Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 15
“You Leave There Feeling Part of Something”: A Qualitative Study of Hospitalized COPD Patients’ Perceptions of Pulmonary Rehabilitation
Authors Spitzer KA ![]() , Stefan MS, Drake AA
, Stefan MS, Drake AA ![]() , Pack QR
, Pack QR ![]() , Lagu T
, Lagu T ![]() , Mazor KM, Pinto-Plata V, Lindenauer PK
, Mazor KM, Pinto-Plata V, Lindenauer PK
Received 16 October 2019
Accepted for publication 24 January 2020
Published 17 March 2020 Volume 2020:15 Pages 575—583
DOI https://doi.org/10.2147/COPD.S234833
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Video abstract presented by Kerry Spitzer.
Views: 438
Kerry A Spitzer, 1 Mihaela S Stefan, 1–3 Aubri A Drake, 1 Quinn R Pack, 1– 4 Tara Lagu, 1, 2 Kathleen M Mazor, 5 Victor Pinto-Plata, 6 Peter K Lindenauer 1, 3, 7
1Institute for Healthcare Delivery and Population Science, University of Massachusetts Medical School-Baystate, Springfield, MA, USA; 2Department of Internal Medicine, Baystate Medical Center, Springfield, MA, USA; 3Department of Medicine, University of Massachusetts Medical School-Baystate, Springfield, MA, USA; 4Division of Cardiovascular Medicine, Baystate Medical Center, Springfield, MA, USA; 5Meyers Primary Care Institute, a Joint Endeavor of the University of Massachusetts Medical School, Reliant Medical Group, and Fallon Health, Worcester, MA, USA; 6Pulmonary and Critical Care Medicine Division, Baystate Medical Center, Springfield, MA, USA; 7Department of Population and Quantitative Health Sciences, University of Massachusetts Medical School, Worcester, MA, USA
Correspondence: Kerry A Spitzer
Institute for Healthcare Delivery and Population Science University of Massachusetts Medical School-Baystate, 3601 Main Street, Springfield, MA 01199, USA
Tel +1 413-794-7909
Email [email protected]
Rationale: Current guidelines recommend that patients hospitalized for acute exacerbations of chronic obstructive pulmonary disease (COPD) initiate pulmonary rehabilitation (PR) shortly after discharge from the hospital. However, fewer than 2 percent of Medicare beneficiaries do so. Few studies have examined hospitalized patients’ perceptions of the barriers and facilitators to enroll in PR. The aim of this study was to develop an understanding of these factors by interviewing patients.
Methods: We conducted semi-structured interviews with patients during a hospitalization for COPD exacerbation in a large teaching hospital. Directed content analysis was used to code and analyze interview transcripts.
Results: Of the 15 patients we interviewed, 9 had participated in PR prior to their hospitalization, 10 were women; 4 were black, and 1 was Hispanic. Facilitators of enrollment included a desire to learn more about the disease, social support, and trust in the health-care provider recommending PR. Barriers to enrollment included lack of awareness, family obligations, lack of motivation, and transportation. For those who had previous experience with PR, but who did not complete the program, another barrier was not feeling well enough. Facilitators to adherence included the educational component of the program; feeling better through exercise; and a social connection with both participants and staff. For some patients. PR contributed to a renewed sense of hope or meaning. Most interviewees expressed interest in a peer coaching program.
Conclusion: Our results highlight the importance of increasing awareness of PR and building trust between the provider and patients to facilitate initial enrollment. Future interventions to improve enrollment and adherence should address the need for education about the benefits of PR and the value of social support.
Keywords: chronic obstructive pulmonary disease, COPD, pulmonary rehabilitation, hospitalization, patient perspectives
Introduction
Annually, over 1.5 million individuals visit the emergency department and approximately 700,000 are hospitalized for Chronic Obstructive Pulmonary Disease (COPD).1 The period after hospitalization is characterized by vulnerability, over half of Medicare beneficiaries hospitalized for COPD will be readmitted within a year and mortality rates approach 26%.2 Pulmonary rehabilitation (PR) is an exercise therapy and self-management program for people with lung disease, including COPD. Randomized control trials and meta-analyses have shown that PR reduces hospital readmissions and improves quality of life.3,4 Current guidelines for the management of COPD exacerbations recommend that patients hospitalized for an acute exacerbation of COPD begin PR shortly after discharge.5 Despite these recommendations, studies have shown that PR is underutilized in the US;6,7 fewer than 2% of Medicare beneficiaries hospitalized for COPD in the US in 2012 received PR within 6 months of their index hospitalization.8 These studies highlight the gap between current guidelines and clinical practice but leave unanswered the question of why so few patients attend PR.
Qualitative research on the experience of living with COPD has highlighted how this chronic disease severely limits individuals’ everyday lives.9 Fear and anxiety about breathlessness and reliance on home oxygen lead to social isolation.10 The stigma associated with the disease prevents individuals from seeking help,11 and those living with COPD often have limited knowledge of their disease and their prognosis, and unmet physical, social, and emotional needs.12 The time when patients are hospitalized is a potential opportunity to engage in a conversation about PR and encourage participation in this underutilized treatment program. While prior qualitative studies have explored why so few people enroll in PR in the outpatient clinical setting,13 to our knowledge, no study in the US has focused on enrollment in PR following a hospitalization for COPD. The purpose of this study was to develop an understanding of patients’ awareness and perceptions of PR and to identify barriers and facilitators to their attending and completing PR upon discharge from the hospital.
Methods
Setting and Design
We conducted in-depth, semi-structured interviews with patients hospitalized for COPD at Baystate Medical Center, a large, urban, teaching hospital in Springfield, Massachusetts that cares for more than 700 patients each year for exacerbation of COPD. The Baystate Health Institutional Review Board approved this study. All participants provided written informed consent prior to data collection.
Patient Selection and Consent
We reviewed the hospital electronic medical record to identify potential subjects for the study. We included patients who were hospitalized for COPD with acute exacerbation; were English-speaking; were not being discharged with hospice services; and were in a physical, neurological, or psychological state where they could communicate. We used purposive sampling to ensure that we included patients of different ages and races. The research team approached patients in the hospital explained the study, and obtained written informed consent. Interviews were conducted in the patients’ hospital rooms (single or double rooms); all participants were offered the opportunity to conduct the interview in a private location. Participants received a $50 gift card for participation.
Data Collection
The interviews covered questions about the patients’ initial diagnosis with COPD; how COPD had affected their lives; the medications that they took to manage their disease; their familiarity with pulmonary rehabilitation; barriers and facilitators in regards to pulmonary rehabilitation participation; and reactions to three interventions we hypothesized would increase enrollment in PR. Interviews ranged from 11 to 29 mins in length. For the purposes of this analysis, we focused on responses to questions related to PR. We collected demographic information including gender, age, race, ethnicity, education, and smoking history. We assessed COPD severity using the modified medical research council Dyspnea Scale (mMRC), which measures functional impairment attributable to dyspnea;14–16 and the COPD assessment test (CAT), which measures the impact of COPD on a person’s life.17 We obtained admitting diagnosis, principal diagnosis, and comorbidities from patient medical records. The interview guide and questionnaire are available in the Supplement.
Transcription and Analysis
Interviews were audio-recorded and transcribed verbatim. Transcripts were analyzed and coded using NVivo 12. Demographic questionnaire responses and clinical data were associated with interview data in NVivo and allowed us to explore whether themes emerged on the basis of these characteristics. We used directed content analysis; our initial codebook was created based on a review of the qualitative literature related to PR and COPD and informed by our interview guide. As we conducted and coded interviews we included emergent codes.18 Interviews were coded iteratively and concurrently with participant recruitment. We continued conducting interviews until we achieved heterogeneity in the participants on the basis of race and ethnicity and reached thematic saturation. The codebook was refined through regular team meetings where a team of five researchers came together to review and discuss the first four interviews. Through this process, the codebook was expanded and refined until we reached agreement on codes and definitions. Subsequently, three team members coded portions of all 15 interviews. One researcher coded all 15 interviews (KS) for all codes; another researcher (AD) was responsible for coding for themes related to the experience of COPD and the other (MS), for codes related to attitudes toward, and barriers and facilitators of PR. Disagreement on codes was discussed in team meetings and resolved through consensus.
Research Team and Reflexivity
The interviews were conducted by female (KS) and non-binary (AD) clinical research coordinators. KS holds a PhD and AD holds an MSW; both have experience with qualitative methods. Interviewers had no prior relationship with the participants and were not involved in their clinical care. The five coders included the clinical research coordinators who conducted the interviews (KS and AD) and three practicing physicians (MS, QP, and TL) who had no involvement in participants’ care.
Results
Participant Characteristics
We approached 35 patients of whom 11 were found to be ineligible, 14 declined, and 15 agreed to be interviewed. Interviews were conducted from August 2017 through April 2018 (Table 1). The majority were female (n=10), and white, non-Hispanic (n=10). The patients’ ages ranged from 45 to over 90 years. The highest level of education obtained was an associate’s degree (n=2). Every patient reported a history of smoking, and 5 patients had smoked in the 30 days prior to hospitalization. COPD assessment test and the modified medical research council Dyspnea Scale (mMRC) scores confirmed that the majority of participants had advanced COPD. We did not screen for prior PR experience, but 9 of 15 patients had attended at least one PR session prior to their current hospitalization.
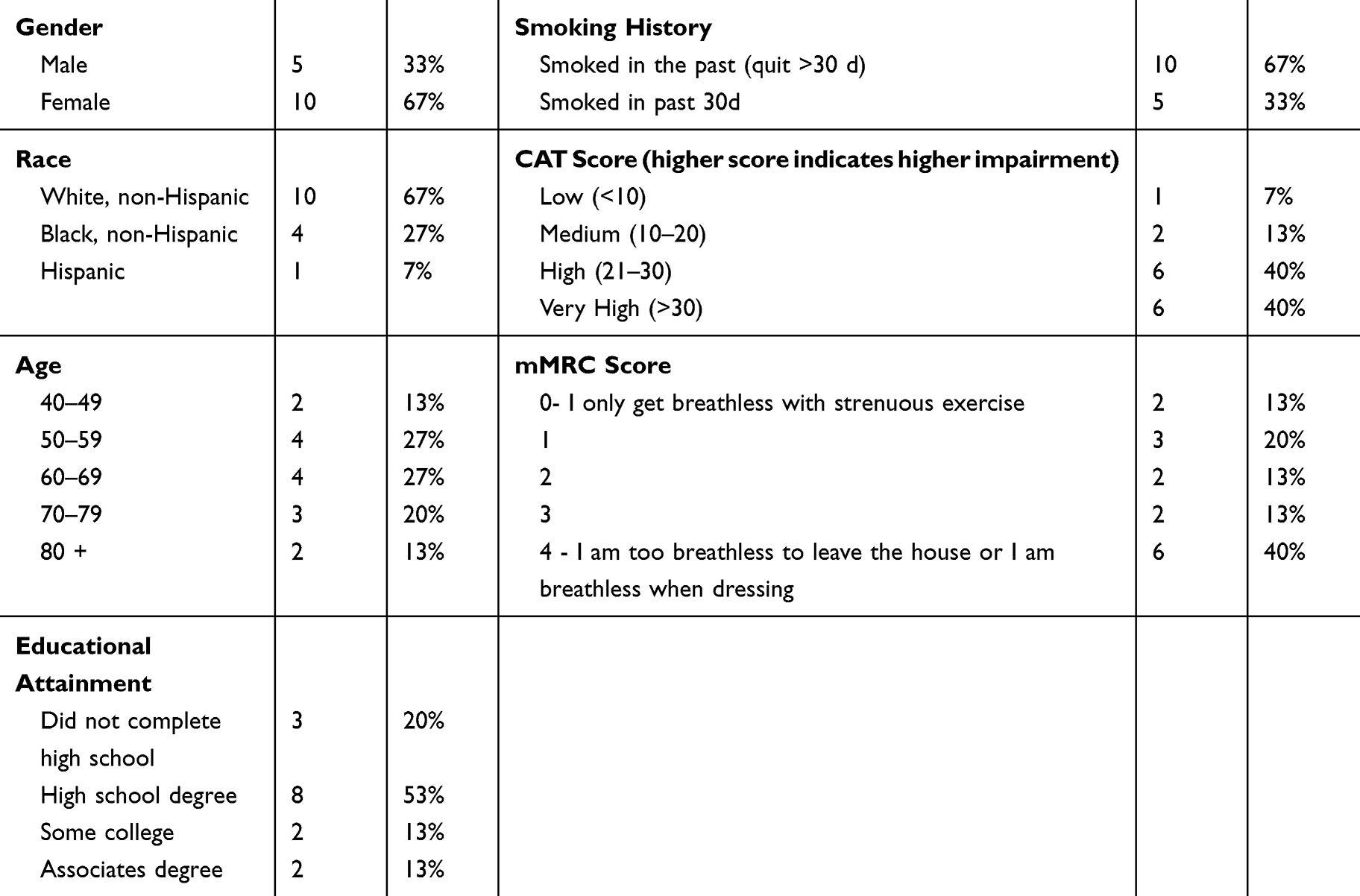 |
Table 1 Interviewee Characteristics |
Interview Themes
Figure 1 presents the themes and subthemes that we identified.
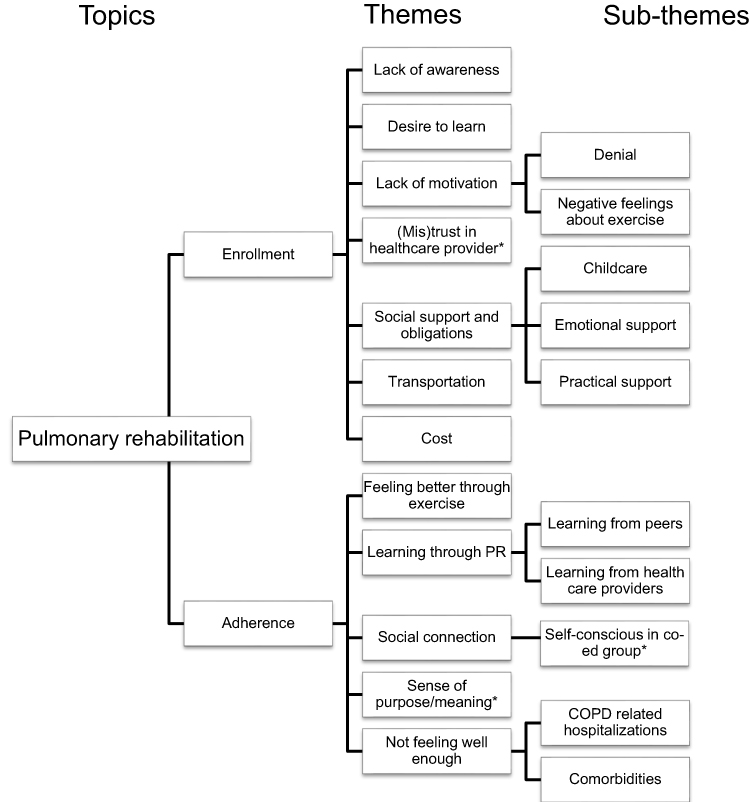 |
Figure 1 Theme and subthemes. Note: *Indicates emergent themes; other themes were present in the preliminary codebook. |
Enrollment in PR
Lack of Awareness of PR
No one reported having refused PR. Those who had never attended PR reported no awareness of PR. For example, a typical exchange in the interviews was:
Interviewer: And are you familiar with the idea of pulmonary rehabilitation?
Interviewee: No, I have no idea what it is. No.
Desire to Learn
While all participants were hospitalized for an acute exacerbation of COPD, they were at different stages in their understanding of their diagnosis. The desire to learn more about COPD was a common theme and one that is relevant to PR, which includes a strong educational component. Some patients were confused about the cause of the disease while others blamed themselves for smoking. Many patients conveyed a strong desire to learn more. A few had turned to social media in order to learn from others with COPD. One woman who had no experience with PR expressed her fear and desire to learn more about COPD:
I was very afraid […] Because it’s like, whoa. I don’t know what it [COPD] is. I don’t know how it works. I don’t know anything about it. That was a big factor, the fear of it, the unknown, I guess. But I would really like to learn, again, how to live with it more successfully.
Individuals who had not participated in PR often asked the interviewers questions about their prognosis. Typical comments included: “It’s like how the hell do I get rid of it [COPD]?” and “Will the lungs improve at all?” Others reflected on their frustration with their lack of information about the disease and its progression.
And I’ve been living with it since [the initial diagnosis] and it’s been deteriorating since. Haven’t gotten better, so I just found out that it ain’t gonna get any better […] And I’ve just been learning to cope with it every day and try to understand it, but nobody is really giving me information on it. I don’t know what to expect. I didn’t know I was gonna get worse.
Lack of Motivation
Several of the participants who had attended PR reflected on their initial lack of interest in PR and the belief that they did not need to change their lives or behaviors to adapt to the disease. One man remarked:
A lot of people say, “I’m feeling okay, I’m doing good.” They don’t realize, the first couple years – I know people that – I was one of them. When I was diagnosed with emphysema, I still smoked for a couple years.
Another woman spoke about her lack of interest in exercise:
it took me a lot to go the first time, because I really didn’t – I thought it was going to be a pain in the ass. Who wants to exercise? I can’t breathe.
Trust in Healthcare Providers
Those who had successfully enrolled in PR often cited the role of a health-care provider, beyond a simple referral, in motivating them. A perception of sincerity translated into trust in the provider, and facilitated enrollment in PR. “The therapist was sincere enough, probably even more so than a doctor would have been.” “I love my pulmonologist. I would stand on my head for him.”
Two individuals who had attended PR reflected on the belief that some patients are mistrustful of health-care workers and believe they are only motivated by their paychecks. One woman stated:
A lot of people think like that, because I was one of them, “I’m just another check,” and it took one lady to show me that I wasn’t; because I had several come to my house. Once I said, “I don’t want to be bothered,” they left, but I really wanted to be bothered. I wanted somebody to […] show me that I’m just not another check to you; […] and then one lady[…] came out greeted me and then after started sitting and having coffee with me and it encouraged me, okay, I’m going to do this, and when I got there [PR], she was my trainer. It worked out really good for me.
Social Support and Obligations
A theme among those who did attend PR was a strong social support network that provided both emotional support and practical assistance with appointments. One man in his 40s relied on his brother to drive him to PR. He felt motivated to attend not just for himself but for his family:
I got nine brothers and a mean mama […] If I don’t go to rehab and do the things that the doctor recommends, I’m going to hear it to the end of the moon, so I’d rather just go and do it than to hear it from my family.
Some respondents, especially women, identified family obligations which prevented them from attending PR. One woman noted:
But when it gets too close to like three o’clock in the afternoon, I can’t because I know my granddaughter is coming out of school.
Transportation
For many, transportation was an issue in either initiating or regularly attending PR. One woman who completed PR in an outpatient setting noted that she would have liked to have attended additional sessions, “but I don’t have access to back and forth now.”
Cost
Cost was infrequently cited as a direct barrier by our interviewees; only two indicated that cost would be a barrier, though many suggested that it might be a barrier for individuals without insurance.
Adherence to Pulmonary Rehabilitation
Many of the factors that influenced peoples’ decisions to attend PR initially also influenced their ability and willingness to adhere. Below we discuss several factors that were unique to adherence.
Feeling Better Through Exercise
Among those who attended several sessions, feeling better physically became a facilitator to continued adherence resulting in a positive feedback loop. One woman who had completed PR reported: “It gave you a little bit of life, a little bit of stamina, more than you could feel, like, all right, I can go up and walk down to the corner today.”
Learning Through PR
Education was a facilitator of adherence. One of the most cited benefits of PR was the learning that occurred: “Every day, we learned something new.” Individuals reported learning through the formal instruction and through their peers. A former PR participant remarked:
I really enjoyed the people a lot, learning about what I have to do with the COPD. Because like, you go twice a week to that and one of those days, once a month we go in a class and we talk for two hours. The instructor talks about COPD and this and that, which is really good because you need to know, you know?
Another stated: “And you’re meeting other people that have it and know more about it than you do, which is a good thing because you can learn from them.”
Social Connection
Many reported that they valued the social connection that they experienced through PR:
Yeah, I wouldn’t mind going back at all. You meet the people, and they have the same problems, so you get to talk about the same problems, you know, same thing, and I’m a people person.
The social connection was a facilitator of adherence, but aspects of exercising in a co-ed group left some of the PR participants uncomfortable. Two women noted that they felt self-conscious exercising in a group setting. One stated: “Well, you have to wear a pack, and you wear one of these [points to nasal cannula] […] you don’t like to be seen by people, but big, black glasses help.” Another woman when asked what she did not like about PR said: “There was guys there just doing it [PR exercises], just like the women were, and they were there just to watch the women exercise.”
Sense of Purpose or Meaning
The benefits of PR contributed to an additional reported outcome and facilitator of adherence: a renewed sense of hope or meaning through PR participation. For many who had completed PR the social connection, learning, and improved management of their COPD symptoms had given them a renewed sense of purpose or meaning.
Well, you learn things, you laugh a little bit. You exercise and you leave there feeling part of something, which sometimes means a lot.
The benefits of exercise for some went beyond feeling better; at least two of the interviewees had previously identified as athletes and with the diagnosis of COPD had felt the loss of their favorite activities. For example, one woman responded to the question about how COPD affected her life by saying: “I had to give up the love of my life, which was golfing.” In addition, one man had been a semi-pro athlete before learning that he had COPD. For these former athletes, the chance to return to a gym setting was a strong motivator.
Not Feeling Well Enough
Many reported that they started PR only to have it interrupted by injuries or hospitalizations. One woman remarked: “But, right after that [enrolling in PR], I ended up breaking my ankle and my leg […] So, I was in a cast so I couldn’t do the exercise anyway.” Another patient reported: “I did participate in pulmonary rehab, but then I just wasn’t feeling good, and I ended up in the hospital again.” In one instance a patient reported that he had started PR, but did not feel that it would make a difference because his disease had progressed so far. He stated, “The doctors, they asked me, and I signed up for it [PR]. Then I went. They’re saying that at this point now, just my lungs are too far gone. They’re not going to do me any good, going [to PR].”
Acceptability of Potential Interventions
We asked participants about their interest in three potential interventions to increase participation in PR: (1): meeting with PR staff during their hospital stay; (2) watching a video that shows the PR facility and individuals participating in PR; and (3) being paired with a “coach” who is also living with COPD and has successfully competed PR. There was broad support for all three. There was enthusiasm for talking with PR staff, particularly as a means of learning more about PR and knowing with whom they would work.
One woman stated: “Yes, like meeting the people beforehand so you have that connection. You know who you are going to be seeing when you come in.” When presented with the idea of meeting the PR staff one man stated:
Yeah, that’s a big thing. Have a team that’s here on the floor with people that are sick with the disease, have them come by before the person is discharged from the hospital, and have them come in and explain to them what they do, how they do it, how many times a day, week, whatever their schedule could be or whatever, and explain to them – say, we can find a way to get you there. […] There’s no literature in here for pulmonary rehabilitation.
Support for watching a video was also coupled with a desire to learn more. When presented with the idea of a video one woman stated: “Oh, yeah. Oh, yeah. Any – any information on that I’m eager to learn.”
The peer-coaching intervention sparked comments indicating interest in coaching as a means of learning from and connecting with a peer who has similar life experience:
They’ve [coaches] been there, they’ve done it. They know what you’re feeling, you know
You know, that would be great, because I think I’m the only one [with COPD] that I know.
We can go together, and exercise, and run out of breath together
Because I can ask questions, and they can tell me things I don’t know that I can learn.
One person was in favor of a coaching program, but pointed out that the effectiveness of the program would depend on the coach and peers’ attitudes: “It depends on the people that you tag up with. Some are going to be too grumpy over what they have and what they have to give up, and they aren’t going to want to talk for any reason.”
Discussion
Despite the lack of awareness of PR, our findings suggest that at the time of hospitalization patients are frequently enthusiastic about the prospect of enrolling in PR as a means of increasing their understanding of the disease, connecting with peers with COPD, and feeling better. Some patients expressed uncertainty about their ability to attend PR due to family obligations, such as childcare, as well as health concerns, including comorbidities. We also found that a lack of motivation to change behavior and mistrust of medical professionals are potential barriers to enrollment in PR. Patients who had attended PR expressed positive attitudes toward PR.
Prior studies examining patient factors related to enrolling in PR have often focused on barriers including a lack of acceptance of the disease, lack of knowledge of the disease or PR, a lack of internal motivation, feeling too ill, lack of social support, lack of transportation, current smoking, depression, and trouble setting goals.24–26 A handful of studies have also examined the reasons why patients fail to complete a full course of PR and have found that patients often drop out for similar reasons.22,27,28 Disler and colleagues organized existing qualitative research on the experience of advanced COPD into three broad analytical themes that are echoed in our findings: individuals’ needs to have a better understanding of their condition, the ongoing and sustained symptom burden, and the psychological impact of the condition.9 Similar to the work of Sohanpal and colleagues, we found that patients wanted to learn more about COPD and were enthusiastic about learning through PR and learning from peers.21 Related to symptom burden, those who had participated reported that PR reduced symptom burden, which encouraged adherence. This finding confirms the work of Thorpe and colleagues that “feeling better” is a strong facilitator of PR.23 Many who had participated in PR reported overcoming initial lack of motivation related to fear and anxiety around exercising and breathlessness, which has been documented in other studies as well.22 Finally, we found evidence to suggest that PR can help to alleviate the negative psychological aspects of the disease and increase social connection.
In addition, our work builds on the work of Harrison et al who suggested that interventions to promote PR need to be compassionate and encourage trust and safety.11 We found that some individuals are initially mistrustful of medical professionals and that sustained and sincere outreach may overcome this barrier to PR. Overall, patients were supportive of the proposed interventions of a visit from the PR staff and a video tour of the PR facility, which might help to facilitate stronger relationships between patients and medical professionals. Individuals were also interested in a peer-coaching program in which hospitalized patients would be connected to peers who have completed PR. Such a program could foster social connections, learning, and practical problem solving around logistics, such as transportation. In this way, peer-coaching might serve to supplement the social support that comes from family and friends, and serve as a bridge until when patients actually being PR.
Another takeaway is that starting the conversation about PR early, before the patient is discharged, might capitalize on a window of opportunity to engage with a patient. Surprisingly, interviews with the individuals with no prior PR experience suggest that many patients hospitalized for COPD are completely unaware of PR, although all expressed interest in learning more or enrolling. While patients are clearly burdened by their disease and the demands of a hospital stay, several also noted that they are a captive audience. In the words of one: “I’m not doing nothing.” Engaging in conversations about PR, and referring patients to PR, or follow-ups with a provider who is knowledgeable of PR, before discharge from the hospital would address the lack of awareness and might increase participation.
Strengths and Limitations
While not an intentional part of the design of this study, we had the advantage of interviewing individuals who had participated in PR and those who had never heard of PR. This allowed us to discuss how individuals overcame barriers to attending PR and hear their reflections on how to increase enrollment in PR. The fact that nine of the 15 people we interviewed had previously attended one or more sessions of PR suggests that our sample may not be representative of the larger population of people living with COPD. Furthermore, our study was conducted in Massachusetts, a state with nearly universal health insurance and relatively generous safety-net programs, which may mean that our finding that cost and transportation were not common barriers is not generalizable outside of the state. Furthermore, we only interviewed individuals who spoke English and individuals who speak a language other than English are likely to face unique barriers to PR tied to language and culture. Nonetheless, our strategy to purposefully sample meant that we spoke with men and women from different racial and ethnic backgrounds.
Conclusion
Our results highlight the importance of increasing awareness of PR and building trust between provider and patient to facilitate initial enrollment following a hospitalization for COPD. They also indicate the importance of education, the benefits of exercise, and increased social connections in encouraging participation. Future research should explore whether an educational intervention combined with peer-coaching could help to increase rates of PR, while also encouraging social connection.
Acknowledgments
The research was supported by the National Heart, Lung, And Blood Institute of the National Institutes of Health under Award Numbers K24HL132008 and R01HL133046. The funders had no role in data collection, management, analysis; study design, conduct, or interpretation of study findings; or the preparation, review, or approval of the manuscript submitted for the publication. Dr. Pack was supported by a grant from the National Heart, Lung and Blood Institute of the National Institutes of Health of Bethesda, MD under award number 1K23HL135440.
Author Contributions
PKL and MS, conceived of and designed the study. KS and AD collected the data. KS, AD, MS, QP, and TL created the codebook and analyzed the data. All authors contributed to the interpretation of the results. KS drafted the manuscript. All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
Dr Victor Pinto-Plata reports being on the Advisory Board for GSK, BI, Sunovion, AZ. Dr Tara Lagu reports personal fees from Yale/CMS, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Ford ES, Croft JB, Mannino DM, Wheaton AG, Zhang X, Giles WH. COPD surveillance—United States, 1999–2011. Chest. 2013;144(1):284–305. doi:10.1378/chest.13-0809
2. Lindenauer PK, Dharmarajan K, Qin L, Lin Z, Gershon AS, Krumholz HM. Risk trajectories of readmission and death in the first year after hospitalization for chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2018;197(8):1009–1017. doi:10.1164/rccm.201709-1852OC
3. Puhan MA, Gimeno-Santos E, Cates CJ, Troosters T. Pulmonary rehabilitation following exacerbations of chronic obstructive pulmonary disease. In: The Cochrane Collaboration, editor. Cochrane Database of Systematic Reviews. Chichester, UK: John Wiley & Sons, Ltd; 2016. doi:10.1002/14651858.CD005305.pub4.
4. Moore E, Palmer T, Newson R, Majeed A, Quint JK, Soljak MA. Pulmonary rehabilitation as a mechanism to reduce hospitalizations for acute exacerbations of COPD. Chest. 2016;150(4):837–859. doi:10.1016/j.chest.2016.05.038
5. Wedzicha JA, Miravitlles M, Hurst JR, et al. Management of COPD exacerbations: a European respiratory society/American thoracic society guideline. Eur Respir J. 2017;49:3. doi:10.1183/13993003.00791-2016
6. Nishi SPE, Zhang W, Kuo Y-F, Sharma G. Pulmonary rehabilitation utilization in older adults with chronic obstructive pulmonary disease, 2003 to 2012. J Cardiopulm Rehabil Prev. 2016;36(5):375–382. doi:10.1097/HCR.0000000000000194
7. Vercammen-Grandjean C, Schopfer DW, Zhang N, Whooley MA. Participation in pulmonary rehabilitation by veterans health administration and medicare beneficiaries after hospitalization for chronic obstructive pulmonary disease. J Cardiopulm Rehabil Prev. 2018. doi:10.1097/HCR.0000000000000357
8. Spitzer KA, Stefan MS, Priya A, et al. Participation in pulmonary rehabilitation following hospitalization for COPD among medicare beneficiaries. Ann Am Thorac Soc. 2018. doi:10.1513/AnnalsATS.201805-332OC
9. Disler RT, Green A, Luckett T, et al. Experience of advanced chronic obstructive pulmonary disease: metasynthesis of qualitative research. J Pain Symptom Manag. 2014;48(6):1182–1199. doi:10.1016/j.jpainsymman.2014.03.009
10. Gysels M, Higginson IJ. Access to services for patients with chronic obstructive pulmonary disease: the invisibility of breathlessness. J Pain Symptom Manag. 2008;36(5):451–460. doi:10.1016/j.jpainsymman.2007.11.008
11. Harrison SL, Robertson N, Apps L, Steiner MC, Morgan MDL, Singh SJ. “We are not worthy” – understanding why patients decline pulmonary rehabilitation following an acute exacerbation of COPD. Disabil Rehabil. 2015;37(9):750–756. doi:10.3109/09638288.2014.939770
12. Clari M, Ivziku D, Casciaro R, Matarese M. The unmet needs of people with chronic obstructive pulmonary disease: a systematic review of qualitative findings. COPD. 2018;15(1):79–88. doi:10.1080/15412555.2017.1417373
13. Keating A, Lee A, Holland AE. What prevents people with chronic obstructive pulmonary disease from attending pulmonary rehabilitation? A systematic review. Chron Respir Dis. 2011;8(2):89–99. doi:10.1177/1479972310393756.
14. Mahler DA, Wells CK. Evaluation of clinical methods for rating dyspnea. Chest. 1988;93(3):580–586. doi:10.1378/chest.93.3.580
15. Henoch I, Strang S, Löfdahl C-G, Ekberg-Jansson A. Health-related quality of life in a nationwide cohort of patients with COPD related to other characteristics. Eur Clin Respir J. 2016;3. doi:10.3402/ecrj.v3.31459.
16. Chhabra SK, Gupta AK, Khuma MZ. Evaluation of three scales of dyspnea in chronic obstructive pulmonary disease. Ann Thorac Med. 2009;4(3):128–132. doi:10.4103/1817-1737.53351
17. Jones PW, Harding G, Berry P, Wiklund I, Chen W-H, Kline Leidy N. Development and first validation of the COPD assessment test. Eur Respir J. 2009;34(3):648–654. doi:10.1183/09031936.00102509
18. Hsieh H-F, Shannon SE. Three approaches to qualitative content analysis. Qual Health Res. 2005;15(9):1277–1288. doi:10.1177/1049732305276687
19. Benzo R, Wetzstein M, Neuenfeldt P, McEvoy C. Implementation of physical activity programs after COPD hospitalizations: lessons from a randomized study. Chron Respir Dis. 2014. doi:10.1177/1479972314562208
20. Meis JJM, Bosma CB, Spruit MA, et al. A qualitative assessment of COPD patients’ experiences of pulmonary rehabilitation and guidance by healthcare professionals. Respir Med. 2014;108(3):500–510. doi:10.1016/j.rmed.2013.11.001
21. Sohanpal R, Seale C, Taylor SJC. Learning to manage COPD: a qualitative study of reasons for attending and not attending a COPD-specific self-management programme. Chron Respir Dis. 2012;9(3):163–174. doi:10.1177/1479972312444630
22. Cox NS, CC O, Lahham A, Holland AE. Pulmonary rehabilitation referral and participation are commonly influenced by environment, knowledge, and beliefs about consequences: a systematic review using the theoretical domains framework. J Physiother. 2017;63(2):84–93. doi:10.1016/j.jphys.2017.02.002
23. Thorpe O, Kumar S, Johnston K. Barriers to and enablers of physical activity in patients with COPD following a hospital admission: a qualitative study. Int J Chron Obstruct Pulmon Dis. 2014;9:115–128. doi:10.2147/COPD.S54457
24. Harris D, Hayter M, Allender S. Improving the uptake of pulmonary rehabilitation in patients with COPD. Br J Gen Pract. 2008;58(555):703–710. doi:10.3399/bjgp08X342363
25. Benzo R, Wetzstein M, Neuenfeldt P, McEvoy C. Implementation of physical activity programs after COPD hospitalizations: lessons from a randomized study. Chron Respir Dis. 2015;12(1):5–10. doi:10.1177/1479972314562208
26. Janaudis-Ferreira T, Tansey CM, Harrison SL, et al. A qualitative study to inform a more acceptable pulmonary rehabilitation program after acute exacerbation of COPD. Ann Am Thorac Soc. 2019. doi:10.1513/AnnalsATS.201812-854OC
27. Sahin H, Naz I. Why are COPD patients unable to complete the outpatient pulmonary rehabilitation program? Chron Respir Dis. 2018;15(4):411–418. doi:10.1177/1479972318767206
28. Fischer MJ, Scharloo M, Abbink JJ, et al. Participation and drop-out in pulmonary rehabilitation: a qualitative analysis of the patient’s perspective. Clin Rehabil. 2007;21(3):212–221. doi:10.1177/0269215506070783
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.