Back to Journals » Patient Preference and Adherence » Volume 17
Young XLH Patients-Reported Experience with a Supportive Care Program
Authors Rothenbuhler A, Gueorguieva I, Lichtenberger-Geslin L, Audrain C, Soskin S, Bensignor C, Rossignol S ![]() , Bertholet-Thomas A, Naudeau L, Bacchetta J, Linglart A
, Bertholet-Thomas A, Naudeau L, Bacchetta J, Linglart A
Received 23 September 2022
Accepted for publication 3 May 2023
Published 9 June 2023 Volume 2023:17 Pages 1393—1405
DOI https://doi.org/10.2147/PPA.S391025
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Anya Rothenbuhler,1 Iva Gueorguieva,2 Lydia Lichtenberger-Geslin,3 Christelle Audrain,1 Sylvie Soskin,4 Candace Bensignor,5 Sylvie Rossignol,4 Aurélia Bertholet-Thomas,6 Lorelei Naudeau,7 Justine Bacchetta,6 Agnès Linglart1,8
1AP-HP, INSERM, Endocrinology and Diabetes for Children, Physiologie et Physiopathologie Endocriniennes, Reference Center for Rare Disorders of Calcium and Phosphate Metabolism, Filière OSCAR, and Platform of Expertise for Rare Disorders, ERN for Rare Endocrine Disorders and ERN BOND, Bicêtre Paris Saclay Hospital, Le Kremlin-Bicêtre, France; 2Pediatric Endocrine Unit Children’s Hospital Jeanne de Flandre, Lille University Hospital, Lille, France; 3Pediatric Department, Abbeville Hospital, Abbeville, France; 4Pediatric Department, Strasbourg University Hospital, Strasbourg, France; 5Departement of Endocrino-Pediatry, Dijon University Hospital, Dijon, France; 6Pediatric Nephrology, Rheumatology, and Dermatology Unit, Reference Center for Rare Diseases of Calcium and Phosphate Metabolism, Reference Center for Rare Renal Diseases, Filières Maladies Rares OSCAR ORKiD and ERK-Net, INSERM 1033, Hôpital Femme Mère Enfant, Faculté de Médecine Lyon Est, Bron, France; 7Patientys-Webhelp Medica, Boulogne-Billancourt, France; 8Paris Saclay University, Bicêtre Paris Saclay Hospital, Le Kremlin-Bicêtre, France
Correspondence: Lorelei Naudeau, Email [email protected]
Purpose: X-linked hypophosphatemia (XLH) is a rare, chronic, genetic condition characterized by renal phosphate wasting and abnormal bone and teeth mineralization. It represents a challenging and multifaceted disease that causes wide-ranging impacts on patients’ lives. In this context, a scientific committee has designed a support initiative for patients treated for XLH: the aXess program. We sought to determine if a patient support program (PSP) could help XLH patients cope with their condition.
Methods: During the 12 months of participation in the aXess program, XLH patients were contacted by phone by a nurse to coordinate their treatment, ensure treatment adherence, and provide motivational interviews. A Pediatric QOL inventory was conducted on all participants at enrollment (D0), at month 6, and month 12.
Results: Altogether, a total of 59 patients were enrolled in the program. Most patients reported an improvement in QOL in all examined dimensions by month 12 (physical, emotional, social, and school, 85.4 ± 0.2 at month 12 versus 75.6 ± 0.3 at enrollment, p< 0.05). Patients were very satisfied with the program, with a mean overall satisfaction score of 9.8 ± 0.6 (on a scale from 0 to 10) at month 6 and 9.2 ± 1.5 at month 12.
Conclusion: Our findings indicate that this program might improve the QOL for patients with chronic conditions such as XLH through patient education, therapy adherence, motivational interviews, and frequent follow-up. It links the home environment and overall illness management, bringing patients, families, and caregivers together.
Keywords: XLH, patient support program, aXess support program, nurses, hypophosphatemia, quality of life, children
Introduction
X-linked hypophosphatemia (XLH) is a rare, genetic, chronic disorder caused by inactivating mutations in the PHEX gene, resulting in elevated levels of circulating FGF23. Increased FGF23 levels lead to hypophosphatemia and suppressed production of active vitamin D, leading to defective bone and tooth mineralization.1–3
The disorder manifests in childhood mainly by hypophosphatemic rickets and dental issues. Its symptomatology is characterized by recurrent dental abscesses, bowed legs, other skeletal deformities (such as craniosynostosis), and short stature, resulting in reduced mobility and discomfort.4–6
Rickets and osteomalacia significantly burden children’s daily lives, including increased pain and reduced physical activity, which may affect their emotional state and self-esteem and increase the proportion of patients displaying overweight and obesity.7,8 In childhood and adolescents, patients with XLH are treated either by conventional therapy (multiple daily oral phosphate supplementation and active vitamin D analogs) or a recently developed targeted therapy (anti-FGF23 antibody burosumab, administrated by a nurse subcutaneously every 14 days).
XLH patients require multidisciplinary care; thus, their management is complex, and a coordination program is of considerable interest.
In 2016, a randomized clinical study of 766 patients treated for cancer found that a simple intervention, such as a web-based tool that allows patients to monitor their symptoms in real-time, triggering warnings to physicians, can have significant benefits, including increased survival.9
In addition, a series of patient support programs have been developed, and their beneficial effect on patients’ adherence to treatment or quality of life has been evaluated.10–13
Patientys’ aXess program is a patient support program for patients with XLH and their families.
The aXess program supports patients and families during periods of stress and uncertainty. Preserving patient adherence to prescription schedules is critical to any effective treatment regimen. The service was provided by trained and certified nurses. Through training, nurses achieve a thorough understanding of the XLH pathophysiology. This critical program component serves as a trusted intermediary between patients and caregivers. In addition, trained nurses work with patients to ensure they adhere to their prescription therapy by coordinating injection schedules.
The overarching purpose of the aXess program is to help patients better manage their disease and complex prescription regimens, increase treatment adherence, and reduce anxiety to enhance their overall quality of life.
The program intends to ascertain patients’ understanding of the disease and treatment (eg, period of dosage adaptation), encourage their autonomy, accompany them in their daily life (eg, follow-up of biological tests), and embolden their compliance to treatment.
The aim of our study was to evaluate how a patient support program may help patients cope with their disease, to determine if it could be associated with patient’s engagement and empowerment of their condition, and if it could help patients to adhere to their treatment regimen, all of which would contribute to an overall improvement in their daily lives and their overall quality of life.
Materials and Methods
Study Design
Twelve-Month Patient Support Program
The aXess program is based on a 12-month phone follow-up of patients.
The program is coordinated by three nurses specifically trained to care for XLH patients. These nurses oversee conducting phone calls, completing surveys, performing motivational interviews, and coordinating all health care providers (pharmacists, physicians, home care nurses, and medical analysis laboratories). Importantly, coordinating nurses oversee educating home care nurses about the disease and treatment of XLH patients.
Outbound calls from a coordinating nurse were provided at enrollment and thereafter at regular intervals to evaluate patients’ compliance, tolerance to the treatment and to collect their lifestyle habits through an interview. The call schedule and frequency were tailored to meet the patient’s needs (patient initiating targeted therapy or already on targeted treatment). A more sustained call frequency, involving a call every two weeks following the first dose, was required for patients starting new treatment. Patients are asked to complete questionnaires on their daily activities and physical and emotional status.
Patients also have access to a free helpline to reach coordinating nurses. At the patient’s request, nurses coordinate with the various actors involved in their care: pharmacists, medical analysis laboratories, and physicians.
The program offers a treatment delivery service from the pharmacy to the patient’s home. The program’s timeline is outlined below:
Consultation with the Prescribing Physician
The physician proposes the aXess program to the patient and completes the consent form with the patient. Prescriptions for the therapy, biological tests, and home treatment administrations are provided.
Registration Validation by the Coordinating Nurse
The nurse of the aXess program records the patient’s follow-up data (recent medical appointments, previous treatment for hypophosphatemia, vitamin D supplements), the baseline quality of life questionnaire, collects contact information for the laboratory analysis, the pharmacy, and contacts the home care nurse to initiate the patient’s care.
Follow-Up by the Coordinating Nurse
The nurse of the aXess program accompanies patients in their treatment titration and/or follow-up to ensure the continuation of the treatment (reminder calls) and the coordination between the various care providers. In addition, treatment delivery can be organized if needed.
Patient satisfaction surveys are conducted over the phone.
Calls
- Registration validation (Day+1 after receiving consent).
- Treatment administration reminder call (2 days before the 1st administration of treatment).
- Following the 1st administration of treatment, a follow-up call is made (Day+2 after administration).
- Follow-up call at month 6 and month 12 to review and coordinate their treatment, ensure treatment adherence, provide motivational interviews and assess the patient’s satisfaction and quality of life.
Patients
Between July 2019 and April 2021, XLH patients were invited by their treating physicians to participate in the aXess patient support program. Eligible patients provided written informed consent to participate.
No patients under conventional therapy were enrolled in the program. All children were either being treated or initiating treatment with burosumab (targeted therapy).
Evaluations
At enrolment (D0), month 6 (M6), and month 12 (M12), all 59 patients underwent a 21–23-item Pediatric quality of life inventory (PedsQL–2)14 evaluation. These intervals were selected so that the program’s potential benefits could be assessed both midway through and at its completion.
The PedsQL Measurement Model was created as a modular approach to measuring pediatric health-related quality of life (HRQOL) in children and adolescents. It encompasses four dimensions: physical, emotional, social, and school functioning.
Specifically, the questionnaire used is the PedsQL 4.0 – Pediatric Quality of Life Inventory Version 4.0 Generic Core Scales par J.W. Varni (2001). There are two types of questionnaires:
- PedsQL Child-Self Report (ages 5–7, 8–12, 13–18) completed by the child/adolescent;
- PedsQL Parent-Proxy Report (2–4 years, 5–7 years, 8–12 years, 13–18 years) completed by the parent/guardian.
The scores are then transformed linearly to a scale between 0 and 100, summed and divided by the number of items completed, with high scores associated with a higher level of performance. The caregivers completed the questionnaires for patients who were too young to fill them out themselves. All questionnaires were complete (all questions answered).
Statistics
The height and BMI z-scores (height-for-age Z and BMI for age Z) were calculated using a SAS macro and reference database (by age and gender) provided by the CDC (Centers for Disease Control and Prevention) on the CDC website (https://www.cdc.gov/nccdphp/dnpao/growthcharts/resources/sas.htm), including the most recent update on 15/12/2022.
There were N=143 assessments (D0, M6, and M12) in all 59 patients for the calculation of the PedSQL score. Scores and sub-scores were described using frequency, mean and standard deviation (SD).
The change from baseline scores (from D0 to M6; from D0 to M12) was tested using a paired t-test and presented using the mean of difference with a 95% confidence interval of the difference and p-value.
The effect of treatment initiation timing (Yes vs No), XLH type (familial vs de novo) was tested using a linear mixed model with a period (as a continuous parameter), tested effect, and period x tested effect interaction as fixed effects; the patient ID was included as a random effect. Least Square (LS) means, and 95% Confidence Intervals (Cis) were provided for each level of the tested effect. The difference between the LS means of the tested effect was presented with its 95% confidence interval and p-value.
A Kenward-Roger Degree of Freedom estimation method was used.
All the statistical analysis was performed using SAS 9.4. A 5% significance threshold was used for all statistical analyses.
Results
Participants’ Characteristics and Enrollment
A total of 59 patients agreed to participate in the aXess patient support program.
The mean ± SD age of participants was 9.8 ± 3.8 years, and two-thirds were female.
All patients were diagnosed with XLH. 22% of participants had de novo XLH, 61% had familial XLH, and 17%, diagnosed with XLH, had no information provided concerning inheritance. The inclusion in the aXess program occurred on average 8.8 years after the diagnosis of XLH (Table 1). Heights z-scores are on average lower than the norm (negative average of −0.90), and the outcomes are comparable whether therapy is initiated or not. The BMI z-scores are generally higher than the norm (a positive average of 0.68), especially in patients starting therapy (0.95) vs the others (0.57). This last point is related to the patient’s age: most patients starting treatment were pre-pubertal (75%). These indicators are consistent with the characteristics of XLH patients. The variation in z-scores was greater for height (1.07) than for BMI (0.77).
 |
Table 1 Baseline Demographic and Disease Characteristics of XLH Patients Monitored in the aXess Program |
At enrollment, 16 patients were initiating targeted therapy, and 43 patients were already being treated with targeted therapy (no patients on conventional therapy were included). Ten patients (62.5%) who started treatment completed 6 months of follow-up, and 6 (37.5%) completed 12 months of follow-up. Thirty-nine (91%) and twenty-nine (67%) of the patients who were already receiving targeted treatment at the time of enrollment completed 6 and 12 months of follow-up, respectively (Figure 1).
 |
Figure 1 Flow chart. The outline of the selection and flow of XLH patients. Abbreviation: XLH, X-linked hypophosphatemia. |
Almost two-thirds of patients (2.7 years-10 years, 61%) were prepubertal at enrollment, and 85% of participants attended school on a regular basis.
Real-Life Follow-Up of Patients in the Program
A total of 154 treatment administrations were monitored for 59 patients. During the program, a total of 59 deliveries were completed.
A total of 45 training courses were delivered throughout the year to educate home care nurses about the disease and treatment of XLH patients. A total of 241 follow-up nurse calls were scheduled. Patients starting therapy received an average of 6.5 calls, compared to 3.2 calls per patient already receiving treatment (Table 2).
 |
Table 2 Number of aXess Nurse Calls to XLH Patients (Subgroups of Patients Initiating Treatment and Patients Already Receiving Treatment), to Pharmacy, to Medical Analysis Laboratory, to Home Care Nurses and to Physician |
During the duration of the program, 384 solicited-patient calls and a total of 1252 inbound and outbound calls were completed. Out of these 1252 inbound and outbound calls, there were 625 calls to the patients, 261 to pharmacists, 212 to home care nurses, 95 to the medical analysis laboratory, and 59 to the prescribing physician.
As expected, most patient-requested calls were from patients who were initiating their treatment at the time of enrollment (Table 2).
Impact of the Patient Support Program on the Quality of Life of Young XLH Patients
PedsQL Results
Tables 3–5 summarize the means and SDS of the PedsQL Generic Core Scales for all children and subgroups of children initiating treatment and children already receiving treatment at the time of enrollment. The overall data (all patients) is shown in Figure 2. Patients already receiving treatment reported higher QOL scores than patients just starting treatment; these differences did not achieve statistical significance. Notably, after 6 months, patients who initiated therapy demonstrated significant improvement in all four components of QOL. This significance did not persist after 12 months except for the school functioning domain. Improvements in all domains were significant in patients already receiving therapy at months 6 and 12.
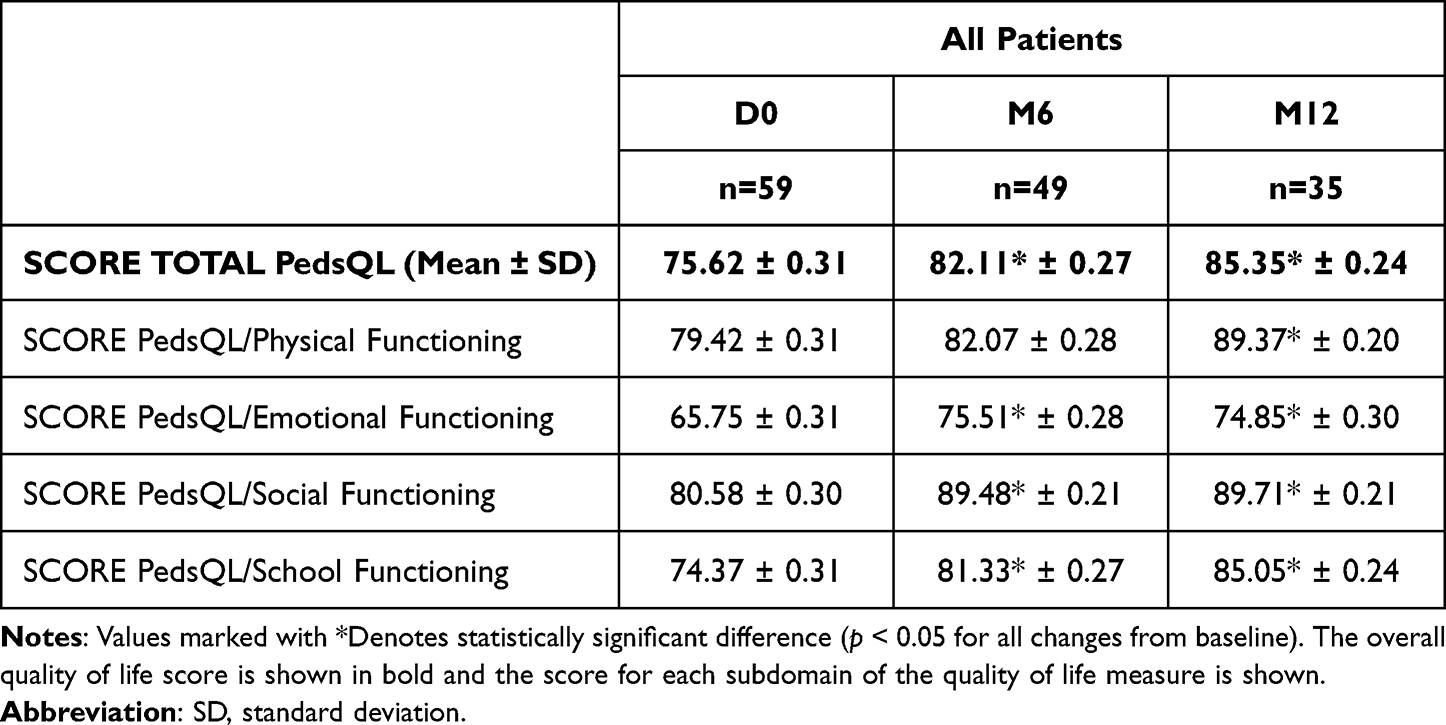 |
Table 3 Change from Baseline (D0) to 6 and 12 Months in the Mean PedSQL Generic Core Scales (Global and Sub-Domains Physical, Emotional, Social, School Functioning) for All Patients |
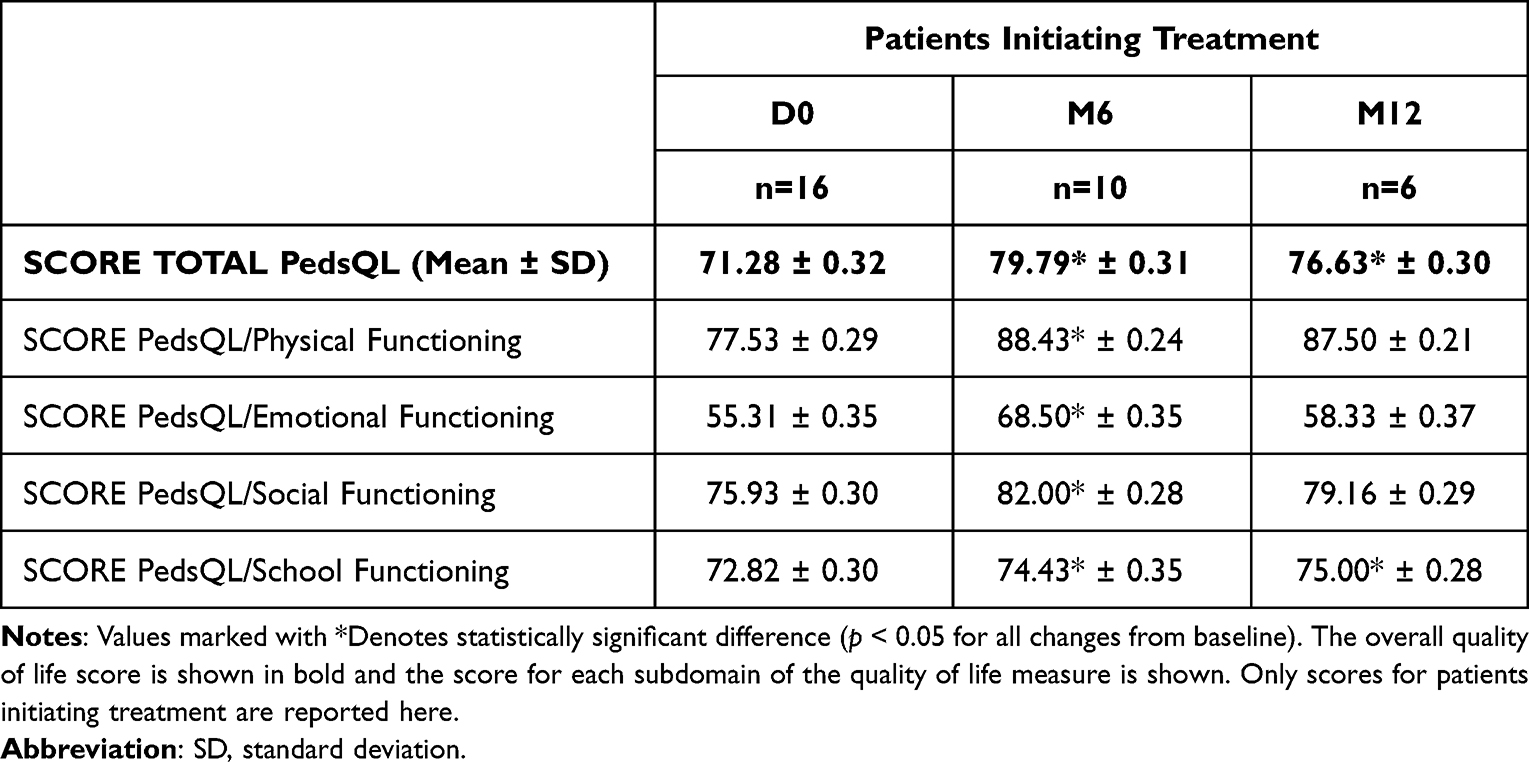 |
Table 4 Change from Baseline to 6 and 12 Months in the Mean PedSQL Generic Core Scales (Global and Sub-Domains Physical, Emotional, Social, School Functioning), Subgroup of Patients Initiating Treatment |
 |
Table 5 Change from Baseline to 6 and 12 Months in the Mean PedSQL Generic Core Scales (Global and Sub-Domains Physical, Emotional, Social, School Functioning), Subgroup of Patients Already Receiving Treatment |
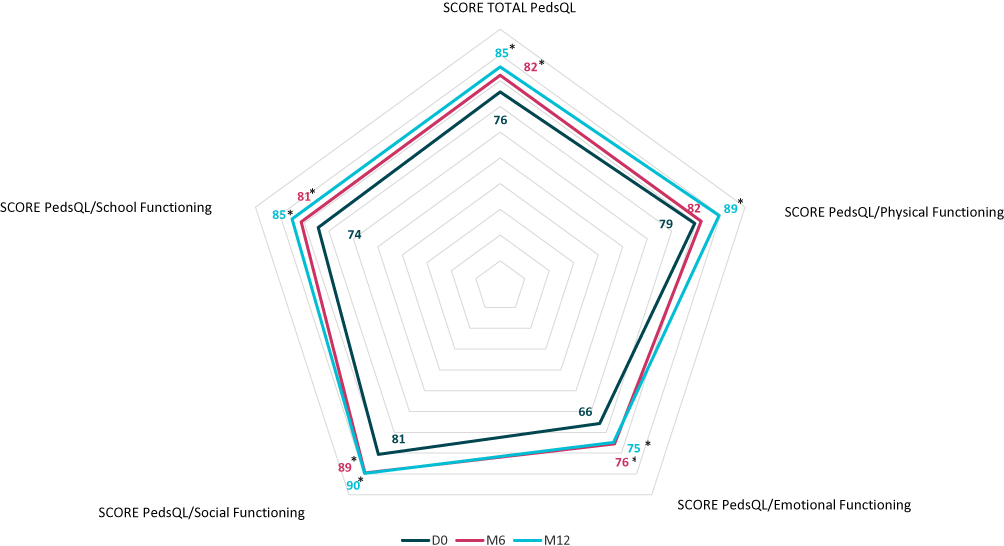 |
Figure 2 Mean change from baseline in PedSQL Generic Core Scales summary scores (Global and sub-domains Physical, Emotional, Social, School functioning) after 6 and 12 months aXess supports. *p < 0.05 for all changes from baseline. |
The mean total scores improved from baseline to month 6 and month 12. By month 6, the best results were seen in the emotional, social, and school domains. No statistically significant improvement was observed in the physical domain (82.0 ± 0.3 at month 6 versus 79.4 ± 0.3 at enrollment, Tables 3–5 and Figure 2). By month 12, the majority of patients reported an improvement in QOL in all measured domains (physical, emotional, social, and school, 85.4 ± 0.2 at month 12 versus 75.6 ± 0.3 at enrollment, Tables 3–5 and Figure 2).
Figure 3 displays the mean survey scores for the PedsQL-2 survey.
 |
Figure 3 Percentage of response to each PedSQL questionnaire item provided by XLH patients supported by aXess support program at DO, M6 and M12 - subgroups of patients initiating treatment and patients already receiving treatment. |
At month 6, both groups reported greater improvement in their emotional functioning (24% and 11% increase, respectively, from day 0). The number of patients reporting feeling sad, feeling angry or having trouble sleeping substantially decreased after 6 months.
At month 12, while patients starting treatment reported a greater benefit in their physical functioning (a 13% rise in score globally and 100% of patients reported that doing chores around the house, lifting something heavy, and taking a shower or a bath by themselves, was never a problem after 12 months), patients already on treatment reported a greater improvement in their school performance (16% score increase, 61% at D0 versus 83% at month 12 reported that paying attention at school was never a problem).
PedsQL scores were further analyzed by (1) whether the patient was in pre- or post-puberty, (2) according to their genetic status (de novo or familial XLH disease). These two variables did not significantly affect mean total QOL scores (data not shown).
Patients’ Satisfaction
Overall, patients were very satisfied with the patient support program. At month 6, participants reported a highly positive impact on their quality of life (patients rated their global satisfaction as 9.8 ± 0.6 on the 1–10 numerical scale) and a very favorable influence on treatment adherence from having access to the aXess program (Table 6).
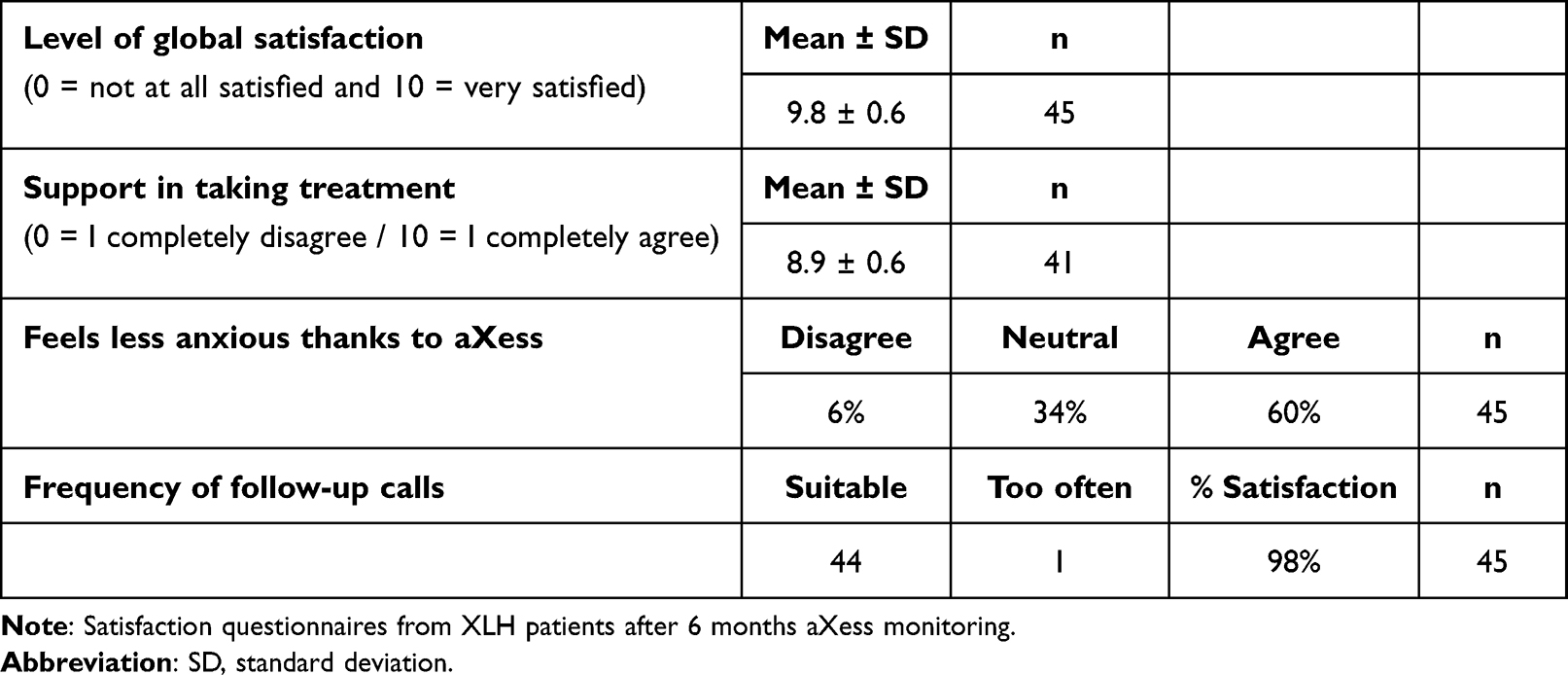 |
Table 6 Perception of the Usefulness of the Patient Support Program After 6 Months aXess Monitoring |
60% of patients reported feeling less anxious thanks to the aXess program, and 98% were satisfied with the frequency of follow-up calls.
At month 12, participants rated their global satisfaction as 9.2 ± 1.5 on the 1–10 numerical scale. The decreased anxiety of living with XLH was evident for 52% of participants reporting reduced stress levels from being on the aXess program, and 97% were satisfied with the frequency of follow-up calls (Table 7).
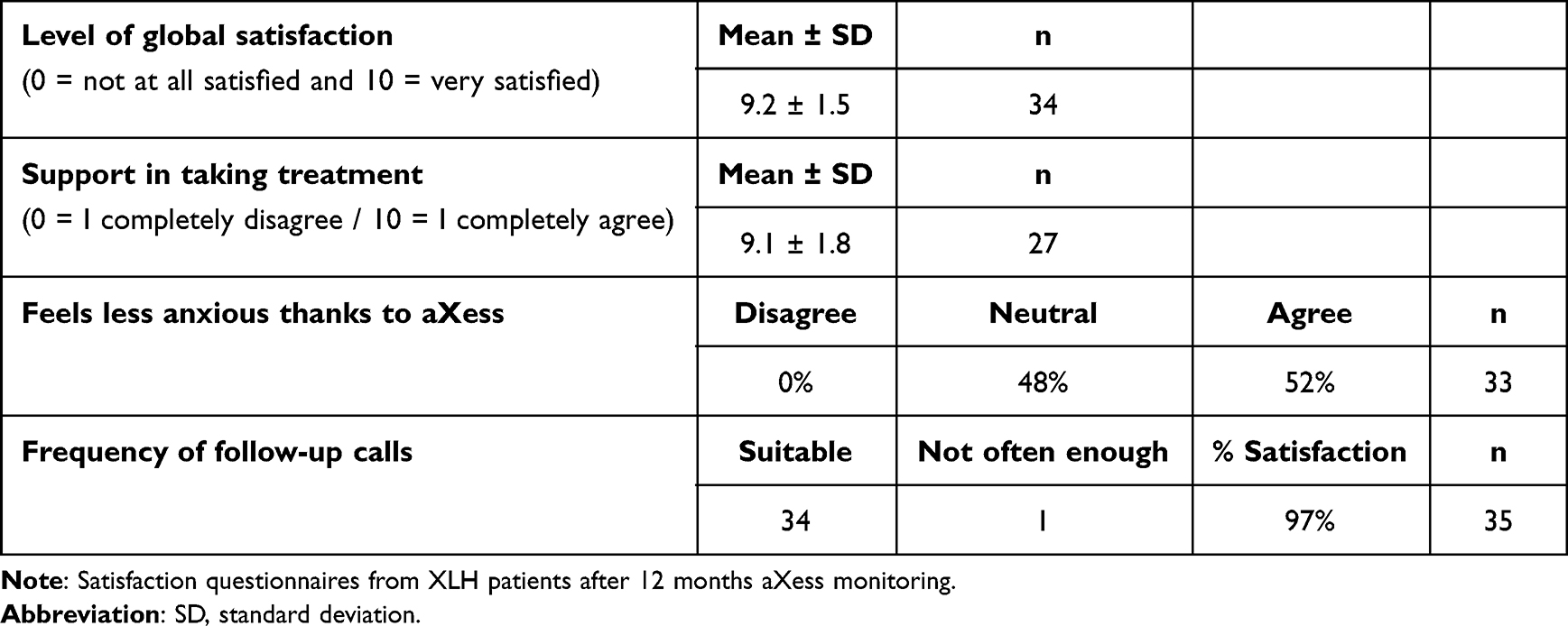 |
Table 7 Perception of the Usefulness of the Patient Support Program After 12 Months aXess Monitoring |
Discussion
XLH is a chronic disorder associated with many complications. The numerous clinical manifestations and symptoms of XLH can have a significant impact on physical function, psychological state, emotions, and general quality of life.
Anxiety, distress, lack of confidence, and low self-esteem are common manifestations of psychological burden in children with chronic diseases, affecting their social relationships and scholastic experience.15
Taken together, these issues may all contribute to a lower health-related quality of life in children with XLH, and one of the main concerns in patients with chronic disorders is to achieve optimal adherence to treatment.
Living with XLH poses a major strain. This multifaceted symptomatology condition has an impact on many aspects of children’s lives. In addition, any chronic condition has the potential to have an influence on the family’s quality of life.
However, little is known regarding the impact of XLH on children’s everyday lives. Therefore, we sought to assess the potential impact of a patient support program in assisting patients and their families in adherence to therapy and their condition management.
Over the period of 2019–2021, the aXess program enrolled 59 patients. Significant improvements in patient challenges were observed over the course of the patient support program.
This study describes the benefit of the aXess patient support program on HRQOL in young patients with XLH, as reported by patients on the PedsQL-2.
Not surprisingly, the majority of patient-requested calls came from patients who were just starting targeted therapy at the time of enrolment, suggesting a greater reliance on the support service.
Interestingly, patients who had previously received targeted treatment had higher QOL scores than patients who had just begun treatment; however, these differences did not reach statistical significance, most likely due to our small sample size.
Improvements in all domains were significant in patients already receiving therapy at months 6 and 12, which was presumably explained by the larger number of patients in this subgroup.
Notably, at month 6, patients consistently reported that they experienced the highest improvement in emotional functioning across all groups. In addition, after 12 months, patients reported significant improvements in their physical and school performances.
Because XLH is a chronic pediatric condition featuring severe symptoms, these findings suggest that it requires a longer period for physical function to improve after therapy is initiated.
More than half of patients reported feeling less anxious thanks to the program. A vast majority of patients rated the support in taking treatment as highly positive (8.9 ± 0.6 and 9.1 ± 1.8 scores at month 6 and month 12, respectively).
Our analysis, however, is not without limitations. First, due to the rarity of the disease, our cohort has a limited number of patients, making it unsuitable to conduct age-specific group analyses or establish a control group. Moreover, while after 6 months, patients who initiated treatment demonstrated significant improvement in all four components of QOL, this significance did not persist after 12 months except for the school functioning domain. This could be attributed to the small number of patients in the 12-month group; thus, it would be interesting to validate the observed improvement in quality of life in a wider population through a larger international study.
Furthermore, because our study lacked a comparator, it would be necessary to determine if the increase in patients’ quality of life was due to the program or the initiation of targeted treatment. The majority of patients (43 patients, 73%) were already on targeted treatment when they were enrolled in the program. Interestingly, our findings show an increase in the quality of life of these patients who were already on treatment, suggesting that the program itself has a favorable effect on the quality of life irrespective of treatment initiation.
Conclusions
According to this study, patients value support from patient support programs like aXess when coping with XLH with a mean overall satisfaction score of 9.8 ± 0.6 (on a scale from 0 to 10) at month 6 and 9.2 ± 1.5 at month 12.
This patient support program was associated with improved patient quality of life in all examined dimensions by month 12 (physical, emotional, social, and school, 85.4 ± 0.2 at month 12 versus 75.6 ± 0.3 at enrollment, p<0.05) and constitutes a cornerstone of the young patient’s care pathway. Assistance with treatment initiation and compliance, understanding their disease, reducing anxiety, and assisting them in becoming self-sufficient contribute to overall improved quality of life. The program links the home environment and overall illness management, bringing together patients, families, and caregivers.
Our observations suggest that this program provides important information regarding children’s and their families’ perceptions on living with XLH and their reported positive experiences with the aXess program. This data may be used to encourage long-term planning of support programs, as well as to highlight the vital need for such services within the healthcare system. Finally, because XLH children’s quality of life is directly tied to the QOL of those around them, investigating the impact and understanding the needs of family members would aid in providing adequate assistance to XLH patients and their caregivers. Based on these preliminary results obtained in France a larger multicentric study involving a larger number of countries would be of great interest.
Data Sharing Statement
Datasets analyzed during the current study are not publicly available but are obtainable from the corresponding author on reasonable request. As part of the aXess support action, patients, their legal representatives, and healthcare professionals grant the right to use the data for communication purposes.
Ethics Approval
The data presented here is collected as part of a patient support program (PSP), according to article 84 of French law n°2009-879 of July 21, 2009. These data were not collected as part of a clinical study, so no ethics committee is seized or competent in this context. The ethics committee CER U-Paris Cité certifies that the research leading to the proposed publication did not need approval from an ethical committee. Regarding data protection, they checked that it was conducted with respect to the law.
Although these data are not collected as part of medical research, the authors confirm that all the guidelines outlined in the Declaration of Helsinki have been followed.
Consent to Participate
Prior to the start of the program, all consents were obtained from the PSP participants’ parents or legal guardians (forms available on request).
Funding
aXess is a patient program managed by Patientys-Webhelp Medica and financially supported by Kyowa Kirin Pharma.
Disclosure
JB, AR and LL report speaker and consulting fees from Kyowa Kirin. AL received fees through her institution for the Phase I/II trial and a research grant from Kyowa Kirin International. LN is an employee of Webhelp Medica. IG reports consulting fees from XLH registry advisory board, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Pavone V, Testa G, Gioitta Iachino S, Evola FR, Avondo S, Sessa G. Hypophosphatemic rickets: etiology, clinical features and treatment. Eur J Orthop Surg Traumatol. 2015;25(2):221–226. doi:10.1007/s00590-014-1496-y
2. Aono Y, Yamazaki Y, Yasutake J, et al. Therapeutic effects of anti-FGF23 antibodies in hypophosphatemic rickets/osteomalacia. J Bone Miner Res. 2009;24(11):1879–1888. doi:10.1359/jbmr.090509
3. Carpenter TO, Imel EA, Holm IA, de Beur SM J, Insogna KL. A clinician’s guide to X-linked hypophosphatemia. J Bone Miner Res. 2011;26(7):1381–1388. doi:10.1002/jbmr.340
4. Haffner D, Emma F, Eastwood DM, et al. Clinical practice recommendations for the diagnosis and management of X-linked hypophosphataemia. Nat Rev Nephrol. 2019;15(7):435–455. doi:10.1038/s41581-019-0152-5
5. Lambert AS, Zhukouskaya V, Rothenbuhler A, Linglart A. X-linked hypophosphatemia: management and treatment prospects. Joint Bone Spine. 2019;86(6):731–738. doi:10.1016/j.jbspin.2019.01.012
6. Rothenbuhler A, Schnabel D, Hogler W, Linglart A. Diagnosis, treatment-monitoring and follow-up of children and adolescents with X-linked hypophosphatemia (XLH). Metabolism. 2020;103S:153892. doi:10.1016/j.metabol.2019.03.009
7. Skrinar A, Dvorak-Ewell M, Evins A, et al. The lifelong impact of X-linked hypophosphatemia: results from a burden of disease survey. J Endocr Soc. 2019;3(7):1321–1334. doi:10.1210/js.2018-00365
8. Zhukouskaya VV, Rothenbuhler A, Colao A, et al. Increased prevalence of overweight and obesity in children with X-linked hypophosphatemia. Endocr Connect. 2020;9(2):144–153. doi:10.1530/EC-19-0481
9. Basch E, Deal AM, Kris MG, et al. Symptom monitoring with patient-reported outcomes during routine cancer treatment: a randomized controlled trial. J Clin Oncol. 2016;34(6):557–565. doi:10.1200/JCO.2015.63.0830
10. Ganguli A, Clewell J, Shillington AC. The impact of patient support programs on adherence, clinical, humanistic, and economic patient outcomes: a targeted systematic review. Patient Prefer Adherence. 2016;10:711–725.
11. Scotte F. The importance of supportive care in optimizing treatment outcomes of patients with advanced prostate cancer. Oncologist. 2012;17(Suppl 1):23–30. doi:10.1634/theoncologist.2012-S1-23
12. Rubin DT, Mittal M, Davis M, Johnson S, Chao J, Skup M. Impact of a patient support program on patient adherence to adalimumab and direct medical costs in crohn’s disease, ulcerative colitis, rheumatoid arthritis, psoriasis, psoriatic arthritis, and ankylosing spondylitis. J Manag Care Spec Pharm. 2017;23(8):859–867. doi:10.18553/jmcp.2017.16272
13. Prèvot G, Stevens J, Leguay A, Brier T, Meijer J, Aguilaniu B. OPALE accompagnement des patients traitÈs pour une fibrose pulmonaire idiopathique. Rev Mal Respir. 2019;36:A142.
14. Varni JW, Seid M, Kurtin PS. PedsQL 4.0 : Reliability and Validity of the Pediatric Quality of Life Inventory Version 4.0 Generic Core Scales in Healthy and Patient Populations. Medical Care. 2001;39(8):800–812.
15. Pinquart M. Self-esteem of children and adolescents with chronic illness: a meta-analysis. Child Care Health Dev. 2013;39(2):153–161. doi:10.1111/j.1365-2214.2012.01397.x
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Sleep Disturbances in Chinese Children with Epilepsy: Associations with Behavioral Problems and Quality of Life
Zhao F, Sun X, Wang Y, Zhou Y, He Y, Wang C, Han F, Liu J, Tsai SY, Wang G, Wang J
Nature and Science of Sleep 2022, 14:1225-1236
Published Date: 2 July 2022
Improving Psychological Health Outcomes in Children with Atopic Dermatitis
Mostafa N, Smith SD
Clinical, Cosmetic and Investigational Dermatology 2023, 16:2821-2827
Published Date: 10 October 2023
Gender and Age Differences in the Relationship Between Smartphone Addiction and Sleep Duration in Korean Children: A Panel Quantile Regression Study
Jeong K, Cho S, Song D, Li R, Han S, Cho HJ, Kim J
Psychology Research and Behavior Management 2024, 17:4183-4192
Published Date: 8 December 2024
Unheard Struggles: Exploring Health-Related Quality of Life Determinants and Coping Mechanisms Among Children with Hearing Loss from Parents and Caregivers Perspective
Lone A
Risk Management and Healthcare Policy 2025, 18:1241-1255
Published Date: 8 April 2025
Impact of Intravenous Ferric Carboxymaltose on Quality of Life in Patients with Iron Deficiency Anemia: A Prospective Observational Study
Bozkuş R, Gemcioğlu E, Sarışen Ş
International Journal of General Medicine 2025, 18:7459-7469
Published Date: 10 December 2025