Back to Journals » Cancer Management and Research » Volume 10
ypTNM category combined with AJCC tumor regression grade for screening patients with the worst prognosis after neoadjuvant chemoradiation therapy for locally advanced rectal cancer
Authors Wei JW, Huang R, Guo SP, Zhang XH, Xi SY, Wang QX, Chang H ![]() , Wang XH, Xiao WW, Zeng ZF
, Wang XH, Xiao WW, Zeng ZF ![]() , Gao YH
, Gao YH
Received 4 July 2018
Accepted for publication 18 September 2018
Published 31 October 2018 Volume 2018:10 Pages 5219—5225
DOI https://doi.org/10.2147/CMAR.S179151
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Antonella D'Anneo
Jiawang Wei,1–3,* Rong Huang,3,* Suping Guo,1,2,* Xuhui Zhang,1,2 Shaoyan Xi,1,4 Qiaoxuan Wang,1,2 Hui Chang,1,2 Xiaohao Wang,1,2 Weiwei Xiao,1,2 Zhifan Zeng,1,2 Yuanhong Gao1,2
1State Key Laboratory of Oncology in South China, Collaborative Innovation Center for Cancer Medicine, Guangzhou, Guangdong, People’s Republic of China; 2Department of Radiation Oncology, Sun Yat-sen University Cancer Center, Guangzhou, Guangdong, People’s Republic of China; 3Department of Oncology, Ganzhou People’s Hospital, Ganzhou, Jiangxi, People’s Republic of China; 4Department of Pathology, Sun Yat-sen University Cancer Center, Guangzhou, Guangdong, People’s Republic of China
*These authors contributed equally to this work
Background: The purpose of this study was to investigate the value of the postsurgical pathological T and N (ypTN) category combined with the American Joint Committee on Cancer-tumor regression grade (AJCC-TRG) in evaluating the prognosis of neoadjuvant chemoradiation therapy (NeoCRT) for locally advanced rectal cancer (LARC) to screen for a subgroup of patients with the worst prognosis.
Patients and methods: In total, 265 patients with LARC were enrolled in the trial. All patients received NeoCRT. Total mesorectal excision was performed 6–8 weeks after the completion of radiotherapy. The surgical specimens were re-evaluated based on the AJCC-TRG (seventh edition) and the AJCC-tumor-node-metastasis (TNM; seventh edition) systems. We followed up these patients and calculated their overall survival (OS), disease-free survival (DFS), local recurrence-free survival (RFS), and distant metastasis (DM)-free survival (MFS) rates through the Kaplan–Meier analysis. The logrank test was further applied to evaluate the predictive value of the ypTN stage combined with AJCC-TRG for several survival indexes.
Results: The median follow-up period was 65.1 months. The 5-year OS, DFS, RFS, and MFS rates were 79.4%, 68.8%, 94.4%, and 76.5%, respectively. There were significant differences in OS, DFS, and MFS rates among different ypT+AJCC-TRG and ypN+AJCC-TRG subgroups. The 5-year OS, DFS, and MFS rates for ypT3–4+TRG 1 and ypT3–4+TRG2–3 subgroups were 73.9% vs 65.3%, 61.2% vs 52.9%, and 65.0% vs 61.5%, respectively. The 5-year OS, DFS, and MFS rates for ypN1–2+TRG 0–1 and ypN1–2+TRG2–3 subgroups were 64.8% vs 54.1%, 44.9% vs 41.7%, and 61.4% vs 46.3%, respectively.
Conclusion: The ypTNM category combined with the AJCC-TRG can more accurately evaluate the prognosis of patients with LARC and identify the subgroup of patients with the worst prognosis and high risk of developing DM, thereby demonstrating clinical significance in guiding individualized postoperative adjuvant therapy and follow-up for LARC.
Keywords: ypTNM, NeoCRT, rectal cancer, locally advanced rectal cancer, LARC, AJCC
Introduction
The postsurgical pathological T and N (ypTN) category is an important factor influencing the prognosis of neoadjuvant chemoradiation therapy (NeoCRT) before surgery for locally advanced rectal cancer (LARC).1–3 However, the prognostic value of postsurgical pathological T category (ypT) has often been challenged. For example, patients are often thought to have ypT3 or ypT4 category disease when postoperative pathological examination shows a small number of deformed atypical cells in the outer membrane layer of the rectal wall or outside the serosa of the rectal wall, but in fact, these patients have good prognosis. In addition, the accuracy of ypN category depends on the number of lymph nodes dissected during surgery, which is further influenced by the age of patients, tumor grade and stage, location of lesions, and quality of surgery.4,5 If the number of dissected lymph nodes is not enough, the postsurgical pathological N category (ypN) is not accurate. Therefore, it is still not very reliable to evaluate the prognosis of LARC based on the ypTN category alone.
Several studies have shown that the tumor regression grade (TRG) had significant correlation with the prognosis of LARC6–10 and is gradually being used to assess the progression of rectal cancer. Thus far, mainly six types of TRG systems have been used, and the American Joint Committee on Cancer (AJCC)-TRG has been found to be better than any other system as it can be more accurate in predicting the occurrence of distant metastasis (DM) due to rectal cancer.11
The purpose of this study is to investigate the value of ypTNM category combined with the AJCC-TRG in evaluating the prognosis of NeoCRT for LARC to screen for the subgroup of patients with the worst prognosis and to provide the foundation for individualized postoperative adjuvant therapy and follow-up.
Patients and methods
Patients
Patients with pathologically diagnosed, nonmetastatic, and resectable LARC were enrolled in the trial between October 1, 2004, and December 30, 2012. All the patients received NeoCRT before surgery; clinical stage was stage II (T3–4N0M0) or stage III (T1–4N1–2M0) according to the seventh edition of the Union for International Cancer Control (UICC)/AJCC tumor-node-metastasis (TNM) classification,12 and the Eastern Cooperative Oncology Group (ECOG) performance status was ≤2. The baseline clinical characteristics of the patients are shown in Table 1.
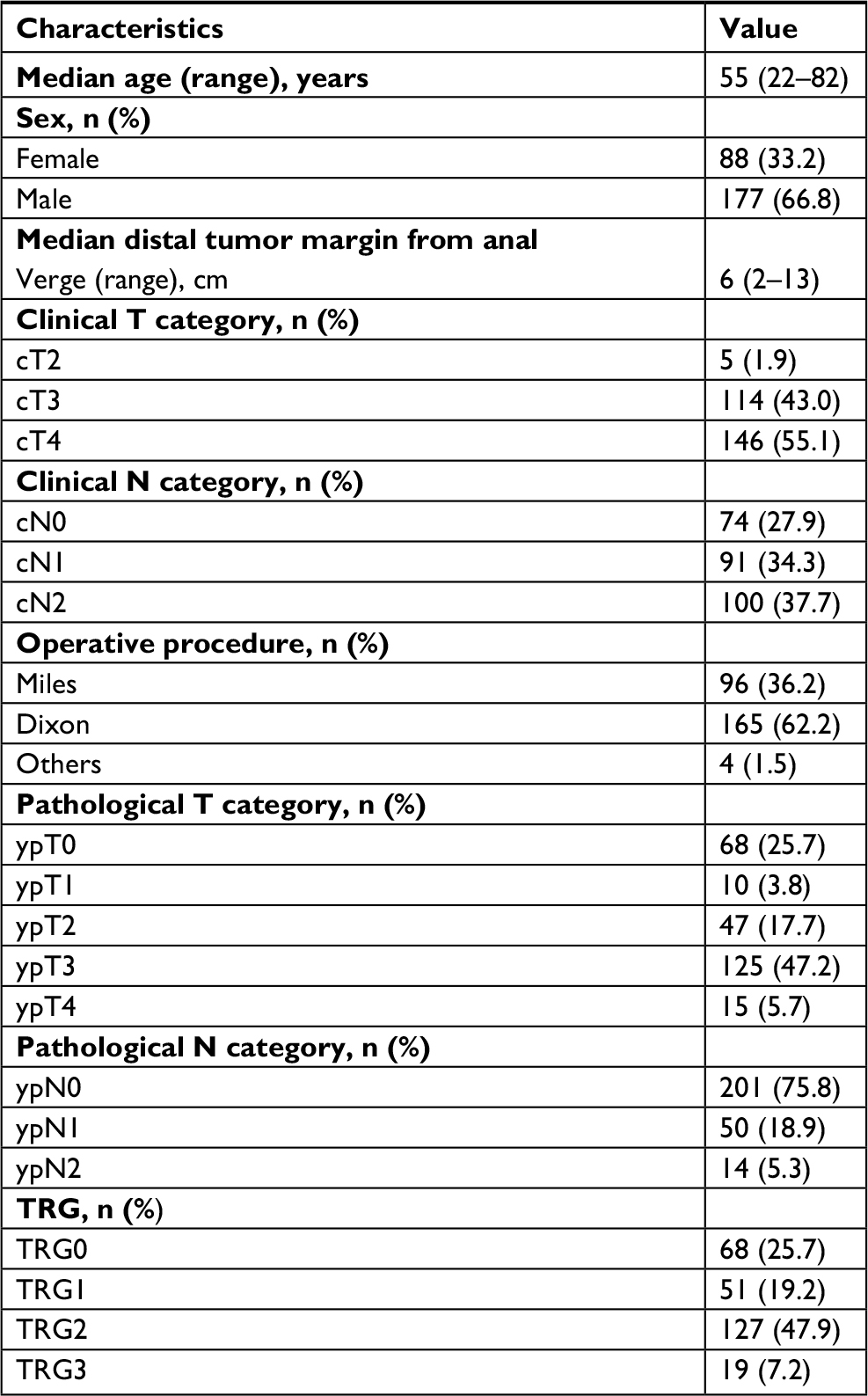 | Table 1 Baseline clinical characteristics and treatment results of the study population Note: Miles, abdominal perineal resection; Dixon, low anterior resection. Abbreviations: TRG, tumor regression grade; ypN, postsurgical pathological N category; ypT, postsurgical pathological T category. |
Ethics approval and consent to participate
Before treatment, all patients received detailed oral and written information on the treatment protocol and possible adverse effects and signed an informed consent. The trial was approved by the institutional review board of our hospital (Sun Yat-sen University Cancer Center) and conducted in accordance with the Declaration of Helsinki.
Grading standard and evaluation method of TRG
According to the tumor regression grading standard of the seventh edition of AJCC,11 TRG0 refers to no residual tumor cells, TRG1 refers to single cells or small groups of cells, TRG2 refers to residual cancer with desmoplastic response, while TRG3 refers to minimal evidence of tumor response. The TRG was independently evaluated by two experienced pathology specialists by reviewing the tissues sections. When the evaluation results were inconsistent, two experienced pathology specialists discussed and reviewed the tissues sections together and then gave the final evaluation.
Treatment
Radiotherapy
All patients were immobilized at a prone position using an AIO Bellyboard and Pelvic Solution System (AIO Solution; Orfit Industries, Wijnegem, Belgium). Volumetric-modulated arc therapy was the irradiation treatment modality used in this study. After a computed tomography (CT)-based simulation, target volumes were delineated according to the guidelines of the International Commission on Radiation Units and Measurements (ICRU) reports 50 and 62. Gross tumor volume (GTV) included the macroscopic tumor and enlarged lymph nodes as visualized on CT or magnetic resonance (MR) images. Clinical target volume (CTV) covered the GTV with a radial margin of 2 cm and included high-risk regions of lymphatic drainage. Conventional fractionation radiotherapy was conducted (2 Gy per fraction, 1 fraction per day, 5 days per week), in which the total doses of GTV and CTV were 50 and 46 Gy, respectively.
Neoadjuvant chemotherapy
During radiotherapy, all patients received neoadjuvant chemotherapy. In total, 242 cases received the oxaliplatin and capecitabine (XELOX) chemotherapy regimen repeated every 21 days, in which 100 mg/m2 oxaliplatin (OXA) was administered on day 1 and 1,000 mg/m2 capecitabine (CAP) was administered twice daily from day 1–14. The other 23 cases received the fluorouracil, leucovorin, oxaliplatin (FOLFOX6) chemotherapy regimen repeated every 14 days, in which 85 mg/m2 OXA, 400 mg/m2 calcium folinate (CF), and intravenous injection of 5-fluorouracil (400 mg/m2) were administered on day 1, with continuous intravenous pump infusion of 5-fluorouracil (2,400 mg/m2) for 46–48 hours.
Radical resection
All patients planned to receive radical rectal resection 6–8 weeks after NeoCRT. The surgery was performed according to the principles of total mesorectal excision (TME).
Adjuvant chemotherapy
Adjuvant chemotherapy with XELOX or FOLFOX6 was started 3–4 weeks after surgery, with a median of four cycles.
Follow-up and endpoints
The frequency of follow-up was once in every 3–4 months within 2 years after treatment and then once in every 6 months thereafter. Follow-up evaluations mainly involved a complete physical examination, digital rectal examination, thoracoabdominal CT scan, endoscopic ultrasonography, pelvic MR imaging scan, and tests of the levels of carcinoembryonic antigen (CEA), and carbohydrate antigen-199 (CA-199).
The primary endpoint was overall survival (OS) rate, which referred to the percentage of patients who were alive after a certain time period from diagnosis. Secondary endpoints were disease-free survival (DFS), local recurrence-free survival (RFS), and DM-free survival (MFS) rates. The DFS rate was defined as the percentage of living patients without local recurrence or DM after a certain time period from diagnosis. In addition, the RFS/MFS ratio was defined as the percentage of patients without local recurrence or DM after a certain time period.
Statistical analyses
OS, DFS, RFS, and MFS rates were determined using the Kaplan–Meier analysis. The logrank test was performed to evaluate whether ypT category, ypN category, AJCC-TRG, ypT+AJCC-TRG, and ypN+AJCC-TRG were candidate risk factors for OS, DFS, RFS, and MFS.
Statistical analyses were conducted using SPSS Statistics Version 19.0 software (IBM Corporation, Armonk, New York, USA). A two-sided P-value <0.05 was considered statistically significant.
Results
Survival
The deadline for follow-up was November 2017, with a follow-up rate of 94.1%. The median follow-up time was 65.1 months (range, 5.7–152.6 months). There were 67 cases of death in the whole group – 1 patient died of pulmonary infection, 1 patient died of diabetes complication, and the other 65 patients died of tumor recurrence or metastasis. The 5-year OS, DFS, RFS, and MFS rates were 79.4%, 68.8%, 94.4%, and 76.5%, respectively. The results are shown in Table 2.
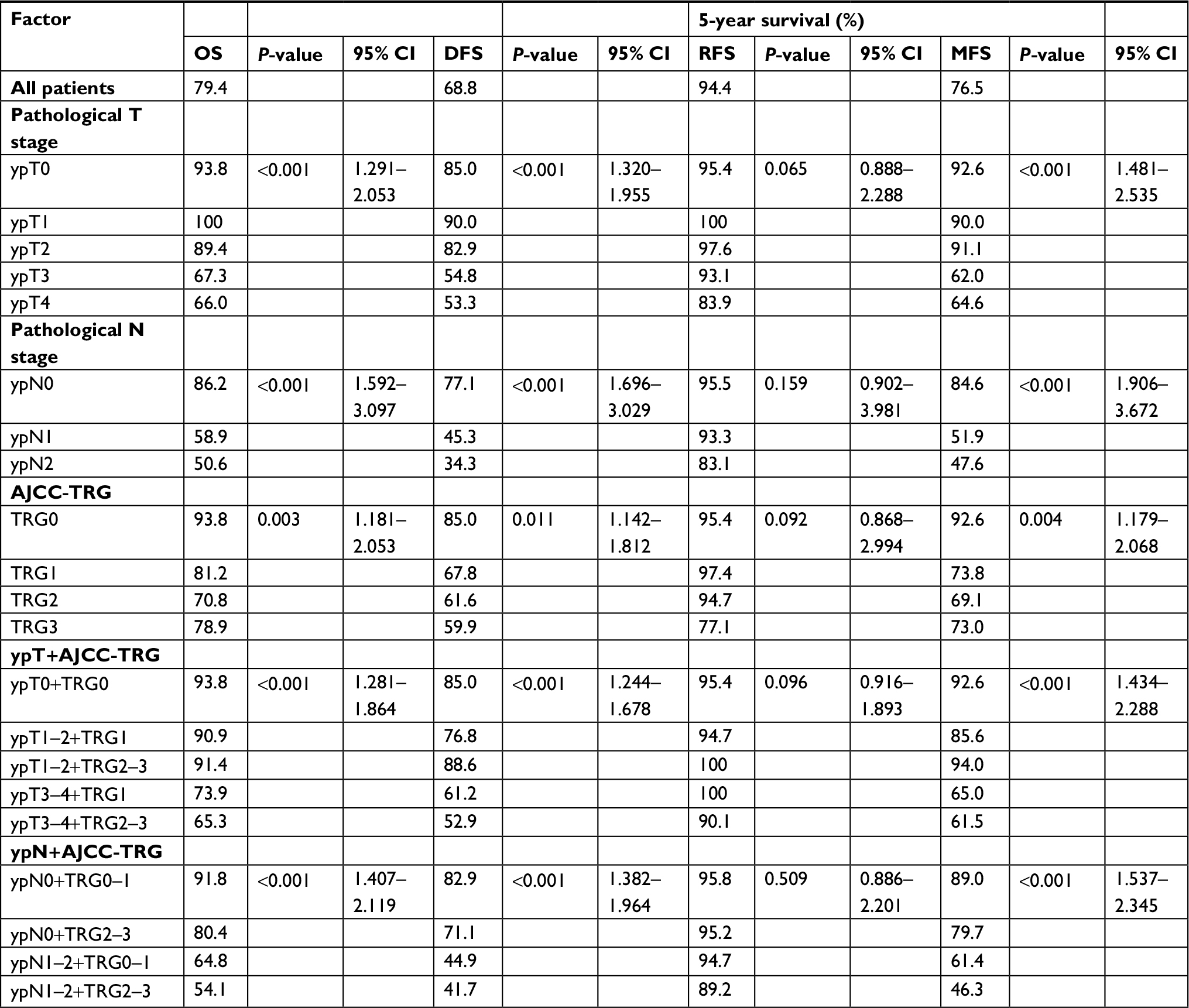 | Table 2 Univariate survival analysis of patients according to different factors Abbreviations: AJCC-TRG, American Joint Committee on Cancer-tumor regression grade; DFS, disease-free survival; MFS, distant-metastasis-free survival; OS, overall survival; RFS, local-recurrence-free survival; ypN, postsurgical pathological N category; ypT, postsurgical pathological T category. |
Associations between ypTN or TRG and prognosis
The 5-year survival rates of different ypT, ypN, and TRG groups are shown in Table 2. The comparisons of survival curves among different ypT subgroups are shown in Figure 1A and B. The comparisons of survival curves among different ypN subgroups are shown in Figure 2A and B.
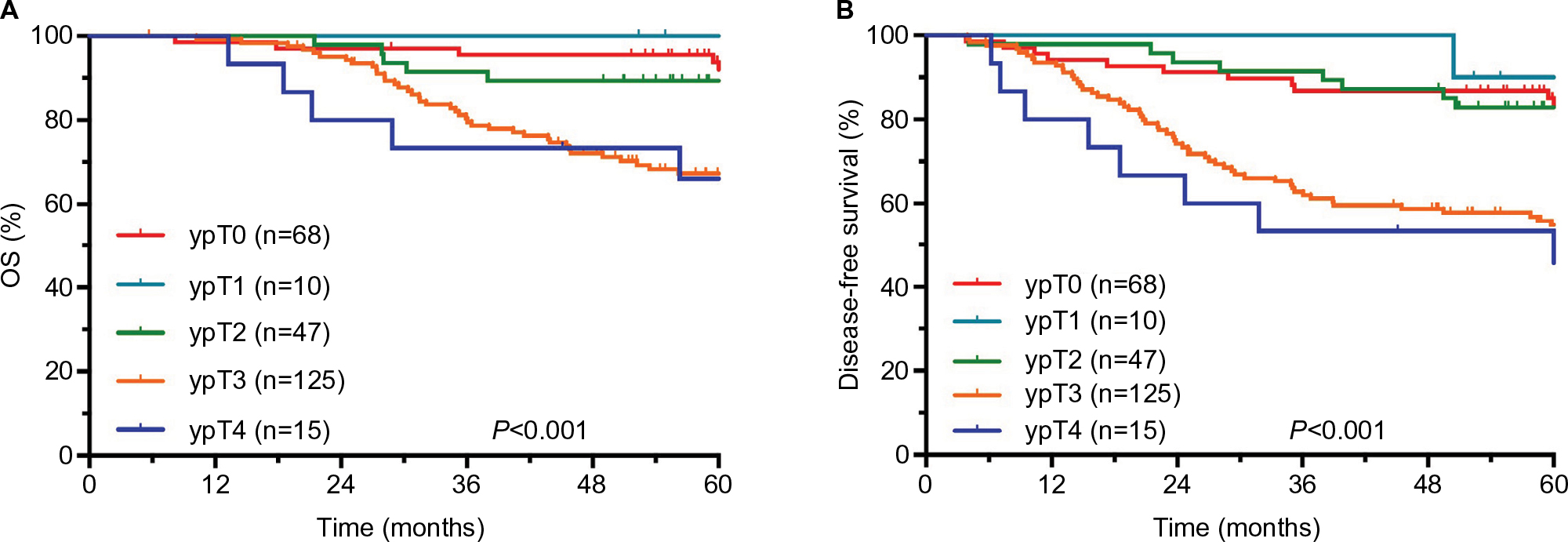 | Figure 1 Results of follow-up evaluations among different ypT subgroups. Notes: (A) OS. (B) DFS. Abbreviations: OS, overall survival; DFS, disease-free survival; ypT, postsurgical pathological T category. |
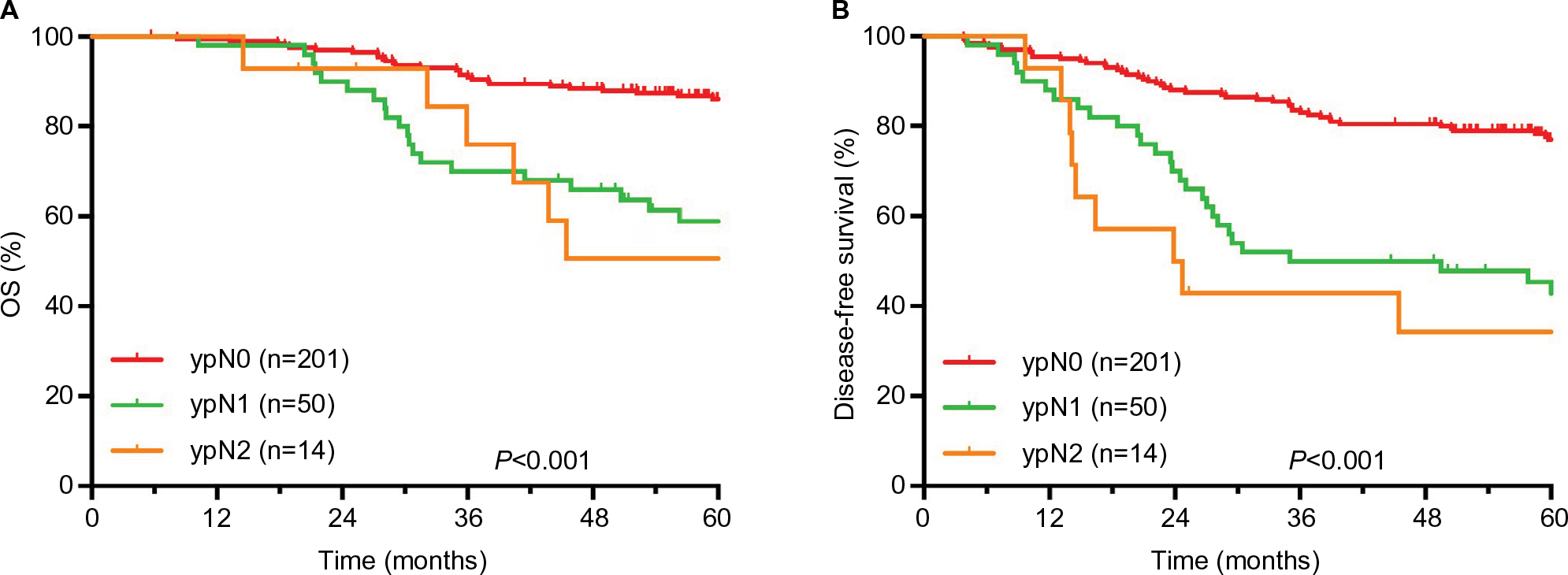 | Figure 2 Results of follow-up evaluations among different ypN subgroups. Notes: (A) OS. (B) DFS. Abbreviations: OS, overall survival; DFS, disease-free survival; ypN, postsurgical pathological N category. |
ypTN stage combined with AJCC-TRG to evaluate prognosis
The comparisons of OS and DFS among different ypT+AJCC-TRG subgroups are shown in Figure 3A and B. The comparisons of OS and DFS among different ypN+AJCC-TRG subgroups are shown in Figure 4A and B. There were significant differences in OS, DFS, and MFS among different ypT+AJCC-TRG and ypN+AJCC-TRG subgroups. Patients in the ypT3−4+TRG2–3 and ypN1−2+ TRG2–3 subgroups had the worst prognosis. The 5-year OS, DFS, and MFS rates for ypT3−4+TRG1 and ypT3−4+TRG2–3 subgroups were 73.9% vs 65.3% (P<0.001), 61.2% vs 52.9% (P<0.001), and 65.0% vs 61.5% (P<0.001), respectively. The 5-year OS, DFS, and MFS rates for ypN1−2+TRG0–1 and ypN1−2+TRG2–3 subgroups were 64.8% vs 54.1% (P<0.001), 44.9% vs 41.7% (P<0.001), and 61.4% vs 46.3% (P<0.001), respectively.
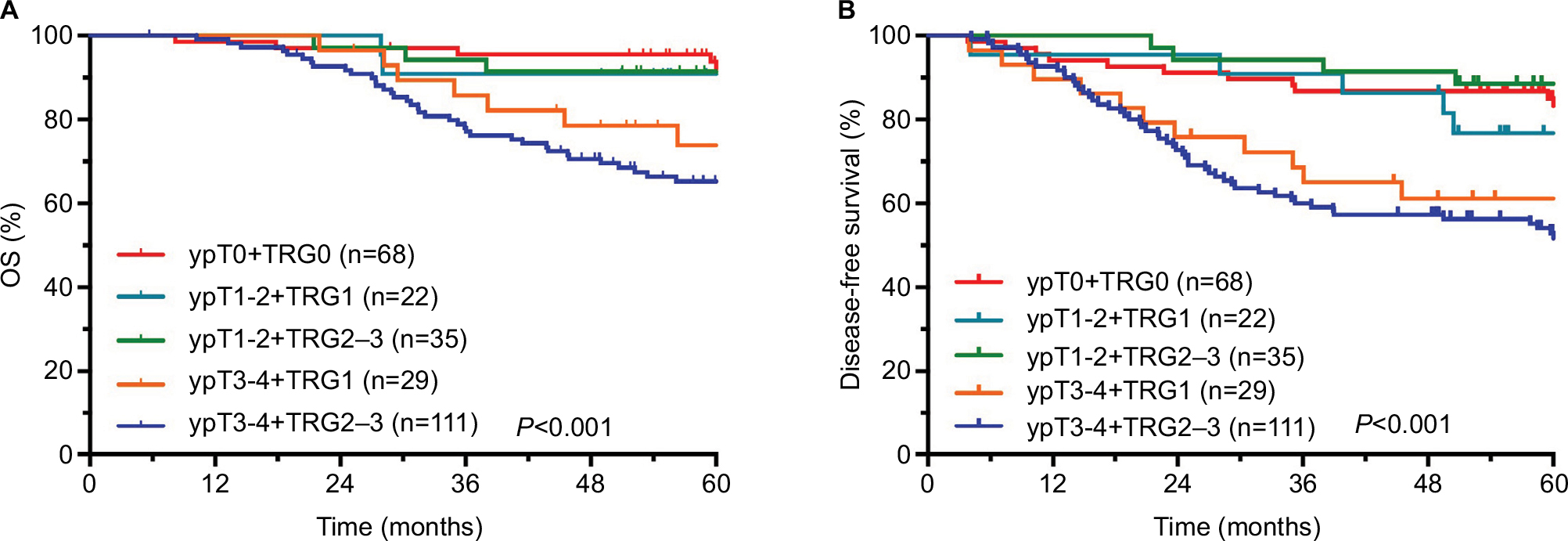 | Figure 3 Results of follow-up evaluations among different ypT+AJCC-TRG subgroups. Notes: (A) OS. (B) DFS. Abbreviations: AJCC-TRG, American Joint Committee on Cancer-tumor regression grade; OS, overall survival; DFS, disease-free survival; ypT, postsurgical pathological T category. |
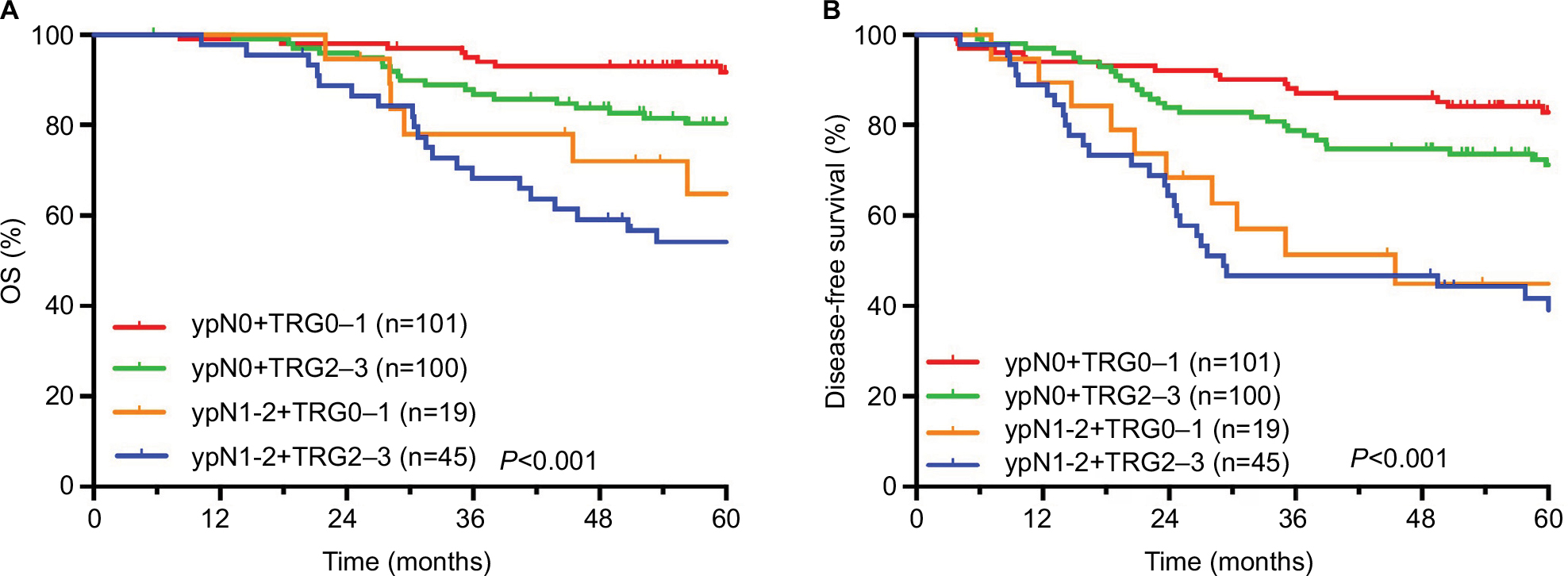 | Figure 4 Results of follow-up evaluations among different ypN+AJCC-TRG subgroups. Notes: (A) OS. (B) DFS. Abbreviations: AJCC-TRG, American Joint Committee on Cancer-tumor regression grade; OS, overall survival; DFS, disease-free survival; ypN, postsurgical pathological N category. |
Discussion
In our study, the prognosis of patients with ypT3–4 and ypN1–2 diseases was significantly worse than that of other patients, with 5-year OS rates of 67.1% and 57.5%, 5-year DFS rates of 54.6% and 42.8%, and 5-year MFS rates of 62.3% and 50.6%, respectively. However, subgroup analysis showed that the prognosis of patients with TRG2–3 disease was worst; the 5-year OS rates of the ypT3–4+TRG2–3 and ypN1–2+TRG2–3 subgroups were 65.3% and 54.1%, the 5-year DFS rates were 52.9% and 41.7%, and the 5-year MFS rates were 61.5% and 46.3%, respectively.
Several studies1–3 have reported that ypT and ypN categories are prognostic factors for OS, DFS, and MFS and that ypN category is an independent prognostic factor. The results of our study further confirmed these conclusions. However, the prognostic value of ypT category is often challenged. For example, patients are often thought to have ypT3 or ypT4 category disease when postoperative pathological examination shows a small number of deformed atypical cells in the outer membrane layer of the rectal wall or outside the serosa of the rectal wall, but in fact, these patients have good prognosis. Our results also suggest that some patients with ypT3-4 disease had a better prognosis than patients with ypT1-2 disease. The accuracy of ypN category depends on the number of lymph nodes dissected during surgery, which is further influenced by the age of patients, tumor grade and stage, location of lesions, and quality of surgery.4,5 If the number of dissected lymph nodes is not enough, the ypN category is not accurate. Therefore, it is not very reliable to evaluate the prognosis of LARC based on the ypTN category alone.
TRG is a type of grading metric used in the histological stratification of tumor response after chemoradiotherapy, and it was first used in the evaluation of the efficacy of concurrent chemoradiotherapy in esophageal, gastric, bladder, and head and neck cancers.13–17 Later, studies reported that TRG had a significant correlation with the prognosis of LARC,6–10 and it was gradually used to evaluate the progression of rectal cancer. There are mainly 6 types of TRG systems at present, which divide the TRG into 3–5 grades, but no unified standards have yet been established. Through the comparison of evaluation results of each system, the AJCC-TRG system was found to be superior to other systems, as it could more accurately predict the occurrence of DM due to rectal cancer.11 The results of this study also showed that the OS, DFS, RFS, and MFS rates were different in LARC patients with different AJCC-TRGs, and the TRG was a factor influencing OS, DFS, and MFS rates (P-values were 0.003, 0.011, and 0.004, respectively). Moreover, we noticed that the TRG was determined by the proportion of residual tumor cells,11,18 which is highly dependent on the technology and experience of pathologist and might be difficult to accurately determine in some cases. In addition, the TRG mainly focuses on the response of primary tumor to treatment, without considering lymph node metastasis. In this study, TRG2–3 subgroups included patients with ypN0 and ypN1–2 stage diseases, and subgroup analysis showed that the 5-year OS, DFS, and MFS rates in the ypN1–2+TRG2–3 subgroups were significantly worse than those in the ypN0+TRG2–3 subgroup (54.1% vs 80.4%, 41.7% vs 71.1%, and 46.3% vs 79.7%, respectively; the P-values were all <0.001). Therefore, it is not accurate to evaluate the prognosis of LARC with AJCC-TRG alone.
The results of this study showed that the main mode of failure for LARC treatment was DM, consistent with the results reported in other studies.19,20 The 5-year MFS rates of the ypT0+TRG0, ypT1–2+TRG1, ypT1–2+TRG2–3, ypT3–4+TRG1, and ypT3–4+TRG2–3 subgroups in this study were 92.6%, 85.6%, 94.0%, 65.0%, and 61.5%, respectively (P<0.001). In addition, the 5-year MFS rates of the ypN0+TRG0–1, ypN0+TRG2–3, ypN1–2+TRG0–1, and ypN1–2+TRG2–3 subgroups in this study were 89.0%, 79.7%, 61.4% and 46.3%, respectively (P<0.001). Obviously, the prognosis of patients in the ypT3–4+TRG2–3 and ypN1–2+TRG2–3 subgroups was significantly worse than that in other subgroups. Hence, minimizing the rates of DM in these subgroups may achieve better long-term results. Therefore, reinforcing postoperative adjuvant therapy is recommended for patients with ypT3–4 or ypN1–2 disease combined with AJCC-TRG2–3, and stronger postoperative adjuvant therapy may improve the long-term survival of these patients. At the same time, these patients also need close follow-up and observation.
Conclusion
The ypTNM category combined with the AJCC-TRG can more accurately evaluate the prognosis of patients with LARC and screen the subgroup of patients with the worst prognosis and high risk of developing DM, thereby demonstrating clinical significance in guiding individualized postoperative adjuvant therapy and follow-up for LARC.
Disclosure
The authors report no conflicts of interest in this work.
References
Quah HM, Chou JF, Gonen M, et al. Pathologic stage is most prognostic of disease-free survival in locally advanced rectal cancer patients after preoperative chemoradiation. Cancer. 2008;113(1):57–64. | ||
Park IJ, You YN, Agarwal A, et al. Neoadjuvant treatment response as an early response indicator for patients with rectal cancer. J Clin Oncol. 2012;30(15):1770–1776. | ||
Rödel C, Martus P, Papadoupolos T, et al. Prognostic significance of tumor regression after preoperative chemoradiotherapy for rectal cancer. J Clin Oncol. 2005;23(34):8688–8696. | ||
Sarli L, Bader G, Iusco D, et al. Number of lymph nodes examined and prognosis of TNM stage II colorectal cancer. Eur J Cancer. 2005;41(2):272–279. | ||
Luna-Pérez P, Rodríguez-Ramírez S, Alvarado I, Gutiérrez de La Barrera M, Labastida S. Prognostic significance of retrieved lymph nodes per specimen in resected rectal adenocarcinoma after preoperative chemoradiation therapy. Arch Med Res. 2003;34(4):281–286. | ||
Fokas E, Liersch T, Fietkau R, et al. Tumor regression grading after preoperative chemoradiotherapy for locally advanced rectal carcinoma revisited: updated results of the CAO/ARO/AIO-94 trial. J Clin Oncol. 2014;32(15):1554–1562. | ||
Vecchio FM, Valentini V, Minsky BD, et al. The relationship of pathologic tumor regression grade (TRG) and outcomes after preoperative therapy in rectal cancer. Int J Radiat Oncol Biol Phys. 2005;62(3):752–760. | ||
Capirci C, Valentini V, Cionini L, et al. Prognostic value of pathologic complete response after neoadjuvant therapy in locally advanced rectal cancer: long-term analysis of 566 ypCR patients. Int J Radiat Oncol Biol Phys. 2008;72(1):99–107. | ||
Dhadda AS, Dickinson P, Zaitoun AM, Gandhi N, Bessell EM. Prognostic importance of Mandard tumour regression grade following pre-operative chemo/radiotherapy for locally advanced rectal cancer. Eur J Cancer. 2011;47(8):1138–1145. | ||
Zhang LN, Xiao WW, Xi SY, et al. Pathological assessment of the ajcc tumor regression grading system after preoperative chemoradiotherapy for chinese locally advanced rectal cancer. Medicine. 2016;95(3):e2272. | ||
Trakarnsanga A, Gönen M, Shia J, et al. Comparison of tumor regression grade systems for locally advanced rectal cancer after multimodality treatment. J Natl Cancer Inst. 2014;106(10). | ||
Edge SB, Compton CC. The American Joint Committee on Cancer: the 7th edition of the AJCC cancer staging manual and the future of TNM. Ann Surg Oncol. 2010;17(6):1471–1474. | ||
Mandard AM, Dalibard F, Mandard JC, et al. Pathologic assessment of tumor regression after preoperative chemoradiotherapy of esophageal carcinoma. Clinicopathologic correlations. Cancer. 1994;73(11):2680–2686. | ||
Becker K, Mueller JD, Schulmacher C, et al. Histomorphology and grading of regression in gastric carcinoma treated with neoadjuvant chemotherapy. Cancer. 2003;98(7):1521–1530. | ||
Lowy AM, Mansfield PF, Leach SD, Pazdur R, Dumas P, Ajani JA. Response to neoadjuvant chemotherapy best predicts survival after curative resection of gastric cancer. Ann Surg. 1999;229(3):303–308. | ||
Rödel C, Grabenbauer GG, Kühn R, et al. Combined-modality treatment and selective organ preservation in invasive bladder cancer: long-term results. J Clin Oncol. 2002;20(14):3061–3071. | ||
Braun OM, Neumeister B, Popp W, et al. Histologic tumor regression grades in squamous cell carcinoma of the head and neck after preoperative radiochemotherapy. Cancer. 1989;63(6):1097–1100. | ||
Shia J, Guillem JG, Moore HG, et al. Patterns of morphologic alteration in residual rectal carcinoma following preoperative chemoradiation and their association with long-term outcome. Am J Surg Pathol. 2004;28(2):215–223. | ||
Sineshaw HM, Jemal A, Thomas CR, Mitin T. Changes in treatment patterns for patients with locally advanced rectal cancer in the United States over the past decade: An analysis from the National Cancer Data Base. Cancer. 2016;122(13):1996–2003. | ||
Sauer R, Liersch T, Merkel S, et al. Preoperative versus postoperative chemoradiotherapy for locally advanced rectal cancer: results of the German CAO/ARO/AIO-94 randomized phase III trial after a median follow-up of 11 years. J Clin Oncol. 2012;30(16):1926–1933. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.