Back to Journals » Journal of Asthma and Allergy » Volume 16
1-Year Prospective Study of the Relationship of Serial Exhaled Nitric Oxide Level and Asthma Control
Authors Ko FWS ![]() , Chan KP, Ng JKC, Ngai JC, Yip WH, Lo RLP, Chan TO, Hui DSC
, Chan KP, Ng JKC, Ngai JC, Yip WH, Lo RLP, Chan TO, Hui DSC ![]()
Received 13 April 2023
Accepted for publication 30 June 2023
Published 14 July 2023 Volume 2023:16 Pages 725—734
DOI https://doi.org/10.2147/JAA.S417117
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Luis Garcia-Marcos
Fanny Wai San Ko,1 Ka Pang Chan,1 Joyce Ka Ching Ng,1 Jenny CL Ngai,1 Wing Ho Yip,1 Rachel Lai Ping Lo,1 Tat On Chan,2 David Shu Cheong Hui1
1Department of Medicine and Therapeutics, the Chinese University of Hong Kong, Hong Kong, People’s Republic of China; 2The Jockey Club School of Public Health and Primary Care, The Chinese University of Hong Kong, Hong Kong, People’s Republic of China
Correspondence: David Shu Cheong Hui, Department of Medicine and Therapeutics, the Chinese University of Hong Kong, Prince of Wales Hospital, 30-32 Ngan Shing Street, Shatin, NT, Hong Kong, Tel +852 35053128, Email [email protected]
Background and Objective: Previous studies found that the fractional nitric oxide concentration in exhaled breath (FeNO) levels in healthy Chinese adults was higher than in White adults. More understanding of serial changes of FeNO levels with asthma control in a real-life clinical setting would be important to explore the utility of this biomarker in routine asthma management. This study assessed the FeNO levels of Chinese asthma subjects with different levels of asthma control and the serial changes with respect to the changes in asthma control over 1 year.
Methods: A 12-month prospective study (subjects recruited between November 2019 and January 2021) with serial measurement of FeNO levels at baseline, 4, 8 and 12 months. Asthma control was assessed by the Global Initiative for Asthma classification, Asthma Control Test (ACT) and Asthma Control Questionnaire (ACQ).
Results: Altogether, 136 subjects (mean age 51.51± 15.09 years, 46[33.8%] male) had successful baseline FeNO measurements. At baseline, the FeNO levels did not show a statistically significant difference for controlled, partly controlled and uncontrolled asthma according to GINA classification, ACT and ACQ. FeNO levels decreased with improving asthma control and stayed at similar levels with unchanged or worsening asthma control for all subjects. For subjects with baseline blood eosinophil levels ≥ 300 cells/μL(n=59), FeNO levels decreased with improving asthma control, stayed similar without change for asthma control and increased with worsening asthma control. Receiver operating characteristic (ROC) analysis with the highest area under curve (AUC) for changes in FeNO levels for improving asthma control was between ≤ − 10 to − 25 ppb at various time points in the 12-month study.
Conclusion: Changes in FeNO levels over time were associated with changes in clinical asthma control, particularly in those with higher blood eosinophil count and are likely more useful than a single time point measurement in managing asthma.
Keywords: asthma, FeNO, serial measurement
Introduction
Measurement of fractional nitric oxide concentration in exhaled breath (FeNO) has been shown to be a non-invasive, quantitative biomarker for eosinophilic airway inflammation. FeNO levels correlated with features of T2 inflammation, in particular with the eosinophil levels in induced sputum and peripheral blood.1–3 Both the innate immune system and the adaptive immune system drive T2 inflammation. The former is triggered by pollutants or infections involving type 2 innate lymphoid cells and the latter is activated by contact with allergens involving type 2 T-helper cells.4 Our recent study found that about 70% of moderate and severe asthma patients had features of type 2 inflammation indicated by elevated blood eosinophils and/or immunoglobulin E (IgE) levels.5
FeNO is now used as a biomarker for guiding the initiation of biologic therapy in asthma.6,7 It can also support the diagnosis of asthma.8,9 A meta-analysis found that when compared to clinical symptoms, tailoring asthma medications based on FeNO levels decreased the frequency of asthma exacerbations. However, FeNO-based approach did not impact day-to-day clinical symptoms, end-of-study FeNO levels, lung function or inhaled corticosteroid (ICS) dose. The studies included in this meta-analysis ranged from 18 to 52 weeks in duration. In addition, the FeNO cutoff values among the studies were variable.10
The latest American Thoracic Society (ATS) guideline on FeNO has made a conditional recommendation that in patients with asthma in whom treatment is being considered, FENO is beneficial and should be used in addition to usual care.8 More understanding of serial changes of FeNO levels with asthma control in a real-life clinical setting would be important to explore the utility of this biomarker in routine asthma management.
Previous studies of FeNO and asthma control were limited to retrospective11 or single-time point assessments.12,13 There are limited prospective adult data on serial FeNO levels and asthma control, with some studies focusing on the relationship with asthma exacerbations and some on children.14,15 Our previous study on FeNO in healthy Chinese populations observed a higher level of FeNO than in the Caucasian population.16 To the best of our knowledge, correlation between changes in FeNO level and changing levels of asthma control among Chinese has not been studied. The latest ATS FeNO guideline has suggested a need for larger trials that evaluate the use of FENO testing to monitor therapy with serial measurements once the FeNO level is established.8
The primary aim of this study was to assess the FeNO levels of Chinese asthma subjects with different levels of asthma control. The secondary aim was to assess serial changes in levels of FeNO in Chinese asthma patients with respect to the changes in asthma control in a real-life clinical setting over 1 year. Understanding the baseline and serial changes in FeNO would contribute more to the potential role of this biomarker.
Methods
This was a prospective study of FeNO levels and asthma control over a period of 12 months. Subjects were recruited between November 2019 and January 2021 from the respiratory clinic of the Prince of Wales Hospital, Hong Kong. The study (ClinicalTrial.gov registration number NCT04125316) was approved by the Joint Chinese University of Hong Kong-New Territories East Cluster Clinical Research Ethics Committee (CREC 2019.395). All recruited subjects had signed informed written consent. The manuscript complied with the Declaration of Helsinki.
Chinese subjects aged between 18 and 90 years who had a diagnosis of asthma were recruited. Asthma was defined as those with a consistent history and prior documented evidence of variable airflow obstruction, with evidence of an increase in FEV1 greater than 12% or 200mL following bronchodilator or bronchial hyperresponsiveness on bronchial provocation testing when stable Exclusion criteria were patients with other known respiratory diseases, including chronic obstructive pulmonary disease, bronchiectasis, tuberculosis with destroyed lung parenchyma, history of lung resection and lung cancer, individuals older than 40 years with a smoking history of more than 10 pack-years, current smokers (smoking in the past 12 months), patients currently randomised in other clinical studies and pregnant women.
Demographic characteristics of the subjects were collected, including age, gender, weight, height, medications, co-morbidities and asthma exacerbations in the past 12 months. Blood tests (including eosinophil count and total IgE levels), spirometry and skin prick tests were performed at baseline. Spirometry (pre- and post-bronchodilator) was performed according to the American Thoracic Society and European Respiratory Society standards.17 The updated predicted spirometry values for Hong Kong Chinese were used to calculate the predicted lung function.18 Skin prick test was performed with a panel of allergen extracts including cat, dog, Dermatophagoides pteronyssinus and Dermatophagoides farinae, aspergillus, mould mix, tree mix and cockroach (ALK, USA and Greer, USA). A minimum wheal size of 3 mm was defined as a positive response.
FeNO levels and asthma control were assessed at baseline, 4, 8 and 12 months. FeNO levels were measured online using a NIOX VERO (Circassia, Uppsala, Sweden) according to ATS/ERS recommendations19 before spirometry. Subjects were tested in a sitting position (with no nose clip), exhaled to residual volume, inserted a mouthpiece, inhaled to total lung capacity, and then exhaled for 10 seconds at a constant flow rate of 50mL/s. The measurement was repeated until three FeNO values varied less than 10% or two values varied less than 5%. The mean FeNO (in ppb) was recorded. Subjects with any upper or lower respiratory tract infection in the past 4 weeks would need to re-scheduled the testing to a later date.
Asthma control in the past 4 weeks was assessed by GINA classification,7 Asthma Control Test (ACT),20 and Asthma Control Questionnaire 5 (ACQ).21 For GINA classifications, subjects were classified as having controlled, partly controlled or uncontrolled asthma based on symptoms.7 For ACT, the scores range from 5 (poor control of asthma) to 25 (complete control of asthma), with higher scores reflecting better asthma control. A score between 20 and 25 represents controlled asthma, while a score of 19 or below represents not well-controlled asthma (partly controlled), and a score less than 16 indicates very poorly controlled asthma (uncontrolled asthma).22 For ACQ5, scores range from 0 to 6 (higher is worse). ACQ ≤0.75 indicated asthma was well-controlled; 0.75–1.5 as a “grey zone” (partly controlled asthma); and ≥1.5 has a high probability that asthma is poorly controlled (uncontrolled asthma).23 We defined changes in levels of asthma control as follows: Improved (improved in at least one level of asthma control, ie, from partly controlled or uncontrolled to controlled, or from uncontrolled to partly controlled), no change (stayed at same level of control), worsened (worsened in at least one level of asthma control, ie, from controlled to partly controlled or uncontrolled, or from controlled to partly controlled). The asthmatic attacks that required treatment of systemic corticosteroids or hospitalization at 12 months were documented (by asking the patient and checking with health records).
Sample size determination is shown in the Supplementary Document, and the minimal sample size required to assess the primary outcome of the study was 132 subjects. Data were analysed by the Statistical Package of the Social Science Statistical software (SPSS) for Windows, Version 28.0.1.0 (IBM SPSS Inc, IL, USA). The clinical characteristics of the subjects were expressed as mean (SD) or median [IQR]. Kruskal–Wallis test was used for between-group comparisons in changes of asthma control. Categorical data were analysed by Fisher’s exact or Chi-square tests. In addition, Receiver Operating Characteristic (ROC) analyses with the calculation of Area Under Curve (AUC) were used to assess the predictive value of FeNO for changes in asthma control. A p-value <0.05 was considered statistically significant.
Results
Altogether, 141 subjects were recruited for this study. Among them, 5 subjects failed the FeNO baseline assessment as they could not master the technique. Only those with successful baseline FeNO values (n = 136) were included in subsequent analyses. Demographic characteristics are shown in Table 1. The mean age of the subjects was 51.51±15.09 years, with 46 (33.8%) male subjects. The mean pre-bronchodilator FEV1% predicted and FEV1/FVC was 80.80 ±20.71 and 70.68±13.54%, respectively. Over 90% of the subjects were on ICS, and no subjects received biologics therapy. At 4, 8 and 12 months, 101, 92 and 94 subjects had successful FeNO measurements, respectively. At 12 months of follow-up, 13 (9.6%) and 3 (2.2%) subjects had asthma exacerbations requiring oral steroids and hospital admissions, respectively, during the study period.
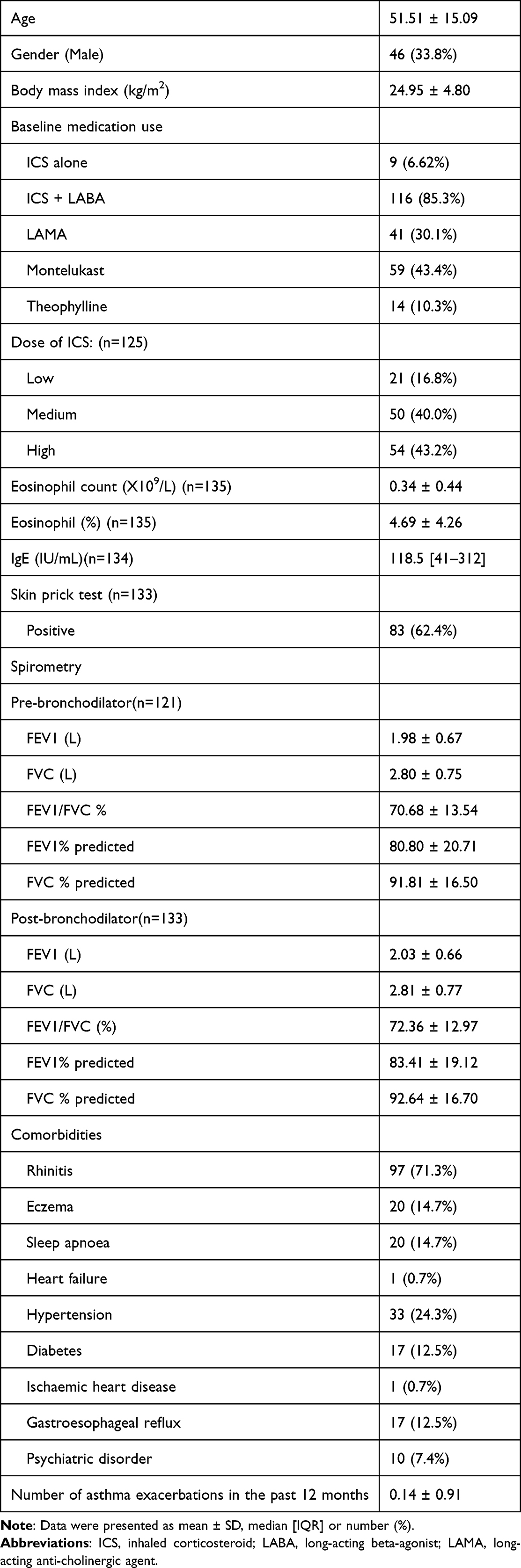 |
Table 1 Demographic Data of the Subjects (n = 136) |
The baseline FeNO levels are shown in Table 2. There was no statistically significant difference in FeNO values in the different levels of asthma control according to GINA, ACT and ACQ at baseline. Cutoff levels of <25, 25 to 50 and >50 ppb of the FeNO for low, intermediate and high FeNO level8 with respect to the different levels of asthma control by GINA, ACT and ACQ are shown in Supplementary Table 1. There were no statistically significant differences in the asthma control for GINA, ACT and ACQ among the suggested cutoff levels of FeNO by the American Thoracic Society.8 Asthma control according to GINA classification, ACT and ACQ at baseline did not have statistically significant differences based on blood eosinophil count at cutoff values of 0.3X109/L and 0.15X109/L (Supplementary Table 2). Baseline inhaled corticosteroid dose had no association with asthma control (Supplementary Table 3) and FeNO levels (Supplementary Table 4).
 |
Table 2 FeNO Levels and Asthma Control at Baseline Visit |
Serial changes of the changes in FeNO levels for changes in asthma control are shown in Table 3 and Figure 1. Those with improvement in asthma control according to the GINA classification had a statistically significant decrease in FeNO levels, while those with the same or worsened asthma control had not much change in FeNO levels, at 4, 8 and 12 months compared to baseline. For asthma control by ACT, subjects with improved asthma control at 4 months had a decrease in FeNO levels compared with baseline, but that was not statistically significant at 8 and 12 months. For asthma control by ACQ, subjects with improvement in asthma control at 4 and 8 months had a decrease in FeNO levels compared to those with the same or worsened asthma control, but the changes were not statistically significant at 12 months.
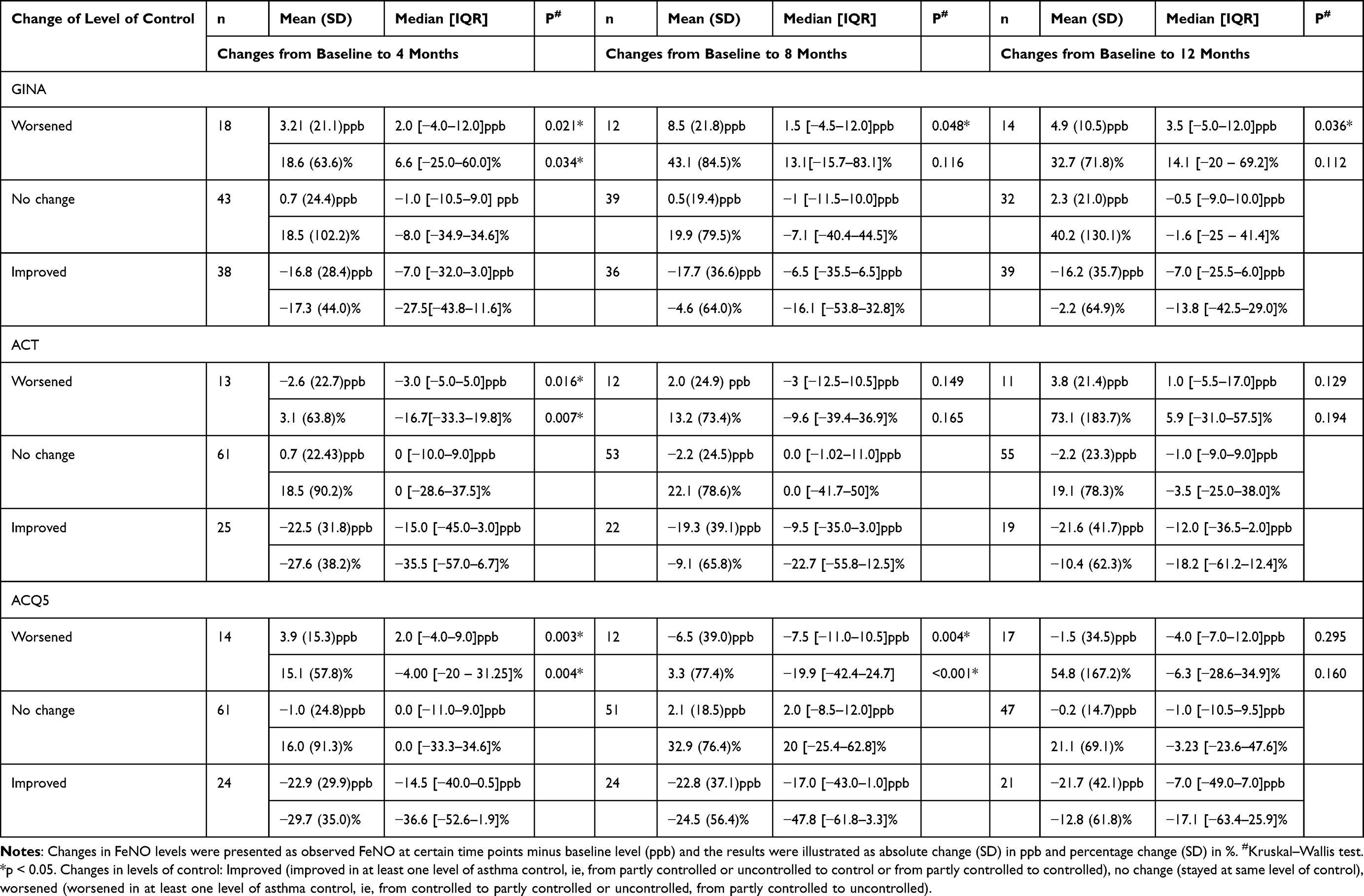 |
Table 3 Changes in Asthma Control and FeNO Levels Over Time |
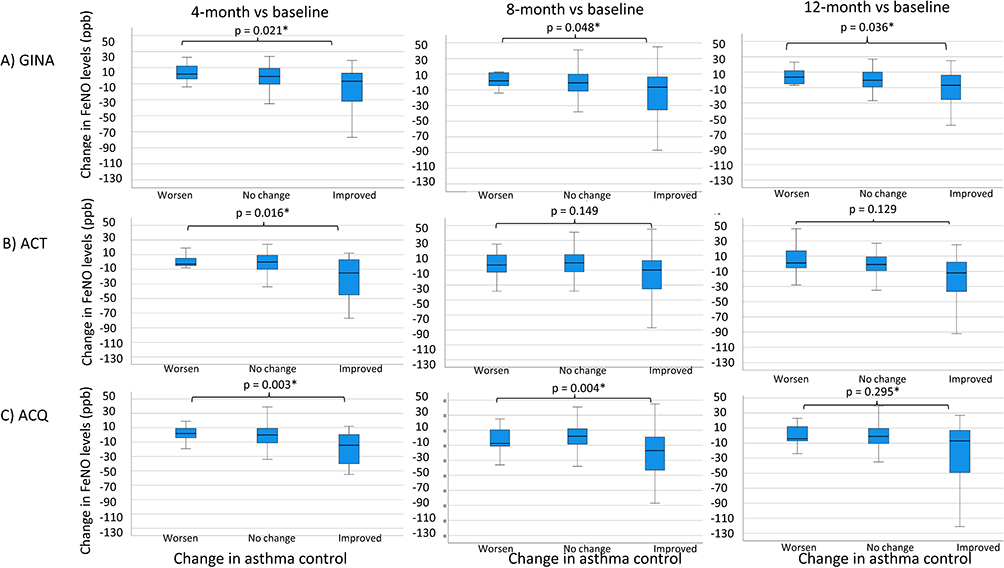 |
Figure 1 Boxplot of change in FeNO levels at 4, 8 and 12 months compared with baseline (all subjects). (A) Global Initiative of Asthma level of asthma control (GINA), (B) Asthma Control Test (ACT), (C) Asthma Control Questionnaire (ACQ). Changes in FeNO levels were presented as observed FeNO at certain time point minus baseline level (ppb). p value was calculated by Kruskal–Wallis test. * = p < 0.05. The solid line represents the median level, the box represents the IQR and the upper / lower whiskers are from the upper/lower quartile to the highest/lowest actual value within the 75th percentile/25th percentile ± 1.5 × IQR. Changes in levels of control: Improved (improved in at least one level of asthma control, ie, from partly controlled or uncontrolled to control, or from uncontrolled to partly controlled), no change (stayed at same level of control), worsened (worsened in at least one level of asthma control, ie from controlled to partly controlled or uncontrolled, from controlled to partly controlled). |
Subjects with eosinophils ≥150 or ≥300 cells/µL were separately analysed, and their results are shown in Supplementary Tables 5 and 6 and Supplementary Figures 1 and 2. A similar pattern was noted, but it was observed for subjects with blood eosinophils ≥300 cells/µL, worsening of asthma control was associated with an increase in FeNO level.
ROC analyses were performed using different cutoffs for changes in FeNO to predict improvement in asthma control. For GINA classification of asthma control, AUCs were highest for these cutoffs for changes in FeNO levels: ≤ −15ppb, ≤-25 ppb and ≤-10 ppb, respectively, for improvement in asthma control at baseline vs 4 months, 8 months and 12 months, while for ACT were ≤ −15 ppb, ≤-25 ppb and ≤-10 ppb respectively and that for ACQ5 were ≤-25 ppb at all time points (p all <0.05) (Supplementary Table 7). Their respective ROC curves are shown in Figure 2. As the ROC analyses for identifying cutoffs for changes in FeNO for worsening asthma control were mostly statistically non-significant, they were not reported.
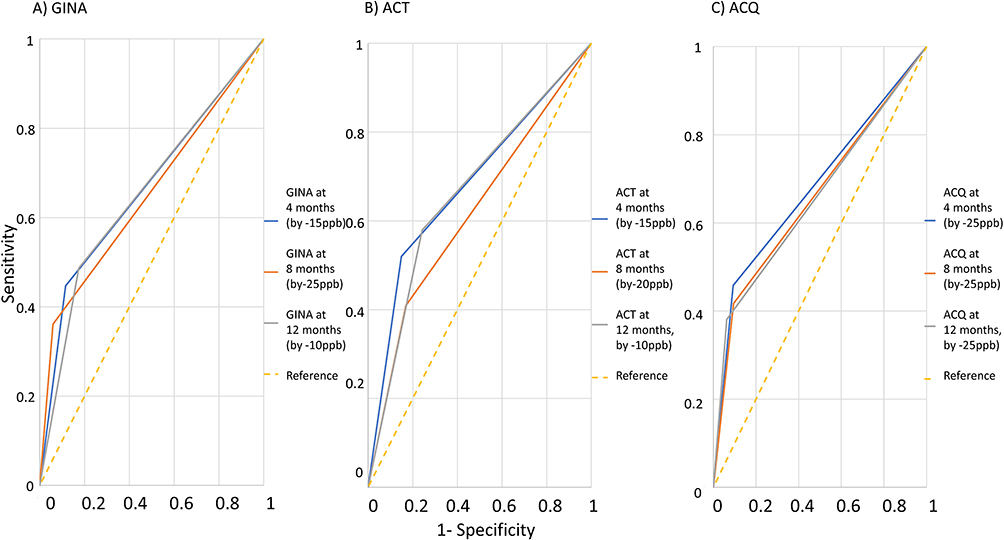 |
Figure 2 ROC curves for predicting the improvement for asthma control at different time points. (A) Global Initiative of Asthma level of asthma control (GINA), (B) Asthma Control Test (ACT), (C) Asthma Control Questionnaire (ACQ). |
Discussion
This is a real-life study to assess the FeNO values of Chinese asthma subjects at various levels of asthma control and the serial changes of FeNO with asthma control over time. At the baseline visit, FeNO levels did not differ among the different groups of asthma control by GINA, ACT or ACQ scores. It was observed that FeNO levels decreased with improving asthma control and stayed at similar levels with unchanged or worsening asthma control for all subjects. For those with baseline blood eosinophil levels ≥300 cells/µL, FeNO levels decreased with improving asthma control, stayed similar without change for asthma control and increased with worsening asthma control. ROC analysis with the highest AUC for changes in FeNO level for improving asthma control was between ≤ −10 to −25 ppb at various time points in the 12-month study.
There are no clear reference values for FeNO for different levels of asthma control. Some previous studies that used FeNO levels to adjust ICS treatment had various cutoffs. For example, in a study involving asthma patients on regular ICS, FeNO levels of ≥24ppb in women and ≥26 ppb in men were used as a guide for stepping up ICS treatment.24 In another study, if the FeNO was >26 ppb (this cutpoint was chosen as this corresponded to a sputum eosinophil count of >2%), ICS treatment was increased; if it was <16 ppb or <26 ppb on two consecutive occasions, treatment was decreased.25
The main idea was to use FeNO as a marker of inflammation, and thus above or below certain points, ICS was titrated to control the inflammation. If we take the median levels of FeNO and GINA classification of asthma control as a reference in this study, those who had controlled asthma had a median value of 27.5ppb and mean value of 36.79ppb, while partly-controlled and uncontrolled asthma had higher levels. Our patients with controlled asthma had FeNO levels above the cutoff used for titrating up ICS in other studies. We did not perform sputum eosinophil assessment for our subjects, which probably could help identify patients with eosinophil airway inflammation and give a better guide for the cutoffs for titration of asthma medications. Our previous studies on Chinese healthy subjects found that the FeNO levels were higher than in the Caucasian population.16 Results in this study might suggest FeNO levels in Chinese asthma subjects were higher than in the Caucasian populations. Further studies with a comparison of the levels of asthma control with control of the amount of anti-inflammatory therapy used would be needed.
Overall, the range of FeNO levels measured for various levels of asthma control using symptom scores in this study was very wide, making that interpretation using a single time point challenging. Some studies found one-off high FeNO level and/or blood eosinophil count had positive associations with asthma symptoms and exacerbations.26–28 Studies on serial FeNO studies with respect to asthma control had variable results. A study found that daily FeNO score at home did not correlate with symptom level.29 Some studies found that FeNO changed with improving or deteriorating asthma control. For example, in patients who received emergency therapy for asthma, repeated measurements of mixed expired NO levels during treatment with glucocorticoids showed a reduction in FeNO levels with an improvement in airway obstruction.30 On the other hand, patients with mild/moderate asthma with their ICS withdrawn and observed for loss of asthma control, increase in FeNO of 10 ppb, 15 ppb or >60% over baseline had positive predictive values that ranged from 80% to 90% for predicting the loss of control.31
There is not much information on the longitudinal study of FeNO in unselected patients. A prospective trial with post hoc data analysis of study of serial FeNO levels using ACQ score 0.75 as the cutoff for well-controlled asthma found that FeNO decreased by 40% and increased by 30% with asthma control optimisation or deterioration, respectively. The serial measurements ranged from 10 to 1129 days. The prediction of FeNO on change of asthma control was better for patients on low-dose ICS compared with those on higher doses.32
In the current study, we found that FeNO decreased with improving asthma control and stayed at similar levels for those with no change or worsening asthma control when all subjects were analysed together. It appeared that only in those with higher blood eosinophil counts, increased FeNO levels were observed with deteriorating asthma control. FeNO levels are affected by many factors,8 including age, height, smoking, and anti-inflammatory medications, and these have to be taken into account during the interpretation. Serial levels of FeNO appeared to reflect changes in levels of asthma control. FeNO is a marker of type 2 inflammation, and it is uncertain if serial FeNO levels are more helpful in detecting changes in asthma control in type 2 high compared to type 2 low subjects. More studies in well-phenotyped patients with a sufficient sample size can give more information on how to interpret the FeNO level changes with respect to asthma control.
We found that a decrease in FeNO level (at a range of between ≤ −10 to −25 ppb) had both a positive predictive value (PPV) and negative predictive value (NPV) of about 70% for improvement in asthma control in our cohort. A previous study found that a cutoff of FeNO level at −15% had similar PPV and NPV for predicting improvement in asthma control as in our study. We were unable to find suitable cutoff values of FeNO for predicting the worsening of asthma control in our study.32 We had a relatively smaller number of subjects with worsening asthma control than those with no change or improved asthma control. In addition, many subjects were on ICS, which would affect the FeNO levels. For asthma control, ACT and ACQ have data on the minimal important difference and were used in clinical trials for assessing the response to therapy.22,33 For FeNO, the clinically important change of FeNO in individual patients is not certain. The latest ATS Clinical Practice Guideline on FeNO suggested at least a 20% change to indicate a significant rise or fall in FENO over time or following an intervention.8
While this study assessed the real-life FeNO changes over time in a Chinese cohort, it was limited by being a single-centre study. In addition, this study was in a tertiary referral centre, and thus the results might not be applicable to asthma patients managed in the general practice. Furthermore, the study was limited by the relatively small sample size with no normal subjects as control. The sample size was based on assessing the single-time measurement of FeNO in Chinese asthma subjects to assess if there was a difference from Caucasian values. We had extended the analyses to assess serial changes in the FeNO levels. We did not assess the serial changes in FeNO level according to the ICS dose in this study as many subjects were on an anti-inflammatory reliever for their asthma control. Without electronic monitoring in a real-life study, the amount of the dose of ICS used could not be recorded accurately. Age and gender of an individual can also affect the FeNO level,16 and these factors were not assessed in this study.
Conclusion
The single-time point measurement of FeNO levels in Chinese patients with controlled asthma appeared higher than that of the cutoffs recommended by clinical trials to step up anti-inflammatory therapy for asthma. When managing asthma, a single measurement of FeNO was not associated with the level of asthma control. However, a serial measure of FeNO showed a decrease in levels with improvement in asthma control as measured by GINA, ACT or ACQ in real-life asthma patients. FeNO levels were observed to increase with worsening asthma control in those with blood eosinophils ≥300 cells/µL. Changes in FeNO level over time were associated with changes in clinical asthma control, particularly in those with high blood eosinophil count and is likely to be more useful than a single time point measurement in the management of asthma.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Funding
This study is supported by the Hong Kong Lung Foundation Grant.
Disclosure
All authors have no conflicts of interest to declare in relation to this manuscript.
References
1. Riise GC, Toren K, Olin A-C. Subjects in a population study with high levels of FENO have associated eosinophil airway inflammation. ISRN Allergy. 2011;2011:792613. doi:10.5402/2011/792613
2. Silkoff PE, Lent AM, Busacker AA, et al. Exhaled nitric oxide identifies the persistent eosinophilic phenotype in severe refractory asthma. J Allergy Clin Immunol. 2005;116:1249–1255.
3. Fleming L, Tsartsali L, Wilson N, Regamey N, Bush A. Longitudinal relationship between sputum eosinophils and exhaled nitric oxide in children with asthma. Am J Respir Crit Care Med. 2013;188:400–402.
4. Maspero J, Adir Y, Al-Ahmad M, et al. Type 2 inflammation in asthma and other airway diseases. ERJ Open Res. 2022;8:56.
5. Ko FW, Wang JKL, Hui DSC, et al. A multi-center study of the prevalence and characteristics of eosinophilic phenotype and high ige levels among Chinese patients with severe asthma. J Asthma Allergy. 2023;16:173–182.
6. Brusselle GG, Koppelman GH. Biologic therapies for severe asthma. N Engl J Med. 2022;386:157–171.
7. Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention; 2022. Available from: www.ginasthma.org.
8. Dweik RA, Boggs PB, Erzurum SC, et al. American Thoracic Society Committee on Interpretation of Exhaled Nitric Oxide Levels for Clinical A. An official ATS clinical practice guideline: interpretation of exhaled nitric oxide levels (FENO) for clinical applications. Am J Respir Crit Care Med. 2011;184:602–615.
9. British Thoracic Society. British guideline on the management of asthma; 2019. Available from: https://www.sign.ac.uk/media/1773/sign158-updated.pdf.
10. Petsky HL, Cates CJ, Kew KM, Chang AB. Tailoring asthma treatment on eosinophilic markers (exhaled nitric oxide or sputum eosinophils): a systematic review and meta-analysis. Thorax. 2018;73(12):1110–1119. doi:10.1136/thoraxjnl-2018-211540
11. Sato S, Saito J, Fukuhara A, et al. The clinical role of fractional exhaled nitric oxide in asthma control. Ann Allergy Asthma Immunol. 2017;119:541–547.
12. Khalili B, Boggs PB, Shi R, Bahna SL. Discrepancy between clinical asthma control assessment tools and fractional exhaled nitric oxide. Ann Allergy Asthma Immunol. 2008;101:124–129.
13. Visitsunthorn N, Prottasan P, Jirapongsananuruk O, Maneechotesuwan K. Is fractional exhaled nitric oxide (FeNO) associated with asthma control in children? Asian Pac J Allergy Immunol. 2014;32:218–225.
14. Abe Y, Suzuki M, Kimura H, et al. Annual fractional exhaled nitric oxide measurements and exacerbations in severe asthma. J Asthma Allergy. 2020;13:731–741.
15. Garcia E, Zhang Y, Rappaport EB, et al. Patterns and determinants of exhaled nitric oxide trajectories in schoolchildren over a 7-year period. Eur Respir J. 2020;56:2000011.
16. Ko FW, Leung TF, Wong GW, Chu JH, Sy HY, Hui DS. Determinants of, and reference equation for, exhaled nitric oxide in the Chinese population. Eur Respir J. 2013;42:767–775.
17. Miller MR, Hankinson J, Brusasco V, et al. Standardisation of spirometry. Eur Respir J. 2005;26:319–338.
18. Ip MS, Ko FW, Lau AC, et al. Updated spirometric reference values for adult Chinese in Hong Kong and implications on clinical utilization. Chest. 2006;129:384–392.
19. American Thoracic Society, European Respiratory Society. ATS/ERS recommendations for standardized procedures for the online and offline measurement of exhaled lower respiratory nitric oxide and nasal nitric oxide, 2005. Am J Respir Crit Care Med. 2005;171:912–930.
20. Nathan RA, Sorkness CA, Kosinski M, et al. Development of the asthma control test: a survey for assessing asthma control. J Allergy Clin Immunol. 2004;113:59–65.
21. Juniper EF, O’Byrne PM, Guyatt GH, Ferrie PJ, King DR. Development and validation of a questionnaire to measure asthma control. Eur Respir J. 1999;14:902–907.
22. Schatz M, Kosinski M, Yarlas AS, Hanlon J, Watson ME, Jhingran P. The minimally important difference of the Asthma Control Test. J Allergy Clin Immunol. 2009;124:719–23 e1.
23. Juniper EF, Bousquet J, Abetz L, Bateman ED, Committee G. Identifying ‘well-controlled’ and ‘not well-controlled’ asthma using the Asthma Control Questionnaire. Respir Med. 2006;100:616–621.
24. Syk J, Malinovschi A, Johansson G, et al. Anti-inflammatory treatment of atopic asthma guided by exhaled nitric oxide: a randomized, controlled trial. J Allergy Clin Immunol Pract. 2013;1:639–48 e1–8.
25. Shaw DE, Berry MA, Thomas M, et al. The use of exhaled nitric oxide to guide asthma management: a randomized controlled trial. Am J Respir Crit Care Med. 2007;176:231–237.
26. Malinovschi A, Fonseca JA, Jacinto T, Alving K, Janson C. Exhaled nitric oxide levels and blood eosinophil counts independently associate with wheeze and asthma events in National Health and Nutrition Examination Survey subjects. J Allergy Clin Immunol. 2013;132:821–7 e1–5.
27. Denlinger LC, Phillips BR, Ramratnam S, et al.; National Heart L, Blood Institute’s Severe Asthma Research Program I. Inflammatory and comorbid features of patients with severe asthma and frequent exacerbations. Am J Respir Crit Care Med. 2017;195:302–313.
28. Soma T, Iemura H, Naito E, et al. Implication of fraction of exhaled nitric oxide and blood eosinophil count in severe asthma. Allergol Int. 2018;67S:S3–S11.
29. Pijnenburg MW, Floor SE, Hop WC, De Jongste JC. Daily ambulatory exhaled nitric oxide measurements in asthma. Pediatr Allergy Immunol. 2006;17:189–193.
30. Massaro AF, Gaston B, Kita D, Fanta C, Stamler JS, Drazen JM. Expired nitric oxide levels during treatment of acute asthma. Am J Respir Crit Care Med. 1995;152:800–803.
31. Jones SL, Kittelson J, Cowan JO, et al. The predictive value of exhaled nitric oxide measurements in assessing changes in asthma control. Am J Respir Crit Care Med. 2001;164:738–743.
32. Michils A, Baldassarre S, Van Muylem A. Exhaled nitric oxide and asthma control: a longitudinal study in unselected patients. Eur Respir J. 2008;31:539–546.
33. Juniper EF, Svensson K, Mork AC, Stahl E. Measurement properties and interpretation of three shortened versions of the asthma control questionnaire. Respir Med. 2005;99:553–558.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.