all subsequent infusions over 30 minutes. Patients should have received study medication for at least four cycles to a maximum of six cycles or until unmanageable toxicity or diagnosis of disease progression if occurring earlier. In the subsequent maintenance phase, patients in arm A and arm B who had experienced complete response (CR), partial response (PR), or stable disease were further treated with Bev monotherapy until disease progression, unmanageable toxicity, or withdrawal of patient consent. If appropriate, patients could also receive BevPem as maintenance therapy at the investigator’s discretion.
Clinical end points
The primary objective of the trial was to prove the noninferior efficacy of a monochemotherapy regimen of BevPem versus a combination-chemotherapy regimen of BevCPem in elderly patients as first-line treatment for advanced or recurrent nonsquamous NSCLC. The primary end point was PFS. The secondary objectives of this trial were to evaluate the efficacy of Bev by overall survival (OS) and overall response rate and assess the safety of Bev in combination with Pem, as well as with carboplatin plus Pem. In particular, the incidence of serious adverse events (SAEs) related to Bev and the incidence of specific AEs, such as wound-healing complications, gastrointestinal perforations, arterial and venous thromboembolic events, hemoptysis, central nervous system bleeding, and other hemorrhages, were investigated. Tumor assessments were performed every second cycle (ie, before cycles 3 and 5 and after cycle 6). Measurements were done according to RECIST criteria, ie, longest diameter of target lesions, determined by the investigators. Safety was evaluated as the incidence of AEs graded using National Cancer Institute Common Terminology Criteria for Adverse Events (version 3.0) and changes in laboratory tests or vital signs.
Statistical methods
Based on the data available for combination therapy with Bev, a median PFS of 5.5 months for BevCPem was expected. Taking into account the available data on PFS in the literature, a difference of 1.5 months seemed justified and acceptable as threshold for noninferiority in median PFS. Assuming equality of the true median PFS, a one-sided significance level of 5%, accrual period of 24 months, and whole-study duration of 42 months, 271 patients had to be recruited. According to the fact that the required statistical power of 80% would be reached by the occurrence of 227 events, the final analysis was done at the time point of appearance of the 227th event.
All other end points were evaluated in an explorative manner. If P-values were calculated (eg, in subgroup comparisons or across treatment arms), they were presented referring to hypotheses of differences between the two treatment arms. Event-related data, such as PFS and OS, were estimated by the Kaplan–Meier method16 and evaluated using the log-rank test. If the Peto and Peto log-rank test17 were not appropriate because of violation of the proportional-hazard assumption, Gehan’s generalization of the Wilcoxon rank-sum test for censored data18 was applied, preferably in its modification by Peto and Peto17 and Prentice.19 To test the noninferiority of the BevPem treatment relative to BevCPem treatment with regard to median PFS, the method for median PFS difference based on asymptotically standard normally distributed test statistics20 was applied. Overall response rate, toxicity, and other event rates were calculated and CIs provided. For comparisons between patient groups, these rates were analyzed by Fisher’s exact test, c2 test, or Mantel–Haenszel test, respectively. Noninferiority assessment was done on the per-protocol set; all other analyses were performed according to the intent-to-treat (ITT) principle.
Results
Patient characteristics
A total of 271 patients were randomly assigned to one of the two treatment regimens at 27 centers throughout Germany. Demographic and baseline disease characteristics were generally well balanced between the groups. Overall, more males than females were included in both treatment groups. Median weight and body-mass index were in the age-adequate range for patients in both arms. Most patients suffered from adenocarcinoma and stage IV disease (Table 1).
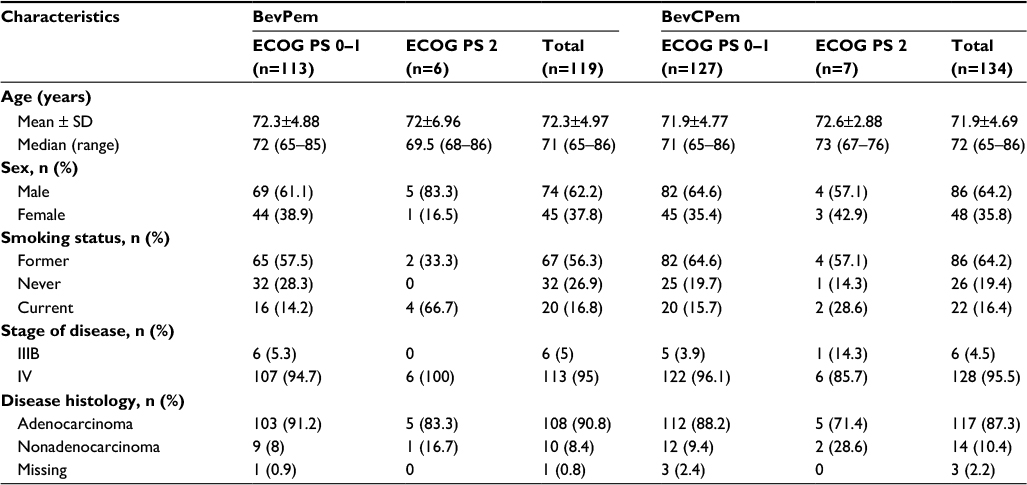 | Table 1 Patient demographic and baseline characteristics Abbreviations: ECOG PS, Eastern Cooperative Oncology Group performance status; BevPem, bevacizumab + pemetrexed; BevCPem, bevacizumab + carboplatin/pemetrexed. |
Analysis sets
Of 271 randomized patients, 253 were included in the safety-analysis set which corresponded to the full-analysis set (ITT). In arm A, 16 patients were excluded from the ITT set. “Screening failure” was the most common reason for the exclusion of patients from the ITT set, which was complemented by “patient received no study medication”. In arm B, two patients were excluded from the different analysis sets (Figure 1). The per-protocol set excluded major protocol violations and consisted of 252 patients. One patient was excluded from the per-protocol set in arm A. The reason for the exclusion of that patient was a reduced Bev dose for several cycles. It thus almost corresponded to the ITT set.
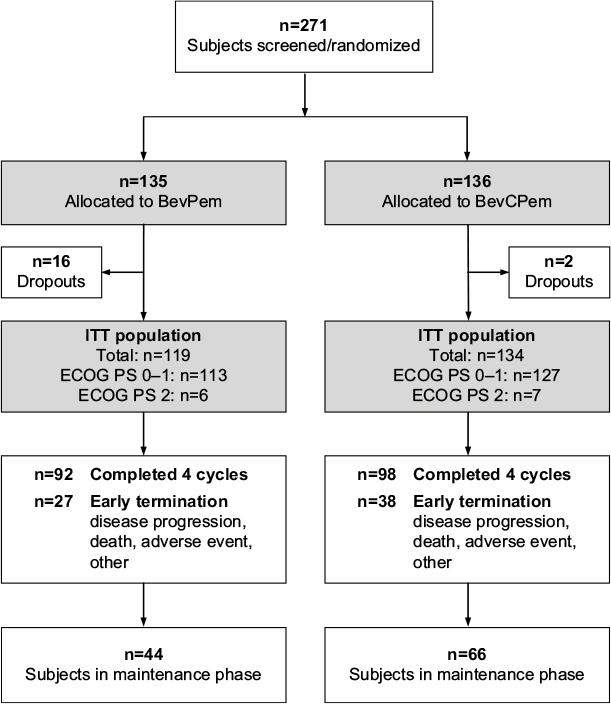 | Figure 1 CONSORT diagram. Abbreviations: CONSORT, Consolidated Standards of Reporting Trials; BevPem, bevacizumab + pemetrexed; BevCPem, bevacizumab + carboplatin/pemetrexed; ECOG PS, Eastern Cooperative Oncology Group performance status; ITT, intention to treat. |
Treatments
Patients received up to six cycles of backbone chemotherapy. Maintenance therapy consisted of Bev with or without Pem in both treatment arms. Overall, the mean number of all treatment cycles (backbone and maintenance chemotherapy combined) was 7.9±6.99 in arm A and 10.5±9.33 in arm B, with up to 28 cycles in arm A and 52 cycles in arm B. In arm A, 119 patients received at least one cycle of backbone chemotherapy, with a median number of four treatment cycles (mean 3.8±1.8). Seventeen patients (14.3%) were treated with one cycle only, and 34 patients (28.6%) received six cycles of the backbone chemotherapy regimen. In arm B, 134 patients were treated with at least one cycle of backbone chemotherapy, also with a median number of four treatment cycles (mean 3.9±1.7). In this arm, 18 patients (13.4%) underwent one cycle and 26 patients (26.9%) received six cycles of backbone chemotherapy.
In arm A, 73 patients (61.3%) did not enter the maintenance therapy phase compared to 64 patients (47.8%) in arm B. Consequently, the median number of maintenance treatment cycles was 0 in arm A, with a mean of 4.1±5.8 cycles. Patients were treated with up to 22 cycles of maintenance therapy (n=1, 0.8%). In arm B, patients were treated with a median number of six cycles of maintenance therapy, and also the mean number of treatment cycles was higher compared to arm A (6.7±8.36). The maximum number of treatment cycles was 46 (n=1, 0.7%).
Efficacy
Non-inferiority of the monochemotherapy BevPem in comparison to the treatment combination BevCPem with respect to the primary endpoint PFS (Figure 2A) could not be demonstrated (P=0.7864). There was a significant difference in favor of the combined treatment with carboplatin in PFS based survival curves, median PFS and hazard ratio in the group of patients with an ECOG PS of 0–1 (Figure 2B). The reverse tendency, favoring the monochemotherapy, was seen in the group of patients with ECOG PS 2 (Figure 2C). However, the small sample size of this group did not allow any reliable conclusion.
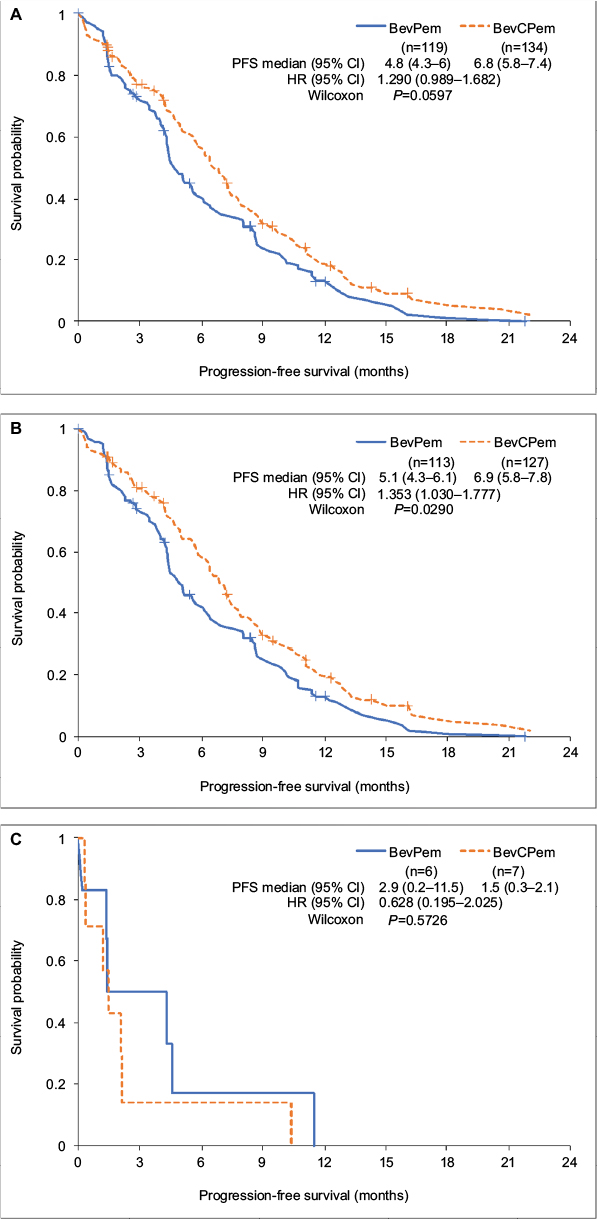 | Figure 2 Kaplan–Meier estimates of progression-free survival (PFS) for the ITT population. Notes: (A) Total population; (B) ECOG PS 0–1; (C) ECOG PS 2. Abbreviations: ITT, intention to treat; ECOG PS, Eastern Cooperative Oncology Group performance status; BevPem, bevacizumab + pemetrexed; BevCPem, bevacizumab + carboplatin/pemetrexed. |
For the overall population relevant differences between the treatments in the secondary endpoint OS were not observed, not even if stratified according to ECOG PS (Figure 3). The one-year survival rate was 0.487 (95% CI 0.389–0.587) and 0.585 (95% CI 0.493–0.665) for BevPem and BevCPem, respectively. Superiority of the treatment combination with carboplatin in the response rate (CR plus PR) and the disease control rate (CR plus PR plus SD) as compared to the monochemotherapy was reached in the group of patients with an ECOG performance status of 0-1 and in patients overall (Table 2). Subgroup analyses with regard to the age revealed a significantly greater benefit for patients younger than 70 years of the combination treatment with carboplatin with median PFS of 8.2 months (95% CI 6.1–9.8) in the BevCPem group compared to 4.9 months (95% CI 4.0–6.9) in the BevPem group (Wilcoxon test P=0.0271) whereas for patients older than 70 years the superiority of the combination treatment was not significant (Figure 4A).
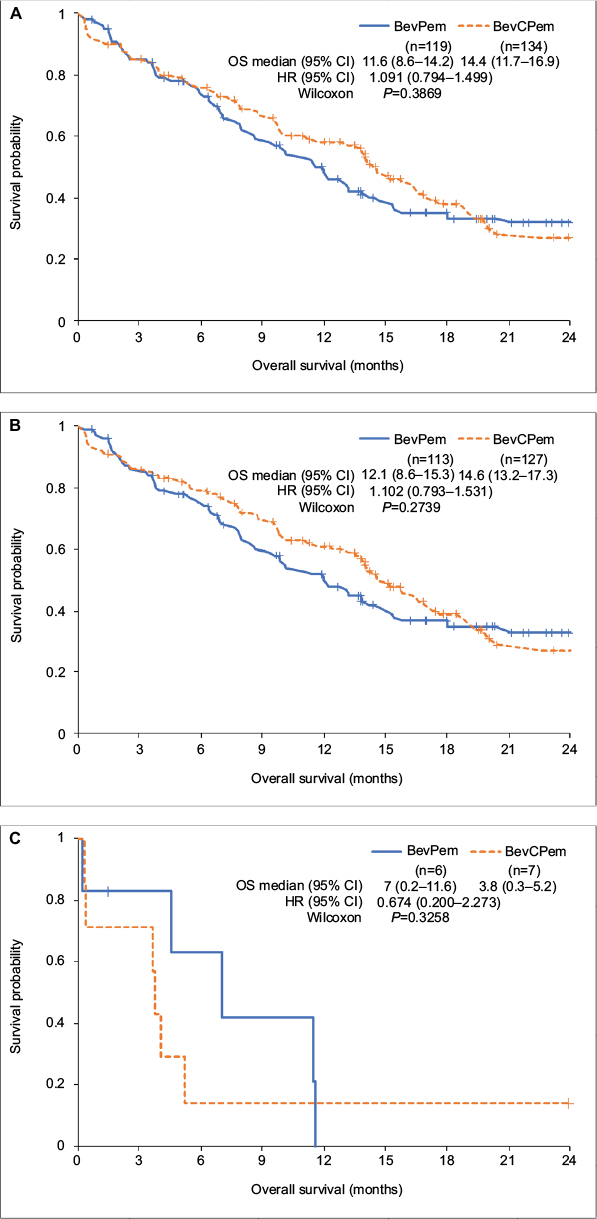 | Figure 3 Kaplan–Meier estimates of overall survival (OS) for the ITT population. Notes: (A) Total population; (B) ECOG PS 0–1; (C) ECOG PS 2. Abbreviations: ITT, intention to treat; ECOG PS, Eastern Cooperative Oncology Group performance status; BevPem, bevacizumab + pemetrexed; BevCPem, bevacizumab + carboplatin/pemetrexed. |
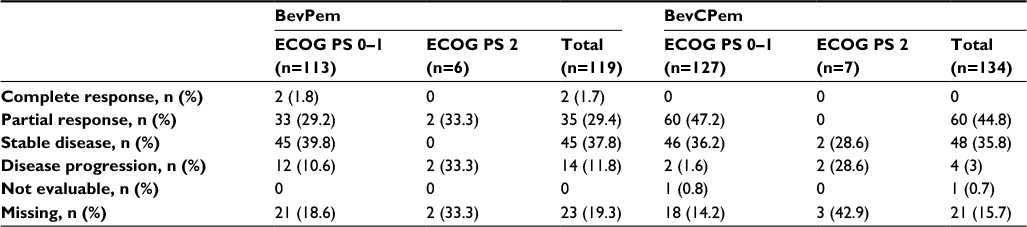 | Table 2 Overall best response according to RECIST Abbreviations: ECOG PS, Eastern Cooperative Oncology Group performance status; RECIST, Response Evaluation Criteria in Solid Tumors; BevPem, bevacizumab plus pemetrexed; BevCPem, bevacizumab plus carboplatin/pemetrexed. |
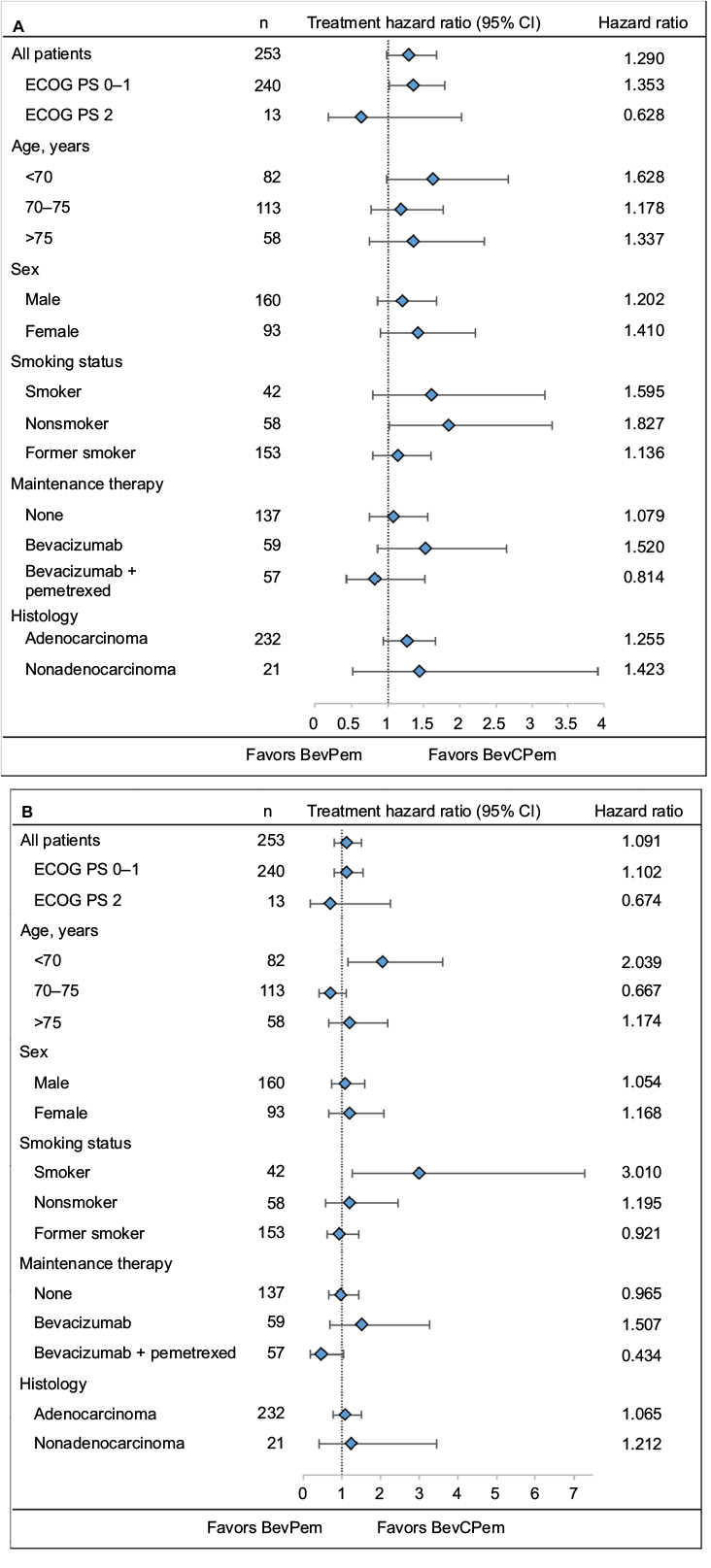 | Figure 4 Forest plots for the intent-to-treat population. Notes: (A) Progression-free survival; (B) overall survival. Abbreviations: ECOG PS, Eastern Cooperative Oncology Group performance status; BevPem, bevacizumab + pemetrexed; BevCPem, bevacizumab + carboplatin/pemetrexed. |
Moreover, as already seen for the primary endpoint PFS the OS was also significantly improved for patients younger than 70 years when treated with BevCPem in comparison to the monochemotherapy (median survival times 17.3 months [95% CI: 13.9–22.7] vs 9.7 months (95% CI 6.9–14.2); Wilcoxon test P=0.0039) but the benefit was less pronounced for the elderly (Figure 4B).
Safety
Overall, SAEs were reported in about half of all patients in both treatment arms (54.6% in arm A and 54.5% in arm B). In about a third of patients, those events were regarded as probably related to study treatment (32.8% in arm A and 32.1% in arm B). In general, both AEs and SAEs were documented at higher patient rates during backbone chemotherapy compared to the maintenance phase. Also, the rate of SAEs probably related to study treatment was more than twice as high during backbone chemotherapy compared to maintenance (27.7% vs 13% in arm A and 28.4% vs 12.9% in arm B).
Rates of patients experiencing Common Terminology Criteria for Adverse Events (CTCAE) grade 3 or 4 toxicities were comparable across the treatment arms (63.9% in arm A and 65.7% in arm B). When analyzed separately, the rate of patients in whom grade 3 events occurred was also similar in both treatment arms (60.5% in arm A and 61.9% in arm B). However, grade 4 toxicities were reported at a rate almost twice as high under BevCPem (17.6% in arm A compared to 31.3% in arm B). This difference was also observed across groups with various ECOG PS.
The majority of grade 4 toxicities occurred in the system-organ class “blood and lymphatic system disorders”, with the most frequently reported events being neutropenia, thrombocytopenia, and leukopenia, which were all found at higher rates under BevCPem. Overall, the three most commonly affected system-organ classes were “general disorders and administration-site conditions” (mainly asthenia and pain), “blood and lymphatic system disorders”, and “gastrointestinal disorders”, for all of which higher rates were observed for BevCPem compared to BevPem (Table 3).
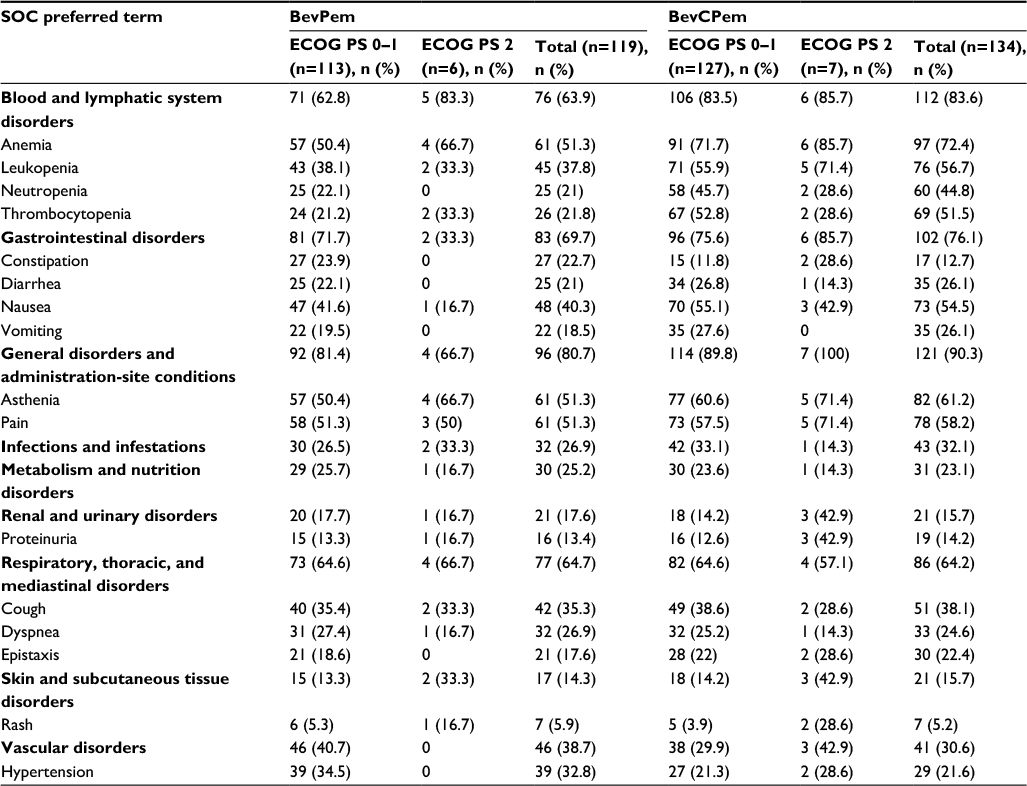 | Table 3 Commonly occurring adverse events (population assessable for safety) Abbreviations: SOC, system-organ class; ECOG PS, Eastern Cooperative Oncology Group performance status; BevPem: bevacizumab + pemetrexed; BevCPem: bevacizumab + carboplatin/pemetrexed. |
A higher rate of patients discontinued the study due to AEs under BevCPem compared to BevPem. While study treatment was delayed in almost a third of patients in both treatment arms, reduction of study medication occurred twice as often in patients treated with BevCPem. AEs of special interest occurring during the 6-month follow-up were arterial and venous thromboembolic events, hypertension, proteinuria, and severe hemorrhages, which were reported at higher rates under BevPem compared to BevCPem.
Discussion
This study failed to demonstrate noninferior efficacy of BevPem versus BevCPem in elderly patients as first-line treatment of advanced metastatic or recurrent nonsquamous NSCLC. The analysis stratified by PS suggested opposite tendencies of treatment effects in the two ECOG PS groups. While patients in good health (ECOG PS 0–1) tended to benefit more from combination treatment with carboplatin, frail patients (ECOG PS 2) tended to benefit more from monochemotherapy. This tendency was seen for PFS and response rates. The diverging responses of the ECOG PS groups to the treatments were more distinctly seen under BevCPem and less pronounced under BevPem. However, the interpretation of differential effects of the treatments depending on the PS of the patients is limited by the imbalanced group sizes. The overall results of the 65plus study were relativized by subgroup analyses according to different age clusters (Figure 4).
Similar conditions were found for the BevCPem group in the PointBreak study,11 with the median age in both studies being 64.6 and 71.2 years. A trend was seen in elderly patients for a slight superiority in PFS of 6 months in the PointBreak study versus 6.8 months in the 65plus study, and OS was 12.6 months versus 14.4 months, respectively. In a secondary analysis of the PointBreak study, Langer et al21 showed a survival benefit for patients aged under 75 years for combination with Bev compared to administration of paclitaxel and carboplatin alone that was not found for patients older than 75 years.
With regard to the safety measures in the 65plus study, no difference between BevPem and BevCPem was observed, as evidenced by comparable rates of patients experiencing both AEs and SAEs. Also, a probable relationship of SAEs to study treatment was seen at comparable rates. However, CTCAE grade 4 events occurred more frequently in patients treated with the combination regimen. Overall, treatment with monochemotherapy was demonstrated to be more tolerable than combination therapy.
Conclusion
Results from the 65plus study suggest that for younger patients and those in good general state of health (ECOG PS 0–1), the addition of carboplatin might be obligatory due to significant benefit, whereas (keeping in mind the expected toxicity) doublet chemotherapy should be carefully considered for elderly patients with impaired ECOG PS, ie, the omission of carboplatin might be an alternative treatment option for this population.
Acknowledgments
We would like to thank all patients, their families, the investigators, and the nurses who participated in this trial. This study was cofunded by Eli Lilly Ltd and Roche Pharma AG, Grenzach-Wyhlen, Germany.
Disclosure
WS reports grants from Pfizer, Lilly, and Merck, and grants and personal fees from Roche Pharma AG, Amgen, Sanofi-Aventis, and AstraZeneca, not related to this work. CPS reports grants from Eli Lilly, including during this study, personal fees from Roche, and grants and personal fees from AstraZeneca, BMS, and Boehringer Ingelheim, not related to this work. MR reports personal fees from Hoffmann-La Roche, Lilly, Boehringer-Ingelheim, AstraZeneca, BMS, MSD, Pfizer, Merck, Celgene, Abbot, and Novartis, not related to this work. The other authors report no conflicts of interest in this work.
References
Non-small Cell Lung Cancer Collaborative Group. Chemotherapy in non-small cell lung cancer: a meta-analysis using updated data on individual patients from 52 randomised clinical trials. BMJ. 1995;311(7010):899–909. | ||
Johnson DH. Evolution of cisplatin-based chemotherapy in non-small cell lung cancer: a historical perspective and the Eastern Cooperative Oncology Group experience. Chest. 2000;117(4 Suppl 1):133S–137S. | ||
Bonomi P, Kim K, Fairclough D, et al. Comparison of survival and quality of life in advanced non-small-cell lung cancer patients treated with two dose levels of paclitaxel combined with cisplatin versus etoposide with cisplatin: results of an Eastern Cooperative Oncology Group trial. J Clin Oncol. 2000;18(3):623–631. | ||
Cardenal F, López-Cabrerizo MP, Antón A, et al. Randomized phase III study of gemcitabine-cisplatin versus etoposide-cisplatin in the treatment of locally advanced or metastatic non-small-cell lung cancer. J Clin Oncol. 1999;17(1):12–18. | ||
Giaccone G, Splinter TA, Debruyne C, et al. Randomized study of paclitaxel-cisplatin versus cisplatin-teniposide in patients with advanced non-small-cell lung cancer. J Clin Oncol. 1998;16(6):2133–2141. | ||
Sandler AB, Nemunaitis J, Denham C, et al. Phase III trial of gemcitabine plus cisplatin versus cisplatin alone in patients with locally advanced or metastatic non-small-cell lung cancer. J Clin Oncol. 2000;18(1):122–130. | ||
Wozniak AJ, Crowley JJ, Balcerzak SP, et al. Randomized trial comparing cisplatin with cisplatin plus vinorelbine in the treatment of advanced non-small-cell lung cancer: a Southwest Oncology Group study. J Clin Oncol. 1998;16(7):2459–2465. | ||
Scagliotti GV, Parikh P, von Pawel J, et al. Phase III study comparing cisplatin plus gemcitabine with cisplatin plus pemetrexed in chemotherapy-naive patients with advanced-stage non-small-cell lung cancer. J Clin Oncol. 2008;26(21):3543–3551. | ||
Sandler A, Yi J, Dahlberg S, et al. Treatment outcomes by tumor histology in Eastern Cooperative Group study E4599 of bevacizumab with paclitaxel/carboplatin for advanced non-small cell lung cancer. J Thorac Oncol. 2010;5(9):1416–1423. | ||
Patel JD, Hensing TA, Rademaker A, et al. Phase II study of pemetrexed and carboplatin plus bevacizumab with maintenance pemetrexed and bevacizumab as first-line therapy for nonsquamous non-small-cell lung cancer. J Clin Oncol. 2009;27(20):3284–3289. | ||
Patel JD, Socinski MA, Garon EB, et al. PointBreak: a randomized phase III study of pemetrexed plus carboplatin and bevacizumab followed by maintenance pemetrexed and bevacizumab versus paclitaxel plus carboplatin and bevacizumab followed by maintenance bevacizumab in patients with stage IIIB or IV nonsquamous non-small-cell lung cancer. J Clin Oncol. 2013;31(34):4349–4357. | ||
Pfister DG, Johnson DH, Azzoli CG, et al. American Society of Clinical Oncology treatment of unresectable non-small-cell lung cancer guideline: update 2003. J Clin Oncol. 2004;22(2):330–353. | ||
Therasse P, Arbuck SG, Eisenhauer EA, et al. New guidelines to evaluate the response to treatment in solid tumors. European Organization for Research and Treatment of Cancer, National Cancer Institute of the United States, National Cancer Institute of Canada. J Natl Cancer Inst. 2000;92(3):205–216. | ||
Oken MM, Creech RH, Tormey DC, et al. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am J Clin Oncol. 1982;5(6):649–655. | ||
US Food and Drug Administration. Guidance for Industry. E6 Good Clinical Practice: Consolidated Guidance. Available from: http://www.fda.gov/downloads/drugs/guidances/ucm073122.pdf. Accessed April 30, 1996. | ||
Kaplan EL, Meier P. Nonparametric estimation from incomplete observations. J Am Stat Assoc. 1958;53:457–481. | ||
Peto R, Peto J. Asymptotically efficient rank in variation test procedures (with discussion). J R Stat Soc. 1972;35(A):185–206. | ||
Gehan EA. A generalized Wilcoxon test for comparing arbitrarily singly-censored samples. Biometrika. 1965;52(1–2):203–223. | ||
Prentice RL. Linear rank tests with right censored data. Biometrika. 1978;65:167–179. | ||
de Silva GT, Logan BR, Klein JP. Methods for equivalence and non-inferiority testing. Biol Blood Marrow Transplant. 2008;15(1 Suppl):120–127. | ||
Langer CJ, Socinski MA, Patel JD, et al. Isolating the role of bevacizumab in elderly patients with previously untreated nonsquamous non-small cell lung cancer: secondary analyses of the ECOG 4599 and PointBreak trials. Am J Clin Oncol. 2016;39(5):441–447. |
Supplementary material
 | Table S1 Ethics committees |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.